Embed Size (px)
Citation preview

114
Combination Treatment of EnalaprilWith Nitrendipine in Rats
With Renovascular Hypertension
Ulrich Otto Wenzel, Udo Helmchen, Wilhelm Schoeppe, Gerd Schwietzer
Abstract We have recently shown that treatment with thecalcium channel blocker nitrendipine may aggravate albumin-uria and glomerular injury in rats with two-kidney, one cliprenovascular hypertension if arterial blood pressure is notreduced. To test whether nitrendipine also exerts its adverserenal effects when normotension is achieved, we examined theeffect of combined therapy with nitrendipine and the convert-ing enzyme inhibitor enalapril on blood pressure, albuminuria,glomerular filtration rate, and morphology of the nonclippedkidney. Rats treated with enalapril alone or in combinationwith the diuretic hydrochlorothiazide or rats treated withnitrendipine alone served as controls. Therapy was started 6weeks after clipping of one renal artery. Nitrendipine alonedid not reduce blood pressure but significantly increasedalbuminuria, diuresis, glomerular filtration rate, and glomeru-lar volume and injury compared with untreated hypertensivecontrols. Increase of glomerular filtration rate, diuresis, andalbuminuria was reversible after withdrawal of nitrendipine.
Treatment with enalapril alone decreased blood pressuresignificantly but not to normotensive levels and was withoutsignificant effect on albuminuria and glomerular morphology.The combination of nitrendipine and enalapril reduced bloodpressure to normotensive levels and not only prevented theincrease of glomerular volume, glomerular filtration rate,diuresis, and albuminuria caused by nitrendipine alone butfurthermore improved glomerular injury and albuminuria tolevels not significantly different from normotensive controls.Enalapril in combination with the diuretic had similar benefi-cial effects on blood pressure, albuminuria, and glomerularinjury. These data demonstrate that the adverse effects ofnitrendipine monotherapy on glomerular structure and func-tion can be prevented by the combination of nitrendipine andenalapril when blood pressure is normalized. (Hypertension.1994^3:114-122.)
Key Words • nitrendipine • enalapril • hypertension,renovascular • albuminuria
In rats with renovascular hypertension, we haverecently shown that treatment with the calciumchannel blocker (CCB) nitrendipine increases al-
buminuria and glomerular hypertrophy and sclerosiscompared with untreated hypertensive control animals.1
However, in those studies nitrendipine did not normal-ize blood pressure. Nitrendipine could have acceleratedthe progression of glomerular injury by preglomerulardilatation, which in the absence of blood pressurereduction results in a rise of glomerular capillary pres-sure. The converting enzyme inhibitor (CEI) enalaprillowered blood pressure, albeit not to normal levels, anddid not influence albuminuria and glomerular sclerosis.1
Clinical studies suggest that the combination of CCBand CEI may be superior in decreasing proteinuriacompared with the respective monotherapy.2 Despitethe evidence for a beneficial effect of this combinationon blood pressure37 and proteinuria2 in hypertensivepatients, there are no data as to the effect of CCB plus
Received April 12, 1993; accepted in revised form October 4,1993.
From the Department of Medicine, University of Frankfurt/Main (U.O.W., W.S., G.S.), and the Department of Pathology,University of Hamburg (U.H.) (Germany).
Parts of this study were presented at the Annual Meeting of theAmerican Society of Nephrology, Baltimore, Md, 1992, and pub-lished in abstract form (7 Am Soc NephroL 1992^3:754).
Correspondence to U.O. Wenzel, MD, University of TexasHealth Science Center at San Antonio, Department of Medicine,Division of Nephrology, 7703 Floyd Curl Dr, San Antonio, TX78284-7882.
CEI therapy on renal parameters in rats with experi-mental renal disease.
Therefore, the aim of the present study was toinvestigate whether the adverse renal effects of nitren-dipine could be prevented by normalization of bloodpressure with combined CCB and CEI therapy. Inaddition, we compared the effect of combined CCB andCEI therapy with a combination of CEI and the diuretichydrochlorothiazide, which also lowered blood pressureto normotensive levels in this model. The reversibility ofthe adverse effects of nitrendipine was tested by with-drawal of the CCB after 6 weeks of therapy. Finally, weexamined whether nitrendipine also exerts its adverseeffects on renal function and structure when given tonormotensive rats.
Methods
Animals and ProtocolStudies were performed in male Sprague-Dawley rats (Savo,
Kisslegg, Germany) that had free access to tap water andstandard rat chow (Sniff, Germany, containing 21% protein,0.25% sodium, and 1% potassium). In rats weighing 120 to 140g, two-kidney, one clip hypertension was induced. For thispurpose, a rigid U-shaped silver clip (0.23 to 0.25 mm internaldiameter) was placed around the right renal artery through aloin incision while the rat was under ketamine/xylazin anes-thesia (Parke-Davis/Bayer, Berlin/Leverkusen, Germany;100/10 mg/kg IM). The nonclipped kidney remained undis-turbed. In sham-operated control rats, the same procedurewas performed without application of a clip.
After 6 weeks without treatment, only hypertensive animalswith systolic blood pressure (SBP) exceeding 165 mm Hg were
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Wenzel et al Nitrendipine and Enalapril in Renovascular Hypertension 115
randomly divided into seven groups: (1) untreated hyperten-sive rats (HC, n=18), (2) untreated normotensive rats (NC,n=10), (3) rats treated with enalapril (100 mg/L drinkingwater, n=9; Merck Sharp & Dohme, Munich, Germany), (4)rats treated with nitrendipine (1 mg/g diet, n=12; Bayer,Leverkusen, Germany), (5) rats treated with enalapril andnitrendipine (ENP+NIT) (same dosage as in monotherapy,n=12), (6) rats treated with enalapril and hydrochlorothiazide(ENP+HCTZ) (enalapril same dosage as in monotherapy;hydrochlorothiazide, 50 mg/L drinking water, n=12; Sigma,Deisenhofen, Germany), and (7) 7 days withdrawal of nitren-dipine after 6 weeks therapy with nitrendipine (PNIT, n=9).
Normotensive control animals gained slightly more weightthan hypertensive animals with or without therapy, so NC ratswere food-restricted for 1 or 2 days per week.
