Embed Size (px)
Citation preview
Current Issues in Drug Therapies: Issues of Safety and Efficacy in
Geriatric Prescribing Margaret Fitzgerald,
DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCCPresident, Fitzgerald Health Education Associates, Inc.
North Andover, MAFamily Nurse Practitioner,
Greater Lawrence (MA) Family Health CenterEditorial Board Member
The Nurse Practitioner Journal, Prescriber’s Letter, American Nurse Today
Member, Pharmacy and Therapeutics CommitteeNeighborhood Health Plan, Boston, MA
© Fitzgerald Health Education Associates, Inc. 1
Objectives
• Having completed the learning activities, the participant will be able to:– Identify the effects of aging and
disease state on pharmacokineticsand pharmacodynamics.
– Recognize safety issues with the use of select medications in the elderly.
© Fitzgerald Health Education Associates, Inc. 2
Prescribing in the Older Adult
• When compared to the younger adult, what is different in the elder? – PD (pharmacodynamics)– PK (pharmacokinetics)– Both? – Neither?
© Fitzgerald Health Education Associates, Inc. 3
General Pharm Rule in Prescribing for the Elder: Consider normative age-related changes and subsequent impact on drug choice and dose.
© Fitzgerald Health Education Associates, Inc. 4
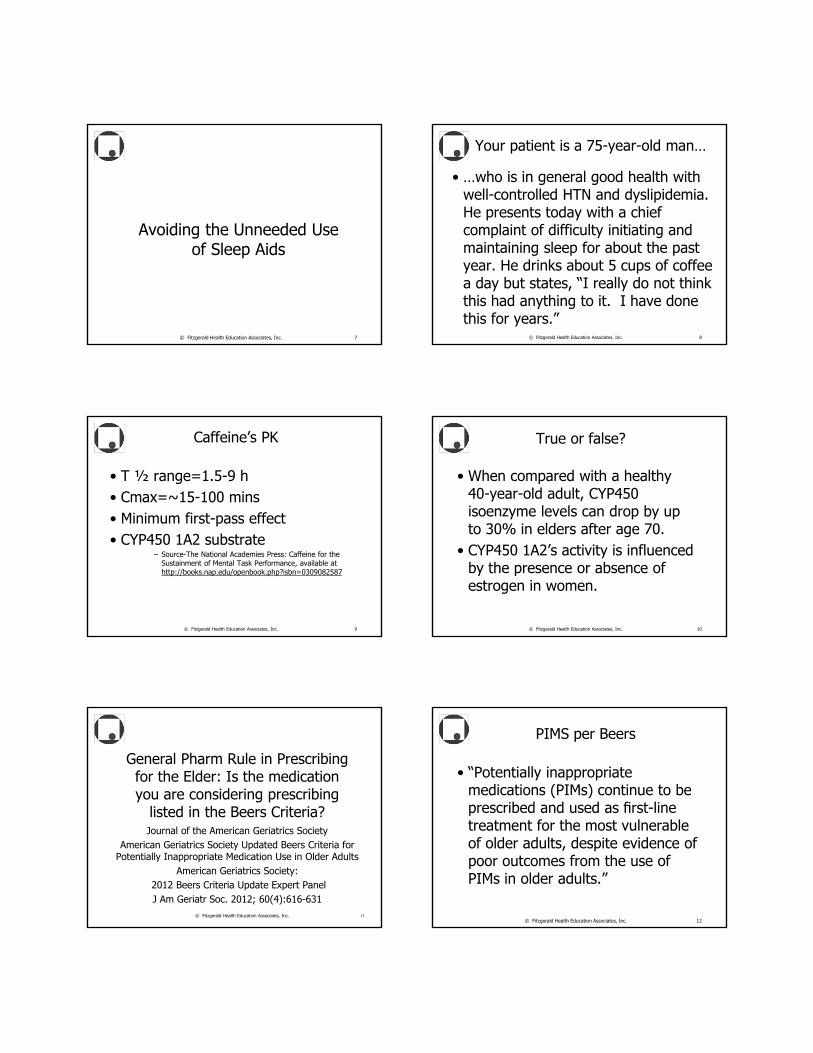
Source- Katzung, BG. (2011) Basic and Clinical Pharmacology (12th ed.) New York: Lange Medical Books/ McGraw-Hill.
