Embed Size (px)
Citation preview

Obsessive-Compulsive Symptoms in Prader-Williand "Prader-Willi-Like" Patients
MATTH EW W. STAT E. M.D .. ELISABET H M. DYKEN S. PII.D .. BETH ROSNER, M.A.. AND RES MART IN, M.D.,
ANll BRYAN H . KINe . M.D.
ABSTRACT
Objective: To compare obsessive-compulsive (OC) symptoms in patients with Prader-Willi syndrome (PWS) and symptoms
in a group of pat ients present ing with "Prader-Willi- like" features but without the gene tic abno rmalit ies associated with
PWS. Method: 16 patients aged 4 through 20 years were evaluated in a clinic specializing in the assessment and manage
ment of behav ioral and food-related problems in PWS . Eight patients were found to have key features of the syndrome but
did not have a PWS genotype. These PWS-like subjects were matched to 8 clinic patients with a confirmed deletion of the
PWS critical region of the paternally derived chromosome 15. All subjects were evaluated for obes ity, 10, food-related prob
lems , maladaptive behav iors, and non-food-related OC symptoms. Results: There were no differences between the 2
groups with respect to mea sures of obesi ty, 10. food-related difficulties, or overall maladaptive behaviors.The PWS group
showed significantly greater numbers of OC symptoms and greater symp tom severity. Conclusions: Patients with PWS
have elevated numbe rs of OC symptoms and significant symptom-related impairment which are not explained by devel
opmental delay, food-related difficulties, or obesity. OC symptoms are part of a behavioral phenotype that accompanies
deletions on the proximal long arm of chromosome 15 in PWS. J. Am . Acad. Child Adolesc. Psychiatry, 1999,38(3):329-334.
Key Words: Prade r-Willi syndrome, obsessive-compulsive disorder, mental retarda tion , behav ioral pheno types.
Prader-Wi lli syndrome (PWS) is character ized by m ultiple co ngenital anoma lies and results from abnormalitiesinv olving th e proximal long arm o f chromoso me 15(H olm et al., 1993). The m ost commo nly recognizedma nifestations of PW S include in fanti le hypoto nia an dfailure to thrive. hypogonad ism , sho rt stature, m ild to
mo derate me ntal reta rda tion, and th e ch ildhood onset
A"""/, I,.d S"/,I"ml/(/' 1 I. l 'JlJH.hom til" (},ild Sllidy COII"r, };,I"UnircrsirvS,.f,oolo(Mt'fli,.in". M 'II' Hare»,
CT (Drs. Si.n , ,/lid /l1'1I'Iin ): thr N(l/ nJ/,,} ,.hialri,. l nstitutr, Unirrrs it v o(
California, I.OJ Angel"J (Dr. /J),I." '//J aud Ms. Rosner): ./Iltl Dep.mmrnts III'!'s} ,.J,i'lIr)'and !'"di,lIri",. f),ITlmlllltl, Hird lma· Al,.di,.,11 (,; '/11,.,. 'Illfl ( }, ildrm ,
Hospital at Dartmonrh, 1." f,ttl IIJII. N H (L)». A·ing).
Presented ,1/ tl ir 1'J'Ni m{'{'ling o( tbr A mrri r.m A,ml"m )' 'if' Cf,ild '/IltlAdoiescrnr !'s),,.f,i,lfry. .\'1I/,/,lIrll'd in /,lIrt f, )' , JII Hi I.illy !'i/{/{ /{,.u ,lr,.f, AII'llI'd
and NIMH 'I'r'l in ing Granr MII-/'J ll(' (Dr. .\'1<111' ) ,/lid NICHIJ !'mgram
Projert Gra/ll !'Ol- H IJ-O.j()OH-.l1 (D rs. SI,If", Dykl'1lJ, Marrin). Tb« authorsIht/lJ ~' \\"~~)'11{ ' ( ,'m,{y, Lori , "~"iJJtI _\ . Afidltl d \\"~ 'ill l'1~ [an II'llli"/~Y, l 'au] Bolit«,
Lisa Davis, Liud« Florry. '/lltl l/ill l.oj k'JI'i,,/i,r thrir inra luahlr contrilnuious 10
If,( lICIA l 'radrr- IFilli tIini c. dJ/l1 ./<WI{'S lrclauan. /)' /I'it/ 1:11115. Grn« I-/s"/I.A ntho nv ( '1111 drn Pal. Paul l.omhroso . am! \\'{tlrt'r ( ;illitlm j in"thei r hdplitl com
ments tlurillg thr /'rep'l1tuio1l (~r ,b is ma nuscript .
/{"priJII r{''!"''m 10 Dr. SI,I/,·. l·liH SliM , };i/I' Ooilt/ SIIlt/)· C;'JI/<'I; };i/, 'Unirrrsitv Sd/(/"I "I' Affdi,.i" ". l .W SOUI!I FroJlhlg" /{Odt!. I!( ). I/o." l(} 7'JOO.Nru- Haren, Cl O(''jl O; e-mail: A1'1/1!'{'u-.SI,I/"!;11};d ,,.l'flu.