In a pilot study we tested whether further blood pressurereduction could be achieved by the combination of nitren-dipine and hydrochlorothiazide (nitrendipine, 1 mg/g food;hydrochlorothiazide, 50 mg/L drinking water, n=6). As hasbeen shown in humans,8 the blood pressure-lowering effect ofthis combination was not significantly different from ratstreated with nitrendipine alone (data not shown).
In addition, we tested whether nitrendipine exerts an effecton renal function and structure of normotensive animals aswas observed in hypertensive animals. Therefore, normoten-sive rats without clip operation were housed for 6 weeks beforebeing treated for 6 weeks with nitrendipine (1 mg/g food,n=6). The protocol and study design were identical to the restof the study. Because normotensive animals treated withnitrendipine gained more body weight, an additional group ofcontrols without food restriction (n=6) was studied for com-parison with the nitrendipine-treated normotensive rats.
Before and during the treatment period, SBP was mea-sured by tail-cuff plethysmography in awake rats. Animalswere placed in individual metabolic cages (Ebeco, CastropRauxel, Germany), and 24-hour urine collections were madefor determination of albuminuria. Albumin concentrationswere measured by nephelometry (Beckman, Munich, Ger-many) using a rabbit anti-rat albumin antibody (CappelLaboratories).
Renal FunctionSix weeks after therapy, rats were anesthetized with thio-
pental (50 mg/kg IP) and placed on a heated operating table.A tracheostomy was performed, and polyethylene catheterswere inserted into the right jugular vein and the ureter of thenonclipped kidney for solute infusion and sample collection. Acannula in the left carotid artery connected to a pressuretransducer (Statham 23Db, Statham Laboratories, Hato Rey,Puerto Rico) allowed measurement of arterial blood pressureand collection of blood.
For replacement of fluid losses associated with anesthesiaand surgery, animals received isoncotic albumin infusion with1 mL/100 g body wt over 30 minutes. A bolus (0.2 mL/100 gbody wt in 10 minutes) of a solution containing 3% inulin in5% glucose was given, followed by an infusion rate of 0.6mL/100 g per hour for a 60-minute control period to reachconstant urine flow. Thereafter, two 30-minute clearanceperiods followed. Urine was collected from the left ureter inpreweighed tubes, and urine volume was determined gravimet-rically. Blood was collected in the middle of each clearanceperiod for determination of inulin concentration, which wasmeasured by anthrone reaction according to Fuhr et al.9
Renal MorphologyAt the end of the clearance periods, kidneys were removed
and weighed. Kidney slices were fixed in 4% buffered Forma-lin, embedded in paraffin, cut in 3- to 4-^im-thick sections, andstained with periodic acid-Schiff.
Histological studies were performed in a blind fashion.Glomerular injury was assessed by a semiquantitative score
(grade 0 to 4) using the method of Raij and Olson as describedearlier.1 Grade 1 represents involvement of up to 25% of theglomerulus, and grade 4 represents injury of 75% to 100% ofthe glomerulus. The number of glomeruli with a score of 1 wasmultiplied by 1, with a score of 2 by 2, 3 by 3, and 4 by 4. Thesenumbers were summed and divided by the number of glomer-uli assessed, including those with a score of zero.
Planimetric examinations of cross-sectional area were per-formed by means of a Zeiss drawing tube in combination witha semiautomatic interactive image-analysis system (Mor-phomat 30, Zeiss, Oberkochen, Germany). Using a serpentinemovement from cortex to medulla and vice versa, the outlinesof 50 consecutively encountered capillary tufts were tracedmanually, and the mean glomerular random cross-sectionalarea (AG) was determined. The average glomerular tuftvolume (VG) was then calculated according to Weibel10 asVG=(/3/k)(AG)3/2, where 0=1.38 and k=l . l and are shapeand size distribution coefficients, respectively.
In addition, the amount of tubulointerstitial damage of theclipped kidney (tubular atrophy and dilatation, interstitialfibrosis) was estimated by examining six fields (magnificationx 100) and semiquantitatively grading the degree of damage ineach field using a scale of 0 to 4+. The mean of six determi-nations was calculated as an index in each tissue specimen. Notubulointerstitial abnormalities were found in normotensivecontrols. Therefore, statistical analysis was not performed inthis group.
The guidelines of the American Physiological Society forexperimental animal research were followed, and approval wasobtained from the animal care committee at the University ofFrankfurt.
Statistical AnalysisData are presented as mean±SEM. Statistical analysis was
performed with the Mann-Whitney-Wilcoxon test. In addition,the Kruskal-Wallis test was performed as a screening test, ifappropriate. Values of P<.05 were considered significant.
ResultsBlood Pressure
The time course for changes in SBP before andduring therapy is shown in Fig 1. At the time ofrandomization, SBP with renal artery stenosis was in-creased to 190±3 versus 114±4 mm Hg in sham-oper-ated controls. After 6 weeks of therapy, enalapril low-ered blood pressure significantly to 142±6 mm Hg, butnot to normotensive control values (117±5 mm Hg). Incontrast, there was no significant decrease of bloodpressure after nitrendipine treatment (175±4 mmHg)compared with HC rats (189±8 mm Hg). ENP+NITand ENP+HCTZ decreased blood pressure to 118±3and 115 ±2 mm Hg, respectively, which was not signifi-cantly different from NC rats. Seven days after with-drawal of nitrendipine, blood pressure was 170 ±7mm Hg, which was not significantly different from theHC rats or nitrendipine-treated group.
Diuresis
As shown in Fig 2, urinary output throughout thecourse of therapy was significantly higher in nitrendipine-treated animals compared with all other groups. Al-though in the second and fourth weeks of therapy urinaryoutput in rats treated with enalapril, ENP+NIT, andENP+HCTZ was significantly increased compared withHC rats, during the sixth week, no significant differencewas found. Urinary output of NC and HC rats was notsignificantly different. Seven days after withdrawal ofnitrendipine, urinary output decreased to 17±2 mL/24 h,
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

116 Hypertension Vol 23, No 1 January 1994
200
180
160
140
120
100
hypertensivecontrols
nitrendipine
enalapril * / +
nitrendipine+enalapril * *
normotensive controls• •
enalapril+hydro-chlorothiazide
10 12 weeks
Therapy
FIG 1. Line graph shows time course of systolic blood pressure measured in conscious rats before and during therapy. *P<.005,**P<.001 vs hypertensive controls; +P<.0025 vs normotensive controls and nitrendipine+enalapril; P<.001 vs enalapril+hydrochlorothlazide.
which differed significantly from the nitrendipine-treatedgroup during the sixth week of therapy (P<.001) but wasnot significantly different from the HC group.
