Embed Size (px)
Citation preview

Ophthalmology Coding: Raise Your “Eye-Q”
Nancy Clark, CPC, COC, CPB, CPMA, CPC-I
1

Disclaimer
The information in this presentation was current at the time the
presentation was compiled. Always consult CPT®, ICD-9-CM, ICD-10-
CM, CMS and commercial payers for specific guidance in reporting
services.
This presentation is designed to provide accurate information in
regard to the subject matter covered. The information includes both
reporting and interpretation of materials in various publications, as
well as interpretation of policies of various organizations. Every
reasonable effort has been made to ensure the accuracy of this
information.
The duplication of this presentation, all or in part, without the express
permission of the presenter, is strictly prohibited.
2

Agenda
• Eye Exam Codes vs. E/M Codes
• Diagnostic Testing Procedures
• Surgical Procedures
• 2017 ICD-10 Updates
3

Eye Exam Codes
• New Patients– 92002 Ophthalmological services: medical examination and
evaluation with initiation of diagnostic and treatment program; intermediate
– 92004 Ophthalmological services: medical examination and evaluation with initiation of diagnostic and treatment program; comprehensive, one or more visits
• Established Patients– 92012 Ophthalmological services: medical examination and
evaluation, with initiation or continuation of diagnostic and treatment program; intermediate
– 92014 Ophthalmological services: medical examination and evaluation, with initiation or continuation of diagnostic and treatment program; comprehensive, one or more visits
4

Intermediate vs. ComprehensiveEye Exams
Intermediate
(92002 or 92012)
• Evaluation of a new or existing condition
• Not necessarily relating to the primary diagnosis
• History• General Medical Examination• External ocular and adnexal
exam• Other diagnostic procedures
as indicated• May include mydriasis for
ophthalmoscopy
Comprehensive(92004 or 92014)
• General evaluation of the complete visual system• Does not need to be performed at one session• History• General Medical Examination• External Examination• Ophthalmoscopic Examination• Gross Visual Fields• Basic Sensorimotor Evaluation• Optional Components, as Indicated:
– Biomicroscopy– Exam with cycloplegia or mydriasis– Tonometry
• Initiation of diagnostic and treatment programs– Prescription of medication– Arranging for special ophthalmological, diagnostic or
treatment services– Consultations – Laboratory procedures – Radiological services
• Carriers may add additional requirements or exceptions
Continued... 5

Examples
Intermediate• History, external examination,
ophthalmoscopy, biomicroscopy for an acute complicated condition (e.g. iritis) – not requiring comprehensive
ophthalmological services
• Interval history, external examination, ophthalmoscopy, biomicroscopy and tonometry in established patient with known cataract – not requiring comprehensive
ophthalmological services
Comprehensive
• Diagnosis and treatment of a patient with symptoms indicating possible disease of the visual system, such as– Glaucoma
– Cataract
– Retinal disease, or
• To rule out disease of the visual system
• New or established patient
6Reference CPT(R) Professional 2016

Bundled Services
• Slit lamp exam
• Keratometry
• Routine ophthalmoscopy
• Retinoscopy
• Tonometry
• Motor evaluation
• Compare to E/M Service…..
7