OH')O-H5(,7 /1)1)i.>HO.\ ·O.\2 1)/$ O'\.OO/O 'I'! }I)') ') hy till' A merican Acade my
of C hild and Adolcsccru I'sychi arr v,
I . AM . ACAIl . Ul ll.I l AlllII ES C. I'S YC Il IATHY. .\ H: \ . ,\ l AHI' I I I I) ') ')
of hyperph agia. whic h reg ula rly lead s to severe foo d related diffi culties incl udi ng food foragi ng and lifethreaten ing ob esity (Prade r ct al., 19 56). H owever. thosewith PWS also su ffer from behavioral and emo tio na ld ifficult ies not rela ted to foo d, incl ud ing temper tantrums, dramatic mood lability. stubbo rn ness, skin pick
in g and obsessive and co m p u lsive sym p to ma to logy(Dykens and Cassidy, 1995; D ykens et al., 1992 , 1996;W hi tman and Accardo. 1987). Moreover. the degree ofresulting psychiatric impairment is often very severe.W hile child ren and ado lescents with PWS have, on average, mi ld levels of cogn itive delay (C urfs et al., 199 1;D yken s cr al., 1992 ), th eir beh avioral and psychiatricdysfunction typically results in highly restri ctive levels ofcare and is often the so urce of enormo us d istress forpatients and their fam ilies (Hodapp et al., 1997).
Recent stud ies have underscored the degree to wh ichchild ren, ado lescents, and ad ults wit h PW S suffer fromnon-food -related obsessive-co m pulsive (OC) sym pto ms(Dykens and Ca ssidy, 19% ; Dykens ct al., 1996; Steiner al., 1994). Dykens and co lleagues found th at PWSsubjects have an average of 3 d ifferent obsessions andcompulsions as measured by the Yale-Brown O bsessiveCo m p ulsive Scale (YBOCS) (D ykens ct al. , 1996 ).
329

STATE ET AI..
Moreover, when PWS patients are compared with nonmentally retarded adults with obsessive-compulsive disorder (OCD), the 2 groups are quite similar, demonstrating equal levels of symptom-related distress andfunctional impairment (Dykens et al., 1996). Thesefindings are particularly striking when contrasted withthe relatively low prevalence of oeD in patients withretardation of mixed etiology (Menolascino et a!', 1986;Vitiello ct a!', 1989).
In addition, Dykcns and Kasari identified a distinctset of signs and symptoms which reliably distinguishedPWS children from children with Down syndrome orwith nonspecific mental retardation. These includedobsessions, compulsions, and skin picking (Dykcns andKasari, 1997). Other studies have supported high ratesof repetitive behaviors, pcrseverativc speech, and skinpicking in subjects with PWS (Clarke ct al., 1996;Schepis er al., 1994; Stein ct a!', 1994).
However, questions remain about the strength of the
association between OC symptoms and the PWS genotype. for instance, OC symptoms could conceivably ariseas a psychological consequence of hyperphagia and maynot be indicative of PWS per se, but rather a secondarycharacteristic of persons with significant food preoccupations. Along similar lines, the combination of excessive appetite and mild to moderate cognitive delay couldlead to repetitive behaviors such as repeated questioningor the need for reassurance which might mistakenly becharacterized as non-food-related OC symptoms, especially when studies rely on parental or caregiver report.Finally, researchers have tended to recruit subjectsthrough PWS advocacy groups (Clarke er al., 1996;Dykcns and Kasari, 1997; Dykens er a!', 1996; Steinet a!', 1994) and therefore have difficulty controlling forthe impact of reporting bias. It could be that parents andguardians of PWS subjects are inadvertently reconcilingtheir reports of oe symptoms with widespread ideasabout how persons with the syndrome generally behave.
To clarify the association of oe symptoms with thePradcr-Willi genotype, we have compared subjects withPWS with a particularly powerful control group whopresented to a clinic specializing in the assessment andtreatment of behavioral problems in PWS. All subjectsincluded in the study presented with key features of PWSincluding obesity, food preoccupations, maladaptivebehaviors, and mild to moderate mental retardation orlearning difficulties. However, patients in our comparison group were found not to have a genetic lesion asso-
330
ciated with PWS. This "PWS-like" group was matchedwith a group of patients with a confirmed diagnosis ofPWS because of a deletion on the paternally derivedchromosome 15. We hypothesized that the 2 groupswould show similar levels of behavioral problems burthat the PWS group would show higher rates of OCsymptoms and symptom-related distress.
METHOD
Subjects
The study included 1(, subjects. 4-20 ycars of agc (mean 12.3years). Eight subjects had PWS associated with a deletion of theI'WS critical region of the paternally inherited chromosome I'i. andHdid not have a PWS genotypc. All study participants presented forevaluation to a clinic specializing in the assessment and treatment ofbehavioral and tood-rclarcd problems in PWS.
