Embed Size (px)
Citation preview

British ournal of Ophthalmology 1995; 79: 910-915
Optic disc measurement: a comparison of indirectophthalmoscopic methods
Anne Fiona Spencer, Stephen A Vernon
AbstractAims-Two methods of indirect ophthal-moscopic estimation ofoptic disc size, the78 dioptre lens and optic disc biometerwere evaluated.Methods-Twenty nine eyes of 29 patientswere measured by both methods and com-pared with optic disc size calculated usingthe three planimetric corrections des-cribed by Bengtsson and Krakau.Results-The closest agreement with theclinical measurements was found usingcorrection 3. There was a significant dif-ference between both the 78 D lens(p<0-0001) and the biometer (p=0-0027)and the planimetric results. There wasalso a significant difference between thetwo clinical methods (p<00001). Bothmethods showed acceptable intraobservervariation (CoV 2-45% and 3-13% respec-tively).Conclusion-Overall, both methods givelarger measurements than planimetry;the 78 D lens by 041 mm and the biometerby 0 15 mm. Neither method gives a satis-factory estimation of optic disc size whencompared with planimetry.(BrJ Ophthalmol 1995; 79: 910-915)
Department ofOphthalmology,University Hospital,NottinghamA F SpencerS A Vernon
Correspondence to:Miss A F Spencer,Department ofOphthalmology, UniversityHospital, NottinghamNG7 2UH.
Accepted for publication17 May 1995
Clinical assessment of the optic nerve head isof great importance in the glaucoma suspect.Ganglion cell loss due to glaucoma causes bothlocalised and generalised changes in the neuro-
retinal rim and an increase in the size of theoptic cup. 14 These changes, which mayprecede visual field loss, may be seen on directophthalmoscopy or at the slit-lamp biomicro-scope with the use of condensing lenses.46However, previous studies have demonstratedthe variability between expert observers inassessing the optic nerve status.7 Optic discsize is known to vary considerably betweenindividuals8 9 yet it has been shown that largeoptic discs are more likely to be classified asglaucomatous and small discs are more likelyto be classified as normal on clinical examina-tion.10 A method of measuring optic disc sizeaccurately in vivo would therefore be of help inassessing whether the optic cup was withinnormal limits for the size of the optic disc andtherefore whether the disc shows glauco-matous damage.
Current methods for in vivo measurementinclude planimetry8 1112 and more complexcomputerised image analysis from stereo-photography'316 including the Humphreyretinal analyser17 and the Rodenstock opticnerve head analyser.'8 These methods aretime consuming or may require specialist
equipment not readily available in the out-patient department. An adaptation of indirectophthalmoscopy for optic disc measurementhas been developed19-21 and is now commer-cially available as the 'optic disc biometer'.More recently, using the same opticalprinciple, the 90 dioptre condensing lens, atthe slit-lamp biomicroscope, has beendescribed for the estimation of optic discsize.22 The 78 dioptre lens yields a larger imagesize than the 90 dioptre lens and thereforeshould be preferable as measurements will notbe at the lower limits of the scale on the slit-beam.The aim of this study was to compare
measurements of optic disc size, by measuringvertical disc diameter, obtained with both in-direct ophthalmoscopic methods - that is,the optic disc biometer and a 78 dioptre con-densing lens, and established planimetricmethods.23 In addition intraobserver vari-ability was assessed for each of the techniques.
Materials and methodsThirty eyes of 30 patients were examined. Onepatient was unable to tolerate the optic discbiometer measurement and therefore theresults from 29 eyes are analysed. There werenine normals, six ocular hypertensives, and 14glaucoma patients. All the patients had a visualacuity of 6/9 or better in the study eye. Twentythree eyes had a refractive error ofup to plus orminus 3 dioptres and six eyes were greater thanplus or minus 3 but less than plus or minus 7dioptres.One eye of each patient was dilated with
tropicamide eyedrops 1% and vertical discdiameter was measured by two observers in arandom order. Both observers were experi-enced in optic disc measurement from pre-vious studies.24 25 The first observer measureddisc diameter at the slit-lamp biomicroscopeusing a 78 dioptre condensing lens. Thesecond observer used the 'optic disc biometer'to measure the vertical disc diameter. Theoptic disc was defined as the area inside thewhite peripapillary scleral ring (Elschnig). Thevertical diameter was defined as the distancefrom the edge of the nerve fibre rim at 12o'clock to the edge of the nerve fibre rim at6 o'clock.
