Embed Size (px)
Citation preview

36
THE PATELLO-FEMORAL JOINTMethods of Diagnosis: Clinical Disorders and Their Treatmen
A. GRiAHM APLEY, F.R.C.S.Consultant Orthopaedic Surgeon, Rowley Bristow Orthopaedic Hospital, Pyrford
The knee has two joints, the tibio-femoral andthe -patello-femoral, but until recent years thesecond has received relatively little attention. Thisneglect is surprising, because the importance oflesions of the extensor mechanism, and the needfor a powerful quadriceps muscle, have long beenappreciated. This article surveys first the methodsof examination of the patello-femoral joint, thenits disorders, and finally the operation of patel-lectomy. The disorders are in two main gioups:displacements (subluxation and dislocation) anddegenerations (chondromalacia and osteoarthritis).All these conditions are linked, for recurrentdislocation and subluxation are potent causes ofchondromalacia which, in turn, is a forerunner ofosteoarthritis.
Examination of the Patello-Femoral JointWith derangement of the knee it is not sufficient
to examine only the tibio-femoral joint; thepatello-femoral joint'also must be examined inevery case. The patient lies on a couch withboth lower limbs exposed. A fixed routine ofexamination should, as always, be employed;first we look, then feel, then move the joint, andfinally examine X-ray films.
Look. The skin is inspected for scars, and theshape of the limb' observed for valgus or varusdeformity. Wasting of the thigh and swelling in;the supra-patellar pouch are easily seen. Finally,we look at the patella itself to see if it is no'rmal inposition, size and shape.
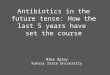
Feel. The skin is palpated for increased warmthand the supra-patellar pouch for excess fluid.When palpating for tenderness, -it is importantnot only to feel the margins of the patella, butalso to push it laterally with one hand, while thefingers of the other feel the lateral portion of itsposterior surface (Fig. i).Move. Extension, flexion and rotation of the
knee are tested, but these are mainly concernedwith tibio-femoral disorders. Two special testsinvolving patello-femoral movement are important.I have used them for a number of years and foundthem consistently helpful.
The Apprehension TestWith one hand the patella is pushed laterally,
while the other hand flexes the knee. If thepatient has recurrent dislocation or subluxation,excess lateral mobility can sometimes be demon-strated. The essence of the test is, however,that as flexion proceeds the patient is usually seento wince. The term ' apprehension test' seemsappropriate because the patient, not unreasonably,is apprehensive lest the displacement be repro-duced during the test (Fig. 2).
The Patellar Friction TestWith the knee straight the patella is moved up
and down, then from side to side; during thesemovements it should be firmly pressed against thefemur (Fig. 3). The diagnostic feature is that agrating sensation may be felt, or pain elicited, ifthe articular cartilage on the back of the patella isirregular, as. in chondromalacia or osteoarthritis.
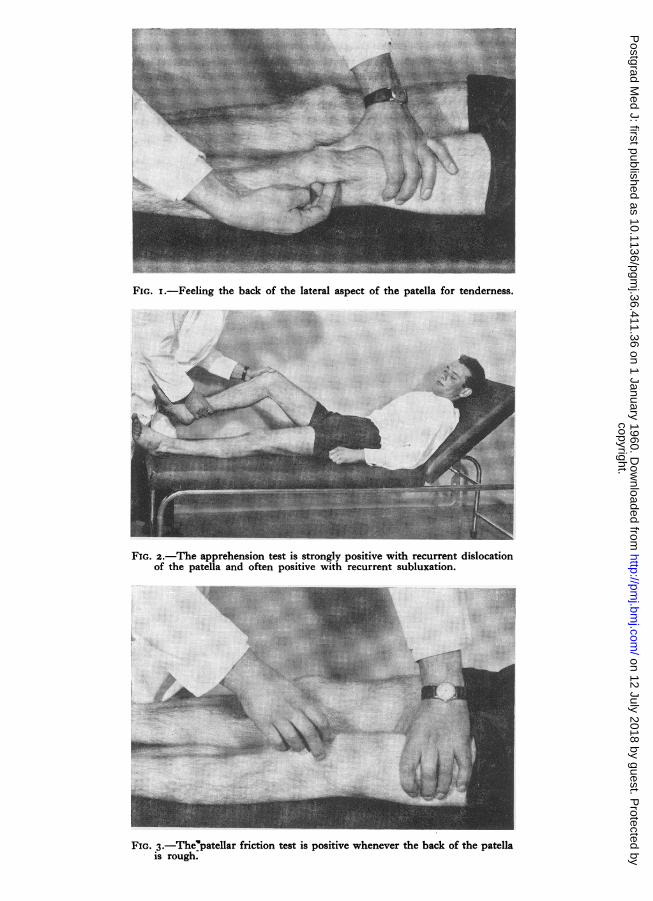
X-rayStandard antero-posterior and lateral views
of the knee are not enough, and a special projec-tion is necessary; this is known as the patello-femoral, tangential or sky-line view (Fig. 4). Inthis view the width of the joint space between thepatella and the lateral femoral condyle may beseen to be diminished, the posterior surface of thepatella may be irregular, or osteophytes may bevisible.