[)uring the first 12 months the clinic was in operation. a total of 8children. adolescents, and young adults presented with behavioralcomplaints. difflcultics with Iood, and mild to moderate mentalretardarion hut either faikd to meet diagnostic criteria for I'WS(Holm et al.. !')'),)l or had previously had genetic rcsring that did notidentify a I'WS genotypc (Anonymous, 1')')6). Patients who presentedto our clinic without .1 confirmed diagnosis of I'WS were o fTc redmolecular gcnetic testing using mcthylarion-scnsit ive restrictioncnzymcs to rule out abnormalirics on chromosome l'j at the locusq l l-q U (Anonymous. 1')')(,; Driscoll cr al., 1')')2). These tests wereperformed in the laboratory of Dr. Wayne Crody at LJCLA. Themcrhylarion-scnsitive restriction cnzyme technique allows identihcarion of the most common types of genetic problems that lead to
PWS including delctionx on the paternally transmitted chromosomeand maternal uniparental disorny (inheriting 2 copies of the maternal chromosome and no paternal chromosome). All patients catcgorizcd as PWS-likc in this study underwent this tcsting and werencg.uiv« fi,r a PWS genotypc.
A total of 60 patients presented to the clinic over the same periodwho met clinical diagnostic criteria for I'WS and/or had confirmatory genctic testing (Anonymous. 1')')(,). From this group, the first Hpatients who presented chronologically to the clinic with confirmeddeletions of chromosome l'j (either by cytogenetic analysis or Huorcsccncc in situ hybridizarion) and who matched the PWS-like grouphy age and gender were idenrificd as the I'WS group.
At rh« time of initial evaluation, (, patients had a diagnosis ofimpulse control disorder not otherwise specified (NOS) (3 from theI'WS group and 3 from the I'WS-like group). One patient in thePWS-like group had a diagnosis of OCD and eating disorder NOS.and one patient from the PWS group had a diagnosis of anxiety disorder NOS. All patients with borderline intellectual functioning ormental rctardarion had the appropriate diagnoses on Axis II. Onep.uicnr from each group had a history of seizures. One patient wasraking medication fill obsessions and compulsions at the time of presentation. This subject was in the PWS-like group and was heingtreated with a selective serotonin rcuprakc inhibitor,
Measures and Procedures
I'arenrs and carcgivers of patients who arranged fill evaluation inour clinic were mailed a previsir packer which they were asked to
cornplcre prior to initial prcscnrarion. This packer included thefililowing:
I A~1 ACAIl. CIIII.l) Alll)I.ES(' PSYCHIATRY, .\H:.\, ~IARCH I')')')

f)"lJ/oj';lilphic QI/'·51iolllll1ili ·. A demograph ic qu esrionnairc requ estediu fo rm arion r~ga rd i ng rhe pati ent's age. sex, IQ. height. weight, living and work arrangcmcn rs, and gen~tic t~st ing status.
};t!,.-Rml/'II Obsrssit» COIJ/pl/Ish·,·Sra!«. Parents a nd caregiver» of allpat ients pr~s~nting 10 the clin ic fill~d UUl an info rma nt version of theYHO C S (C ood man ct al., 1'J89a ,b ), whic h has been shown 10 hawguo d reliabil ity and validi ty (see Skc kercc er al., 1'J96: and Tay lor,1'J'J'i ). T he version used in thi s srudv co nsists uf a 'i6-item check listuf (K : sym p to ms which is drawn ' fro m th e ad u lt ve rsio n u f th eYHOCS, th ough it covers all sym plOm areas co n tained in th e chi ldversion's checklist. Each item is rated as ht'ing pres~nt ever or in rhepr evio us week. Three addit ional ite ms asses s sy m plOm severi ty.Infi lllll ants art' asknl to rare. on a S-po in t xcale , the extent 10 wh ichobsession a nd compulsions ( I) art' tim e-consurn ing: (2) are di stressful : and (3) cause social or occupat ion al im pairment (0 = none, 1 =m ild , 2 = moderate, .~ = severe, and If = ext reme). For the infurmalllvers ion of the checklist, YHO C S item s arc reworded 10 reHcct inl o rmanr rather than self-ratings ,
Child IMltll'ior Chl'ckliJI. The C hild Rellavior Chccklisr (CHCl.)(Achenba ch , 1'J91) is a widely used instr ument consisting of 112beh avio rs that arc rated on a scale from 0 10 2 (0 = not pr~s~nt; 1 =somew hat or somet imes true: 2 = vcrv t rue or often true). Tlu- ( :RCl.includes 8 "narrow-ha nd" and 2 bro :ltl-f.lClOr T sco res which den ot eoveral l in rcr na lizin j; a nd cxt crual izin g beha vior s. C RC L T sco resgreate r than 70 art' co nsidered 10 be in th e range of clinica l significance. T he C BC L is both a reliable an d valid mea sure uf psych opath ology in ch ildren and adolescents and has been used successfu lly inpreviou s studi es o f p~rsons with mental rerarda rion.