78 DIOPTRE LENS MEASUREMENTSThe Haag-Streit slit-lamp biomicroscope usedhad been calibrated before the study (seebelow). The 78 dioptre lens used was manu-factured by Volk. The lens has a magnificationconstant of 0-86 (instruction manual, Volk).
910
on June 5, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.79.10.910 on 1 October 1995. D
ownloaded from

Optic disc measurement: a comparison of indirect ophthalmoscopic methods
The optic disc was viewed with the 78 D lensas in a normal clinical examination. The lenswas held in front of the patient's eye and theoptic disc brought into focus by moving thebiomicroscope away from the lens. A narrowvertical slit-beam of light, focused on thesurface of the optic disc, was progressivelyreduced in size from 5 mm until it was judgedto correspond to the size of the disc. The beamheight was then recorded, by the secondobserver, from the scale on the slit-lamp. Thiswas then reset to 5 mm and the measurementwas repeated twice, the first observer wastherefore 'blind' to the results. As the slit-lampbeam height scale is calibrated in 0s 1 mm, thereading was judged to the nearest 0 05 mm.
The mean ofthe three measurements, adjustedfor the magnification factor, was then used incomparison with the other methods ofmeasurement.
OPTIC DISC BIOMETER MEASUREMENTSThe details of this instrument have beendescribed elsewhere.19-21 This adaptation ofindirect ophthalmoscopy comprises a 15dioptre condensing lens within an 'opticalspacer' which has a fixation target at theprincipal plane of the lens. A pair of electronicdigitised calipers is then used to makemeasurements of the optic disc diameter.Three measurements of each patient were
taken, the calipers were closed between eachreading and the calibration checked (thatis, the digitised reading was zero). Theywere then opened progressively until theywere judged to correspond to the vertical discdiameter. When the footswitch was depressedthis reading was transferred to a micropro-cessor unit which automatically calculated thevertical disc diameter. As the measurementsseen on the calipers is not the same as thecomputed optic disc size the observer wasalso 'blind' to the results obtained. Themean of the three readings was used for com-parison with the other methods of measure-ment.One patient was unable to cooperate with
measurements by the biometer, being unableto tolerate indirect ophthalmoscopy with a dimlight. Therefore only 29 eyes were included inthese results.
SLIT-BEAM CALIBRATIONA focused slit-beam of light was projected ontoa card on which were printed parallel lines atdifferent distances apart. The distancebetween five pairs of lines ranging from 1-5mm apart was measured with a micrometerscrew gauge by two observers, the mean beingtaken as the true distance. The size of the slit-beam was then adjusted to coincide with thedistance between the two lines and this wasread off the scale on the biomicroscope in a
similar manner to that employed for the discheight. The slit-beam was found to be 02 mmsmaller than the scale across the range of 1 to 5mm calibrated. The results were adjustedaccordingly.
PHOTOGRAPHIC CORRECTIONSThe vertical disc diameter was calculatedfrom photographic slides using the estimatesdescribed by Bengtsson and Krakau.23 Photo-graphs of the optic discs were taken at thehighest magnification, 30 degree setting, with aTopcon fundus camera. A camera constant forthe camera used was calculated by the methoddescribed by Bengtsson and Krakau.23 Theaxial length and corneal curvature of the eyeswas measured using calibrated instruments(Coopervision ultrascan digital A and JavalSchiotz keratometer) and spectacle refractionswere performed by experienced optometric staffat a separate examination. The photographicslides of the optic discs were projected onto ascreen and the optic disc vertical diameter(using the same criteria as described above)was measured by two independent observersand the mean reading taken. All three estimatesdescribed in Bengtsson and Krakau's paperwere then applied to the mean image heightobtained - that is, using (a) axial length only, (b)spectacle correction only, and (c) using specta-cle correction and keratometry.
