Embed Size (px)
Citation preview

BritishJournal ofOphthalmology, 1990,74,700-701
Choroidal osteoma (osseous choristoma): an atypicalcase
G Cennamo, G Jaccarino, G de Crecchio, G Liguori
AbstractA case of choroidal osteoma presenting in a22-year-old girl is reported. The tumour,unilateral and in a juxtapapillary site, appearedmarkedly elevated on the retinal plane, notflat or slightly elevated as in previous reports.Visual acuity was not affected, and there was acomplete absence of subjective symptoms.Echography, fluorangiography, computerisedtomography, and visual field tests were per-formed. Echography is the best method foridentifying and differentiating this lesion froma malignant tumour.
UniversitA degli Studi diNapoli, I Faculta diMedicina e Chirurgia,Istituto di ClinicaOculisticaG laccarino
II FacultA di Medicina eChirurgiaIstituto di OftalmologiaG CennamoG de CrecchioG LiguoriCorrespondence to:Professor G Cennamo, ClinicaOculistica, II Policlinico, viaPansini 5, Napoli, Italy.Accepted for publication22 March 1990
Choroidal osteoma, or osseous choristoma, wasfirst described by Gass et al in 1978.' It is usuallypresent from birth and typically has a lowdevelopment potential. It presents unilaterally inmost cases, has a predilection for the female sex,and favours a juxtapapillary location, becomingclinically manifest when it involves the macula.It is usually diagnosed during the second andthird decades of life.2Ophthalmoscopy shows a circumscribed,
irregularly ovoid or round mass with definedborders. The colour is related to the degree ofthinning and depigmentation of the overlyingretinal pigment epithelium,' varying from adiffuse reddish orange, thus resemblingchoroidal haemangioma, to a yellowish whitecoloration which gradually shades peripherallyinto pinkish yellow, becoming indistinguishablefrom the surrounding healthy area.4We report here a case of choroidal osteoma
which, because ofits atypical features, presentedparticular diagnostic problems.
..
Figure 2 B-scan echogram showing a solid mass lesion ofextremely high reflectivityshadowing all the structures behind it.
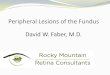
Figure I Left eye. A solid mass located in thejuxtapapillaryregion ofthe lower nasal quadrant. The mass had ayellowishwhite centre and was elevatedfrom the retinal plane.
Case reportA 22 year-old-girl presented without any pre-vious relevant medical history. The right eye wasnormal. In the left eye the visual acuity was 60/60and the anterior segment normal. A fundusexamination revealed a solid mass of approxi-mately 6x6 papillary diameters located in thejuxtapapillary region of the lower nasal quad-rant. The mass was elevated from the retinalplane by about 5 dioptres and had a yellowishwhite centre and pinkish yellow sloping edges(Fig 1). Standardised echography5 showed thelesion as a solid, raised subretinal mass with anextremely high reflectivity, observable even atthe anterior surface of the lesion and shadowingthe sclera and also the posterior orbital tissues6(Fig 2). The echographic images of the lesionwere of foreign body type, showing spikes ofextremely high reflectivity from the retinalsurface corresponding to the tumour site (Fig 3).In the remaining areas the thickness of the retinaand choroid was normal; the optic nerve was alsoof normal diameter and reflectivity.
Fluorescein angiography showed a pattern ofirregular hyperfluorescence overlying the tumourand evidence of diffuse staining of the tumoursurface during the later stages. Numerouscapillaries on the surface ofthe choroidal osteomawere present in the early phase of the angiogram(Fig 4). CT showed a radiodense lesion adjacentto the left optic nerve head, at the posterior pole,of the same density as normal bone (Fig 5).When the patient was seen a year after the first
observation, no variations of the mass werenoted.
