Embed Size (px)
Citation preview

June 2020HK$ 100
www.hkma.org
LIVECME
持 續 醫 學 進 修 專 訊
B U L L E T I N
Immunotherapy for
Allergic Rhinitis –
Current Status
Dr. CHOW Chun Kuen

Editorial 2
Spotlight 4Immunotherapy for Allergic Rhinitis – Current Status
Cardiology 9Exertional Dyspnea In Patient With Known Heart Murmur
Dermatology 11Pigmented Mole on right post-auricular region
Answer Sheet 12CME Notifications 14Meeting Highlights 15CME Calendar 17
Contents
The Hong Kong Medical Association is dedicated to providing a coordinated CME programme for all members of the medica l profess ion. Under the HKMA CME Programme, a CME registration process has been created to document the CME efforts of doctors and to provide special CME avenues. The Association strives to foster a vibrant environment of CME throughout the medical profession. Both members as well as non-members of the Association are welcome to join us. You may contact the HKMA Secretariat for details of the programme.
HKMA CME Programme or CME Bulletin Advertising Enquiry
Tel: 2527 8452Fax: 2865 0943Email: [email protected]: 5/F, Duke of Windsor Social Service
Building, 15 Hennessy Road, Hong KongWebsite: www.hkma.org
Please read the articles and answer the questions. Pa r t i c ipan ts i n the HKMA CME Programme w i l l be awarded cred i t po in ts under the Programme for return ing the completed answer sheet v ia fax (2865 0943) or by mail to the HKMA Secretariat on or before submission deadline. Questions may also be answered online at www.hkma.org. Answers to questions will be provided in the next issue of the HKMA CME Bulletin.
HKMA CME Bulletin – MONTHLY SELF-STUDY SERIES to help you grow!
NOTICEMedical knowledge is constantly changing. Standard safety precautions must be followed, but as new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may become necessary or appropriate. Readers are advised to check the most current product information provided by the manufacturer of each drug to be administered to verify the recommended dose, the method and duration of administration, and contraindications. It is the responsibility of the practitioner, relying on experience and knowledge of the patient, to determine dosages and best treatment for each individual patient. Neither the Publisher nor the Authors assume any liability for any injury and/or damage to persons or property arising from this publication.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of it by its manufacturer.
No parts of articles can be reproduce without the express permission of the editor.
CME Bulletin & Online Editorial Board
Chief EditorDr. LAM Ho 林賀醫生Dr. WONG Bun Lap, Bernard 黃品立醫生
Executive CommitteeDr. CHAN Yee Shing, Alvin 陳以誠醫生Dr. CHENG Chi Man 鄭志文醫生Dr. CHEUNG Hon Ming 張漢明醫生Dr. CHOI Kin 蔡 堅醫生Dr. HO Chung Ping, MH, JP 何仲平醫生Dr. HO Hung Kwong, Duncan 何鴻光醫生Dr. LAM Tzit Yuen, David 林哲玄醫生Dr. LI Sum Wo, MH 李深和醫生Dr. TSE Hung Hing, JP 謝鴻興醫生
CardiologyDr. CHEN Wai Hong 陳偉康醫生Dr. HO Hung Kwong, Duncan 何鴻光醫生Dr. LEE Pui Yin 李沛然醫生Dr. LI Siu Lung, Steven 李少隆醫生Dr. WONG Bun Lap, Bernard 黃品立醫生Dr. WONG Shou Pang, Alexander 王壽鵬醫生Dr. WONG Wai Lun, Warren 黃煒倫醫生
Cardiothoracic SurgeryDr. CHENG Lik Cheung 鄭力翔醫生Dr. CHIU Shui Wah, Clement 趙瑞華醫生Dr. CHUI Wing Hung 崔永雄醫生Dr. LEUNG Siu Man, John 梁兆文醫生
Colorectal SurgeryDr. CHAN Cheung Wah 陳長華醫生Dr. LEE Yee Man 李綺雯醫生Dr. TSE Tak Yin, Cyrus 謝得言醫生
DermatologyDr. CHAN Hau Ngai, Kingsley 陳厚毅醫生Dr. HAU Kwun Cheung 侯鈞翔醫生
EndocrinologyDr. LEE Ka Kui 李家駒醫生Dr. LO Kwok Wing, Matthew 盧國榮醫生
ENTDr. CHOW Chun Kuen 周振權醫生
Family MedicineDr. LAM King Hei, Stanley 林敬熹醫生Dr. LI Kwok Tung, Donald, SBS, JP 李國棟醫生
GastroenterologyDr. NG Fook Hong 吳福康醫生
General PracticeDr. YAM Chun Yin 任俊彥醫生
General SurgeryDr. LAM Tzit Yuen, David 林哲玄醫生Dr. LEUNG Ka Lau 梁家騮醫生
Geriatric MedicineDr. KONG Ming Hei, Bernard 江明熙醫生Dr. SHEA Tat Ming, Paul 佘達明醫生
HaematologyDr. AU Wing Yan 區永仁醫生Dr. MAK Yiu Kwong, Vincent 麥耀光醫生
Hepatobiliary SurgeryDr. CHIK Hsia Ying, Barbara 戚夏穎醫生Dr. LIU Chi Leung 廖子良醫生
Medical OncologyDr. TSANG Wing Hang, Janice 曾詠恆醫生
NephrologyDr. CHAN Man Kam 陳文岩醫生Dr. HO Chung Ping, MH, JP 何仲平醫生Dr. HO Kai Leung, Kelvin 何繼良醫生Dr. LAM Man Fai 林萬斐醫生Dr. LEE Hoi Kan, Achillers 李海根醫生
NeurologyDr. FONG Chung Yan, Gardian 方頌恩醫生Dr. TSANG Kin Lun, Alan 曾建倫醫生
NeurosurgeryDr. CHAN Ping Hon, Johnny 陳秉漢醫生
Obstetrics and GynaecologyDr. CHAN Kit Sheung 陳潔霜醫生
OphthalmologyDr. LIANG Chan Chung, Benedict 梁展聰醫生Dr. PONG Chiu Fai, Jeffrey 龐朝輝醫生
Orthopaedics and TraumatologyDr. IP Wing Yuk, Josephine 葉永玉醫生Dr. KONG Kam Fu 江金富醫生Dr. POON Tak Lun 潘德鄰醫生Dr. TANG Yiu Kai 鄧耀楷醫生
PaediatricsDr. CHAN Yee Shing, Alvin 陳以誠醫生Dr. TSE Hung Hing, JP 謝鴻興醫生Dr. YEUNG Chiu Fat, Henry 楊超發醫生
Plastic SurgeryDr. NG Wai Man, Raymond 吳偉民醫生
PsychiatryDr. LAI Tai Sum, Tony 黎大森醫生Dr. LEUNG Wai Ching 梁偉正醫生Dr. WONG Yee Him, John 黃以謙醫生
RadiologyDr. CHAN Ka Fat, John 陳家發醫生Dr. CHAN Yip Fai, Ivan 陳業輝醫生
Respiratory MedicineDr. LEUNG Chi Chiu 梁子超醫生Dr. WONG Ka Chun 黃家進醫生Dr. WONG King Ying 黃琼英醫生Dr. YUNG Wai Ming, Miranda 容慧明醫生
RheumatologyDr. CHAN Tak Hin 陳德顯醫生Dr. CHEUNG Tak Cheong 張德昌醫生
UrologyDr. CHEUNG Man Chiu 張文釗醫生Dr. KWOK Ka Ki 郭家麒醫生Dr. KWOK Tin Fook 郭天福醫生Dr. MAK Siu King 麥肇敬醫生
Vascular SurgeryDr. TSE Cheuk Wa, Chad 謝卓華醫生
HKMA SecretariatMs. Jovi LAM 林偉珊女士Miss Irene GOT 葛樂詩小姐Miss Ivy IP 葉珈甄小姐Mr. Jeff CHENG 鄭嘉信先生
持續醫學進修專訊HKMA CME Bulletin


