Embed Size (px)
Citation preview

Leukemia Research 31 (2007) 1327–1338
Clinical review
On the evidence for seasonal variation in the onset ofacute lymphoblastic leukemia (ALL)
Fei Gao a,∗, Kee-Seng Chia b, David Machin a,c,d
a Division of Clinical Trials and Epidemiological Sciences, National Cancer Centre, Singaporeb Centre for Molecular Epidemiology, National University of Singapore, Singapore
c School of Health and Related Research, University of Sheffield, UKd Children’s Cancer and Leukaemia Group (formerly UKCCSG), University of Leicester, UK
Received 3 February 2007; received in revised form 3 February 2007; accepted 2 March 2007Available online 4 May 2007
Abstract
Inconsistent seasonal patterns in peak presentation of acute lymphoblastic leukemia have been reported but no formal synthesis of publishedreports has been attempted to date. We extracted monthly tabulations of cases from publications and reanalysed using an angular methodologyand the von Mises distribution. Twenty-four articles from 11 countries in locations ranging from 35.05◦S to 65.01◦N were identified. Formalsynthesis established weak evidence for seasonality in adults and children. Were seasonality present, and arising from a climatic determinant,one might anticipate peaks of an increasing magnitude as the associated latitude moved away from the equator. No such pattern was apparent.© 2007 Elsevier Ltd. All rights reserved.
Keywords: Acute lymphoblastic leukemia; Angular methods; Seasonality; von Mises distribution
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13282. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1328
2.1. ALL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13282.2. Literature search . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13282.3. Statistical analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1328
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13293.1. Studies identified . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13293.2. Reported conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1329
3.2.1. First symptom . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13293.2.2. Onset . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13293.2.3. Arrival to hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13293.2.4. Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1329
3.2.5. Registration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13343.3. Angular reanalysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13343.4. Influence of age and latitude . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13353.5. Estimating lag . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1336
∗ Corresponding author at: Division of Clinical Trials & Epidemiological Sciences, National Cancer Centre, 11 Hospital Drive, Singapore 169610,Singapore. Tel.: +65 62369442; fax: +65 62250047.
E-mail address: [email protected] (F. Gao).
0145-2126/$ – see front matter © 2007 Elsevier Ltd. All rights reserved.doi:10.1016/j.leukres.2007.03.003

1328 F. Gao et al. / Leukemia Research 31 (2007) 1327–1338
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1336Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1337
. . . . . .
1
trtsGNhssoipitoedrgaIghtcso
(raas
2
2
nbddl
t
ieae
2
aoo
suwAw
2
tmfpdGsi((tpistatnfc(
(tr
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
Many infectious and some chronic diseases have charac-eristic seasonal onsets [1] and in certain cases, these seasonalhythms may provide insight into potential risk factors forheir development [2,3]. The first published interest in theeasonality of leukemia appears to be that of Lambin anderard [4] (see Allan [5]) in Belgium and which reported aovember–February peak of acute leukemia. Since then thereave been numerous reports concerned with investigating theeasonality of presentation of leukemia. While many of thesetudies have not identified an obvious seasonal pattern [6],thers have found significant seasonal variation [2,7]. Thenconsistency perhaps reflecting various levels of betweenopulation heterogeneity and different patterns of seasonal-ty induced by possible causative agents. It is also possiblehat seasonality may be more pronounced within subtypesf leukemia or within particular age groups. Thus, Gilmant al. [8] found little evidence of seasonality in a nationalataset from Great Britain, but have noted seasonality in aegional dataset from the West Midlands, England. They sug-est: “further work on seasonality needs more sophisticatednalysis, controlling for broad geographical heterogeneity”.n fact methodological differences both in terms of patientroups studied and statistical techniques employed may alsoave obscured underlying patterns. However, no formal syn-hesis of published reports has been attempted to date. As aonsequence, the aetiology of leukemia with respect to a sea-onal (including climatic as expressed by latitude) componentr otherwise remains uncertain.
In this study we focus on acute lymphoblastic leukemiaALL) and review the previous publications on seasonality,eanalyse wherever possible using a common methodology toscertain if there is any effect of latitude and between childrennd adults in respect to the timing and strengths of any peakso established.
. Methods
.1. ALL
Although the current ALL classification follows the Inter-ational Classification of Diseases, 9th Revision (ICD-9) [9]ecause of the time-span covered not all studies used thisefinition. Although there are some histological differences
ependent on maturity of the cells, we consider both acuteymphatic leukemia and acute lymphocytic leukemia as ALL.The leukemias often have somewhat insidious onsets andhe precise onset may be hard to pinpoint. In the studies
atdi
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1337
dentified, investigators used dates corresponding to differ-nt ‘event’ types: onset of symptoms; onset of clinical signs;rrival to hospital; diagnosis and registration (Table 1). Forxpository purposes we term these as the ‘start’.
.2. Literature search
To identify all published studies concerned with season-lity in ALL the distinction between the different cell typesf leukemia was not made initially. We began with the bibli-graphy of Allan and Douglas [10].
The next stage was a further comprehensive literatureearch repeated systematically over time until February 2006sing the PubMed database. The terms used in the searchingere: seasonality AND leukemia, seasonal AND variation*
ND leukemia. The references in those studies identifiedere also searched.
.3. Statistical analysis
Only one publication used precise dates of start forheir analyses, while the majority either included summated
onthly or seasonal tabulations (or these could be extractedrom text figures) upon which they based their analyses. Torovide a common standard to both individual and groupedata sets we have adopted the angular methods detailed byao et al. [11]. Data are first transformed to a standard year
et at 360 days, or 12 months of equal duration, so that eachndividual or mid-month can be represented as a point θ
0◦ ≤ θ < 360◦) on a circle of unit radius with coordinatessin θ, cos θ). To examine for the presence of a distinct peakhe von Mises distribution was used. This assumes a singleeak for seasonality and has two parameters (μ, κ), where μ
s the date of the peak and κ is related to the inverse of thetandard deviation of the distribution. The latter is also relatedo the magnitude of the peak, R. Small values of R would usu-lly indicate the absence of seasonality whilst those close tohe maximum of 1 would indicate a very sharp peak in theumber of cases. The Mardia statistic, χ2
M, with 2 degrees ofreedom tests for departures from a uniform distribution ofases over the year. Peak dates are presented in the formatmonth, day) of a 365-day year.