E/M Codes with1997 Eye Exam Elements
• History
• Exam
– Test visual acuity (Does not include determination of refractive error)
– Gross visual field testing by confrontation
– Test ocular motility including primary gaze alignment
– Inspection of bulbar and palpebral conjunctivae
– Examination of ocular adnexae including lids (eg, ptosis or lagophthalmos), lacrimal glands, lacrimal drainage, orbits and preauricular lymph nodes
– Examination of pupils and irises including shape, direct and consensual reaction (afferent pupil), size (eg, anisocoria) and morphology
– Slit lamp examination of the corneas including epithelium, stroma, endothelium, and tear film
– Slit lamp examination of the anterior chambers including depth, cells, and flare
– Slit lamp examination of the lenses including clarity, anterior and posterior capsule, cortex, and nucleus
– Measurement of intraocular pressures (except in children and patients with trauma or infectious disease)
Exam (Continued)…• Ophthalmoscopic examination through dilated
pupils (unless contraindicated) of– Optic discs including size, C/D ratio,
appearance (eg, atrophy, cupping, tumor elevation)and nerve fiber layer
– Posterior segments including retina and vessels (e.g., exudates and hemorrhages)
• Brief assessment of mental status including – Orientation to time, place and
person– Mood and affect (e.g.,
depression, anxiety, agitation)• Exam Level
– Problem Focused• 1 - 5 elements
– Expanded Problem Focused • 6 + elements
– Detailed• 9 + elements
– Comprehensive• Perform and document• Every element in the eye exam category• Perform and document at least 1
element in Neurological/Psychiatric• Medical Decision Making
8

Considerations for UsingE/M vs. an Eye Exam
• What does the documentation support?
• Diagnosis specific regulations
– For certain insurance companies eyelid and adnexa diagnoses may not be considered medically necessary for some components of eye exam
• Know your carriers’ requirements and patients’ insurance
– Routine or Medical
– Frequency Allowed
• Very detailed consultation/patient visit may support E/M
9

Routine Eye Exams
• Most carriers use CPT® 92002 – 92014 with “Z” codes– Z01.00, Encounter for examination of eyes and vision without
abnormal findings– Z01.01, Encounter for examination of eyes and vision with abnormal
findings• Use additional code to identify abnormal findings
• Alternatively, Medicaid and some carriers use– S0620 Routine ophthalmological examination including refraction;
new patient – S0621 Routine ophthalmological examination including refraction;
established patient – These codes include 92015, Determination of refractive state
• Medicare does not reimburse for routine (screening) exams– Note signs/symptoms/disease processes
10

Diagnostic Testing Procedures
• Important Reimbursement Concepts
– Multiple Procedure Payment Reductions (MPPR)
– Bilateral Procedures
• Extended Ophthalmoscopy
• Fluorescein and Indocyanine Green Angiography
• Fundus Photography
• Ophthalmic A and B Scans
• Visual Field Testing
11

Multiple Procedure Payment Reductions (MPPR)
• Identify appropriate reductions• Reduction to 80% of allowed fee schedule for the
technical component (TC) of certain diagnostic ophthalmology procedures
• Applies to subsequent procedures when multiple procedures are furnished to the same patient on the same date of service
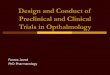
• Does not apply to the Professional Component (PC)• Identify using MPFS Payment Policy Indicators multiple
surgery column– 7 = Diagnostic ophthalmology services subject to the MPPR
methodology– 0 = No payment adjustment rules for multiple procedures apply
12

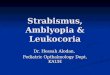
Multiple Procedure Payment Reductions Example
CPT® Code 92235
CPT® Code 92250
Total
Payment
Before Reduction
Total
Payment After Reduction
Payment
Calculation
PC $46.00 $23.00 $69.00 $69.00 No Reduction
TC $92.00 $53.00 $145.00 $134.40 $92.00 +
(80% x
$53.00)
Global $138.00 $76.00 $214.00 $203.40 $69.00 +
$92.00 +
(80% x $53.00)
Http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R1149OTN.pdf

Medicare Physician Fee SchedulePayment Policy Indicators
14www.cms.gov
7

Bilateral Procedures
• Identify appropriate reimbursement for bilateral procedures
• Use MPFS
• Bilateral Surgery Indicator– 1= Payment is 150% fee schedule for bilateral.
– 2= No increase. Procedure is already bilateral.
– 3= Each eye is coded independently at 100% of FS. Bilateral = 200% of FS
– 0= Payment adjustment for bilateral does not apply.
15