Summary of Age-related Changes
© Fitzgerald Health Education Associates, Inc. 5
Adults age 20-30 y Adult age 60-80 y
% body weight as water 60% 53%
Lean muscle mass Baseline =>20% reduction
% body weight as fat26-33% (women)
18-20% (men)
38-45% (women)
36-38% (men)
Serum albumin (average) 4.7 g/dL (47 g/L)
3.8 g/dL (38 g/L)
Relative kidney weight 100% 80%
Relative hepatic blood flow 100% 55-60%
Singla and Morrill:Warfarin Maintenance
Dosages in the Very Elderly• The mean daily warfarin dose was
significantly lower with increasing age; the mean ± S.D. daily dose for patients younger than 75 years was 4.9 ± 2.6 mg/day, while that for patients 85 years or older was 3.5 ± 2.6 mg/day. – Source- http://www.ajhp.org/content/62/10/1062.abstract
© Fitzgerald Health Education Associates, Inc. 6
Avoiding the Unneeded Use of Sleep Aids
© Fitzgerald Health Education Associates, Inc. 7
Your patient is a 75-year-old man…
• …who is in general good health with well-controlled HTN and dyslipidemia. He presents today with a chief complaint of difficulty initiating and maintaining sleep for about the past year. He drinks about 5 cups of coffee a day but states, “I really do not think this had anything to it. I have done this for years.”
© Fitzgerald Health Education Associates, Inc. 8
Caffeine’s PK
• T ½ range=1.5-9 h• Cmax=~15-100 mins• Minimum first-pass effect• CYP450 1A2 substrate
– Source-The National Academies Press: Caffeine for the Sustainment of Mental Task Performance, available at http://books.nap.edu/openbook.php?isbn=0309082587
© Fitzgerald Health Education Associates, Inc. 9
True or false?
• When compared with a healthy 40-year-old adult, CYP450 isoenzyme levels can drop by up to 30% in elders after age 70.
• CYP450 1A2’s activity is influenced by the presence or absence of estrogen in women.
© Fitzgerald Health Education Associates, Inc. 10
General Pharm Rule in Prescribing for the Elder: Is the medication you are considering prescribing
listed in the Beers Criteria? Journal of the American Geriatrics Society
American Geriatrics Society Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults
American Geriatrics Society:2012 Beers Criteria Update Expert PanelJ Am Geriatr Soc. 2012; 60(4):616-631
© Fitzgerald Health Education Associates, Inc. 11
PIMS per Beers
• “Potentially inappropriate medications (PIMs) continue to be prescribed and used as first-line treatment for the most vulnerable of older adults, despite evidence of poor outcomes from the use of PIMs in older adults.”
© Fitzgerald Health Education Associates, Inc. 12
Avoid medications with systemic anticholinergic effect due to risk of
confusion, urinary retention, constipation, visual disturbance, and hypotension.
The adverse effectscould lead to polypharmacy
and risk of delirium.
© Fitzgerald Health Education Associates, Inc. 13
Medications with Significant Anticholinergic Effects
• 1st generation antihistamines– Chlorpheniramine (Chlor-Trimeton®)– Diphenhydramine (Benadryl®)– Hydroxyzine (Atarax®)– Cyproheptadine (Periactin®)– Promethazine (Phenergan®)
© Fitzgerald Health Education Associates, Inc. 14
First Generation Antihistamines
• Additional comments from Beers Criteria– Clearance reduced with advanced age– Tolerance develops when these
products used as hypnotic
© Fitzgerald Health Education Associates, Inc. 15
Commonly Used Meds in Elder with Anticholinergic Effect
• Examples– Oxybutynin (Ditropan®) immediate
release vs sustained release• SR form=Better tolerance with similar
therapeutic efficacy
• Examples– Amitriptyline vs. nortriptyline
© Fitzgerald Health Education Associates, Inc. 16
Oxybutynin in a Sustained Release Patch Form
• Oxytrol for women• Above=Full branded name for this
indication
– Indication=OAB– Identical dose as the Rx formulation– Labeling restricted to women due to
licensing• Safety, efficacy data presented to
FDA=Limited to women Fitzgerald Health Education Associates, Inc. 17
Avoid using medications where there is little evidence of benefit
but evidence of risk.
