Embed Size (px)
Citation preview

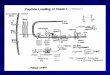
Off the shelf strategy for CAR-T therapy using cord blood
Martino Introna

TCR
MHC I
Target cell
Tumorcell
++
CIK cellRestricted
killingNon MHC-restricted
killing
CD3/CD8/CD56 T/EMRA
DNAM1LFA1
CD56NKG2DNKp30
Adapted by Pievani et al, Blood, 2011

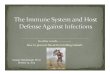
Study Design
BM or PB transplant
Taperedimmunosuppressionand chemotherapy
only if needed
Molecular or cytogenetic or hematologic
RELAPSE
1st Standard
DLI(1x106/kg)
2ndStandard
DLI(1x106/kg)
1stCIK
infusion
2ndCIK
infusion
3rdCIK
infusion
Follow-up
Combina-tion
1st CIK cells infusion
2nd CIK cells infusion
3rd CIK cells infusion
1 1x106/Kg 1x106/Kg 5x106/kg
2 1x106/Kg 5x106/kg 5x106/kg
3 1x106/Kg 5x106/kg 10x106/kg
4 5x106/kg 5x106/kg 10x106/kg
3 weeks 3 weeks 3 weeks 3 weeks
Introna M. et al, BBMT, 2017

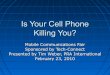
Study FlowPatients enrolled in the study protocol (N=74)
Patients allocated to CIK treatment (N=60)
Patients completing study protocol (N=43)
1ST DLI
2ND DLI
1ST CIK
2ND CIK
3RD CIK
2 death before starting therapy
4 disease progression and death1 GvHD
3 disease progression and death2 GvHD1 drop out
7 disease progression and death2 GvHD
4 disease progression and death1 insufficient cell supply1 hemolitic anemia2 GvHD
1 excluded for protocol violation
Introna M. et al, BBMT, 2017

Introna M. et al, BBMT, 2017
Clinical outcomes according to type of relapse
AML
ALL

Characteristics All (N=73) Pediatrics (N=15) Adults (N=58)
Preparative regimen, N(%)MAC 53 (72.6) 12 (80.0) 41 (70.7)RIC 20 (27.4) 3 (20.0) 17 (29.3)
Stem cell source*, N(%)PB 42 (59.2) 2 (14.3) 40 (70.2)BM 29 (40.8) 12 (85.7) 17 (29.8)
Donor, N(%)SIB 37 (50.7) 5 (33.3) 32 (55.2)MUD 31 (42.4) 8 (53.4) 23 (39.6)HLA aploidentical 5 (6.9) 2 (13.3) 3 (5.2)
Relapse type, N(%)Hematologic 44 (60.3) 6 (40.0) 38 (65.5)Molecular + Cytogenetic 29 (39.7) 9 (60.0) 20 (34.5)
Months from diagnosis to HSCT, median (range) 6 (2-102) 24 (5-62) 5 (2-102)
Months from HSCT to relapse, median (range) 6 (0.5-124) 6 (1-26) 6 (0.5-124)
Introna M. et al, BBMT, 2017

CIK II STUDY ACKNOWLEDGMENTS
USC Hematology of Bergamo, ItalyDr. F. Lussana, Dr. A. Algarotti, Dr. F. Delaini, Dr. A. Grassi, Dr. C. Micò,Dr. M. L. Ferrari, Dr. E. Todisco, Dr. C. Pavoni, Prof. A. RambaldiDiv. Hematology and TMO, Bolzano, ItalyDr. I. Cavattoni, S. Deola
Center of Cell Therapy “G. Lanzani”, Bergamo, ItalyDr. M. Introna, Dr. J. Golay, Dr. E. Gotti, Dr. R. Valgardsdottir
Department of Pediatrics, University of Milano-Bicocca, Fondazione MBBM, Monza, ItalyProf. E. Biagi, Dr. A. Balduzzi, Dr. A. Rovelli, Dr. S. Napolitano, Dr. G. Sgroi, Dr. E. Marrocco, Prof. A. BiondiDepartment of Hematology, Monza, ItalyDr. M. ParmaApheresis Unit, Monza, ItalyDr. P. Perseghin
Laboratory of Cell and Gene Therapy “S. Verri”, Monza, ItalyDr. G. Gaipa, Dr. D. Belotti, Dr. B. Cabiati

