Embed Size (px)
Citation preview

J. Neurosurg.: Spine / Volume 9 / November 2008
J Neurosurg Spine 9:000–000, 2008
483
An abnormally low CSF pressure (< 6 cm H2O in the lateral recumbent position), in the absence of lumbar puncture or known trauma within the cen
tral nervous system, is clinically referred to as spontaneous intracranial hypotension and is typically characterized by postural headaches.15 This uncommon condition has been reported more frequently in the past decade with the widespread use of MR imaging. However, when a CSF leak is in the cervical region of the vertebral column, it can be very difficult to locate despite the recent advances in imaging. An EBP performed in the lumbar region has been found to be very effective in treating cases of intracranial hypotension due to lumbar puncture.1,7 Performing an EBP in the cervical region can be very challenging given the narrow space, that the volume of blood to inject is not known, and the proximity to important neurological structures. Although cases in which an EBP has been applied at the thoracic and low cervical regions have been reported in the recent literature,2,6,8,10,19 to our knowledge
only 2 cases involving an EBP procedure performed at the C2 level have been reported.9,14 The uniqueness of the present case report lies in the neurological presentation of bilateral recurrent subdural hematomas due to a high cervical dural tear and in the nonsurgical conservative treatment.
Case Report
History and Presentation. This 56yearold previously healthy man presented to our hospital with a 4month history of progressively worsening headache and pain in the neck accompanied by nausea and vomiting. Headache was primarily occipital in location and radiated to the parietal region bilaterally. His symptoms were absent when lying down and worse when sitting up or standing. He did not have any fever.
The patient’s symptoms had started 4 months earlier as low back pain following a day of heavy physical activity. When he did not get any relief after taking nonsteroidal antiinflammatory drugs for pain for about 2 weeks, he was evaluated by his primary care physician.
J. Neurosurg.: Spine / Volume 9 / November 2008
J Neurosurg Spine 9:483–487, 2008
Occult cervical (C1–2) dural tear causing bilateral recurrent subdural hematomas and repaired with cervical epidural blood patch
Case report
AsokumAr BuvAnendrAn, m.d.,1 richArd W. Byrne, m.d.,2 mAruti kAri, m.d.,1 And Jeffrey s. kroin, Ph.d.1
Departments of 1Anesthesiology and 2Neurosurgery, Rush University Medical Center, Chicago, Illinois
The authors report the case of a 56yearold previously healthy man who presented with a 4month history of postural headache accompanied by nausea and vomiting. The results of initial imaging studies of the brain were normal. Repeated MR imaging demonstrated bilateral subdural hematomas which were drained and reaccumulated over a period of time. Spinal myelography revealed a cerebrospinal fluid leak at the C1–2 level. A cervical epidural blood patch, with repeated injections of 10 ml autologous blood at the site of the leak, dramatically improved the headache within 24 hours and eliminated the recurrent subdural hematomas. The results of followup computed tomography of the brain at 1, 4, 8, and 16 weeks were normal, and at 1year followup the patient was completely free of symptoms and working. (DOI: 10.3171/SPI.2008.9.11.483)
key Words • bilateral subdural hematoma • cervical dural tear • epidural blood patch • spontaneous intracranial hypotension
483
Abbreviations used in this paper: CSF = cerebrospinal fluid; EBP = epidural blood patch.
A. Buvanendran et al.
484 J. Neurosurg.: Spine / Volume 9 / November 2008
After a physical examination of the patient’s back and neck, the primary care physician recommended massage therapy and chiropractic manipulation. The patient stated that he developed a newonset headache and pain in the neck immediately after the massage therapy. The symptoms worsened even further during the next 2 days. He consulted a chiropractor who referred the patient to the emergency service of a local hospital. At the emergency room a CT scan was performed and did not show any gross abnormality.