EDITORIALCME in the period of COVID
It seems that we are adapting quite well to the new mode of CME in the period of COVID. The HKMA is providing
more lunch time seminars than ever before via Facebook Live. I hope that you can take the time to “attend” enough
of them so as not to worry about your CME points at the end of this year.
Well, I do miss the old days. By old days, I just mean a few months ago, maybe just last year. I miss the delicious
lunches at our Central Club House. I miss the round table discussion of relevant and of course irrelevant issues
before the lectures. I am looking forward of the return of such in the near future. We shall organize again “real” and
virtual lunch seminars in parallel.
For the web-based seminars, we are now mainly using Facebook Live. The CME team is constantly look at and
trying on other modalities of delivery of the seminars, including using Zoom and Webinar. Please take note of our
notices before joining the seminars and help trying on different modes of delivery.
Suggestions and feedbacks are welcome.
Dr. CHENG Chi Man
Chairman, CME Organizing Sub-Committee
Policy for HKMA CME Lecture Online Scheme
1. Doctors must have a Facebook Account to join the CME Lecture Online.2. Registration of Lecture will close 1 week before the lecture.3. Doctor could only view 1 LECTURE at one time only, if doctors are found to attend two CME Lectures that with
overlapping time period, only CME Points from 1 lecture will be recorded. Doctors might be penalized by the MCHK for non-compliance.
4. Doctors must watch the lecture at real time.5. Doctors MUST complete lecture quiz within 2 hours after the lecture. Late submission of the quiz will not be
accepted. 1 CME point will be awarded afterward.6. Registration can be done by scan the QR code on CME Bulletin Cover and complete the online form or registration
through HKMA website.7. You are recommended to connect to Wi-Fi on your mobile device or computer while watching the lecture through
Facebook Live. Unstable internet connection will cause interruption to your viewing.8. In case of technical issue and broadcast interruption, please be patient while our technicians will work on fixing the
problem; the video should resume in a few minutes.9. Due to copyright issue, the Facebook group is exclusive for doctors who have registered; and the video recording,
PowerPoint slides and quiz link MUST not be shared with non-registrants.

4 HKMA CME Bulletin 持續醫學進修專訊 June 2020 www.hkma.org
Spotlight
Dr. CHOW Chun KuenSpecialist in Otorhinolaryngology
Immunotherapy for Allergic Rhinitis – Current Status
Background
Allergic rhinit is (AR) is the commonest cause for nasal symptoms. Acute al lergic rhinit is is related to the mast cell release after exposure to specific allergen and causes rhinorrhea, sneezing, itchiness and watery eyes. Chronic allergic rhinitis presents with nasal obstruction, pain, and sinusitis, most related to mediators of cell response that result in cellular proliferation. Various studies suggest that the cumulative prevalence of rhinitis is about 10-20% of the population and shows an increasing trend. Allergic rhinitis often develops in children who already have some evidence of atopy. Severely atopic children trend to develop eczema in infancy, asthma at 5-10 years and rhinitis at 10-15 years-of-age. Untreated rhinitis results in interference with daily activit ies and impaired sleep quality. In Hong Kong, the most common cause of perennial allergic rhinitis is house dust mite (Dermatophagoides farina and Dermatophagoides pteronyssinus). The most desirable treatment is to identify the responsible al lergen and avoidance when possible. Pharmacotherapy can be used for symptomatic control if allergen avoidance is inadequate or not possible. In general practice surveys, a third of children and almost two thirds of adults report partial or poor response with pharmacotherapy for allergic rhinitis. (1, 2) Allergen immunotherapy (AIT) is indicated in severe allergic rhinitis that does not respond to conventional pharmacotherapy and allergen avoidance measures.
Introduction of specific allergen immunotherapy(AIT)
AIT or hyposensitization was introduced in 1911 for treatment of asthma and other al lergic diseases. AIT involves the repeated administration of specific allergen extracts to allergic individuals and thus induces tolerance to the allergen. This results in long-term relief of symptoms and improvement in quality of life during subsequent natural allergen exposure. It is the only treatment modality that has been shown to modify the underlying pathophysiology of the IgE mediated allergic disease, with long term benefits after cessation of the therapy. Selection of patients for AIT requires accurate identification of an underlying allergic symptoms trigger through a combination
of clinical history and skin and/or blood tests for allergen specific IgE. (Fig. 1) In our centre, house dust mite allergens attribute to 80% of the positive skin-prick testing for allergic rhinitis.
Figure 1. Allergen skin-prick testing for allergic rhinitis
Mechanism
Although evidences have shown AIT to be effect ive in symptoms control of patients with allergic rhinitis, the exact mechanism of how it works is not clear ly known. Both antibody-mediated and cell-mediated mechanisms have been found to be relevant. It was suggested that AIT stimulates the production of allergen-specific blocking IgG4 antibodies that affects the binding of allergen to the specific IgE antibody. It reduces the release of histamine and subsequent cellular responses, thus relieves the symptoms. However, the level of blocking IgG antibody generally does not correlate with the degree of clinical improvement or the efficacy of AIT. For the cell-mediated mechanism, recent studies showed that AIT induces Th1 lymphocytes cellular activity to increased production of cytokine and interferon, with the concomitant inhibition of Th2 cell proliferation. This in turn results in a decrease in allergic responses, such as eosinophilic infiltration, IgE production and mediators release. These events are accompanied by suppression of allergen-induced T cell-dependent late responses in the skin and lung and long-term disease suppression after discontinuation of treatment. In contrast to usual pharmacotherapy, AIT is the only treatment that has this potential to modify the course of allergic disease.

