Embed Size (px)
Citation preview
Oesophageal-, and gastric tumor
SZTE Onkoterápiás Klinika
Epidemiology of oesophageal cancer
• Increasing incidence, 250-300 new tu/year in
Hungary
• Male:female = 10:1
• Mainly squamosus cell- and adenocc.
• unfavourable prognosis, after resection 1 year
survival 70%, 2 year 25-30%, 5 year 15-18%
• Frequently advanced disease at dg. (inop.T3-T4)
Localisation
• Neck part: fraom the cricoid cartillage to thorax
• Thoracic part:
upper third to the bifurcation(18-24 cm)
midle. third bifurcation (24-32 cm)
lower third up to 40 cm
abdominal part: cardio-oesophageal junction
cardia ca 2-3 cm.
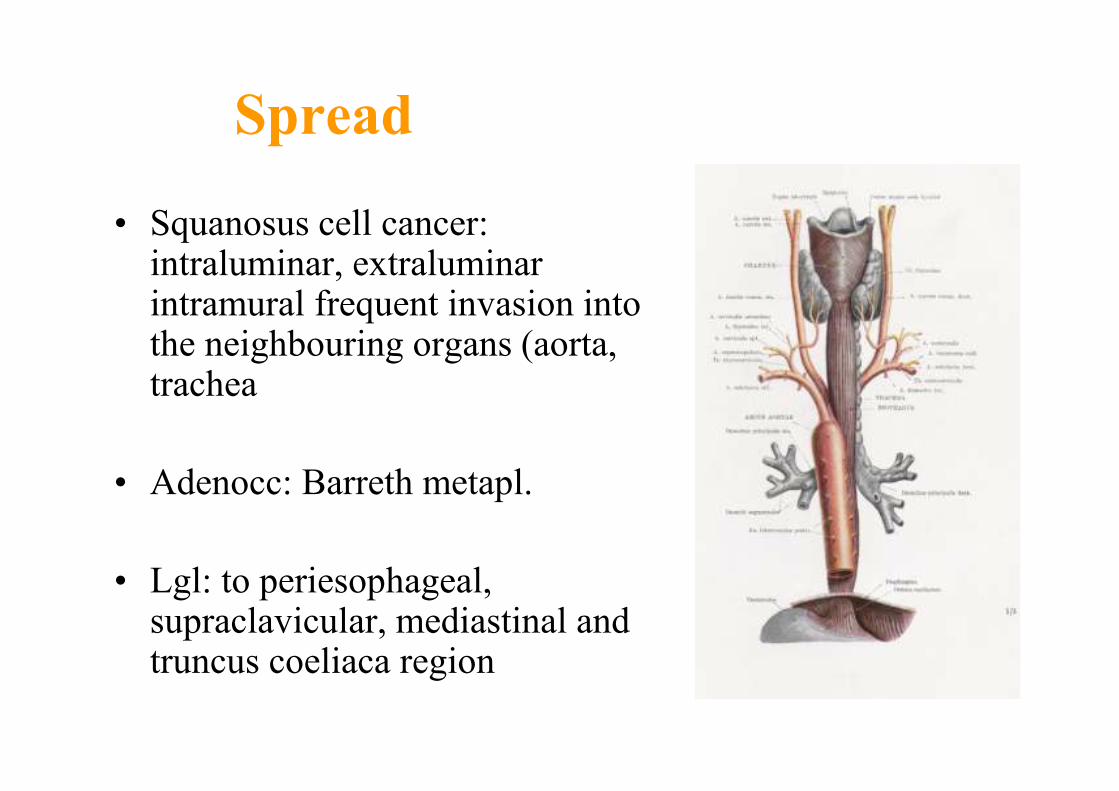
• Squanosus cell cancer: intraluminar, extraluminar intramural frequent invasion into the neighbouring organs (aorta, trachea
• Adenocc: Barreth metapl.
• Lgl: to periesophageal, supraclavicular, mediastinal and truncus coeliaca region
Spread
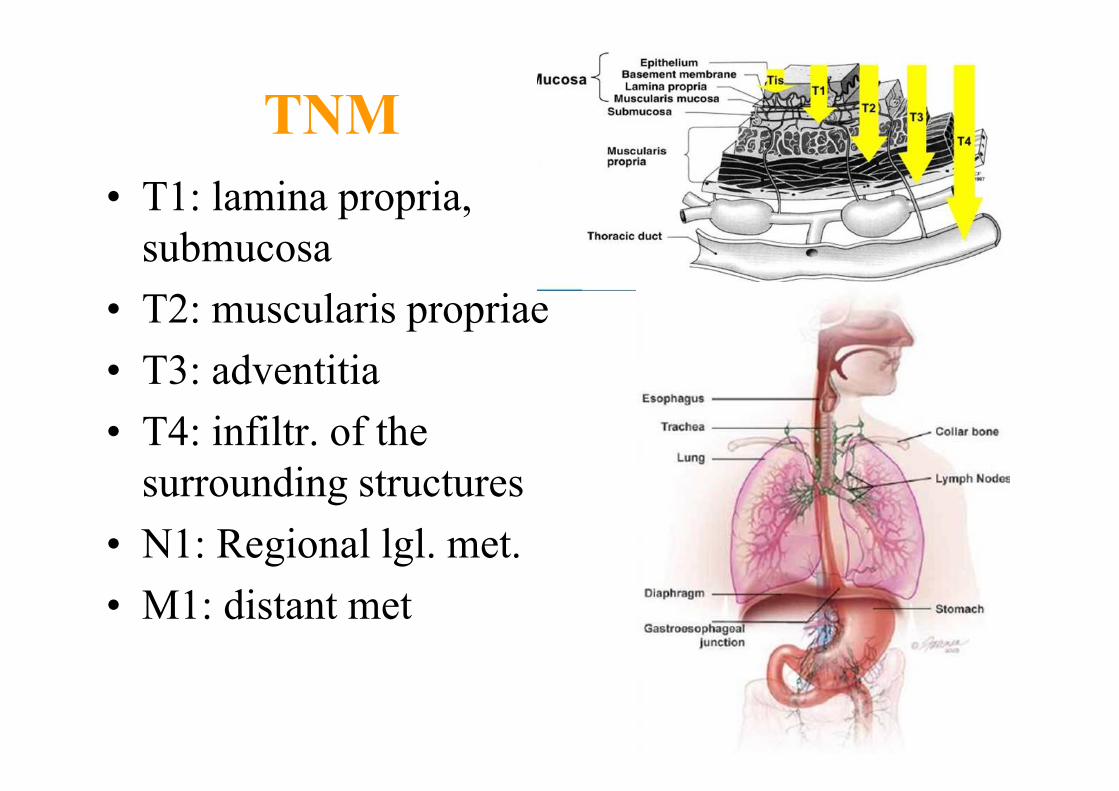
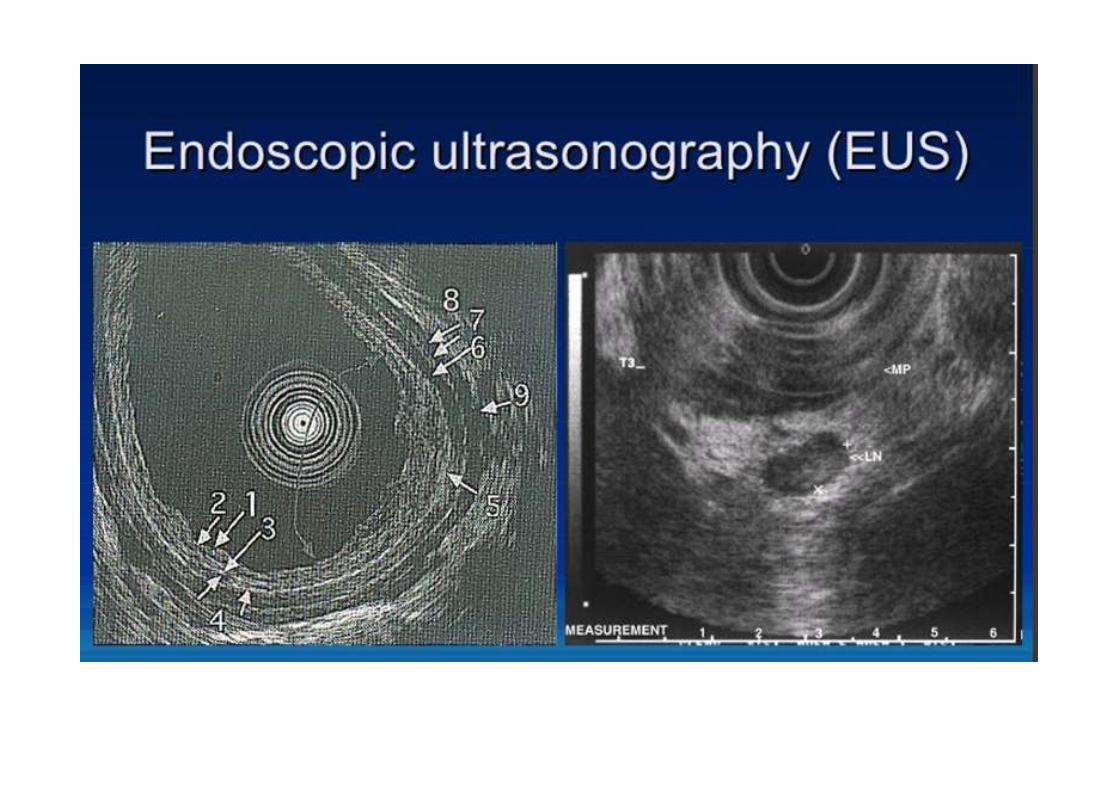
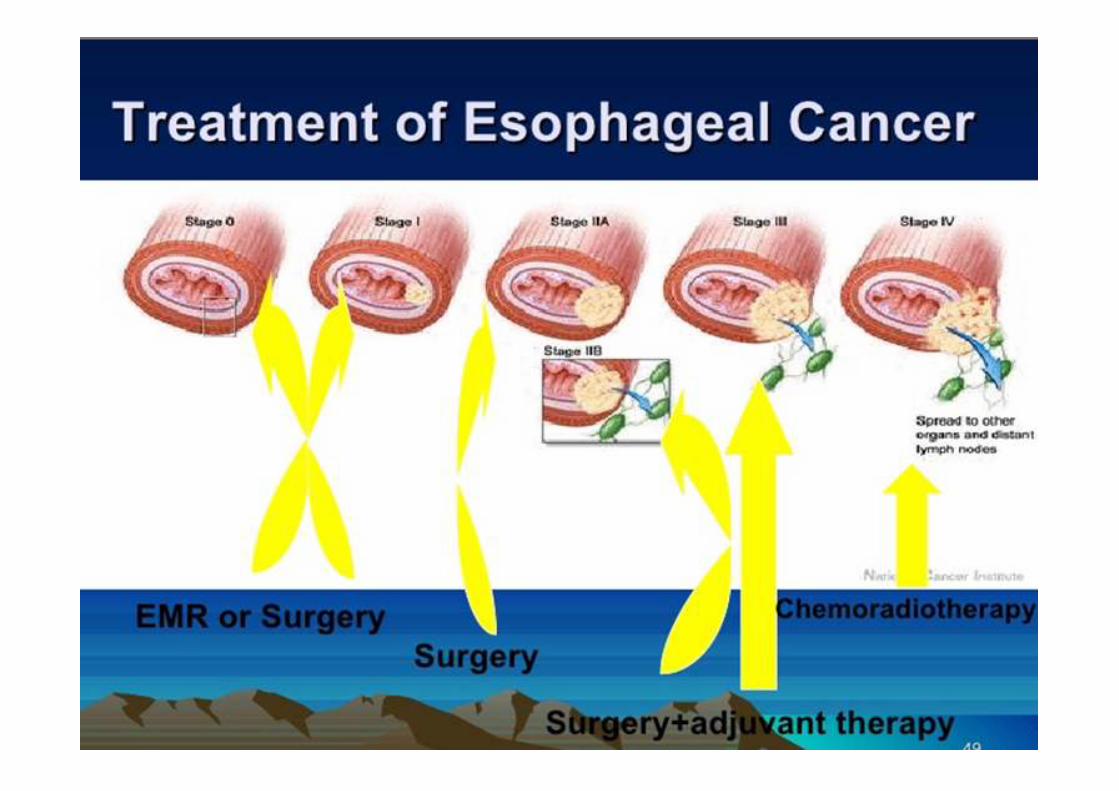
• T1: lamina propria,
submucosa
• T2: muscularis propriae
• T3: adventitia
• T4: infiltr. of the
surrounding structures
• N1: Regional lgl. met.