Although explicit formulae for 95% confidence intervalCI) of the peak date μ are available, these depend on rela-ively large sample approximations and so these have beeneplaced by ‘bootstrap’ methods (see Gao et al. [11]) for
ll situations regardless of study size. However, althoughhe majority of the methodology is applicable to groupedata, the ‘bootstrap’ method of calculation for CI’s requiresndividual dates for each subject within the study. To pro-
Researc
vnodac
at
3
3
as[rpic
wro
Entb
bWtwIcl
[ip
trltwAm
D[(
gi
3
bcusttobo
3
cNLls
3
d[swnMeNwn0fs[
3
wds(
t
3
F. Gao et al. / Leukemia
ide these, the corrected monthly counts (rounded to theearest integer) were assumed to be distributed uniformlyver the corresponding bin of 30◦ (1 month) and a ran-om sample equal to the number of cases within the binre taken from that bin to provide the ‘individual’ θ for thealculations.
The corrected monthly data over the years were plotted inrepeated histogram format, beginning with July, full year,
o end June, to emphasize the circular nature of the calendar.
. Results
.1. Studies identified
The bibliography of Allan and Douglas [10] lists 45rticles published between 1934 and 1987 on aspects of sea-onality of leukemia. However one article appeared twice12] and 8 of these 44 were not relevant to our aims. Of theemaining 36 articles, there were 16 non-English languageublications in 8 languages (French, German, Italian, Pol-sh, Russian, Spanish, Serbian, Ukrainian) of which 1 had noitation date and we were not able to trace.
The literature search identified 39 articles, but only 12ere relevant or had not been identified previously. From the
eferences in those studies listed by Ross et al. (Table 2) [13]ne additional article was identified [14].
This process identified a total of 49 articles (17 non-nglish language). Of these, 24 articles, comprising 11ations, have examined seasonal variation in the presenta-ion of ALL specifically. These are summarised with somerief comment in Table 1.
For convenience of tabulation the studies are ordered firsty their latitude (South to North) and then by longitude (fromest to East) in Table 1. In several of the studies conducted,
he precise geographical location of the study populationas not reported. In others the whole country was included.
n these circumstances we have taken the nearest major orapital city (of country or state) to define the latitude andongitude.
Six studies do not provide monthly data [15–20] while one21] provides monthly data on onset but not the correspondingnformation on diagnosis although they indicate the lattereaks in November.
Studies have been conducted in South Africa with lati-ude 35.05◦S, and in the Northern hemisphere with latitudesanging from 1.16◦N (Singapore) to 65.01◦N (Northern Fin-and) and longitude ranging from 123.39◦W (Oregon, USA)o 103.51◦E (Singapore). No studies South of latitude 40◦Sere identified, and none from Central and South America,ustralasia, most of Africa, Eastern Europe, India, China anduch of Asia.
The periods covered ranged from 1931 to 1934 [18] inenmark to the most current 1996–2000 from Shiraz, Iran21]. The size of the groups ranged from 27 to 5532 casesmedian 310). Many were also confined to particular age
am(a
h 31 (2007) 1327–1338 1329
roups, for example, 0–3 years in Denmark [20] to all agesn the USA [22].
.2. Reported conclusions
The abbreviated conclusions from these studies, as giveny the corresponding investigators, are detailed in the finalolumn of Tables 2–6 , which are each confined to a partic-lar ‘start’ measure. These ‘start’ measures include onset ofymptom (3 populations), onset of clinical signs (7), arrivalo hospital (2), diagnosis (33) and registration (1). Most ofhe earlier studies are based on the examination of symptomsr onset and the later studies on the date of diagnosis. Wester-eek et al. [23] and Karimi and Yarmohammadi [21] reportedn both symptoms and diagnosis.
.2.1. First symptomFor first symptoms (Table 2), all 3 studies are confined to
hildren although the age groups are not entirely consistent.o strong evidence of a (single) peak was indicated in Greaterondon [24] and Greater Manchester and Lancashire, Eng-
and [23] while in Shiraz, Iran [21] there was a statisticallyignificant peak noted (October) for children (0–15 years).
.2.2. OnsetThe findings with respect to the 7 studies of onset are
iverse (Table 3). Most are confined to the young except Lee7] who also studied those aged 20–44 years. For children aummer peak was noted in England and Wales [7] contrastingith a Southern Hemisphere winter peak from June to Augustoted in Capetown, South Africa [16] and spring peak fromarch to May noted in the USA [15]. On the other hand
vidence for a bimodality of peaks was reported from Easternebraska, USA [25]. No strong evidence of a (single) peakas indicated in Oregon, USA [26]. Mainwaring [17] onlyoted an excess in the summer (May–October) for cases aged–4 years, although not statistically significant, and no peakor cases aged 5–15 years in Liverpool, England. The onetudy of adults suggests a summer peak in England and Wales7].
.2.3. Arrival to hospitalTwo studies were identified (Table 4). A significant peak
as reported at January 3, in this case using individual patientata, in Skovde, West Gotaland Region, Sweden [27], whereeasons are markedly different but the sample size is small79 cases).
No strong evidence of a (single) peak was indicated inhose 0–79 years in Russia [28].