Albumin Excretion
Albumin excretion is depicted in Fig 3. After 6weeks of therapy, albuminuria in the nitrendipine-
80
60
40
20
0
f̂ ———;
*
•
^ ^
• ,
nitrendipine+enalapril
1
. #
normotensivecontrols
nitrendipine
enalapril+hydro-chlorothiazide
; enalapril
hypertensivecontrols
10 12 weeks
Therapy
FIG 2. Line graph shows time course depicting urine output before and during therapy. *P<.001 vs all other groups; #P<.05 vsenalapril, nitrendipine+enalapril, and enalapril+hydrochlorothiazlde.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Wenzel et al Nitrendipine and Enalapnl in Renovascular Hypertension 117
40
30
NC HC ENP NTT NTT ENP POTT+ENP +HCTZ
FIG 3. Bar graph shows albumin excretion of various groups after6 weeks of treatment NC indicates normotensive controls; HC,hypertensive controls; ENP, enalapril-treated group; NIT, nitren-dipine-treated group; NIT+ENP, nltrendipine+enalapril-treatedgroup; ENP+HCTZ, enalapril+hydrochlorothlazide-treated group;and PNIT, animals 7 days after withdrawal of nitrendipine. *P< .005,"P<.001 vs HC; +P<.01, + +P<.005 vs ENP.
treated rats increased significantly (f<.005) comparedwith HC rats. There was a numerical decrease ofalbuminuria after enalapril treatment; however, thisdifference was not statistically significant comparedwith HC rats. The combination of nitrendipine andenalapril not only prevented the increase of albumin-uria seen after nitrendipine alone but also decreasedalbuminuria significantly more than enalapril alone(P<.001 versus HC rats). A similar significant de-crease of albuminuria was found with the combinationtherapy of ENP+HCTZ. Albuminuria of animalstreated with ENP+NIT and ENP+HCTZ was notsignificantly different from normotensive controls butwas significantly lower than enalapril alone. Sevendays after withdrawal of nitrendipine, albuminuriasignificantly decreased compared with the nitren-dipine group during the sixth week of therapy and wasno longer significantly different from HC rats.
Glomerular Filtration RateAs shown in Fig 4, glomerular filtration rate (GFR)
factored by kidney weight was significantly higher innitrendipine-treated rats (1.97±0.28 mL/min per gramkidney weight) than in HC rats (1.22±0.17 mL/min pergram). The combination of nitrendipine and enalaprilsignificantly prevented this increase (1.7±0.29 mL/minper gram, not significant versus HC rats). No signifi-cant difference existed between HC rats and ratstreated with enalapril (1.07±0.17 mL/min per gram)or ENP+HCTZ (1.5±0.17 mL/min per gram). Afterwithdrawal of nitrendipine, GFR in these rats wasnumerically lower (0.91±0.12 mL/min per gram) thanin HC rats; however, this difference was not signifi-cant. GFR of the enalapril-treated group (P<.05) andafter withdrawal of nitrendipine (PNIT, P<.005) wassignificantly lower than in NC rats. When GFR wasnot factored by kidney weight, this difference was nolonger significant between the enalapril-treated group(2.03+0.23 mL/min) and NC rats (2.0±0.20 mL/min)but was still significant (P<.05) between PNIT(1.50±0.16 mL/min) and NC rats. When GFR was notfactored for kidney weight, the values were for HC
NC HC ENP NTT NTT ENP PNTT+ENP +HCTZ
FIG 4. Bar graph shows glomerular filtration rate factored bykidney weight of nonclipped kidney after 6 weeks of treatment.KW indicates kidney weight; NC, normotensive controls; HC,hypertensive controls; ENP, enalapril-treated group; NIT, nitren-dipine-treated group; NIT+ENP, nitrendipine+enaiapril-treatedgroup; ENP+HCTZ, enalapril+hydrochlorothiazide-treatedgroup; and PNIT, animals 7 days after withdrawal of nitrendipine.*P<.05 vs HC; #P<.005, $P<.05 vs NC.
rats, 1.93±0.17; nitrendipine-treated rats, 3.88±0.52;ENP+NIT-treated rats, 2.89±0.35; and ENP+HCTZ-treated rats, 2.54±0.22 mL/min. The significance ofthe differences remained the same regardless ofwhether GFR data were factored by kidney weight.
Glomerular Morphology, Nonclipped KidneyThe effects of the different drugs on glomerular
injury were similar to their effects on albuminuria. Asshown in Fig 5, glomerular injury in HC rats wassignificantly higher compared with NC rats. Nitren-dipine significantly increased glomerular lesions com-pared with HC rats, which persisted after withdrawalof nitrendipine. ENP+NIT not only significantly pre-vented the increase of glomerular injury but alsodecreased glomerular injury significantly comparedwith HC rats. Representative glomeruli with segmen-tal injury from a nitrendipine-treated animal are
HC ENP NIT NTT ENP PNTT+ENP +HCTZ
FIG 5. Bar graph shows glomerular injury score of nonclipped(left) kidney in various groups. NC indicates normotensivecontrols; HC, hypertensive controls; ENP, enalapril-treatedgroup; NIT, nitrendipine-treated group; NIT+ENP, nttren-dipine+enalapriWreated group; ENP+HCTZ, enalapril+hydro-chlorotriiazide-treated group; and PNIT, animals 7 days afterwithdrawal of nitrendipine. *P<.05, "P<.001 vs HC; +P<.05,
1, + ++P<.005 vs ENP; #P<.001 vs NIT.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

118 Hypertension Vol 23, No 1 January 1994
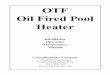
FIG 6. Top: Light micrograph of renal cortex shows two gkxner-ull with segmental glomerular Injury from rat receiving nitren-dlpine. Bottom: Photomicrograph shows two gkxneruli withoutnoticeable glomerular changes from rat receiving nitrendlpineand enalapril (periodic acid-Schiff stain).
shown in Fig 6, top, and glomeruli without noticeablestructural changes from a rat receiving ENP+NIT inFig 6, bottom. Enalapril did not influence glomerularchanges, whereas injury was decreased significantly inthe ENP+HCTZ-treated group compared with HCrats. Glomerular injury was not significantly differentbetween ENP+NIT- and ENP+HCTZ-treated rats,but both groups had significantly less glomerular in-jury than enalapril alone.
