Embed Size (px)
Citation preview

LONG TERM CARE
TODAYF A L L / W I N T E R 2 0 1 4 V O L U M E 2 5 , I S S U E 3 $ 4 . 9 5
P U B L I S H E D B Y T H E O N T A R I O L O N G T E R M C A R E A S S O C I A T I O N
Celebrating excellent care: Quality Awards 2014

FALL/WINTER 20142 LONG TERM CARE TODAY

3LONG TERM CARE TODAYFALL/WINTER 2014
LONG TERM CARE
TODAYV O L U M E 2 5 I S S U E 3 F A L L / W I N T E R 2 0 1 4
Long Term Care Today is published by:
Ontario Long Term CareAssociation for the CanadianLong Term Care Community
EDITORIALJudy Irwin
Senior Manager, Communications905-470-8995, ext. 33
ADVERTISING SALESMichelle Gradini
Tel: 905-470-8995, ext. 39Fax: 905-470-9595
Administration & Publishing Offices:Ontario Long Term Care Association,
345 Renfrew Dr.,Markham, ON L3R 9S9Tel: (905) 470–8995Fax: (905) 470–9595
Visit www.oltca.com to stayinformed with all the latest articles,
LTC facilities, research, seminars,careers and much more.
FEATURES8 Celebrating excellent care: OLTCA’s Quality Awards 2014
15 The quality award teams
16 Enhancing residents’ quality of life through careand constructionBy Janice Keefe, PhD, E. Kevin Kelloway, PhD, and Ann McInnis, RN, MSN
20 Removing level of careforms in long-term carehomes and addressing thepalliative care gapBy Dr. Jill Oliver and Dr. Paula Chidwick
24 Creating priceless memories for residents By Sadie Friesner
26 The “Granny Cam”: thegood, the bad, and the lawBy Erin Kuzz and Gerald Griffiths
30 New order sets in long-term care support complex careBy Dr. Amir Ginzburg, Dr. Stuart Egier,and Lori Brown
DEPARTMENTS6 FrontlinesGreat news for Ontario's seniors: Close to 300 long-term care homes will be renovated or rebuiltBy Candace Chartier
8
24
26
15

FALL/WINTER 20144 LONG TERM CARE TODAY
LONG TERM CARE
TODAYLONG TERM CARE TODAY
is published quarterly by theOntario Long Term Care Association.
All editorial material published inLong Term Care Today represents
the opinions of the authors and not necessarily those of the Ontario
Long Term Care Association.
Discussions, views and recommendationsas to medical procedures, choice of
treatments, dosage or other medicallyspecific matters are the responsibility ofthe authors. No responsibility is assumedby the publisher or publishing partnersfor any information, advice, errors or
omission contained herein.
The inclusion of advertising and sponsored material in Long Term CareToday does not constitute a guarantee
or endorsement of any kind by the Ontario Long Term Care Association.
Subscription Rates*:Canada–$15 (1 year), $27 (2 years)
US–$21 (1 year), $33 (2 years)Single copies and back issues–$4.95
Subscription enquiries, back issue requests and changes of address to:
Carmen Williams905-470-8995, ext. 22
© 2014 by the Ontario Long Term CareAssociation. All rights reserved.
Reproduction without credit to thepublication is strictly prohibited.
ISSN 1183-1618
RETURN UNDELIVERABLECANADIAN ADDRESSES TO:
Ontario Long Term Care Association,3rd Floor, 345 Renfrew Dr.,
Markham, ON L3R 9S9
Visit www.oltca.com for more information on LTC facilities, research, seminars, careers and much more.
Call for article submissionsLong Term Care Today magazine is looking forsubmissions from the long-term care communityon innovation and best practices. Published quarterly, our articles are educational and provide evidence- and outcome-based materialsto a broad range of readers within the sector.
If you want more information or are interested insubmitting an article, please contact Judy Irwinat [email protected].
FEATURES34 Highlights of the Qualityand Innovation Forum
38 Professional Directory
38 Long Term Care Today ad index
34
In October, the Ontario Long Term CareAssociation released a new annual statusreport titled This is Long-Term Care 2014.It contains the latest data about long-term care residents in Ontario, and provides the sector's perspective on recent changes and challenges.
The report highlights that due to recentchanges to the admission criteria forlong-term care, residents are now moving to homes at a later stage whentheir physical and cognitive health is
more fragile and their care needs are higher. As one example, a significantly larger percentage of residents need more assistancewith daily activities such as eating and toileting, often becausetheir loss of cognitive function means they no longer know how to do these activities.
The report also explains sensitive issues such antipsychotic use and the increasing spotlight on quality of care. Copies can be downloaded from www.oltca.com.


FALL/WINTER 20146 LONG TERM CARE TODAY
FRONTLINES
Close to 300 long-termcare homes to be renovated or rebuilt
Ontario seniors received great news this fall. As promisedin the 2014 provincial budget, the Ontario government isproceeding with a program to significantly renovate or rebuild approximately 300 homes in the province, equivalentto roughly 30,000 long-term care beds. Redevelopmentwill mean that residents will live in attractive, modernizedhomes that are more appropriate for their needs.
Earlier this year I toured several long-term care homes inOntario and had the opportunity to see the benefits ofsome modernized facilities up close. The dining rooms aresmaller and more intimate, the halls are wider, and thereare more private rooms. Older homes, many with four-bedrooms and cramped living spaces, simply don’t meet theneeds of today’s residents, particularly when more than60 percent of residents have Alzheimer’s or dementia. Private rooms and other home-like amenities help to create a safe and comfortable living environment that respects residents’ privacy and dignity. Individual roomsalso help with infection control.
And these newer homes feel like homes, not facilities.They are very attractive—warm and light-filled, with thekind of paint colours, trim, and decorating touches thatyou might have in your own home. Family members andnew residents are often surprised and pleased by thehome-like environments.
There are several months of planning and schedulingahead, and then homes will begin redevelopment in thefall of 2015.
An increased focus on quality improvement
2015 is a big year for other reasons as well. Starting inApril, homes will begin submitting quality improvementplans to the government, as hospitals have been doing forseveral years. It’s a shift going on across health care—everyone is being asked to track and report data thatshows they are providing high quality care, and the resultsare made available to the public.
When these results are reported in the media, often thespotlight is on areas that need improvement. That’s one of the reasons it’s so important to showcase the many excellent programs that are making a difference.
This issue of Long Term Care Today features the winnersof the Ontario Long Term Care Association’s 2014 Qualityand Innovation Awards. From the development of a newdiabetes care protocol to a home nominated by its residentsfor positive culture change, it’s clear that long-term carehomes are dedicated to improving the lives of their residents in every way they can.
An independent panel of judges for our awards, includingrepresentatives from universities and the Ministry ofHealth and Long-Term Care, told us they were impressedby what they learned was going on in Ontario homes.They’ve urged us to share not only the award-winning entries, but other submissions as well. We’ll be featuringthese stories in upcoming issues of Long Term Care Today—stories about reducing antipsychotic use, preventingfalls, improving wound care, and more.
Historically, long-term care homes have not had much information about what everyone else is doing. Learningabout other homes’ successful programs helps everyoneto think outside the box about what is possible. LTCT
B Y C A N D A C E C H A R T I E R
Candace Chartier is CEO of the Ontario Long Term CareAssociation.