ANALYSISThe mean of each observer's readings are com-pared by simple regression analysis with theplanimetric results and with each other. Thelevel of agreement is also demonstrated.26 Thecoefficient of variation is calculated for bothindirect methods of examination as a measureof intraobserver variation.
Results
MEASUREMENT OF OPTIC DISC SIZE BY 78 DLENS AND OPTIC DISC BIOMETERThe range of optic disc size measured, themean, and SD of the 29 eyes which were ableto be measured by both the 78 D lens and theoptic disc biometer, are detailed in Table 1.The measurements made by the 78 D lenshave been multiplied by 1-16 (as the magnifi-cation factor for the lens is 0 86).
MEASUREMENT OF OPTIC DISC SIZE FROM THEPROJECTED SLIDESFrom a scattergram plot of the two observers'measurements ofvertical optic disc diameter ofthe 29 eyes measured, the regression liney=0-983x+0-2712 is calculated. This shows avery strong correlation r=0970 (p<0 0001)between the two observers. Agreement wasexamined by plotting the difference between
Table 1 Optic disc size comparedfor the three photographicestimates with the 78 D lens and biometer measurements(mm)
Smallest Largest Mean of SD ofMethod disc disc 29 eyes 29 eyes
Estimate 1 1-335 2-441 1-736 0-210Estimate 2 1-374 2-276 1-740 0-185Estimate 3 1-365 2-388 1-709 0-20578 D lens 1-48 2-53 2-119 0-237Biometer 1-249 2-311 1-860 0-249
911
on June 5, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.79.10.910 on 1 October 1995. D
ownloaded from

Spencer, Vernon
Table 2 The correlation for each of the three photographic estimates with the 78 D lensand biometer measurements, for the 23 eyes within plus or minus 3 D and all 29 eyes
23 Eyes 29 Eyes
Planimetnic Indirect Correlation Correlationestimate method coefficient r p Value coefficient r p Value
Estimate 1 78 D lens 0-5449 0-0059 0-4178 0-0216Biometer 0-3639 0-0805 0-2936 0-1153
Estimate 2 78 D lens 0-6890 0-0002 0-5378 0-0022Biometer 0-5431 0-0061 0-4301 0-0178
Estimate 3 78D lens 0-6922 0-0002 0-5286 0-0027Biometer 0-5604 0 0044 0-4207 0-0205
the two measurements against the mean.Observer A did not read consistently higher orlower than observer B at any size of optic discas the slope of the regression line is not signifi-cant (r=0-065, p=0 735). There is also noconstant difference as the regression line(y=0-250x+ 16&64) passes through zero atthe overall mean optic disc size. There is nosignificant difference between the twoobservers' measurements by a two tailed pairedStudent's t test (p=0-931). The mean of themeasurements was therefore used in furthercalculations.
COMPARISON WITH BENGTSSON AND KRAKAU SCALCULATIONSThe three estimates were then applied tothe mean image height obtained from thephotographic slides. The mean, SD, andrange of optic disc size obtained are comparedwith the 78 D lens and biometer measure-ments in Table 1. The 78 D lens measure-ments and the biometer measurements wereplotted against the photographic measure-ments, using each of the three estimates,and simple regression analysis performed(Table 2).
Estimate 1 based on ultrasonographyThe 78 D lens measurements were signifi-cantly different from the photographic mea-surements by a paired two tailed Student's ttest (p<00001). There was also a significantdifference between the biometer and photo-graphic measurements by the same test(p=00218).
E 2.6 ,E, 2.4
e 2.02
al, 1 -/-/CU1.8(D
E) -
c16 - 23 eyeswithin +/-3D14 _ * 6 eyes +/-3to 7D
a 1.21.4 1 6 1.8 2.0 2.2 2.4 2.6Photographic estimate 3 (mm)
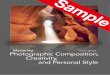
Figure 1 78 D lens measurements of optic disc size arecompared with the photographic measurements calculatedusing estimate 3. The regression line for the 23 eyes withinplus or minus 3 D ofemmetropia is shown. The line ofidentity is also shown.
Estimate 2 based on spectacle refractionThe 78 D lens measurements were signifi-cantly different from the photographicmeasurements by a paired two tailed Student'st test (p<00001). There was also a significantdifference between the biometer and photo-graphic measurements by the same test(p=00112).