Glomerular volume of HC rats (1.14±0.06 iirrfxlO6)was significantly increased compared with NC rats(0.95±0.04 ^m3xl06) (Fig 7). Glomerular volume wassignificantly higher (P<.005) in the nitrendipine-treatedgroup (1.63±0.12 ^m'xlO6) compared with HC rats.This increase persisted after withdrawal of nitrendipine(1.45±0.04 /i,m3xl06). The combination of enalapriland nitrendipine prevented the increase of glomerularvolume significantly (1.16±0.07 /xm3xl06, P<.01) com-pared with nitrendipine-treated rats or the PNIT groupand was not significantly different from the HC group.
General CharacteristicsThere were no differences among the groups with
regard to body weight (Table 1). Weights of thenonclipped kidneys of all treated and untreated hyper-tensive groups were significantly higher compared withNC rats, and no significant differences existed amongthe treatment groups. Weights of the clipped kidneyswere significantly lower in the nitrendipine andENP+HCTZ groups and after withdrawal of nitren-
I
NC HC ENP NTT NTT ENP PNIT+ENP +HCTZ
Fra 7. Bar graph shows glomerular volume of nonclipped (left)kidney. NC Indicates normotensive controls; HC, hypertensivecontrols; ENP, enalapril-treated group; NIT, nitrendipine-treatedgroup; NIT+ENP, nltrendlpine + enalapril-treated group;ENP+HCTZ, enalapril+hydrochlorothlazide-treated group; andPNIT, animals 7 days after withdrawal of nitrendipine. *P<.05 vsENP, P<.025 vs ENP+HCTZ, P<.01 vs NIT+ENP, and P<.005vs HC; **P<.025 vs ENP, P<.01 vs NIT+ENP and ENP+HCTZ,and P<.0025 vs HC; #P<.05 vs HC; P<.025 vs ENP, NIT+ENP,and ENP+HCTZ; and P<.001 vs NIT and PNIT.
dipine compared with NC rats. There was also asignificant difference between the ENP + HCTZ-treated group and HC rats.
Morphology, Clipped KidneyTable 2 shows morphological data of the clipped
kidney. In the clipped kidney of HC and nitrendipine-treated rats, only few focal areas of tubular atrophy withaccompanying moderate interstitial fibrosis and infiltra-tion by mononuclear cells were found. In contrast, theclipped kidney of rats treated with enalapril, ENP+NIT,and ENP+HCTZ showed prominent and diffuse atrophyof tubules with flattened epithelium and widened orcystically dilated lumina occasionally containing eosino-philic hyaline casts. The interstitium was widened, fi-brotic, and infiltrated. Periglomerular fibrosis and occa-sionally glomerular collapse were found. These findingsare consistent with earlier reports of the effect of chronicCEI therapy on the clipped kidney in rats with renovas-cular hypertension.11-13 No significant differences werefound between HC rats and the treatment groups forglomerular volume of the clipped kidneys. The glomeru-lar volume of the clipped kidney in the ENP+HCTZ-treated group was significantly lower than in the nitren-dipine-treated group (P<.001).
Nitrendipine in Normotensive ControlsAs shown in Table 3, no significant differences were
found between normotensive rats treated with nitren-dipine for 6 weeks and their controls for body weight,kidney weight, glomerular injury, glomerular volume,GFR, blood pressure, and albuminuria (6 weeks oftherapy). However, nitrendipine significantly increasedurinary output.
DiscussionThis study demonstrates that the combination of
nitrendipine and enalapril prevents the adverse effectsof nitrendipine monotherapy on glomerular function
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Wenzel et al Nitrendipine and Enalapril in Renovascular Hypertension 119
TABLE 1. General Characteristics of Study Groups
Group
Normotensive controls
Hypertensive controls
Nitrendipine
Enalapril
Nitrendlplne+enalapril
Enalapril+hydrochlorothlazlde
Nitrendipine (withdrawal)
Body Weight, g
417±16
442±16
400±10
440±15
426±14
415±11
431±14
Kidney
Right
1.26±0.05
1.19±0.04
1.06±0.04t
1.16±0.07
1.10±0.09
1.01±0.08t§
1.08±0.03t
Weight, g
Left
1.20±0.04*
1.65±0.08
1.88±0.10
1.94±0.14
1.82±0.12
1.73 ±0.04
1.68±0.05
Withdrawal indicates animals 7 days after withdrawal of nitrendipine.*P<.0025 vs hypertensive controls, P<.001 vs all other groups.tP<.05, tP<.001 vs normotensive controls.§P<.05 vs hypertensive controls.
and structure in rats with hypertension-induced kidneydisease. This combination was also superior to enalaprilalone in reducing blood pressure and maintaining kid-ney integrity. The combination of enalapril and hydro-chlorothiazide, however, was as effective with respect toblood pressure lowering, protection of kidney function,and preservation of morphology as nitrendipine andenalapril combined. Also, the increases in GFR, diure-sis, and albuminuria after nitrendipine alone were re-versible within a short period after withdrawal of theCCB. Finally, nitrendipine given to normotensive ratsdid not exert the adverse effects that were seen in thehypertensive rats.
Protective effects of CCB have been demonstrated invarious animal models of renal disease.14"20 However,few studies found adverse effects of CCB on renalparameters.121-23 The effects of CCB on glomerularhemodynamics are variable, and this group of drugs mayexert cytoprotective effects through prevention of cal-cium overloading, reduction of metabolic activity, de-crease of free radical formation, and antiproliferativeand antiplatelet aggregatory effects.26-28
In addition to nonhemodynamic mechanisms, CEImay be beneficial in preventing the progression of renaldisease by a hemodynamic mechanism, ie, decrease ofsystemic blood pressure and lowering of glomerularcapillary pressure. Because a CEI and CCB may protectrenal function by different mechanisms, it might beuseful to combine both drugs in the treatment ofhypertension and chronic renal disease, especially in a
TABLE 2. Morphology of the Clipped Kidney
Group
Hypertensive controls
Nitrendipine
Enalapril
Nitrendipine+enalapril
Enalapril+hydrochlorothiazide
TubuloJnteratrualDamage (Score)
0.58±0.05
0.55±0.05
2.00±0.33*
2.40±0.26tt
3.00±0.26t§
GlomerularVolume,
0.82±0.04
0.90±0.05
0.73±0.06
0.74±0.03
0.73±0.02||
model in which either drug alone was not successful inpreventing progression of chronic renal failure.