• M1: distant met
TNM
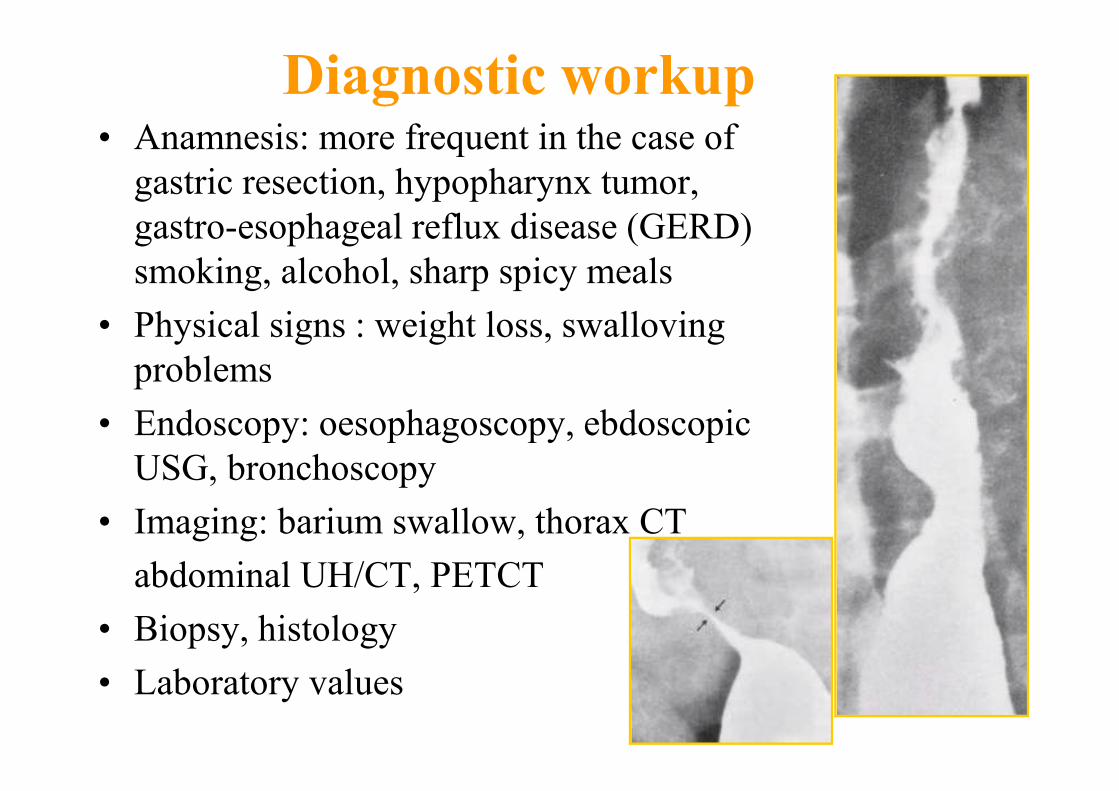
Diagnostic workup• Anamnesis: more frequent in the case of
gastric resection, hypopharynx tumor,
gastro-esophageal reflux disease (GERD)
smoking, alcohol, sharp spicy meals
• Physical signs : weight loss, swalloving
problems
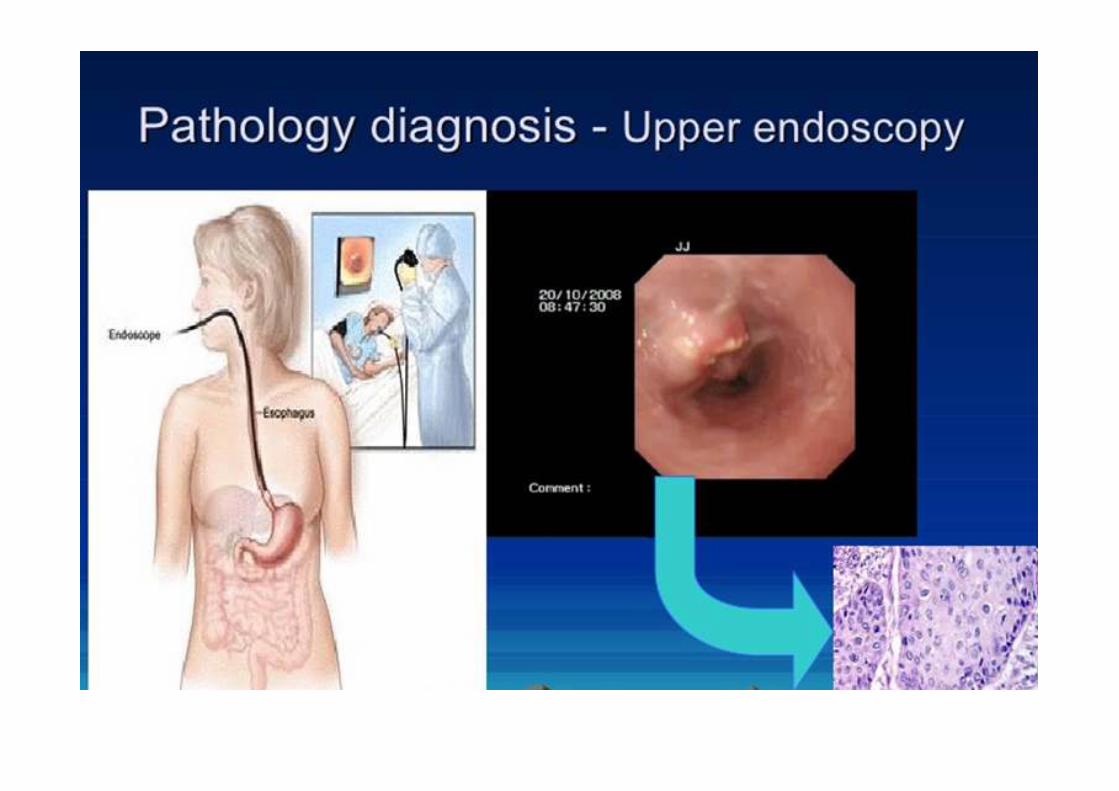
• Endoscopy: oesophagoscopy, ebdoscopic
USG, bronchoscopy
• Imaging: barium swallow, thorax CT
abdominal UH/CT, PETCT
• Biopsy, histology
• Laboratory values
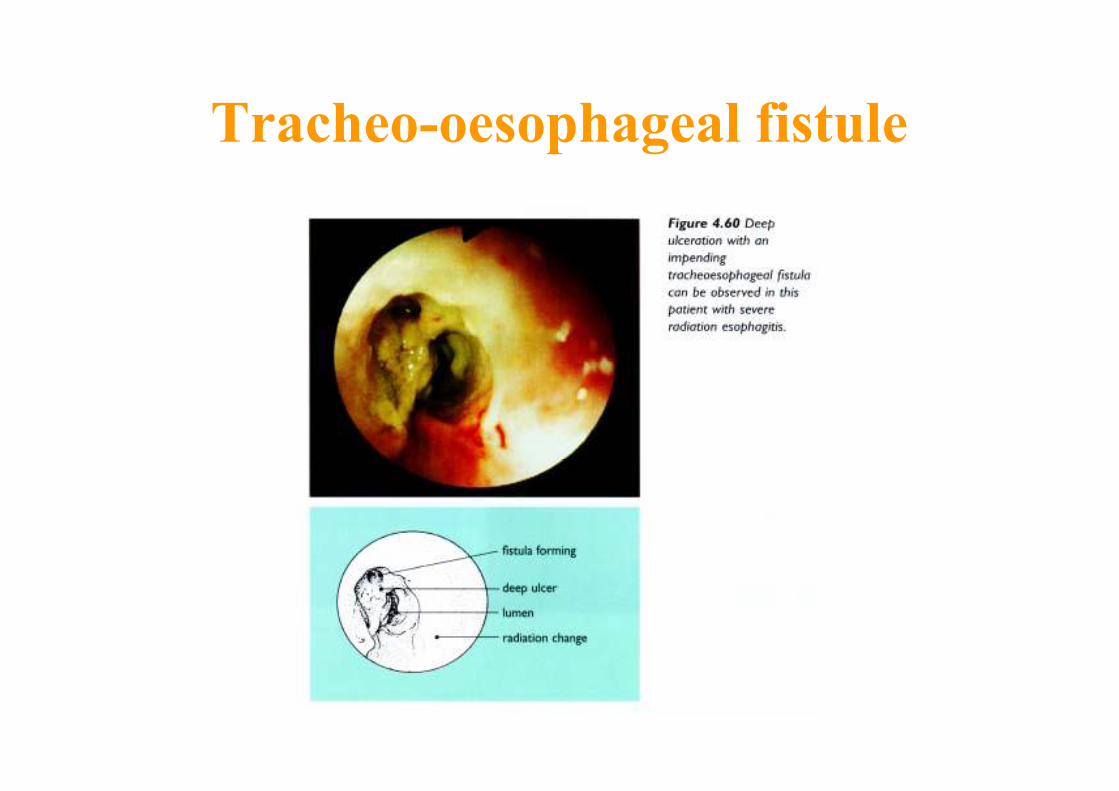
Tracheo-oesophageal fistule


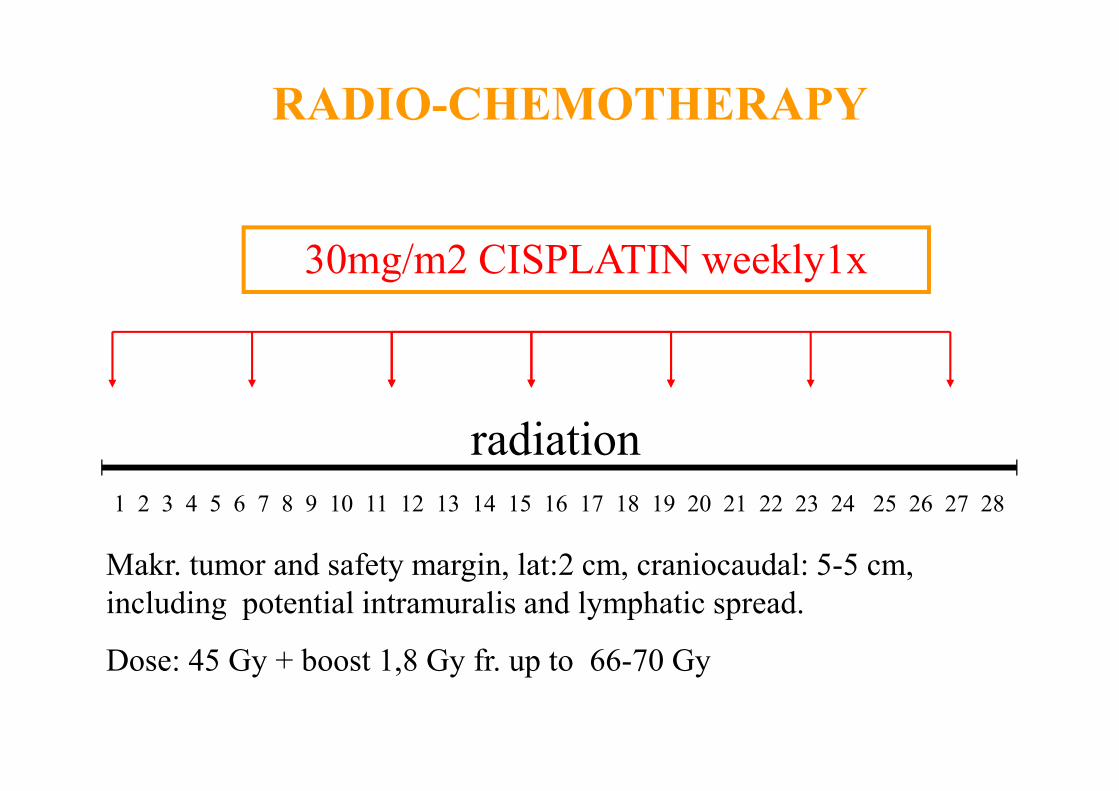
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
30mg/m2 CISPLATIN weekly1x
radiation
RADIO-CHEMOTHERAPY
Makr. tumor and safety margin, lat:2 cm, craniocaudal: 5-5 cm,
including potential intramuralis and lymphatic spread.
