Embed Size (px)
Citation preview
OBJECTIVES
• Recognize risk factors for OSA
• Recognize potential complications of OSA
• Know how diagnose OSA
• Discuss treatment options
Snoring can be more than just noise!!New Insights to Obtructive Sleep Apnea
• Sheila Y. Garris, M.D., F.A.C.P., F.A.S.H.• Associate Professor Clinical Internal Medicine, EVMS• Certified Clinical Hypertension Specialist• President, Contemporary Medicine Specialists• Past President Leadership Board ADA Hampton Rds
Epidemiology
• Current Environment– OSA prevalence and importance– 4-7% adults affected– Men:women =10:1– 80-90% undiagnosed– Most affected age 40-70 with an Increase in prevalence by 7-20% ages 35-60 --Perimenopausal/menopausal women
more affected and is offset by ERT therefore gender difference is offset by age.
--Can affect children
33% of adults are at risk for OSA
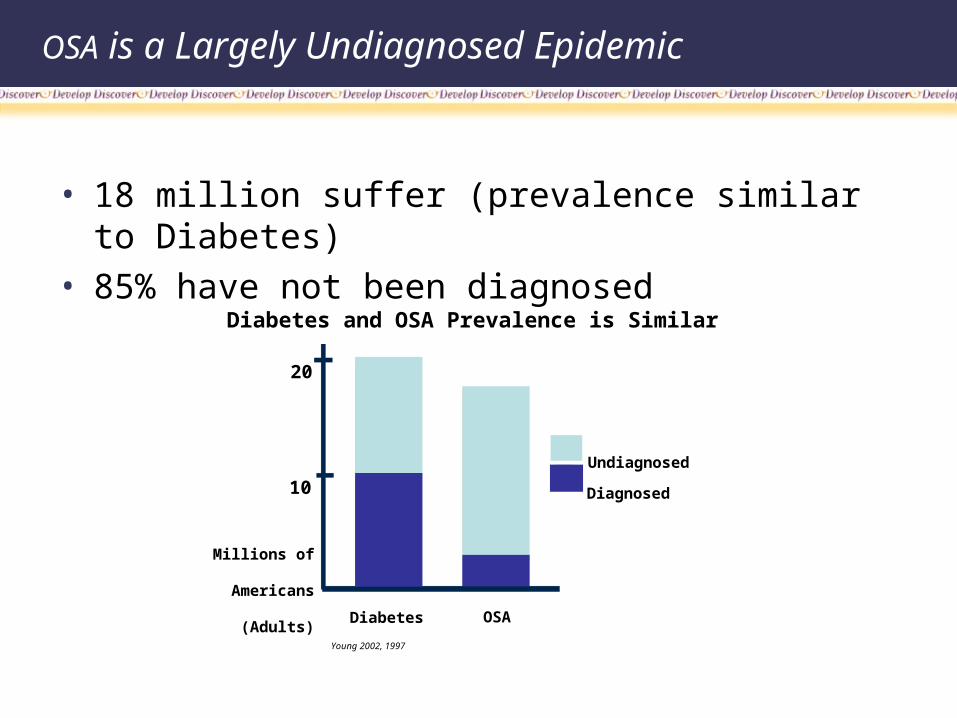
OSA is a Largely Undiagnosed Epidemic
• 18 million suffer (prevalence similar to Diabetes)
• 85% have not been diagnosed
Diabetes and OSA Prevalence is Similar
Diabetes OSA
Undiagnosed
Diagnosed
Millions of
Americans
(Adults)
10
20
Young 2002, 1997
Elevated Risk Factors
Male, overweight BMI>30 Over 40 years of age Neck size 17 or greater Family history of OSA Smoking Excessive alcohol use Ethnic origin: African American, Hispanic Small oralpharynx
Risks
Definition
• A condition of frequent episodes breathing pauses.
• Pauses due to sleep induced complete or partial airway collapse.
• Often results in O2 desaturation.