FALL/WINTER 20148 LONG TERM CARE TODAY
Residents are so thrilled with Grey Gables’ culturechange initiative that they nominated the municipalhome in Markdale for the 2014 Culture Change
Home of the Year award. It recognizes efforts to create ahome-like environment, enhancing quality of life and honouring residents’ choice and voice.
Administrator Jennifer Cornell says the nomination andrecognition validate the concerted and dedicated team effort to make Grey Gables a vibrant place to call home.
Culture change is an evolution that requires a vision thateveryone is part of and understands, Cornell says. Theprocess for change began at Grey Gables in 2012, whenthe home engaged a leadership coach and began a visioning process. Focused conversations took place withresidents, staff, families, volunteers, and “anybody whohad an idea they wanted to share,” Cornell says.
The team discovered that Grey County’s newly developedtagline, “Colour It Your Way,” matched closely to the findings from the visioning process. From there, they defined the Grey Gables “Colour It” vision (see below).
“Our values guide us in the way we provide care and service, everything from the bedside care, the food wecook, to the programs we offer—all the things we do,”Cornell says.
The Colour It culture focuses on ongoing relationship-building, celebrating successes, and learning from challenges. The close collaboration and high level of engagement generates widespread support and empowerspeople to act to perpetuate the positive culture.
“We always have this vision that we collaborated on together and can fall back on and say, ‘What’s the impactof this decision we’re making? Is it going to Colour It theway we want?’”
Since 2009, the Ontario Long Term Care Association has recognized excellence in long-term care through itsannual Quality Awards program. Submissions go througha rigorous analysis by an external panel of judges with
expertise in quality from universities, government, andlong-term care homes. Long Term Care Today asked the2014 award winners to identify the factors that helpedmake their programs a success.
Culture Change Home of the Year: Grey Gables, Markdale
A resident participates in the Grey Gables celebration.
Celebrating excellent care: OLTCA’s Quality Awards 2014
ommunitypportunityeadershiprganizational quality and safetyare the centre of all we doelationshipsntegrityomorrow
Each letter in “Colour It” represents a core value
of Grey Gables: COLO
“U”
RIT

9LONG TERM CARE TODAYFALL/WINTER 2014
For example, detailed job routines for care staff have beenreplaced by huddles at the start of every shift so personalsupport workers determine what they’ll do each day tocare for residents.
“This way, they can be more flexible, they can respond toan individual resident's changes or requests, and it honoursstaff’s skills and knowledge because they know what todo,” Cornell says.
It’s a shift to a greater focus on care and service from being task-oriented, which is more meaningful and fulfilling for those giving and receiving care.
Grey Gables also modified its language to be more home-like; residents, for instance, are not admitted to the homebut instead move in. A decorating committee is leadingphysical enhancements such as placing memory framesoutside residents’ rooms for cherished pictures.
The home also created a video about Colour It, which wasinspired by success stories that residents and staff wereasked to share during the change process.
“We started looking at what we knew we were already doing and that helped open the doors to what more waspossible,” Cornell says.
Culture change has generated many benefits, includingmore consistent, transparent, and inclusive communication,and more consistency in care and service delivery guidedby residents’ choices and voices.
“People feel more part of a team. Honouring the staff’sknowledge and skills has had a positive impact, as peoplework together to find solutions,” Cornell says.
Feedback from families has been positive and, in a recentsurvey of residents, 93 percent said they feel the supportthey receive helps them to live their lives the way they want.
Successes from OMNI Health Care’s comprehensivediabetes program helped the Peterborough-basedlong-term care provider earn this year’s Innovation
of the Year award.
OMNI launched its diabetes program in February 2013.The initiative is focused on evidence-based order sets addressing several aspects of diabetes care, includingnursing assessment, dietary and foot care, and sick-daymanagement.
The program has now been established in all 18 OMNIhomes.
A collaborative effort between registered staff membersand community partners, including hospitals, clinicians,and dietitians, made the order set a reality.
Funding for the program was made possible byBoehringer Ingelheim (Canada) Ltd. and Eli Lilly (Canada) Inc., as well as a partnership with Medical Pharmacies and In Initiative.
By having better control of diabetes, residents can avoidhospital visits, which in turn improves quality of life whilehelping reduce the burden on the acute-care system.
The protocols are also designed to save time. For example, a hypoglycemic event can take more than twohours to correct. If a hypoglycemic event happens duringa staff shortage, it compounds the stress level and canprolong treatment. But with the protocols, team memberscan quickly assess the situation and resolve it in a timelymanner.
Innovation of the Year: Comprehensive diabetes program by OMNI Health Care and Boehringer Ingelheim

FALL/WINTER 201410 LONG TERM CARE TODAY
In the case of a hypoglycemic event, this can have tremendous impact on the person. Research indicates elderly people often have heart attacks or strokes withineight weeks of a hypoglycemic event due to its impact on the body.
By responding quickly or even eliminating the risk, there'sa large-scale trickle-down effect, says Shawn Riel, OMNI’schief operating officer.
“The more events that we can eliminate, the better qualityof life residents will have, and the lower health-care costswill be,” she says.
Medications were also assessed to find the pharmaceuticalsthat work best with the over-65 population. Every quarter
a review is conducted to determine the success of interdisciplinary interventions on residents.
OMNI president and CEO Patrick McCarthy emphasizesthe efforts that went into developing this program.
“There were hundreds and hundreds of hours of work,reaching out to engage the physicians locally and to work with registered staff and administration at the homes to make sure that we got it right and to listen toany constructive feedback that we were able to get,” he says.
“We were able to get the documentation of statistics tohelp support the need for change and to really make itwork from that perspective.”
Quality Improvement Workplace of the Year: A culture of safety at Winbourne Park, Ajax
OLTCA’s Quality Awards 2014
also reduces costs associated to people being off workdue to injury, she adds.
The Ajax long-term care home also has several teams thatpromote safety education. These include the safe work-place assessment team (S.W.A.T.), the safe ambulation liftand transfer team, (S.A.L.T.), and the infection-controlteam. Each of these teams played a role in helping thehome earn the award, Rayside says.
Rayside says she and the rest of the Winbourne Park teamwere honoured to receive the accolade.
“It was phenomenal,” she says. “We didn’t expect to receive [the award]. It was certainly rewarding for themanagement team but I think even more rewarding for the frontline staff.”
Winbourne Park in Ajax was commended byjudges in OLTCA’s quality awards program fortheir outstanding commitment to supporting a
culture of safety and quality, involving employees at everylevel, from frontline staff to management.
Since late 2009, Winbourne Park Long Term Care Centrestaff members have had only two injury-related days off.This outstanding result, which stems from several educa-tional interventions, earned the Revera long-term carehome the Quality Improvement Workplace of the Yearaward for 2014.
The award recognizes members that excel in physical, environmental, and occupational health and safety, promotion of health and wellness among staff and volunteers, and the development of a supportive environment and culture of learning.
Winbourne Park executive director Beverley Rayside attributes the success to the home’s educational initiativesand to the fact that staff members provide most of theeducation. Some of the main staff educational areas include safe ambulation lifts and transfers, employee wellness, weight loss, and promotion of flu vaccination.
“We also share information with people at staff meetingsat every opportunity we have,” Rayside says, adding thatsuccessful interventions and educational initiatives areshared corporately and among other long-term carehomes.
Rayside says the low rate of staff injury has had a positiveimpact on staff morale. Should an injury occur, Raysidesays the management team will provide staff with alternatework to ensure they get back to work safely. Aside fromkeeping staff members’ morale high, the low injury rate Winbourne Park's efforts include promoting the flu shot.
Flu
Shot⁄

11LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201412 LONG TERM CARE TODAY
Supporting long-term care residents to maintain theirindependence and mobility through an effectivesustainable falls prevention program earned
Elginwood Long Term Care Centre top honours as theQuality Improvement Team of the Year.
Executive director Dian Cairns says receiving the OLTCAaward has elevated the team’s focus on enhancing thequality of life and care for Elginwood’s 124 residents.
“We were honoured to win this award and that we weresuccessful with this initiative because we had results,”Cairns says.
In fact, Elginwood has reduced the number of falls by 50 percent in the home area where the prevention program was first introduced in March 2012. The monthlyaverage has dropped to about five or six falls from the 14 that had occurred before the initiative began— and it’s remained consistent with the commitment and engagement of staff.
“They are invested in the initiative because they havecome up with the solutions, they’ve been able to see thedata very clearly, and they can see the results,” Cairnssays.
For residents, preventing falls lessens the risk of a majorfracture, which can diminish their quality of life throughthe loss of mobility and independence, Cairns says. Recovery can be difficult, particularly for residents whohave cognitive challenges.
The falls prevention program is part of Health Quality Ontario’s (HQO’s) Residents First project, which involvedElginwood and 55 other Revera long-term care homes.
With the support of an HQO Residents First facilitator, amultidisciplinary team from Elginwood used state-of-the-artquality improvement processes to reduce the number ofresident falls.
Anna Kim, Elginwood’s associate director of care and Residents First facilitator, says comparisons of falls in different home areas at different times revealed when falls were at a higher risk of occurring, so staff developedstrategies to reduce falls during those times.
One of the key strategies was making a personal supportworker (PSW) available 30 minutes earlier in the afternoonto support residents during the shift change of the carestaff.
Other changes included a new toileting plan to ensure thatresidents can access the bathroom; a falling star programwith the star symbol used to identify residents at a highrisk of falls so that staff members can be proactive; andeducation with residents, families, and staff membersaround such things as the use of call bells, high-low beds,and floor mats.
“It’s a holistic view of how we can prevent falls, and welook at every strategy and try to take action,” Cairns says.
An array of quality improvement tools acquired throughResidents First helped team members devise effectivestrategies, collect and review data, and track results, Kimand Cairns say.
“These tools really helped us highlight exactly what washappening, helped us brainstorm strategies and reviewour data and see where we were going,” Kim says.
“It was really good for making a clear goal and what wewere going to do, so it keeps people focused,” Cairns says.
The tools become part of staff members’ repertoire for notonly bringing the falls prevention initiative to Elginwood’sother home areas but also enhancing quality in other areas of care.
Cairns and Kim agree staff engagement was an importantfactor in this quality improvement process and the resultingpositive outcomes. Changes in behaviour are comple-mented by a heightened sense of conscientiousness thatwill serve Elginwood’s quality enhancement efforts in thefuture.
OLTCA’s Quality Awards 2014
Quality Improvement Team of the Year: Falls prevention at Elginwood, Richmond Hill
Catch a fallingstar!
Elginwood uses a falling star symbol to help identify residents at a high risk of falls.

13LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201414 LONG TERM CARE TODAY
members are spending less time answering family members’ questions because they can now easily accessall the information they need, Sullivan says.
Sullivan says the major lesson for PLTC was seeing thebreadth of the positive impact Home We Care has on familymembers and frontline staff. He says family members havebeen constantly signing up for the program.
“Once people get on this, they’ll find it well worth it,” hesays.
Colin LeBrun, Home We Care’s president and CEO, saysthe success PLTC has seen from the app is precisely theoutcome he was hoping for. Long-term care homes, henotes, get a flurry of calls from family members every dayasking for updates on their loved one.
For people using the app, there is a seamless communica-tion line and staff members can spend less time on thephone and more time with residents, he adds.
“It’s a win-win for everybody,” he says. “It’s a win for thehome and it’s a win for the family member who wants toknow what’s going on.”
The Best New LTC Product or Service of the Year isawarded to a new or significantly improved product orservice developed or launched by an OLTCA commercialmember, judged by OLTCA active members as most likelyto have a positive impact on long-term care if more widely adopted. LTCT
Best New Long-Term Care Product Award: Home We Care smartphone app
Asmartphone app developed to provide long-termcare residents’ families with up-to-date informationon their loved ones has earned Home We Care and
Provincial Long Term Care Homes (PLTC) the Best NewLong-Term Care Product or Service of the Year Award.
The app, called Home We Care, was piloted at four ofPLTC’s five long-term care homes where it was met withenthusiasm, says Richard Sullivan, PLTC’s corporate manager of marketing and public relations.
With the application, which is available at app stores andonline, care providers document residents’ care plans andnurses’ notes, which are transmitted to family memberswho may then choose to speak with their loved one or thecare provider. The application, which can be customized,also allows family members to stay apprised of anychanges in the care plan.
Information is transferred in real time, directly from thepoint-of-care system in the homes.
“This has been a tremendous convenience for [families] to see at a glance how their loved one is doing,” Sullivansays, adding the app is an excellent tool for increasingtransparency.
By providing family members with important informationabout their loved ones’ care, the app has also led to increased time spent with residents at the homes where it has been piloted—a success due to the fact that staff
Home We Care app
OLTCA’s Quality Awards 2014

15LONG TERM CARE TODAYFALL/WINTER 2014
The 2014 Quality Awards were presented
during the Ontario Long Term Care
Association’s Quality and Innovation
Forum in June, which showcased best
practices and successful policies,
resources, and tools implemented by
Ontario’s long-term care providers.
Winbourne Park, Ajax
OMNI Health Care
Home We Care and Provincial Long-Term Care (PLTC) LTCTGrey Gables, Markdale
Elginwood, Richmond Hill
The quality award teams

FALL/WINTER 201416 LONG TERM CARE TODAY
In Nova Scotia, the long-term care sector has been undergoing significant changes as part of the ContinuingCare Strategy, with a number of new and replacementnursing homes opening over the last eight years. At thesame time, the province has been changing the staffingmix with an expanded scope of practice for continuing care assistants (similar to personal support workers). A research team looked at how residents, family, andstaff rated quality of life based on different models ofphysical surroundings and staffing.
“If you’ve seen one nursing home, you’ve seen themall.” While this statement may have held true 30years ago, today the long-term care landscape is
far from uniform.
Nova Scotia has approximately 7,000 publicly fundednursing home beds in 89 licensed facilities which are operated by a mix of providers (e.g., for-profit, not-for-profit).The new and replacement nursing homes were built withphysical designs that incorporate several smaller households(pods or units) with 9–16 residents per household.
The households offer private rooms and baths for residents,as well as a kitchen, dining, and living room area.
In addition to the design of these new facilities, thestaffing mix within these new homes was adjusted to support direct care providers (known as continuing careassistants in Nova Scotia) to perform regular tasks such as personal care, but also for household-level tasks such as housekeeping and dietary. In addition to thesesystem-level changes, individual facilities are adoptingphilosophies that emphasize resident-centered care.
These changes have implications for residents, their families, and the staff that work in these homes but theimpact of these changes is not fully understood.
The Care and Construction research team, a partnershipbetween researchers and representatives from the long-term care sector, sought to look deeper into the impact ofdifferent models of care (e.g., physical design, staff scopeof practice) on resident quality of life within Nova Scotianursing homes from three perspectives: residents, familymembers, and staff.
The main question was, “To what extent and in what waysdo differences in the nursing home model of care impactresident quality of life?”
To answer this question, nursing homes representing threemodels of care participated in the study.
1. New full-scope: household design, with continuingcare assistants responsible for all tasks, including dietary and housekeeping;
Enhancing residents’quality of life throughcare and constructionB Y J A N I C E K E E F E , P h D , E . K E V I N K E L L O W A Y , P h D , A N D A N N M C I N N I S , R N , M S N
Janice Keefe, PhD, is Professor of Family Studies & Gerontology and Lena Isabel Jodrey Chair in Gerontology at Mount Saint Vincent University in Halifax. E. Kevin Kelloway, PhD, is the Canada Research Chair in Occupational Health Psychology at Saint Mary’s University in Halifax. Ann McInnis, RN,MSN, was senior leader of a long-term care facility inHalifax at the time of study.