Dose: 45 Gy + boost 1,8 Gy fr. up to 66-70 Gy
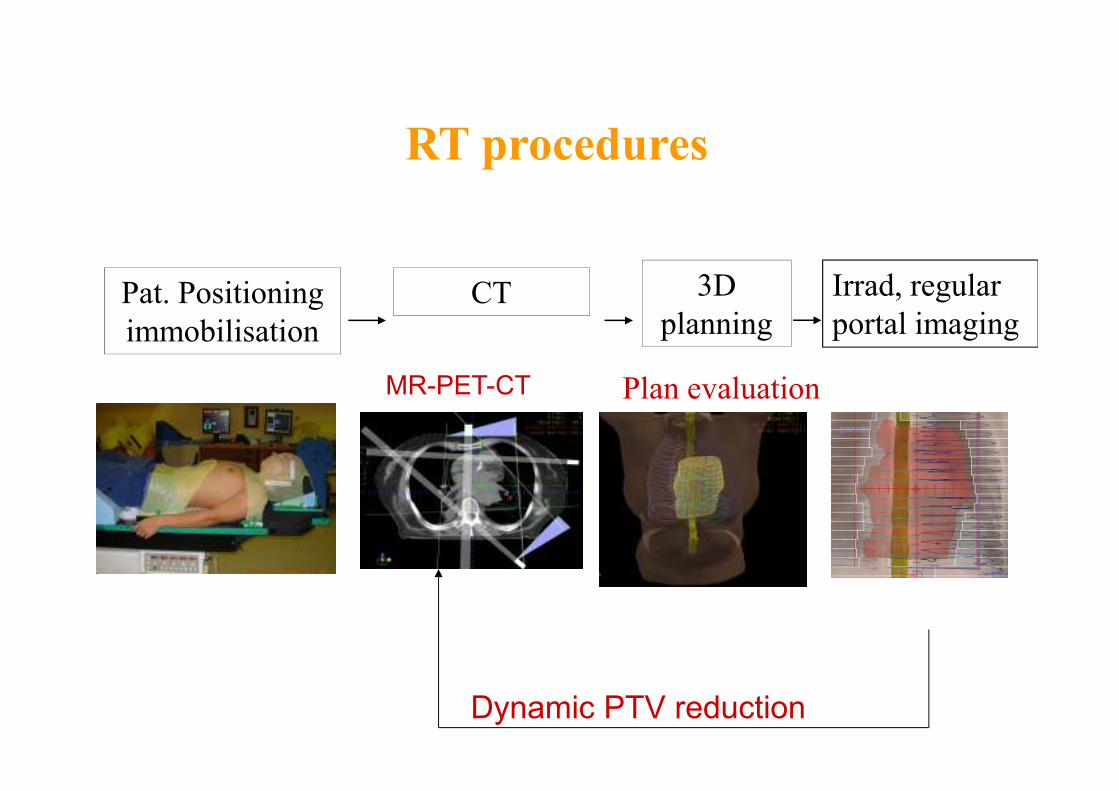
3D
planning
RT procedures
Pat. Positioning
immobilisation
CT
MR-PET-CT
Dynamic PTV reduction
Plan evaluation
Irrad, regular
portal imaging
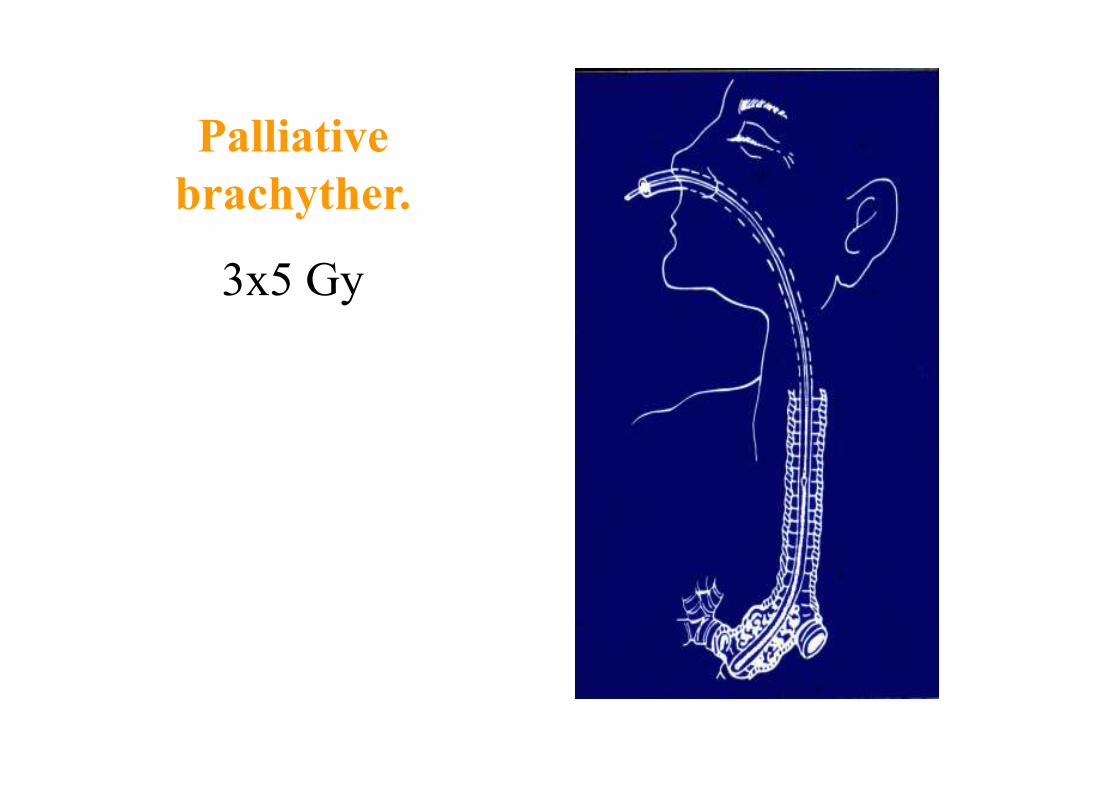
Palliative
brachyther.
3x5 Gy
Gastric cancer
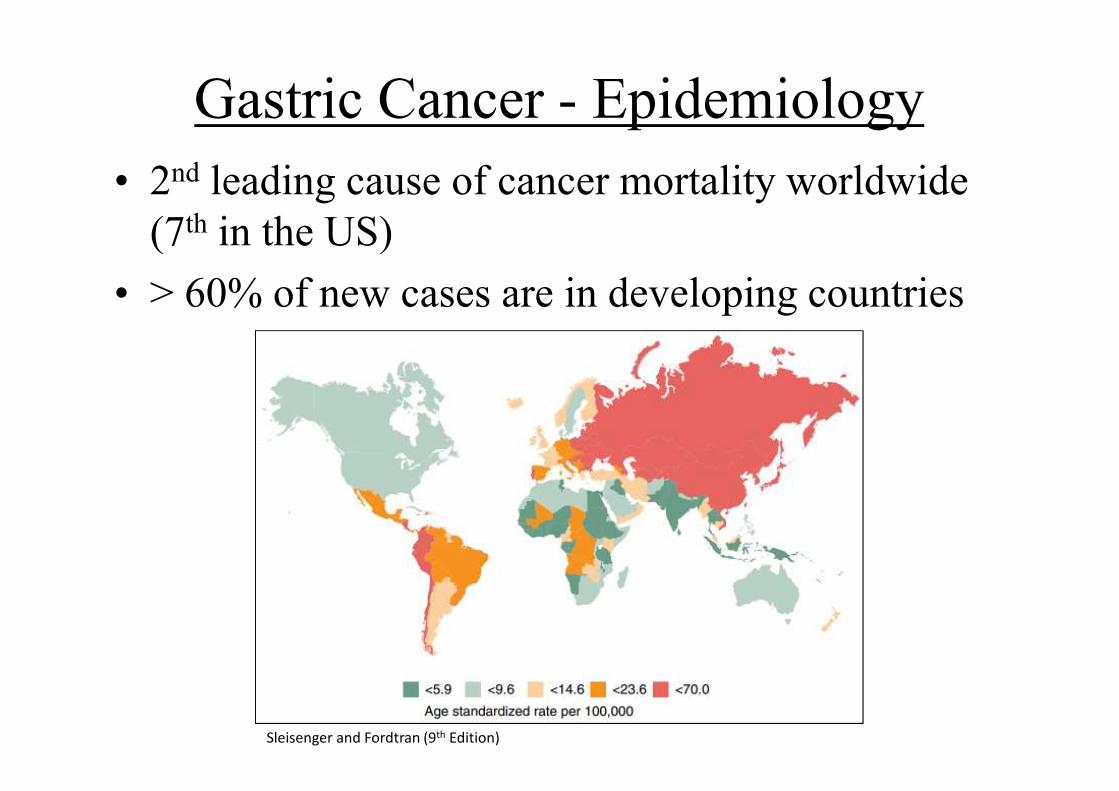
Gastric Cancer - Epidemiology
• 2nd leading cause of cancer mortality worldwide
(7th in the US)
• > 60% of new cases are in developing countries
Sleisenger and Fordtran (9th Edition)
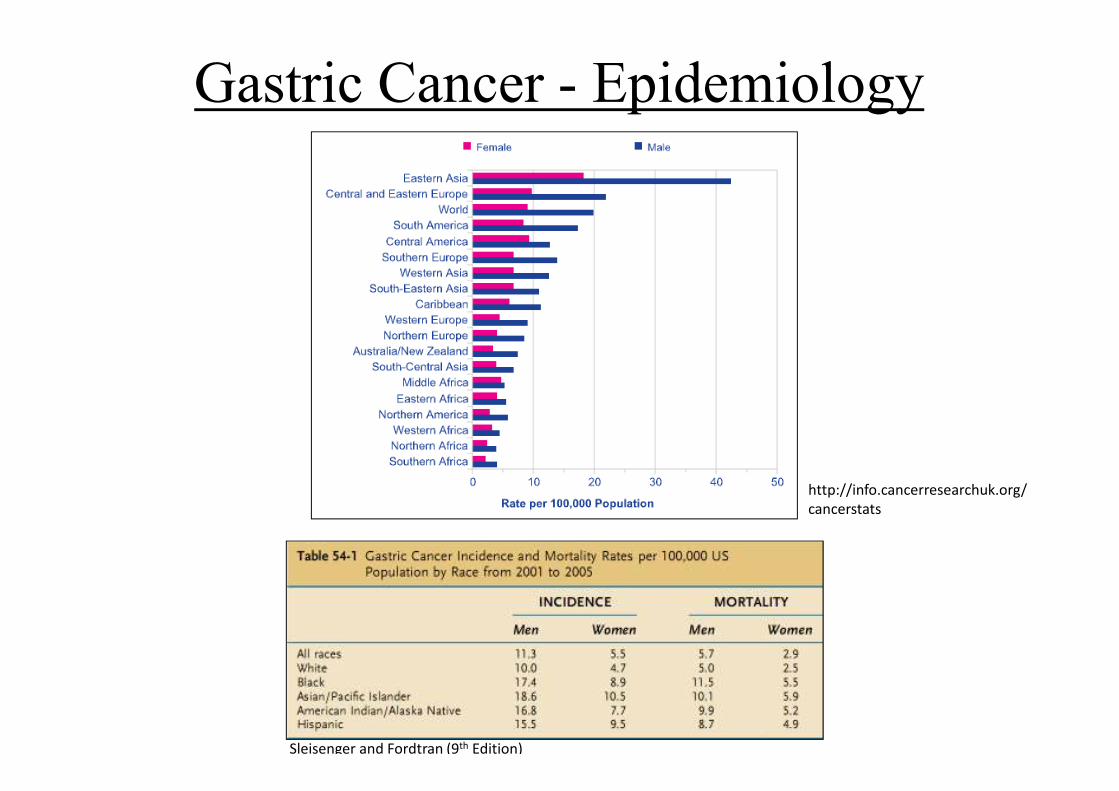
Gastric Cancer - Epidemiology
http://info.cancerresearchuk.org/
cancerstats
Sleisenger and Fordtran (9th Edition)
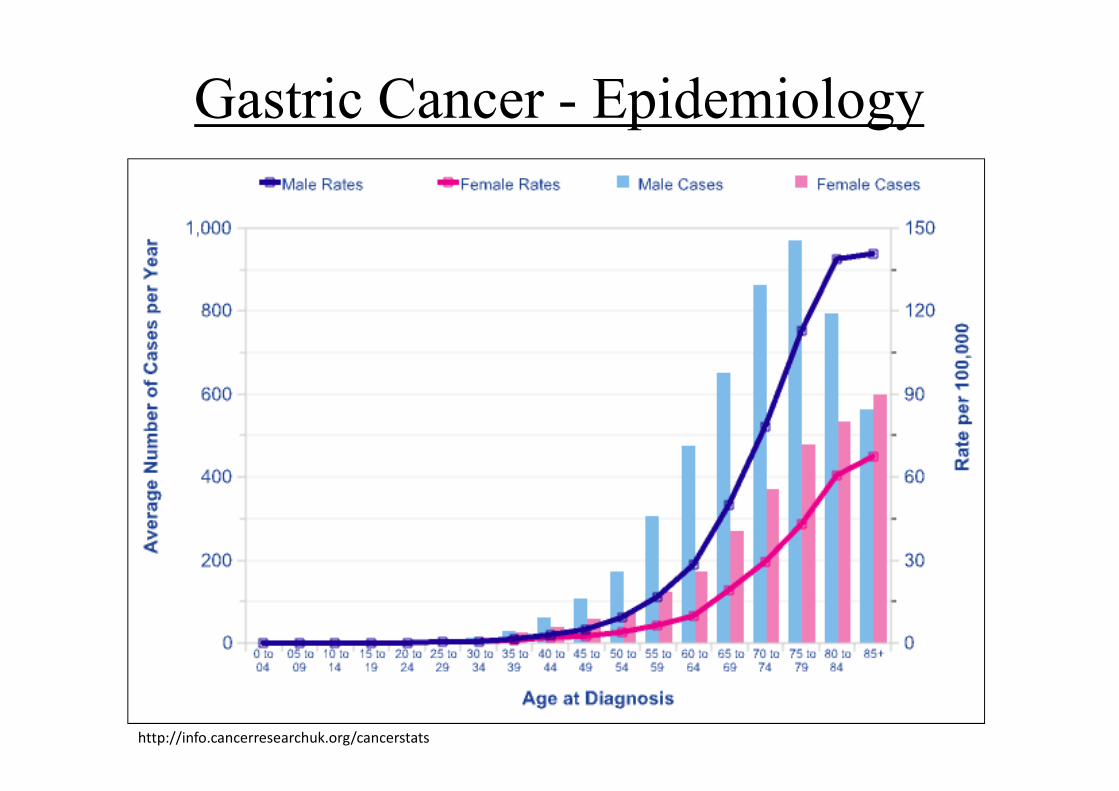
Gastric Cancer - Epidemiology
http://info.cancerresearchuk.org/cancerstats
�Diet appears to be a significant factor.
�A diet high in smoked foods and low in fruits
and vegetables may increase the risk of gastric
cancer.