After neurological workup, including brain MR imaging, revealed no explanation for the headaches, the distinct postural nature of the patient’s symptoms was recognized and intracranial hypotension was suspected. The patient was then referred to a local pain clinic where a lumbar EBP procedure (15 ml of blood injected) was performed; the patient was sent home immediately after the procedure. After about 24 hours of relief, the patient’s symptoms reappeared and he was brought to the emergency service of our hospital.
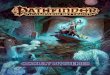
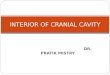
Operation and Postoperative Course. Magnetic resonance imaging of the brain revealed bilateral subdural hematomas (Fig. 1A). The patient became confused and progressively symptomatic from the subdural hematomas, necessitating surgical drainage. Because of the distinct postural nature of his headaches, an idiopathic CSF leak was suspected. An MR image of the spine did not reveal evidence of CSF leak (Figs. 1B and C). Due to our suspicion of a CSF leak, a lumbar EBP procedure was performed with 20 ml of autologous blood (with bed rest for 24 hours after the procedure), resulting in relief of headache and associated symptoms for a week. Nevertheless, the patient’s symptomatic subdural hematomas recurred and he presented again to the emergency service (Fig. 2A), requiring surgical drainage of the hematomas. After the second subdural drainage surgery a spinal column CT myelogram was performed. This study revealed an occult C1–2 CSF leak (Figs. 2B and 2C).
Since 2 lumbar EBPs had failed, after obtaining con
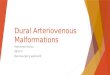
sent and explaining the risk, we took the patient to the operating room for cervical EBP placement. The epidural space was entered at C6–7 using the lossofresistance technique with the aid of fluoroscopic guidance and with the patient in the prone position. A radioopaque epidural catheter was then threaded up to the junction of C1–2, with the position confirmed by injection of contrast medium demonstrating cervical nerve root spread (Fig. 3). The epidural needle was removed and the catheter secured, and the patient was then turned supine. The patient was oriented and could cooperate for a complete neurological examination. Sterile autologous blood (10 ml) was injected via the catheter slowly with frequent neurological examination over a period of 30 minutes. The catheter was then flushed with 1 ml of saline and left in place, to allow a repeat injection the next day if needed. The patient was transferred to the neurointensive care unit for monitoring and remained at bed rest. The following day, in the intensive care unit, the patient had a dramatic improvement in symptoms, but still had a slight headache when an upright posture was attempted. A test dose of lidocaine (3 ml of 1.5%) was injected via the catheter to confirm that the epidural catheter had not migrated. With the patient fully awake to cooperate for repeated neurological examination, a second EBP was applied, again using 10 ml of autologous sterile blood, and the epidural catheter was then pulled out. The patient was instructed to observe strict bed rest for the next 24 hours. After the second cervical EBP procedure, the patient’s postural headache symptoms improved dramatically within 24 hours. Followup CT scans of the brain at 1, 4 (Fig. 4), 8, and 16 weeks showed no recurrence of hematomas. All the patient’s symptoms resolved. He returned to his regular work 3 months after the treatment; and at 1year followup he was asymptomatic.
DiscussionA patient with intracranial hypotension typically pre
Fig. 1. A: Axial T2weighted brain MR image obtained at presentation showing bilateral subdural hematomas. B: Sagittal cervical MR image obtained before subdural hematoma evacuation because of our suspicion of CSF leak. C: Sagittal thoracolumbar MR image obtained before subdural hematoma evacuation.
J. Neurosurg.: Spine / Volume 9 / November 2008
Epidural blood patch at the C1–2 level
485
sents with headache, nausea, vomiting, and neck stiffness. Several conditions, including viral meningitis, migraine, tension headaches, cervicogenic headaches, sub arachnoid hemorrhage, intracranial tumors and other spaceoccupying lesions, and sagittal sinus thrombosis can produce a clinical picture similar to that of spontaneous intracranial hypotension. However, intracranial hypotension should be included in the list of differential diagnoses (suspected) when the above symptoms worsen when the patient is sitting or standing and improve when the patient is lying down. Low opening CSF pressure (< 6 cm of water) is also a typical finding in patients with intracranial hypotension, although, in cases of CSF leaks that are small and/or intermittent, the opening CSF pressure can be seemingly normal. When subdural hematomas are present, the pressure may be normal or high.