.2.4. DiagnosisAmong the 33 studies that examined diagnosis (Table 5),
peak in October for children (0–3) was noted in Den-ark [20] and a similar peak in November for children
0–15) was also noted in Shiraz, Iran [21]. There weregreater number of cases during summer (May–October)

1330 F. Gao et al. / Leukemia Research 31 (2007) 1327–1338
Table 1Published studies identified on the seasonality of ‘start’ of ALL (first author only cited for brevity)
Study Latitude Longitude Period ‘Start’ Age (year) N
Lanzkowsky (1964), Capetown, South Africa 35.05S 18.00E Not given Onset 0.1–13 27Gao (2005), Singapore 1.16N 103.51E 1968–1999 Diagnosis All 939Gao (2005), Hawaii, USA 21.18N 157.52W 1973–1999 Diagnosis All 393Karimi (2003), Shiraz, Iran 29.37N 52.33E April 1996–March 2000 Symptom diagnosis 0–15 211Harris (1987), Metropolitan Atlanta, Georgia,
USA33.45N 84.23W 1975–1980 Diagnosis 0–19 60
Gao (2005), Metropolitan Atlanta, Georgia,USA
33.45N 84.23W 1975–1999 Diagnosis All 570
Gao (2005), Los Angeles, USA 34.03N 118.15W 1992–1999 Diagnosis All 1363Harris (1987), (Albuquerque),a New Mexico,
USA35.05N 106.39W 1973–1980 Diagnosis 0–19 73
Gao (2005), (Albuquerque), New Mexico, USA 35.05N 106.39W 1973–1999 Diagnosis All 587Hayes (1961), Winston-Salem, North Carolina,
USA36.06N 80.15W 1943–1958 Diagnosis 0–78 86
Gao (2005), San Jose-Monterey, USA 36.78N 121.54W 1992–1999 Diagnosis All 320Harris (1987), San Francisco-Oakland,
California, USA37.47N 122.25W 1973–1980 Diagnosis 0–19 184
Gao (2005), San Francisco-Oakland, California,USA
37.47N 122.25W 1973–1999 Diagnosis All 1236
Fraumeni (1963), (Washington, DC), USA 38.54N 77.02W 1958–1961 Onset 0–15 237Walker (1982), (Washington, DC), USA 38.54N 77.02W 1969–1977 Diagnosis All 1783Ross (1999), (Washington, DC), USA 38.54N 77.02W 1989–1991 Diagnosis 0–19 5532Harris (1987), (Salt Lake City), Utah, USA 40.46N 111.53W 1973–1980 Diagnosis 0–19 114Gao (2005), (Salt Lake City), Utah, USA 40.46N 111.53W 1973–1999 Diagnosis All 693Harris (1987), (Lincoln), Nebraska, USA 40.48N 96.40W 1973–1980 Diagnosis 0–19 89Harris (1984), (Lincoln), Eastern Nebraska,
USA40.48N 96.40W 1971–1980 Onset 0–14 101
Harris (1987), (Iowa city), Iowa, USA 41.40N 91.32W 1973–1980 Diagnosis 0–19 211Gao (2005), (Iowa city), Iowa, USA 41.40N 91.32W 1973–1999 Diagnosis All 1082Harris (1987), (Hartford), Connecticut, USA 41.46N 72.41W 1973–1980 Diagnosis 0–19 191Gao (2005), (Hartford), Connecticut, USA 41.46N 72.41W 1973–1999 Diagnosis All 1063Meighan (1965), (Portland), Oregon, USA 42.10N 123.39W 1950–1961 Onset 0–14 214Harris (1987), Metropolitan Detroit, Michigan,
USA42.20N 83.03W 1973–1980 Diagnosis 0–19 172
Gao (2005), Metropolitan Detroit, Michigan,USA
42.20N 83.03W 1973–1999 Diagnosis All 1173
Efimov (1989), Alma-ATA, Kazakhstan, Russia 43.15N 76.57E 1983–1986 Arrival 0–70 100Ramenghi (1983), Turin, Italy 45.04N 7.40E 1971–1982 Diagnosis 0.25–14 301Harris (1987), Seattle, Washington State, USA 47.36N 122.20W 1974–1980 Diagnosis 0–19 127Gao (2005), Seattle, Washington State, USA 47.36N 122.20W 1974–1999 Diagnosis All 1063Thorne (1998), (Exeter), England 50.43N 3.31W 1976–1995 Diagnosis 0–14 420Lee (1963), (London/Cardiff), England and
Wales51.30N 1.62W 1946–1960 Onset 0–44 674
Douglas (1999), (London/Cardiff), England andWales
51.30N 1.62W 1984–1993 Diagnosis 0–79 1369
Till (1967), Greater London, England 51.30N 0.10W 1952–1961 Symptom 0–9 372van Steensel-Moll (1983), (The Hague), The
Netherlands52.06N 4.18E 1973–1980 Diagnosis 0–14 233
Badrinath (1997), (Norwich), East Anglia,England
52.23N 0.49E 1971–1994 Diagnosis All 515
Gilman (1998), (Birmingham), West Midlands,England
52.30N 1.50W 1971–1994 Registration All 1340
Mainwaring (1966), Liverpool, England 53.25N 2.55W 1955–1964 Onset 0–14 52Westerbeek (1998), Greater Manchester and
Lancashire, England53.45N 2.30W 1954–1996 Symptom Diagnosis 0–14 1070
Sorensen (2001), (Copenhagen), Denmark 55.40N 12.35E 1950–1994 Diagnosis 0–3 458Engelbreth-Holm (1935), (Copenhagen),
Denmark55.40N 12.35E 1931–1934 Onset 0–14 95
Gao (2005), Skovde, Sweden 58.24N 13.50E 1977–1994 Arrival All 79Timonen (1999), (Oulu), Northern Finland 65.01N 25.28E 1972–1986 Diagnosis ≥16 64
a Locations in parenthesis refer to major or capital cities.

F. Gao et al. / Leukemia Research 31 (2007) 1327–1338 1331
Table 2Published results and angular analysis—first symptom of ALL
Study Age (year) N R κ Date of peak (μ) 95% CI (bootstrap) Mardia (χ2) p-value Peak reported
Karimi (2003),a
Shiraz, Iran0–15 211 0.052 0.104 October 31 June 27 to March 15 1.142 0.565 Oct (p < 0.005)b
Till (1967), England 0–9 372 0.003 0.006 December 10 June 11 to May 25 0.007 0.997 Absent (–)
Westerbeek (1998),England
0–1.4 72 0.102 0.205 July 20 April 10 to November 24 1.491 0.475 –1.5–8 719 0.042 0.084 March 17 December 23 to July 20 2.558 0.278 Absent (p = 0.377)
9–14 264 0.052 0.103 January 23 September 22 to May 24 1.408 0.495 Absent (p = 0.525)
0–14 1055 0.033 0.066 March 09 November 23 to June 05 2.303 0.316 Absent (p = 0.456)a Monthly data are obtained from their text figures.b Indicates those reported by authors, not derived from Mardia.