Recurrent Dislocation of the PatellaCausesI. MUSCLE WEAKNESSThe patella may be dislocated by a single major
injury. Uniless, after reduction, the quadricepsmuscle is redeveloped to its full power, dislocationmay recur, because wasting of the quadriceps isusually most marked in the vastus medialis, amuscle which helps prevent lateral shift of thepatella.
2. ANATOMICAL ABNORMALITIESWith genu valgum the patella is more likely to
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
aJ,
FIG. i.-Feeling the back of the lateral aspect of the patella for tenderness.
~~~~~~~.}F:.;.:::. ..e g.. ez..
... ... ..... .# .......
FIG. 2.-The apprehension test is strongly positive with recurrent dislocationof the patella and often positive with recurrent subluxation.
;mSz;.-.......
2'=V S-LFIG. 3. The'patellar friction test is positive whenever the back of the patella
is rough.
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
38 POSTGRADUATE MEDICAL JOURNAL January [960
-
a.!
*:
:.|aSrE* .:. .:. '>i}.. .:: -e wegE
FIG. 4.-The tangential or skyline view.
dislocate because the line of pull of the quadricepswhen the knee is valgus tends to displace thepatella laterally.With normal muscle dislocation of the patella
is prevented by contact with the ridge on thelateral femoral condyle. This checking mechanismfails if the ridge is poorly developed, if the patellais too small or too high, or if the knee normallyextends beyond i8o deg.
It should be emphasized that the majority ofpatients with recurrent dislocation of the patellahave no gross abnormality and the cause of thedislocation is not obvious.
PathologyDislocation is always to the lateral side. The
capsule on the medial side of the patella is tornand, if it fails to unite properly, lateral laxitypersists. Repeated dislocation damages the con-tiguous surfaces of patella and femoral condyle;degenerative changes follow which may result inflattening of the condyle, so facilitating furtherdislocations.
SymptomsThe patient complains of attacks during which
the knee suddenly gives way, moves out of posi-tion, and may get stuck. As the patella displacesto the lateral side of the lateral femoral condylethe patient may be thrown to the ground. If thepatella remains in this position the knee is stuckin acute flexion. This history is much more
dramatic than that of locking due to a tornmeniscus, with which the lesion was formerlyconfused.As a rule the patella spontaneously slips back
to its normal position; sometimes it is reducedby the patient or a bystander, and occasionally thepatient is brought to hospital with the patellastill dislocated. The first dislocation may havefollowed a definite injury; subsequent attacksoccur while walking, running or cycling, and tendto come out of the blue without warning. Betweenattacks, the knee seems normal.
SignsRecurrent Dislocation
of Patella Torn Medial Meniscus
More common in females More common in malesKnee locks acutely flexed Knee locks slightly flexedPatient thrown to the Patient sinks to the
ground groundTender above joint line Tender on the joint lineApprehension test positive Apprehension test nega-
tiveRotation painless Rotation painful
Girls in their late teens are the chief sufferers,though boys are sometimes affected and thecondition may occur in young adults. Sometimesit is bilateral.The appearance of the dislocated knee is un-
mistakable. The joint is held flexed, the patellais on the lateral side of the knee facing outwards,
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
january I960 APLEY: The Patello-Femoral Joint 39
and the uncovered medial femoral condyle con-stitutes an abnormal prominence. This pro-minence on the inner side is so obvious that thepatient may mistakenly suppose that the patellahas displaced medially. Between attacks the signsare as follows:
Look: The knee may be valgus or the quad-riceps wasted, but usually the appearance isnormal.