© Fitzgerald Health Education Associates, Inc. 18
Antiarrhythmic Drugs (Class Ia, Ic, III) Per Beers Criteria
• “Avoid antiarrhythmic drugs as first-line treatment of atrial fibrillation.”
© Fitzgerald Health Education Associates, Inc. 19
Antiarrhythmic Drugs (Class Ia, Ic, III) Per Beers Criteria
(continued)
• “Data suggest that rate control yields better balance of benefits and harms than rhythm control for most older adults.”
© Fitzgerald Health Education Associates, Inc. 20
Antiarrhythmic Drugs (Class Ia, Ic, III)
• Examples– Amiodarone– Dronedarone– Flecainide– Procainamide– Propafenone– Quinidine– Sotalol
© Fitzgerald Health Education Associates, Inc. 21
Antiarrhythmic Drugs (Class Ia,Ic,III) per Beers Criteria
(continued) • “Amiodarone use is associated with
multiple toxicities, including thyroid disease, pulmonary disorders, and QT interval prolongation.”
© Fitzgerald Health Education Associates, Inc. 22
In an older woman with recurrent UTI, consider alternative other
than chronic antimicrobial therapy.
© Fitzgerald Health Education Associates, Inc. 23
Estrogens with or without Progestins per Beers Criteria
• “Topical vaginal cream: Acceptable to use low-dose intravaginal estrogen for the management of dyspareunia, lower urinary tract infections, and other vaginal symptoms.”
© Fitzgerald Health Education Associates, Inc. 24
Per Beers Criteria: True or false?
• There is evidence that vaginal estrogens for treatment of vaginal dryness is safe and effective in women with breast cancer, especially at dosages of estradiol dose <25 mcg twice weekly.
© Fitzgerald Health Education Associates, Inc. 25
In this era of “treat to goal,” be aware the age-related variations
in therapeutic target.
© Fitzgerald Health Education Associates, Inc. 26
AACE Medical Guidelines for Clinical Practice for Developing a Diabetes
Comprehensive Care Plan
• For older adults who are frail or with anticipated life expectancy of <=5 years, A1C goal should be <=8% (0.08 proportion), as the risks of hypoglycemia outweigh the benefits of stringent glycemic control.
– Source- https://www.aace.com/files/dm-guidelines-ccp.pdf
© Fitzgerald Health Education Associates, Inc. 27
According to Up To Date
• All patients with diabetes mellitus have a goal blood pressure <140/90 mmHg.– ACCORD=3.4 meds for tight BP control vs
2.1 meds for less strict
• We suggest (weaker recommendation) an attempt to lower the systolic pressure below 130 to 135 mmHg (preferably less than 130 mmHg) if it can be achieved without producing significant side effects.
© Fitzgerald Health Education Associates, Inc. 28
According to Up To Date (continued)
• We recommend a goal blood pressure of less than 130/80 mmHg in patients with diabetic nephropathy and proteinuria (=>500 mg/day). Patients with microalbuminuria are treated similarly to diabetic patients without proteinuria.
© Fitzgerald Health Education Associates, Inc. 29
Hypertension in the Elderly
ACCF/AHAExpert Consensus Document
Available at http://content.onlinejacc.org/cgi/content/full/j.jacc.