Table 3Published results and angular analysis—onset of ALL
Study Age (year) N R κ Date of peak (μ) 95% CI (bootstrap) Mardia (χ2) p-value Peak reported
Lanzkowsky (1964),South Africa
0.1–13 27 Winter:June–August (–)a
Fraumeni (1963),USA
0–15 237 Spring:March–May(p = 0.035)
Harris (1984), USA 0–4 61 0.092 0.185 March 12 October 13 to July 20 1.033 0.567 –5–9 26 0.146 0.295 June 22 February 02 to October 31 1.105 0.576 –
10–14 14 0.402 0.877 May 02 March 23 to July 23 4.519 0.104 –
0–14 101 0.116 0.234 April 25 January 18 to July 08 2.739 0.254 Spring:March–April andSummer–Autumn:August–September(p < 0.05)
Meighan (1965), USA 0–14 214 0.060 0.120 June 29 April 04 to October 18 1.543 0.462 Absent (–)
Lee (1963), Englandand Wales
0–19 506 0.101 0.203 July 20 June 12 to August 24 10.331 0.006 Summer (–)20–44 168 0.054 0.109 July 12 February 21 to December 03 0.987 0.611 Summer (–)
0–44 674 0.089 0.179 July 19 June 11 to August 26 10.740 0.005 –
Mainwaring (1966),England
0–4 24 Summer:May–October(p > 0.05)
5–14 28 Absent (–)
cifU
TP
S
E
G
Engelbreth-Holm(1935), Denmark
0–14 95
a Indicates those reported by Authors, not derived from Mardia.
ompared to winter (November–April) in children (0–14)n East Anglia, England [2]. In contrast a summer peakor children (0–19) was reported from Washington, DC,SA [13] while up to 3 peaks within the year had pre-
vU
y
able 4ublished results and angular analysis—arrive to hospital
tudy Age (year) N R κ Date of peak (μ)
fimov (1989),Russiaa
0–70 100 0.092 0.185 March 04
ao (2005),Sweden
0–19 63 0.229 0.458 January 14≥20 16 0.303 0.606 November 29
All 79 0.229 0.458 January 03a Monthly data are obtained from their text figures.b Indicates those reported by Authors, not derived from Mardia.
–
iously been identified in each of 9 other locations in theSA [29].No strong evidence of a (single) peak was indicated in the
oung (0–19 years) and adults (≥20) in Singapore (individ-
95% CI (bootstrap) Mardia (χ2) p-value Peak reported
October 03 to June 30 1.692 0.429 Absent (–)b
December 08 to March 27 6.278 0.043 JanuarySeptember 07 to February 12 2.692 0.260 Absent
November 17 to February 10 7.875 0.020 January

1332F.G
aoetal./L
eukemia
Research
31(2007)
1327–1338Table 5Published results and angular analysis—diagnosis of ALL
Study Age (year) N R κ Date of peak (μ) 95% CI (bootstrap) Mardia (χ2) p-value Peak reported
Gao (2005), Singapore 0–19 684 0.056 0.111 July 24 May 30 to October 20 4.188 0.123 Absent≥20 253 0.055 0.109 November 04 July 15 to March 17 1.506 0.471 Absent
All 939 0.040 0.080 August 14 May 01 to October 29 2.993 0.224 Absent
Gao (2005), Hawaii, USA 0–19 263 0.074 0.147 April 29 February 08 to July 28 2.836 0.242 Absent≥20 130 0.070 0.140 February 02 September 17 to June 16 1.270 0.530 Absent
All 393 0.056 0.112 April 05 December 21 to July 20 2.457 0.293 Absent
Karimi (2003), Shiraz, Irana 0–15 211 November (p < 0.05)b
Harris (1987), Atlanta, USA 0–19 60 0.121 0.244 December 02 August 08 to April 23 1.760 0.415 February, June,October (p < 0.01)
Gao (2005), Atlanta, USA 0–19 358 0.045 0.091 January 10 October 12 to May 24 1.492 0.474 Absent≥20 212 0.108 0.216 July 05 April 23 to September 04 4.898 0.086 Absent
All 570 0.012 0.024 June 21 November 07 to October 03 0.158 0.924 Absent
Los Angeles, USA 0–19 907 0.050 0.100 May 14 March 09 to July 24 4.494 0.106 Absent≥20 456 0.025 0.049 February 17 September 11 to July 13 0.548 0.760 Absent
All 1363 0.035 0.070 April 30 January 21 to July 17 3.298 0.192 Absent
Harris (1987), New Mexico, USA 0–19 73 0.109 0.220 May 14 February 02 to September 09 1.743 0.418 February, June,October (p < 0.01)
Gao (2005), New Mexico, USA 0–19 376 0.066 0.132 June 14 March 25 to August 22 3.260 0.196 Absent≥20 211 0.025 0.050 August 20 March 05 to February 04 0.263 0.877 Absent
All 587 0.046 0.093 June 24 January 30 to August 30 2.546 0.280 Absent
Hayes (1961), USA 0–78 86 0.211 0.431 March 28 February 15 to May 08 7.623 0.022 Absent (p < 0.5)
Gao (2005), San Jose-Monterey, USA 0–19 226 0.039 0.079 January 23 September 08 to May 15 0.697 0.706 Absent≥20 94 0.096 0.192 July 30 April 13 to December 18 1.715 0.424 Absent
All 320 0.002 0.004 October 23 July 12 to June 10 0.003 0.999 Absent
Harris (1987), Oakland, USA 0–19 184 0.027 0.055 August 04 February 18 to January 07 0.277 0.871 February, June,October (p < 0.01)
Gao (2005), Oakland, USA 0–19 761 0.046 0.093 August 03 May 18 to October 28 3.269 0.195 Absent≥20 475 0.014 0.027 September 27 April 20 to February 27 0.169 0.919 Absent
All 1236 0.032 0.064 August 10 May 29 to November 16 2.493 0.288 Absent