OSA Deprives Organs of Oxygen
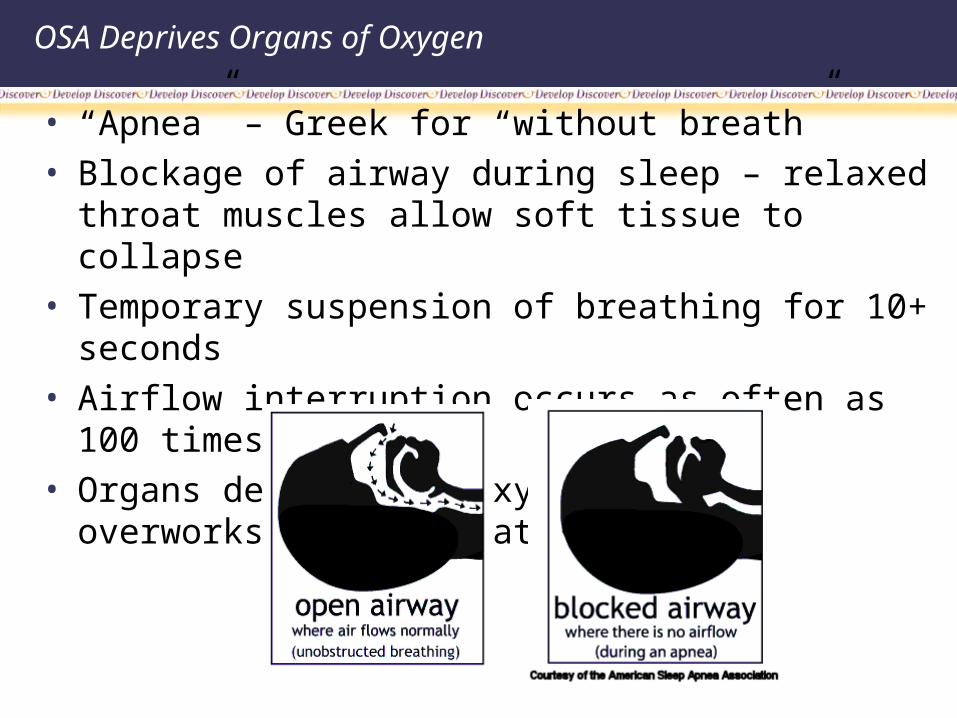
• “Apnea” – Greek for “without breath”
• Blockage of airway during sleep – relaxed throat muscles allow soft tissue to collapse
• Temporary suspension of breathing for 10+ seconds
• Airflow interruption occurs as often as 100 times/night
• Organs deprived of oxygen – heart overworks to compensate
Common Signs of Sleep Apnea
• Loud or disruptive snoring• Gasping or choking during sleep• Restless sleep• Loss of energy• Excessive daytime sleepiness• Morning headaches• Dry or sore throat• Depression, irritability or difficulty concentrating• High blood pressure• Weight gain• ADHD in children/behavioral problems /poor grades
OSA Increases Co-Morbid Health Risks
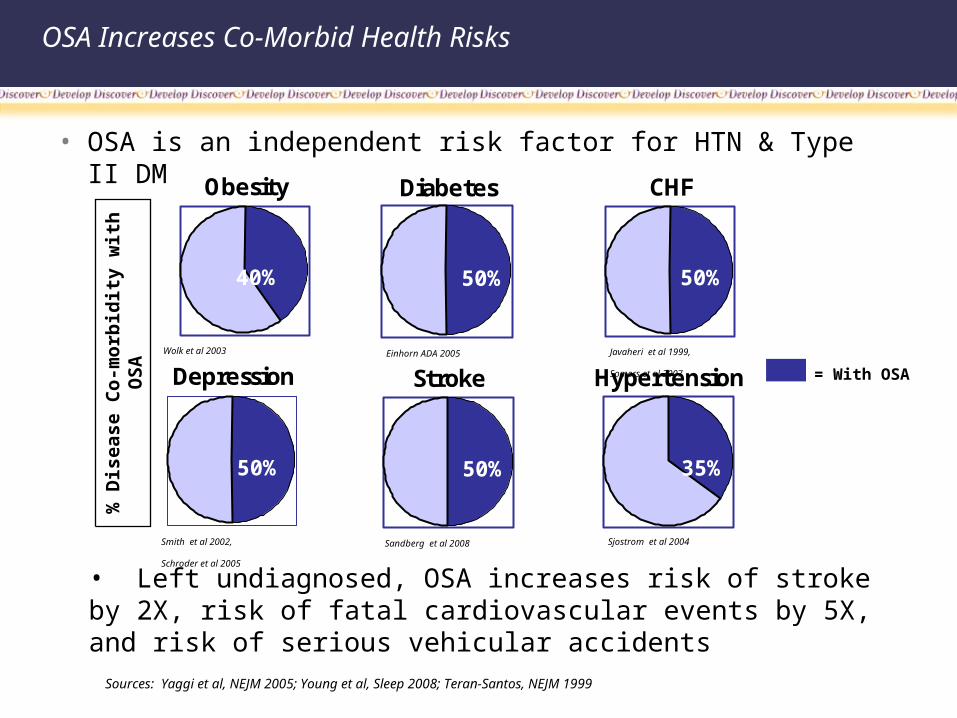
• OSA is an independent risk factor for HTN & Type II DM
Obesity
Depression
40%
Diabetes
50%
CHF
50%
50%
Stroke
50%
Hypertension
35%
Wolk et al 2003 Javaheri et al 1999,
Somers et al 2007
Einhorn ADA 2005
Sjostrom et al 2004Sandberg et al 2008Smith et al 2002,
Schroder et al 2005
• Left undiagnosed, OSA increases risk of stroke by 2X, risk of fatal cardiovascular events by 5X, and risk of serious vehicular accidents
% D
isease C
o-m
orb
idit
y w
ith
O
SA
= With OSA
Sources: Yaggi et al, NEJM 2005; Young et al, Sleep 2008; Teran-Santos, NEJM 1999