5HKMA CME Bulletin 持續醫學進修專訊 June 2020www.hkma.org
Spotlight
The mechanisms involved in sublingual AIT have been shown to be similar to those observed with subcutaneous AIT. Additional local immune modulating mechanisms are possibly involved in the sublingual region and draining lymph nodes of the nose and upper respiratory tract (3).
Methodology
Subcutaneous immunotherapy
Subcutaneous AIT should only be performed by trained staff in a specialist facility with immediate access to physician and resuscitation facilities. The standardized allergen extract injections are usually given in deep subcutaneous route at the outer surface of upper arm. (Fig. 2) Peak expiratory flow rate should be measured before and 30 minutes after injections. Any immediate (0-30 minutes) and delayed local or systemic reactions should be observed. Injections should be postponed in the presence of respiratory infection, concurrent illness, current asthma, or symptoms due to concomitant allergen exposure. AIT protocols, in general, involve weekly injections of escalated dose of allergen for 8-16 weeks during an induction phase, followed by monthly maintenance injections for a period of 3-5 years.
Figure 2. Deep subcutaneous injection of standardized allergen at the outer surface of upper arm
Sublingual immunotherapy
Sublingual AIT involves administration of standardized dose of allergen extracts of drops or tablets (Fig. 3) under the tongue with advice to retain for 2 minutes before swallowing. Food and beverage are not recommended for the following 5 minutes. The first dose should be taken in the specialist centre for observation of immediate reaction for a period of at least 30 minutes. Then it is followed by daily self-administration of sublingual drops or tablets at home. Administration should be postponed in presence of oral wound or inflammation and concurrent illness. Onset of clinical effect is expected in 8-14 weeks. The recommended maintenance treatment duration is 3 years for long term clinical benefit after cessation of treatment.
Effectiveness in allergic rhinitis
Systematic reviews in Cochrane Database have shown that subcutaneous AIT is highly effective in allergic rhinitis, in patients with seasonal pollen allergy (4) and also in patients with perennial house dust mites allergy(5). Clinical efficacy is demonstrated by a marked reduct ion in symptoms, requirements for anti-allergic medication and improvement of quality of life. In one randomized controlled trial of 410 patients with grass pollen allergy showed a 30% decrease in seasonal symptoms, a 44% reduction in usage of anti-allergic medication and a marked improvement in quality of life during the pollen season (6). AIT is effective in both seasonal and perennial disease.
A Cochrane systematic review and meta-analysis of 60 studies of which 49 (4589 participants) were suitable for pooled analysis (7) showed that sublingual AIT was effective for seasonal and perennial rhinitis. Recent randomized controlled tr ials of subl ingual tablet AIT have provided consistent evidence of efficacy with decreases in symptoms and rescue medication during the season, resulting in registration of two sublingual tablet vaccines in the USA (8,9). Three large trials of sublingual tablet AIT have been performed that included a total of 4022 participants with perennial rhinitis and IgE sensitivity to house dust mites (10-12) Tablets were taken daily for 12 months. All 3 trials showed evidence of efficacy in rhinitis with a clear dose response and an 18% to 28% reduction in combined symptom-medication scores compared with placebo-treated groups.
Long-Term benefit
AIT has been shown, in several studies, to confirm long-term benefit following discontinuation. In one double-blind placebo-controlled withdrawal study, 3-4 years grass pollen subcutaneous AIT was shown to result in long-term reduction in symptoms and rescue medication for at least 3 years
Figure 3. Sublingual immunotherapy tablets with a standardized dose of house dust mite allergen extract available in Hong Kong

6 HKMA CME Bulletin 持續醫學進修專訊 June 2020 www.hkma.org
Spotlight
following discontinuation (13). There is some evidence that AIT may reduce the onset of new allergen sensitivities in children (14, 15). In a prospective randomized controlled trial of pollen AIT in children with seasonal allergic rhinitis, development of asthma was followed up over a period of 10 years. In 2-7 years following cessation of immunotherapy, there was a persistent 2-3 fold reduction in the risk of development of physician-diagnosed asthma compared to controls (16).
Sublingual tablet treatment for 3 years was shown to have disease-modifying effects resulting in clinical benefit that persisted for at least 2 years after stopping the treatment (17, 18).
These studies illustrate the important prophylactic value of AIT, which is unlike anti-allergic medications where relapse of symptoms occurs immediately following their discontinuation. Therefore, it had been suggested that AIT should be started early, even in children with well controlled symptoms (19) because it has a preventive effect on the progression from rhinitis to asthma. The family physician is recommended to discuss AIT with the patients early in the disease process.
Safety
Both subcutaneous AIT and sublingual AIT have a good safety profile. A limitation of the subcutaneous injection route of AIT is the risk of potential side effects, which include systemic allergic reactions, occasional anaphylaxis and, even, fatalities. Risk factors for systemic reactions include extremely high sensitivity, co-seasonal allergen exposure, a history of previous systemic reactions, and, the presence of bronchial asthma. Relative contraindications to AIT for safety reason are co-existent uncontrolled asthma, patients taking beta blocker, patients with active immunological disease, children younger than 5 years-old and pregnancy. Fatal and near fatal reactions to subcutaneous AIT are very rare in children. (20) In one study reporting 26 fatalities over a 30 year period within the United Kingdom, in most of them had bronchial asthma (21). Similar reports from the USA (22) highlight the increased risk of side effects and occasional fatalities in asthmatic subjects. Asthma can become worse while the patient is on AIT and therefore it needs to be adequately controlled before commencement of AIT.
In general, sublingual AIT is well-tolerated. Minor local side effects include oral itching, lip and tongue swelling, occurring in up to 50% of participants. They are largely self-limiting and resolving within 1-2 weeks of initiation of treatment. In one recent large study in children and adults, more severe local symptoms have been reported in 5-8% of subjects and resulted in withdrawal from the study in 5% of participants.(23) Eosinophilic esophagitis presenting dysphagia or dyspepsia
has been reported in isolated cases and it subsided after discontinuation of treatment.
Cost-effectiveness
In comparison to symptomatic drug treatment, AIT has been shown to be more cost-effective for both healthcare cost and societal cost in the long run. An Italian study of sublingual AIT (Stalorals, Stallergenes) in adults with seasonal rhinitis and asthma (24) evaluated the costs for an observation period of 6 years. The break-even point in favour of sublingual AIT was achieved in the fourth year when only healthcare costs were considered but was achieved in the second year when societal costs were also evaluated. A French study in children and adults treated with sublingual AIT or subcutaneous AIT (Alustals and Stalorals, Stallergenes), for both seasonal and perennial rhinitis and asthma (25) reported similar findings, with immunotherapy most cost effective in dust mite allergy in adults and pollen allergy in children. One study (26) reported that sublingual route may be a less expensive choice of AIT than subcutaneous route (PhostalTM, Stallergenes) from all study perspectives (society, patient and NHS).
Conclusion
A IT i s i nd i ca ted i n adu l t s and ch i l d ren w i th seve re al lergic rhini t is that does not respond to convent ional pharmacotherapy and allergen avoidance measures. Selection of patients for AIT requires accurate identif ication of an underlying allergic symptoms trigger through a combination of clinical history and skin and/or blood tests for allergen specific IgE. The efficacy of AIT depends on correct patient selection, the type of allergen and the method of treatment. AIT is more effective in seasonal pollen allergy and perennial house dust mite allergy. Individual assessment and administration of AIT by experienced specialists is important to tailor a safe and effective treatment for each patient.
Both subcutaneous AIT and sublingual AIT have been shown to reduce allergy symptoms, use of anti-allergic medications and improve the quality of life. The benefit is long-lasting for some years after cessation of treatment. Evidences also showed preventive effect on the progression from rhinitis to asthma and onset of new allergy in children.
Asthma is a risk factor for systemic reaction of AIT. The safety profile of sublingual AIT appears to be superior to subcutaneous AIT. Sublingual AIT has also been shown to more cost effective than subcutaneous method in one study. Research into quality of life benefits and pharmaco-economic evaluation of benefits in a larger population will be essential to support widespread use of AIT.