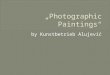
Estimate 3 based on refraction and keratometryThe results of the 78 D lens measurements byobserver 1 and the photographic measure-ments are compared in Figure 1. The biometermeasurements by observer 2 are compared inFigure 2. The best correlation between thereadings is found with this photographic esti-mate and the 78 D lens (r=0-692, p=0-0002for regression line y=0-951x+0O543) for the23 eyes within plus or minus 3D ofemmetropia.As before the 78 D lens measurements were
significantly different from the photographicmeasurements by a paired two tailed Student'st test (p<0-0001). There was also a highlysignificant difference between the biometerand photographic measurements by the sametest (p=0 0027).
For the six eyes with a higher refractive errorthere was a greater disparity between thephotographic and 78 D lens measurementsthan for the 23 eyes within plus or minus 3dioptres of emmetropia. A Mann-Whitney Utest showed this to be highly significant(p=0-0001). Similarly the disparity betweenthe photographic and biometer measurementswas significantly greater for the six eyes withhigh refractive errors (p<0-0001).Agreement can also be examined by plotting
the difference between the vertical discdiameter calculated by the photographicmethod (using estimate 3) and the 78 Dlens against the photographic measurements(Fig 3). Overall, the 78 D lens measures largerthan the photographic method by a mean of0-41 mm, taking into account the magnifica-tion factor for the lens (X0*86). There is a ten-dency for the 78 D lens to further overestimatethe size of the smaller discs, but the slope of theregression line (y=0 263x+1*81, r=0 299) isnot significant (p=0 109). Nineteen of the
E
Ecn
E._omE0
2.6
2.4
2.2
2.0
1.8
1.6
1.4
1.2
o 0 0O°o0
o ,p4,X, 0 23 eyes within +/-3D
* 6eyes +/-3to 7D
1.4 1.6 1.8 2.0 2.2 2.4 2.6Photographic estimate 3 (mm)
Figure 2 Biometer measurements of optic disc size arecompared with the photographic measurements calculatedusing estimate 3. The regression line for the 23 eyes withinplus or minus 3 D ofemmetropia is shown. The line ofidentity is also shown.
912
on June 5, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.79.10.910 on 1 October 1995. D
ownloaded from

Optic disc measurement: a comparison of indirect ophthalmoscopic methods
coE 1.X E 1-0C
C 0.8
a E 0.6
0-4
0-2, *-
)0.2
.)0 0-0
" -0.2
m-0
005._Cl
- °U L
0000 0 0-0 0 0
- q 0 0
--0__O -------------------------------_
U U0 23 eyes within +/-3D* 6eyes3to 7D
.~I
1.6 1.8 2.0 2.2Photographic estimate 3 (mm)
2.4
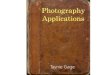
Figure 3 Agreement between the optic disc size measuredby the 78 D lens and by photographic estimate 3. Thedifference between the two measurements is plotted againstthe photographic measurement for each of the 29 eyes. Theregression line is shown.
measurements lie outside the mean differenceplus or minus 0 -1 mm (63%) and nine lie out-side the mean plus or minus 02 mm (30%). Ifthe magnification factor is not applied the 78 Dlens measurements are still larger by a meanof 012 mm and differ significantly by pairedStudent's t test (p=0 0047) from theplanimetric measurements. Correlation isunchanged and when agreement is examinedthe scatter of results is also unchanged.Agreement between the optic disc biometer
and photographic measurements (using esti-mate 3) is demonstrated similarly in Figure 4.The biometer measures, on average, 0-15 mmlarger than the photographic method. Theregression line (y=O0 166x+ 1 *760, r=0*2 14)also shows a tendency for the biometer tofurther overestimate the size of the smalleroptic discs but this is not significant(p=02571). Twenty of the measurementslie outside the mean difference plus orminus 0 1 mm (69%) and 11 lie outside themean difference plus or minus 0-2 mm(38%).