Pathophysiology
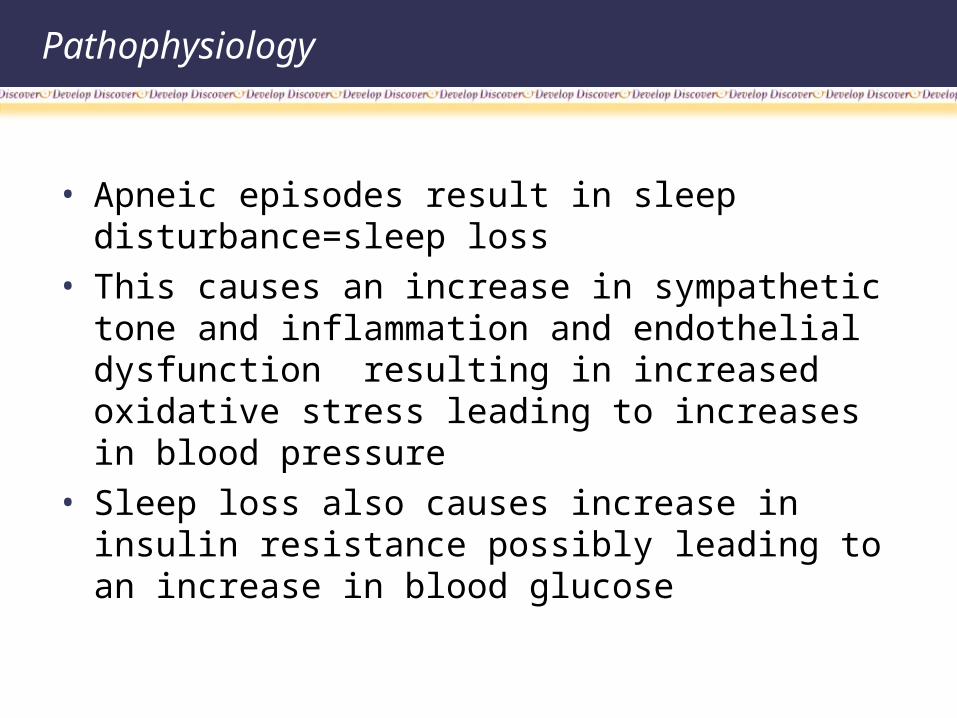
• Apneic episodes result in sleep disturbance=sleep loss
• This causes an increase in sympathetic tone and inflammation and endothelial dysfunction resulting in increased oxidative stress leading to increases in blood pressure
• Sleep loss also causes increase in insulin resistance possibly leading to an increase in blood glucose
Pathophysiology
OSA Impacts QOL and Cost of Care
• Aggravates / causes - Gastroesophageal reflux GERD
- Obesity (cortisol release from apnea events)
- Headaches
- Frequent urination
- Erectile dysfunction
- Cardiac arrhythmias
- Cognitive impairment
• In aggregate, these generate significant medical expense
Excessive Fatigue Can Lead to Poor Performance
WORK
MOTOR VEHICLE
OPERATION
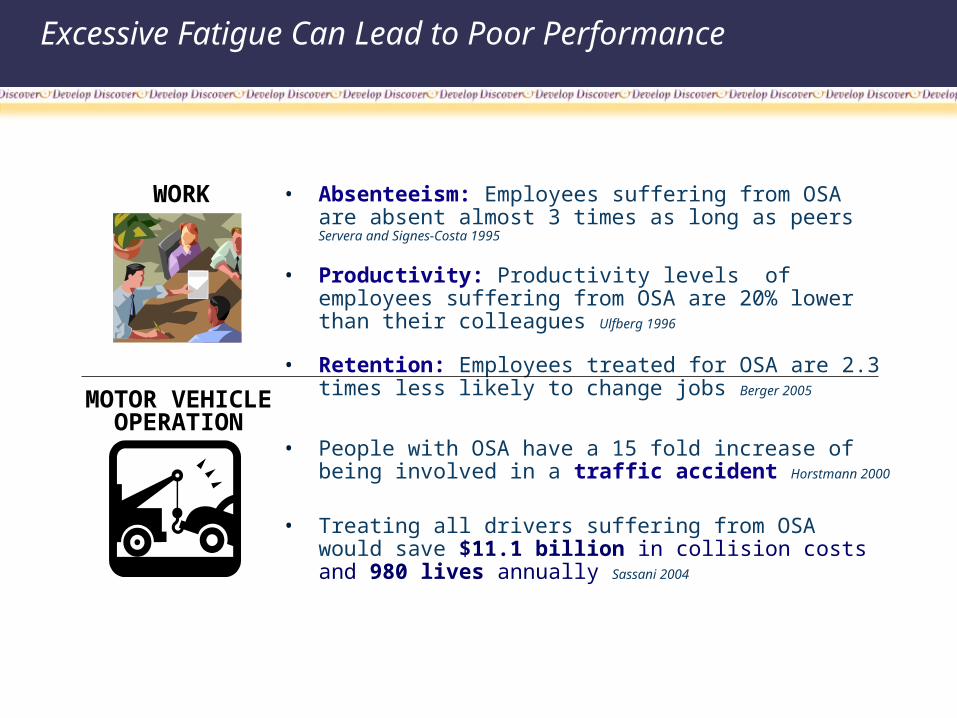
• Absenteeism: Employees suffering from OSA are absent almost 3 times as long as peers Servera and Signes-Costa 1995
• Productivity: Productivity levels of employees suffering from OSA are 20% lower than their colleagues Ulfberg 1996
• Retention: Employees treated for OSA are 2.3 times less likely to change jobs Berger 2005
• People with OSA have a 15 fold increase of being involved in a traffic accident Horstmann 2000