During the initial evaluation in clin ic, th ese measures were reviewedwi th a clin ician (M .W.S.. E.M .D.. H,H ,K. ). All the pati ents in th estudy had a co m pleted set of instrumen ts. Sym pto m endorsem entso n th e YROCS whi ch pert ained 10 food were di scarded. For exampic. the checklist item "ritua lized cating behavior s" was not inc ludedin the tally of symplOms. On present at ion 10 rhe clini c. all patientshad vita l signs mea sured and reco rded . includ ing heart rate . bloodpressure . he ight. weight. and head ci rcu mference , Body mass index(B M !) was calculated hy the for m ula wei ght (kgl/ he igh t ( ml ~
(Smal ley et al., 1990) , Paricn rs and ca regive rs were cli nically int erviewed by o ne of the author s (M .W.S.. E. M .D .. H.H.K.l, and . inGISCS in whi ch recent cognitiw t~st ing was not available, an IQ evaluati o n was performed by a clin ician experien ced in cognitiw assessmcnr of patients with mental reta rdati on synd romes (E.M.D.).
RESULTS
Subject Characteristics
The PWS and PWS-like groups of patients werematch ed for age and gender and then assessed for significant differences in IQ. height. weight, BMI. and tot alC BC L scores. One-way analyses of variance (ANOVAs)revealed no sign ifican t differen ces between groups.However, BMI approached statistical significance. withthe PWS-like group tending to be more obese than thePWS group. Table 1 shows the means, standard deviation s, and F values for all comparisons. Given the trendtoward significance in a measu re of obesity, an additional analysis was undertaken to assess for any correla-
I . AM . t\C A D CIIIl.D AIll lI ESC . I'SYU IIAT RY. \ H: \ . .~I A I{( II I'>')')
oc:n SYMPTOM S AND I'RAD ER-WILI.I SYNDROM E
TABLE 1Subject C haracrerisrics
I'W S " I'W S-Likc"
Mean SD Mean SD F P
Age 12.4 4. ') 12.2 ').9 0.0076 .93IQ ')7 15.4 70. 6 23 1.7 'i .20Weig ht 126 .4 50 .4 16'i 102.9 0 .909 ..16BMI 25 .9 8.9 j(1.4 11.6 4. 18 .06.Ioral C HC I. 66 .7 17 .1 6R.9 23 0 .0 49 .82
Noli': Subjec ts with and wi tho u t I'rader-Willi syndrome (I'WS)were mat ched for age and sex an d then co m pared with respeCl to thevar iables listed in th e tabl e. HMI = bod y mass index calcu lated asweighr in kilograms di vided by height in meters squared: e ReL =C hild Behavior Checklis t (sec text).
rion between BMI, YBOCS scores, or total CBCL score.None of these were significant.
YSOCS
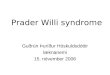
Both the number and severity of OC symptoms werecompared across groups using a Mann-Whitney U test.A nonparametric statistical analysis was chosen becauseof the small numbers in each group and the uncertaindistribution of the data. The Prader-Willi group showedsignificantly more OC sympto ms than the PWS-likecont rols. Figure 1A shows the distribution of scores forYBOCS symptom number and the mean s and standa rddeviations for each group. Relative to controls, subjectswith PWS also had sign ifica ntly higher ratings o fsymptom severity (Fig. 1B).
CSCL
To clarify these findings, we conducted follow-upone-way ANOVAs with 4 selected items from the CBCL:obsessions, overeating, compulsions, and skin picking.In all 16 subjects, endorsements on the CBCL itemregarding obsessions were related to food. Consistentwith our hypotheses. the 2 groups had similarly highlevels of food obsession s and overeating. However, thePWS group demonstrated significam ly more compulsions and skin picking than conrrols. Table 2 summarizes the means, standa rd deviations, and F values forthe PWS and PWS-like groups.
DISCUSSION
Patients with PWS had significantly higher numbersof non-food-related OC sympto ms as well as significantly increased levels of symptom-related severity com-
331

STA TE ET AI..
12 A 12 B
10 10'Il:
~ ~0 aI- a a:a, w~ * >>- w 6C/) 6 C/)
C/) C/)
o o0 4 0 4CD CD>- >-
2 2
00PWS "PWS-L1KE" PWS "PWS-L1KE"
Fig 1 A: 'Ior.il numbcr of Yale-Brown I.JI",'ssiw Com pukivc Se dl' (YI\( )( :~I Sl'I11Pto/ll.S ill subj"us wirh .uid with oUI Pr.ld",-Willi syl1 drnl11l' (pWS). I'm the pW~ group: 111 ' ''111 = (, , 2 ~ : ~I) 0 4,H(" I'm the pWS -lik,' subjects: I11l'.Il1
1..)7: SI) = IA I , ' /, 0 ,0 I ~ , 1\: YI\()(:S sYl11ptol11 wvcritv SlO rl'S t ~ Jr p.uicnt-, with and without pW'S, For till' pWS
group : 111 ' '' 111 = .l. ~ : Si l = 1.77, I;m the pWs -lik,' sl1bi,'cIS: I11l' .Il1 = I.H 7: Sll = 2.2'), 'r = ,O,)H, T hree sl'wr ityrrl.ucd qw..·, t io ll' .irc (o l. i11'11 (0 calc ul.ue the \ l.'Vl.: rit y index. T he: m aximu m po\"i!JIl' .... UHl· j ... 12.