Extended Ophthalmoscopy
CPT® Codes 92225 and 92226• 92225 Ophthalmoscopy, extended,
with retinal drawing (e.g. for retinal detachment, melanoma), with interpretation and report; initial
• 92226– …Subsequent
• Routine ophthalmoscopy is part of general and special ophthalmologic services and is not reported separately– Modifier 25 usage for significantly
separate procedure
• Unilateral procedure– Reimbursed at 100% for each eye
• No MPPR reduction
Documentation Requirements• Retinal drawings
– Appropriate size, color, detail
• Documentation in the patient’s medical record for a diagnosis of glaucoma includes– A separate detailed drawing of the optic
nerve – Documentation of cupping, disc rim, pallor,
and slope– Documentation of any surrounding
pathology around the optic nerve.
• Medical necessity for each eye examined
• Document that the pupil was dilated and what drug was used
• All findings and a plan of action should be documented in notes
Continued... 16

Extended Ophthalmoscopy Indications and Limitations
Indications
• Medically reasonable and necessary:
– Neoplasm
– Trauma
– Abnormalities of the macula, retina or choroid
– Specified other acute symptoms & chronic conditions
• Review LCD’s, available for Palmetto, CGS, NGS and First Coast
Limitations
• Should not be routinely used on both eyes of every patient on all visits.
• Routine ophthalmoscopy and biomicroscopy are part of an ophthalmologic examination and are not separately payable
• Not reimbursable within the global period of ophthalmic surgery unless distinct
• Not performed with other testing (i.e. fundus photography, flouresceinangiography)
17

Fluorescein Angiography
CPT® Codes• 92230 Fluorescein angioscopy
with interpretation and report • 92235 Fluorescein Angiography
(includes multiframe imaging) with interpretation and report
• Taking photos of inner eye vessels using fluorescein dye
• Frequency as often as every 8 weeks to assist in management of retinopathy
• Unilateral procedure– Reimbursed at 100% for each eye
• Subject to MPPR reduction
Indications and Guidelines• Initial evaluation of a patient with
abnormal findings of the fundus/retina
• Patients presenting with sudden vision loss
• Evaluation of patients with – Diabetic retinopathy– Chorioretinitis, chorioretinal scars,
dystrophies, hemorrhage, rupture or detachment
– Known retinal or macular disorders– Ocular tumors, visual loss in systemic
disease, and optic disc disease
• Written report• Review LCD’s, available at First Coast,
CGS, Palmetto
18

Indocyanine Green Angiography (ICG)
CPT® Code
• 92240 Indocyanine-Green Angiography (includes multiframe imagine) with interpretation and report
• Taking photos of eye using ICG dye
• Frequency is dependent on performance of Fluorescein Angiography and disease process
• Unilateral procedure– Reimbursed at 100% for each eye
• Subject to MPPR reduction
Indications and Guidelines• A valuable diagnostic adjunct
to fluorescein angiography in the evaluation of – Retinal neovascularization– Choroid neovascularization– Serous detachment of retinal
pigment epithelium– Hemorrhagic detachment of
retinal pigment epithelium– Retinal hemorrhage
• Written report• Review LCD’s available at First
Coast, CGS, Palmetto
Continued... 19

Fluorescein and ICG Angiography Limitations
• ICG angiography must be performed under the direct supervision of a physician when done by a non-physician practitioner
• Some state law excludes optometrists from performing invasive procedures, including ICG
– New Jersey and New York State
• Contraindicated for patients allergic to iodine
• Not medically necessary for evaluation of background diabetic retinopathy
20

Fundus Photography
CPT® Code
• 92250 Fundus photography with interpretation and report
• Bundled with 92240, ICG Angiography
• Bilateral procedure, no additional reimbursement– May use modifier 52 for one
eye
• Subject to MPPR
• Review LCD’s, available at First Coast, NGS, CGS
Indications and Guidelines• Use of a retinal camera to
photograph regions of the vitreous, retina, choroid, and optic nerve (posterior segment)
• Documents changes in baseline retinal findings and track disease progression
• Images may be either photographic or digital and become part of the patient’s permanent record. – Usually taken through a dilated pupil
• A single series of photographs will be reimbursed where clinically indicated
21