• Treating all drivers suffering from OSA would save $11.1 billion in collision costs and 980 lives annually Sassani 2004
Primary Care Physicians: “Front Line” for OSA Management
SSI focuses on training PCPs to diagnose & treat OSA, because most co-morbid at-risk patients are already in their care.
• 37.5% of patients in PCP practices have signs of sleep disorder and should be screened for OSA risk assessment Netzer 1999
• At diagnosis, avg. OSA patient has been symptomatic for ~7 years
– Has seen FP ~17 times & sub-specialist ~9 times Rahaghi 1999
“Knowing what we know about OSA and how it affects health & quality of life, it is imperative that as PCPs on the front line, the diagnosis of OSA is not missed and is appropriately treated.”*
“We have to think of this as a lifelong illness…we will be managing it in a new way…it requires primary care involvement – it cannot be managed by specialists alone.” * Kingman P. Strohl, MD (IM /Pulmonologist)
Professor of Medicine, Director of Center for Sleep Education & Research, Case Western Reserve School of Medicine
Amit Khanna, MD, DABSM, DABFM Medical Director of Charles Cole Mem. Hospital Sleep Disorder Center
* From Understanding the Diagnosis & Treatment of OSA, 2009, Temple University School of Medicine, CME Course

Diagnosis
• Who should be screened?