TABLE 2O ne-Way Analysis of Variance of Fou r Items From the C B( :L
Comparing I'WS and "I'W S-Likl''' Croups
C BC L item ')')( )Vl'll':lling I.') 0,7(, I'i 11.5') I J, I ,224
C BC L item ')( )hsl',,,ions
(regard ing lood ) 1.(, 0.')2 i .» (1.5 ') 1.27 .272C BC L item (,(,
( .o rn pulsions I A IL7') 0,') O,7f, ').44 ,05 ')
C BC I. item ')1'
Skin picking I.'i IJ..\') (L') 0, 7(, 2 1.71 J )()0 4
N olt': C BC I. ~ C hi ld Behavio r C heck list; I'WS = I'rader-Wi llisynd rome,
pa red with co ntrols. O ur find ings are parti cularl y rob ustin that we compared subject s wi th PWS with a group ofage- and gender-mat ch ed d evelo p menta lly del ayed ,obese . food-preoccupied sub jects , Importantly. PW Sand PWS-like groups were simi lar with respect to IQ .levels of food-related di fficult ies, and overall levels ofpsychopathology based o n C BC:L sco res, W h ile th ePWS-l ike gro up tended toward h igh er mean weightsth an th e PW S grou p, ne ither weigh t no r BMI wasrelated [0 OC sym pw ms, sym pto m seve rity, o r maladaptive behaviors in eithe r grou p,
Our find ings are co nsistent with recent stud ies demonstrat ing high rat es of OC: sym pto ms in people withPWS (Dykens er al. , 19% ; Stein et al., \994) and delin-
I'WS " I'W S-Likl'''
Mean xn Mean xn F p
eating a distin ct ive behavioral phenotype for Prader-Wi llisubjects. In particular, O C sympto ms clearly d istingu ishpersons with PW S versus those with mental retarda tiono f m ixed et io logies or o the r ge ne tic ca uses, suc h asDown syndrome and Srnirh-Magenis synd rome (D ykensand Kasari , 1997; Smi th et al., \998). The present studyexpands on the current literature by allowing us to con trol for so me of the key ph en ot ypi c features of PW Swhile assessing the relat ion ship hetween OC sym ptomsand geno type .
In ligh t of th ese data. the he ightened levels of OCsymptoms in PW S cannot be acco unted for sim ply as aresult of patients havin g food preoccupations, obesity,and/or developmental delay. T he 2 groups were equallyfood-obsessed, had similar cog nitive abilities. and hadsimilar degrees of obe sity. It is possible that eating di fficu lt ies are experi enced di fferently by PWS pati ents thanby other developmentally delayed . obese adolescents andchildren and th erefo re result in part icularly severe psychological outco mes. However, all the available ind icesmeasured suggest that the 2 gro ups of pat ients in th isstudy not only were equally subject to food -related problems bur also were equ ally pron e to psychopathology ingenera l, thou gh not the development of O C sym ptomsin part icular.
Report ing biases are unlikely to have influ enced thesefindings. If parents and caregivers of PW S pat ients weremis tak ing food preoccupations with o ther non -fo odrelated OC symptoms, one wou ld presume that the par-
3.n I , A .\1. A ( AI ) . C II II I) ,\ I H ) II :,',( ' , 1'" YCIi IA TR Y, IH : I , ~lARCI I I ') '!')

ents and caregivers of the PWS-Iike subjects would demonstrate a similar propensity. Also, given the composition of the control group, the bias toward reportingsymptoms consistent with PWS would likely influenceboth sets of subjects. This is particularly the case as thePWS-like group generally sought evaluation because aclinical diagnosis of PWS had been suggested. In practice, it was usual for parents and caregivers of subjects inthis group to be familiar with the clinical picture of PWSand to present with a stated hope of obtaining a diagnosis.
The emerging identification of a behavioral phenotype in PWS raises the intriguing question of how theunderlying genetic lesion(s) might lead to these complexneuropsychiatric symptoms. In the case of PWS, no distinct brain area has been identified as grossly pathological by neuroimaging techniques, though there is but asingle controlled study in the current literature (Milleret al., 1996). The syndrome is thought, however, toinvolve significant hypothalamic dysfunction. Thishypothesis is supported by the common occurrence ofgrowth hormone abnormalities, temperature and sleepabnormalities, and delayed sexual maturation in PWS(Bray, 1992; Seyler et al., 1979; Swaab, 1997). In addition, a recent neuropathological study in PWS found adecrease in oxytocin (OXT) secreting neurons in thehypothalamic paravcntricular nucleus of postmortemPWS brains compared with matched control brains(Swaab ct al., 1995). OXT abnormalities have been linkedto OC symptoms more broadly through research whichhas demonstrated abnormally high levels of this neuropeptide in the CSF of a subgroup of patients with OCD(Leckman et al., 1994; Swedo et al., 1992). In addition,we have identified OXT elevations in the CSF of 5patients with PWS (Martin et al., 1998) compared withcontrols. It is difficult to reconcile the apparently conflicting findings that OC symptoms and PWS appear in somecases to be associated with increased CSF OXT whilethere also seems to be a significant decrease in OXT neurons in at least one important CNS nucleus in PraderWilli subjects. It is possible, however, that the techniquesused to identify OXT neurons in Swaabs study were notable to distinguish between a paucity of OXT-secretingcells and a normal population of cells that had been relatively depleted of OXT Regardless, what is clear at present is that multiple lines of investigation point to thehypothalamus as the prime brain region for additionalresearch into the relationship between the genetic underpinnings of PWS and its many behavioral consequences.