Feel: The patella may be too small or toohigh and, for a few days after an attack, there istenderness medial to the patella where thecapsule has been torn. If dislocation has beenrepeated the lateral portion of the posteriorsurface of the patella may be tender.Move: Flexion and extension of the knee may
be full and painless and rotation may be normal,but the patella is unduly mobile laterally andthe apprehension test is strongly positive. Thistest is reliable and almost invariably diagnostic.After repeated attacks the patellar friction testalso becomes positive, indicating that articularcartilage degeneration has occurred.X-ray: It is necessary to exclude a loose body,
but in most cases the X-ray appearance isnormal.
TreatmentThe first time a patella dislocates it must be
reduced, the joint aspirated if necessary, and theknee splinted in the straight position. A plastertube is applied from the groin to the malleoli, andthe anterior third of this plaster is removed sothat a firm backslab remains. On the next daythe patient is taught quadriceps exercises. As soonas she can easily lift her leg she is allowed up andtaking weight. Walking is encouraged, and re-peated muscle exercises insisted upon. The backslab is removed for daily exercises; after six weeksit is discarded and knee movements regained byactive exercise.
If dislocation has become recurrent operativetreatment is essential, for the patient is liable tofall while crossing a road or walking down stairs.Formerly, a number of different operations werein vogue such as elevation of the lateral femoralcondyle (Albee), or reinforcement of the medialcapsule with fascia (Gallie). These have nowbeen abandoned; instead, the patella is either re-aligned more medially or is excised.
Patellar Re-alignmentThis is indicated when only a few attacks have
occurred and there is no evidence of chondro-malacia patellae. A lateral para-patellar incisionis used and is extended distally, inclining to themedial side and ending two inches below thetibial tubercle. The patellar ligament is defined
ItI "
I II I
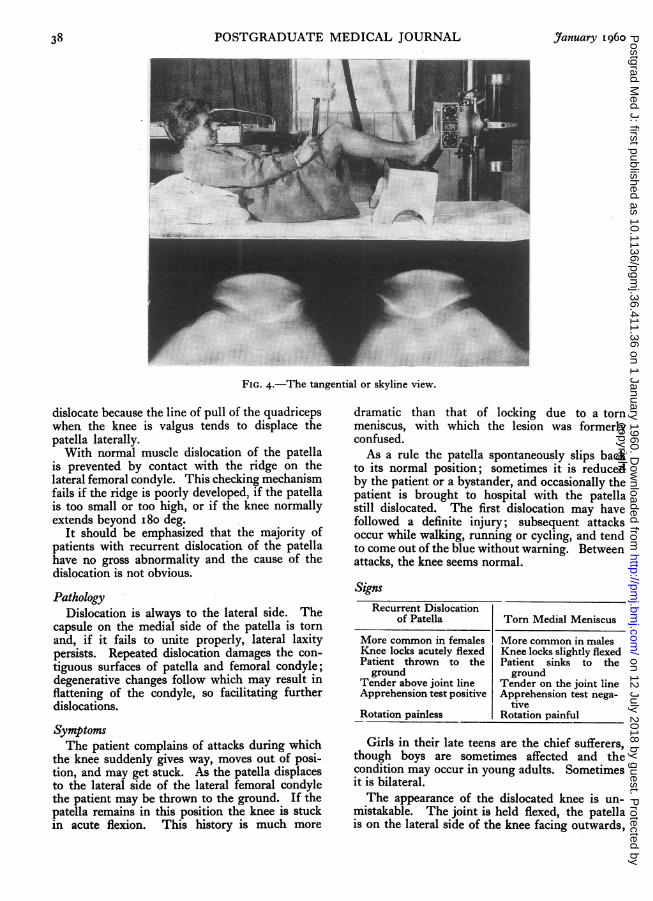
FIG. 5.-The insertion of the ligamentum patellae istransplanted distally and medially.
and detached together with a rectangular block ofbone including its insertion. The capsule lateralto the patella is then divided in the line of theincision to allow the bone to be moved mediallywithout tension. A cavity is prepared in thetibia, 3-in. medial to and below the tibial tubercle.The block of bone bearing the patellar ligamentis fitted into the cavity; it may either be latchedsecurely in position or is fastened with sutures,staples or a screw (Fig. 5). The medial capsuleis plicated, but the lateral capsule is left unsutured.A splint is worn for six weeks.
