Embed Size (px)
Citation preview

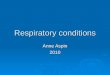
Oesophageal Atresia

Complete obliteration or discontinuity of the lumen.
Esophagus divided into a upper(proximal) & a lower(distal) pouch
May or may not be associated with a tracheal fistula

Types
A B

C D ECommonest (90%)

Abnormal pathology
•Blind upper pouch
•Fistula between trachea & distal pouch
Resulting problems
•Aspiration – saliva/milk
•Pneumonia
•Distension of stomach
•Gastroesophageal reflux – chemical pneumonitis

Antenatal history
• polyhydramnios

Clinical features
-Antenatal – polyhydramnios
-Drooling of saliva
-if fed, milk regurgitates
-Respiratory distress
-Abdominal distension

Diagnosis

Pre op Treatment
•Upper pouch suction•Antibiotics •Head end elevation to prevent reflux
•Respiratory support

Surgery •Thoracotomy(Rt.)
Ligation of fistula
Esophageal end to end anastomosis

Surgery• If gap between the 2 esophageal ends
is too much then we have to divert
•Cervical esophagostomy- outlet for saliva•Gastrostomy- for feeding •Esophageal replacement when the child is about older

Prognosis•Birthweight•Associated anomalies – VACTERL•pneumonia

Long term
•Stenosis•Motility problems

CONGENITAL DIAPHRAGMATIC HERNIA

Development of diaphragm
• Septum transversum
• Pleuroperitoneal membrane
• Esophageal mesentery
• Mesoderm of body wall

If diaphragm not developed completely
Bowel that is returning into abdominal cavity enters thoracic cavity
Impaired development of lungs

• Can be detected antenatally
• Prognosis is worse if it is diagnosed before 24 weeks, stomach in chest

Clinical features
• Respiratory distress- cyanosis, tachpnoea, tachycardia, sternal retraction
• Scaphoid abdomen
• Pseudo dextrocardia
• Absent breath sounds on left side

hypoxia
Pulmonary vasoconstriction
Pulmonary hypertension
Persistent fetal circulation (R to L shunt)

Diagnosis


Treatment
• Physiological emergency
• May need ventilatory support & stabilization
• Control pulmonary hypertension

Surgical treatment
• Laparotomy & repair of the defect


Newer treatment options
• Antenatal – PLUG therapy
• Post natatally – liquid ventilation, high frequency ventilation