78 D lens and optic disc biometer measurementscomparedThere was a stronger correlation between the78 D lens and biometer measurements(r=0-870, p<00001) than between eitherclinical method and the photographicmeasurements for all 29 eyes. If the twomethods are compared by a paired two tailedStudent's t test they show significantly differ-ent measurements (p<O0000 1). Over all opticdisc sizes, the biometer measures smaller thanthe 78 D lens, the regression line(y=0-250x+1.925, r=0.133) is not signifi-cant (p=0485) showing that the differencedoes not vary significantly as disc sizeincreases.
Intraobserver variation for 78 D lensmeasurementsThe coefficient of variation was calculated asthe square root of the mean value of thevariance of the measurements taken threetimes for each of the 29 optic discs and thendivided by the mean measured disc diameter.
a EX E 1-0.2 0.8
E 0.6.2 _
3 0.4O 0.
E E 0.0.0-;:(D L -0-4Cen
r- L--.44L 0t@ - -0-2c6 X<a< --
o 23 eyes within +/-3D-o * 6 eyes 3 to 7D_ 0
0
-o~~o&oo 0 0
-C.---*~0
0-
1.6 1.8 2.0 2.2 2.4Photographic estimate 3 (mm)
Figure 4 Agreement between the optic disc size measuredby the optic disc biometer and by photographic estimate 3.The difference between the two measurements is plottedagainst the photographic measurementfor each of the 29eyes. The regression line is shown.
As the mean variance is 0-0027 and themean measured disc size is 2 119 mm, thecoefficient of variation is 00245.
Intraobserver variation for optic disc biometermeasurementsThe coefficient of variation was calculated asabove using the mean value of the variance ofthe measurements taken three times for each ofthe 29 optic discs and then divided by themean measured disc diameter.As the mean variance is 0-0034 and the
mean measured disc size is 1X860 mm, thecoefficient of variation is 0X0313.
DiscussionBoth of the above clinical methods of estimat-ing optic disc size share the same opticalprinciple, that of indirect ophthalmoscopy. Areal aerial inverted image is formed and this isviewed either, if using the 78 D lens, by focus-ing the slit-lamp biomicroscope, or the imagefalls on the screen at the principal plane of thecondensing lens, if using the optic disc bio-meter. It would therefore be expected thatboth methods would yield similar readings inindividual eyes. However, this study showsthat, in our hands, the two methods differsignificantly from each other and from estab-lished planimetric techniques.The 78 D lens measurements were, on
average, 0-41 mm larger and the biometermeasurements 0 15 mm larger than the thirdphotographic estimate which uses spectaclerefraction and comeal curvature. The closestcorrelation between the planimetric andclinical methods was found using this photo-graphic estimate as noted in previous studiesof optic disc size estimation.24 25 As the 78 Dlens measurements are so much larger thanplanimetry when corrected with the manu-facturer's magnification factor (0 86) thissuggests that their calculations for the correc-tion factor are not correct when the lens is usedat the Haag-Streit slit-lamp biomicroscope. Ifthe uncorrected measurements are used the78 D lens measures 0 12 mm larger on averageand correlation with planimetry is unchanged.Correlation alone only shows the strength of
913
r-L
on June 5, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.79.10.910 on 1 October 1995. D
ownloaded from

Spencer, Vernon
the relation between the measurements, notthe agreement. Our results differ from a recentpublication22 in which the 90 D lens was usedto estimate optic disc size at the slit-lamp,where a higher correlation with planimetrictechniques was obtained. Both methods usedin this study demonstrate marked scatter of theresults when agreement is examined26 (as inFigs 3 and 4) and surprisingly a substantialnumber of measurements were outside plus orminus 0-2 mm from the mean differencebetween the measurements (30% for the 78 Dlens and 34% for the biometer). The biometerand 78 D lens appeared to further overestimatethe size of the smaller discs but this was notstatistically significant. This factor cannot becompared with the 90 D lens study as agree-ment (see above) was not assessed by theauthor. It would be interesting to see the datafrom that study replotted as it is likely that the90 D lens also overestimates the smaller opticdiscs.
