Embed Size (px)
Citation preview

Sec. .Sci. Med. Vol. 30. No. I. PP. 3544, 1990 Printed in Great Britain. All rights reserved
0277-9536~90 53.00 + 0.00 Copyright c 1990 Pergamon Press plc
ONTARIO’S UNDERSERVICED AREA PROGRAM REVISITED: AN INDIRECT ANALYSIS
MALCOLM ANDERSON and MARK W. ROSENBERG
Department of Geography, Queen’s University, Kingston, Ontario, Canada K7L 3N6
Abstract-Financial incentive programs are used in various developed and developing countries to effect change in the geographic distribution of physicians. The Underserviced Area Program of Ontario is the longest running financial incentive program in Canada. It is described in detail and analyzed for its effectiveness in solving the problems of the maldistribution of physicians in northern Ontario. Using location quotients as an indirect measure shows that the maldistribution of physicians continues despite the implementation of the program. It is argued that the unidimensional solution of financial incentives cannot be used to solve the multidimensional issue of accessibility to health care in rural and remote areas.
Key words-physician maldistribution, location quotients, accessibility
INTRODUCTION Accessibility to health care is a multidimensional issue [ 11. It encompasses socio-cultural and political- economic influences, service providers and con- sumers. Within this broad perspective, one particularly important issue is the relationship be- tween the spatial distribution of physicians, con- sumers and health status.
In the province of Ontario, Canada’s most popu- lous province, universal health insurance was adopted in 1969 in accordance with the Federal Government’s 1966 Medical Care Act. Under this scheme (now known as the Ontario Health Insurance Plan-OHIP) universal coverage to the same medical care became available to all citizens in the province. Concomitant with the adoption of universal health care insurance came the recognition that economic access had to be linked to improved geographic access.
To meet this additional responsibility the Ontario Ministry of Health introduced, in 1969, the Underser- viced Area Program to address the underservicing problem in northern Ontario (Figs 1 and 2). In subsequent years the program was extended to in- clude areas in southern Ontario also considered to be underserviced.
The problems of the maldistribution of physicians and underserviced areas are neither nationally unique nor new. They are found in developed and developing countries alike and persist over long periods of time.
For these reasons, the theory behind the distribu- tion of physicians and international experience are reviewed. The Underserviced Area Program in the province of Ontario, Canada is then examined in detail. How successful has the program been? Loca- tion quotients for Ontario counties between 1956 and 1986 are used as indirect measures to assess the changing distribution of physicians in the province. The results of the analysis are then discussed in the context of the multidimensional nature of access to health care delivery.
THEORY AND INTERNATIONAL EXPERIENCE
The study of the distribution of physicians and underserviced areas is well documented in the geo-
graphical literature [24]. Two types of methodolo- gies are generally employed in these studies. The first is the calculation and mapping of population to physician ratios. Ratios are compared and areas classified as under- or overserviced based on an ideal population to physician ratio. The second methodol- ogy employed takes the number of physicians or the population to physician ratio per area as the depen- dent variable and one or several measures as indepen- dent variables. These are used in some form of the general linear model ‘to explain’ the distribution of physicians and the mapping of residuals can be used to identify under or overserviced areas.
Underlying both methodologies are the concepts of supply, demand and equilibrium theory. The number of physicians in an area or the population to physi- cian ratio are surrogate measures of the supply of health care services for the area. The characteristics of the population chosen as independent variables are surrogate measures of the demand for health care services for the area. Equilibrium is achieved where all variance in the dependent variable is explained by the independent variables or where one has a ‘perfect fit’ of the relationship between supply and demand. The fact that this does not occur (there is residual ‘unexplained’ variance) is generally interpreted as the mismatch between supply and demand. In its econo- metric form, the difference between the equilibrium supply and demand point and any other point is resolved through market adjustments in supply or demand.
In the policy arena, governments have increased the supply of physicians, tried to reduce demand for medical services and most commonly have used im- plicit or explicit financial incentives to induce physi- cians to locate in underserviced areas to resolve the disequilibria between the over-supply of physicians in some areas and unmet demand in others. The use of these strategies is recognition of the dominance of these methodologies and the theoretical perspective they represent in various countries regardless of whether a nation has a centrally planned or ‘free’ market health care delivery system.
It is not our intent to argue that this theoretical perspective should be rejected on ideological grounds or to dismiss it as fatally flawed on methodological
35

36 MALCOLM ANDERSON and MARK W. ROSESBERG
NORTHERN
ONTARtO
ONTARIO
Fig. 1. Northern and Southern Ontario.
grounds. Instead, we examine whether lack of supply under- and overserviced areas [5]. There was a per- or demand can be used to explain the maldistribution ception in the 1960s and early 70s of a crisis in terms of physicians and how a financial incentives program of physician manpower supply [6]. Thus new medical has operated. Further, we consider other factors that schools were opened and increasing numbers of go beyond the limits of this theoretical perspective. foreign physicians entered the country [7j.