�Other factors related to the incidence of gastric
cancer include chronic inflammation of the
stomach, anemia, gastric ulcers, H. pylori
infection, genetics, Smoking, a diet poor in
fiber, and Drink alcohol
Etiology
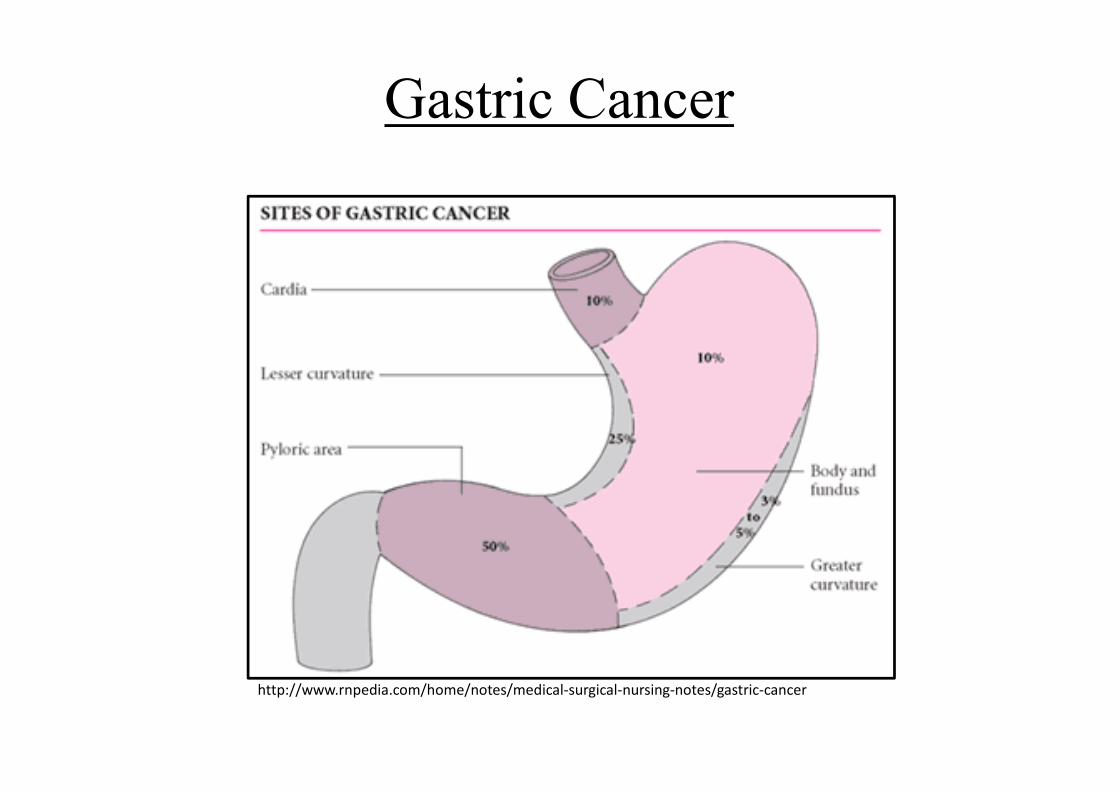
Gastric Cancer
http://www.rnpedia.com/home/notes/medical-surgical-nursing-notes/gastric-cancer
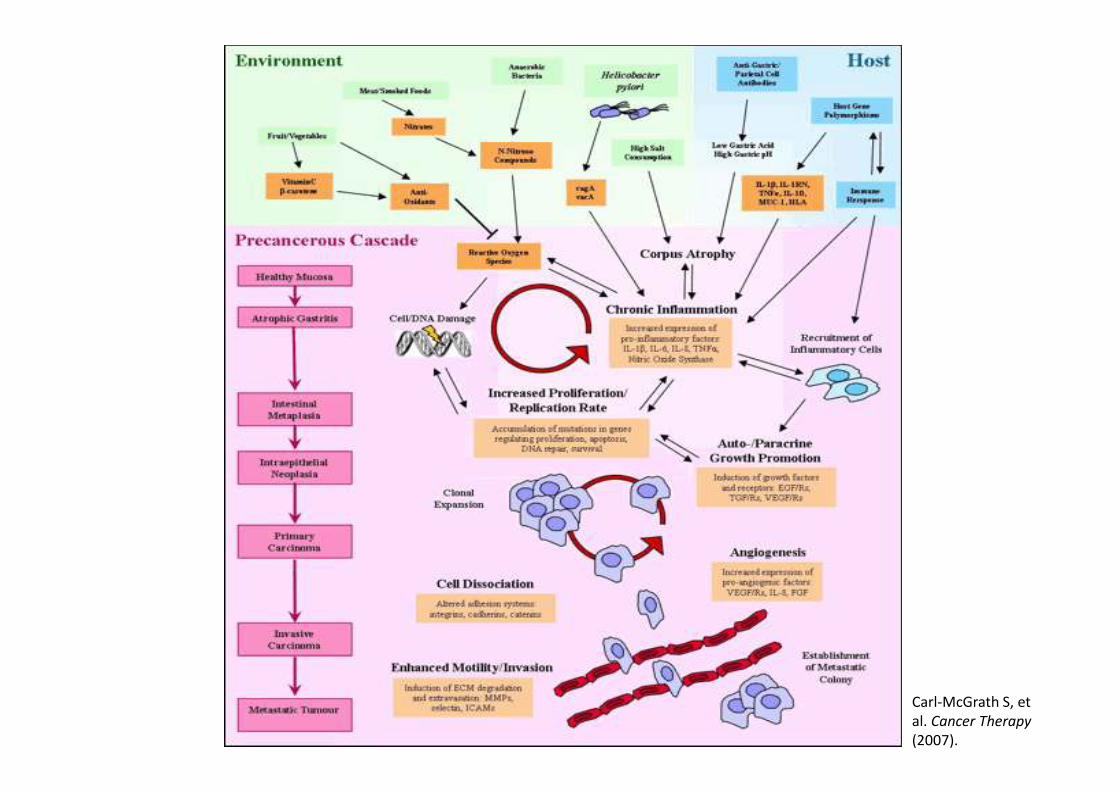
Carl-McGrath S, et
al. Cancer Therapy
(2007).
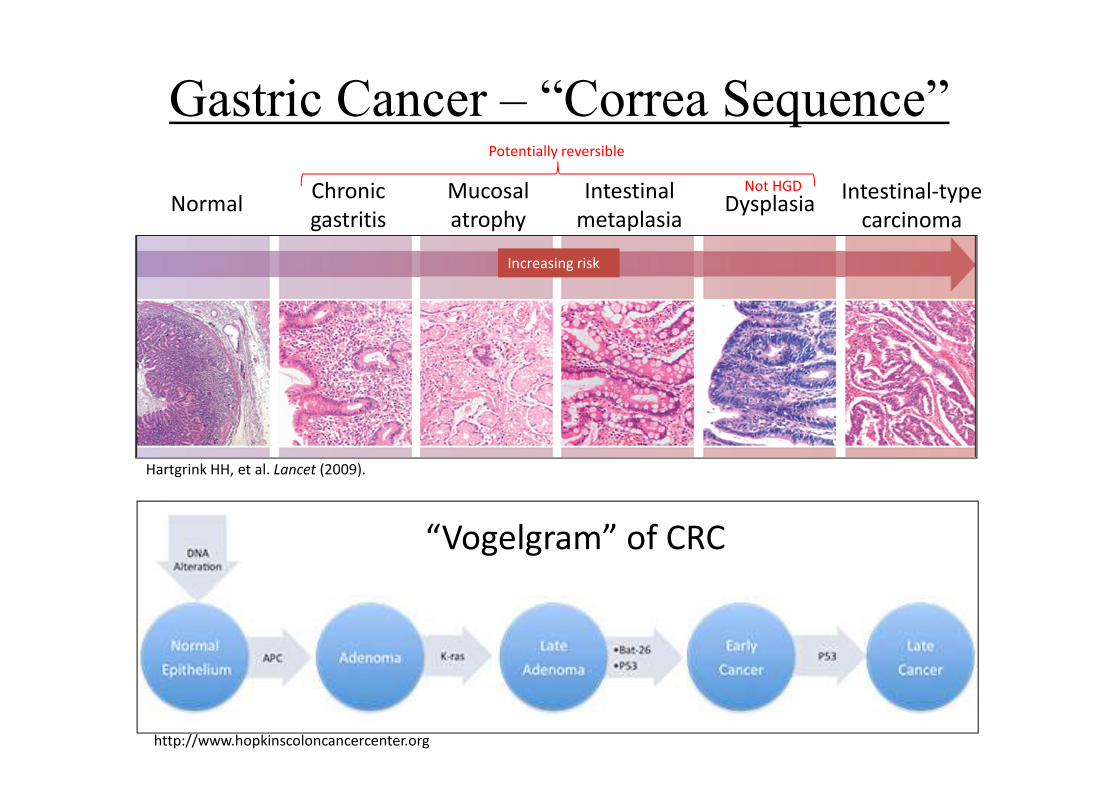
Gastric Cancer – “Correa Sequence”
“Vogelgram” of CRC
http://www.hopkinscoloncancercenter.org
Increasing risk
NormalChronic
gastritis
Mucosal
atrophy
Intestinal
metaplasia
Intestinal-type
carcinomaDysplasia
Potentially reversible
Not HGD
Hartgrink HH, et al. Lancet (2009).
Gastric Cancer - Pathogenesis
• H. pylori (HP) is main pathogenic factor in development of chronic AG and IM (AG risk: 1-3%/yr of infection)
• Classified as class I carcinogen by WHO in 1994– Plays role in ∼ 60% of gastric ca cases
• Atrophic gastritis and IM may regress after HP eradication – Healthy carriers don’t have ↓ gastric ca post-eradication– Those with premalignant lesions do � ? “point of no return”
• Only 1-2% of HP-infected pts develop gastric ca (2-3-fold increased risk)
Tan YK and Fielding JWL. Eur J Gastroenterol and Hepatol (2006).Vauhkonen M, et al. Best Prac & Res Clin Gastroenterol (2006).
Carl-McGrath S, et al. Cancer Therapy (2007).Sleisenger and Fordtran (9th Edition)
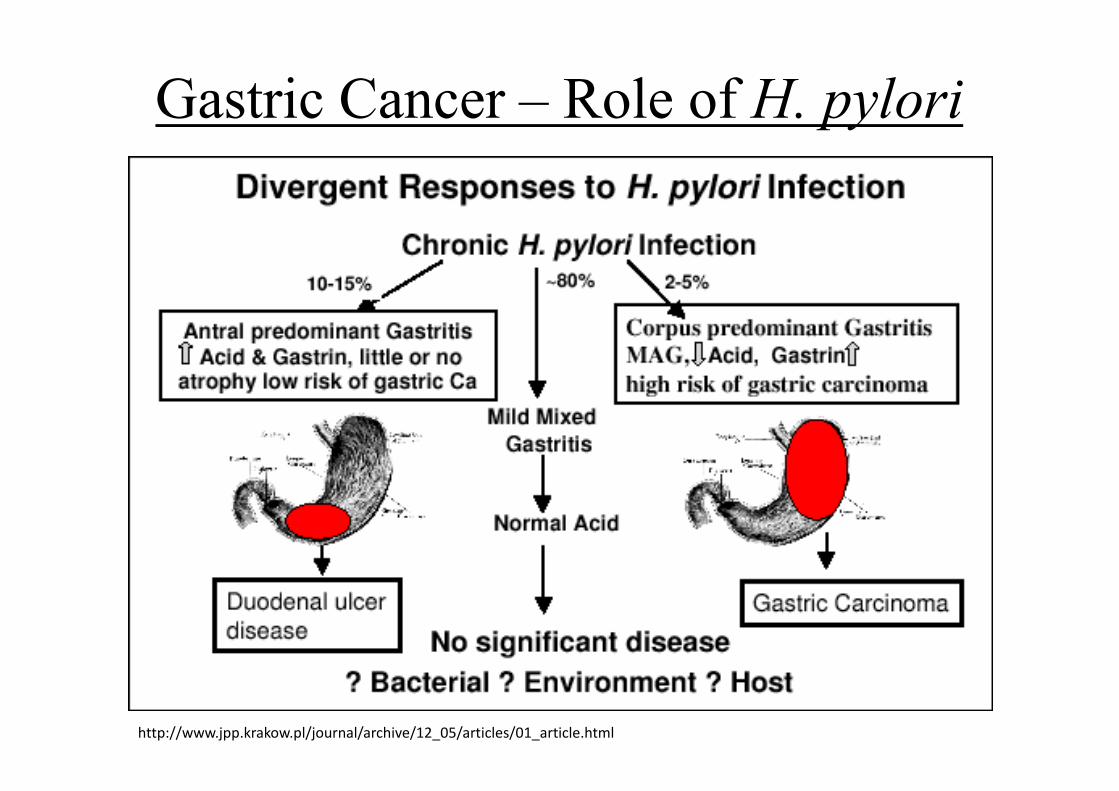
Gastric Cancer – Role of H. pylori
http://www.jpp.krakow.pl/journal/archive/12_05/articles/01_article.html
Gastric Cancer – Clinical Presentation
• Initial diagnosis usually delayed due to lack of early symptoms
– Only 50% have non-specific GI sxs (i.e. dyspepsia) �indistinguishable from benign disease
– Sxs may improve with PPI (“healing” of malignant ulcer � up to 37% have ca missed on EGD)
– Should withhold PPI for new dyspeptic sxs in pts > 45 y.o. until after EGD
• Up to 90% of Western gastric ca pts first present with advanced cancer
Carl-McGrath S, et al. Cancer Therapy (2007).Tan YK and Fielding JWL. Eur J Gastroenterol and Hepatol (2006).
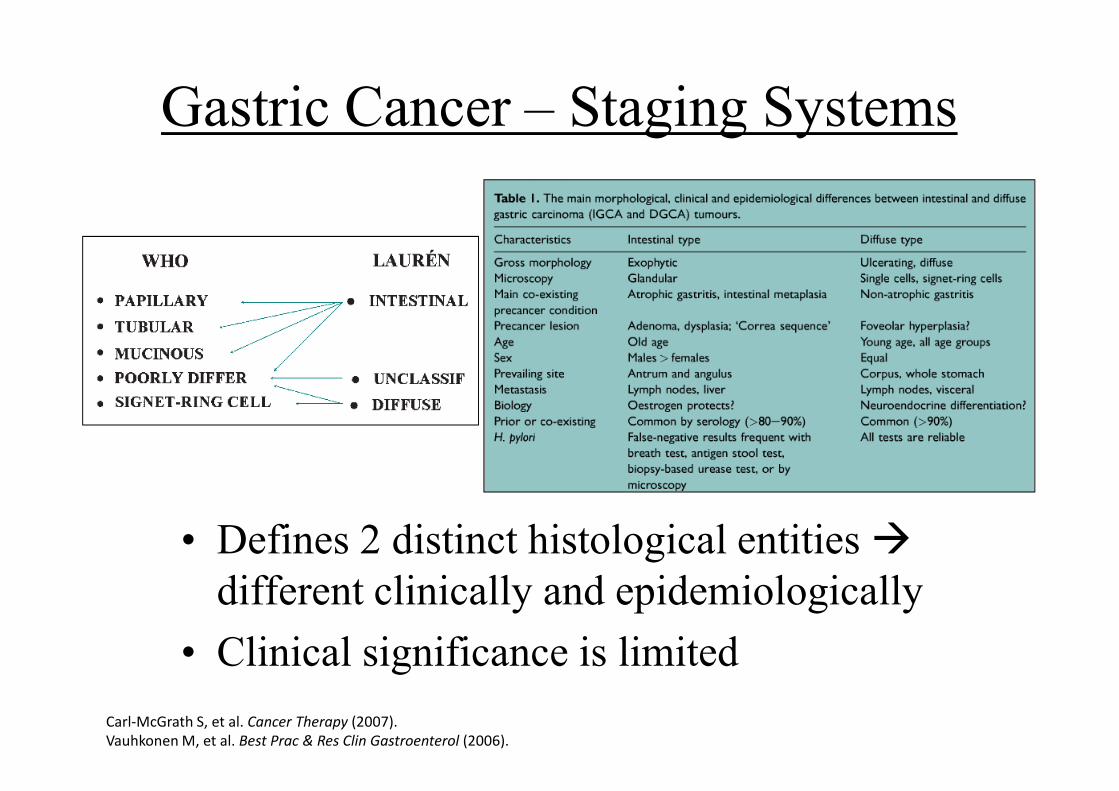
Gastric Cancer – Staging Systems
• Defines 2 distinct histological entities �
different clinically and epidemiologically
• Clinical significance is limited
Carl-McGrath S, et al. Cancer Therapy (2007).