Walker (1982), USA 0–2 243 0.064 0.128 December 29 September 25 to April 02 1.988 0.370 Absent (–)3–9 607 0.063 0.127 April 18 January 22 to June 12 4.891 0.087 Absent (–)10–19 346 0.014 0.028 March 30 October 16 to September 09 0.133 0.936 Absent (–)0–19 1196 0.035 0.069 March 26 December 20 to June 16 2.859 0.239 Absent (–)20–49 207 0.060 0.120 September 20 May 22 to January 17 1.481 0.477 Absent (–)50–69 172 0.174 0.354 October 03 August 30 to November 12 10.442 0.005 Absent (–)≥70 208 0.093 0.186 March 31 January 21 to June 08 3.579 0.167 Absent (–)≥20 587 0.039 0.078 September 30 May 21 to January 14 1.770 0.413 Absent (–)
All 1783 0.011 0.021 March 19 October 12 to August 23 0.397 0.820 Absent (–)

F.Gao
etal./Leukem
iaR
esearch31
(2007)1327–1338
1333
Ross (1999), USA 0–19 5532 0.029 0.058 July 09 May 24 to August 12 9.397 0.009 Summer (p = 0.01)
Harris (1987), Utah, USA 0–19 114 0.063 0.126 August 10 April 12 to December 29 0.897 0.639 February, June,October (p < 0.01)
Gao (2005), Utah, USA 0–19 499 0.035 0.070 March 29 November 21 to August 08 1.212 0.546 Absent≥20 194 0.059 0.117 November 17 June 11 to February 13 1.319 0.517 Absent
All 693 0.019 0.039 February 15 September 03 to July 13 0.517 0.772 Absent
Harris (1987), Nebraska, USA 0–19 89 0.119 0.240 April 26 December 17 to August 22 2.528 0.283 April, August,December (p < 0.05)
Iowa, USA 0–19 211 0.034 0.068 March 04 September 28 to August 23 0.483 0.786 April, August,December (p < 0.05)
Gao (2005), Iowa, USA 0–19 674 0.037 0.074 February 12 October 01 to May 28 1.861 0.394 Absent≥20 408 0.011 0.022 August 04 March 19 to February 07 0.096 0.953 Absent
All 1082 0.019 0.038 February 14 August 23 to July 07 0.788 0.674 Absent
Harris (1987), Connecticut, USA 0–19 191 0.078 0.157 February 02 November 01 to June 26 2.334 0.311 April, August,December (p < 0.05)
Gao (2005), Connecticut, USA 0–19 653 0.024 0.048 February 12 September 14 to July 20 0.766 0.682 Absent≥20 410 0.005 0.010 June 07 November 04 to October 05 0.021 0.989 Absent
All 1063 0.014 0.028 February 20 September 27 to July 31 0.429 0.807 Absent
Harris (1987), Detroit, USA 0–19 172 0.100 0.201 February 16 December 02 to April 25 3.439 0.179 April, August,December (p < 0.05)
Gao (2005), Detroit, USA 0–19 768 0.045 0.089 January 26 October 28 to April 20 3.045 0.218 Absent≥20 405 0.031 0.062 October 05 May 20 to February 21 0.772 0.680 Absent
All 1173 0.027 0.054 January 05 August 16 to May 03 1.719 0.423 Absent
Ramenghi (1983), Turin, Italy 0.25–4 166 0.044 0.088 August 28 April 08 to January 24 0.641 0.726 Absent (–)5–9 91 0.068 0.136 October 27 June 09 to March 25 0.840 0.657 Absent (–)10–14 44 0.249 0.513 January 13 November 13 to March 15 5.438 0.066 Absent (–)0.25–14 301 0.043 0.087 November 16 June 25 to March 20 1.139 0.566 Absent (–)
Harris (1987), Seattle, USA 0–19 127 0.087 0.174 February 17 October 23 to May 14 1.909 0.385 April, August,December (p < 0.05)
Gao (2005), Seattle, USA 0–19 696 0.033 0.066 September 18 June 01 to January 22 1.523 0.467 Absent≥20 367 0.066 0.131 May 23 March 16 to October 09 3.146 0.208 Absent
All 1063 0.024 0.047 July 19 March 08 to December 07 1.164 0.559 Absent
Thorne (1998), South-West, England 0–14 420 Absent (–)
Douglas (1999), England and Wales 0–14 789 0.019 0.038 May 28 December 23 to November 16 0.555 0.758 Absent (p = 0.529)15–79 580 0.029 0.058 February 01 August 25 to June 03 0.968 0.616 Absent (p = 0.521)0–79 1369 0.013 0.025 March 25 October 25 to August 25 0.430 0.806 Absent (p = 0.630)
Von Steensel-Moll (1983), The Netherlands 0–14 233 0.038 0.076 January 10 August 22 to May 15 0.672 0.715 Absent (–)

1334 F. Gao et al. / Leukemia Research 31 (2007) 1327–1338Ta
ble
5(C
onti
nued
)
Stud
yA
ge(y
ear)
NR
κD
ate
ofpe
ak(μ
)95
%C
I(b
oots
trap
)M
ardi
a(χ
2)
p-va
lue
Peak
repo
rted
Bad
rina
th(1
997)
,Eas
tAng
lia,E
ngla
nd0–
1427
10.
118
0.23
7Ju
ly13
May
24to
Sept
embe
r03
7.50
00.
024
Sum
mer
:M
ay–O
ctob
er(p
≤0.
01)
≥15
244
0.09
40.
189
Aug
ust1
4M
ay12
toN
ovem
ber
134.
306
0.11
6Su
mm
er:
May
–Oct
ober
(p≤
0.01
)
All
515
0.10
30.
206
July
26Ju
ne23
toA
ugus
t30
0.83
50.
004
Sum
mer
:M
ay–O
ctob
er(p
<0.
001)
Wes
terb
eek
(199
8),a
Eng
land
0–1.
474
0.17
90.
363
Aug
ust2
7Ju
ne20
toN
ovem
ber
044.
728
0.09
4–
1.5–
873
00.
056
0.11
1Ju
ne22
Apr
il03
toSe
ptem
ber
044.
520
0.10
4A
bsen
t(p
=0.
072)
9–14
266
0.01
40.
029
Febr
uary
26Se
ptem
ber
18to
Aug
ust2
10.
109
0.94
7A
bsen
t(p
=0.
980)
0–14
1070
0.04
20.
085
July
03A
pril
11to
Sept
embe
r11
3.84
90.
146
Abs
ent(
p=
0.09
5)
Sore
nsen
(200
1),D
enm
ark
0–3
458
Oct
ober
(–)
Tim
onen
(199
9),N
orth
ern
Finl
and
≥16
640.