LACK OF SUPPLY OR DEMAND?
Given that physicians can make their own location decisions how can governments and medical organi- zations affect this decision making process to improve the distribution of physicians over a given spatial area? One response in Canada during the 1960s was to increase the absolute numbers of physicians. This move, however, only increased the gap between
Table 1 shows the growth in numbers of physicians and physician to population ratios for three time intervals from 1961 to 1985. Clearly there have been significant improvements. Overall Canada’s ratio has improved from 1:857 in 1961 to 1:491 in 1985. This has been associated with an absolute increase in physicians from 21,266 to 51,966. Throughout this period, Ontario and British Columbia have had better ratios than the other provinces while New- foundland, New Brunswick, Saskatchewan and the
COUNTIES OF ONTARIO
: :=:I 3 flqh
a nlaqlm 10 nmllton-wultrwth ,, wotrloo II Prth 13 Hura 14 hea 1, ti.”
li Y&opdltan 1orato 25 Durham 24 Wstarllo 25 Nu*dm 26 Hdburton
39 Clnqwry 40 Pr*KOtt 41 RUlSdl 42 Ottow-Cerlsta 43 uonltoulbl 44 Pony 9wnd 45 wipiwlnp 49 nml8kominq 47 Sudburv 49 Alqomd 49 Coshrone 50 Knoro 51 lhvndr Boy 52 Rainy Riwr
Fig. 2. Counties of Ontario.
SOUTHERN ONTARIO

Ontario’s Underserviced Area Program revisited 37
Table I. Growth in number of physicians in Canada, 1961-1985 (including residents and interns)
1961 1979 1985
tot. No. P@P tot. No. PwP tot. No. PIPOP
Newfoundland 230 1991 732 758 97s 596 PEI 91 1149 120 983 165 77s Nova Scotia 706 1044 1388 595 1805 489 New Brunswick 455 1314 741 909 956 753 Quebec 6167 853 10,846 J73 14,393 459 Ontario 8040 776 15,121 544 19,481 469 Manitoba 1120 823 I732 588 2162 497 Saskatchewan 951 973 130s 702 1623 628 Alberta 1356 982 2731 663 4186 567 British Columbia 2150 758 4328 568 6152 471 Yukon - - 23 948 28 811 NWT - - 30 1410 40 1273
Canada 21,266 857 39,104 585 51,966 491
Sources: Judek S. Royal Commission on Health Services, Medical Manpower in Canada, 1964. Health Personnel in Canada, 1986. Health & Welfare.
territories have had high ratios in comparison. The total number of active physicians (excluding residents and interns) in Canada increased by 25% between 1979 and 1986, from 36,444 to 45,594 [8]. The above data rule out the lack of supply of physicians being the explanation for the lack of physicians in rural and northern areas. Given our theoretical framework, the alternative is to examine demand or rather the lack of it.
There are several reasons why rural areas have been considered unattractive to physicians. Two provincial government reports stress the following factors: isolation from professional colleagues and lack of educational opportunities, overwork (from a continual demand for services), increasing stress, lack of acceptable housing, limited social and cultural amenities, difficulty of finding temporary replace- ments, lack of medical resources/technology, con- straint on fee income and its growth potential, high cost of living and the high cost of establishing a practice [8,9]. In addition, rural practice is considered by some physicians as not giving professional satis- faction. Physicians are unable to use certain skills, have to resort to ‘band-aid’ medicine and often interesting cases have to be referred out.
From the point of view of the public, it has been their unmet demands, especially in northern and rural communities, which have led them to lobby provin- cial governments to intervene in the physician loca- tion process throughout the country. They generally feel that medical students are not adequately trained for rural practice as most of their training takes place in well equipped hospitals in the southern parts of Canada. There is also the suggestion that a bias may exist in medical schools against rural practice [9, p. 171.
Only one of the factors cited above, constraint on fee income and its potential growth, suggests a lack of demand for physicians in rural and northern areas. This is, however, contradicted by the noneconomic factors; most importantly, overwork (from a contin- ual demand for services) and the resulting stress which is also cited in the same reports.
Individual communities or isolated areas may not be able realistically to support the same mix of general practitioners and specialists found in major urban areas. The complaints of these communities,
however, regarding the lack of physicians and the complaints of physicians in these areas about over- work and stress do not suggest a lack of demand for health care services. The maldistribution of physi- cians, therefore, can only be explained at a theoretical level as a function of market failure.
GOVERNMENT RESPONSES: THE UNDERSERVICED AREAS PROGRAIM
OF ONTARIO
With the exception of Yukon and Northwest Ter- ritories, it is provincial governments who are respon- sible for the delivery of health care. Their concern for the availability of medical care in rural areas and the disproportionate representation of physicians in ur- ban centers compared with rural areas [lo] is a de facto recognition of market failure between the sup- ply and demand for physicians. The maldistribution has required governments and medical organizations to intervene in the traditional market demand and supply of physicians and to initiate policies directed at improving access to primary care in rural isolated areas.