Ophthalmic A and B Scans
CPT® Codes• 76510 Ophthalmic ultrasound,
diagnostic; B-scan and quantitative A-scan performed during the same patient encounter
• 76511 … quantitative A-scan only • 76512 … B-scan (with or without
superimposed non-quantitative A-scan)
• 76513 … anterior segment ultrasound, immersion (water bath) B-scan or high resolution biomicroscopy
• Unilateral procedure– Reimbursed at 100% for each eye
• Subject to MPPR reduction
Indications and Guidelines• Ophthalmic ultrasound, AKA ocular
echography, uses high frequency sound waves to examine the eye structure and diagnose disorders
• A-scan is 1-D, used for simple cataract• B-scan ultrasound, AKA bright scan,
cross sectional 2-D view of the eye structure– For dense cataract or precluded
visualization of the posterior segment of eye
• A-scan covered under Medicare when performed prior to cataract surgery– Usually only 1 A or B scan in 12 month
period
• Codes subject to 26/TC split• LCD’s available at NGS and CGS
22

Ophthalmic A Scan and Optical Coherence Biometry
CPT® Codes
• 76519 Ophthalmic biometry by ultrasound echography, A-scan with intraocular lens power calculation
• 92136 Ophthalmic biometry by partial coherence interferometry with intraocular lens power calculation
• PC is unilateral– Reimbursed at 100% for each eye
• TC is bilateral– No increase in reimbursement
– Subject to MPPR reduction
Indications and Guidelines
• Cataract extraction with lens implantation
• 2 methods for Intraocular Lens (IOL) determination
• Measures length of eye
• Covered under Medicare when performed prior to cataract surgery
• Medicare allows more than one scan if surgery is postponed
23

Visual Field Testing
CPT® Codes• 92081 Visual field examination, unilateral or
bilateral, with interpretation and report; – Limited examination (e.g., tangent screen,
Autoplot, arc perimeter, or single stimulus level automated test, such as Octopus 3 or 7 equivalent)
• Very limited screening test only
• 92082– …Intermediate examination (e.g., at least 2
isopters on Goldmann perimeter, or semiquantitative, automated suprathresholdscreening program, Humphrey suprathresholdautomatic diagnostic test, Octopus program 33)
• Used for suspected neurological damage
• 92083– …Extended examination (e.g., Goldmann visual
fields with at least 3 isopters plotted and static determination within the central 30 degrees or quantitative, automated threshold perimetry, Octopus program G-1, 32 or 42, Humphrey visual field analyzer full threshold programs 30-2, 24-2, or 30/60-2)
• Suspected slow progressive dimming of peripheral vision (glaucoma)
Guidelines
• CPT descriptions indicate extent and types of visual field
• Number of isoptersdocumented needed to support level
• Written report
• Bilateral
– No increase in reimbursement
– Can use modifier 52 for one eye
• Subject to MPPR
24Continued...

Visual Field TestingIndications
• Disorder of the eyelids potentially affecting the visual field
• Prosthesis difficulties in an anophthalmicsocket
• Advanced glaucoma or suspected glaucoma
• Disorder of the optic nerve, the neurological visual pathway, or retina
• Recent intracranial hemorrhage, mass or increased pressure
• Recent occlusion and/or stenosis of cerebral arteries, transient cerebral ischemia or giant cell arteritis
• History of a cerebral aneurysm, pituitary tumor, occipital tumor or other condition potentially affecting the visual fields
• A visual field defect demonstrated by gross visual field testing
• Significant recent eye injury• Unexplained visual loss• Part of an initial workup for buphthalmos,
congenital anomalies of the posterior segment or congenital ptosis
• Disorder of the orbit, potentially affecting the visual field
• Pale or swollen optic nerve • New functional limitations which may be
due to visual field loss (i.e., reports by family that patient is running into things)
• Use of a medication (e.g., Plaquenil) which has a high risk of potentially affecting the visual system
• Initial evaluation for macular degeneration• Review LCD’s at WPS, NGS and CGS
25