259
0.53
7Ja
nuar
y29
Dec
embe
r23
toM
arch
148.
611
0.01
4O
ctob
er–D
ecem
ber,
Janu
ary–
Mar
ch(p
=0.
006)
aN
ote
data
for
‘sym
ptom
’gi
ven
inTa
ble
3.b
Indi
cate
sth
ose
repo
rted
byA
utho
rs,n
otde
rive
dfr
omM
ardi
a.
FcU
un1fWiwipeSM
3
ac
3
egcRwM
FtYntm0t
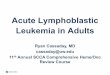
ig. 1. Repeated histogram (from July, full year, to end June) of monthlyounts of diagnosis of ALL with the von Mises fit in those 0–19 years inSA (1989–1991) (data from Ross et al. [13]).
al data) and each of 11 locations in the USA [27]. Similarlyo differential patterns in 6 age-specific groups (0–2, 3–9,0–19, 20–49, 50–69 and >70) from the USA have beenound [22], none were indicated in those aged 0–78 years in
inston-Salem, North Carolina, USA [30], 0–14 and 15–79n England and Wales [6]. For adults, the peak in summeras also indicated in East Anglia [2]. However a strong peak
n October–December and a less pronounced second wintereak in January–March for adults (>16) was noted in North-rn Finland [31]. Absence was also noted in Turin, Italy [32],outh-West, England [19], The Netherlands [14] and Greateranchester and Lancashire, England [23].
.2.5. RegistrationOnly one study examined registration (Table 6) and noted
summer excess in the West Midlands, England [8] in bothhildren and adults.
.3. Angular reanalysis
Our reanalyses, using the standardised methodology ofstimating the parameters of the von Mises distribution, areiven in Tables 2–6. As one might expect, some of theseonfirmed those of the original investigators. For example,oss et al. [13] reported a summer peak (p = 0.01) in diagnosishich we confirm with an estimated peak of July 9 (95% CIay 24 to August 12, p = 0.009) (Fig. 1, Table 5).However, many inconsistent findings were also found.
or example, applying the Mardia test to the appearance ofhe first symptom in children (0–15 years) of Karimi andarmohammadi [21] gives p = 0.565 (non-statistically sig-ificant) in contrast to the original report using Chi-square
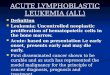
est (p < 0.005) (statistically significant). The significant sum-er onset reported by Lee [7] is confirmed for those aged–19 (July 20, R = 0.102, p = 0.006) but is not confirmed forhose 20–44 (July 12, R = 0.054, p = 0.611). However, Fig. 2

F. Gao et al. / Leukemia Research 31 (2007) 1327–1338 1335
Table 6Published results and angular analysis—registration
Study Age (year) N R κ Date of peak (μ) 95% CI (bootstrap) Mardia (χ2) p-value Peak reported
Gilman (1998),England
0–14 805 0.050 0.100 September 09 July 11 to November 23 4.047 0.132 Summer: May–October (–)a
≥15 535 0.092 0.185 July 07 May 28 to August 10 9.099 0.011 Summer: May–October (–)
June
ir[a2wga(
bcpA
Fci
tsi
3
children and/or adolescents (most often classified as 0–19).Amongst these there is little evidence of a strong seasonalcomponent to ALL whatever the start chosen (R ranging
All 1340 0.057 0.114 August 04a Indicates those reported by Authors, not derived from Mardia.
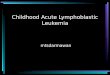
llustrates similar patterns in these two age groups and theelative paucity of data for the adults. Conversely, Hayes30] reported absence of seasonal variation using χ2 (quotedmbiguously as p < 0.5) while Mardia gives p = 0.022 (March8, R = 0.211) (Fig. 3a, Table 5). Walker and van Noord [22]ere not able to identify a significant peak in any age-specificroups in the USA, while the angular methodology identifiespeak in those aged 50–69 (October 3, R = 0.174, p = 0.005)
Fig. 3b, Table 5).The angular analysis suggested that some claims for a
imodal form for the number of cases, and hence 2 peaks,ould not be substantiated. Thus Fig. 4 shows that the singleeak von Mises distribution describes the data of Harris andl-Rashid [25], and Timonen [31] reasonably well, indicates
ig. 2. Repeated histogram (from July, full year, to end June) of monthlyounts of onset of ALL with the von Mises fit in those 0–19 and 20–44 yearsn England and Wales (1946–1960) (data from Lee [7]).
f
Fmi[N
16 to September 17 8.722 0.013 –
he paucity of data supporting both claims for bimodality anduggests that the second is based on a shortfall of diagnosesn December alone.
.4. Influence of age and latitude
We identified 21 studies that reported specifically on
rom 0.003 to 0.229, median 0.048 with p-values ranging
ig. 3. Repeated histogram (from July, then full year, then end in June) ofonthly counts of diagnosis of ALL with a von Mises fit. (a) Aged 0–78 years
n Winston-Salem, North Carolina, USA (1943–1958) (data from Hayes30]). (b) Aged 50–69 in USA (1969–1977) (data from Walker and vanoord [22]).

1336 F. Gao et al. / Leukemia Researc
Fig. 4. Repeated histogram (from July, then full year, then end in June) ofmonthly counts of ALL with a von Mises fit. (a) Aged 0–14 years in East-e(T
fN1ea[cia
tp0eeaay3
bJObeo
3
oacpa920
4
yoertqHtuuvofmrc
soaoawfipRab
rn Nebraska, USA (1971–1980) (onset from Harris and Al-Rashid [25]).b) Aged ≥16 years in the Northern Finland (1972–1986) (diagnosis fromimonen [31]).
rom 0.006, 0.007, 0.009, 0.043, 0.087 through to 0.997).evertheless the magnitude of R over the ages 0–4, 5–9 and0–14 of 0.092, 0.146 and 0.402 (Table 3) increases in East-rn Nebraska, USA [25] as it does for those aged 0.25–4, 5–9nd 10–14 (R = 0.044, 0.068, 0.249) (Table 5) in Turin, Italy32] but patient numbers are small with only 101 and 301ases, respectively. Neither is this trend observed in the stud-es from Washington, DC, USA [22] and Greater Manchesternd Lancashire, England [23].