• How are patients screened ?
• Physical exam
• Those with snoring with:• 1) daytime drowsiness &/or• 2) short term memory loss• 3) AM headache• 4) depression /mood alterations• 5) nocturia• 6) GERD, DM, CHF, IHD. RESISTANT HTN!!!
Diagnosis
• Two tests are available• 1) Epworth sleepiness scale (see handout) score
>10 suggestive of sleep apnea-Used to evaluate subjective sleepiness but not as effective as:
• 2)Berlin scale- has sensitivity of 88% with a specificity of 77%
• Three categories:• 1)snoring/stop breathing (pos if any one is pos)• 2)fatigue after sleep /falling asleep while
driving/fatigue after sleep /falling asleep during wakeful hours unintentionally (pos if any one is pos)
Diagnosis
• 3)resistant HTN/BMI>30 • If any 2 categories are pos then patient is at high
risk for having OSA
• PE• Measure BMI with vitals• Evaluation of upper airway (elongated
uvula/enlarged tonsils/low soft palate etc. • Measure neck size• Cardiopulmonary evaluation
Diagnosis
• Two types of lab evaluations• 1) PSG-polysomography single night testing• 2) HST-home sleep testing multi-night testing
• Both measure;• 1) O2 desaturation• 2) chest wall movement• 3) apnea/ hypopneas• 4) heart activity• 5) air flow• 6 ) snoring
PSG vs. HST
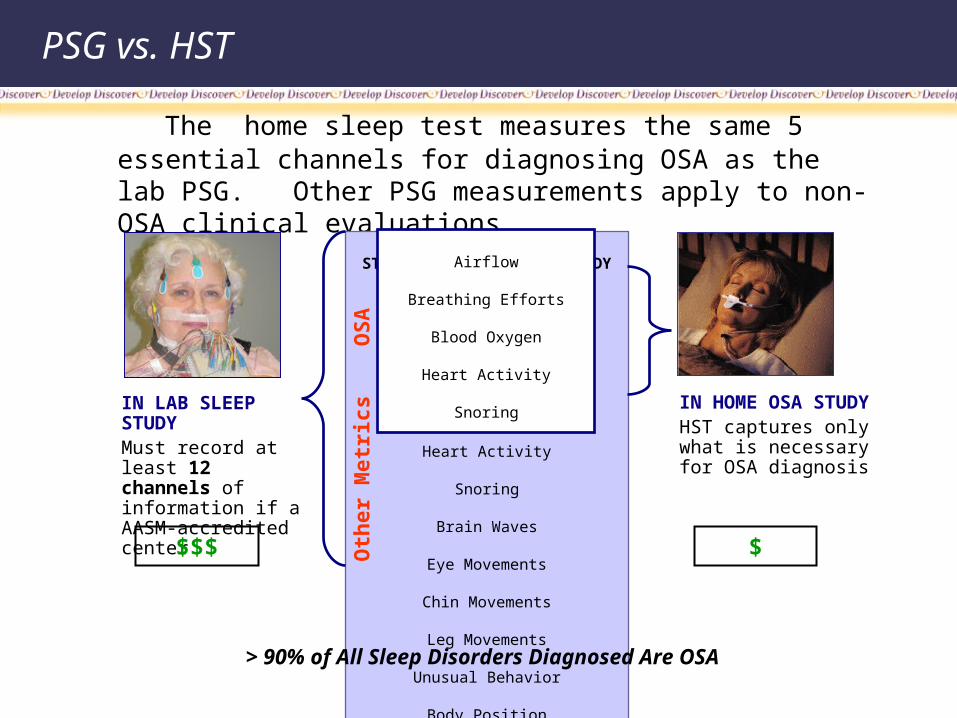
The home sleep test measures the same 5 essential channels for diagnosing OSA as the lab PSG. Other PSG measurements apply to non-OSA clinical evaluations.