Policies designed to influence the location behavior of physicians can be split into two broad categories: administrative controls and financial incentives [2]. Administrative controls are negative, usually restrict- ing the location possibilities for physicians new to an area. Such policies are presently being used in British Columbia and Quebec and are being considered by other provinces as a means to even out physician distribution. These types of control have met with opposition by many in the medical establishment [1 l-131.
In conjunction with administrative controls, but more commonly used on their own, financial incen- tive programs are designed to induce physicians to locate in northern and rural areas. The most common policy is that of providing financial incentives in exchange for return of service in designated underser- viced areas. Of the programs that exist in Canada where financial incentives are employed, the Ontario Underserviced Area Program (UAP) is the longest standing. For this reason, it is used as a case study.
The UAP was established in October 1969 follow- ing an increasing number of complaints received

38 MALCOLM ANDERSON and MARK W. ROSENBERG
from northern communities regarding accessibility to physician services. Initially, the program was established for northern communities but was soon extended to encompass ‘underserviced’ areas throughout the province. Presently, there are 30 northern and 5 southern communities requiring physicians through the program [14].
To be eligible, a physician must hold a license to practice in Ontario, hold a letter from the College of Physicians and Surgeons of Ontario indicating he/she is eligible for a license and be a Canadian or landed immigrant [14]. Vacancies are listed monthly in an information kit supplied by the Ministry of Health and the choice of where to locate based on this listing is up to the individual physician.
Bass and Copeman note that the ‘underserviced designation is based on the following factors: number and type of physicians in the area, their availability, population structure and its seasonal fluctuation, socio-economic status of the area, local demand for medical care, availability of housing and facilities for physicians and the area’s health needs and resources [15-171.
It is the local municipality’s responsibility to ensure adequate facilities and accommodation are provided. One hundred and twenty-six modem clinics have now been established. The Ministry of Northern Develop- ment and Mines provides up to 66% of capital with remaining funds coming from the federal and provin- cial governments and the communities themselves [17]. There is no provision for relocation expenses although municipalities may provide some form of assistance. Where possible the program attempts to establish physicians in groups of two or more.
The primary incentive of the program is an income tax free grant of S40,OOO which is paid quarterly (%lO,OOO/yr over 4 yr). The program also has an option instead for physicians to receive a guaranteed net professional income of $38,000 [14]. These amounts have not changed since 1980 [16].
In addition to these two components for estab- lished physicians, the program offers bursaries and preceptorships to medical students. These student programs were discontinued in 1974 due to “fiscal restraints and monetary conditions” [16]. More sig- nificantly, many students opted out of the program when it came time for their return of service require- ment. In addition, it was felt that enough response was being received by established physicians to the incentives program (181. It was not until 1978, with increasing numbers of practice vacancies that the program was reinstated. Between 1969 and 1974, of the 220 students who received bursaries only 110 fulfilled their service obligation. Of these, 73 re- mained in the community afterwards [17, 191.
Thirty-six bursaries of $5000 are awarded annually to Ontario students. Funded by the Ministry of Northern Development and Mines, students are ex- pected to return service in an underserviced area following their training [20].
By 1973,203 doctors had been on the UAP [ 151. By 1979 this figure had risen to 499, 275 of whom were still in practice. In 1979 the program was extended to include a limited number of incentive grants for specialists. These physicians received $20,000 paid over a 4 yr period. There was a high turnover of these
specialists due mainly to communities not providing ‘modern attractive facilities’ [15]. Presently, psychia- trists are most in demand with incentive grants for this one specialty up to $40,000 [20].
In addition to resident specialists, traveling special- ists visit northern communities to meet the local needs on a regular basis, providing consultation to both patients and staff. There are 16 nursing stations plus additional stations supplied by the federal gov- ernment on Indian reservations. Qualified nurses with clerical support maintain regular contact with doc- tors in the nearest communities. Administered by the nearest health unit the stations are visited at least once a week by a physician.
Recognizing the even greater difficulty in attracting specialists to northern areas, the Ontario Ministry of Health recently announced a Northern Medical Specialist Incentive Program which will run in associ- ation with the UAP. Designed to increase the number of specialists in northern Ontario, the program will again provide incentive grants of $40,000 paid over 4 yr. Incentives for traveling specialists will also be increased [20].
Outside the program other policies have been directed towards improving service in the north. As of 1981, four aircraft were used for ambulance ser- vices in the north. Between July 1981 and July 1982, 7253 patient transfers were handled using this service [ 191. There are also special programs such as those in Pickle Lake and Armstrong where the College of Family Physicians provide services on a rotational basis among its 2500 members [19].
Every northern community is also invited to take part in a 5 day recruitment tour of Ontario medical schools. Financed by the Ministry of Northern Affairs and Ministry of Health, the UAP also assists these communities in finding other health workers such as dentists and physiotherapists [19]. Over 50 communities participate in this promotional tour of southern Ontario.