Merker M, et al. BBMT 2019
DLI CIK
MFD 17 31%
3 8%
MUD 25 45%
10 28%
MMFD 13 24%
23 64%
Overt Relapse


10
100
1000
10000
100000
1 2 3 4 5 6 7
TNC
x10
6
X-VIVO X-VIVO+HS
Optimization of method to expand CIK from banked CBUs
Golay et al. Cytotherapy 2018
Adding 1% human serum improves CIK cellexpansion from banked CBUs

0
20
40
60
80
100
120
NKG2DCD27
CD28
CD137
CD154
CD11a
CD49d
CD200R
CD244
CD274
CD272
CD279
CD152
CD223
CD366
% P
ositi
ve c
ells
CD8+ subset CB-CIKPB-CIK
**
**
N=6
0
20
40
60
80
100
CD3+ CD3+CD56+ (CIK) NK
% P
ositi
ve c
ells
Phenotype of CB-CIK in 1%HSAB is similar to that of PB-CIK
0
20
40
60
80
100
CD4+ CD8+
% P
ositi
ve c
ells
***
***CB-CIK N=8PB-CIK N=8CB-CIK N=8
PB-CIK N=8
J Golay, et al. Cytotherapy 2018

0
20
40
60
80
100
CD4 CD8
% P
ositi
ve c
ells
CB-CIKPB-CIK
0
20
40
60
80
100
CD4 CD8
% P
ositi
ve c
ells
CB-CIKPB-CIK
CD
56
CD3
CB-CIK
N=8
PB-CIKA
B
C
*
***
***
J Golay, et al. Cytotherapy 2018

Kill
Tumor cell CIK
Bispecific antibody
Target Effector

-20
0
20
40
60
80
100
120
% L
ysis
CB-CIK1 vs REHCB-CIK2 vs REHCB-CIK3 vs BJABPB-CIK1 vs REHPB-CIK2 vs REHPB-CIK3 vs BJAB
- + - + - + BLINA
1:1 3:1 10:1 E:T
0
20
40
60
80
100
CIK-CB PB-CIK
% L
ysis
K562A B
N=3 N=6
***
******
0
20
40
60
80
100
120
- + - + - +
% L
ysis
CB-CIKPB-CIK
N=3
1:1 3:1 10:1
BLINA
*
*
*C
E:T J Golay, et al. Cytotherapy 2018

0
20
40
60
80
100
120
0 10 20 30 40 50 60 70
Surv
ival
(%)
Time (days)
0
20
40
60
80
100
120
0 10 20 30 40 50 60 70
Surv
ival
(%)
Time (days)
A BCB-CIK PB-CIK
CTRLBLINACIKCIK+BLINA
******
J Golay, et al. Cytotherapy 2018
NOD SCID mice inoculated iv with 106 ALL-2 cells

Start Cell yield at the end of culture Release criteriaTheoretical yield of CIK from whole CBUa
CB-CIK batch number
TNC (x106) put in culture
% CD3+ Days
Fold increaseTNC
TNC x106
CIK x106
% CD3+
%CIK
% NK
%live cells
Other quality controlsb
CIKx106 CIKx106/kg
CB-CIK1 300 46.6 25 22.9 6871 3270 97.9 47.6 2.1 85.3 Pass 11454 163.5CB-CIK2 230 54.2 23 6.4 1472 610 98.3 41.4 1.6 86.3 Pass 1173 16.7CB-CIK3 302 36.5 17 8.5 2574 1387 92.6 53.9 7.0 89.9 Pass 2312 33.0CB-CIK4 732 43.0 20 6.2 4563 1725 91.5 37.8 8.4 95.1 Pass 1725 24.6Median 301 44.8 21.5 7.5 3332 1079 99.3 44.5 4.6 88.1 NA 2018 28.8
Yields and quality of CIK cells expanded from banked CBUs in GMP
aYields were calculated considering the blood volume used for expansion relative to the total CBU volumes available and, in case of CBU1, the actual fraction of TNC put in culture, with respect to total TNCs obtained after washing the CB material on day 0.bGMP quality controls include <7 IU/ml endotoxin, sterility for aerobic and anaerobic microorganisms, absence of mycoplasm
J Golay, et al. Cytotherapy 2018