17LONG TERM CARE TODAYFALL/WINTER 2014
2. New-augmented: household design, with continuingcare assistants providing care needs and limited dietary and housekeeping; and
3. Traditional: floor/unit design, with continuing careassistants providing only care needs, while otherstaff provide dietary and housekeeping services.
What were the important findings?
The results showed that, on average, residents, family, andstaff perceived a positive resident quality of life across themodels of care, though there was a range of both positiveand negative responses.
While the average scores of resident quality of life werepositive in all three models, the residents, family, and staffrated resident quality of life more positively in the modelsof care that featured the new physical design and differentstaffing approach (i.e., new full-scope and new-augmented)when compared to traditional homes.
To understand what was contributing to the differences inresident quality of life, a number of factors were examined.The results showed that there was not a direct relationshipbetween resident quality of life and model of care. Instead,model of care had an indirect effect on resident quality oflife through two factors: relationships and home-likeness.This was an important finding, as it suggests that residentquality of life can be enhanced regardless of model ofcare, while at the same time demonstrating that the models with smaller neighbourhoods and different staffingapproaches were uniquely supporting relationships andhome-likeness.
These two factors, along with the factor of working environment, contribute to understanding the impact ofmodel of care on resident quality of life.
Relationships matter
Relationships are important. The importance of relationshipsin supporting resident quality of life stood out in all parti-cipant groups. Not surprisingly, residents with friendshipand companionship in their lives reported higher quality of life. Feeling as though they were contributing was important, as residents who felt that they were able tohelp and advise others had a higher quality of life.
Having access to private and/or community spaces andbeing supported in the development of relationships wasalso linked to positive resident quality of life.
For residents and staff, open and honest communicationbased in mutual respect was related to positive residentquality of life. This included a feeling of “friendship” between residents and the staff providing their care.
The relationships of family members and staff also had animpact on resident quality of life. The presence of clearand open communication channels, and an overall respectand friendliness between family members and staff werefound to be related to positive quality of life of residents.
Fostering a home-like environment
Home-likeness of the nursing home was shown to have apositive impact on resident quality of life. For residents,home-likeness was assessed by the ambiance or warmthof the space; it “felt like home.” For family members and
The methodologyResident quality of life was examined from three different perspectives: resident, family, and staff, inthree models of care. A mix of data collection methodsallowed the team to balance the inclusion of a largenumber of participants while also examining more in-depth contextual factors. This article focuses onthe results of surveys with residents, family, and staff, but the study also included interviews, focusgroups, participant observation, and resident activitymonitoring.
To understand what factors contribute to residentquality of life, each survey contained the interRAISurvey on Nursing Home Quality of Life© (tailored toeach perspective), and some additional questions.The surveys were administered in 2012. Throughanalysis of the responses to the interRAI quality oflife questions, using exploratory and confirmatoryfactor analyses, the team identified four componentsof quality of life that were shared among residents,family, and staff in their assessments of resident quality of life. These four components were Care and Support, Autonomy, Activities, and Food.
To examine the potential predictors of quality of life,a number of variables were considered. These includeddemographic variables (e.g., gender, age), residentcharacteristics (e.g., cognitive and physical health),participant perceptions of the nursing home (e.g., relationships among staff, family, and residents,home-likeness), and facility characteristics (e.g.,model of care, facility size). The specific variables included in the analyses varied across the three perspectives. Multilevel modelling was used to examine the associations between these variablesand resident quality of life.
Who took part?Of the 319 nursing home residents who completedthe survey (administered in person by a research assistant), 78% were female, 39% were aged 85 orolder, 80% had no or mild cognitive impairment, and46% had lived in the nursing home two years orlonger. Of the 397 family members who completedthe survey, 78% were female, 36% were aged 65 orolder, and 64% were the son/daughter of a resident.And of the 862 staff members who completed thesurvey, 91% were female, with an average age of 44,and had worked in the nursing home an average of almost nine years.

FALL/WINTER 201418 LONG TERM CARE TODAY
staff, home-likeness was measured by both the physicaland intangible characteristics of the space (i.e., cleanliness,coziness, attachment to space). From both the family andstaff perspective, positive resident quality of life was related to residents maintaining connection to the community outside the nursing home.
Our workplace, your home
From the staff perspective, there were three elements ofthe work environment that were found to positively influence their perception of resident quality of life.
The first factor was having a clear vision of what was expected of them in their role.
The second was degree of skill use, including learning newskills and using a broad range of existing skills in theirdaily work.
The third factor was working with supervisors whodemonstrate qualities of transformational leadership. Staff with supervisors who used this leadership style feltrecognized as individuals and trusted, experienced encouragement and recognition, and had a sense of cooperation among their team.
How to enhance resident quality of life—inputfrom the sector
The study's results were shared at a day-long workshopwith almost 70 representatives from the long-term caresector. Participants were encouraged to actively participatein discerning the implications of the results and in identifying possible ways in which the results could be applied at the practice and policy levels. Specifically, participants were asked to consider ideas for action relative to the study's three key results—relationships,home-likeness, and working environment.
Ideas to enhance resident quality of life
When seeking to foster positive relationships, nursinghome staff and management play a sizable role in enhancing resident quality of life.
Success begins with hiring practices that take into consideration an individual's suitability with the home'sculture and philosophy of care. Staff could also benefitfrom modelling and coaching to help improve their skillbase and instill cooperation and teamwork as a value ofthe organization. The offer of continued education/trainingopportunities for staff shows an investment in their potential as individuals, and helps to broaden the skillbase of staff.
Staff play a critical role in encouraging resident-to-residentrelationships, by identifying meaningful commonalitiesand interests among residents and ensuring that opportu-nities exist for residents to foster those connections. Getting family members involved in the nursing home,
though an ambassador program or family council, couldalso have a positive impact on the resident experience.
Because the notion of home-likeness may mean somethingdifferent from one person to the next, it could be beneficialfor nursing home administrators and staff to ask whattheir residents and family members feel contribute to ahome-like environment.
Some changes that could improve home-likeness in anyfacility include the reduction of unnecessary signage; ensuring there are safe ways for residents to access theoutdoors and engage in their communities; and being creative about how shared rooms and spaces are dividedto create more private conversation areas.
To create a working environment that supports residentquality of life, one option could be to adopt a collaborativepractice model, ensuring that each member of the teamfeels valued in their contribution to the care provided inthe facility.
Administrators could find ways to support staff in gettingto know their residents, and residents getting to knowtheir staff, by providing consistent staffing assignmentswhenever possible. When changes need to be madewithin the nursing home, administrators could considerfinding ways to consult with all of the groups that wouldbe impacted by such changes (residents, family members,staff, unions, administration).
Though this research was conducted in the Nova Scotiacontext, the findings on the importance of relationships,home-likeness, and working environment can be applied,with some creativity, in long-term care homes elsewhere.
This research was part of the Care and Construction: Assessing the Impact of Model of Care on Nursing Home Resident Quality of Life project with funding from the Canadian Institutes of Health Research and the Nova Scotia Health Research Foundation. For more information about the Care and Construction project, visit www.careandconstruction.ca or email [email protected]. LTCT

19LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201420 LONG TERM CARE TODAY
Removing level of careforms in long-term carehomes and addressing thepalliative care gap
William Osler Health System, in cooperation with participating long-term care homes in the Central West Local Health Integration Network (LHIN), recentlycompleted an Ethics Quality Improvement Project withthe goal of reducing errors related to consent, capacity,and substitute decision-making before long-term careresidents are transferred to Osler’s Emergency Department. Dr. Jill Oliver and Dr. Paula Chidwick explain what they learned in the course of this research.
We had learned through a previous project thatmany errors stemmed from the use of the levelof care form, which can drive treatment decisions
and transfers to the emergency department in ways notinitially intended by the form.
Sometimes these errors meant that residents receivedcare they didn’t want, and which provided no benefit.Other times residents wanted care, and could have benefited from it, but they didn’t receive it.
With this project, we wanted to decrease these errors byremoving the level of care form and improving the processaround decision-making prior to transfer. This goal waslargely achieved through LHIN-wide ethics support andeducation, including the use of a checklist to minimize errors, and a different form of documentation (called an“Individualized Summary”) in selected homes in the LHIN.
We believed that by reducing errors, we could reduce thenumber of LTC residents who eventually died in hospitalafter being transferred there two to three times or more in the two months prior to their death. We thought this number would decrease by at least 10%; in fact, over theproject year, it decreased by 18%.
B Y D R . J I L L O L I V E R A N D D R . P A U L A C H I D W I C K
We also found a gap around palliative care that we believeneeds to be addressed in order to build on this initial success.
Some LTC residents were not able to easily access the palliative care that they needed in their own long-termcare home; in other words, they did not have easy accessto palliative care. For example, some residents got accessto palliative care only by first being sent to the hospitalwhere they were admitted for palliative care, or returnedto the LTC home with a palliative care plan in place. Repeated trips to hospital pose risks for residents facingan expected death, as palliative care might be delayed until further acute interventions are attempted, maybe fora second, third, or fourth time.
And some residents unfortunately never accessed the palliative care that they needed, dying in the emergencydepartment before a hospital bed became available or areturn to their home was arranged.
Why does this happen? Why are there so many obstaclesbetween LTC residents facing an expected death and having palliative care in place? We believe that in LTCthere is a complex of beliefs and practices—likely carriedover from the use of the level of care form—that can continue to affect decision-making about treatment ingeneral, and palliative care in particular.
The level of care form typically outlines options—from palliative care in the home to aggressive care in the hospital—from which the substitute decision-maker isasked to choose. We found that even when the level ofcare form is removed, palliative care plans—even whenthey are strongly recommended—are still often presentedas one option among others. This approach changes themeaning of the substitute decision-maker’s decision; instead of choosing to consent or not to the team’s proposed treatment plan, the substitute decision-makerchooses the plan itself. This is an error, as a treatment planmust be proposed by the practitioner seeking consent.
In addition to a passive approach to the proposal of a palliative treatment plan, some substitute decision-makersbelieve that decisions about transfer are really decisionsabout treatment and no treatment (see Figure 1).
Dr. Jill Oliver is a Community Ethicist and Dr. PaulaChidwick is Director of Research & Corporate Ethicsat William Osler Health System. They would like tothank both William Osler Health System and the long-term care homes that participated in this project for their continued interest and support. For a referenced copy of this article, contact Dr. Oliver at [email protected].

