Embed Size (px)
Citation preview

OCULAR MYASTHENIA GRAVIS AND HASHIMOTO'S THYROIDITIS
ROBERT H. OSHER, B.S., AND J. LAWTON SMITH, M.D. Miami, Florida
The coexistence of ocular myasthenia gravis and Hashimoto's thyroiditis has, to our knowledge, not been previously reported. Two of our patients with this combination showed a favorable response to medical therapy.
CASE REPORTS
Care 1—This 37-year-old white woman, first seen here in January 1974, complained of double vision of nine months' duration. She had no visual complaints until April 1973, when she noted horizontal diplopia while driving her car. By November 1973, the diplopia had progressed and was primarily vertical in nature. Hospitalizaton revealed diplopia in all directions of gaze characterized by extreme variability. Although there was no blepharoptosis, a goiter was found, as well as a head tremor that had been present for seven years. Laboratory studies showed a negative Werner test with a 24-hour radioactive iodine uptake (RAI) of 33% that fell to 9% after liothyronine sodium (Cytomel) suppression. A Tensilon test was negative. Thyroid scan showed asymmetry of the gland with a prominent right lobe.
In January 1974, examination revealed normal visual acuity, visual fields, pupils, fundi, and ocular tensions. Bilateral pathologic eyelid retraction was evident. The ocular motility showed limitation of the medial rectus and inferior rectus muscles in the right eye. The head tremor was evident, as well as a goiter the size of a tangerine (Fig. 1), and the family history was contributory (two sisters had goiters). A quantitative Tensilon test was positive in yielding a "perverse" response in that the left hypertropia measured in the primary position with the Maddox rod turned into a right hypertropia during the test. The clinical diagnosis of ocular myasthenia gravis was made, and the patient began receiving 60 mg of orally administered pyridostig-mine bromide (Mestinon), three times a day.
Five days later she reported that after only six pyridostigmine bromide tablets the diplopia was essentially gone except in right gaze. The patient was hospitalized for endocrine studies in February 1974. The thyroid gland was diffusely enlarged with no nodules, bniits, or thrills. Serum cholesterol, T-4, and T-3 were normal ; thyroid stimulating hormone (TSH) was elevated, and thyroglobulin and micro-
From the Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami School of Medicine, Miami, Florida.
Reprint requests to J. Lawton Smith, M.D., P.O. Box 520875, Miami, FL 33152.
somal antibodies were negative. Despite the absence of autoantibodies, the clinical impression was Hashimoto's thyroiditis, and she was started on suppressive doses of thyroid hormone to decrease the TSH and prevent additional enlargement of the gland.
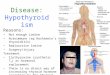
In March 1974, she became agitated, the diplopia became more severe, and blepharoptosis developed on the left. A needle biopsy of the thyroid histo-logically confirmed the clinical diagnosis of Hashimoto's thyroiditis (Fig. 2).
On April 29, the patient returned and was taking 60 mg of pyridostigmine bromide, four times a day, and two grains a day of thyroid hormone. She reported she was seeing double about 25% of the time. Examination revealed a slight eyelid retraction on the right and moderate blepharoptosis on the left. Ductions of the left eye were full, but there was slight limitation of adduction of the right eye. Pred-nisone therapy in the Seybold-Drachman regimen1
was begun to better control the ocular myasthenia, and the thyroid supplement was reduced to one grain a day. The patient later reported that when the dosage of 40 mg prednisone, every other day, was reached the blepharoptosis completely disappeared. After receiving 100 mg of prednisone, every other day, three to four pyridostigmine bromide tablets, and one grain of thyroid hormone every day, she felt well ; the double vision was reduced to 10%, and only on right gaze.
Case 2—This 26-year-old black woman, first seen in November 1973, complained of double vision of two months' duration. The patient gave birth to a normal child on July 20, 1973, and at that time noted the onset of hoarseness and daily headaches. In late September, diplopia began, and she was re-
Fig. 1 (Osher and Smith). Case 1. Thyroid enlargement.
1038

VOL. 79, NO. 6 MYASTHENIA GRAVIS 1039
·*: *'Jv
ί"*«ΒΪ*>««ι*,-
-- -s^» > ^ ■',„%;
=fc /̂r̂ N . ' · *# Λ -"'" '^»»ifä-v;* ' f : " * s ™ ■
T'rt-T***t« * -"* ' k
Fig. 2 (Osher and Smith). Case 1. Needle biopsy of thyroid; typical Hashimoto's thyroiditis (hematoxylin and eosin, approximately XlOO).
ferred for neuro-ophthalmologic consultation. On Nov. 16, examination revealed normal visual
acuity, visual fields, pupils, fundi, and ocular tensions. The motility findings revealed a left hyper-phoria, greatest in upgaze and to the left. The initial impression was Brown's superior oblique tendon sheath syndrome. A prism with 8 diopters base down for the left eye was prescribed.