7HKMA CME Bulletin 持續醫學進修專訊 June 2020www.hkma.org
Spotlight
Answer these on page 12 or make an online submission at: www.hkma.org. Please indicate whether the following statements are true or false.
1. In Hong Kong, the most common cause of perennial allergic rhinitis is house dust mite.
2. In general practice surveys, a third of children and almost two thirds of adults report partial or poor response with pharmacotherapy for allergic rhinitis.
3. I m m u n o t h e r a p y c a n n o t m o d i f y t h e u n d e r l y i n g pathophysiology of the IgE mediated allergic disease.
4. Immunotherapy stimulates the production of allergen-specific blocking IgG4 antibodies.
5. Th1 lymphocytes cellular activity suppresses allergen-induced T cell-dependent late responses in the skin and lung.
6. Subcutaneous injection immunotherapy can be given in the presence of respiratory infection, concurrent illness, current asthma, or symptoms due to concomitant allergen exposure.
7. Sublingual administration of allergen should be postponed in presence of oral wound or inflammation and concurrent illness.
8. Onset of AIT clinical effect is expected in 2-3 weeks. The recommended maintenance treatment duration is 1 years for long term clinical effect after cessation of treatment.
9. There is no evidence that immunotherapy may reduce the onset of new allergen sensitivities in children.
10. The safety profi le of subcutaneous immunotherapy appears to be superior to sublingual route.
Complete Spotlight, 1 CME Point will be awarded for at least five correct answersSelf-Assessment
Questions:Q&A
Answer to May 2020Spotlight 1 – COVID-19: Perspectives From A Nephrologist1. T 2. F 3. T 4. F 5. F 6. F 7. T 8. F 9. T 10. T
Spotlight 2 – LUTS Management – Tips and Risks in the Primary Care Setting1. T 2. F 3. T 4. T 5. F 6. T 7. T 8. T 9. F 10. T
References:
1. Meltzer EO, Blaiss MS, Derebery MJ, et al. Burden of allergic rhinitis: results from the Pediatric Allergies in America survey. J Allergy Clin Immunol 2009;124: Suppl:S43-S70.
2. White P, Smith H, Baker N, et al. Symptom control in patients with hay fever in UK general practice: how well are we doing and is there a need for allergen immunotherapy? Clin Exp Allergy 1998;28:266-270.
3. Canonica GW1, Cox L, Pawankar R Sublingual immunotherapy: World Allergy Organization position paper 2013 update. World Allergy Organ J. 2014;28;7:6.
4. Calderon MA, Alves B, Jacobson M, Hurwitz B, Sheikh A, Durham S. Allergen injection immunotherapy for seasonal allergic rhinitis. Cochrane Database Syst Rev 2007;(1):CD001936.
5. Calderon MA, Penagos M, Lagos M, Garcia-Nunez I, Carr V, Sheikh A, et al. Allergen injection immunotherapy for perennial allergic rhinitis. Cochrane Database Syst Rev 2016.
6. Frew AJ, Powell RJ, Corrigan CJ, Durham SR; UK Immunotherapy Study Group. Efficacy and safety of specific immunotherapy with SQ allergen extract in treatment-resistant seasonal allergic rhinoconjunctivitis. J Allergy Clin Immunol. 2006;117:319-25.
7. Radulovic S, Calderon MA, Wilson D, Durham S. Sublingual immunotherapy for allergic rhinitis. Cochrane Database Syst Rev 2010;(12):CD002893.
8. Didier A, Worm M, Horak F, Sussman G, de Beaumont O, Le Gall M, et al.Sustained 3-year efficacy of pre-and coseasonal 5-grass-pollen sublingual immunotherapy tablets in patients with grass pollen-induced rhinoconjunctivitis. J Allergy Clin Immunol 2011;128:559-66.
9. D a h l R , K a p p A , C o l o m b o G , e t a l . E f f i c a c y a n d s a f e t y o f sublingual immunotherapy with grass allergen tablets for seasonal allergicrhinoconjunctivitis. J Allergy Clin Immunol. 2006 Aug;118(2):434-40.
10. Bergmann KC, Demoly P, Worm M, Fokkens WJ, Carrillo T, Tabar AI, et al. Efficacy and safety of sublingual tablets of house dust mite allergen extracts in adults with allergic rhinitis. J Allergy Clin Immunol 2014;133:1608-14.
11. Mosbech H, Canonica GW, Backer V, de Blay F, Klimek L, Broge L, et al. SQ house dust mite sublingually administered immunotherapy tablet (ALK) improves allergic rhinitis in patients with house dust mite allergic asthma and rhinitis symptoms. Ann Allergy Asthma Immunol 2015;114:134-40.
12. Demoly P, Emminger W, Rehm D, Backer V, Tommerup L, Kleine-Tebbe J. Effective treatment of house dust mite-induced allergic rhinitis with 2 doses of the SQ HDM SLIT-tablet: results from a randomized double-blind, placebo-controlled phase III trial. J Allergy Clin Immunol 2016;137:444-51.
13. Durham SR, Walker SM, Varga EM, Jacobson MR, O’Brien F, Noble W, Till SJ, Hamid Q and Nouri-Aria K. Long term clinical efficacy of grass pollen immunotherapy. New Engl J Med 1999;341:468-475.
14. Des Roches A, Paradis L, Menardo JL, Bouges S, Daures JP and Bousquet J. Immunotherapy with a standardized Dermatophagoides pteronyssinus extract. VI. Specific immunotherapy prevents the onset of new sensitizations in children. J Allergy Clin Immunol 1997;99:450-53.
15. Pajno GB, Barberio G, De Luca F, Morabito L and Parmiani S. Prevention of new sensitizations in asthmatic children monosensitized to house dust mite by specific immunotherapy: A six-year follow-up study. Clin Exp Allergy 2001;31:1392-1397.
16. Jacobsen L, Niggemann B, Dreborg S, et al. Specific immunotherapy has longterm preventive effect of seasonal and perennial asthma: 10-year followup on the PAT study. Allergy 2007;62:943-948.
17. Durham SR, Emminger W, Kapp A, de Monchy JG, Rak S, Scadding GK, et al. SQ-standardized sublingual grass immunotherapy: confirmation of disease modification 2 years after 3 years of treatment in a randomized trial. J Allergy Clin Immunol 2012;129:717-25.
18. Didier A, Malling HJ, Worm M, Horak F, Sussman GL. Prolonged efficacy of the300IR 5-grass pollen tablet up to 2 years after treatment cessation, as measured bya recommended daily combined score. Clin Transl Allergy 2015;5:12.
19. Calderon MA, Gerth van Wijk R, Eichler I, et al. Perspectives on allergenspecific immunotherapy in childhood: an EAACI position statement. Pediatr Allergy Immunol 2012;23:300-306.
20. Amin HS, Liss GM, Bernstein DI. Evaluation of near-fatal reactions to allergen immunotherapy injections. J Allergy Clin Immunol 2006;117:169-175.
21. Committee on Safety of Medicines. Desensitisation vaccines. BMJ 1986;293:949.
22. Bukantz SC, Bagg AS, Lockey RF. Adverse effects and fatalities associated with subcutaneous allergen immunotherapy. Clin Allergy Immunol. 2008;21:455-68
23. Maloney J, Bernstein DI, Nelson H, Creticos P, H ebert J, Noonan M, et al. Efficacy and safety of grass sublingual immunotherapy tablet, MK-7243: a large randomized controlled trial. Ann Allergy Asthma Immunol 2014;112:146-53.
24. Berto P, Passalacqua G, Crimi N et al. Economic evaluation of sublingual immunotherapy vs symptomatic treatment in adults with pollen-induced respiratory allergy: the Sublingual Immunotherapy Pollen Allergy Italy (SPAI) study. Ann Allergy Asthma Immunol 2006; 97:615–21.
25. Omnes LF, Bousquet J, Scheinmann P et al. Pharmacoeconomic assessment of specific immunotherapy versus current symptomatic treatment for allergic rhinitis and asthma in France. Eur Ann Allergy Clin Immunol 2007; 39:148–56.
26. Pokladnikova J, Krcmova I, Vlcek J. Economic evaluation of sublingual vs subcutaneous allergen immunotherapy. Ann Allergy Asthma Immunol 2008; 100:482–9. 120