Ficoll/ Wash
Initialexpansion
Medium/large scale expansion in bioreactors
Product wash and medium exchange intofreezing medium
-Gas perm. bags/G-REX/flasks--differentproducts: CIK, T cells
-Sepax: +/-ficoll-Differentcellsources(PB, CB, aphereticmaterial)
-Bioreactor type (Xuri/Quantum/G-REX)-Peristaltic pump (Gatherex)-Growth conditions (cell conc, reperfusion timing, media)-Comparison with flasks-Cell growth measurement methods-T cells, CIK, BET, -Automation
-Sepax-Freezing medium (Cryostor/plasma+ DMSO)-Stability studies-Automation
STEP 1 STEP 3 STEP 4 STEP 5
Options and flow chart for CIK expansion in closed systems (+/-CAR)
-Electropor. In closed system(4D-Nucleofector™ LV Unit)-different cellsources (CB, PB, Aph)
STEP 2
Gene transduction

Initial expansion Medium/large scale expansion in bioreactors
XURI BIOREACTOR
Optimization of expansion steps
Flask
G-REX
Standard method in flasks
G-REX

CIK Expansion in XURI vs FLASK ( 2 validations after some optimization)
A. Time course B. Mean fold increase of TNC at the end of culture with respect to start
N=2 N=2
9-10 days 10-14 days
Or

Add large amount of medium at start
Incubate 10-12 days in standard incubator
Faster growth due to better gas exchange
Gas-permeablemembrane at the bottom
G-Rex vessels
Version with tubings to connect to Sepax/ gatherex to load and collect cells in closedsystem

0
50
100
150
200
250
0 9-11 21-22
Fold
incr
ease
Days
FlasksFlasks ->G-Rex
N=3
flasks
G-Rex or flasks
0
50
100
150
200
250
0 9-11 21
Fold
incr
ease
Days
0.25x106/cm2
0.5x106/cm21x106/cm2
N=3
flasks
CIK Expansion in G-Rex vs FLASK ( set up)
Different cell densities in G.Rex
9-10 days
10-12 daysor

0
20
40
60
80
100
120
0 10
Fold
incr
ease
Days
0.25x106/cm20.5x106/cm21.0x106/cm2
N=2
0
100
200
300
400
500
0 10-11 21To
tal c
ell n
umbe
r (x1
06)
Days
G-RexFlasksN=3
Only 1 G-REX (10-14 days) Only Flasks
CIK Expansion in G-Rex vs FLASKs (optimization)
or
Set up G-Rex Comparison flasks G-REX
PBMC Harvest

CIK-PB in flasks or G-Rex show equivalent cytotoxicityagainst K562
N=3

N=3
*
*
*
NK CIK
Overall phenotype at end of culture is similar for CIK in G-Rex vs flasks, but lower % CD3+CD56+

0 10 20 30 40 50 60 70 80 days
ALL-2 iv survival
CIKBlina
Exp 1734Efficacy of
CIK-G alone andcombined withBlina in ALL2
model
0 10 20 30 40 50 60 700
50
100
CIK-G + blina vs vehicle p=0,0016** Mantel CoxCIK-G vs vehicle p=0,0016** Mantel CoxCIK-G vs CIK-G +Blina p=0,038* Mantel Cox
CIK-G +Blina
vehicleCIK-G
days
Surv
ival
(%)
****
CIK-G are effective in vivo in mice (+/-blinatumomab) in Ph+ ALL model

CIK from CB or PB (latter expanded in G-REX) do not induce GvHD in NSG mice
(Sarah Tettamanti, Fondazione MBBM, Monza, Italy)
0
20
40
60
80
100
120
0 50 100 150 200
Surv
ival
(%)
Days
PBMCCIK-PB in G-RexCIK-CB

Theoretical yields of CIK in G-REX based on initial validations
50x106
PBMC
3x109 TNC
1x109 CIK1 liter and about 10 days
(1 G-REX 100M)
500x106
CB MNC
30x109 TNC
10x109 CIK10 liter and about 10 days
(4 G-REX 500CS)
PB small scale
CB large scale