STANDARD IN LAB SLEEP
STUDY
Airflow
Breathing Efforts
Blood Oxygen
Heart Activity
Snoring
Brain Waves
Eye Movements
Chin Movements
Leg Movements
Unusual Behavior
Body Position
Sleep Architecture
IN LAB SLEEP STUDYMust record at least 12 channels of information if a AASM-accredited center
IN HOME OSA STUDYHST captures only what is necessary for OSA diagnosis
Airflow
Breathing Efforts
Blood Oxygen
Heart Activity
Snoring
$$$ $
OS
AO
ther
Met
rics
> 90% of All Sleep Disorders Diagnosed Are OSA
Diagnosis
The diagnosis of sleep apnea is made if the AHI is >15
OR >5 with PMH of HTN/ stroke/ daytime sleepiness/ Insomnia/ IHD mood disorders
AHI=apneas+hypopneas/1hr must be at least 10 sec long and associated with 4% desaturation
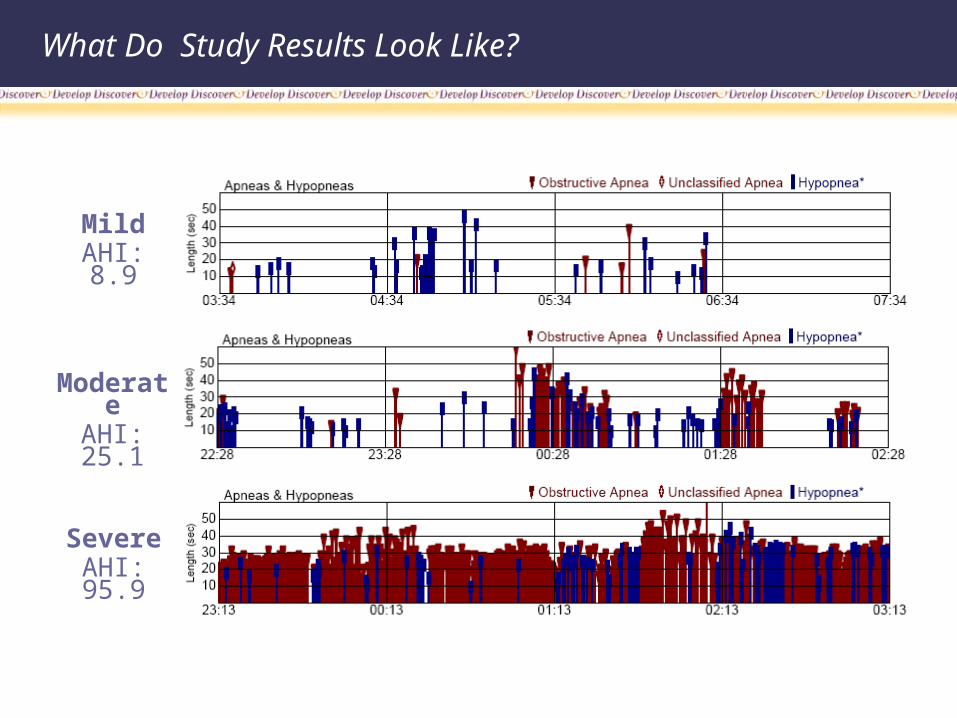
What Do Study Results Look Like?
MildAHI: 8.9
Moderate
AHI: 25.1
SevereAHI: 95.9
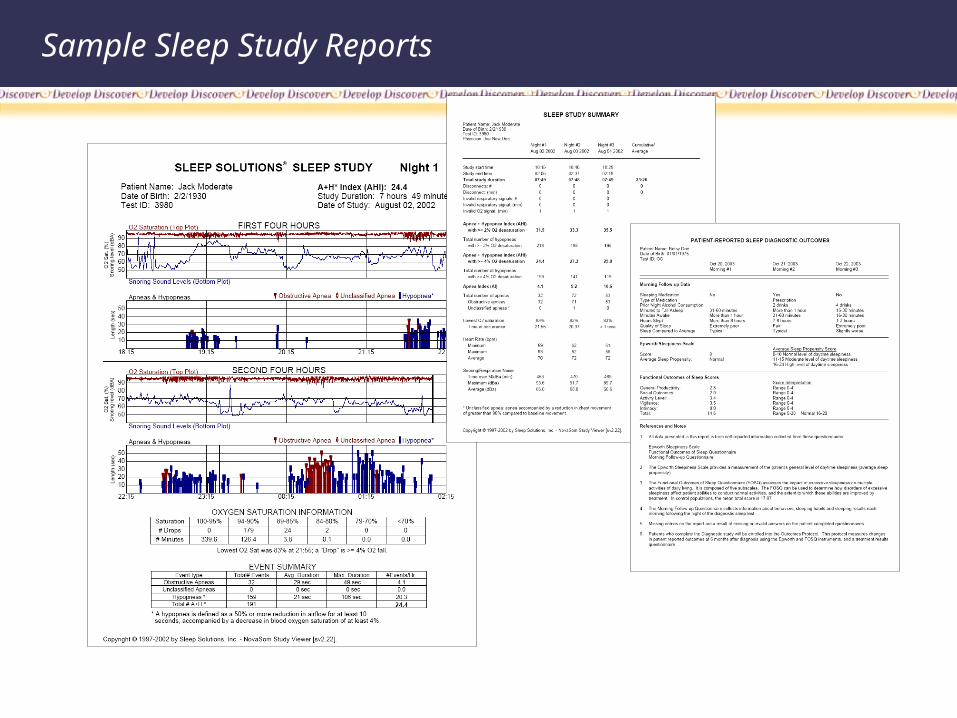
Sample Sleep Study Reports
Limitations of PSG Lab Tests
Sleep labs were designed to perform comprehensive measurement tasks, but not to be efficient at OSA diagnosis:
• Cost - $2,000-3,000 test – 3 to 4 times the cost of portable test
• Decreased accessibility
• Patient refusal to go to sleep lab for testing
• Completion rates – walk-outs, “1st night” effect (false negatives)
• Inability to sleep in lab
Limitations of HST
• Inadequate number of clinical trials
• Best data in mild OSA patients with PSG
• Does not avoid need for sleep lab
• Can’t do split testing ie. Dx 1st four hours/CPAP titration last four hours
Treatment
• Who should we treat?• How should we treat?
• Treat all patients with an AHI>30 with CPAP, BIPAP, APAP, or UPPP (if above not tolerated /effective)
• All patients with AHI>5<30 with symptoms/with symptoms/ co-morbid conditions.
• Dental devices in those with mild OSA ie., those with symptoms with AHI>5 who are intolerant of CPAP etc.
OSA Can Be Easily Treated
• Patients feel better and most health costs decrease with CPAP treatment