PatellectomyThis is indicated if degenerative changes have
developed on the articular cartilage of the patella.If there have been several attacks such changesare inevitable even if clinically unrecognized atfirst and McFarland (1948) advocates patellectomy
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
40 POSTGRADUATE MEDICAL JOURNAL January I960
as the routine treatment. The technique of theoperation is described later.Each of the above operations is seen to have its
own clear-cut indications; each also has its ownspecial complication. Following re-alignment,chondromalacia, which- was perhaps too early tohave been recognized previously, may progress.Following patellectomy, the patellar tendon andligament may dislocate in the same way as thepatella, though this complication is rare. Thetreatment of advancing chondromalacia is patel-lectomy; the treatment of recurrent ligamentdislocation is re-alignment. It is therefore seenthat either of the two operations may occasionallyneed to be followed by the other.
Recurrent Subluxation of the PatellaThe patient, usually a young girl, complains
of repeated giving way of the knee, of momentarycatches of pain, and sometimes of recurrentswelling. The patella moves laterally, teeters onthe femoral condyle and instead of displacingcompletely it returns to its normal position. Ifthe patient is asked to describe the very firsttime the knee gave trouble (a question whichshould never be omitted with any knee derange-ment) sometimes she may recall a completedislocation.The history is less dramatic than that of re-
current dislocation, but the condition is morecommon and is more often mis-diagnosed as atorn meniscus. The absence of the characteristichistory and signs of a torn meniscus, together witha positive apprehension test, should enable anaccurate diagnosis to be made. Chondromalaciaeventually supervenes and the treatment ispatellectomy.
Chondromalacia PatellaeCauseThis important condition was first described in
Scandinavia (Owre, 1935). The articular cartilageof the patella, which is normally much thickerthan that of the femoral condyle, is very liable tobe damaged by repeated minor falls on to theknee-cap or by a single major injury. Thecartilage may also be damaged by recurrent sub-luxation or dislocation as already described.
PathologyThe articular cartilage loses its normal smooth
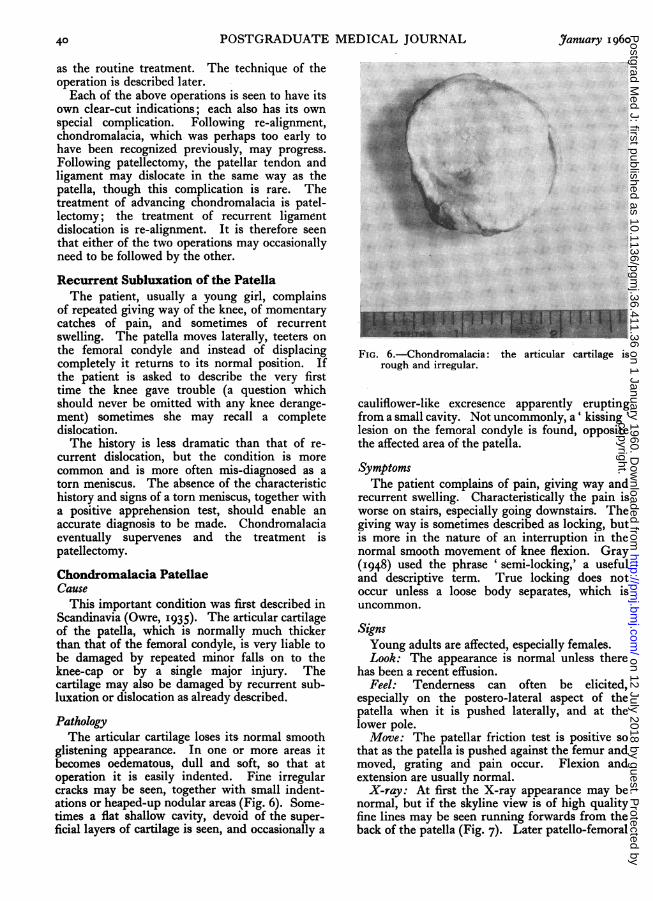
glistening appearance. In one or more areas itbecomes oedematous, dull and soft, so that atoperation it is easily indented. Fine irregularcracks may be seen, together with small indent-ations or heaped-up nodular areas (Fig. 6). Some-times a flat shallow cavity, devoid of the super-ficial layers of cartilage is seen, and occasionally a
...:... ..S> 4.. ........ ....4: ...