The Ministry of Health places medical students, interns and residents in northern communities for a period usually between 1 and 3 months to expose students to northern practice before graduating. There are also direct links between southern universi- ties and northern communities such as Sioux Look- out Zone Hospital and the University of Toronto and an outreach program with the University of Western Ontario.
Presently there are over 575 physicians on the UAP working in over 200 communities [14]. The attrition rate has been between 5 and lO%/yr [16], but more recently has dropped to less than 5% indicating a high degree of satisfaction at least from the physi- cian’s point of view [14].
AN INDIRECT ASSESSMENT
The geographic distribution of physicians in Ontario is not a new issue for academics or policy analysts. Using physician to population ratios Spaulding and Spitzer [21] observed that, on average, there were an extra 414 people per doctor in northern Ontario compared to the south in 1961. By 1971 this figure had increased to 473. They add, however, that for primary physicians the ratio had improved for the

Ontario’s Underserviced Area Program revisited 39
Table 2. Physicians in Ontario, 1986
District
Family Specialist
N % N % Total
Southwest 979 49 1025 51 2004 Central West 1330 49 1384 51 2714 Central East 3711 47 4129 53 7840 Eastern 1138 43 1501 57 2639 Northeast 466 61 293 39 759 Northwest 200 65 109 35 309
Source: Physician Manpower in Ontario. Ontario Physician Man- power Data Centre, 1987.
north; moving from 1 to 2158 in 1961 to 1 to 2038 in 1971. Southern Ontario had only a slight rise from 1 to 1689 to 1 to 1694.
Similarly, Quenneville [22] indicated that most northern Ontario counties showed a decrease in their ratios between 1964 and 1974 as indeed had most southern counties.
Having modeled the change in location patterns of physicians in Ontario, Thrall and Tsitanidis [23] concluded that areas which had relatively good access to health services before the introduction of OHIP continued to do so after it was implemented. Areas that were poorly served prior to OHIP did not experience any change.
The Ontario Physician Manpower Data Center reported that in the four districts of southern On- tario, between 51 and 57% of registered physicians are specialists (see Table 2). In contrast, in the two northern districts just 35 and 39% of registered physicians are specialists [24].
For the northwest and northeast districts of Ontario 13.7% of general practitioners and 8% of specialists are female compared with the whole of Ontario figures which are 21 and 14% respectively [24]. In other respects, northern Ontario physicians
are similar in composition to those in the rest of the province (Table 3). They have similar age distribu- tions and sources of medical degree (181.
There are differences, however, in the numbers and distribution of these physicians. While the LJAP has been considered a success, there are still reports of severe shortages of health services in some areas. A recent survey indicated an immediate shortage of 150 physicians, nurses and other medical staff in northern Ontario [18].
Using physician to population ratios, it is clear that there are now more physicians serving the northwest and northeast districts (see Table 4). Each northern county experienced between 35 and 80% improve- ment in its ratio between 1956 and 1986. Similarly, the province as a whole improved its ratio by over 40%, moving from 971 people per physician in 1956 to 560 in 1986. More importantly though, has there been a redistribution of physicians to improve acces- sibility for northern residents to the level experienced by those living in southern Ontario?
Three measures can be used to examine this ques- tion: population per physician ratios, comparison to an absolute standard or location quotients. They are all closely related. The weakness of the population per physician ratio is that it only indicates whether one area has a higher or lower ratio than another. Comparing the ratio to an absolute standard over- comes this problem but there are the issues of how the standard is determined, its relevancy to the particular health care system and its time dependency. Location quotients overcome these problems by treating the ratio of physicians in a given geographic unit to the total number of physicians in all geographic units compared to the population in a given geographic unit compared to the total population of all geo- graphic units. It specifically indicates whether an area is underserviced or overserviced as compared to all geographic units.
Table 3. Phvsician characteristics in Ontario. 1986
sex (%) Age (%) Degree (%I
District M F 26-35 3650 51+ Ont. Can. Other*
Southwest 86 14 20 42 38 62 10 28 Central West 84 16 19 41 30 57 10 33 Central East 80 20 21 44 35 58 12 30 Eastern 81 19 21 45 34 52 19 29 Northeast 88 12 27 40 33 54 13 33 Northwest 85 I5 30 35 35 51 16 33
*Includes physicians whose degree origin is ‘unknown’. Source: Physician Manpower in Ontario. Ontario Physician Manpower Data Centre, 1987.