… so why is OSA under diagnosed today?
• Heart Health: One month of CPAP improves daytime blood pressure, heart rate and left ventricular function Kaneko 2003
• Stroke and CHF: With CPAP treatment, stroke risk is reduced 35% and CHF is reduced 20% Becker 2003
• Diabetes: After-meal blood glucose levels can be reduced with compliant CPAP therapy Babu 2005
• Hypertension: Effective OSA therapy has been associated with a 10mm Hg fall in blood pressure Harsch 2004
The Tipping Point: CMS Approval of HST
Recent evaluations by Medicare, AHRQ, AASM & AAO have validated the vital role of HST in OSA diagnosis:
• AHRQ comprehensive clinical literature review August 2007
• New AASM Guidelines issued December 2007
• CMS coverage determination – CPAP with HST March 2008
• AAO-HNS statement applauding CMS decision March 2008
Patients Now Have a Choice in Sleep Diagnosis and Treatment
“This is a great victory for patients who may suffer from OSA and the numerous medical issues caused by sleep apnea,”
said Academy spokesman Eric Mair, MD, who testified before CMS in support of changing the national coverage
determination. “Because home testing will now be an option, scores of patients who may have otherwise gone
undiagnosed will be able to seek the best treatment for OSA, and hopefully see an improvement in their quality of
life. With this change, CMS has taken a bold step forward to overcome the limitations of the current system and
ensure patients nationwide have access to the best care available.”
Questions?
_ _ _ _ _ _ _
References
Somers V, et al circulation 2003 107:2589=94
Flemons WW. N England J Med.2002 :347(7):498-504
Young T. et al. Arch Int Med. 2002;162:893—36
Punjabi N et al AM J Epidemiology 2004;160(6):521-30
Logan AG J HTN,2001;19:2271-7
Levie P, et al Eur Respir J. 2005;25:514-20
Institutes of Medicine Sleep disorders and sleep deprivation: an unmet public health problem
American Academy of Sleep Medicine. Sleep Apnea Fact Sheet 2008