Invasive procedures have been the most commonly reported causes of intracranial hypotension. However,
intracranial hypotension following manipulative therapy such as massage and chiropractic therapy has also been reported.16 Although in our patient it was not determined what the exact cause of intracranial hypotension was, we believe that the massage therapy did play a role in worsening the CSF leak and the associated symptoms. The downward displacement of the cerebrum and the brainstem due to intracranial hypotension exerts a shearing force on the bridging veins in the subdural space causing them to bleed bilaterally into the space,4,5,15 which is what probably happened in our patient twice.
Computed tomography myelography, radionuclide scanning, or MR imaging can be used to confirm the clinical diagnosis of CSF leak. Radionuclide scans are less useful than CT myelograms for initial screening.15 Magnetic resonance images and CT myelograms may reveal pachymeningeal enhancement, CSF accumulation in the subdural space, subdural hematomas, compression of
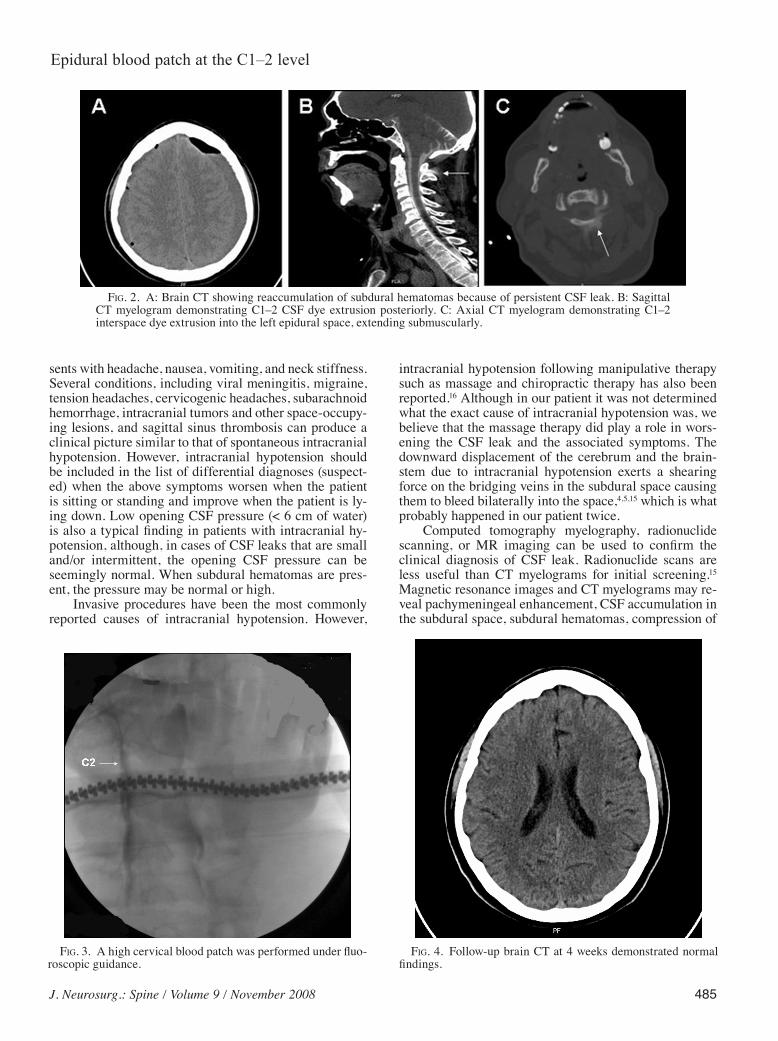
Fig. 2. A: Brain CT showing reaccumulation of subdural hematomas because of persistent CSF leak. B: Sagittal CT myelogram demonstrating C1–2 CSF dye extrusion posteriorly. C: Axial CT myelogram demonstrating C1–2 interspace dye extrusion into the left epidural space, extending submuscularly.