Table 4. Physicianpopulation ratios for northern Ontario counties, 1956-1986
1956 1961 1966 1971 1976 1981 1986
Norrheasr Algoma I : 1675 I:1513 I:1171 I:1140 I:836 I:867 I:749 Cochranc 1:1446 I:1621 I:1264 I:1183 I:976 I:950 I:781 Manitoulin 1~3687 I:3725 I:3575 I:1562 I:1362 I : 3667 I:755 Nipissing I:1639 I:1217 I:1114 1:1111 I:834 I:787 I:705 Parry Sound I:1653 I:1347 I:1133 I:1008 I:883 I:780 I:752 Sudbury Mun & R I:1943 I:1238 I:1153 I:1138 I:1095 I:939 I:728 Timiskaming I:1289 I:1108 I:1310 I : 1367 I:911 I:765 I:840
Northwest Kenora I:1562 I:1608 I:1749 I:1566 I:1160 I:1142 I:839 Rainy River I:1960 I:1769 I:1844 I:1515 I:854 I:991 I:880 Thunder Bay I:1159 I:1117 I:984 I:962 I:749 I:794 I:708
Source: Ontario Medical Directories 1956-1981. Ontario Physician Data Center, 1987. Census Canada 1956-1986.
SSM 3wI--D

40 MALCOLM ANDERKJN and MARK W. ROSENBERG
The location quotient is calculated as follows:
LQ: = (P:l~o~f)l(P:,,/po~:,,)
where
LQ: = location quotient for region i at time t; Pi = number of physicians in region i at time t;
POP, ’ = population of region i at time 1; Cl = total number of physicians in all regions in
time t; POP :0, = total population in all regions in time t.
A value of less than 1.0 indicates an under-represen- tation of physicians while greater than 1.0 indicates an over-representation. A value of 1.0 indicates a geographic unit has exactly the number of physicians its population warrants, given its share of the total population. Furthermore, Joseph and Phillips note that “values below unity are compressed in the range 0 to 1 .O, whereas values above unity may range from 1.0 to infinity, so that a location quotient of 0.5 reflects an amount of underservicing equivalent to the overservicing implied by a value of 2.0” [2, p. 791.
The data used in the location quotient analysis come from three sources. The population data are from the Censuses of Canada for the respective years analyzed. The physician distribution data come from the Canadian Medical Association’s Canadian Medi- cal Directory for 1956-1981. The 1986 physician data come from the Ontario Physician Manpower Data Centre.
Until 1977, when the Ontario Physician Manpower Data Centre was established, the Canadian Medical Directory was the only consistent source of informa- tion on physicians and their locations. It includes all full-time, part-time and nonpracticing physicians as well as interns and residents who are members of the Canadian Medical Association. The Ontario Physi- cian Manpower Data Centre allows one to distin- guish practicing full and part-time physicians from nonpracticing physicians and interns and residents.
The effect of the differences in definition can be compared for 1981. Using the Canadian Medical Directory, the number of physicians in Ontario is 15,452. Using the Ontario Physician Manpower Cen- tre data, the number of physicians in Ontario is 13,334. This suggests that the Canadian Medical Directory inflates the number of physicians by about 15.8%. Since the Ontario Physician Manpower centre only identifies 267 active physicians not involved in patient care in 198 1, most of the inflation is the result of counting interns and residents who are concen-
trated in those counties with university health sci- ences centers. If nonpracticing physicians, interns and residents were deleted from the calculations for 1956-1981, the effect on location quotients would be to increase slightly the values for northern Ontario Counties, decrease slightly the values for southern Ontario Counties in general and in particular to decrease the values in counties where there are univer- sity health sciences centers.
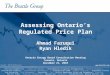
Between 1956 and 1986, not one county in north- em Ontario recorded a location quotient equal to 0.8 or better (see Table 5). With the exceptions of Thunder Bay, Cochrane and Timiskaming, northern counties showed some degree of improvement. The important point to consider, however, is that no county in northern Ontario presently has a location quotient which indicates that the proportion of physi- cians to the total number of physicians in Ontario is equal to the proportion of the county population to the total provincial population even after 17 yr of the UAP (1969-1986).
The counties of southern Ontario can be divided into four distinct groups (Figs 2-5). At each interval, the highest values are consistently recorded in the counties of Frontenac, Ottawa-Carleton, Metropoli- tan Toronto, Middlesex and Hamilton-Wentworth. This is not surprising as each county contains a university health science center and has a higher than average proportion of specialist physicians.
Of the remaining 40 counties in southern Ontario, 9 counties had location quotients below 0.5 and 12 counties had location quotients of 0.5-0.749. The other counties had location quotients approaching unity. In 1986, the counties with the lowest values (location quotients less than 0.5) also had less than 20% of their physicians registered as specialists.
In the counties of northern Ontario and those in southern Ontario where location quotients are below 0.75, and are not adjacent to counties with location quotients above unity, people are truly underserved. For the people of these counties, it cannot be argued that the lack of physicians within their county boundaries can be offset by cross boundary travel to counties with over-supplies of physicians.
In southern Ontario, counties where location quo- tients are below 0.75 and are adjacent to counties with location quotients above unity, the undersupply of physicans may not be as serious an issue because cross boundary travel to counties with over-supplies of physicians can remedy the problem (see below).