8 HKMA CME Bulletin 持續醫學進修專訊 June 2020 www.hkma.org
Spotlight-2

Cardiology
9www.hkma.org HKMA CME Bulletin 持續醫學進修專訊 June 2020
Q&A Please answer ALL questionsAnswer these on page 12 or make an online submission at: www.hkma.org.
1. What would be the most likely diagnosis?A. Mitral stenosis due to chronic rheumatic heart
diseaseB. Mitral regurgitation due to rupture papillary
muscleC. Congestive heart failure due to atrial septal defectD. Bicuspid aortic valve with aortic stenosisE. None of the above
2. Which of the following medication should NOT be given to this lady?A. Furosemide (Lasix)B. AspirinC. Warfarin
D. DigoxinE. Metoprolol (Betaloc)
A 42-year-old lady with good past health presented to your clinic with progressively increased exertional dyspnea for few months. She was told to have some heart murmur during body checkup many years ago but did not seek medical attention. Physical examination revealed heart rate 118/min with irregularly irregular pulse. There was diastolic rumbling murmur best heart over apex of precordium and crepitations over bilateral lung bases.
ECG was performed and noted atrial fibrillation. Echocardiogram was done and showed satisfactory left ventricular systolic function, dilated left atrium, thickened mitral valve leaflet, restricted mitral valve opening with characteristics doming of the anterior mitral valve leaflet (Fig 1). The mean gradient across mitral valve was 12mmHg with mitral valve area 0.97cm2. There was mild mitral regurgitation and moderate tricuspid regurgitation.
Exertional Dyspnea In Patient With Known Heart Murmur
After medical treatment, her symptoms improved a bit but remained in New York Heart Association (NYHA) functional class II.
3. Which of the following(s) would be the most appropriate treatment in this lady?a. Pacemaker implantationb. Percutaneous coronary intervention (PCI)c. Percutaneous transvenous Mitral
Commissurotomy (PTMC)d. Open heart surgery
A. a. and d.B. b. and c.C. c. or d.
D. c. and d.E. None of the above
The content of the June 2020 Cardiology Series is provided by:Dr. CHUI Shing Fung
MBChB (CUHK), MRCP (UK), FHKCP, FHKAM (Medicine), Specialist in CardiologyDr. WONG Chi Yuen
MBBS (HK), FHKCP, FHKAM (Medicine), FRCP (Edin), Specialist in Cardiology六月臨床心臟科個案研究之內容承蒙徐城烽醫生及黃志遠醫生提供。
Complete Cardiology case, 0.5 CME POINT will be awarded for at least 2 correct answers in total
Fig1

10 www.hkma.orgHKMA CME Bulletin 持續醫學進修專訊 June 2020
May Answers
Cardiology AnswersDiscussion:
This patient was presented with f lash pulmonary edema possibly precipitated by hypertensive crisis. Flash pulmonary edema or acute pulmonary edema (APO) is a life-threatening condition that occurs due to elevated cardiac filling pressure and rapid accumulation of fluid in the lung interstitium1. It commonly occurs in patients with systolic or diastolic heart fai lure. In patient with diastolic heart fai lure, factors that increases the diastolic filling pressure such as tachycardia or hypertensive crisis will precipitate the development of APO1. Paroxysmal hypertensive crisis such as in this patient requires special attention and workups for secondary hypertension, such as pheochromocytoma, or renovascular hypertension2. Renovascular hypertension is usually caused by bilateral renal artery stenosis (RAS). The pathophysiology was poorly understood but was generally thought to be related to impaired natriuresis and excessive activation of the renin-angiotensin-aldosterone axis. One of the few class I indicat ions for revascularization in patients with RAS is cardiac disturbance syndromes – APO with hypertension and more than 10mmHg gradient across renal artery3. This patient underwent renal artery revascularization and stenting (Figure 3). Her aortic systolic pressure before the stenting was 270mmHg, which dropped down to 150mmHg after stenting (Figure 4). She weaned off most of her blood pressure medication afterwards and did not attend again for SOB.
The content of the May 2020 Cardiology Series is provided by:Dr. TAN GuangMing
MBChB, MRCP, FHKCP, FHKAM (Medicine), Specialist in CardiologyDr. CHEUNG Shing Him, Gary
MBBS, MRCP, FHKCP, FHKAM (Medicine), Specialist in Cardiology)五月臨床心臟科個案研究之內容承蒙譚廣明醫生及張誠謙醫生提供。
Answer: 1 E, 2 E, 3 E, 4 E.
Figure 4: Intraoperative aortic pressure recording before and after stenting.
Figure 3: Renal artery angiogram before and after stenting.
Reference:
1. Gandhi SK, Powers JC, Nomeir AM et al. The pathogenesis of acute pulmonary edema associated with hypertension. N Engl J Med. 2001 Jan 4;344(1):17-22.
2. Chiong JR1, Aronow WS, Khan IA et al. Secondary hypertension: current diagnosis and treatment. Int J Cardiol. 2008 Feb 20;124(1):6-21.
3. Marloe Prince, Jose D. Tafur and Christopher J. White, When and How Should We Revascularize Patients With Atherosclerotic Renal Artery Stenosis? JACC: Cardiovascular Interventions. 2019 Mar 25;12(6):505-517.
Dermatology Answers1. B
The diagnosis is Pityr iasis Alba. The face is the most common site affected, although the neck, arms, and shoulders can also be involved.
2. CPityr iasis alba is more common among patients with history of atopy. Although the etiology remains unknown, it is commonly characterized as a minor manifestation of atopic dermatit is. Thyroid disorders, diabetes and autoimmune disease are commonly associated with vitiligo. Cardiometabolic diseases such as diabetes and dyslipidemia are prevalent among patients with psoriasis.
3. FalsePityriasis alba occurs predominately in children and the adolescent. Both sexes can be affected, though a slight male preponderance has been reported in the past.
4. BWood’s lamp examination helps distinguish Pityriasis alba from vitiligo by its characteristic features. Skin scrapings for mycology is used to diagnose tinea faciei and it may take weeks to confirm. A skin biopsy is rarely required for Pityriasis alba. A screening blood test is required for the associated diseases of vitiligo but is not necessary for the diagnosis of Pityriasis alba.
5. CPityriasis alba usually resolves within months so reassurance with an early review, use of emollients and sunscreen or application of low potency topical steroid cream are the mainstays of treatment for this boy. Phototherapy should be considered only for extensive or refractory lesion.
Dermatology Series for May 2020 is provided by: Dr. LEUNG Wai Yiu, Dr. TANG Yuk Ming, William, Dr. CHAN Hau Ngai,
Kingsley, Dr. KWAN Chi Keung and Dr. NG Shun ChinSpecialists in Dermatology & Venereology
五月皮膚科個案研究之內容承蒙梁偉耀醫生、鄧旭明醫生、 陳厚毅醫生、關志強醫生及吳順展醫生提供。