In this study the combination of CEI and CCB washighly protective for the kidney. However, the addition ofa diuretic to enalapril increased its effectiveness to asimilar extent. Because triple therapy fails to normalizeblood pressure in this model of renovascular hypertension,as we have shown previously, the role of blood pressureper se in the progression of renal disease in this model ofhypertension is difficult to determine.1 It is unclearwhether the protection afforded by combination therapy isachieved by blood pressure normalization or is due to thespecific hemodynamic effect of enalapril of a decrease ofglomerular capillary pressure. However, enalapril mono-therapy failed to normalize blood pressure and also didnot exert significant protective effects on the nonclippedkidney, whereas enalapril combined with a diuretic de-creased both significantly, therefore, it seems that for CEItherapy, strict blood pressure control is an essential con-dition for inhibition of the progression of renal disease inthis model of hypertension. It remains to be determinedwhether in other models of renal disease the theoreticallyattractive combination of a CEI and CCB will result ingreater preservation of renal function over either agentalone or over the combination of enalapril with a diuretic,when normalization of blood pressure is also achieved bythe respective monotherapies.
The beneficial effect of CEI in lowering blood pressureand preventing the progression of renal disease has been
TABLE 3. Nitrendipine In Normotensive Rats
*P<.01, tP<-001 vs hypertensive controls.#><.01, ||P<.001 vs nitrendipine-treated rats.§P<.01 vs enalapril-treated rats.
Parameter
Body weight, g
Kidney weight, g
Glomerular injury, score
Glomerular volume, ^m 3 x i0"
Blood pressure, mm Hg
Albuminuria, mg/24 h
Diuresis, mL/24 h
Glomerular filtration rate, mL/mln
Nitrendipine(n=6)
514±9.0
1.44±0.04
0.030±0.08
1.34±0.11
107.5±5.0
0.41 ±0.09
23.3±3.8*
2.33±0.27
Controls(n=6)
481±10
1.37±0.02
0.028±0.07
1.26±0.06
118.8±3.0
0.32±0.12
13.3±0.9
2.66±0.24
*P<.025 vs controls.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

120 Hypertension Vol 23, No 1 January 1994
demonstrated in many animal models (for review, seeReference 29). In most studies, CEI treatment was initi-ated shortly after the onset of renal disease. However, iftherapy is initiated after a delay, as in the present study,CEIs are less effective in decreasing proteinuria, glomer-ular injury, and the progression of renal disease.3034
Nonetheless, in two recently published studies CEI ther-apy failed to decrease or normalize proteinuria and glo-merular damage despite the early start of therapy.35-36
Furthermore, suppression of the renin-angiotensin systemby a high salt diet impairs37-38 whereas stimulation of therenin-angiotensin system by diuretics or salt restrictionenhances the capacity of CEIs or angiotensin II antago-nists to lower blood pressure and prevent the progressionof renal disease.21-39 The angiotensin II antagonist sarala-sin strongly lowered blood pressure in rats with acutetwo-kidney, one clip hypertension, but the antihyperten-sive effect decreased with duration of hypertension, andsaralasin was less effective in subacute and finally wasineffective in chronic renovascular hypertension, whenplasma renin activity was lower than in the acute phase.40
Thus, it is not unexpected that in our study enalaprilstarted 6 weeks after induction of renovascular hyperten-sion lowered blood pressure only to a small extent and waswithout significant effect on albuminuria and glomerularinjury. Addition of a diuretic enhanced the therapeuticpotential of enalapril to lower blood pressure and de-crease renal damage probably because of volume and/orsodium depletion with consequent stimulation of therenin-angiotensin system. A similarity can be found in theantihypertensive treatment of patients: black and elderlyhypertensive patients tend to have a less-activated renin-angiotensin system and usually do not respond as well toCEI as do white or young patients with high bloodpressure. However, combination with a diuretic improvesthe response of blood pressure to CEI in bothpopulations.41
Besides the critical role of high blood pressure, impor-tant parameters that lead to the progression of chronicrenal disease in rats are glomerular hyperfiltration andhypertrophy.14-4244 These two factors are not invariablyassociated; an increase in GFR does not necessarily leadto the development of glomerulosclerosis unless there is aconcomitant increase in glomerular size.43-45 Our experi-ments show persistence of high blood pressure, increasedGFR, and increased glomerular volume in nitrendipine-treated animals. Therefore, these three variables have tobe considered as possible mediators of the increasedglomerular damage after nitrendipine monotherapy.
