Embed Size (px)
Citation preview

Neuro-Ophthalmology, 33, 36–38, 2009Copyright C© Informa Healthcare USA, Inc.ISSN: 0165-8107 print / 1744-506X onlineDOI: 10.1080/01658100802593104
Optical Coherence Tomographic Findingsin Susac Syndrome
Cengiz Aras, Sema Arvas, and Didar UcarDepartment of Ophthalmology,
Cerrahpasa Medical School,Istanbul University,
Istanbul, Turkey
ABSTRACT
Purpose: To report optical coherence tomographic (OCT) findings in Susac syndrome. Methods: A15-year-old girl who had symptoms of deafness and encephalopathy was referred with a provisionaldiagnosis of Susac syndrome. Funduscopy revealed cotton wool spots and ischaemic cloudy swellingof the retina. Results: OCT taken from the abnormal retinal area showed increased reflectivity of theinner retinal layers and decreased reflectivity from the outer retinal layers and the retinal pigmentepithelium due to shadowing. Neither intraretinal nor subretinal fluid were observed on the OCTimaging. OCT findings were compatible with the accepted view that the retinal pathology in Susacsyndrome is due to arteriolar occlusion. Conclusion: OCT may be used as a complementary diagnosticmethod to fluorescein angiography in Susac syndrome.
Keywords: optical coherence tomography; Susac syndrome
INTRODUCTION
Susac syndrome is a microangiopathy involving thebrain, cochlea, and retina.1 Ocular findings duringacute phase of the disease are retinal ischaemic whiten-ing (cloudy swelling caused by occlusion of branchretinal arterioles); cotton wool spots; opacification ofthe walls of retinal arterioles; box-car segmentation,and (where the macula is involved) a cherry-redspot. Flourescein angiography typically demonstratesleakage of affected arterioles which may or may not beassociated with signs of retinal infarction.2,3
Optical coherence tomography (OCT) is a noninvasivetechnique that obtains cross sectional retinal images.OCT may be helpful in the evaluation of retinal lesionsdue to different retinal pathologies. We report on OCTfindings in a case of Susac syndrome.
Accepted 1 November 2008
Address correspondence to Cengiz Aras M.D., 4 Kısım T.O. 94 BlokD1, Atakoy-Istanbul 34753-01, Turkey. E-mail: [email protected]
MATERIAL-METHODS
A 15-year-old girl with a provisional diagnosis ofSusac syndrome was referred from our NeurologyDepartment for an ophthalmic examination. She had ahistory of severe headaches, sudden onset of deafness,dysarthria and sphincter dysfunction. T2-weightedmagnetic resonance imaging (MRI) had revealed mul-tiple hyperintense lesions in the brain, both supra-and infra-tentorial. Examination of the cerebrospinalfluid showed a high protein, few lymphocytes and nooligoclonal bands on CSF protein electrophoresis. Diag-nostic laboratory studies including cerebrospinal fluidanalysis did not reveal any evidence of connective tis-sue disorder, procoagulant state or infectious disease.Electroencephalography showed diffuse bioelectricalslowing.
Visual acuities were 20/20 in both eyes. Ocularbiomicroscopic examination was normal bilaterally.Intraocular pressures with applanation tonometer were19 mmHg in the right eye (RE) and 20 mmHg in the lefteye (LE). Funduscopic examination with a 90-Diopter
36
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Lib
rary
of
Hea
lth S
ci-U
niv
of I
l on
12/0
1/14
For
pers
onal
use
onl
y.