.:........ ., ..
0g r
... ....
...
FIG. 6.-Chondromalacia: the articular cartilage isrough and irregular.
cauliflower-like excresence apparently eruptingfrom a small cavity. Not uncommonly, a' kissing 'lesion on the femoral condyle is found, oppositethe affected area of the patella.
SymptomsThe patient complains of pain, giving way and
recurrent swelling. Characteristically the pain isworse on stairs, especially going downstairs. Thegiving way is sometimes described as locking, butis more in the nature of an interruption in thenormal smooth movement of knee flexion. Gray(I948) used the phrase ' semi-locking,' a usefuland descriptive term. True locking does notoccur unless a loose body separates, which isuncommon.
SignsYoung adults are affected, especially females.Look: The appearance is normal unless there
has been a recent effusion.Feel: Tenderness can often be elicited,
especially on the postero-lateral aspect of thepatella when it is pushed laterally, and at thelower pole.Move: The patellar friction test is positive so
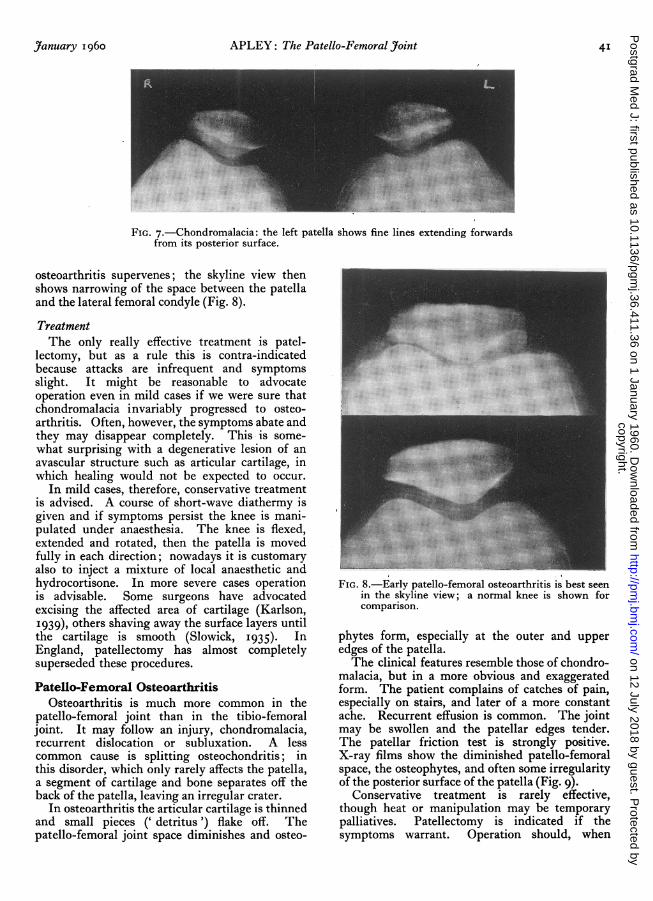
that as the patella is pushed against the femur andmoved, grating and pain occur. Flexion andextension are usually normal.X-ray: At first the X-ray appearance may be
normal, but if the skyline view is of high qualityfine lines may be seen running forwards from theback of the patella (Fig. 7). Later patello-femoral
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
Yanuary I960 APLEY: The Patello-Femoral Yoint 4I
FIG. 7.-Chondromalacia: the left patella shows fine lines extending forwardsfrom its posterior surface.
osteoarthritis supervenes; the skyline view thenshows narrowing of the space between the patellaand the lateral femoral condyle (Fig. 8).
TreatmentThe only really effective treatment is patel-
lectomy, but as a rule this is contra-indicatedbecause attacks are infrequent and symptomsslight. It might be reasonable to advocateoperation even in mild cases if we were sure thatchondromalacia invariably progressed to osteo-arthritis. Often, however, the symptoms abate andthey may disappear completely. This is some-what surprising with a degenerative lesion of anavascular structure such as articular cartilage, inwhich healing would not be expected to occur.