Because enalapril and nitrendipine combined loweredblood pressure and prevented the rise of GFR and glo-merular volume, it is difficult to decide which factor wasresponsible for the increased albuminuria and glomerularinjury after therapy with nitrendipine. Withdrawal ofnitrendipine normalized GFR and albuminuria withindays, whereas glomerular volume and blood pressureremained high, so it seems likely that the hyperfiltrationper se is responsible at least in part for the increasedalbuminuria in nitrendipine-treated rats. In many experi-mental models of renal disease, glomerular sclerosis andproteinuria are associated with increased single-nephronGFR and two of its determinants, increased glomerularcapillary pressure and flow, and changes in permselectiv-ity. Attenuation of these alterations either by CEI ordietary protein restriction largely prevents proteinuria and
the development of glomerular injury, indicating thathyperfiltration (and/or some hemodynamic determinantthereof) might play a role in the initiation and progressionof glomerular disease.46-47
However, it should be mentioned that the role ofhyperfiltration and glomerular hypertrophy in the pro-gression of nondiabetic renal disease in humans remainsto be determined.48-49 Although large randomized, con-trolled, and prospective clinical trials on the effect ofblood pressure control on the course of renal function inpatients with kidney disease are lacking, there is circum-stantial evidence from epidemiologic and clinical stud-ies that treatment of hypertension is the most importantcriterion for ameliorating the downhill course of renalfunction in patients with chronic renal failure.48-50-51
To our knowledge, this is the first experimental modelof hypertension and renal disease in which an increase ofglomerular volume after therapy with CCB is present. Themechanism of the increased glomerular volume in nitren-dipine-treated rats remains unclear. However, some con-siderations apply. First, the increased glomerular volumeis not a functional consequence caused by nitrendipinebecause it persisted after withdrawal of the drug. This is inaccordance with the results of Yoshida and coworkers,43
who found no correlation between glomerular capillarypressure or single-nephron GFR and volume of individualglomeruli. Second, nitrendipine does not act as a pharma-cologic growth factor for glomeruli in general, because theglomerular volume in the clipped kidney of the nitren-dipine-treated rats and the glomerular size of normoten-sive rats were not increased after nitrendipine treatment.This is in agreement with the in vivo and in vitro data. Invivo studies found either no change52 or decrease ofglomerular volume after therapy with CCB,14-23 and CCBinhibited synthesis of DNA and cell growth in mesangialcells53-54 and smooth muscle cells (for review, see Refer-ence 55). However, one study found a weak enhancementof smooth muscle cell proliferation by nitrendipine.56
Whereas in normotension and in the absence of affer-ent renal vasoconstriction CCBs have only marginal effectson renal hemodynamics, as shown in our nitrendipine-treated normotensive rats, their role in hypertensive ani-mals and in states of angiotensin U-induced renal vaso-constriction is different In those pathophysiological states,CCBs are able to increase GFR by preferential preglo-merular dilatation, whereas efferent arteriolar tone ispreserved.57 It is therefore not surprising that nitrendipineincreased GFR in the nonclipped kidney of Goldblatt rats,which have a high, probably angiotensin H-mediated,preglomerular resistance.58-59 The increase of GFR duringchronic treatment in our study confirms the results ofHuang,60 who found an increase of GFR in the nonclippedkidneys of anesthetized Goldblatt hypertensive rats afteracute administration of nifedipine. Although an increaseof GFR may be advantageous in many states of chronicrenal disease, hyperfiltration could also be detrimental inthe long term, especially if it is associated with an insuffi-cient blood pressure control, as in the present study.42
Despite the increased glomerular damage, GFR innitrendipine-treated animals was not impaired but evenincreased compared with all other groups. The effect ofnitrendipine on the remaining intact glomeruli to hyper-filtrate probably compensated for the loss of filteringglomeruli during nitrendipine. However, after with-drawal of nitrendipine, the increased GFR was not only
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

Wenzel et al Nitrendipine and Enalapril in Renovascular Hypertension 121
reversible but even numerically decreased. This couldbe caused by the decreased number of intact glomeruliafter nitrendipine treatment with the consequence of adecreased total GFR, which was masked by the hyper-filtration caused by nitrendipine.
Because diuresis increased shortly after nitrendipinewas started and decreased promptly after it was with-drawn, it seems unlikely that the increased diuresis is theconsequence of structural alterations in the kidney causedby nitrendipine. Rather, it may be either a consequence ofaugmented filtered load secondary to increased GFR or aresult of a direct effect of CCB on tubular reabsorption orboth.61 Dihydropyridine CCBs also are known to increaseurinary /32 microglobulin excretion, suggesting a decreaseof tubular protein reabsorption, possibly caused by anincrease in tubular flow.62 Such a mechanism also maycontribute to the increase of albuminuria during nitren-dipine in our study.
We feel that the results of this study confirm ourprevious hypothesis that the adverse effects of the CCBnitrendipine on glomerular function and structure areprobably caused by preglomerular dilatation and insuf-ficient blood pressure reduction, facilitating a rise ofglomerular pressure.1 Because addition of a CEI, knownfor its specific glomerular pressure-lowering effects, andsimultaneous blood pressure reduction to normotensivelevels ameliorated the negative effects of nitrendipine.This hypothesis is further supported by the recentobservation by Fenoy et al63 of an increased glomerularcapillary pressure after the CCB clentiazem and by thefinding of an increased glomerular capillary pressure byRemuzzi and coworkers64 after treatment with nitren-dipine in MWF/Ztm rats. Additionally, Benstein et al25
recently described an increase of proteinuria and glo-merular sclerosis after administration of the CCB nifed-ipine to rats with remnant kidneys and establishedinjury.
In summary, the combination of nitrendipine and enal-april ameliorates the adverse renal effect of nitrendipineby lowering blood pressure to normotensive levels. In-creased GFR, diuresis, and albuminuria after nitrendipineare reversible after withdrawal, whereas increased glomer-ular injury and glomerular volume persist. Nitrendipinedoes not exert its adverse effects on the kidney in nor-motensive animals. Addition of nitrendipine or a diureticto enalapril increases its effectiveness in lowering bloodpressure and protecting the kidney, and no significantdifference exists with regard to blood pressure control anddecrease of renal injury between both combination ther-apies. Therefore, it seems that strict blood pressure con-trol, which is only obtained by a combination therapyincluding a CEI in this model of hypertension, is necessaryfor protection of the kidney.
AcknowledgmentsSupported by the German Research Foundation (We 1688/
1-1, Schw 249/2-2/2-3). We thank Dr Hanna E. Abboud(University of Texas, San Antonio) and Dr Rolf Stahl (Uni-versity of Frankfurt, Germany) for critical reading of themanuscript and acknowledge the excellent technical assistanceof Barbara Bisiorek and Ursula Kneissler.
References1. Wenzel UO, Goetz T, Schoeppe W, Helmchen U, Schwietzer G.
Adverse effect of the calcium channel blocker nitrendipine on
nephrosclerosis in rats with renovascular hypertension. Hyper-tension. 1992;20:233-241.
2. Balcris GL, Bamhill BW, Sadler R. Treatment of arterial hyper-tension in humans: importance of therapeutic selection. Kidney Int.1992;41:912-919.
3. Brouwer RML, Bolli P, Erne P, Conen D, Kkjwski W, Buhler FR.Antihypertensive treatment using calcium antagonists in combinationwith captoprQ rather than diuretics. J Cardwvasc PharmacoL 1985;7:88-91.
4. Guazzi MD, Cesare ND, Galli C, Salvioni A, Tramontana C,Tamborini G, Bartorelli A. Calcium-channel blockade withnifedipine and angiotensin converting-enzyme inhibition with cap-topril in the therapy of patients with severe primary hypertension.Circulation. 1984;70:279-284.
5. Morgan TO, Anderson A, Jones E. Comparison and interaction oflow dose felodipine and enalapril in the treatment of essentialhypertension in elderly patients. Am J Hypertens. 1992^:238-243.