HLA A HLA B HLA DR11 2 8 18 11 172 24 35 51 11 142 30 13 44 7 11
24 29 18 44 7 112 3 7 35 11 153 33 35 65 1 13
11 30 18 35 11 171 2 51 57 7 132 11 35 50 1 71 23 44 49 7 112 24 35 44 4 131 32 35 51 11 133 11 35 44 4 143 26 38 51 11 132 24 51 62 4 132 24 44 51 8 162 24 44 49 11 132 24 18 58 16 17
24 26 7 35 1 153 24 8 35 16 171 2 52 63 13 152 2 44 51 1 15
25 68 18 51 11 153 32 18 44 7 11
11 24 51 52 11 1526 68 35 44 11 132 24 38 61 11 133 24 13 35 7 111 2 37 57 10 111 2 18 3901 1 16
The 30 CBU with the most frequent
haplotypes in Italy
IBMDRItalian Bone Marrow Donors Registry
In collaboration with Nicoletta Sacchi and Anna Maria Gallina, IBMDR, E.O. Ospedali Galliera, Genova

Minimal HLA matching present in different allo-HSCT settings
Allogenic transplant with CBUHLA A HLA B HLA C HLA DRB1*
x x x xy y y y
Haplo-identical transplantHLA A HLA B HLA C HLA DRB1
x x x xy y y y
Haplo-matching CB-CIK (3/6)HLA A HLA B HLA C HLA DRB1
x x x xy y y y
* High resolution
In collaboration with Nicoletta Sacchi and Anna Maria Gallina, IBMDR, E.O. Ospedali Galliera, Genova

HLA matching
Patient HLAHLA A HLA B HLA DR1
11 24 18 39 15 16
Banked CB CIK unit HLAHLA A HLA B HLA DR1
02 24 18 58 16 17
At least 3/6 matching
In collaboration with Nicoletta Sacchi and Anna Maria Gallina, IBMDR, E.O. Ospedali Galliera, Genova

simulation
80 consecutive ASST-PG23 Hematology transplantedpatients
5 batches from each cord blood unit => 150 batchesbanked from the 30 CB selected units
60/80 patients with positive matching75%

Sponsor: Fondazione Tettamanti

Modification and expansion of mononuclear precursors by the SB system
Magnani CF. et al, Oncotarget, 2017

Ø 15-20 patientsØ Da 1 x 106 a 15x106 /kg
dose escalation
Sponsor:Fondazione Tettamanti Strutture:Pediatric patientsASST-Monza, Ospedale San Gerardo – Monza, IT Adult patientsASST-Bergamo, Papa Giovanni XXIII – Bergamo, IT
NCT03389035
Phase I/Iia trial with allogeneicCIK cells transduced by SB CAR CD19 in adult and pediatric ALL patients relapsed after HSCT

Magnani CF. et al, Oncotarget, 2017
CD19.CAR redirect CIK-cell activity against CD19+ cells.

Magnani CF. et al, Oncotarget, 2017
Specific cytokine production of CD19.CAR CIK cells.

Magnani CF. et al, Oncotarget, 2017
In vivo anti-tumor activity of CD19.CAR

CIK
Gene non-viral transfection manufacturing
Viral vectorsEfficient /standardized but time-
consuming, expensive, non random integration
TRANSPOSONSMobile DNA elements naturally occurring in
the genome
Easy to purify, non-immunogenic, random pattern of integration
Cytokine Induced Killer (CIK) as effector cells
Cytokine Induced Killer cells (CIK)
T cells with NK-like cytotoxicity,
enriched in CD3+CD56+
Clinical experience with allogeneic CIK: feasible, safe and well tolerated with reduced risk of GVHD, included in 5
patients with CIK from haploidenticaldonors
(Introna et al. BBMT 2017, EudraCTN°2008-003185-26)

USS Centro di Terapia Cellulare «G. Lanzani», ASST Papa Giovanni XXIII, Bergamo
J. Golay RAQC. CapelliO. PedriniE. GottiR. ValgardsdottirF. CorrentiI. CattaneoS. ZaninelliS. TettamantiC. CuofanoM. Introna QP
USC Hematology, ASST Papa Giovanni XXIII, Bergamo
PI: Prof. A. RambaldiG. GrittiF. Lussana
Hematology,ASST Monza Ospedale S Gerardo
Prof A. BiondiE. BiagiCF. MagnaniN. TurazziS. Tettamanti
Laboratorio di Terapia Genica e Cellulare“Stefano Verri”, ASST Monza Ospedale S Gerardo
G. GaipaB. CabiatiD. Belotti