I. AM. ACAD. CIIIII) AIH)I.FS( I'SYCIIIATRY.\H:\. ,\IAR('1I 1')')<)
oc:n SYMPTOMS AND PRADER-WIl.l.I SYNDROME
Several methodological shortcomings limit the strengthof our findings. This study relied on a relatively smallnumber of patients, limited by the rarity of our naturalcontrol group. Larger numbers would have allowed foran analysis of OC symptom profiles both within andbetween groups as well as for some assessment of genotype-phenotype relationships in PWS patients. Furthermore, the study was naturalistic in that it includedpatients who presented for clinical evaluation. A~ a result,patients with other psychiatric and medical diagnosesand those taking medications were not excluded. Ofnote, only a single patient was being treated with anantiobsessional medication at the time these symptomswere assessed. This subject was in the PWS-like group.However, excluding this patient in a repeated analysis ofthe data had no impact on the statistical significance ofany of the results.
While the 2 groups appear to very similar along anumber of important criteria, there may have been someundetected differences between them, apart from thedifferences in genetic status, which would account forthe significant findings with respect to OC symptoms.Moreover, while the molecular genetic techniques usedto distinguish the 2 groups are able to identify more than95% of patients with the PWS genotype, it is possiblethat some patients in our PWS-like group could havehad an undetected PWS genotype. However, given thedirection of the differences found between the 2 groups,inclusion of PWS patients in our PWS-Iike group wouldhave served to minimize the differences between groups,making our findings even less likely to represent a type Ierror. It should be noted that our PWS group consistedonly of patients whose syndrome was caused by a deletion of chromosome 15. While at present there do notappear to be important phenotypic differences betweenpatients with varying types of lesions associated withPWS (Cassidy et al., 1997; Mitchell et al., 1996), furtherinvestigations are needed to clarify this issue as it pertains to behavioral and psychiatric sequelae. Under thecircumstances, we considered it prudent to rely on ahomogeneous group with respect to genetic causation.
Despite these limitations, our data extend findingsfrom several groups regarding the presence of OC symptoms in PWS patients and the central role of such symptoms in the PWS behavioral phenotype. The ongoingclarification of this phenotype may provide relevantinformation to psychiatrists and other physicians whotreat persons with PWS. Moreover, the continuing inves-
333

STATE ET AI..
tigation into the relationsh ips between genetic abnormalities and behavioral phenotypes promises to shednew light on the com plex int erpla y of genes, brain, andbehavior in the etiology of psychiatric illnesses.
Clinical Implications
The elucidation of particular psych iatri c sym pto mclusters in persons with PWS will help clinicians anticipate and recognize key behavioral difficulties that afflictthese pat ients and will highli ght for clinicians the importance of assessing and treat ing all the varied aspects ofthis synd ro me. A better understanding of th e PWSbehavioral phenotype should also provide families andpatients with a sounder basis for their expectations aboutthe course and natural history of the disorder. Finally, theclarificati on of th e relationship between OC sympto msand PWS ma y serve as an impetus for mu ch-neededclinical in vestigations of an tiobsessio nal tr eatments,pharmacological and otherwise. aim ed at helping thosewith PWS.