Fig. 3. A high cervical blood patch was performed under fluoroscopic guidance.
Fig. 4. Followup brain CT at 4 weeks demonstrated normal findings.

A. Buvanendran et al.
486 J. Neurosurg.: Spine / Volume 9 / November 2008
underlying parenchyma, and herniation of the brainstem. In our case, however, the presence of bilateral subdural hematomas may have obscured low pressure changes in the brain on the MR image. Full spinal MR imaging was unrevealing. This case demonstrates the continued importance of myelography in cases of CSF leak, although there is always the concern that a CSF leak could occur as a result of the myelography procedure itself. In the future, newer sequence techniques in MR myelography may provide highquality images of the subarachnoid space without the need for radiation or intrathecal contrast material.18
Conservative management for occult CSF leak with bed rest, hydration, caffeine, abdominal binders, and analgesics may be useful initially, and in some cases may even be the only treatment required. If conservative management fails, then an EBP performed in the lumbar region is an initial choice of treatment. The first lumbar EBP performed at another hospital did give shortterm symptom relief, and that is why we choose to perform this relatively lowrisk, commonly performed procedure at our hospital. A lumbar EBP increases the intrathecal pressure by compressing the dural sac and also seals the defect, if the leak is in the lumbar region. However, a lumbar EBP may not be as effective in sealing a leak that is located higher in the cervical region. This may be because the blood introduced via the lumbar region may not effectively seal the defect. Sealant effect of the blood in the epidural space is more crucial than the tamponade effect in providing longlasting relief from symptoms. An EBP performed directly at the site of the leak will seal the dural defect more effectively.2 This has been confirmed in rat experiments in which an EBP at the site of a dural leak restored CSF pressure to normal, but an EBP injection 2 cm away was unsuccessful.11 In our case, the patient did not obtain lasting relief following either of the 2 lumbar EBPs. The repeated formation of bilateral subdural hematomas and the relatively long duration of symptoms in this patient indicate the chronicity of the condition that also may have contributed to the failure of the lumbar EBPs. In cases such as this, locating the site of the leak on a CT/myelogram and performing an EBP directly at that site is very effective in providing dramatic and longlasting relief, as was seen in our patient. However, caution needs to be observed when performing cervical EBP, and as in this case the patient has to be able to cooperate with repeated neurological examinations during the slow injection of the epidural blood. We did not perform the CT myelography first because of the presence of symptomatic bilateral subdural hematomas and our concern that the lumbar puncture necessary for CT myelography might worsen the patient’s condition by lowering his intracranial pressure or causing a confounding lumbar CSF leak because his thecal sac was under pressure due to the intracranial subdural hematomas
Cranial subdural hematomas have been reported as a rare complication of spinal surgery17 and of spinal fluid drainage.3 Only 2 other previous cases have been reported in which a spontaneous occult CSF leak has caused cranial subdural hematomas.12,13 As in our case, the hematomas recurred prior to CSF leak repair, illustrating
the necessity of identifying and repairing the CSF leak immediately after evacuating the hematomas. This is the first case of spontaneous CSF leak leading to cranial subdural hematomas repaired by a high cervical blood patch. Although we cannot be absolutely certain that the high cervical dural tear caused the subdural hematomas, treatments that did not target the cervical region did not prevent recurrence of the subdural hematomas. Only when we targeted the cervical leak did the recurrent subdural hematomas and patient’s symptoms resolve.
Complications of cervical EBPs include spinal cord and nerve root compression, chemical meningitis, intrathecal injection of blood, seizures, and stiffness of the neck.
Given the seriousness of the complications, patients should be monitored closely during the procedure as well as for several hours after the procedure. In addition, the exact amount of blood to be injected for these procedures has not been studied; given the narrow nature of cervical structures compared with the lumbar region, however, we anticipated that 10 ml blood would achieve the desired effect of sealing the dural tear. For some physicians, a direct surgical repair may be an appropriate option. In conclusion, in cases in which a postural headache precedes the formation of subdural hematomas, a strong suspicion of occult CSF leak should be maintained.