Scanning Computerized Ophthalmic Diagnostic Imaging (SCODI)
CPT® Codes• 92132 Scanning computerized
ophthalmic diagnostic imaging, anterior segment, with interpretation and report, unilateral or bilateral
• 92133 Scanning computerized ophthalmic diagnostic imaging, posterior segment, with interpretation and report, unilateral or bilateral; optic nerve
• 92134 Scanning computerized ophthalmic diagnostic imaging, posterior segment, with interpretation and report, unilateral or bilateral; retina
Guidelines
• Retinal thickness analysis
• Codes indicate area of eye examined (anterior, optic nerve, retina)
• AKA Heidelberg Retina Tomograph (HRT) study
• 92133 and 92134 bundled per NCCI edits
• Bilateral procedure, no increase in reimbursement
• Subject to MMPR
Continued... 26

SCODI
Indications• Glaucoma
– Valuable diagnostic tool in the diagnosis and treatment of glaucoma
– Enable discernment of changes of the nerve fiber even in advanced cases of glaucoma.
– 2 exams per eye per year maximum for most carriers
• Retinal disorders– Including macular abnormalities– 2 exams per eye per year for
disease management– Up to one exam per month for
active treatment
Limitations
• Considered experimental for certain disorders:– Narrow angle, suspected
narrow angle, mixed narrow & open angle glaucoma
– Determination of IOL
– Iris tumor
– Calculation of lens power for cataract patients who have undergone prior refractive surgery
• Review LCD’s available at First Coast, Novitas, CGS, NGS, WPS
27

Surgical Procedures
• Cataract Surgery
• Blepharoplasty/Blepharoptosis
28

Cataract Surgery CPT® Codes • 66830 Removal of secondary membranous cataract (opacified posterior lens
capsule and/or anterior hyaloid) with corneo-scleral section, with or without iridectomy (iridocapsulotomy, iridocapsulectomy) – Excise posterior lens capsule due to cloudy and thickened lens after cataract surgery
• 66840 Removal of lens material; aspiration technique, 1 or more stages – Floating lens material after artificial lens implantation
• 66850 Removal of lens material; phacofragmentation technique (mechanical or ultrasonic) (e.g., phacoemulsification), with aspiration – Mechanical or ultrasound to break down lens material and remove
• 66852 Removal of lens material; pars plana approach, with or without vitrectomy – Incision through pars plana (middle of eye between retina and iris); access vitreous
• 66920 Removal of lens material; intracapsular– Removal of lens and surrounding capsule; freezes lens on cryoprobe
• 66930 Removal of lens material; intracapsular, for dislocated lens– May be result of trauma or Marfan’s syndrome
• 66940 Removal of lens material; extracapsular (other than 66840, 66850, 66852)– Leaves elastic capsule in place for implantation of IOL
Continued... 29

Cataract Surgery CPT® Codes (continued)
• 66982 Extracapsular cataract removal with insertion of intraocular lens prosthesis (1-stage procedure), manual or mechanical technique (eg, irrigation and aspiration or phacoemulsification), complex, requiring devices or techniques not generally used in routine cataract surgery (eg, iris expansion device, suture support for intraocular lens, or primary posterior capsulorrhexis) or performed on patients in the amblyogenic developmental stage – Complex code is intended to differentiate the extra work performed during the intraoperative
or postoperative periods in a subset of cataract operations• A miotic pupil which will not dilate sufficiently to allow adequate visualization of the lens in the
posterior chamber of the eye, and requires additional techniques• Pediatric cataract surgery • The use of capsular dye for the assisted visualization of the anterior capsule in performing
capsulorhexis (anterior capsule made in a smooth circular pattern vs “can opener” technique)
• 66983 Intracapsularcataract extraction with insertion of intraocular lens prosthesis (1 stage procedure) – Removes lens and capsule; inserts lens prosthesis
• 66984 Extracapsular cataract removal with insertion of intraocular lens prosthesis (1 stage procedure), manual or mechanical technique (e.g., irrigation and aspiration or phacoemulsification)– Elastic capsule is retained; IOL inserted
30