Vauhkonen M, et al. Best Prac & Res Clin Gastroenterol (2006).
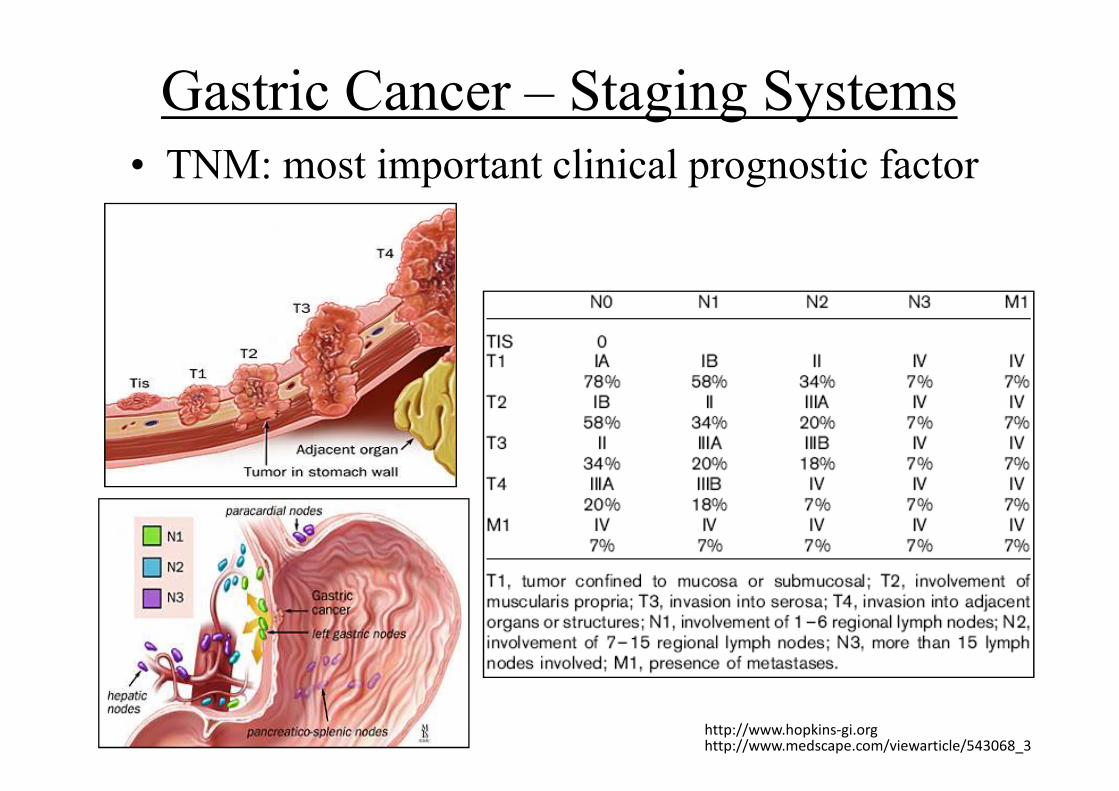
Gastric Cancer – Staging Systems
• TNM: most important clinical prognostic factor
http://www.hopkins-gi.orghttp://www.medscape.com/viewarticle/543068_3
Spread
•Multicentricity characterizes up to 20% of gastric cancers.
•Direct extension (lesser and greater omentum, liver and
diaphragm, spleen, pancreas, transverse colon)
•regional and distant nodal metastases:perigastric, gastroepiploic,
and porta hepatis lymphnode regions
•hematogenous metastases (liver, lungs, bone, brain); and
peritoneal metastases.
Pathology
• Adenocarcinoma is the predominant form: 95%– Subtypes: intestinal or diffuse; mixed types (rare). Often preceded by
intestinal metaplasia.
– Diffuse-type cancers are composed of infiltrating gastric mucous cells that infrequently form masses or ulcers.
• Primary lymphoma of the stomach is increasing in frequency
• Stromal tumors GI stromal tumors (GISTs) are mesenchymal tumors of the GI tract, most commonly arising from the stomach. GISTs commonly express KIT (CD117)
• Other histologic types Infrequently, squamous cell carcinomas, small-cell carcinomas, and carcinoid tumors. Metastatic spread of disease from primaries in other organs(eg, breast cancer and malignant melanoma) is also seen occasionally.
Prognostic factors
• Stage, PFS
• Patients with cancers of the diffuse type fare worse than those with intestinal-type lesions.
• Aneuploidy may predict a poor prognosis in patients with adenocarcinoma of the distal stomach.
• High plasma levels of vascular endothelial growth factor (VEGF) and the presence of carcinoembryonic antigen (CEA) in peritoneal washings predict poor survival in surgically resected patients.
• As with colorectal cancer, intratumoral levels of dihydropyrimidine dehydrogenase (DPD) may be prognostic of gastric cancer. Low levels appear to predict better response to fluorouracil (5-FU)–base chemotherapy and longer survival.
Diagnose• Anamnesis: gastric diseases, GERD,
gastritis, ulcus, polyp, very salty, spicy dietmight dispose, helicobacter pylory?
• Physical examinations: loss of weight, hindered gastric discharge, pain
• Endoscopy: gastroscopy
• Imaging: gastric rtg?,
• abdominal UH/CT
chest rtg, chest CT
Biopsy, histology
• Labors
Screening and diagnosis
• Screening is effective in high-incidence areas. Mass screening, as has been practiced in Japan since the 1960s, has probably contributed to the 2.5-fold improvement in long-term survival compared with Western countries, though differences in biology may also play a role.
• Endoscopy.
• CT scan Once a diagnosis has been established and careful physical examination and routine blood tests have been performed, a CT scan of the chest, abdomen, and pelvis
• Endoscopic ultrasonography (EUS)
• Capsule video endoscopy A capsule containing a tiny camera is swallowed by the patient. 2 pictures per second are taken. The capsule can be especially helpful in imaging the small intestine.
• Laparoscopy Laparoscopy is particularly suited to detect small-volume visceral and peritoneal metastases missed on CT prior to curative intent locoregional - or preoperative CRT
• PET scan may be used to show metastatic disease and may also be helpful in assessing response to neoadjuvant therapy.
Gastric Cancer - Treatment
• For Tis, studies have shown > 95% 5- and 10-yr survival with endoscopic resection
• Lap gastrectomy recommended for T1N0/T2N0 � scarce long-term data
• Pre- and post-op XRT doesn’t change survival
• Adjuvant/neoadjuvant chemo has minimal survival benefit– May benefit pts with advanced gastric ca
• Post-op chemo/XRT might improve survival
Hartgrink HH, et al. Lancet (2009).
Gastric Cancer – The Japan Story
• In 1960, gastric ca accounted for 51.6% of deaths
in men and 38.4% in women
• Mass screening program started for > 40 y.o.
• Significant increase in diagnosis of early gastric ca
and improved survival
• Now 60% of gastric cancers are diagnosed as early
cancers (10-20% in Western countries)Tan YK, et al. Eur J Gastroenterol & Hepatol (2006).
Is Gastric Cancer Preventable?
• Preceded by very prolonged latency period
• Precancerous cascade exists (IGCA)
• H. pylori is responsible for majority of gastric ca.
• Serum markers show some relation with cancer risk
– Pepsinogen: ↓ levels associated with atrophic gastritis
– HP Abs: Screening tool for dyspeptic pts < 45 y.o. (sens
97%, spec 87%) � if Ab neg, pt doesn’t need EGD
Tan YK and Fielding JWL. Eur J Gastroenterol and Hepatol (2006).Correa P. Gut (2004).
Radical surgery
• Radical surgery
– Distal tumors: subtotal gastrectomy
– In all other localisation: total gastrectomy
• Lymphadenectomy (LA):
– limited (D1),
– extended (D2)
• min. 15 lgl.
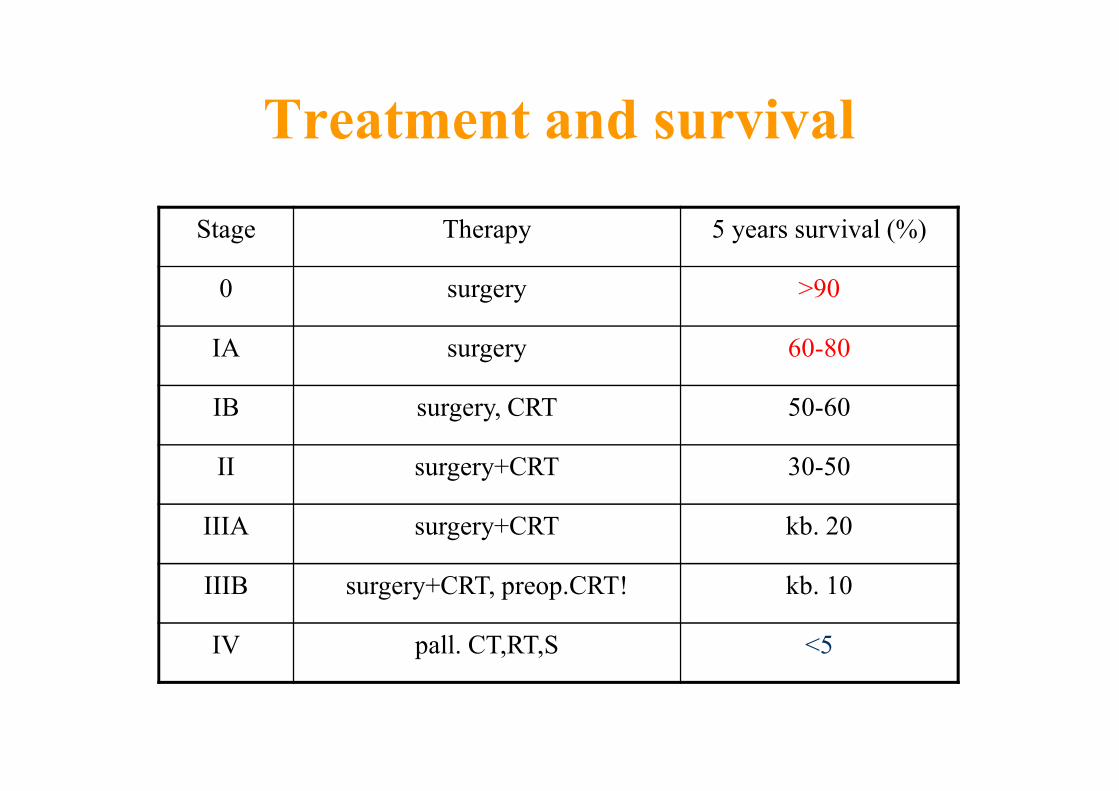
Treatment and survival
Stage Therapy 5 years survival (%)
0 surgery >90
IA surgery 60-80
IB surgery, CRT 50-60
II surgery+CRT 30-50
IIIA surgery+CRT kb. 20
IIIB surgery+CRT, preop.CRT! kb. 10
IV pall. CT,RT,S <5
43
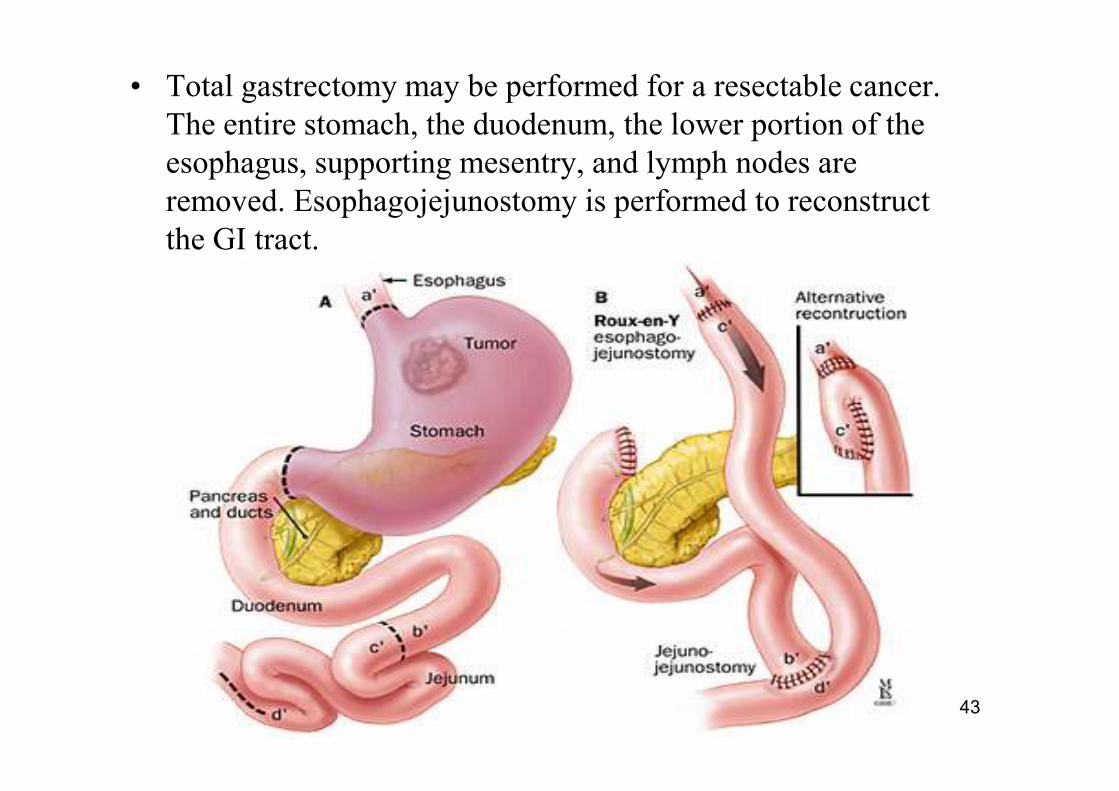
• Total gastrectomy may be performed for a resectable cancer.