Many of Ontario’s counties are, however, areally
Table 5. Location auotients for northern Ontario counties, 19561986
1956 1961 1966 1971 1976 1981 1986
Algoma 0.580 Cochrane 0.739 Manitoulin 0.263 Nipissing 0.594 Parry Sound 0.588 Sudbury Mun & District 0.718 Timiskaming 0.754
Kcnora 0.622 Rainy River 0.49s Thunder Bav 0.838
Norrhearr 0.623 0.684 0.592 0.576 0.2S3 0.152 0.775 0.719 0.700 0.707 0.761 0.695 0.740 0.612
Northwest
0.586 0.458 0.533 0.434 0.844 0.814
0.646 0.714 0.615 0.610 0.539 0.438 0.663 0.715 0.731 0.676 0.647 0.545 0.539 0.655
0.660 0.602 0.156 0.727 0.734 0.610 0.748
0.747 0.716 0.741 0.793 0.744 0.769 0.666
0.470 0.514 0.501 0.667 0.486 0.699 0.577 0.636 0.765 0.796 0.721 0.791
Sources: Ontario Medical Directories 1956-1981. Ontario Physician Manpower Data Center, 1987. Census Canada 19561986.

Ontario’s Underserviced Area Program revisited
NORTHERN ONTARIO
LOCATION OUOTIENTS
m > 1.000
m .750 - ,999
a ,500 - ,749
0 < .500
SOUTHERN ONTARIO
41
Fig. 3. Location quotients by county, Ontario, 1956.
larger than countries in other parts of the world. This means that within counties, even those where there are university health science centers (location quo- tients above 1 .O), communities may be geographically distant from the university health science center and underserved. For example, Frontenac County in east- em Ontario is 120 km from its southern edge on Lake Ontario to its northern edge. It has a location quo- tient of 1.841 because of the university health sciences center in a city on the shores of Lake Ontario. The rural townships of the northern part of the county have only a few general practitioners making these underserved areas within the county.
It should also be noted that in some cases, changes in location quotient scores are a result of changes in
the size of the population not changes in the number of physicians. For example, Victoria county, having had a value of 0.586 in 198 1 ‘leapt’ to 1.013 in 1986. In actual fact, the number of physicians increased by just one specialist. The changing location quotient value is due to a heavy loss of population (a decline of 11% between 198 1 and 1986).
While Ontario’s population increased by 4.2% between 1976 and 1981, the northern districts experi- enced a slight decline (0.3%). More significantly, while Ontario’s population again rose between 1981 and 1986 (by 5.2%), northern Ontario suffered an overall loss of 2%. Thus improved location quotient values in northern Ontario have been assisted by falling population levels.
LOCATION OUOTIENTS
m > 1.000
&$cJ *750 _ *ggg
a .500 - .749
0 < .500
Fig. 4. Location quotients by county, Ontario, 1966.

MALCOLM ANDERSON and MARK W. ROSENBERG
NORTHERN ONTARIO I
LOCATION OUOTIENTS
m > 1.000 fgzJ .750 - .999
a .500 - .749
( < ,500
Fig. 5. Location quotients by county, Ontario, 19%.
Given the population, number of physicians and location quotient of each county in northern Ontario in 1986, a redistribution of approx. 366 physicians would have to take place to bring the location quotients in northern Ontario to approximate unity. Clearly, there is a need for more physicians in the north. That point is not disputed. What is con- tentious is notion of the redistribution of 366 physi- cians and how to achieve this.
If there are distribution problems for all physicians comparing counties in southern and northern On- tario, the distribution problems for specialists are even greater. For all of northern Ontario, there were no specialists in allergies and immunology, geriatrics, infectious diseases, and pediatric surgery as well as several medical laboratory specialties in 1986. There
was only one specialist for all of northern Ontario in dermatology, endocrinology, nephrology, neurology, and rheumatology. Needless to say, that if these data were converted to location quotients as well as the data for many other specialties where there are only two or three physicians for all of northern Ontario using the relevant age and gender specific data for the population variables, location quotients would be extremely low for every county of northern Ontario.
DISCUSSION
It is difficult to assess accurately the effectiveness of the UAP. More physicians are now practising in northern Ontario than there were prior to 1969, but that is true of the rest of the province as well. Second,
NORTHERN ONTARIO
LOCATION OUOTIENTS
Fig. 6. Location quotients by county, Ontario, 1986.

Ontario’s Underserviced Area Program revisited 43
there is no way of knowing whether there would be more, less or the same number of physicians had there not been a program in effect. To these queries we could perhaps ask the hypothetical questions of would the program have been more effective had incentives other than financial been offered and is the north receiving a particular type of physician as a result of the financial incentives?