6. Singer DRJ, Markandu ND, Shore AC, McGregor GA. Captopriland nifedipine in combination for moderate to severe essentialhypertension. Hypertension. 1987;9:629-633.
7. Kloke HJ, Wetzels JFM, Van Hamersvelt HW, Koene RAP,Kleinbloesem CH, Huysmans FTM. Effects of nitrendipine andcilazapril on renal hemodynamics and albuminuria in hypertensivepatients with chronic renal failure. J Cardiovasc PharmacoL 1990;16:924-930.
8. Sarvetti A, Magagna A, Innocent! P, Ponzanelli F, Cagianelli A,Cipriani M, Gandoln E, Del Prato C, Ballestra AM, Saba P,Giuntoli F, Panebianco G, Amigoni S. The combination of chlor-thalidone with nifedipine does not exert an additive antihyper-tensive effect in essential hypertensives: a crossover multicenterstudy. J Cardiovasc Pharmacol 1991;17:332-335.
9. Fuhr J, Kaczmarczyk J, Kruttgen CD. Eine einfache colorme-trische Methode zur Inulinbestimmung fur Nierenclearanceunter-suchungen bei Stoffwechselgesunden und Diabetikern. KlinWochenschr. 1955^3:729-730.
10. Weibel ER. Stereological Methods: Practical Methods for BiologicalMorphometry. London, England: Academic Press Iwr, 1979:51-57.
11. Michel JB, Dussaule JC, Choudat L, Auzan C, Nochy D, Corvol P,Menard J. Effects of antihypertensive treatment in one-dip, twokidney hypertension in rat. Kidney Int. 1986;29:1011-1020.
12. Jackson B, Franze C, Sumithran E, Johnston CI. Pharmacologicnephrectomy with chronic angiotensin converting enzyme inhibitortreatment in renovascular hypertension in the rat. / Lab Clin Med.1990;115:21-27.
13. Groene HJ, Helmchen U. Impairment and recovery of the clippedkidney in two kidney, one clip hypertensive rats during and afterantihypertensive therapy. Lab Invest. 1986^4:645-655.
14. Dworkin LD, Benstein JA, Parker M, Tolbert E, Feiner HD.Calcium antagonists and converting enzyme inhibitors reducerenal injury by different mechanisms. Kidney Int. 1993;43:808-814.
15. Dworkin LD, Levin RI, Benstein JA, Parker M, Ullian ME, KimY, Feiner HD. Effects of nifedipine and enalapril on glomerularinjury in rats with deoxycorticosterone-salt hypertension. Am JPhysiol 1990;259:F598-F604.
16. Dworkin LD, Feiner HD, Parker M, Tolbert E. Effects ofnifedipine and enalapril on glomerular structure and function inuninephrectomized SHR. Kidney InL 1991^39:1112-1117.
17. Harris DCH, Hammond WS, Burke TJ, Schrier RW. Verapamilprotects against progression of experimental chronic renal failure.Kidney Int. 1987;31:41-46.
18. Huelsemann JL, Sterzel RB, McKenzie DE, Wilcox CS. Effects ofa calcium entry blocker on blood pressure and renal functionduring angiotensin-induced hypertension. Hypertension. 1985;7:374-379.
19. Jarusiripipat C, Chan L, Shapiro JI, Schrier RW. Effect of long-acting calcium entry blocker (anipamil) on blood pressure, renalfunction and survival of uremic rats. J Pharmacol Exp Ther. 1992;260:243-247.
20. Aguas AP, Nickerson PA. Effect of verapamil on blood pressureand lesions in heart and kidney of rats made hypertensive bydeoxycorticosterone (DOC). Am J PathoL 1983;110:48-54.
21. Brunner FB, Thiel G, Hermle M, Bock HA, Mihatsch MJ.Long-term enalapril and verapamil in rats with reduced renal mass.Kidney InL 1989;36:969-977.
22. Brunner FP, Bock HA, Hermle M, Thiel G, Mihatsch MJ. Controlof hypertension by verapamil enhances renal damage in a ratremnant kidney model. Nephrol Dial Transplant. 1991;6:420-427.
23. Tolins JP, Raij L. Comparison of converting enzyme inhibitor andcalcium channel blocker in hypertensive glomerular injury. Hyper-tension. 1990;16:452-461.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

122 Hypertension Vol 23, No 1 January 1994
24. Jackson B, Johnston CI. The contribution of systemic hypertensionto progression of chronic renal failure in the remnant kidney: effectof treatment with an angiotcnsin converting enzyme inhibitor or acalcium inhibitor. J Hypertens. 1988;6:495-501.
25. Benstein JA, Feiner HD, Ohsumi F, Tolbert E, Dworkin LD.Impact of salt restriction and calcium antagonists on renal hyper-trophy, function and sclerosis in rats with remnant kidneys andestablished injury. J Am Soc NephroL 19923:734. Abstract.
26. Epstein M, Loutzenhiser R. Potential applicability of calciumantagonists as renal protective agents. In: Epstein M, LoutzenhiserR, eds. Calcium Antagonists and the Kidney. Philadelphia, Pa:Hanley & Belfus, Inc; 1990:275-298.
27. Chan L, Schrier RW. Effects of calcium channel blockers on renalfunction. Annu Rev Med 1990;41:289-302.
28. Dworkin LD. Effects of calcium channel blockers on experimentalglomerular injury. J Am Soc NephroL 1990;l:S21-S27.
29. Keane WF, Anderson S, Aurell M, De Zeeuw D, Narins RG,Povar G. Angiotensin converting enzyme inhibitors and pro-gressive renal insufficiency. Ann Intern Med 1990;lll:503-516.
30. Beukers JJB, Van Der Wai A, Hoedemaeker PJ, Weening JJ.Converting enzyme inhibition and progressive glomerulosclerosisin the rat. Kidney Int. 198732:794-800.
31. Meyer TW, Anderson S, Rennke HG, Brenner BM. Reversingglomerular hypertension stabilizes established glomerular injury.Kidney Int. 198731:752-759.
32. Ikoma M, Kawamura T, Kakinuma Y, Fogo A, Ichikawa I. Causeof variable therapeutic efficiency of angiotensin enzyme inhibitoron glomerular lesions. Kidney Inl 1991;40:195-202.
33. Feld LG, Cachero S, Van Liew JB. Enalapril and renal injury inspontaneously hypertensive rats. Hypertension. 1990;16:544-554.