The entire stomach, the duodenum, the lower portion of the
esophagus, supporting mesentry, and lymph nodes are
removed. Esophagojejunostomy is performed to reconstruct
the GI tract.
Neoadjuvant Chemotherapy
MAGIC Trial
• Evaluate the efficacy of preoperative and postoperative ECF vs. surgery alone
• 503 patients, stage II or greater
• Adenocarcinoma stomach/ge junction/distal esophagus
• ECF was chosen secondary to high RR in two prior randomized trials for locally advanced and metastatic gastric cancer
Schema
Arm A Surgery alone-(type of surgery and extent
of nodal dissection left to discretion of surgeon)
Arm B ECF x 3 -> surgery -> ECF x 3
Epirubicin (50mg/m2) D1
Cisplatin (60mg/m2) D1
Fluorouracil (200mg/m2) CIVI D1-21
Cycles q3weeks
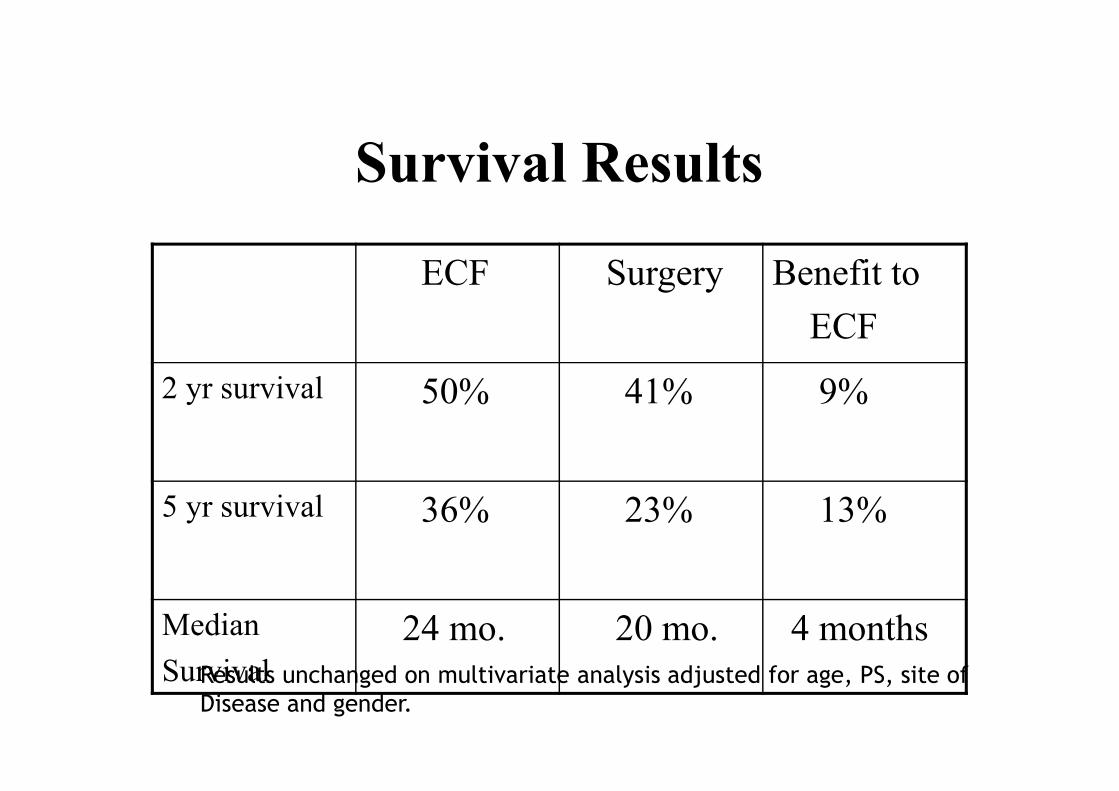
Survival Results
ECF Surgery Benefit to
ECF
2 yr survival 50% 41% 9%
5 yr survival 36% 23% 13%
Median
Survival
24 mo. 20 mo. 4 months
Results unchanged on multivariate analysis adjusted for age, PS, site of
Disease and gender.
Conclusions for Magic Trial
• First trial with neoadjuvant chemotherapy to show PFS/OS benefit
• Pathologic staging showed improvement in downsizing of primary tumor
• Chemotherapy tolerated fairly well
• Value of post-operative chemotherapy unknown (only 42% completing tx)
• Follow-up study: Magic B planned comparing ECX perioperative with ECX +bevacizumab perioperative.
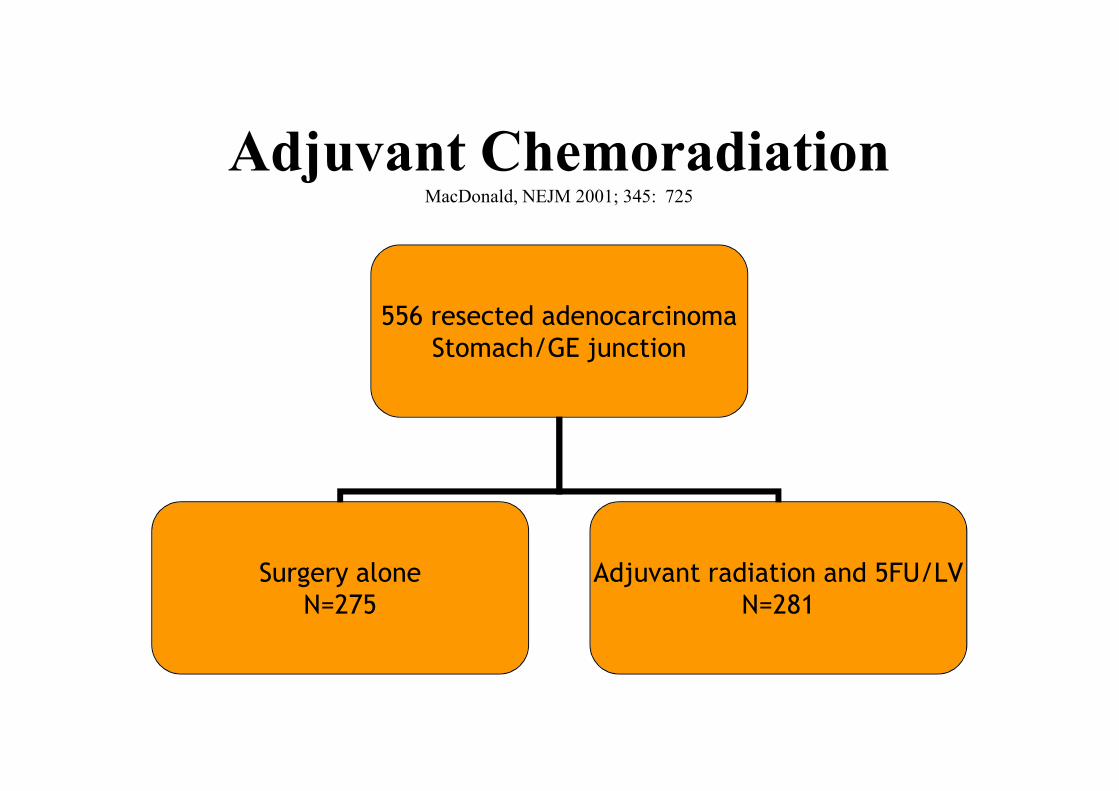
Adjuvant ChemoradiationMacDonald, NEJM 2001; 345: 725
556 resected adenocarcinoma
Stomach/GE junction
Surgery alone
N=275
Adjuvant radiation and 5FU/LV
N=281
Results-Median f/u 5 YearsMacDonald NEJM 2001; 345: 725
• Median OS:
Surgery alone - 27 months
Chemoradiation - 36 months (p<0.005)
• DFS:
Surgery alone – 19 months
Chemoradiation – 30 months (p<0.001)
• Pivotal trial establishing chemoradiation as standard of care in United States
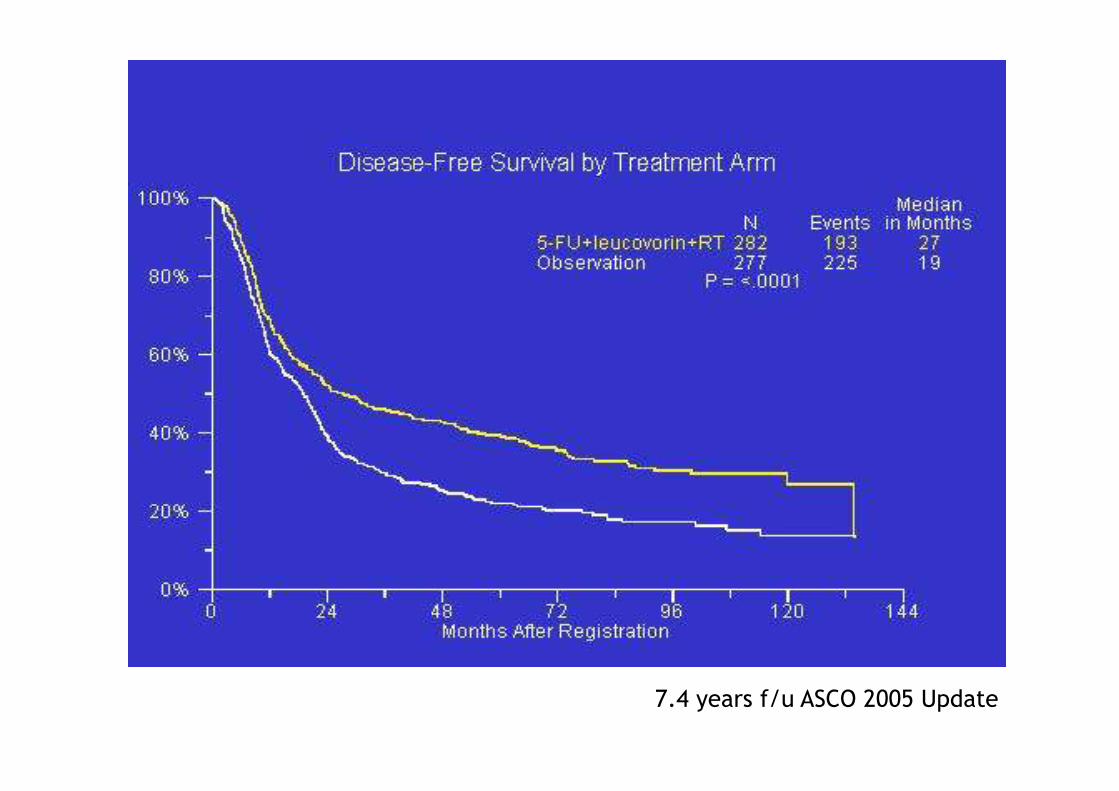
7.4 years f/u ASCO 2005 Update
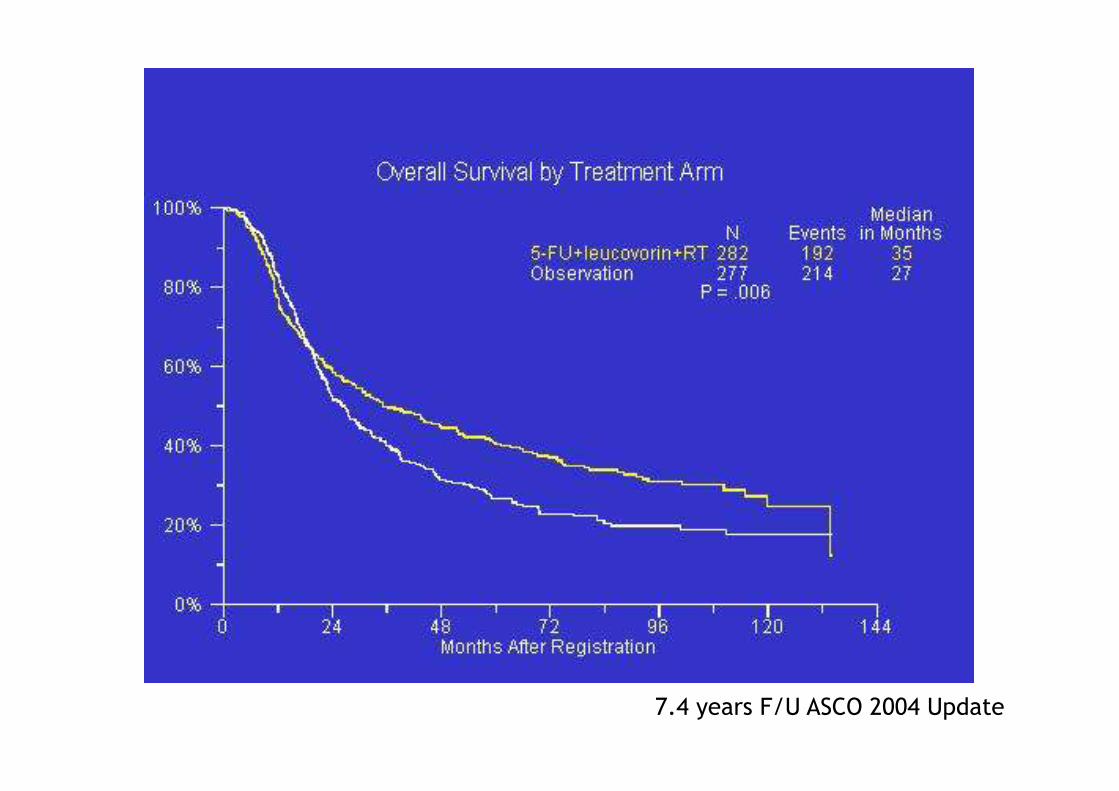
7.4 years F/U ASCO 2004 Update
• Subgroup analysis showed the benefit of