For adults too, essentially speaking those 20 years or more,he reanalysis confirms some of the published findings. Inarticular we confirm the suggestion of a summer peak (July7, p = 0.011) in those aged 15 or more indicated by Gilmant al. [8] from the West Midlands, England (Table 6). How-ver there are a few exceptions, thus although Hayes [30]
nd Walker and van Noord [22], for a subgroup aged 0–78nd those 50–69 years, reported an absence of peak our anal-sis identified peaks at March 28 (p = 0.022) and October(p = 0.005), respectively. Further Timonen [31] suggests am
gw
h 31 (2007) 1327–1338
imodal distribution with peaks in October–December andanuary–March while we identified January 29 (p = 0.014).ne possible explanation for the differences in peaks coulde that the studies were conducted at different latitudes. How-ver, no clear association between day of peak and latitude isbserved.
.5. Estimating lag
Only two studies provide direct information on the effectf different start times by reporting on month of first symptomnd date of diagnosis for the same cases and both refer tohildren. The estimated lag in those aged 1.5–8 is from aeak of symptoms at March 17 (Table 2) to peak diagnosist June 22 (Table 5), a lag of 3 months [23]. For those aged–14, the corresponding peaks are January 23 and February6 or a lag of 1 month. A 1 month lag was reported in children–15 although an angular analysis was not possible [21].
. Discussion
The total of 24 articles, published over a period of 70ears, involving more than 27,000 cases from 11 countriesver a range of latitudes from 35.05◦S to 65.01◦N, that havexamined the seasonality in presentation of cases with ALLepresents a great deal of resource focussed on a single ques-ion. We were motivated in conducting this review by thisuestion and presumed it had been answered in the literature.owever a preliminary review revealed that the situation in
his respect was not at all clear. In particular, investigators hadsed a variety of ‘start’ dates, dealt only with cumulated data,sed a plethora of methods for analysis and often failed to beery precise as to when (in the calendar year) any peak(s) hadccurred. It also became clear that most, if not all of the dataor these studies had been collected for other purposes, pri-arily for cancer registration with the month of start recorded
ather than the actual date, from which only basic tabulationsould be obtained rather than patient specific detail.
Among the identified studies (Table 1), most report sea-onal variation of ALL either in the USA or UK. As in manyther epidemiologic investigations, the case group is oftenselected series derived from admission or clinical visits tone or more hospitals or death certificate series, rather thanpopulation-based identification of all incidence cases. Itould appear that no study data, had been primarily collected
or the specific purpose of investigating seasonality and so its not so surprising that it may be sub optimal for this pur-ose. For example, the Surveillance, Epidemiology, and Endesults database used by Walker and van Noord [22], Harrisnd Al-Rashid [25], Harris et al. [29] and Gao et al. [27] haveeen established to enumerate cases as only the year and the
onth of the diagnosis are reported and not the actual day.Some earlier work [33] on seasonality of suicides sug-ested that an angular methodology assuming a single peakithin a calendar year and having a von Mises distribution

Researc
fGIbauar
s‘rtfca
amdrebbmocomisa
pE[E[mgAsmtpd
oHnhamtcs
top
A
tEUG
R
[
[
[
[
[
[
[
[
[
[
[
F. Gao et al. / Leukemia
orm may provide a suitable (statistical) methodology, seeao et al. [11], which could be applied across all studies.
f appropriate, the common methodology would facilitateetween study comparisons. The evidence we have from thengular reanalysis of the ALL studies is that for most pop-lations investigated the distribution describes the data welllbeit in the majority of cases the evidence for any peak isather weak.
The discrepancies between the evidence of possible sea-onal variation provided by the angular analysis and theoriginal’ analysis, suggests that the conclusions drawn withespect to seasonality, or the lack thereof, may depend onhe particular analytical method adopted. Some of these dif-erences are substantial whilst others are small and may nothange the interpretation a great deal. A common analyticalpproach is clearly desirable.
Despite a now common methodology with the addeddvantages of providing confidence intervals around the esti-ated peak dates and their strength via R, there remained
ifficulties of interpretation across all studies both withespect to time lags between start dates of ALL and any influ-nce of patient age. We were only able to quantify the lagetween date of first symptom and diagnosis in children, asetween 1 and 3 months. The former date would seem theore appropriate for seasonality studies but it was the date
f diagnosis, which is likely to be determined by local healthare circumstances and accounting (perhaps) for the paucityf data in December in the study of Timonen [31], that wasost often used. Indeed Westerbeek et al. [23] found signif-
cant seasonal variation for Hodgkin’s disease only in firstymptom and not in diagnosis (see also Higgins et al. [34]nd Gao et al. [35]).
Evidence for statistically significant seasonality, using a< 0.05 for this, was found in (sub) populations includingngland and Wales (0–19 years) [7], Western Sweden (0–19)
27], USA (0–78) [30], USA (50–69) [22], USA (0–19) [13],ast Anglia, England (0–14) [2], Northern Finland (≥16)
31] and West Midlands, England (≥15) [8], although withultiple testing some of these may be spurious findings. In
eneral terms no consistent evidence for the seasonality ofLL whether in adults or children has established. Were sea-
onality present, and arising from a climatic determinant, oneight anticipate an increasing R as the associated latitude of
he study population moved away from the equator. No suchattern was apparent nor was there a consistent shift in peakates with latitude.
So despite extensive study, neither presence nor absencef a seasonal component to ALL has been firmly established.owever, it seems likely that if there is a seasonal compo-ent, then it is not strong and (were it present) unlikely toave major aetiological importance. It is recognised that non-etiological factors, such as differing health care systems,
ay disguise the true patterns of onset of any disease andhese will have played some role in the presentation of ALLases. If these issues are to be resolved then a prospectivetudy using individual patient information, common diagnos-
[
h 31 (2007) 1327–1338 1337
ic criteria and an onset of symptoms ‘start’ date, conductedver wide a range of geographical areas and the same calendareriod is required.
cknowledgments
We would like to thank following people for help inranslating non-English articles. Ingela Krantz (German),leonora Belfiore (Italian), Edyta Bajak (Polish, Serbian,krainian), Sue Ablett and Faina Vikhanskaia (Russian),ilda Piaggio (Spanish).
eferences
[1] Linet MS. The leukemias: epidemiologic aspects. New York: OxfordUniversity Press; 1985. p. 185–222.