Blepharoplasty/Blepharoptosis
• Blepharoplasty CPT® Codes
– 15820 Blepharoplasty, lower eyelid;
– 15821 … with extensive herniated fat pad
– 15822 Blepharoplasty, upper eyelid;
– 15823 … with excessive skin weighting down lid
• Blepharoptosis CPT® Codes
– 67901 Repair of blepharoptosis; frontalis muscle technique with suture or other material (e.g., banked fascia)
– 67902 … frontalis muscle technique with autologous fascial sling (includes obtaining fascia)
– 67903 … (tarso) levator resection or advancement, internal approach
– 67904 …(tarso) levator resection or advancement, external approach
– 67906 …superior rectus technique with fascial sling (includes obtaining fascia)
– 67908 …conjunctivo-tarso-Muller's muscle-levator resection (e.g., Fasanella-Servattype)
• Brow Ptosis CPT® Codes
– 67900 Repair of brow ptosis (supraciliary, mid-forehead or coronal approach)Continued... 31

Blepharoplasty/Blepharoptosis Indications
Indications• When performed as functional/reconstructive
procedures
• Blepharoplasty procedures to correct– Visual impairment due to dermatochalasis or
blepharochalasis
– Symptomatic redundant skin which is resting on upper lashes
– Chronic, symptomatic dermatitis of pretarsal skin
– Prosthesis difficulties in an anophthalmic socket
• Blepharoptosis repair to correct
– Visual impairment due to droop or displacement of the upper lid
• Brow ptosis repair to correct
– Visual impairment due to droop or displacement of the brow
– Brow malposition which would prevent adequate correction of dermatochalasis, blepharochalasisor blepharoptosis
Documentation Guidelines*• Visual Fields
– Taped and Untaped– Upper visual field improvement at least
20% taped (8 degrees)– Showing Visual Field obstruction of at least
30 degrees
• Documentation of Medical Necessity– Patient’s complaint that defines the
functional deficit– Difficulty reading or driving due to upper
eyelid drooping– Looking through the eyelashes or seeing
the upper eyelid skin– Chronic blepharitis
• Photographs– Front and side views
*Guidelines vary by carrier 32

ICD-10-CM Updates 2017Chapter 7: Diseases of the Eye and Adnexa
• 12 Deleted Codes
• 100 New Codes
• 8 Revised Codes
• 6th Characters for new and revised codes
– 1 = Right eye
– 2 = Left eye
– 3 = Bilateral
– 9 = Unspecified eye
33

ICD-10-CM UpdatesRetinal Vein Occlusions
Deleted Codes
• H34.81x: Central retinal vein occlusion– Right, Left, Bilateral or
Unspecified
• H34.83x: Tributary (branch) retinal vein occlusion
– Right, Left, Bilateral or Unspecified
New Codes
• H34.81xx: Central retinal vein occlusion, OR
• H34.83xx: Tributary (branch) retinal vein occlusion
• 7th character indicates– With macular edema (7th = 0)
– With retinal neovascularization (7th = 1)
– Stable (7th = 2)
• 6th character still indicates Right, Left, Bilateral or Unspecified
34

ICD-10-CM UpdatesNonexudative Age-Related Macular Degeneration
Deleted Codes
• H35.31: Nonexudative age-related macular degeneration
New Codes
• H35.31xx: Nonexudative age-related macular degeneration
• 7th character indicates– Stage unspecified (7th = 0)
– Early dry stage (7th = 1)
– Intermediate dry stage (7th = 2)
– Advanced atrophic withoutsubfoveal involvement (7th = 3)
– Advanced atrophic with subfovealinvolvement (7th = 4)
• 6th character still indicates Right, Left, Bilateral or Unspecified
35