adjuvant chemoradiation did not differ with
regards to:
T stage
N stage
Tumor location-proximal vs. distal
Extent of LN dissection D0 vs. D1 vs. D2
Difficulties in irradiation planning
• Definiotion of target volume (GV):
– tumorbed
– anastomosis
– regional lymphnodes
• perigastrical, around the a. coeliaca, hepatoduodenal,
peripancreatic, periaortic, lien hylus, hepatic portal,
paraoesophageal
• Reduced ratiation tolerance of the surrounding
healthy tissues (liver, bowels, kidney, spinal
cord)
Method - KT
• Chemotherapy - 4 cycle – in each 4 weeks
5-FU 425 mg/m2, LV 20 mg/m2
1-5. day,
1-1 cycle before and after RT
5-FU 400 mg/m2, LV 20 mg/m2
1-4. and 1-3. days,
1. and 5. weeks of RT
Method - RT• Radiotherapy:
– CT- based 3D radiation planning
– CTV, PTV definition
– Dose-limits for organs at risk
– CT- based simulation
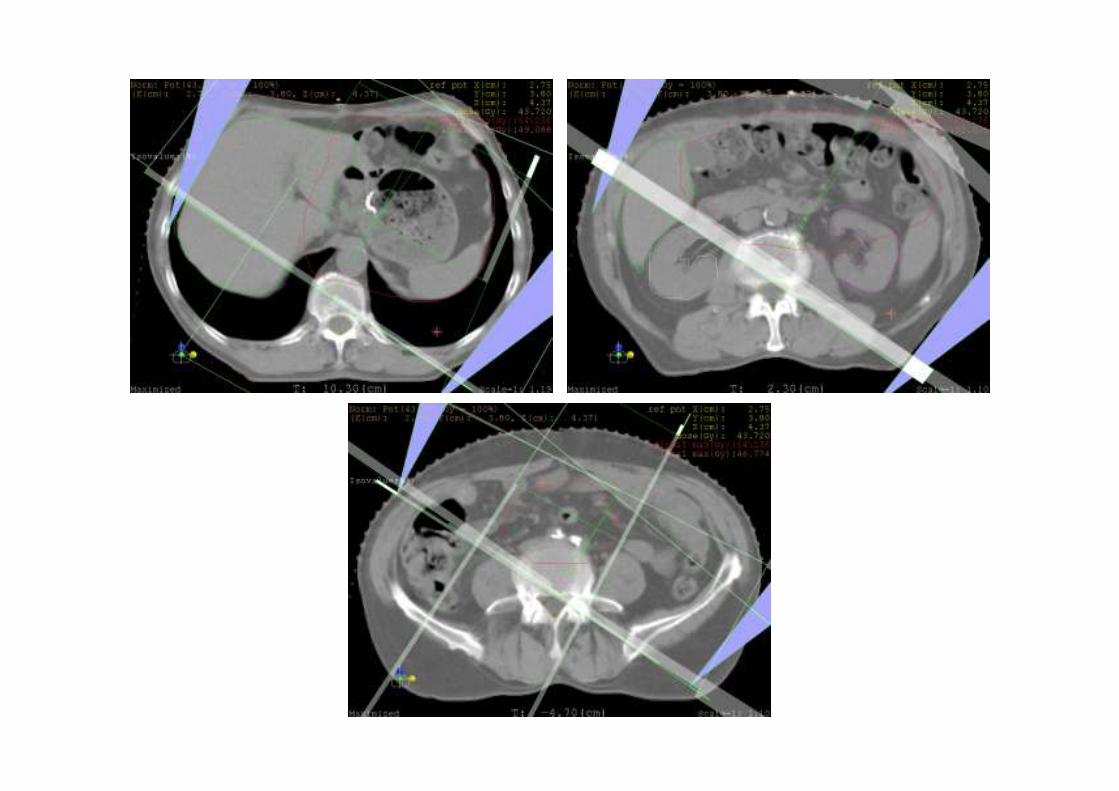
– Conformal 15 MV fotonfields
– Dose: 25x1,8 = 45 Gy
• No. of fields: 4,9±1,8 (3-8)
• Dose homogenity (-5,+7%): 90±3 (85-95%)
• Remark: camera-renography is performed at each patient because of theexpected late nephrotoxicity!
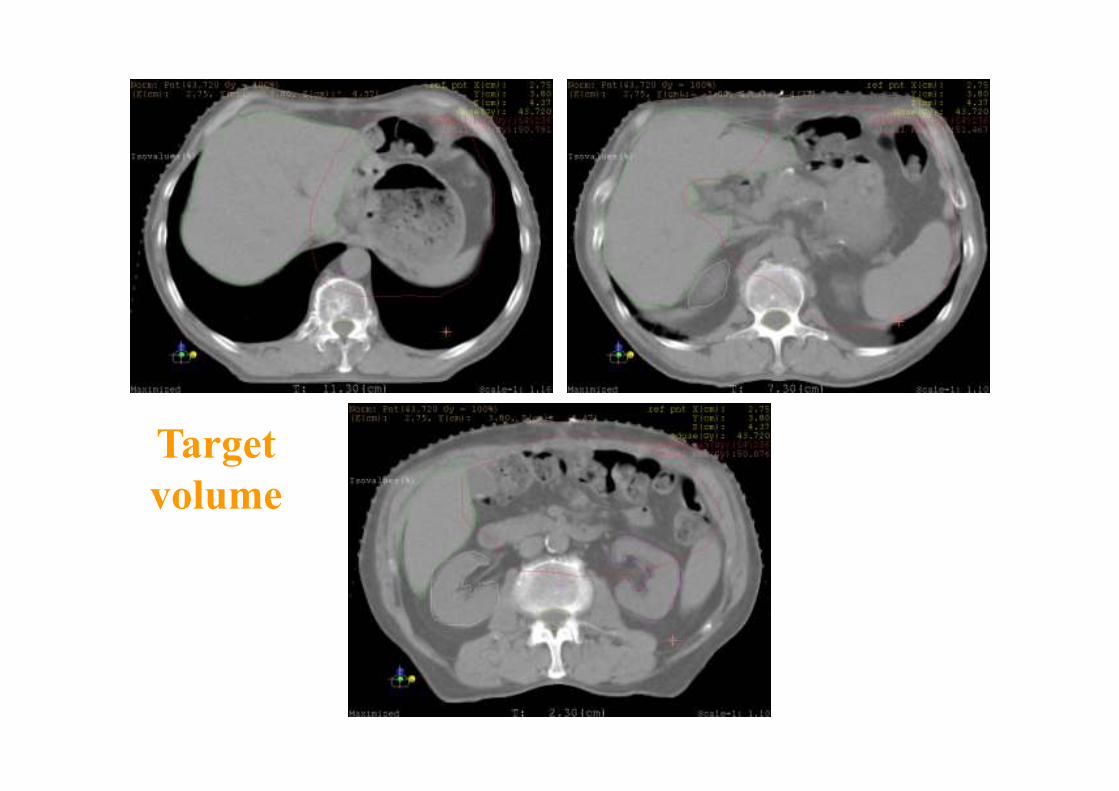
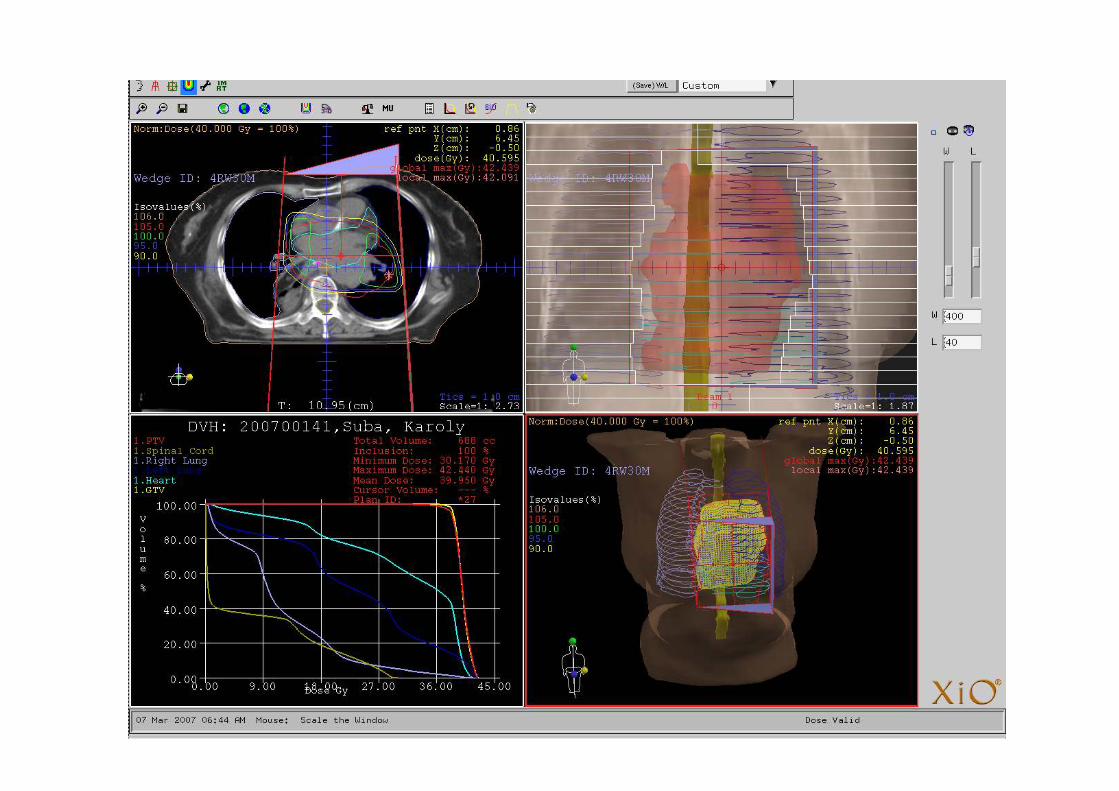
Target
volume
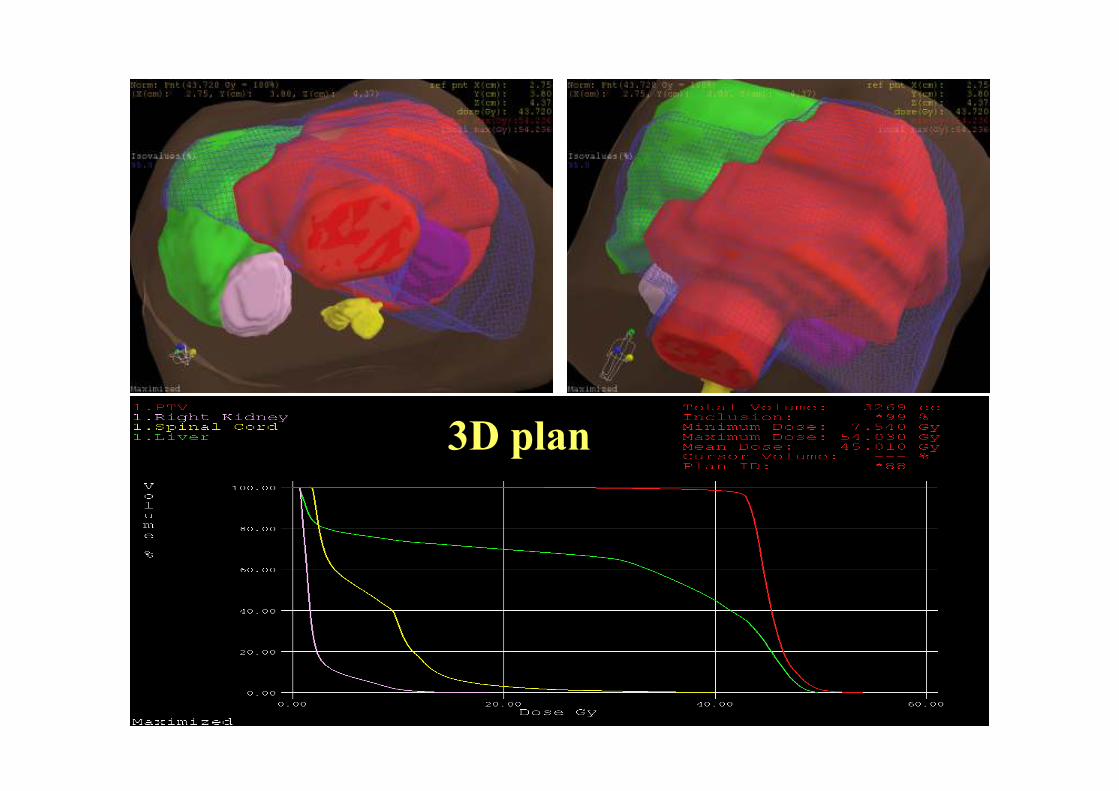
3D plan
Palliative therapy
• In the case of inoperability:– RT: 45-50,4 Gy, + 5-FU
– CTX
• Palliative CTX for metastatic tumor
– FAM (5FU-Adriamycin-Mitomycin) /gold standard in the
years of 1980/
– 5FU-Cisplatin
– Xeloda-Cisplatin
– ELF (Etopozid-LV-5FU)
– Mono-Xeloda
New CTX agents
• Campto (irinotecan):topoizomerase
inhibitor
• Taxánok: docetaxel, paclitaxel
• Oxaliplatin: 3. generation of platina
• Xeloda (capecitabine): oral 5FU-prodrug
• Biological response modifyers
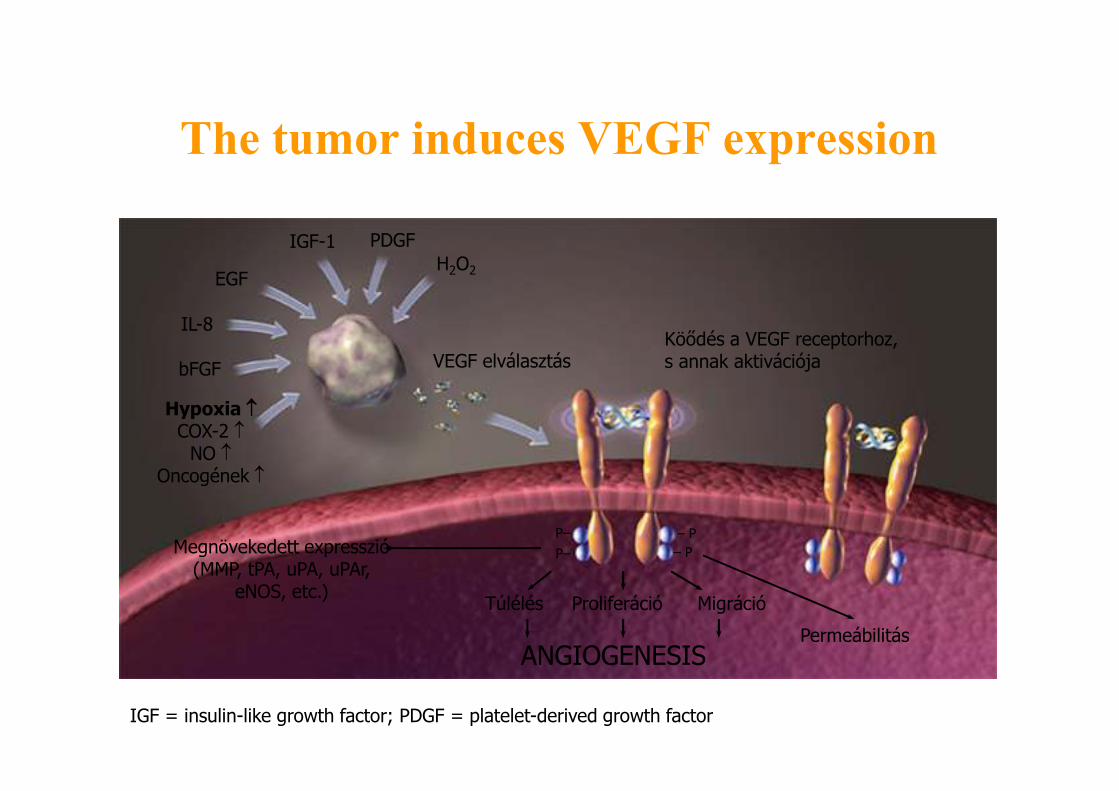
The tumor induces VEGF expression
EGF
IGF-1 PDGF
IL-8
bFGF
Hypoxia ↑↑↑↑COX-2 ↑
NO ↑Oncogének ↑
VEGF elválasztásKöődés a VEGF receptorhoz,s annak aktivációja
H2O2
ProliferációTúlélés Migráció
ANGIOGENESISPermeábilitás
Megnövekedett expresszió(MMP, tPA, uPA, uPAr,
eNOS, etc.)