11www.hkma.org HKMA CME Bulletin 持續醫學進修專訊 June 2020
DermatologyDermatology Series for June 2020 is provided by:
Dr. KWAN Chi Keung, Dr. TANG Yuk Ming, William, Dr. CHAN Hau Ngai, Kingsley, Dr. LEUNG Wai Yiu and Dr. NG Shun Chin
Specialists in Dermatology & Venereology六月皮膚科個案研究之內容承蒙關志強醫生、鄧旭明醫生、陳厚毅醫生、
梁偉耀醫生及吳順展醫生提供。
Q&A Please answer ALL questionsAnswer these on page 12 or make an online submission at: www.hkma.org.
1. What is your differential diagnosis?a) Melanomab) Basal cell carcinomac) Seborrhoeic keratosisd) Melanocytic naevuse) All of the above
2. This lesion must be benign as it was asymptomatic. (True or False)
3. What will you do then?a) Just keep observe, as it is a benign lesionb) Swab for bacterial culture, as there is a small
erosionc) Swab for herpes simplex virus PCR, as there is
a small erosiond) Skin biopsye) Both (b) and (c)
A 86 year-old gentleman came with his daughter complained a black mole at right post-auricular region for 2 years. His daughter noticed the mole was increasing in size. However, this gentleman did not have any symptom or complaint about the mole. Physical examination reviewed a black hyperpigmented papule at the right post auricular region with irregular edge and small erosion on the surface. (Figure)
Pigmented Mole On Right Post-auricular Region
Complete Dermatology case, 0.5 CME POINT will be awarded for at least 3 correct answers in total
4. What is/are the treatment(s) for this elderly?a) Reassurance and observationb) Systemic antibioticsc) Systemic anti-viral agentd) Surgical excisione) Both (b) and (c)
5. The lesion may relate to sun damage. (True or False)?

ANSWER SHEET
Answer Sheet
June 2020
Name Signature:
HKMA Membership No.
Contact Tel No.:
HKID No. - xxx(x)
Please return thecompleted answer sheetto the HKMA Secretariat(Fax: 2865 0943) on orbefore 15 July 2020for documentation.If you completethe exercise online,you are NOT required toreturn the answer sheet by fax.
Please answer ALL questions and write the answers in the space provided.
A maximum of 20 points can be awarded for se l f -study per year and no upper limit of CME points for attending CME lectures
DermatologyCardiologyComplete Dermatology, 0.5 CME point will be awarded for at least three correct answers
Complete Cardiology, 0.5 CME point will be awarded for at least two correct answers
11 22 33 4 5
(revised in August 2019)
CME Physical Lecture Policy and ProcedureRegistration1. Please complete the reply slip and return to HKMA Secretariat in person
or by fax/mail/email.2. Enrollment priorities will be given to doctors who have purchased
packages. For Community Network Lectures, priorities will be given to doctors from that Community Network with Packages, then doctors from that Community Network.
3. No walk in or on-site payment will be accepted. Attendance without registration will not be recognized and CME point will not be accredited.
4. Please ensure that your registration is confirmed before attending lecture. Only successfully registered doctors who paid could attend the lecture.
5. The HKMA Secretariat will notify doctors who have successfully enrolled to arrange for payment. If doctors have not arranged for payment within a specified period after the notification, the seat will be released to doctors on waiting list without further notice.
Payment1. All HKMA CME lectures that involve registration and enrollment through
the HKMA would require the collection of lecture fee (unless otherwise specified).
2. The lecture fee is $50 for HKMA members and $100 for non-members per lecture.
3. Online payment is available to doctors who have registered the HKMA website online system. One transaction is for one lecture only.
4. Packages could be purchased through cash or cheque only.5. Cash payments have to be paid in person at HKMA Secretariat and
cheque payments have to be mailed or paid in person at HKMA Secretariat.
6. Fee can be paid together in one cheque for lecture within the same month. Only combined cheque payment for not more than 2 packages will be accepted.
7. No refund or transfer will be allowed after payment is made. Payment cannot be transferred to other lectures or for other specified doctors.
CME Online Payment & CME Self-Studies SeriesCME Online PaymentThe HKMA is excited to introduce online payment for CME Lectures:1. Login to CME Portal to apply for a lecture2. Receive SMS notification3. Pay online!
Online payment available ONLY for attending a single lesson, payment for package is unavailable currently.CME Self-Studies SeriesYou can register the CME Lectures and finish the CME Self-Studies Series within the webpage (www.hkma.org).Don’t wait! Please register and create your own account through https://www.thkma.org/members/register.php (1st time register account is limited on desktop ONLY) to experience our new Members Portal.Information for ParticipantsSpecial weather arrangementWhen Tropical Storm Warning Signal No. 8 (or above) or a Black Rainstorm Warning Signal is in force within 3 hours of the commencement time, the relevant CME function will be cancelled. (i.e. CME starting at 2:00 pm will be cancelled if the warning signal is hoisted or in force any time between 11:00 am and 2:00 pm).The function will proceed as scheduled if the signal is lowered three hours before the commencement time. (i.e. CME starting at 2:00 pm will proceed if the warning signal is lowered at 11:00 am, but will be cancelled even if it is lowered at 11:01 am).When Typhoon No. 8 Signal or a Black Rainstorm signal is in force after CME commencement, announcement will be made depending on the conditions as to whether the CME will be terminated earlier or be conducted until the end of the session.The above are general guidelines only. Individuals should decide on their CME attendance according to their own transportation and work/home location considerations to ensure personal safety.General lecture policy1. Doctor should sign for own CME.2. Registration will cease when Q & A Session starts.3. No recording unless permission is granted by the HKMA.4. If doctor has attended CME Lecture and CME Live at the same point of
time, only CME Points for the Lecture would be counted.5. The HKMA will investigate when non-compliance at CME Session is
reported, further action will be considered to ensure all CME activities are properly held.
6. For enquiries, please contact the CME Department of the HKMA Secretariat at 2527-8452.
SPOTlightComplete Spotlight, 1 CME point will be awarded for at least 5 correct answers
1 2 3 4 5 6 7 8 9 10