21LONG TERM CARE TODAYFALL/WINTER 2014
Some see staying in the long-term care home as “doingnothing” or as “giving up” or providing no treatment. Thisbelief is apparent whenever substitute decision-makersask if their loved ones will continue to be fed or engagedin activities if decision-makers consent to a palliativetreatment plan. Other substitute decision-makers believethat to advocate for their loved one, they must advocatefor aggressive hospital care to do everything possible toprevent death.
The level of care form also unnecessarily ties location with treatment options (see Figure 2). It artificially tiespalliative care to a specific location; if a resident or substitute decision-maker chooses less medically aggressive, more palliative-focused care, then they alsohave to choose to remain in the long-term care home. Toleave the option of hospital care open, residents or theirsubstitute decision-makers have to choose a level thatkeeps transfer to hospital as a possibility—although theselevels often include more aggressive treatment. We foundthat even when the form is removed, location remains a major point of discussion in the consent process. Substitute decision-makers were often asked to make adecision about where their loved one would be cared for,along with their decision of what care their loved onewould receive.
Each of these elements contributes to the palliative caregap, and we think there are good reasons to questioneach one. First, the Health Care Consent Act is clear thatthe role of the health care provider is to propose treat-ment, and this is echoed in the College of Physicians andSurgeons of Ontario’s “Consent to Medical Treatment” and“Decision Making for the End-of-Life” policy statements.
The most difficult decisions about goals of care can arisewhen a resident is approaching end of life.
First, the physician plays an important role in assessingwhen this happens and determining at that time what ispossible, and what is proposed.
Second, the belief among some substitute decision-makersthat TRANSFER = TREATMENT and NO TRANSFER = NOTREATMENT is simply mistaken; there is also the option ofpalliative care in place at the long-term care home.
Third, if the resident has no specific wishes about wherehis or her care takes place, there is no reason to discussthe location of care in advance. The Health Care Consent
Act states that when consent to a plan has been obtained,the health care provider can assume that the consent alsoincludes continuing to receive the same treatment at another location. It is most important that palliative care is provided at the end of life—the location where it is provided can be identified and adjusted as the patient’scondition requires.
The palliative care gap is a concern not only because ofthe personal costs that it imposes on individual residentsand their families, but also because of the system-widecosts it can involve. As stated earlier, when residents cannot easily access palliative care in their own long-termcare home, they will often be transferred to the hospitalinstead. The Ontario Regulation of the Long-Term CareHomes Act requires long-term care homes to hold residents’beds up to 30 days while the resident is in the hospital.That “bed” represents the resident’s home, and residentshave the right to return to it after discharge from hospital.Since the bed is held, there are two costs associated withone person: for the bed in the hospital (paid for by taxdollars), and for the bed in the LTC home (paid for by taxdollars, the resident, or a combination of the two).
These double costs are justifiable whenever the care thatthe resident requires is not available in their home (e.g.,chemotherapy or surgery); they are not justifiable when
Figure 1.
Figure 2.

FALL/WINTER 201422 LONG TERM CARE TODAY
hospital care simply replicates the care available in theirlong-term care home. It became clear throughout thecourse of this project that there are many cases in whichhospital-provided palliative care could have been providedin the home. This duplicated palliative care is even moreproblematic if you consider the non-monetary costs it imposes on those people at end of life who can only access palliative care in the hospital.
In our next Ethics Quality Improvement Project we will tryto expand the project by replacing the level of care formin other long-term care homes in our LHIN, and also bycreating new options so that LTC residents can more easily access palliative care in place. We think that locationof care will become irrelevant as the concept of “team” isexpanded to include both long-term care and the hospital,and as technology is used to bridge the gap that existsnow.
These will be natural consequences that will flow from focusing on care that residents want and that providesbenefits to them—because a treatment plan can’t be bothpatient-centered and location-centered at the same time.
References
College of Physicians and Surgeons of Ontario. 2006a. “CPSO PolicyStatement: Consent to Medical Treatment.” Policy #4-05.
http://www.cpso.on.ca/CPSO/media/uploadedfiles/policies/policies/policyitems/Consent.pdf?ext=.pdf Accessed July 14th, 2014.
College of Physicians and Surgeons of Ontario. 2006b. “CPSO PolicyStatement: Decision Making for the End-of-Life.” Policy #1-06.http://www.cpso.on.ca/CPSO/media/uploadedfiles/policies/policies/policyitems/End-of-Life.pdf?ext=.pdf Accessed July 14th, 2014.
Hawryluck, Laura, Sibbald R, Chidwick P. 2013. “The Standard of Care andconflicts at the End of Life in critical care: Lessons from medical-legalcrossroads and the role of a quasi-judicial tribunal in decision-making.”Journal of Critical Care. Vol. 28, Issue 6. December. p. 1055-1061.http://www.jccjournal.org/article/S0883-9441(13)00191-3/abstract Accessed July 14th, 2014.
Health Care Consent Act, 1996. http://www.e-laws.gov.on.ca/html/statutes/english/elaws_statutes_96h02_e.htm. Accessed July 14th, 2014.
Sibbald, Robert, Paula Chidwick, Mark Handelman, Andrew B. Cooper.2011. “Checklist to Meet Ethical and Legal Obligations to Critically Ill Patients at the End of Life.” Healthcare Quarterly. Vol. 14. No. 4. p. 60 –66. http://consentqi.ca/wp-content/uploads/2013/02/Sibbald_2011_Checklist _HQ_vol14_no4_Sibbald1.pdf Accessed July 14th, 2014.
Oliver, Jill and Paula Chidwick. 2013. “Pilot Project: Ethical Issues in Transfer of Seniors from Long-term Care to Osler ED. Final Report –March 2013.” William Osler Health System. Internal Document.
Oliver Jill, and Paula Chidwick. 2014. “Transfers of LTC Residents to Hospital EDs: An Ethics Quality Improvement Project to Minimize Non-beneficial and Unwanted Hospital Transfers and Maximize System Efficiency.” Healthcare Quarterly Vol.17 No.1. p. 54 – 59.
Ontario Regulation 79/10 made under the Long-term Care Homes Act2007. http://www.e-laws.gov.on.ca/html/source/regs/english/2010/elaws_src_regs_r10079_e.htm#BK175. Accessed July 14th, 2014. LTCT

23LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201424 LONG TERM CARE TODAY
Sadie Friesner, R/TRO, is a recreation therapist atBradford Valley.
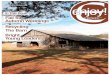
You don’t usually associate long-term care with theoutdoors, but roasting marshmallows, sitting besidea crackling fire, and reminiscing about memories
past were all something the Recreation Therapy staff atBradford Valley wanted to help our residents achieve. Theidea grew into an amazing overnight camping trip thatfour of our residents will never forget.
Last summer, Bradford Valley, in partnership with YogiBear’s Jellystone Park in Toronto, had an overnight outing.Recreation Therapy Assistants Carolyn Owen and Cheri Marques wanted to give their residents an unforgettableexperience to help them be themselves, express themselves,and achieve true leisure-time enjoyment.
At first our planning team had some apprehension and fearof the unknown. How would medications be given? Wherewould residents sleep? How would we help toilet them?These were all questions we answered through planning,assessment, and persuasion. The recreation team plannedthe outing with a detailed itinerary and assessed each resident to ensure they had the ability and would be wellenough to be out of the facility overnight. We were able topersuade three nurses to volunteer their time to administermedications at the appropriate times at the camp site.
Recreation and leisure program facilitation is an interdisci-plinary approach, and through programs like this, we are
Creating priceless memoriesfor residentsB Y S A D I E F R I E S N E R
starting to educate different departments on the amazingbenefits to the well-being our residents are experiencing during different recreation programs.
And how was the camping trip? Breakfast was cookedover the fire, marshmallows were toasted, and the fresh airdid everyone good. We could not have asked for a bettertrial for an overnight trip, and the partnership with thecampground worked out perfectly. One of our participants,who is 99 years old, kept telling the staff what an amazingexperience it was for her.
For us, it was all about helping them keep their leisurenormal; moving into long-term care should not negateprevious leisure experiences nor should it prevent new experiences. With the success of this overnight trip, a second camping trip was held later in the summer, andthere was an overnight “Trip to Toronto” complete with a Blue Jays game.
These activities give our residents the opportunity to feellike they belong. We’re sharing this story because wehope to change the way staff in long-term care thinkabout leisure and recreation, and to help them plan meaningful programs with adaptations to improve thelives of the residents. Those adaptations are easy on ourend when the experiences for residents are priceless. LTCT
Janet enjoying breakfast around the fire.Dien and Carolyn on their way to the campground.

25LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201426 LONG TERM CARE TODAY
At least four U.S. states have passed laws permitting residents in long-term care facilities to maintain surveillance cameras in their rooms. But what is the lawin Canada? Are “Granny Cams” permissible? What arethe competing interests, benefits and risks? Lawyers Erin Kuzz and Gerald Griffiths gave an interesting and informative presentation on this topic at this year’sOLTCA convention, and share their perspective withLong Term Care Today readers.
Video surveillance of resident abuse in North American long-term care homes has made forshocking headline news. It has also inspired fierce
debate about the use of covert cameras, often referred to as “Granny Cams.” Some argue the Granny Cam is necessary to deter resident abuse as well as to defendagainst frivolous and unfounded allegations of abuse. Others say it represents an unnecessary and illegal breachof resident and employee privacy.
Regardless of your point of view, use of a Granny Cam engages the interests of a variety of parties and a range ofOntario and Canadian laws. This article will identify thoseinterests and laws, and offer best practices for long-termcare operators.
GRANNY CAM USE — THE DEBATE
Industry groups and privacy rights activists have fiercelydebated for and against the Granny Cam. Interestingly,there is no obvious line separating those in favour andthose opposed to the technology. One might assume residents and families would be in favour, whereas health-care workers and their employers would be opposed. Butthis is not the case, as the two sides of the debate includerepresentatives of all parties.
Advocates in favour point to the peace of mind a GrannyCam can provide a family by deterring resident abuse,neglect and theft,1 a worker by protecting him/her againsta false accusation, and an employer by providing objective,accurate information on which to operate its business.
Those opposed to the Granny Cam argue it represents abreach of privacy, promotes lack of trust, and negativelyimpacts employee motivation. Organized labour has longfought against the use of any form of surveillance in theworkplace on the basis it threatens the important role ofactive management. Opponents also argue the GrannyCam will encourage litigation which, in turn, will cause anincrease in insurance premiums of home operators.2 Onthe other hand, some U.S. nursing homes have reported a
The “Granny Cam”: the good,the bad, and the lawB Y E R I N K U Z Z A N D G E R A L D G R I F F I T H S
significant reduction in insurance premiums as a result ofinstalling Granny Cams, with one Florida nursing home reporting an annual drop from $57,000 to $10,000.3
ARE GRANNY CAMS LEGAL IN ONTARIO?
Unlike in the United States where four states have passedlaws relating to the use of the Granny Cam in a long-termcare home,4 no such legislation exists in Ontario. That said,the Long-Term Care Homes Act,5 Personal Information andProtection of Electronic Documents Act,6 and PersonalHealth Information Protection Act,7 as well as the CriminalCode,8 common law and the concept of “reasonable expectation of privacy” in a unionized workplace, are eachengaged by the use of a Granny Cam.
Navigating these laws can be difficult. Some apply to allforms of Granny Cam use. Others apply depending uponwho uses the technology and whose privacy interests areaffected. Let’s look at the potential impact of each ofthese laws as they apply generally, and then look at thelaws which apply specifically to a long-term care home.
LAWS OF GENERAL APPLICATION
CRIMINAL LAWThe Criminal Code applies across Canada, and prohibitscertain types of recordings, including an audio recordingof a private communication made without the consent of at least one of the parties to the conversation.9 TheCriminal Code also prohibits “voyeurism” which is thecovert surveillance of a resident in his/her room where nudity or sexual activity is captured.10 The exception iswhere the recording is made for the “public good” and

27LONG TERM CARE TODAYFALL/WINTER 2014
may include the installation of a camera in response to aspecific concern of abuse or theft.
To avoid inadvertently committing a criminal offence, a bestpractice is to ensure, wherever possible, there is consentof the informed resident, and the audio component of therecording is turned off.
COMMON LAW Historically, our courts have not recognized a self-standingright to privacy in Ontario. However, this changed in 2012when the Ontario Court of Appeal recognized a new, butlimited, tort of invasion of privacy called “intrusion uponseclusion.” This tort has five elements: (i) there must be intentional or reckless conduct; (ii) that invades a person’sprivate affairs; (iii) without lawful justification; (iv) in amanner that is highly offensive to a reasonable person;and (v) which causes distress, humiliation or anguish.11
The tort is intended to address egregious invasions into the most private issues such as health and financialinformation.12 And while this tort is still in its infancy, a targeted recording undertaken in good faith, for the purposeof protecting a resident, is unlikely to be captured by thistort.
The Personal Information Protection and Electronic Documents Act (PIPEDA)In Ontario,13 PIPEDA governs the collection, use and disclosure of personal information in a commercial activity.Generally speaking (there are exceptions), the individualabout whom the personal information is collected, used ordisclosed, must consent to such activity.
PIPEDA does not apply to a long-term care home’s collection of personal information of employees. However,long-term care homes can have obligations under PIPEDAin relation to several types of individuals, including resi-dents, their family members and guests at the home.Where a video camera may capture personal informationabout any of these latter individuals, consent may be required, and could be obtained by specifically asking aresident for permission or installing signs above the homeentrance advising guests they may be subject to covertsurveillance.
Where a Granny Cam is installed by a resident or familymember, PIPEDA is unlikely to apply because: (a) PIPEDAonly applies to personal information collected “in thecourse of a commercial activity,”14 and (b) PIPEDA doesnot apply to personal information collected “for a personalor domestic purpose.”15 In analyzing whether surveillanceis “commercial” or for a “personal or domestic purpose,”adjudicators have focused on the specific purpose forwhich the surveillance was initiated, and its intended use.On this basis, a video recording by a private person forpersonal interest or even in the context of litigation has generally been considered to lack a “commercial character.”16
Even where PIPEDA does apply, consent is not requiredwhere: (a) the knowledge of the person subject to the
surveillance would compromise the availability of thefootage; and (b) the surveillance is carried out reasonablyfor purposes related to investigating an illegal activity.17
Finally, guidelines established by the Privacy Officer ofCanada (the body overseeing compliance with PIPEDA)state an organization conducting covert video surveillanceshould have policies in place which govern how and whensurveillance will be conducted.18
LAWS THAT SPECIFICALLY APPLY TO A HOMELong-Term Care Homes Act (LTCHA)The LTCHA contains a Residents’ Bill of Rights19 which applies like a contract between the resident and home.20
The Bill of Rights places certain privacy obligations on the home in relation to its residents, including that everyresident has the right to “privacy in treatment and in caring for his or her personal needs,” “to communicate inconfidence…and consult in private,” as well as to “meetprivately…in a room that assures privacy.”21
Privacy rights under the Bill of Rights are not absolute,and consent to intrude upon privacy can be obtained from a resident. A home seeking to install a camera shouldtherefore ensure it has obtained consent from any affectedresident or his/her authorized decision-maker.
Similarly, if a home is aware of the installation of a cameraby a resident or a resident’s family member, the home maybe obligated to take steps to protect the privacy rights ofother residents under the Bill of Rights. This may includeraising the issue with affected residents to confirm theyconsent to the continued use of the Granny Cam.
Personal Health Information Protection Act (PHIPA)PHIPA requires a resident’s consent to collect, use or disclose his or her “personal health information.”22 Thisterm is broadly defined23 and includes records that relate to an individual’s physical or mental health or theproviding of care to that individual. To obtain or use arecording that includes this type of information, a homeshould obtain consent from the resident or authorized decision-maker.24
EMPLOYEE PRIVACY RIGHTSOur courts have not yet recognized a self-standing rightto privacy in relation to surveillance of a non-unionizedemployee while at work. Invasive workplace surveillancewas found to be a contributing factor to a finding of constructive dismissal in one case;25 however, the court in that case clearly stated that video surveillance of a non-unionized employee is not prohibited in Ontario.26
The situation is different in a unionized setting. Arbitratorshave found that a unionized employee has an expectationof privacy such that only a “reasonable” installation of acamera is permissible (e.g., in response to a specific problem such as theft or abuse). To this end, an arbitratorwill evaluate the purpose of the surveillance, availability ofalternative, less intrusive forms of information gathering,location of the camera (e.g., what information is gathered),duration of recording, and who has access to the footage.