Previous authors have described both directand indirect ophthalmoscopic methods ofoptic disc analysis and the use of theGoldmann fundus contact lens at the slit-lamp.27 28 The latter method required agraticule27 or a calculated correction factorwhich varied with the refraction of the eye.28No magnification constant was calculated forthe contact lens and the 'normal range' of opticdiscs measured differed from that describedby planimetric and histological studies.8 9Increasing refractive error is known to causeinaccuracies in both direct and indirectmethods.27 Refractive error influences theimage size produced if the focal plane of thecondensing lens does not coincide with theanterior focus of the eye. At the slit-lamp bio-microscope with the 78 D lens, the imageobtained may appear 'focused' adequately totake a reading with the slit-beam, when in factthe lens is not exactly at the anterior focus ofthe eye. This may account for some of the dis-parity between the readings obtained with the78 D lens and planimetry. However, for ourobserver the method appears highly repeatableas there was a low coefficient of variation. Asthe 78 D lens measures greater even in theemmetropic eye this suggests that the dispari-ties are not merely in the position of the con-densing lens but a correction factor for themagnification of the eye may need to be calcu-lated for eyes of greater refractive error. This issupported by the significantly greater disparityfound between the measurements for the sixeyes with higher refractive errors. The smallnumber of eyes of higher refractive errorexamined in this study does not permit the cal-culation of correction factors for increasingametropia. Many glaucoma suspects aremyopic and although the majority will not havemarked ametropia this will restrict the use ofindirect ophthalmoscopic methods to estimatedisc diameter in these patients.Montgomery in his report of the optic disc
biometer19 21 explained the importance of thepositioning of the optical spacer. The opticalspacer (which incorporates the condensinglens) needs to be held steady at a distance from
the patient's eye where the best focus isachieved; it requires the operator to have alarge hand span to facilitate this manoeuvre. Itis quite probable that the different resultsachieved with the instrument in comparisonwith planimetry are due to the lens beingmoved in relation to the anterior focus of theeye. The technique also requires coordinationof the optical spacer, the digitised calipers, andthe footswitch to take a measurement andtherefore is not as simple to perform as the78 D lens measurement at the slit-lamp. Withincreasing ametropia we would expect the dis-parity between the biometer and planimetricresults to increase and indeed our findings con-firm this. However, this does not account forall the disparity with planimetry as we mightexpect that operator error would induce amarked intraobserver variation and this wasnot the case. It should also be noted that noprevious publication on the biometer comparesit with established planimetric techniques.
Assessment of the size of the optic disc, evenby more sophisticated techniques, relies on theinterpretation of the optic disc boundary.Although the two observers in this study usedtwo different techniques to measure the opticdisc diameter both observers were experiencedin optic disc assessment from previousstudies.2425 In addition, they had previouslyshown very little interobserver variability inidentifying the optic disc boundary24 so itwould seem unlikely that the differencesbetween the planimetric and clinical methodswere due to great variability between theobservers' recognition of the optic discboundary. The optic disc biometer itself hasbeen assessed previously for interobserver vari-ability29 and median interobserver differencewas shown to be 4 45%. The observer usingthe 78 D lens showed a low intraobserver vari-ability similar to that found by the sameobserver using the Zeiss four mirror contactlens to measure disc diameter25 and also con-sistent with the previous study published usingthe 90 D lens.22 Although a small error causedby interobserver variability of the clinicalmethods will affect the calculations of correla-tion and agreement this alone would notaccount for the relatively poor correlation andagreement between the indirect ophthalmo-scopic and planimetric measurements.