34. Podjarny E, Bernheim JL, Pomerany A, Rathaus M, Pomeranz M,Green J, Berheim J. Effect of timing of antihypertensive therapy onglomerular injury: comparison between captopril and diltiazem.Nephrol Dial Transplant 1993;8:501-506.
35. Kimura K, Toja A, Matsuoka H, Sugimoto T. Renal arteriolardiameters in spontaneously hypertensive rats: vascular cast study.Hypertension. 1991;18:101-110.
36. O'Donnel MP, Kasiske BL, Katz SA, Schmitz PG, Keane WF.Lovastatin but not enalapril reduces glomerular injury in Dahlsalt-sensitive rats. Hypertension. 1992;20:651-658.
37. Fabris B, Jackson B, Johnston CI. Salt blocks the renal benefits oframiprfl in diabetic hypertensive rats. Hypertension. 1991;17:497-503.
38. Gavras H, Brunner HR, Vaughan ED, Laragh JH. Angiotensin-sodium interaction in blood pressure maintenance of renal hyper-tensive and normotensive rats. Science. 1973;180:1369-137Z
39. Terzi F, Beaufils H, Laouri D, Burtin M, Kleinknecht C. Renaleffect of antihypertensive drugs depends on sodium diet in theexcision remnant kidney model. Kidney Int. 1992;42354-363.
40. Carretero OA, Gulati OA. Effects of angiotensin antagonist in ratswith acute, subacute, and chronic two-kidney renal hypertension.J LabClin Med 1978;91:264-271.
41. The Joint National Committee on Detection, Evaluation, andTreatment of High Blood Pressure. The fifth report of the JointNational Committee on Detection, Evaluation and Treatment ofHigh Blood Pressure (JNCV). Arch Intern Med 1993;153:154-183.
42. Brenner BM. Nephron adaptation to renal injury or ablation. AmJ PhysioL 1985;249:F324-F337.
43. Yoshida Y, Fogo A, Ichikawa I. Glomerular hemodynamic changesvs. hypertrophy in experimental glomerular sclerosis. Kidney Int.198935:654-660.
44. Jacobson HR. Chronic renal failure: pathophysiology. Lancet.1991;338:419-423.
45. Miller PL, Rennke HG, Meyer TW. Glomerular hypertrophyaccelerates hypertensive glomerular injury in rats. Am J PhysioL1991;261:F459-F465.
46. Zatz R, Anderson S, Meyer TW, Dunn BR, Rennke HG, BrennerBM. Lowering of arterial blood pressure limits glomerular sclerosisin rats with renal ablation and experimental diabetes. Kidney Int.198731(suppl 20):123-129.
47. Anderson S. Systemic and glomerular hypertension in progressiverenal disease. Kidney Int. 1988;34(suppl 25):119-121.
48. National High Blood Pressure Education Program. National highblood pressure education program working group report on hyper-tension and chronic renal failure. Arch Intern Med 1991;151:1280-1287.
49. Rudberg S, Person B, Dahlquist G. Increased glomerular filtrationrate as predictor of diabetic nephropathy: an 8-year prospectivestudy. Kidney Inl 1992;41:822-828.
50. Luft F, Johnston CI. Are calcium antagonists of value in amelio-rating the course of chronic renal disease? Kidney Int. 1992;41(suppl36):114-118.
51. Brazy PC, Stead WW, FitzwiUiam JF. Progression of renal insuf-ficiency: role of blood pressure. Kidney Int. 198935:670-674.
52. Fogo A, Yoshida Y, Yared A, Ichikawa I. Importance ofangiogenic actions of angiotensin II in the glomerular growth ofmaturing kidneys. Kidney Int. 199038:1068-1074.
53. Roth M, Keul R, Emmons LR, Horl WH, Block LH. Manidipineregulates the transcription of cytolrine genes. Proc Natl Acad SciUSA. 1992;89:4071-4075.
54. Shultz PJ, Raij L. Effect of amlodipine on mesangial cell prolif-eration and protein synthesis. Am J Hypertens. 1992^:912-914.
55. Jackson CL, Schwartz SM. Pharmacology of smooth muscle cellreplication. Hypertension. 1992;20:713-736.
56. Absher MP, Baldor L, Warshaw DM. Effects of nitrendipine ongrowth activity in cultured vascular smooth muscle cells.J Cardiovasc Pharmacol 1988:12(suppl 4):104-106.
57. Loutzenhiser R, Epstein M. Renal microvascular actions ofcalcium antagonists. J Am Soc NephroL 199O;1:S3-S12.
58. Ichikawa I, Ferrone RA, Duchin KL, Manning M, Dzau VJ,Brenner BM. Relative contribution of vasopressin and angiotensinII to altered renal microcirculatory dynamics in two-kidneyGoldblatt hypertension. Ore Res. 1983^3^92-602.
59. Schwietzer G, Gertz KH. Changes of hemodynamics and glo-merular ultrafiltration in renal hypertension of rats. Kidney Int.1979;15:134-143.
60. Huang WC Antihypertensive and bilateral renal response tonifedipine in 2-kidney, 1-dip Goldblatt hypertensive rats. RenalPhysioL 1986;9:167-176.
61. DiBona GF, Sawin LL. Renal tubular site of felodipine. J PharmacolExp Ther. 1984;228:420-424.
62. Krusell LR, Christensen CK, Lederballe Pedersen O. Acute natri-uretic effect of nifedipine in hypertensive patients and nor-motensive controls: a proximal tubular effect? Eur J ClinPharmacol 198732:121-126.
63. Fenoy FJ, Milicic I, Mistry M, Mecca T, Roman RJ. Effect ofclentiazem on arterial pressure and renal function in normotensiveand hypertensive rats. / Pharmacol Exp Ther. 1992;261:470-475.
64. Remuzzi A, Imberti O, Bertani T, Remuzzi G. An angiotensinconverting enzyme inhibitor, but not a calcium antagonist,prevents proteinuria and glomerulosclerosis in the rat. J Am SocNephrol 19923:748. Abstract.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

U O Wenzel, U Helmchen, W Schoeppe and G Schwietzerhypertension.
Combination treatment of enalapril with nitrendipine in rats with renovascular
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.23.1.114
1994;23:114-122Hypertension.
http://hyper.ahajournals.org/content/23/1/114World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOffice. Once the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertension Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from