In mild cases, therefore, conservative treatmentis advised. A course of short-wave diathermy isgiven and if symptoms persist the knee is mani-pulated under anaesthesia. The knee is flexed,extended and rotated, then the patella is movedfully in each direction; nowadays it is customaryalso to inject a mixture of local anaesthetic andhydrocortisone. In more severe cases operationis advisable. Some surgeons have advocatedexcising the affected area of cartilage (Karlson,I939), others shaving away the surface layers untilthe cartilage is smooth (Slowick, I935). InEngland, patellectomy has almost completelysuperseded these procedures.
Patello-Femoral OsteoarthritisOsteoarthritis is much more common in the
patello-femoral joint than in the tibio-femoraljoint. It may follow an injury, chondromalacia,recurrent dislocation or subluxation. A lesscommon cause is splitting osteochondritis; inthis disorder, which only rarely affects the patella,a segment of cartilage and bone separates off theback of the patella, leaving an irregular crater.
In osteoarthritis the articular cartilage is thinnedand small pieces (' detritus') flake off. Thepatello-femoral joint space diminishes and osteo-
FIG. 8.-Early patello-femoral osteoarthritis is best seenin the skyline view; a normal knee is shown forcomparison.
phytes form, especially at the outer and upperedges of the patella.The clinical features resemble those of chondro-
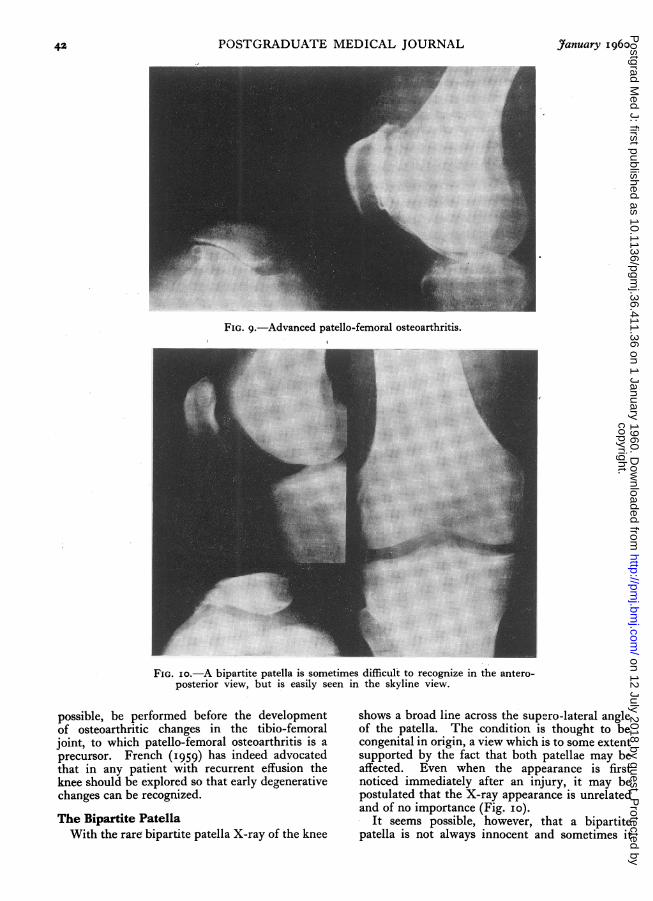
malacia, but in a more obvious and exaggeratedform. The patient complains of catches of pain,especially on stairs, and later of a more constantache. Recurrent effusion is common. The jointmay be swollen and the patellar edges tender.The patellar friction test is strongly positive.X-ray films show the diminished patello-femoralspace, the osteophytes, and often some irregularityof the posterior surface of the patella (Fig. 9).
Conservative treatment is rarely effective,though heat or manipulation may be temporarypalliatives. Patellectomy is indicated if thesymptoms warrant. Operation should, when
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
42 POSTGRADUATE MEDICAL JOURNAL January i960
A
FIG. 9.-Advanced patello-femoral osteoarthritis.