Further inaccuracies may be due to theplanimetric techniques. Bengtsson andKrakau's previous calculations30 have beenshown to be equivalent to Littman's algorithmsto correct for the magnification factor of theeye, when using the Zeiss fundus camera.31This study uses their most recent planimetriccorrections23 which have been shown to corre-late well with disc diameter measured in vivowith the Zeiss four mirror contact lens25 andwith the Heidelberg retina tomograph (HRT)confocal scanning laser ophthalmoscope.24The HRT measurements were smaller than theplanimetric measurements, if the size differ-ence is corrected for then good agreement isachieved. All planimetric methods will includeerror as at present they cannot be verified reli-ably in living eyes. Optic disc size calculations
914
on June 5, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.79.10.910 on 1 October 1995. D
ownloaded from

Optic disc measurement: a comparison of indirect ophthalmoscopic methods
using Littman's formula were shown to differfrom measurements during vitrectomy.32Other investigators have demonstrated thatdecentration of the object, alteration of the eyeto camera distance, and increasing ametropiacan cause a large variation in the measuredfrom the calculated magnification.33-35However, planimetric calculations are atpresent the 'gold standard' with which newmethods of optic disc measurement are com-pared.The 78 D lens and optic disc biometer tech-
niques both appeared to be repeatable with acoefficient of variation of 2-45% and 3 13%respectively. This is comparable with the3*07% calculated from the figures given in the90 D lens study.22 Intraobserver variation hasbeen assessed for the optic disc biometer pre-viously as 2.7%.19 Both methods, therefore,show an acceptable low variability for a clinicaltechnique of measurement.Of the two techniques employed in this
study, the 78 D lens is simpler and shows a
better correlation but poorer agreement withplanimetry. Better agreement may, however,be achieved by eliminating the manufacturer'smagnification factor from the calculations asthis reduces the mean difference between the78 D lens and planimetry to 0 12 mm. It maybe a useful technique for a rapid assessment ofwhether the optic disc is unusually large or
small, providing that the clinician knows thenormal range of disc size for this method.Alternatively, extrapolating from our results,we suggest that an approximation of optic discdiameter can be obtained by dividing the discsize, measured with the 78 D lens, by 0-86 andsubtracting 0-41 mm. One must rememberthat, after this calculation, there is only likely tobe a 70°/O chance of the result obtained beingwithin plus or minus 0-2 mm of the planimet-ric calculation, based on the results of .an
experienced observer.We wish to thank Mr Ahmed Sadiq for his help with measure-ment of the vertical optic disc diameter from photographicslides and Mr Peter Pawson for his help with clinical datacollection.
1 Jonas JB, Gusek GC, Naumann GOH. Optic discmorphometry in chronic primary open-angle glaucoma I.Morphometric intrapapillary characteristics. Graefes ArchClin Exp Ophthalmol 1988; 226: 522-30.
2 Yablonski ME, Zimmeman TJ, Kass MA, Becker B.Prognostic significance of optic disc cupping in ocularhypertensive patients. Am Ophthalmol 1980; 89: 585-92.
3 Tuulonen A, Airaksinen PJ. Initial glaucomatous optic diskand retinal nerve fibre layer abnormalities and their pro-gression. Am Ophthalmol 1991; 111: 485-90.
4 Pederson JE, Anderson DR. The mode of progressivedisc cupping in ocular hypertension and glaucoma.Arch Ophthalmol 1980; 98: 490-5.
5 Sommer A, Polack I, Maumenee E. Optic disc parametersand onset of glaucomatous field loss 1. Methods and pro-gressive changes in disc morphology. Arch Ophthalmol1979; 97: 1444-8.
6 Caprioli J, Miller JM, Sears M. Quantitative evaluation ofthe optic nerve head in patients with unilateral visual field
loss from primary open-angle glaucoma. Ophthalmology1987; 94: 1484-7.
7 Varma R, Steinman WC, Scott IU. Expert agreement inevaluating the optic disc for glaucoma. Ophthalmology1992; 99: 215-21.
8 Jonas JB, Gusek GC, Guggenmoos-Holzmann I, NaumannGOH. Variability of the real dimensions ofnormal humanoptic discs. Graefes Arch Clin Exp Ophthalmol 1988; 226:332-6.
9 Quigley HA, Brown AE, Morrison JD, Drance SM. The sizeand shape of the optic disc in normal human eyes. ArchOphthalmol 1990; 108: 51-7.
10 Heijl A, Molder H. Optic disc diameter influences theability to detect glaucomatous optic disc damage. ArchOphthalmol (Copenh) 1993; 71: 122-9.
11 Bengtsson B. The variation and covariation of cup and discdiameters. Arch Ophthalmol (Copenh) 1976; 54: 804-18.
12 Jonas JB, Gusek GC, Naumann GOH. Optic disc, cup andneuroretinal rim size, configuration and correlations innormal eyes. Invest Ophthalmol Vis Sci 1988; 29: 1151-8.