Disclaimer
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
References
1. Coombs DW, Hooper D: Subarachnoid pressure with epidural blood patch. Reg Anesth 4:3–6, 1979
2. Cousins MJ, Brazier D, Cook R: Intracranial hypotension caused by cervical cerebrospinal fluid leak: treatment with epidural blood patch. Anesth Analg 98:1794–1797, 2004
3. Dardik A, Perler BA, Roseborough GS, Williams GM: Subdural hematoma after thoracoabdominal aortic aneurysm repair: an underreported complication of spinal fluid drainage? J Vasc Surg 36:47–50, 2002
4. Fernandez E: Headaches associated with low spinal fluid pressure. Headache 30:122–128, 1990
5. Fishman RA, Dillon WP: Dural enhancement and cerebral displacement secondary to intracranial hypotension. Neurol-ogy 43:609–611, 1993
6. Frank LR, Paxson A, Brake J: Spontaneous intracranial hypotension–a case report. J Emerg Med 28:427–430, 2005
7. Gormley JB: Treatment of postspinal headache. Anesthesiol-ogy 21:565–566, 1960
8. Hayek SM, Fattouh M, Dews T, Kapural L, Malak O, Mekhail N: Successful treatment of spontaneous cerebrospinal fluid leak headache with fluoroscopically guided epidural blood patch: a report of four cases. Pain Med 4:373–378, 2003
9. Inamasu J, Nakatsukasa M: Blood patch for spontaneous intracranial hypotension by cerebrospinal fluid leak at C1-2. Clin Neurol Neurosurg 109:716–719, 2007
10. Kantor D, Silberstein SD: Cervical epidural blood patch for low CSF pressure headaches. Neurology 65:1138, 2005
11. Kroin JS, Nagalla SKS, Buvanendran A, McCarthy RJ, Tuman KJ, Ivankovich AD: The mechanisms of intracranial pressure modulation by epidural blood and other injectates in a postdural puncture rat model. Anesth Analg 95:423–429, 2002

J. Neurosurg.: Spine / Volume 9 / November 2008
Epidural blood patch at the C1–2 level
487
12. Mikawa S, Ebina T: Spontaneous intracranial hypotension complicating subdural hematoma: unilateral oculomotor nerve palsy caused by epidural blood patch. No Shinkei Geka 29: 747–753, 2001
13. Mizuno J, Mummaneni PV, Rodts GE, Barrow DL: Recurrent subdural hematoma caused by cerebrospinal fluid leakage. Case report. J Neurosurg Spine 4:183–185, 2006
14. Rai A, Rosen C, Carpenter J, Miele V: Epidural blood patch at C2: diagnosis and treatment of spontaneous intracranial hypotension. AJNR Am J Neuroradiol 26:2663–2666, 2005
15. Schievink WI: Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA 295:2286–2296, 2006
16. Schievink WI, Louy C: Precipitating factors of spontaneous spinal CSF leaks and intracranial hypotension. Neurology 69: 700–702, 2007
17. Sciubba DM, Kretzer RM, Wang PP: Acute intracranial sub
dural hematoma following a lumbar CSF leak caused by spine surgery. Spine 30:E730–E732, 2005
18. Stone JA: MR myelography of the spine and MR peripheral nerve imaging. Magn Reson Imaging Clin N Am 11:543–558, 2003
19. Waguri N, Tomita M, Hayatsu K, Okamoto K, Shimoji K: Epidural blood patch for treatment of spontaneous intracranial hypotension. Acta Anaesthesiol Scand 46:747–750, 2002
Manuscript submitted March 20, 2008.Accepted August 4, 2008.Address correspondence to: Dr. Asokumar Buvanendran, De part
ment of Anesthesiology, Rush University Medical Center, 1653 W. Congress Parkway, Chicago, Illinois 60612. email: [email protected].