– P
– P
P–
P–
IGF = insulin-like growth factor; PDGF = platelet-derived growth factor
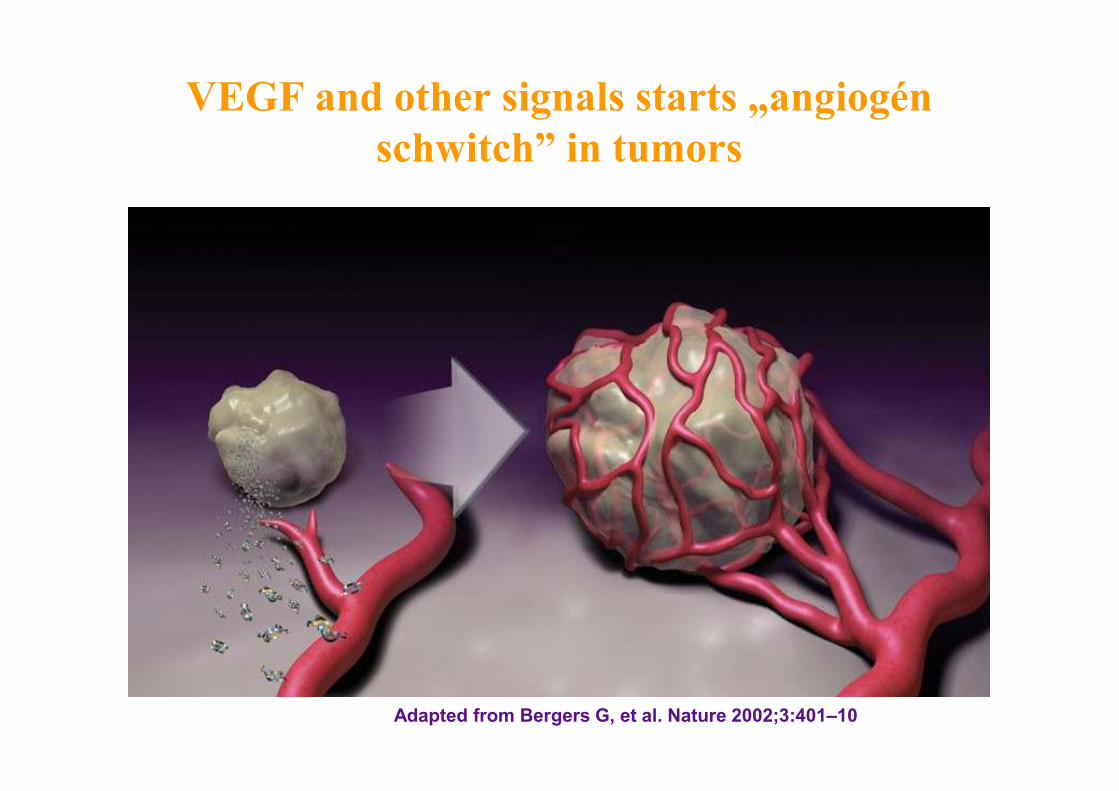
VEGF and other signals starts „angiogén
schwitch” in tumors
Adapted from Bergers G, et al. Nature 2002;3:401–10
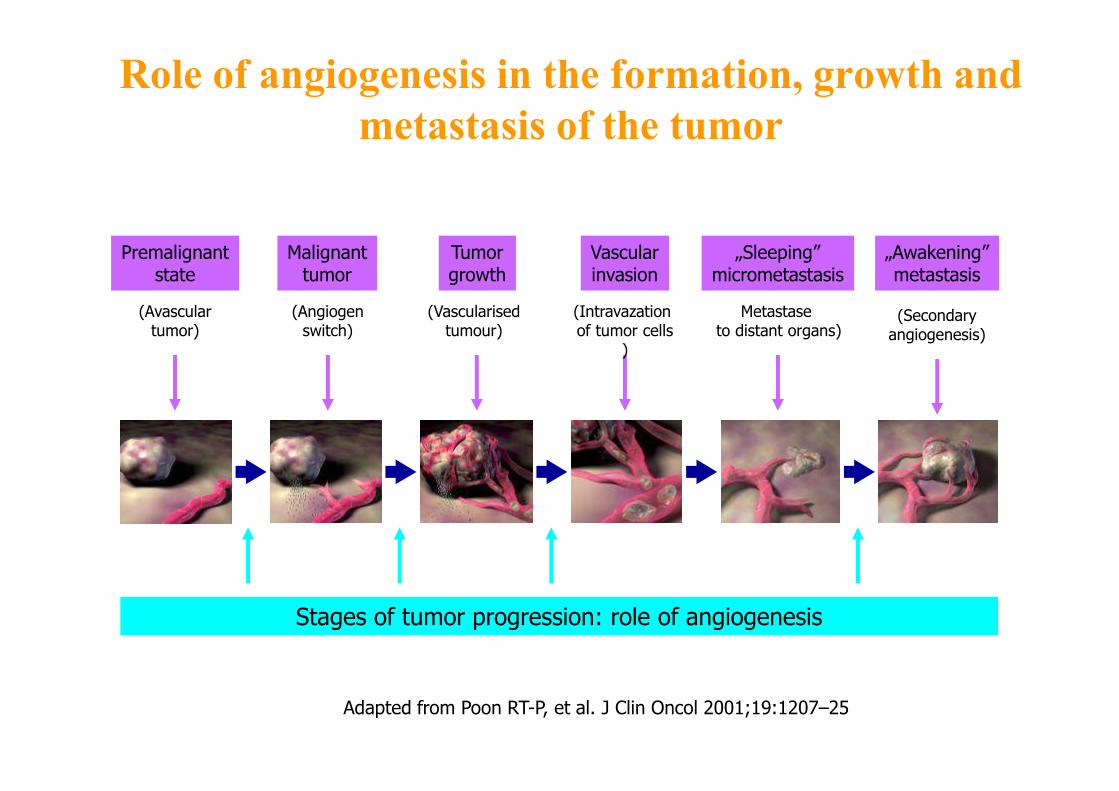
Role of angiogenesis in the formation, growth and
metastasis of the tumor
Adapted from Poon RT-P, et al. J Clin Oncol 2001;19:1207–25
Stages of tumor progression: role of angiogenesis
Premalignantstate
Malignanttumor
Tumorgrowth
Vascularinvasion
„Sleeping”micrometastasis
„Awakening”metastasis
(Avasculartumor)
(Angiogenswitch)
(Vascularisedtumour)
(Intravazationof tumor cells
)
Metastaseto distant organs)
(Secondaryangiogenesis)
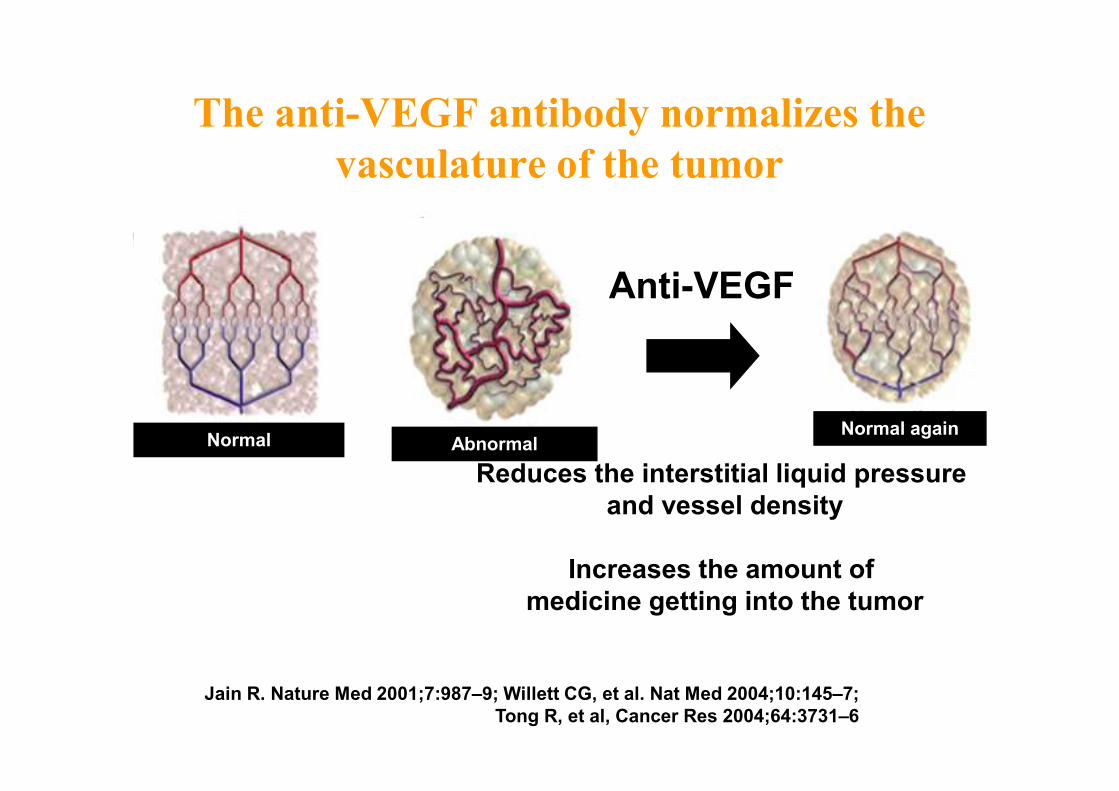
Anti-VEGF
Reduces the interstitial liquid pressure
and vessel density
Increases the amount of
medicine getting into the tumor
The anti-VEGF antibody normalizes the
vasculature of the tumor
Jain R. Nature Med 2001;7:987–9; Willett CG, et al. Nat Med 2004;10:145–7;
Tong R, et al, Cancer Res 2004;64:3731–6
NormalNormal again
Abnormal





