14 www.hkma.orgHKMA CME Bulletin 持續醫學進修專訊 June 2020
CME Live
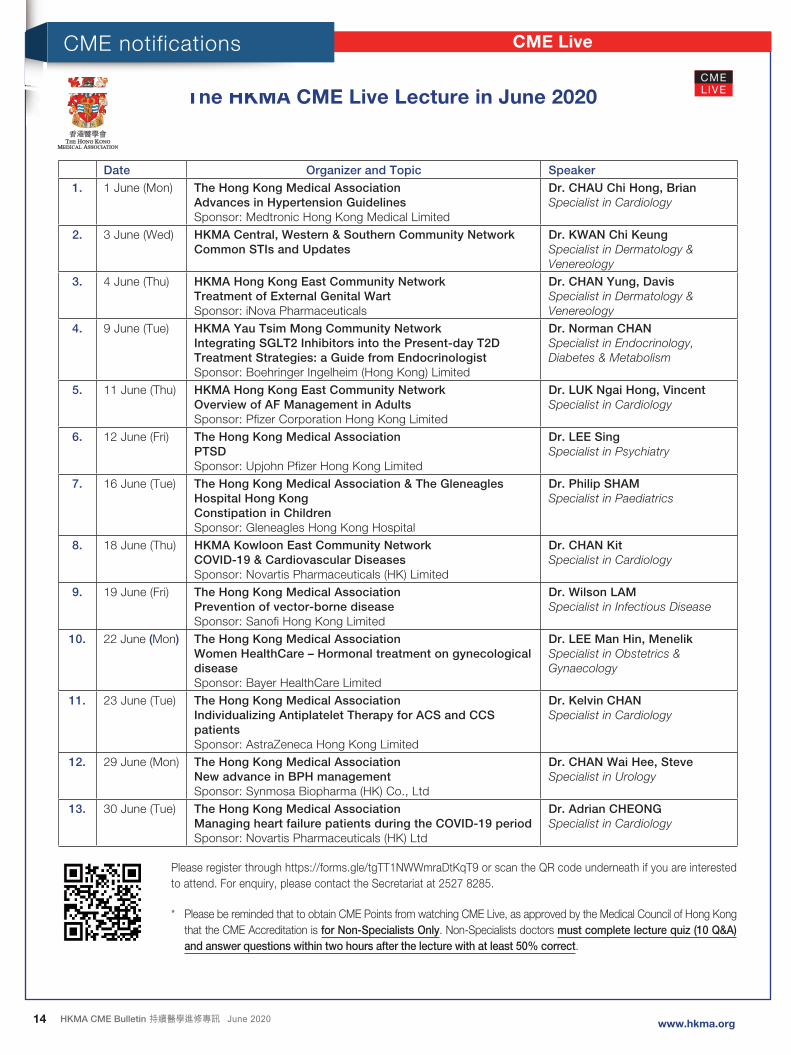
The HKMA CME Live Lecture in June 2020
Date Organizer and Topic Speaker
1. 1 June (Mon) The Hong Kong Medical AssociationAdvances in Hypertension GuidelinesSponsor: Medtronic Hong Kong Medical Limited
Dr. CHAU Chi Hong, BrianSpecialist in Cardiology
2. 3 June (Wed) HKMA Central, Western & Southern Community NetworkCommon STIs and Updates
Dr. KWAN Chi KeungSpecialist in Dermatology & Venereology
3. 4 June (Thu) HKMA Hong Kong East Community NetworkTreatment of External Genital WartSponsor: iNova Pharmaceuticals
Dr. CHAN Yung, DavisSpecialist in Dermatology & Venereology
4. 9 June (Tue) HKMA Yau Tsim Mong Community NetworkIntegrating SGLT2 Inhibitors into the Present-day T2D Treatment Strategies: a Guide from EndocrinologistSponsor: Boehringer Ingelheim (Hong Kong) Limited
Dr. Norman CHANSpecialist in Endocrinology, Diabetes & Metabolism
5. 11 June (Thu) HKMA Hong Kong East Community NetworkOverview of AF Management in AdultsSponsor: Pfizer Corporation Hong Kong Limited
Dr. LUK Ngai Hong, VincentSpecialist in Cardiology
6. 12 June (Fri) The Hong Kong Medical AssociationPTSDSponsor: Upjohn Pfizer Hong Kong Limited
Dr. LEE SingSpecialist in Psychiatry
7. 16 June (Tue) The Hong Kong Medical Association & The Gleneagles Hospital Hong KongConstipation in ChildrenSponsor: Gleneagles Hong Kong Hospital
Dr. Philip SHAMSpecialist in Paediatrics
8. 18 June (Thu) HKMA Kowloon East Community NetworkCOVID-19 & Cardiovascular DiseasesSponsor: Novartis Pharmaceuticals (HK) Limited
Dr. CHAN KitSpecialist in Cardiology
9. 19 June (Fri) The Hong Kong Medical AssociationPrevention of vector-borne diseaseSponsor: Sanofi Hong Kong Limited
Dr. Wilson LAMSpecialist in Infectious Disease
10. 22 June (Mon) The Hong Kong Medical AssociationWomen HealthCare – Hormonal treatment on gynecological diseaseSponsor: Bayer HealthCare Limited
Dr. LEE Man Hin, MenelikSpecialist in Obstetrics & Gynaecology
11. 23 June (Tue) The Hong Kong Medical AssociationIndividualizing Antiplatelet Therapy for ACS and CCS patientsSponsor: AstraZeneca Hong Kong Limited
Dr. Kelvin CHANSpecialist in Cardiology
12. 29 June (Mon) The Hong Kong Medical AssociationNew advance in BPH managementSponsor: Synmosa Biopharma (HK) Co., Ltd
Dr. CHAN Wai Hee, SteveSpecialist in Urology
13. 30 June (Tue) The Hong Kong Medical AssociationManaging heart failure patients during the COVID-19 periodSponsor: Novartis Pharmaceuticals (HK) Ltd
Dr. Adrian CHEONGSpecialist in Cardiology
Please register through https://forms.gle/tgTT1NWWmraDtKqT9 or scan the QR code underneath if you are interested to attend. For enquiry, please contact the Secretariat at 2527 8285.
* Please be reminded that to obtain CME Points from watching CME Live, as approved by the Medical Council of Hong Kong that the CME Accreditation is for Non-Specialists Only. Non-Specialists doctors must complete lecture quiz (10 Q&A) and answer questions within two hours after the lecture with at least 50% correct.
CME notifications