FIG. io.-A bipartite patella is sometimes difficult to recognize in the antero-posterior view, but is easily seen in the skyline view.
possible, be performed before the developmentof osteoarthritic changes in the tibio-femoraljoint, to which patello-femoral osteoarthritis is aprecursor. French (1959) has indeed advocatedthat in any patient with recurrent effusion theknee should be explored so that early degenerativechanges can be recognized.
The Bipartite PatellaWith the rare bipartite patella X-ray of the knee
shows a broad line across the supero-lateral angleof the patella. The condition is thought to becongenital in origin, a view which is to some extentsupported by the fact that both patellae may beaffected. Even when the appearance is firstnoticed immediately after an injury, it may bepostulated that the X-ray appearance is unrelatedand of no importance (Fig. io).
It seems possible, however, that a bipartitepatella is not always innocent and sometimes it
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
January I960 APLEY: The Patello-FemoralJoint 43
may produce patello-femoral symptoms and signs.The patient presents with symptoms resemblingthose of chondromalacia. The ' crack' may bepalpable on its anterior surface, the supero-lateral angle of the back of the patella may betender and the patellar friction test is usuallypositive. In the few cases in which symptomshave merited operation I have found a ' step'between the two portions of the patella, andthrough a short incision have removed the smallersupero-lateral portion. This limited procedureappears to have relieved the symptoms completely.
PatellectomyA knee without a patella can be, in all other
respects, a normal knee (Brooke, 1937). In thepreceding pages various indications for patel-lectomy have been described; the operation isalso indicated in transverse gap fractures of thepatella and in those stellate fractures where theposterior surface of the bone is irregular. It mustbe emphasized that an essential feature of theoperation is repair of the extensor mechanism.Unless the patellar tendon and ligament are firmlyjoined together, active knee extension will belimited and the knee will inevitably give way. Tobe stable a knee must have no ' lag' in extension;the term ' lag' is used to mean that when thepatient has actively straightened the knee, furtherpassive extension is still possible.
TechniqueA tourniquet is necessary, but, unless it is
applied while the knee is held flexed, it will sub-sequently be difficult or impossible to pull thepatellar tendon down sufficiently for adequatesuture.The operation itself is performed with the knee
straight. A transverse incision is best, for theskin creases are transverse and the resulting scaris scarcely visible. If, however, the diagnosis isin doubt and it is not certain that patellectomy willprove necessary, a vertical para-patellar incisionis used, for this gives better exposure of the joint.The skin is reflected and the ligamentous fibres
on the front of the patella are incised verticallyand dissected off the bone. These fibres, which arefirmly attached, must be meticulously scraped offwith a sharp scalpel, so that not a scrap of softtissue is left on the bone. One corner of thepatella is then lifted up and dissected free. Thiscorner is then held in strong forceps and pulledforwards so that the remainder of the bone maybe shelled out, the knife always cutting as closeto the bone edge as possible. The interior of thejoint and the femoral condyles are then inspected.The deep layer of the extensor apparatus is
repaired with mattress sutures of strong chromic
..* :.. .........
.:.. ...i::.....g.
...
.~.:....
*.. .......:
[ ~ ~ ~~ ~ ~ ~~~:.......:!i Ge:.::;.: ..
.'.:.:::: ::..:.: ;. :. : : :
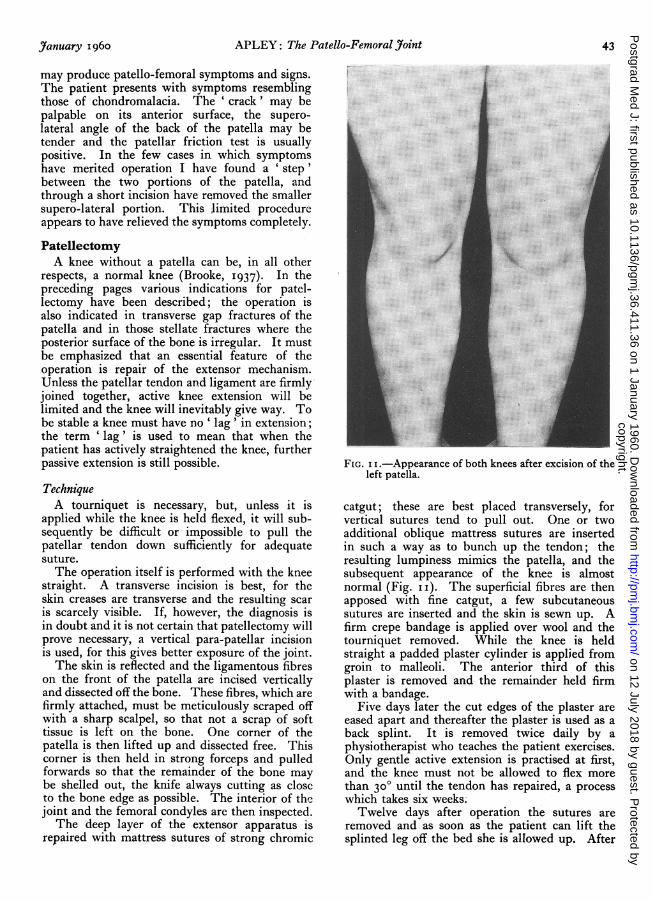
FIG. i I.-Appearance of both knees after excision of theleft patella.