ICD-10-CM UpdatesExudative Age-Related Macular Degeneration
Deleted Codes
• H35.32: Exudative age-related macular degeneration– Lacks stage and involvement
– Lacks laterality
New Codes
• H35.32xx: Exudative age-related macular degeneration
• 7th character indicates– Stage unspecified (7th = 0)
– With active choroidal neovascularization(7th = 1)
– With inactive choroidal neovascularization (7th = 2)
– With inactive scar (7th = 3)
• 6th character still indicates Right, Left, Bilateral or Unspecified
36

ICD-10-CM UpdatesPrimary Open-Angle Glaucoma
Deleted Codes
• H40.11Xx: Primary open-angle glaucoma– Identified stage but not
laterality
– Used Placeholder “X” in 6th
character position
New Codes
• H40.11xx: Primary open-angle glaucoma
• 7th character indicates– Stage unspecified (7th = 0)
– Mild stage (7th = 1)
– Moderate stage (7th = 2)
– Indeterminate stage (7th = 3)
• 6th character now indicates Right, Left, Bilateral or Unspecified
37

ICD-10-CM UpdatesNew Codes
• H53.04x: Amblyopia suspect• H59.33x: Postprocedural hematoma of “X” eye
and adnexa following an ophthalmic procedure• H59.34x: Postprocedural hematoma of “X” eye
and adnexa following other procedure• H59.35x: Postprocedural seroma of “X” eye and
adnexa following an ophthalmic procedure• H59.36x: Postprocedural seroma of “X” eye and
adnexa following other procedure• 6th character identifies laterality
38

ICD-10-CM UpdatesRevised Codes
Revised From
• H59.31x: Postproceduralhemorrhage and hematoma of “X” eye and adnexa following an ophthalmic procedure
Revised To
• Postprocedural hemorrhage and hematoma of “X” eye and adnexa following an ophthalmic procedure
39

ICD-10-CM UpdatesDiabetes with Ophthalmic Manifestations
Code range E08 through E13 add laterality
Example: Deleted
• E08.321 Diabetes mellitus due to underlying condition with mild nonproliferative diabetic retinopathy with macular edema
Added • E08.3211 Diabetes mellitus due to
underlying condition with mild nonproliferative diabetic retinopathy with macular edema, right eye
• E08.3212 Diabetes mellitus due to underlying condition with mild nonproliferative diabetic retinopathy with macular edema, left eye
• E08.3213 Diabetes mellitus due to underlying condition with mild nonproliferative diabetic retinopathy with macular edema, bilateral
• E08.3219 Diabetes mellitus due to underlying condition with mild nonproliferative diabetic retinopathy with macular edema, unspecified eye
40

ICD-10-CM UpdatesDiabetes with Ophthalmic Manifestations
• Additional codes identify increased ophthalmic conditions– With proliferative and nonproliferative diabetic retinopathy
• Stable, mild, moderate, severe, or not indicated, with or without macular edema
– Diabetic macular edema resolved following treatment– Traction retinal detachment involving or not involving the
macula– Combined traction retinal detachment and rhegmatogenous
retinal detachment– New codes identify laterality and bilaterality
• Example– E11.3413 Type 2 diabetes mellitus with severe nonproliferative
diabetic retinopathy with macular edema, bilateral
41

Resources
• Medicare Coverage Database– https://www.cms.gov/medicare-coverage-database/indexes/lcd-alphabetical-
index.aspx?Cntrctr=379&name=&DocType=Active&LCDId=33467&ContrId=379&ver=13&ContrVer=1&CntrctrSelected=379*1&s=34%7c48%7c53%7c58&bc=AggAAAQAAAAAAA%3d%3d&
• Medicare Physician Fee Schedule– https://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/PhysicianFeeSched/index.html
43