15www.hkma.org HKMA CME Bulletin 持續醫學進修專訊 June 2020
The Hong Kong Medical Association
Dr. WONG Bun Lap, Bernard presenting a CME Live Lecture on 8 May 2020
Group photo taken on 16 May 2020 From left: Dr. TSUI Tsun Miu (2nd speaker) and Dr. WONG Yu Hong (1st speaker)
Dr. AU YEUNG Yick Cheung presenting a CME Live Lecture on 16 May 2020
Dr. TONG Chun Yip Peter presenting a CME Live Lecture on 31 May 2020
Group photo taken on 6 May 2020From left: Dr. LAW Yim Kwai, Dr. YIK Ping Yin (moderator) and Dr. C yrus TSE (speaker)
Dr. WONG King Ying presenting a CME Live Lecture on 31 May 2020
Dr. Dorothy TAM delivering a CME Live Lecture on 20 May 2020
Dr. CHAN Kit Jacky presenting a CME Live Lecture on 31 May 2020
The HKMA Central, Western and Southern Community Network (CW&SCN) ~ Dr. YIK Ping Yin
Dr. WONG Chun Kuen presenting a CME Live Lecture on 13 May 2020
The HKMA Kowloon West Community Network (KWCN) ~ Dr. TONG Kai Sing
Meeting Highlights
The HKMA Hong Kong East Community Network (HKECN) ~ Dr. CHAN Nim Tak, Douglas
Dr. Kelvin CHAN delivering a CME Live Lecture on 7 May 2020 From left: Speakers Dr. Kelvin KWOK and Dr. Stanley LO in photo during the CME Live Lecture on 21 May 2020
Dr. YEUNG Kwok Kit giving a CME Live Lecture on 19 May 2020

16 www.hkma.orgHKMA CME Bulletin 持續醫學進修專訊 June 2020
The HKMA New Territories WestCommunity Network (NTWCN) ~Dr. CHEUNG Kwok Wai, Alvin
The HKMA Shatin Community Network (SCN) ~Dr. MAK Wing Kin
The HKMA Kowloon East Community Network (KECN) ~ Dr. AU Ka Kui, Gary
The HKMA Yau Tsim Mong Community Network (YTMCN) ~ Dr. CHENG Kai Chi, Thomas
SubscriptionAvailable
HKMA members are entitled to a FREE copy of CME Bulletin. Subscription is opended to sponsors and interested individuals.
Meeting Highlights
Prof. Gar y WONG (speaker) presenting a CME Live Lecture on 12 May 2020
Dr. LOO Ching Kong delivering a CME Live Lecture on 22 May 2020
Dr. CHUNG Yiu Kei presenting a CME Live Lecture on 29 May 2020
Dr. Jacky CHAN giving a CME Live Lecture on 14 May 2020
Dr. KWOK Yuk Lung delivering a CME Live Lecture on 28 May 2020
Dr. HO Kwok Tung giving a CME Live Lecture on 26 May 2020

CME Calendar
17HKMA CME Bulletin 持續醫學進修專訊 June 2020www.hkma.org
June 2020
1 June 2020(Mon)2:00 – 3:00 pm
The Hong Kong Medical AssociationAdvances in Hypertension GuidelinesHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
1
3 June 2020(Wed)2:00 – 3:00 pm
HKMA Central, Western & Southern Community NetworkCommon STIs and UpdatesHKMA Facebook CME Live LectureMiss Antonia Lee – Tel: 2527 8285
1
4 June 2020(Thu)2:00 – 3:00 pm
HKMA Hong Kong East Community NetworkTreatment of External Genital WartHKMA Facebook CME Live LectureMs. Candice Tong – Tel: 2527 8285
1
9 June 2020(Tue)2:00 – 3:00 pm
HKMA Yau Tsim Mong Community NetworkIntegrating SGLT2 Inhibitors into the Present-day T2D Treatment Strategies: a Guide from EndocrinologistHKMA Facebook CME Live LectureMs. Candice Tong – Tel: 2527 8285
1
11 June 2020(Thu)2:00 – 3:00 pm
HKMA Hong Kong East Community NetworkOverview of AF Management in AdultsHKMA Facebook CME Live LectureMs. Candice Tong – Tel: 2527 8285
1
12 June 2020(Fri)2:00 – 3:00 pm
The Hong Kong Medical AssociationPTSDHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
1
16 June 2020(Tue)2:00 – 3:00 pm
The Hong Kong Medical Association & The Gleneagles Hospital Hong KongConstipation in ChildrenHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
3
18 June 2020(Thu)2:00 – 3:00 pm
HKMA Kowloon East Community NetworkCOVID-19 & Cardiovascular DiseasesHKMA Facebook CME Live LectureMiss Antonia Lee – Tel: 2527 8285
1
19 June 2020(Fri)2:00 – 3:00 pm
The Hong Kong Medical AssociationPrevention of Vector-borne DiseaseHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
1
22 June 2020(Mon)2:00 – 3:00 pm
The Hong Kong Medical AssociationWomen HealthCare – Hormonal Treatment on Gynecological DiseaseHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
1
23 June 2020(Tue)2:00 – 3:00 pm
The Hong Kong Medical AssociationIndividualizing Antiplatelet Therapy for ACS and CCS patientsHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
1
29 June 2020(Mon)2:00 – 3:00 pm
The Hong Kong Medical AssociationNew Advance in BPH ManagementHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
1
30 June 2020(Tue)2:00 – 3:00 pm
The Hong Kong Medical AssociationManaging Heart Failure Patients During the COVID-19 PeriodHKMA Facebook CME Live LectureHKMA CME Dept. – Tel: 2527 8452
1
Receiving Electronic Copy Of CME Bulletin
The CME Bulletin has been mailed to members on the 15th of each month since year 2000. As an initiative to protect the environment and smart costing, HKMA encourages members to receive these documents via email or read them online at the HKMA website (http://www.hkma.org/), rather than receiving hard copies by post.
If you would like to receive the CME Bulletin by email, or to complete the self-assessment questions on the HKMA website, please indicate your preference by filling in the reply slip below.
REPLY SLIPI would like to receive the HKMA CME Bulletin (chose either one below)
By email (Please provide your valid email address):
By downloading from the HKMA website (http://www.hkma.org/)
Name: HKMA Membership No:
Signature: Date:
Please return the completed form to us by fax (2865 0943) or email ([email protected]).