Susac Syndrome
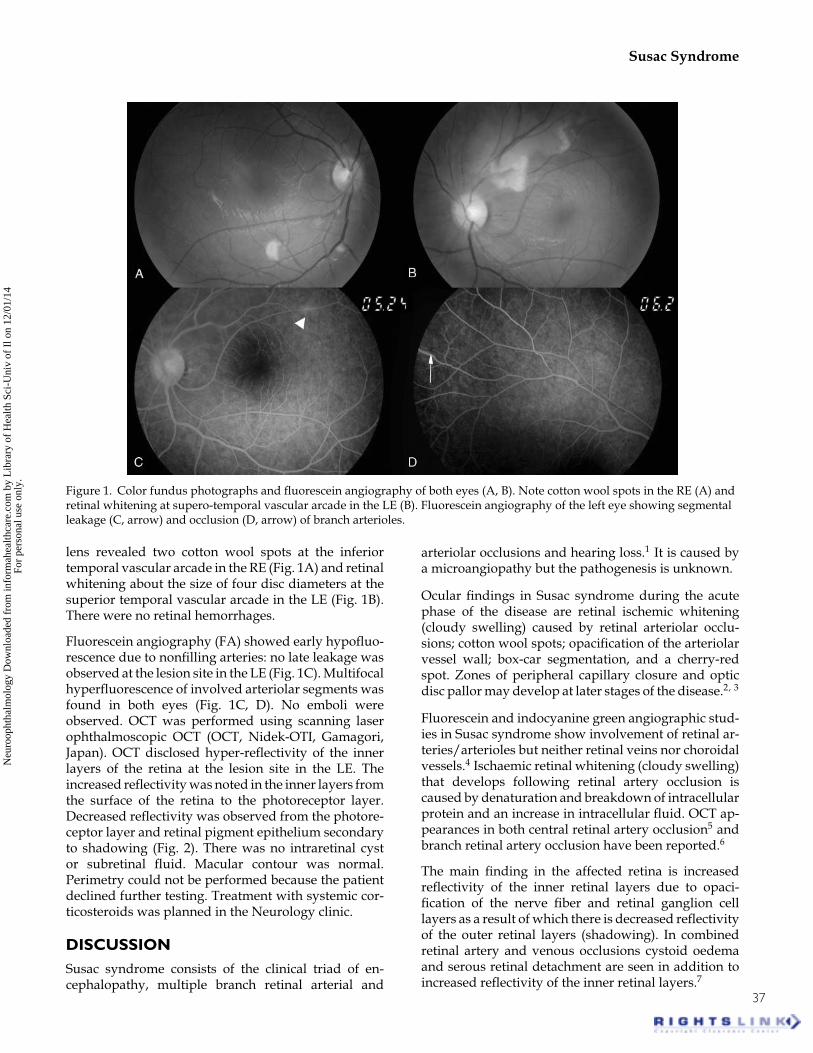
Figure 1. Color fundus photographs and fluorescein angiography of both eyes (A, B). Note cotton wool spots in the RE (A) andretinal whitening at supero-temporal vascular arcade in the LE (B). Fluorescein angiography of the left eye showing segmentalleakage (C, arrow) and occlusion (D, arrow) of branch arterioles.
lens revealed two cotton wool spots at the inferiortemporal vascular arcade in the RE (Fig. 1A) and retinalwhitening about the size of four disc diameters at thesuperior temporal vascular arcade in the LE (Fig. 1B).There were no retinal hemorrhages.
Fluorescein angiography (FA) showed early hypofluo-rescence due to nonfilling arteries: no late leakage wasobserved at the lesion site in the LE (Fig. 1C). Multifocalhyperfluorescence of involved arteriolar segments wasfound in both eyes (Fig. 1C, D). No emboli wereobserved. OCT was performed using scanning laserophthalmoscopic OCT (OCT, Nidek-OTI, Gamagori,Japan). OCT disclosed hyper-reflectivity of the innerlayers of the retina at the lesion site in the LE. Theincreased reflectivity was noted in the inner layers fromthe surface of the retina to the photoreceptor layer.Decreased reflectivity was observed from the photore-ceptor layer and retinal pigment epithelium secondaryto shadowing (Fig. 2). There was no intraretinal cystor subretinal fluid. Macular contour was normal.Perimetry could not be performed because the patientdeclined further testing. Treatment with systemic cor-ticosteroids was planned in the Neurology clinic.
DISCUSSIONSusac syndrome consists of the clinical triad of en-cephalopathy, multiple branch retinal arterial and
arteriolar occlusions and hearing loss.1 It is caused bya microangiopathy but the pathogenesis is unknown.