[2] Badrinath P, Day NE, Stockton D. Seasonality in the diagnosis of acutelymphocytic leukemia. Br J Cancer 1997;75:1711–3.
[3] Douglas S, Cortina-Borja M, Cartwright R. Seasonal variation in theincidence of Hodgkin’s disease. Br J Haematol 1998;103:653–62.
[4] Lambin P, Gerard MJ. Variations de frequence saisonnieres de laleucemie aigue. Sang 1934;8:730–2.
[5] Allan TM. Seasonal onset of acute leukaemia. Br Med J 1964;2:630.[6] Douglas S, Cortina-Borja M, Cartwright R. A quest for seasonality in
presentation of leukemia and non-Hodgkin’s lymphoma. Leuk Lym-phoma 1999;32:523–32.
[7] Lee JAH. Seasonal variation in leukemia incidence (letter to the editor).Br Med J 1963;2:623.
[8] Gilman EA, Sorahan T, Lancashire RJ, Lawrence GM, Cheng KK. Sea-sonality in the presentation of acute lymphooid leukemia. Br J Cancer1998;77:677–8.
[9] World Health Organization. International classification of diseases. 9thRevision. Geneva: World Health Organization; 1977.
10] Allan TM, Douglas AS. Seasonal variation in health and diseases. Abibliography. London and New York: Mansell; 1994. p. 230–4.
11] Gao F, Chia KS, Krantz I, Nordin P, Machin D. On the application of thevon Mises distribution and angular regression methods to investigatethe seasonality of disease onset. Stat Med 2006;25:1593–618.
12] Knox G. Epidemiology of childhood leukemia in Northumberland andDurham. Br J Prev Soc Med 1964;18:17–24.
13] Ross JA, Severson RK, Swensen AR, Pollock BH, Gurney JG, RobisonLL. Seasonal variations in the diagnosis of childhood cancer in theUnited States. Br J Cancer 1999;81:549–53.
14] van Steensel-Moll HA, Valkenburg HA, Vandenbroucke JP, van ZanenGE. Time space distribution of childhood leukemia in the Netherlands.J Epidemiol Commun Health 1983;37:145–8.
15] Fraumeni JF. Seasonal variation in leukemia incidence (letter to theeditor). Br Med J 1963;2:1408–9.
16] Lanzkowsky P. Variation in leukemia incidence (letter to the editor). BrMed J 1964;1:910.
17] Mainwaring D. Epidemiology of acute leukemia of childhood in theLiverpool area. Br J Prev Soc Med 1966;20:189–94.
18] Engelbreth-Holm J. An die jahrezeit gebundene schwankungen imvorkommen akuter leukose. Klin Wsher 1935;14:1677–9.
19] Thorne R, Hunt LP, Mott MG. Seasonality in the diagnosis of childhoodacute lymphoblastic leukemia. Br J Cancer 1998;77:678.
20] Sorensen HT, Pedersen L, Olsen J, Rothman K. Seasonal variation in
month of birth and diagnosis of early childhood acute lymphoblasticleukemia. JAMA 2001;285:168–9.21] Karimi M, Yarmohammadi H. Seasonal variations in the onset of child-hood leukemia/lymphoma: April 1996 to March 2000, Shiraz, Iran.Hematol Oncol 2003;21:51–5.

1 Researc
[
[
[
[
[
[
[
[
[
[
[
[
338 F. Gao et al. / Leukemia
22] Walker AM, van Noord PA. No seasonality in the diagnosis of acuteleukemia in the United States. J Natl Cancer Inst 1982;69:1283–7.
23] Westerbeek RM, Blair V, Eden OB, Kelsey AM, Stevens RF, WillAM, et al. Seasonal variations in the onset of childhood leukemia andlymphoma. Br J Cancer 1998;78:119–24.
24] Till MM, Hardisty RM, Pike MC, Doll R. Childhood leukemia ingreater London: a search for evidence of clustering. Br Med J 1967;3:755–8.
25] Harris RE, Al-Rashid RA. Seasonal variation in the incidence ofchildhood acute lymphocytic leukemia in Nebraska. Nebr Med J1984;69:192–8.
26] Meighan SP, Knox G. Leukemia in children: epidemiology in Oregon.Cancer 1965;18:811–4.
27] Gao F, Nordin P, Krantz I, Chia K-S, Machin D. Variation in the seasonal
diagnosis of acute lymphoblastic leukemia: evidence from Singapore,USA and Sweden. Am J Epidemiol 2005;162:753–63.28] Efimov ML, Vasil’eva GS, Kovalenko VR, Pozdniakova AP, GriskinG. Seasonal variations of first clinical manifestations of acute leukemiain humans. Gematol Transfuziol 1989;34:61–4.
[
[
h 31 (2007) 1327–1338
29] Harris RE, Harrell Jr FE, Patil KD, Al-Rashid RA. The seasonal riskof pediatric/juvenile acute lymphocytic leukemia in the United States.J Chronic Dis 1987;40:915–23.
30] Hayes DM. The seasonal incidence of acute leukemia. Cancer1961;14:1301–5.
31] Timonen TT. A hypothesis concerning deficiency of sunlight, coldtemperature, and influenza epidemics associated with the onset ofacute lymphoblastic leukemia in northern Finland. Ann Hematol1999;78:408–14.
32] Ramenghi U, Miniero R, Pastore G, Saracco P, Madon E. Variazioni sta-gionali nell’insorgenza delle leucemie acute nel bambino. Min Pediatr1983;35:1001–4.
33] Parker G, Gao F, Machin D. Seasonality of suicide in Singapore: datafrom the equator. Psychol Med 2001;31:549–53.
34] Higgins CD, dos-Santos-Silva I, Stiller CA, Swerdlow AJ. Season ofbirth and diagnosis of children with leukemia: an analysis of over 15000UK cases occurring from 1953–95. Br J Cancer 2001;84:406–12.
35] Gao F, Machin D, Khoo KS, Ng EH. Seasonal variation in breast cancerdiagnosis in Singapore. Br J Cancer 2001;84:1185–7.