2011.01.008Developed in collaboration with the American Academy of Neurology, Association of Black Cardiologists, American Geriatrics Society, American Society of Hypertension, American Society of Nephrology, American Society for Preventive Cardiology, and the European Society of Hypertension
30© Fitzgerald Health Education Associates, Inc.
Target Blood PressureGoals in the Elderly
• Although the optimal BP treatment goal in the elderly has not been determined, a therapeutic target of <140/90 mmHg in persons aged 65-79 years and a SBP of 140-145 mmHg, if tolerated, in persons aged≥80 years is reasonable.
© Fitzgerald Health Education Associates, Inc.31
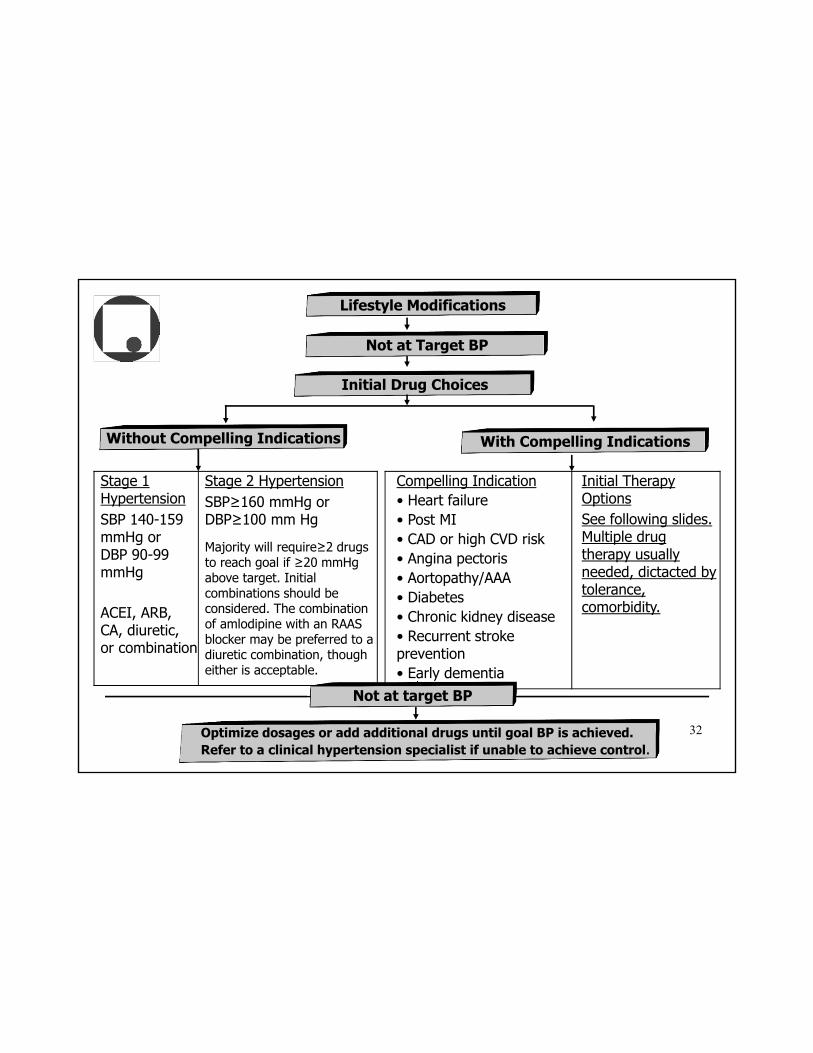
Stage 1 HypertensionSBP 140-159 mmHg or DBP 90-99 mmHg
ACEI, ARB, CA, diuretic, or combination
Stage 2 HypertensionSBP≥160 mmHg or DBP≥100 mm Hg
Majority will require≥2 drugs to reach goal if ≥20 mmHg above target. Initial combinations should be considered. The combination of amlodipine with an RAAS blocker may be preferred to a diuretic combination, though either is acceptable.