Two weeks later, the patient stated that the diplopia was somewhat better with the prism but she was dissatisfied with its weight and bulk. A quantitative Tensilon test revealed that the left hyper-phoria increased from an initial value of 6 diopters to 15 prism diopters within two minutes after the injection and then returned to the initial value. This paradoxic response was a positive test. Thyroid function tests were performed and revealed normal protein bound iodine (PBI), butanol-extractable iodine serum (BEI), T-3, T-4, and RAI values.
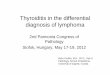
By Dec. 11, she developed an obvious blepharo-ptosis of the right upper eyelid. She showed a Co-gan's eyelid twitch sign, weakness of downgaze in the right eye, and some weakness of upgaze in both eyes. The Tensilon test was repeated and promptly relieved the blepharoptosis (Fig. 3). Thyroid enlargement was evident on inspection (Fig. 4). Chest roentgenograms were negative for an anterior me-diastinal mass. She received 60 mg of pyridostig-mine bromide, three times a day, and noted improvement of blepharoptosis and diplopia within two weeks.
Endocrinologie examination showed an enlarged thyroid gland without nodules, bruits, or thrills, with normal thyroid function tests, and after three weeks on 0.2 mg of levothyroxine sodium (Syn-throid) daily, the RAI suppressed to 0. We clinically diagnosed Hashimoto's thyroiditis and recommended 0.3 mg of levothyroxine sodium daily.
The pat'ent had a recurrence of diplopia and was started on combined corticosteroids and pyrido-stigmine bromide. The diplopia and blepharoptosis abated and she discontinued the corticosteroids. However, the diplopia recurred and she was again placed on the combination therapy. Within several days the diplopia cleared. The patient recently reported no ocular complaints on prednisone, pyrido-stigmine bromide, and levothyroxine sodium therapy.
DISCUSSION
Ocular myasthenia gravis is a form of the disease characterized by blepharoptosis and diplopia in patients who, for all practical purposes, have no other symptoms relating to the skeletal or bulbar musculature. The blepharoptosis affects one or both eyes, and in either case is usually asymmetric. Since fatigue and variability are hallmarks of the disease, the

1040 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1975
Fig. 3 (Osher and Smith). Case 2. Top, before Tensilon; bottom, after Tensilon.
blepharoptosis may be minimal on awakening and commonly increases later in the day. The extraocular muscle involvement in myas-thenia gravis may result in ophthalmoplegia of one or several muscles. The motility patterns may mimic gaze palsies, internuclear ophthalmoplegias, or nystagmoid disorders. The ophthalmoplegia is always external, as the pupil is not affected. The majority of myasthénies with initial ocular manifestations will progress to a more generalized form of the disease. However, we see many patients with involvement symptomatically restricted to the ocular muscles for years with a good general prognosis.
History alone can provide the diagnosis of ocular myasthenia gravis. Diurnal variation, effects of rest and exertion, remission,
and a family history of endocrine diseases, such as goiter or diabetes mellitus, should be noted. Old photographs are helpful in documenting the onset of the blepharoptosis. Prolonged upgaze commonly aggravates the blepharoptosis, and this point (the fatigue phenomenon) aids in the diagnostic process. Cogan's eyelid twitch sign is another useful diagnostic test.2 When the patient shifts fixation from downgaze to the primary position, a transient overshoot of the blepharoptotic eyelid may be seen. Although not pathogno-monic, and less commonly encountered than the fatigue phenomenon, this sign suggests ocular myasthenia gravis.
Pharmacologie testing with intravenously administered Tensilon should confirm the diagnosis. We found the following helpful in assessing the Tensilon test: (1) we used only fresh single-dose ampules of Tensilon; (2) we did not perform the test at the beginning of the ocular examination, since patients may experience nausea or cramps, thus preempting the remainder of the examination; (3) if the patient presents with blepharoptosis, upgaze must be maintained in order to increase blepharoptosis to the maximum. Then, while the patient is maintaining upgaze, 1 ml (10 mg) of fresh Tensilon should
Fig. 4 (Osher and Smith). Case 2. Thyroid enlargement.