13 Balazsi AG, Drance SM, Schulzer M, Douglas GR.Neuroretinal rim area in suspected glaucoma and earlychronic open-angle glaucoma. Arch Ophthalmol 1984;102: 1011-4.
14 Takamoto T, Schwartz B. Reproducibility of photogram-metric optic disc cup measurements. Invest Ophthalmol VisSci 1985; 26: 814-7.
15 Schwartz B. New technique for the examination of the opticdisc and their clinical application. Trans Am AcadOphthalmol Otolaryngol 1976; 81: 227-35.
16 Portney GL. Photogrammetric analysis of volume asym-metry of the optic nerve head cup in normal, hypertensiveand glaucomatous eyes. AmJ Ophthalmol 1975; 80: 51-5.
17 Dandona L, Quigley HA, Jampel HD. Variability of depthmeasurements of the optic nerve head and peripapillaryretina with computerized image analysis. Arch Ophthalmol1989; 107: 1786-92.
18 Caprioli J, Klingbeil U, Sears M, Pope B. Reproducibility ofoptic disc measurements with computerized analysis ofstereoscopic video images. Arch Ophthalmol 1986; 104:1035-9.
19 Montgomery DMI. Measurement of optic disc andneuroretinal rim areas in normal and glaucomatous eyes -a new clinical method. Ophthalmology 1991; 98: 50-9.
20 Montgomery DMI. Clinical disc biometry in earlyglaucoma. Ophthalmology 1993; 100: 52-6.
21 Montgomery DMI. The optical spacer - a simple devicewhich extends the scope of indirect ophthalmoscopy.BrJ Ophthalmol 1992; 76: 45-6.
22 Ruben S. Estimation of optic disc size using indirect bio-microscopy. Bry Ophthalmol 1994; 78: 363-4.
23 Bengtsson B, Krakau CET. Correction of optic discmeasurements on fundus photographs. Graefes Arch ClinExp Ophthalmol 1992; 230: 24-8.
24 Spencer AF, Vernon SA. Vertical optic disc diameter - theHeidelberg Retina Tomograph against photographs.Invest Ophthalmol Vis Sci 1995; 36: 796-803.
25 Spencer AF, Vernon SA. Optic disc measurement with theZeiss 4-mirror contact lens. Br J Ophthalmol 1994; 78:775-80.
26 Bland JM, Altman DG. Statistical methods for assessingagreement between two methods of clinical measurement.Lancet 1986; i: 307-10.
27 Franceschetti A, Bock RH. Megalopapilla: a new congenitalanomaly. Am J Ophthalmol 1950; 33: 227-34.
28 Beuchat L, Safran AB. Optic nerve hypoplasia: papillarydiameter and clinical correlation. Y Clin Neuro-ophthalmol1985; 5: 249-53.
29 Pyott AAE, Montgomery DMI. Inter-observer variation inclinical optic disc biometry. Eye 1993; 7: 452-6.
30 Bengtsson B, Krakau CET. Some essential optical featuresof the Zeiss fundus camera. Arch Ophthalmol 1977; 55:123-31.
31 Mansour AM. Measuring fundus landmarks. InvestOphthalmol Vis SCi 1990; 31: 41-2.
32 Bartz-Schmidt KU, Weber J, Heinmann K. Optic disc sizecalculations using Littmann's formula differs from in vivomeasurements of the optic disc during vitrectomy. InvestOphthalmol Vis Sci 1993; 34: 1505.
33 Pach J, Pennell DO, Romano PE. Optic disc photogram-metry: magnification factors for eye position, centration,and ametropias, refractive and axial; and their applicationin the diagnosis of optic nerve hypoplasia. Ann Ophthalmol1989; 21:454-62.
34 Lotmar W. Dependence of magnification upon the camera-to-eye distance in the Zeiss fundus camera. ArchOphthalmol 1984; 62: 131-4.
35 Arnold JV, Gates JWC, Taylor KM. Possible errors in themeasurement of retinal lesions. Invest Ophthalmol Vis Sci1993; 34: 2576-80.
915
on June 5, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.79.10.910 on 1 October 1995. D
ownloaded from