REFERENCESAchcnhach TM (1')<) 1). /11,/1/1,,11 fi/l' 1/'" tInld Brharior O".,Hi.'r/-j- IH 111111
/99 / I 'm!i ll'. Burlington : Un ivcrxitv ofVermo nt Ik paf[llll'nl of PsychiatryAnonymous (1')')(,), Diagnostic tesling f, ,, I'radn-Wi lli .uid Angk'lllall syn
drorn cs: rq'o f[ of rh c AS ~H ; /ACIsIC Te:st and -1" d lllOlogy Transl': rCornm irrcc. .111/./ 1//1111 ( ;1'111'1 ~ H : I O H ~-I OH H
Bray CA (1')<) 2), (;l'I1el ic. hyporh al.un ic and end ocrine lealu re.s of dini caland experimental obesity, I'rog Brain Res 'J.):.n .\- ,\40
( :a ~ ..idy SH. Fllr..;yd ll ' 1\1. Il t'cgl' f S ct ill. ( ]l) l)7), ( :olll l' ari \o !1 o f plu-norvp «between p.u icm« wirh Prudcr-\X!illi wn d rom« due..' ( 0 dl"h:l ion 1'1«.) ;lnduni p.u cn rnl dis o m y I ~ . .111/ ./ /l ll'l i ( ';'111'1 (,H:4,\.\ - !tIJ O
C larke DJ. Bon H , Chu ng Me:. Srurmcy p, Wl,hh 'I' ( 1') % ). Maladapt iv,'behaviou r in I'r.ulcr -\Xli lli syndro nll' in ad ult lit':, ./ 11111,11" ,-, IJi'lIbil R,',40: I ~')- I()~
Curt, LIs·1, Wiegers AM . So m mer» JR. Borghgrad" M , Fryns.lP ( 1') ') 1),Strength ., ilnd wl';lkIlC."i ."ie.:s in rhe.: ( ognirive.: protl le.: of Y(HlIlgste.:rs withI'rader-W illi wndronll' , Uill (,('lIt'14lH.IO· -4 ,\!t
Dr iscoll D.I. Wal ;' rs ~t1'~ W illiams CA el OIl. (1')')2). AD NA nll'l hl'lalionimprint, de.:re..· rmi ncd hy the..' sex of the.' p~lre..'nt . d i s l in ~lI i shcs rhe Angdmanand Pr,u,Ic..'r-W illi synd rome.:s_(;l"IlOmio 1.\:917- 924
DykCll s EM . Cass idy SB ( I 'J'J ~ ) . Corrl'b tes of m.lladapl ivc hel", vior in ch ildrClland adulls wilh Prader-Willi syndro me. .111/ ./ /l/rd ( ;1'11(/ (,o:~4(,-~4'J
Dykl'tlS EM. ( :assidy SB (1')')(,). I'radl'r-Willi synd roml': gClll'lil', heluvioraland rreall1lelll issul'S, C" i ltl Ad" I,·,.. I',, '.-!,i,lI r C'/ill N"rlf, Am 4:'J 1.\-')27
DyketlS EM, f {odap p RM . Walsh K, N,,, I, l..l (1')'J2). Adaptivl' and maladaplive hehavior in I'rader-Willi synd rome. / Am A.-tid Cf,ild Ad"I"./t' I',y,-f,i·IIlry ,I I: 11.\1-11.\(,
DyketlSEM, Kasari C ( 1'J')7) , Malad,lplive hduvior in child ren with I'r,llkrW illi .\ynd ronlc. [ )own .\ynd rome..·. and non spc( ihC nK'nral rc..'rartlatiol1.Am./ MI'1I/ R(/ ,ml 102:22H- 237
334
lJykClls EM. l.cckm.m .IF. Cas.s idy SB ( (')')(,). Ob sessioll.s ,Ind compulsionsin l' rudcr-Willi wndr o rn c. I C/liIrl / '< l'CIlOl l h .-f,itl l r y .F : 'J'J~ - 100 2
(;oodman WK, I'ri,:e LH, Rasmuss,'n SA 1'1 aL (1,)!l'Ja). T he Yale-BrownO h' l'.ssiw Co mpulsive Scah-, I: development , USl', and reliabi lity, Ar../'( ,;'11 1 '~ ),..f,i.I/IY 4(" 100(,- 10II
( ;oodnun \XlK . l'ricc l.H, Rasmussen SA "I OI l. ( ") H'Jh). The Yale-BrownO h"'" iw Com pulviv« Sealt'. II: validity Arch ( '(11 Psvcbiatrv 4(" 10!2- 1O 1(,
Hodapp RM , Dykcns EM. Masino 1.1 . (1'J')7). Families o j' children withl'rader-\'(' illi synd rome: slrc..'s.\-supporr and rel.n ions 10 ( hild cha racteriSlirs, ./ AUli'1I/ [ ),,/, lJ i.wrd 27: 11 - 24
Hol m VA, Cassid y SH, Butler M(; cr al. ( I'J').\), I'rader -W illi syndro me:UJIl."il'n SUS diagll o."i tk cr iter ia. l 'cdiatrics'); :j l)H-402
l.cckman .1 1\ ( ;ood man W K, North \XI(; ct OI l. (1')')4) . Elevated ccrchrospina!fluid lcvcl-, of oxyto cin in ohse..·ssi\'e-co mp ulsivt.' d isorder. tl n-" ( ; l'11
1 '~)'("i, l/r)' ~ I :7 S2-79 2