Ocular findings in Susac syndrome during the acutephase of the disease are retinal ischemic whitening(cloudy swelling) caused by retinal arteriolar occlu-sions; cotton wool spots; opacification of the arteriolarvessel wall; box-car segmentation, and a cherry-redspot. Zones of peripheral capillary closure and opticdisc pallor may develop at later stages of the disease.2, 3
Fluorescein and indocyanine green angiographic stud-ies in Susac syndrome show involvement of retinal ar-teries/arterioles but neither retinal veins nor choroidalvessels.4 Ischaemic retinal whitening (cloudy swelling)that develops following retinal artery occlusion iscaused by denaturation and breakdown of intracellularprotein and an increase in intracellular fluid. OCT ap-pearances in both central retinal artery occlusion5 andbranch retinal artery occlusion have been reported.6
The main finding in the affected retina is increasedreflectivity of the inner retinal layers due to opaci-fication of the nerve fiber and retinal ganglion celllayers as a result of which there is decreased reflectivityof the outer retinal layers (shadowing). In combinedretinal artery and venous occlusions cystoid oedemaand serous retinal detachment are seen in addition toincreased reflectivity of the inner retinal layers.7
37
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Lib
rary
of
Hea
lth S
ci-U
niv
of I
l on
12/0
1/14
For
pers
onal
use
onl
y.

C. Aras et al.
Figure 2. OCT image obtained from the area of retinal infarction showing cloudy swelling in the LE. There is increasedreflectivity of the nerve fiber layer and decreased reflectivity of photoreceptor layer and pigment epithelium. Note the absenceof intra or subretinal fluid.
OCT findings in Susac syndrome have not previouslybeen reported: in our case the OCT findings arecompatible with retinal arteriolar occlusion (Fig. 2).The absence of cystoid changes and subretinal fluidin our case confirms the lack of retinal venous andchoroidal involvement in the pathogenesis of cloudyswelling in Susac syndrome. Our findings lend furtherevidence that this disorder is caused by arteriolardamage.
OCT may be used as a complementary diagnosticmethod to fluorescein angiography in Susac syndromewhere there is doubt that the retinal damage is causedexclusively by arteriolar occlusion.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authorsalone are responsible for the content and writing of thepaper.
REFERENCES1. Susac JO, Egan RA, Rennebohm RM, Lubow M. Susac’s
syndrome: 1975–2005 microangiopathy/autoimmune endothe-liopathy. J NeurologSci. 2007;257:270–272.
2. O’Halloran HS, Pearson PA, Lee WB, Susac JO, Berger JR.Microangiopathy of the brain, retina, and cochlea(Susac syn-drome): A report of five cases and a review of the literature.Ophthalmology 1998;105:1038–1044.
3. Turner BW, Digre KB, Selton C. Susac syndrome. OtolaryngolHead, Neck Surg. 2008;118:886–887.
4. Martinet N, Fardeau C, Adam R, et al. Fluorescein andindocyanine green angiographies in Susac syndrome. Retina2007;27:1238–1242.
5. Falkenberry SM, Ip MS, Blodi BA, Gunther JB. Optical coher-ence tomography findings in central retinal artery occlusion.Ophthalmic Surg Lasers Imaging 2006;37:502–505.
6. Karacorlu M, Ozdemir H, Arf Karacorlu S. Optical coherencetomography findings in branch retinal artery occlusion. Eur JOphthalmol. 2006;16:352–353.
7. Shwartz SG, Hickey M, Puliafito CA. Bilateral CRAO and CRVOfrom thrombocytopenic purpura: OCT findings and treatmentwith triamcinolone acetonide and bevacizumab. OphthalmicSurg Lasers Imaging 2006;37:420–422.
38
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Lib
rary
of
Hea
lth S
ci-U
niv
of I
l on
12/0
1/14
For
pers
onal
use
onl
y.





