FALL/WINTER 201428 LONG TERM CARE TODAY
IS VIDEOTAPE EVIDENCE ADMISSIBLE IN COURTOR AT ARBITRATION?
Just because videotape evidence may be “legal” to obtaindoes not mean the evidence is admissible in court or at arbitration. Similarly, illegally obtained video evidence maystill be admitted in court where the evidence is relevantand an accurate depiction of what occurred.27
In the unionized context, grievance arbitrators haveadopted two approaches to determine whether videotapeevidence is admissible. The “relevance” standard adoptedby courts, and the “reasonableness” standard which assesses whether the surveillance was reasonable in thecircumstances, applying the factors identified above (thepurpose of the surveillance, availability of alternative, lessintrusive forms of information gathering, location of thecamera, duration of recording, and who has access to thefootage).
TIPS AND BEST PRACTICES
Whether, when and how to employ a Granny Cam is not astraightforward answer. Many privacy laws are new orevolving as quickly as the surveillance technology itself.As homes navigate these challenging issues, the followingare offered as tips and best practices.
Where a Granny Cam is installed by a home:
1. The Granny Cam should not audio record in violationof the Criminal Code. Where the audio is turned on,consent of one party to any conversation is required.
2. The Granny Cam should be targeted to capture specific conduct and used in the least intrusive manner possible. This includes positioning the camerato avoid capturing any nudity or sexual activity.
3. The home should have in place policies governinghow and when a Granny Cam will be used.
4. Signs should be prominently posted advising individuals they may be subject to surveillance.
5. If the camera is in a resident’s room, consent shouldbe obtained of a resident and any roommate capturedby the Granny Cam.
Where a Granny Cam is installed by a resident or familymember:
1. Such use is not prohibited, provided the Granny Camis not used in a criminal or egregious manner suchthat it constitutes “intrusion upon seclusion.”
2. A home must be mindful of the impact on other residents.

29LONG TERM CARE TODAYFALL/WINTER 2014
3. If the home is aware the surveillance intrudes uponanother resident’s privacy protected under the Bill ofRights, the home should take steps to confirm theresident’s consent to the surveillance.
To learn more and for assistance addressing privacy andsurveillance issues in a long-term care or related home,contact a member of Sherrard Kuzz LLP. The informationcontained in this article is provided for general informationpurposes only and does not constitute legal or other professional advice. Reading this article does not create a lawyer-client relationship. Readers are advised to seekspecific legal advice from Sherrard Kuzz LLP (or other legal counsel) in relation to any decision or course of action contemplated.
1. Toben, Bradley J.B. and Matthew C. Cordon. “Legislative Stasis: TheFailures of Legislation and Legislative Proposals Permitting the Use ofElectronic Monitoring Devices in Nursing Homes” (2007) 59 Baylor L.Rev. Vol. 3 675 at 698 [Baylor].
2. Ibid. at 695.
3. Ibid. at 696.
4. Texas, New Mexico, Maryland and Oklahoma require consent of the res-ident and any affected roommate to install a Granny Cam.
5. S.O. 2007 c.8 [the “LTCHA”].
6. S.C. 2000 c. 5 [“PIPEDA”].
7. S.O. 2004, c. 3 [“PHIPA”].
8. R.S.C. 1985, c C-46.
9. Criminal Code at s. 183.1 and 184.
10. Criminal Code at s. 162.
11. Jones v. Tsige (2012), 108 OR (3d) 241at para. 71 [Jones v. Tsige].
12. Ibid. at para. 72.
13. This may differ in other provinces.
14. PIPEDA at paragraph 4(1)(a).
15. PIPEDA at paragraph 4(2)(b).
16. See e.g. State Farm Mutual Automobile Insurance Co. v. Canada (Privacy Commissioner), [2010] F.C.J. No. 889; Ferenczy v. MCI MedicalClinics et al., [2004] O.J. No. 1775.
17. PIPEDA at paragraph 7(1)(b).
18. Office of the Privacy Commissioner of Canada Reports and Publications.“Guidance on Covert Video Surveillance in the Private Sector. Online:http://www.priva.gc.ca/information/pub/.
19. Supra, note 3 at s. 3 (the “Bill of Rights”).
20. Bill of Rights, supra note 5, at section 3(3).
21. Bill of Rights, supra note 5, at section 3(1).
22. The form of consent may vary and some exceptions do apply to thisrequirement.
23. PIPEDA at s. 7(1).
24. PHIPA at s. 29.
25. Colwell v. Cornerstone Properties Inc., 2008 CanLII 66139 (ON SC).
26. Ibid. at para. 30.
27. R. v. Nikolovski, [1996] 3 S.C.R. 1197; R. v. Jamieson, [2004] O.J. No.1780 (S.C.J.). LTCT

FALL/WINTER 201430 LONG TERM CARE TODAY
The Ontario Long Term Care Association’s recent report,This is Long-Term Care 2014, shows that the prevalenceof many chronic conditions in long-term care has risenby 5 to 12% in just five years. Staff need evidence-basedsupport to care for an increasingly clinically complexpopulation, and order sets can provide a large part ofthis support. Dr. Amir Ginzburg, Dr. Stuart Egier, and LoriBrown, NP, are part of a team that developed and testedorder sets in long-term care.
Over the last three years, Trillium Health Partnershas been working collaboratively with long-termcare, community, and government partners to
bring order sets into long-term care, with the OntarioLong Term Care Association’s endorsement and with funding from Canada Health Infoway (see Project partners).
Order sets are detailed instructions for the care of residentswith specific conditions. They translate best practiceguidelines and evidence from the medical literature and other trusted sources into a checklist format that provides clear information and instructions about resident care.
Order sets for 50 different conditions in long-term carewere developed and tested at pilot sites using a compu-terized tool (see Order sets for long-term care). These setswere not simply adopted from acute care. Each order setwas developed from scratch by drawing on the expertiseof long-term care clinicians, pharmacists, and content specialists, combined with the experience of long-termcare corporate, home, and clinical leadership. The ordersets are also aligned with long-term care sector regulationsand legislation. Feedback from users at the pilot sites wasincorporated into the final versions of the order sets.
New order sets in long-termcare support complex careB Y D R . A M I R G I N Z B U R G , D R . S T U A R T E G I E R , A N D L O R I B R O W N
To date, thousands of order sets representing tens ofthousands of unique patient care orders have been com-pleted via computer entry at the pilot sites. The project’smethods and results are expected to be published in ajournal article in the coming year. The project demonstratedthe importance and value of incorporating order sets intolong-term care, helping frontline providers to provide evidence-based care to residents with increasing medicalcomplexity.
LTC organizations will be able to access order sets for freeby participating in the Canadian Computerized ProviderOrder Entry (CPOE) Toolkit. LTC order sets will be postedin the winter. The LTC order set content is also availablevia PatientOrderSets.com for subscribers to their network.
Amir Ginzburg is a General Internist and Medical Director, Quality and Performance at Trillium HealthPartners in Mississauga. He is an Assistant Professorat the Institute of Health Policy, Management andEvaluation at the University of Toronto. Stuart Egieris a family physician in Mississauga and the MedicalDirector of the McCall Centre for Complex Care,Eatonville Care Centre, Brampton Extendicare andMississauga Extendicare Long Term Care Homes. Lori Brown is a Nurse Practitioner and Coordinator at Mississauga Halton LHIN’s Nurse Practitioners Supporting Teams Averting Transfers (NPSTAT), ateam providing acute, episodic care to residents inthe LHIN’s 27 Long-Term Care Homes.
Project partners■ Trillium Health Partners (project sponsor and
complex continuing care pilot site)■ Nurse Practitioners Supporting Teams Averting
Transfers (NPSTAT)■ Ontario Long Term Care Association■ Canada Health Infoway■ Eatonville LTCH (LTC pilot site)■ Extendicare Mississauga (LTC pilot site)■ McCall Centre (LTC pilot site)■ PatientOrderSets.com (vendor for order sets and
associated technology)
Order sets are successful when:
➤ Corporate and LTC home leadership are critical tofoster an environment of change and adoption ofthe information technology
➤ Training and support of staff and providers are essential, and should be based on an IT changereadiness assessment and change managementmodel
➤ Order sets must be adapted by an organization’sproviders and staff to local factors
➤ Order sets must be reviewed by the organization at specific intervals, usually annually or biannually,to ensure the content remains valid

31LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201432 LONG TERM CARE TODAY
LTC Acquired Pneumonia Order SetLTC Acute Exacerbation of Chronic Obstructive
Pulmonary Disease Order SetLTC Arterial Ulcer Management Order SetLTC Atrial Fibrillation Stable Resident Order SetLTC Cat, Dog, Human Bite Management Order SetLTC Cellulitis (Uncomplicated) Order SetLTC Cellulitis Diabetic Foot Order SetLTC Cellulitis Facial Order SetLTC Chronic Obstructive Pulmonary Disease Stable
Management Order SetLTC Congestive Heart Failure Acute Exacerbation
Order SetLTC Conjunctivitis Order SetLTC Constipation Management Order SetLTC Custom Correction-Dose Insulin Order SetLTC Dehydration Order SetLTC Depression Order SetLTC Diabetes Management for Eating Resident Order SetLTC Diabetes Management for NPO Resident
Order SetLTC Diabetes Management for Sick Resident Order SetLTC Diabetes Management for Tube Feeding Resident
Order SetLTC Diabetic Foot Ulcer Order SetLTC Dyslipidemia Treatment Order SetLTC End-of-Life Order SetLTC Enteral Feeding Tube Insertion Order SetLTC Enteral Nutrition Order SetLTC General Admission Order SetLTC Herpes Zoster (Shingles) Order SetLTC Hypoglycemia Management AlgorithmLTC Hypoglycemia Management Clinical ProtocolLTC Hypothyroidism Order SetLTC Influenza Symptom Management Order SetLTC Intertrigo Management Order SetLTC Lab and Diagnostic Investigations Order SetLTC New Diarrhea, Suspected Clostridium Difficile
Clinical ProtocolLTC Pain Management Order SetLTC Parkinson's Disease Order SetLTC Parotitis Order SetLTC Practitioner Blank Order SetLTC Skin Tear Order SetLTC Suspected, Confirmed Clostridium Difficile
Order SetLTC Uncomplicated Gastroesophageal Reflux Disease
Order SetLTC Urinary Tract Infection Treatment Order SetLTC Usual Correction-Dose Insulin Order SetLTC Venous Leg Ulcer Management Order SetLTC Viral Respiratory Tract Illness Order SetLTC Vulvo-vaginitis Order SetLTC Wound Care Order SetComplex Continuing Care Acquired Pneumonia
Order SetComplex Continuing Care Cellulitis Diabetic Foot
Order SetComplex Continuing Care Dehydration Order SetComplex Continuing Care VTE Prophylaxis Order Set
Order sets for long-term careWhat order sets do
Well-designed standard order sets—both electronicand paper formats—have the potential to:
■ Integrate and coordinate care by communicatingbest practices through multiple disciplines, levelsof care, and services
■ Modify practice through evidence-based care■ Reduce variation and unintentional oversight
through standardized formatting and clear presentation of orders
■ Enhance workflow with pertinent instructionsthat are easily understood, intuitively organized,and suitable for direct application to current information-management systems
■ Reduce the potential for medication errorsthrough integrated safety alerts and reminders
■ Reduce unnecessary calls to physicians for clarifications and questions about orders.
Reprinted from the Institute for Safe MedicationPractices Guidelines for Standard Order Sets(www.ismp.org). LTCT

33LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201434 LONG TERM CARE TODAY
Highlights of the Quality and Innovation Forum
Sophia Thomas and Beverley Rayside at the Winbourne Park table.
Jennifer Cornell, Lisa Thompson, and Lynne Johnson at the Grey Gables table.
Lifetime Achievement Award to Muriel “Babe” Aisbitt: Bill Tedfordand his daughter Debbie (both centre) receive an award on behalf of
Muriel Aisbitt, with Candace Chartier, Julia King, and David Jarlette.
Nursing Leadership Awards 2014: Mya Kitts, Susan Sajadian,Chantel Weatherbed, Sunleen Rathor, Deborah Beckman,
Brenda Irwin, and Candace Chartier.
how well they are doing. There were also several discussionsabout making sure that data is interpreted correctly andput in the right context by media.
Participants enjoyed the inspiring presentations in the Innovators’ Den, which offered the opportunity to learnabout everything from reducing antipsychotic medicationsto smartbed technology. And the efforts of Quality Awardwinners, on display for everyone to see and discuss, werea significant highlight of the conference. The independentpanel of judges was impressed by the calibre of awardsubmissions. They recommended that the Ontario Long Term Care Association publicize the work of othersubmissions as well as the award winners, to help moregood ideas spread across long-term care. Watch for theirstories in future issues of Long Term Care Today.
Starting in 2015, the Quality and Innovation Forum will be combined with OLTCA’s annual Research Day to bringresearch, quality, and innovation under the same roof—where they belong. The conference, called “This is Long-TermCare,” will be held in Toronto from November 23–25, 2015.
It’s not easy to choose highlights from the Ontario LongTerm Care Association’s Quality and Innovation Forum,held in June. There was a high level of interest in all the
sessions, in the award winners’ displays, and at the annualAwards Gala. But there were some key take-home pointsfor participants.
In April 2015, long-term care homes in Ontario will be required to implement quality improvement plans (QIP).Popular speaker and consultant Geneviève Lukenda-Lundtalked about some of the challenges long-term carehomes are experiencing, and provided specific steps thathomes can take to develop plans. Her session provideduseful and practical information for frontline and managerial staff in homes.
Two panels on data quality explained and emphasized theimportance of having good data and reporting it publicly.Good data, the panelists said, gives everyone solid evidenceto make decisions and helps homes to improve care. Public reporting also helps organizations to focus on areasthat are considered priorities and to be accountable for

35LONG TERM CARE TODAYFALL/WINTER 2014
Panelists Corrine McIsaac, Jayne Warwick, Dr. Paul Beaulne, and Aimee Merkley.
The OMNI Diabetes Protocol table with Chris Brockington and Shawn Riel.
Panelists Connie Paris, Dr. John Hirdes, and Dr. Walter Wodchis.
Poonam Kathuria, Trillium Talent Resource Group.
Alexa Granger and Andy Hind at the MyndTec display.Speaker Geneviève Lukenda-Lund explains quality improvement.

FALL/WINTER 2014
Christine Ozimek and Colin LeBrun discuss the Home We Care app.
Enjoying the Human Touch massage chair. LTCT
Greig Nishio helps Krista Griffin to sign up with OLTCA’s “Better Seniors’ Care” campaign.
Bill O’Neill with Jocelyn Hunt of the Alzheimer Knowledge Exchange.


FALL/WINTER 201438 LONG TERM CARE TODAY
PROFESSIONAL DIRECTORY
V O L U M E 2 5 I S S U E 3 F A L L / W I N T E R 2 0 1 4
If you are interested in receiving information about any of the following advertisers, contact: OLTCA,905-470-8995, ext. 39or email [email protected]
3M . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Achieva Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31ArjoHuntleigh . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Canada Brokerlink . . . . . . . . . . . . . . . . . . . . . . . . . . OBCCardinal Health Canada . . . . . . . . . . . . . . . . . . . . . . . . . 7Centric Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . IFCEvac Chair . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Georgian College . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32itacit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . IBC
Maytag Canada . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Medical Pharmacies Group . . . . . . . . . . . . . . . . . . . . . 19Medco Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37N.S. Smith Realty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Rexall Specialty Pharmacy . . . . . . . . . . . . . . . . . . . . . 28SCA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5SCA/Tork . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Sherrard Kuzz LLP . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Silver Meridian . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Long Term Care Today Ad Index

39LONG TERM CARE TODAYFALL/WINTER 2014

FALL/WINTER 201440 LONG TERM CARE TODAY