Sources such as Copeman [ 15, 16,201 and Bass and Copeman [17] suggest that the program has indeed been a success. Without falling back on a ‘what if the program had not been in place’ perspective, the indirect measures discussed above appear to suggest that while some change has been made, northern Ontario is as underserviced compared to the rest of the province as it was in 1956. Northern Ontario in particular is suffering shortages in qualified psychia- trists, obstetricians, orthopedic surgeons, anes- thetists and dermatologists. Clearly, northern residents are not adequately catered for in terms of accessibility under the 1966 Medical Care Act. The UAP has gone some way to improve the situation but inequities in the present system still remain-similar to the situation prior to 1969.
In the introduction, it was suggested that accessi- bility to health care is a multidimensional issue. For all intents and purposes, however, the UAP is a unidimensional solution based on financial incen- tives. Although this may ease the burden of a north- em practice, it is not enough. What is needed is greater attention given to quality of life factors such as work environment, social/recreational facilities, opportunities for further training, and suitable hous- ing. In addition, more publicity needs to be given to the positive features of a northern practice, more importance placed on rural practice in medical schools and more support facilities made available to northern medical practitioners. Consideration also needs to be given to the families of physicians, the unique characteristics of the residents of underser- viced areas and alternative methods for delivering health care.
In the early 197Os, “the biggest problem in getting a doctor to stay in a rural community [was] the doctor’s wife. If she [was] not kept happy and busy, she [would] persuade the doctor to leave . . . . Availability of good educational facilities is one of the major concerns of the wife” [15]. Today, despite the somewhat dated remarks above, quality of life is still an important consideration-one that warrants as much if not more attention than that given to financial incentives which presumably are attempts to make-up for perceived lifestyle inadequacies. AS one northern general practitioner commented “The draw- back is still the time commitment. They try to entice people with money, but no money in the world can pay for that [work] overload” [18]. Other anecdotal evidence suggests more should be done for northern communities and physicians other than just financial incentives [25].
Another important consideration is the specific requirements of the northern population. Forty-five percent of aboriginal people in Ontario live in the northern counties [26] and their specific health needs differ from those of European descent. Those physi- cians working in the north should be made aware of
their specific health concerns before they commence their northern practice.
Northwestern Ontario has the highest crime rates of all Ontario [27] and fatalities caused by drinking and driving in the north are above the provincial average [28]. In short, medical practice in northern Ontario must go further than addressing just the physiological needs of communities. Physicians must be trained and prepared to remedy the social ills as part .of a multidimensional health care service which in turn would influence the nature and extent of physiological health needs. Presently, the UAP has no provision for such training.
There is also a set of strategies that should be implemented in conjunction with the above consider- ations but could be implemented regardless of the resolution of the physician distribution problem. The increased recruitment and utilization of nurse practi- tioners and paramedics and the legalization of mid- wifery are ways of improving health care delivery. If physicians or alternative health care personnel cannot be in place in an area, subsidized travel should be available for patients and close relatives to go to urban centers for the necessary treatment.
FINAL COMMENTS
Accessibility to health care is a multidimensional issue. Of prime importance in the context of accessi- bility is the distribution of physicians. In countries developed and underdeveloped, the maldistribution of health care delivery resources is reflected in an under-representation of physicians in rural areas.
At the theoretical level, regardless of ideological context, it has been and continues to be common to treat physician distribution as a supply and demand issue. Where governments have recognized the mis- match of supply and demand, intervention has gener- ally taken the form of increased financial incentives to locate in underserviced areas.
The distribution of physicians has been examined in detail in this paper by analyzing the Underserviced Area Program of the province of Ontario, Canada. Using location quotients, there appears to be little improvement in physician distribution in the north compared to southern Ontario. The mapping of location quotients revealed certain areas being under- serviced compared to others. This provided the groundwork for further discussion of physician ac- cess and the problems of treating a multidimensional issue with a unidimensional solution.
Programs have been implemented (and will con- tinue to be) to improve the maldistribution of health care resources in developed and developing countries alike. Most common is the use of financial incentives and, more recently, disincentives for locating in cer- tain areas. (For example, the province of Quebec has instituted a program of disincentives for locating in certain designated urban areas.)
The medical profession has the power and moral obligation to provide services to those in need accord- ing to the Hippocratic Oath they take. If restrictions are imposed to limit the number of general practi- tioners, for example in metropolitan areas, then we may see a decline in general practice graduates and a rise in the numbers of specialists whose services can

44 MALCOLM AF~DERKIN and MARK W. ROSENBERG
only be used in urban centers. The onus is on the medical profession to instill both moral and func- tional significance to rural practice in medical school curricula. Together with a period of rural service, students would then be better trained and would recognize the opportunities to serve rural areas, becoming more familiar with the supply of rural medical resources and specific rural concerns.
From a government perspective, there needs to be coordination of action and policy on behalf of all levels of government. The problems that each faces are similar, as indeed are the methods used to remedy the situation. Advocated then is a mechanism whereby those ‘players’ involved with physician and health care distribution in underserviced areas can meet and coordinate ideas and policy on a nationwide basis. The collective experience of all regions must help to facilitate a better understanding of the prob- lems currently faced.