VOL. 79, NO. 6 MYASTHENIA GRAVIS 1041
be administered intravenously while observing the eyelid position. Photographs before and after the injection are helpful as objective confirmation of the response ; ( 4 ) if there is no blepharoptosis but a conspicuous limitation of motility, Tensilon is administered, and the test is positive when the motility pattern is markedly altered; (5 ) if the patient has neither obvious blepharoptosis nor gross limitation of ocular motility at the time of examination, the quantitative Tensilon test is helpful. The patient fixes a light at distance, and the phorias are measured in the primary position, right, and left gaze, with a Maddox rod and Wrisley rotary prism. Measurements are repeated until there is a quantitative reproducibility. Tensilon is then administered, and the deviations are measured every 30 seconds for three to four minutes, or until no further change occurs. A negative quantitative Tensilon test will reveal no change in the distance vertical phoria, and no change to less than 3 prism diopters in the horizontal phoria (stress may slightly increase convergence input by 1 or 2 prism diopters) . A positive quantitative Tensilon test conventionally reveals a significant decrease in the deviation. However, an increase in the deviation (paradoxic response), or conversion of an esotropia to an exotropia deviation or of a right hyperdeviation to a left hyperdeviation (perverse response), may be seen and indicates myasthenia gravis.3 The latter reactions may indicate a differential response of various extraocular muscles to the drug.
Other tests have been employed in combination with Tensilon, such as Tensilon tonography, and optokinetic electronystag-mography.
Hashimoto's thyroiditis, also known as lymphocytic thyroiditis and struma lympho-matosa, is probably the most common form of chronic thyroiditis and also the most common cause of pr imary hypothyroidism. Women are more often affected than men ( 9 : 1 ) , especially during the third to fifth decades. The family history is often con
tributory for goiter and other autoimmune disorders.
The histologie appearance of the gland is a diagnostic tool. A diffuse lymphocytic infiltration of the stroma exists with development of lymphoid follicles and germinal centers. Plasma cells and macrophages intermingle with other cellular elements. The "Askanazy cells" that represent the destruction of epithelial cells are pathognomonic for this disorder. A n increase in the interacinar connective tissue also occurs at the expense of normal thyroid architecture.
The cardinal physical finding is a diffusely enlarged, firm thyroid gland that is two to three times the normal size. The onset is insidious, usually without production of local symptoms. Infrequently, pressure on the trachea or esophagus may result in discomfort, dysphagia, or a choking sensation. An occasional patient will present localized pain that can simulate the disorders of acute or subacute thyroiditis.
Although many of these patients have no initial complaints, symptoms of hypothyroidism are present in 2 0 % at the first examination. Malaise and fatigue may be the only subtle indications since functional impairment is usually mild. Changes in voice, skin, hair, weight, and intolerance to cold may provide the classic signs of hypothyroidism. Severe myxedema, characterized by slow mentation, speech and movement, pericardial and pleural effusions, and interstitial edema, is an infrequent presentation.
Ocular involvement may occur in either the euthyroid or hypothyroid patient with Hashimoto's disease. The ophthalmopathy cannot be clinically differentiated from that associated with Graves' disease.4 Although the relationship between myasthenia gravis and hyperthyroidism is well known, the association of myasthenia gravis and hypothyroidism is less well recognized. In our experience, the occurrence of classic thyroid ophthalmopathy syndromes in the chemically and clinically euthyroid patients is common in ophthalmologic practice and is still unappre-

1042 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1975
ciated by internists. However, we found only 12 cases of concomitant Hashimoto's disease and generalized myasthenia gravis; none of these were published ophthalmic reports.
The laboratory findings are helpful in establishing the diagnosis of Hashimoto's thyroiditis. There is usually a positive serologie response for thyroid autoantibodies, either to thyroglobulin, other colloid antigens, or the microsomal antigen of epithelial cells. However, the mere presence of autoantibodies is not pathognomonic, since they also may be found in Graves' disease, nonsuppurative thyroiditis, and rarely in thyroid carcinoma. Furthermore, a negative test does not rule out the diagnosis of Hashimoto's disease, but high titers are found only in Hashimoto's disease and Graves' disease.
The erythrocyte sedimentation rate tends to be elevated, the serum gamma globulins are often high, and the cephalin flocculation test may be positive. Serum PBI and the RAI tests may be elevated, normal, or low. The elevated thyroid function tests may occur in early stages of the disease, whereas low PBI and RAI values tend to occur later when thyroid architecture is replaced by lymphoid and fibrous tissue. Owing to faulty synthesis of hormone, hypersection of TSH results. Thyrotropin injection fails to increase the RAI or level of serum T-4. The fact that long-acting thyroid stimulator has been absent and that T-3 administration will suppress the RAI (Werner test) may aid in laboratory differentiation between a nervous patient with Hashimoto's thyroiditis and the patient with Graves' disease.
However, if the physician palpates the thyroid and obtains appropriate laboratory tests, the diagnosis can be established with a needle biopsy, done as an outpatient procedure.