Mart in A. St.uc MW, Anderson t ;lsll,t OI l. ( I')')H), Ccrcbrospinal tluid levels ofoxyn x in in Pr.uler -W illi xyn dromc: a prelimina ry repo rt . Hioll~~)'( ""ill/l')l
44: 1.\4')-U~2
Mcn ol .isc ino 1'1. lcviras A, ( ;reill"r C (!')H(,) . The na tu re and type's of men tal illness in 1I11' mentally retarded . /',yef,opf,' lI"IlI,'((J[ 11111122:10(,0-10 71
Miller I.. Angulo M. Pricc D. "Elneja S (1')')(,), MR of the pituitary in patientswith l'r.uk-r-W illi syndrome: ,i ll' dctcrmi natiun and imaging find ing."I hli,u r R.ulio! 2ll:4.\-47
Mitchd l J. S, hinl el A, Langlois S "I 'll. ( I'J')()). Comparison of phcnu rype inun iparcn ral J i."i ol11)' and deletion Prade.: r-Willi synd rum c: Sl'X ."i pt:'l it'l l."d iff,·ren,,'s. .111/ .1Mn l (;t'ltt'l (,~ : I.\.I- I.\()
Pradcr A. Iahha n A. \Xlilli II ( I,)~('), Fin Symlrotll von Adiposiu.s, Klcinwuchs,Kryprorch ismu-, und ()ligophrL' nil' nach myo ronicarigcm ZlIstr;lIld imNeugeborenal ler, Sd""t'iz /l/nl WIr,ef,l'w,-hr H(,:1260-1 2(, I
Srhepis C. Failla 1'. S i ra~u"l M. Rom ano C (1'J')4), Skin-p icking: the bestcu taneous t<,'afllrl' in thl' re..·co~n i l.a t i on o f Prader-W illi svn d ro m c, /IJI.I[ )"""lIIlol _\.\ :H(,(,-H (,7
Seyln LE, Arulananrha m K. O 'Connor C F (1')7' )). l lypcrgon adorrop ichypogon ad isn: in th e Prudcr-Labh urr-W illi .' ynd rom,', '/ 1'1'(/i,l/r ')4 :
4 .\~ -4 .17
Skck ercc ( ; , lro vt R. 1I0~'Hl K (['J')(,). Th e Yak·-Browll (ll" " , iw C o m pulsiw Scale: interview versus self-report. IIt'f" II' RI'J Tbcr .\ 4 : (, 7 ~- (,H4
Smalley KL, Knerr AN. Kendrick ZV. Colliver .lA. Owen ( l E (1')')0). Rcas
,, 'ssml'nl of hody m.LS' indices, .111/ ./ eli" Nutr ~ 2 :40 ~ -40H
SllI id l At: . I )ykcfl ~ E. ( ;n'l' l1bl"l~ I: ( }t)\)H) , Bl.:h..vi or.rl phl.:llo typt· of Sm ith ·
'\ l.tg,'nis synd rome (del )7p 11.2), 1111/ ./ Mn l (,;'11" 1HI:17') · IH'>Slein 1).1 . Kc.u ing ] . Zar H.I . Hnll.mdcr I' (1')')4 ). A survey of rhc phcnnmc
nology and pharl11 ,ll orh crap y of com pulsive and i mpll l ~ ive-aggrc_"i\ i \'l'
,y m(lro l1l\ in Pr.idcr-Wi lli syndrome, J Nruropsvchiatry Cl ilJ Nr urosri(>:2,1·-2')
Swaah Ill' ( I')')?). I'rader-W illi 'y lld ro me '1I1<l lhe hypol halamu s. I k lll/\m l ill ir SII/'/'[ 4 2 .\ : ~ O-~ 4
Swaab Il l'. I'urh a .IS. Hofman MA ( I ,) ') ~ ) , Alln 'll iollS in Ihl' hypolhalamicp;lravl"lHril."ular nudell\ and it.\oXylocin neu ron s (put;llivl' s.n il'ry n ,lIs) inI'radn -Willi synd ronll': ,I ' lIIdy of Ii\'<' ClVes, ./ (.Ii" 1:'1Id"O"i ",, 1 ,\In.'"HO : ~ 7 ,\-~"')
Swedo SF , l.eon."d I II., Kru" i MJp el al. (1')')2) . Cereh r"'p ina l tluid1Ie..·un Khcl1li.\t ry ill child rcn aud adl .ll'sn·urs \\,jrh lJhst:'ssive..·-<.:nl11pulsiVl"distlrd e..·r. An"h ( J't'll 1 ~( }'l"hiil[I")' !J<):2 'J- 5(J
'l:lylor S ( I')')~ ). Ass(Ss lll ~nt of ;,hsessiollS and w llll' ulsion" reliabililY. validity ;llld !'lcnsirivi ry to rrcatm ent l,f1<" cts. C/ill 1 ~\yd1()/ Ri,t , 1,):2(ll--2<J(,
Viliell" B. Spreal S. Bl'har I) ( I'JH'»). ( l hsl'.Isivc-wlll l' ulsivc disorder in Illenlally tl'lardl'd pati"nls. ./ N",." /l lm l [)iJ 177:2.12-2,1()
Whitlll 'ltl BY, A'Tard" I' ( \'JH7). EnlOtio tl.ll SYllll'tolllS in Prader-\Xli lli 'yndrollle adol",r.'nt ' , tl lI/./ M l'rI (;ml'l 2 H :H')7-')() ~
I. AI-I. ACA I1. C II I 1.11 ..\ l lt ll. F.SL I'SYC Ii IAT RY, .I M: .I , 1-.1AI(I: II \""')