Finally, physicians and policy makers alike need to add a humanist perspective to a problem that for the most part has been approached with statistics and financial incentives in hand. Quality of life consider- ations for both those demanding and those supplying health services should be of prime importance to everyone in resolving the problem of medically under- served areas.
Acknowledgements-We would like to express our appreci- ation to Carolyn Fielding for her assistance with the com- puter cartography.
1.
2.
3.
4.
5.
6.
7.
8.
REFERENCES
Rosenberg M. W. Linking the geographical, the medical and the political in analysing health care delivery. Sec. Sci. Med. 26, 179-186, 1988. Joseph A. E. and Phillips D. A. Accessibility and utiliiation: Geographical Perspectives on Health Care Deliverv. Hamer & Row. New York, 1984. Rosenberg MI W. Accessibility to health care: a North American perspective. Prog. Human Geogr. 7, 78-87, 1983. Rosenberg M. W. General approaches to health care delivery. In Themes in Medical Geography (Edited by Akhtar R.). Harwood, London. In press. Joseph A. E. and Bantock P. R. Measuring potential physical accessibility to general practitioners in rural areas: a method and case study. Sot. Sci. Med. 16, 85-90, 1982. Bean I. W. Future manpower needs in G.P. Can. Med. Ass. Jl. 97, 1573-1577, 1967. In 1961 there was a total of 21,266 physicians (including interns and residents) in Canada. See Judek S. Royal Commission on Healih Services: Medical Manpowe; in Canada. The Queen’s Printer, Ottawa, 1964 and Health and Information Division. Active Civilian Physicians by Type of Physician, Canada, by Province, 1987, Depart- ment of National Health and Welfare, Ottawa, 1988. In December, 1979, there were 18,000 specialists and 18.444 neneral and familv mactitioners. By December,
9.
10.
11. 12. 13. 14.
15.
16.
17.
18. 19.
20.
21.
22.
23.
1986, these numbers had risen to 22,061 and 23,533 respectively. Standing Committee on Medical Man- power. Annual Report, 1987, Manitoba Health Services Commission, Winnipeg, 1988 and Health and Informa- tion Division. Interprovincial Migration of Physicians, Department of National Health and Welfare, Ottawa, March 1988. Report of the Minister’s Advisory Committee on Rural Medical Practice. Rural Medical Practice, Regina, Saskatchewan, 1985. For example, 78.1% of licensed medical practitioners in Manitoba are located in Winnipeg. In Winnipeg, the ratio of population per physician is 393 to 1 whereas for remote areas of Manitoba, it is 1006 to I (Toronto Star 12 March, 1987). Toronto Star 24 March, 1987. Winnipeg Free Press I June, 1987. Vancouver Sun 23 April, 1988. Ministry of Health. Underserviced Area Program Kit, June, 1988 Vacancies, Government of Ontario, Toronto, 1988. Copeman W. J. 177 of 203 doctors stay in underserviced area. Ontario Med. Rev. 774-776, December 1973. Copeman W. J. Underserviced Area Program: a IO-year success story. Ontario Med. Rev. 523-524, 532, October 1980. Bass M. and Copeman W. J. An Ontario solution to medically underserviced areas: and evaluation of an ongoing program. Can. Med. Ass. II. 113, 403407, 1975. The Toronto Star 8 November, 1987. Ontario Council of Health. Medical Manpower for Ontario. Ontario Ministry of Health, Toronto, 1983. Copeman W. J. The Underserviced Area Program of the Ministry of Health of Ontario. Can. Family Phys. 33, 1683-1685, 1987. Spaulding W. B. and Spitzer W. 0. Implications of medical manpower trends in Ontario. 1961-1971. On- tario Med. Rev. 39, 527-533, 1972. Quenneville G. M. J. The distribution of physicians in Ontario 1964 to 1974. Unpublished thesis. Department of Geography, University of Windsor, Windsor. Canada,-1975: Thrall G. I. and Tsitanidis J. G. A model of the change, attributable to government health insurance plans, in location patterns of physicians-with supporting evidence from Ontario, Canada. Environ. Plann. C: Govnmt Policy 1, 45-55, 1983.
24. Ontario Physician Manpower Data Center. Physician Manpower in Ontario. Government of Ontario, Toronto, 1987.
25. The New Democratic Party of Ontario. Miles to go. Health care in northern Ontario. Report of the Ontario NDP Caucus. New Democratic Party of Ontario, Toronto, November 1984.
26. 24,945 aboriginal people live in northern Ontario repre- senting 14% of the total northern Ontario population. Statistics Canada. Profires Part 2. Census of Canada. Suoolv and Services Canada, Ottawa, 1986.
27. Pr&cial Secretariat for Justice. Jusrice Statistics. 05ce of the Solicitor General of Ontario, Toronto, 1984.
28. Provincial Secretariat for Justice. A Report of the Inter- ministerial Committee on Drinking and Driving. Office of the Solicitor General of Ontario,?oronto, August 1974.