catgut; these are best placed transversely, forvertical sutures tend to pull out. One or twoadditional oblique mattress sutures are insertedin such a way as to bunch up the tendon; theresulting lumpiness mimics the patella, and thesubsequent appearance of the knee is almostnormal (Fig. ii). The superficial fibres are thenapposed with fine catgut, a few subcutaneoussutures are inserted and the skin is sewn up. Afirm crepe bandage is applied over wool and thetourniquet removed. While the knee is heldstraight a padded plaster cylinder is applied fromgroin to malleoli. The anterior third of thisplaster is removed and the remainder held firmwith a bandage.
Five days later the cut edges of the plaster areeased apart and thereafter the plaster is used as aback splint. It is removed twice daily by aphysiotherapist who teaches the patient exercises.Only gentle active extension is practised at first,and the knee must not be allowed to flex morethan 300 until the tendon has repaired, a processwhich takes six weeks.Twelve days after operation the sutures are
removed and as soon as the patient can lift thesplinted leg off the bed she is allowed up. After
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL January I960
six weeks the splint is left off at night and forperiods during the day when the patient is nottaking weight. Vigorous extension exercises arenow practised and active flexion encouraged. Thesplint is not finally discarded until the patient hasregained powerful quadriceps and has no trace oflag in extension.
AcknowledgmentsI would like to thank Mr. G. Hadfield, F.R.C.S.,
for his help in preparing this article, and Mr. K.
Fensom of the Department of Clinical Photo-graphy for the illustrations.
REFERENCESBROOKE, R. (1937), Brit. J. Surg., 24, 733.FRENCH, P. R. (I959), Paper read at Brit. Orth. Ass., October
'959.GRAY, C. (I948), Brit. med. 7., 1, 427.KARLSON, S. (I939), Acta chir. scand., 83, 347.McFARLAND, B. (I948),J. Bone yt. Surg., 30b, i58.OWRE, A. (I936), Acta chir. scand., 77, Supp. 41.SLOWICK, F. A. (I935), New Engql. Y. Med., 213, I6o.
RENAL DISEASE(Postgraduate Medical Journal, November 1959)
Price 6s. 6d. post free
RECENT DEVELOPMENTS IN THE STUDY HAEMODIALYSISOF THIE KID)NEY 'OF THEKIDNEYF. M. Parsons, B.Sc., M.B., Ch.B.A. A. G. Lewis, B.Sc., M.D., M.R.C.P. F M P
RENAL BIOPSY AND DIURETICSGLOMERULONEPHRITIS H. G. Lloyd-Thomas, M.A., M.B., M.R.C.P.J. H. Ross, M.D., M.R.C.P.
RECENT ADVANCES IN THE TlREATMENT URINARY DIVERSIONOF RENAL DISEASE John Hopewell, F.R.C.S.A. G. Spencer, M.D., M.R.C.P.
AORTOGRAPHY RENAL ARTERY STENOSISI. H. Griffiths, F.R.C.S. Kenneth Owen, M.S., F.R.C.S.
Published byTIE FE:LLOWSHIP OF POSTGRADUATE MEDICINE
60, Portland Place, London, W.1
copyright. on 12 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.411.36 on 1 January 1960. Dow
nloaded from