DiscussionThe 5 dioptres elevation from the plane rendersthis case atypical. The clinical picture of thistumour - its location, unilaterality, its arisingfrom a single focus, and the patient's age when it
700
on August 29, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.11.700 on 1 N
ovember 1990. D
ownloaded from

Choroidal osteoma (osseous choristoma): an atypical case
imxmti&-_A WPAINure 3 Echogram obtained with standardised A-scan echography showing a lesion ofveryi reflectivity and posterior shadowing due to the presence ofbone tissue in the choroidal layer.arrow indicates a very low spike obtainedfrom the outer sclera.
was first observed facilitated its diagnosticdifferentiation from metastatic carcinoma,poorly pigmented malignant choroidal mela-noma, optic nerve tumours involving theposterior pole of the eye, choroid ossification(typical of the phthisical eye), retinoblastoma,and choroid haemangioma. But it is echographythat allows an exact differential diagnosis to bemade. Ultrasonically osteoma presents as a solidmass with a single spike of extremely highreflectivity which is not spontaneously mobile,with marked acoustic shadowing of the tissuebehind the lesion.
Ultrasonically malignant melanoma presentswith a regular, medium to low reflectivity withsudden rapid, spontaneous movements of thespikes indicating the presence of abnormalvascularisation. In contrast, the reflectivity ofthe metastatic carcinoma is medium to high andirregular, and spontaneous movements of thespikes are absent. With both these lesions, whenshadowing of the posterior orbital tissues is
Figure 4 Fluorescein angiography showing a pattern ofirregular hyperfluorescence overlyingthe tumour in the venous phase.
Figure 5 Computerised axial tomography scan showing thepresence ofa bony plaque in thejuxtapapillary region adjacentto the left optic nerve head.
present it is never so pronounced as it is inosteoma. The presence of a normal optic nervewith standardised A scan rules out the presenceof a primitive neoplastic tumour of this struc-ture.7
Ossification of the choroid is typical of thephthisical eye. The phthisical eye, because ofincreased thickness and folds of the choroid,shows a shadowing ofthe posterior orbital tissues.Moreover this shadowing may be due to calcifi-cation of the choroid, which is present in a veryadvanced stage of the disease and distributed in amottled fashion, not in a single mass as inosteoma. In retinoblastoma, in contrast tochoroid osteoma, there is no single spike of highreflectivity of foreign body type but rather aseries of spikes of high reflectivity originatingboth from the surface and from the neoplasticmass. These are referable to the presence ofirregularly distributed calcification inside thetumour.8
In conclusion, owing to clinical similaritieswith osteoma serious problems of differentialdiagnosis are encountered with calcified hae-mangioma of the choroid. CT and echographymakes identification and differentiation ofosteoma and calcified haemangioma possible.Osteoma presents as a single, compact, calcifiedmass, while calcified haemangioma presentsas bone surrounded by many large vascularchannels.91. Gass JDM, Guerry RK, JackRL, Harris C. Choroidal osteomas.
Arch Ophthalmol 1978; 96: 428-35.2 Baum M, Pinkerton AR, Berler DK, Kramer KK. Choroidal
osteomas. Ann Ophthalmol 1979; 11: 1849-51.3 Mc Leod BK. Choroidal osteomas presenting in pregnancy. Br
J Ophthalmol 1988; 72: 612-4.4 Gass JDM New observations concerning choroidal osteomas.
IntOphthalmol 1979; 1: 71-84.5 Ossoimg KC. In: Dallow CRL, ed. Standardised echography:
basic principles, clinical applications and results in ophthalmicultrasonography: comparative techniques Int Ophthalmol Clin1979; 19: 127.
6 Santoni G, Ricci AL, Lupidi G, Ciorba E, Fiore C. Choristomeosseux de la choroide bilateral et microphtalnie asymetrique.JFrOphtalmol 1988; 11: 363-7.
7 Ossoinig KC, Cennamo G, Frazier-Byrne S. Echographicdifferential diagnosis of optic nerve lesion. Doc OphthalmolProc Ser 1981; 29: 327-32.
8 Ossoinig KC, Cennamo G, Green RL, Weyer SML. Echo-graphic results in the diagnosis of retinoblastoma. DocOphthalmol Proc Ser 1981; 29: 103-7.
9 Reese AB. Tumours of the eye. 3rd ed. New York: Harper andRow, 1976: 266-7.
701
on August 29, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.11.700 on 1 N
ovember 1990. D
ownloaded from