The diagnosis must be made for three reasons. First, there may be an increased incidence of thyroid malignancy in patients with Hashimoto's disease. This was as high as 12% in one series and is not surprising since papillary carcinoma of the thyroid is TSH-
dependent, and in the patient with Hashimoto's thyroiditis, the levels of TSH are elevated.5 Secondly, these patients also have an increased incidence of other autoimmune disorders, including Sjögren's syndrome, pernicious anemia, Graves' disease, rheumatoid arthritis, Addison's disease, idiopathic throm-bocytopenic purpura, autoimmune hemolytic anemia, and systemic lupus erythematosus. Finally, the treatment gives satisfactory results.
Treatment—The management of the patient with ocular myasthenia and Hashimoto's thyroiditis may be difficult since the thyroid status may be intimately related to the severity of the myasthenia. Since there is contradictory evidence, we recommend treating each disease separately but recognize that an interplay may exist. Surgery was the treatment for Hashimoto's thyroiditis but is now indicated only if there are significant pressure signs or a suspicion of concemitant neoplasm. The current treatment of choice for Hashimoto's disease is suppressive therapy with either desiccated thyroid, T-3, or T-4. The size of the thyroid gland rapidly reduces, providing relief from pressure symptoms and cosmesis. Signs and symptoms of hypothyroidism are also diminished. Finally, since levels of TSH decrease, the risk of thyroid carcinoma is reduced.
The treatment of ocular myasthenia gravis is symptomatic but important. Mechanical aids as simple patching, blepharoptosis crutches, or prism glasses may be helpful. As surgery is not indicated because of the variability of the motility patterns, the choice is medical therapy. Anticholinesterase drugs such as neostigmine bromide (Prostig-mine), pyridostigmine bromide, and ambe-nonium chloride (Mytelase) provide one mode of treatment. However, corticosteroids combined with anticholinesterase drugs have been effective treatments. We start the ocular myasthénie patient on an initial dose of 60 to 120 mg of orally administered pyridostigmine bromide, three times a day. If he is not controlled on this regimen, he is placed

VOL. 79, NO. 6 MYASTHENIA GRAVIS 1043
on 180, mg one at 8:00 A.M. and one at 8:00 P.M. daily. If additional control is necessary, corticosteroids are added. The Seybold-Drachman regimen1 minimizes early weakness and other side effects by gradually increasing the corticosteroid dosage. The patient is started on 25 mg-prednisone, on alternate days, that is increased by 12.5 mg every third dose until 100 mg, or an optimal response at a lower dose is reached. A significantly larger percentage of patients with ocular myasthenia gravis can be treated than we were formerly able to treat with cholines-terase agents alone.
SUMMARY
Two patients had ocular myasthenia gravis coexistent with Hashimoto's thyroiditis. A 37-year-old woman presented with diplopia and displayed a head tremor and thyroid enlargement. Thyroid function tests showed an elevated thyroid stimulating hormone ( T S H ) . A quantitative Tensilon test yielded a "perverse" response and a needle biopsy indicated Hashimoto's disease. A 26-year-old woman presented with diplopia and subsequently developed blepharoptosis and thyroid enlargement. Examination revealed Cogan's eyelid twitch sign, a paradoxical quantitative Tensilon test, and laboratory studies revealed normal thyroid function tests.
Treatment was directed at each disease en
tity separately. Ocular myasthenia gravis was managed with an anticholinesterase agent in combination with oral corticosteroids that provided additional control. Suppressive therapy with desiccated thyroid hormone reduced the size of the thyroid gland, diminished the signs and symptoms of hypothyroidism, and lowered the levels of TSH, possibly decreasing the risk of thyroid carcinoma. Both patients showed gratifying responses to therapy.
ACKNOWLEDGMENTS
We thank Robert B. Katims, M.D., for endocrinologie studies on these patients, and B. Bercaw, M.D., for referring a patient
REFERENCES
1. Seybold, M. E., and Drachman, D. B. : Gradually increasing prednisone in myasthenia gravis. N. Engl. J. Med, 290:81, 1974.
2. Cogan, D. G. : Myasthenia gravis. Arch. Oph-thalmol. 74:217, 1965.
3. Retzlaff, J. A., Kearns, T. P., Howard, F. M., and Cronin, J. L. : Lancaster red-green test in evaluation of edrophonium effect in myasthenia gravis. Am. J. Ophthalmol. 67:13, 1969.
4. Wyse, E. P., McConahey, W. M., Woolner, L. B., Scholz, D. A., and Kearns, T. P. : Ophthal-molopathy without hyperthyroidism in patients with histologie Hashimoto's thyroiditis. J. Clin. Endocrino! Metab. 28:1623, 1968.
5. Lindsay, S., Dailey, M. E., Friedlander, J., Yee, G., and Soley, M. H. : Chronic thyroiditis. A clinical and pathological study of 3S4 patients. J. Clin. Endocrinol. Metab. 12:1578, 1952.