Compelling Indication• Heart failure• Post MI• CAD or high CVD risk• Angina pectoris• Aortopathy/AAA• Diabetes• Chronic kidney disease• Recurrent stroke prevention • Early dementia
Initial Therapy OptionsSee following slides. Multiple drug therapy usually needed, dictacted by tolerance, comorbidity.
Optimize dosages or add additional drugs until goal BP is achieved. Refer to a clinical hypertension specialist if unable to achieve control.
Not at target BP
Lifestyle Modifications
Initial Drug Choices
Not at Target BP
With Compelling IndicationsWithout Compelling Indications
32
Information in the following slides outline differences in
recommendations or conditions not mentioned in JNC-7.
© Fitzgerald Health Education Associates, Inc. 33
• Aortopathy/aortic aneurysm– Thiazide diuretic,
beta blocker, ACEI, CCB
© Fitzgerald Health Education Associates, Inc. 34
Compelling Indications for Use of Select Meds in Elder w/HTN
• Recurrent stroke prevention– Thiazide diuretic,
ACEI, ARB, CCB
© Fitzgerald Health Education Associates, Inc. 35
Compelling Indications for Use of Select Meds in Elder w/HTN
(continued)
General Pharm Rule in Prescribing for the Elder: While PD does not change with aging, some age-related physical changes will result in less drug effect.
© Fitzgerald Health Education Associates, Inc. 36

Age-related Changes Influencing Pharmacodynamics
• Age-related changes in vascular, pulmonary, cardiac tissue– Decrease in effect of beta-adrenergic
agents• Beta2-agonists such as albuterol,
salmeterol• Beta antagonists such as metoprolol,
carvedilol
© Fitzgerald Health Education Associates, Inc. 37
Additional Therapeutic Choices with Less Age-related Impact
• Inhaled anticholinergic – Tiotropium, ipratropium bromide
• Calcium channel blockers– Dihydropyridines (DHP) such as
amlodipine– Non DPH such as verapamil, diltiazem
• Some evidence of increased sensitivity to Non-DPH PR-prolonging effects in elder
© Fitzgerald Health Education Associates, Inc. 38
Discontinue medications that likely should not have been started in the first place.
© Fitzgerald Health Education Associates, Inc. 39
PPI Use: Third Leading Drug Class in Sales
Risks vs. Benefits References-
Proton Pump Inhibitors: Appropriate use and safety concerns. Pharmacist’s Letter/Prescriber’s
Letter 2010 (Updated March 2011); 26(7):260705.
© Fitzgerald Health Education Associates, Inc. 40
Consequences ofLong-term PPI Use
• Rebound hypersecretion– 60% to 90% using PPIs for =>2
months – Explains why reports increased GI
symptoms with discontinuation• Considering tapering medication with
reducing dose, followed by every other day use, H2RA, antacid use for symptoms
© Fitzgerald Health Education Associates, Inc. 41
Consequences ofLong-term PPI Use
(continued)
• Potential decrease in absorption of select micronutrients requiring acid stomach environment– Iron, vitamin B12 – Supplementation needs not established
© Fitzgerald Health Education Associates, Inc. 42
Consequences of Long-term PPI Use
(continued)
• Increased fracture risk in epidemiologic studies, noted in male and female– Associated with 25% increase in overall
fractures, 47% increase in spinal fractures in postmenopausal women
• Calcium citrate absorption less affected by altered gastric acidity
© Fitzgerald Health Education Associates, Inc. 43
Consequences ofLong-term PPI Use
(continued)
• Magnesium absorption– Increase risk hypomagnesaemia
noted with Mg depleting medication use such as thiazide and loop diuretics
– Digoxin toxicity risk increased with low Mg
© Fitzgerald Health Education Associates, Inc.44
PPI: CYP450 2C19 Inhibitors
• Lansoprazole– Prevacid®
• Omeprazole– Prilosec®
• Pantoprazole– Protonix®
• Rabeprazole– AcipHex®
• Esomeprazole– Nexium®
• Source-http://medicine.iupui.edu/clinpharm/ddis
• Click on Clinically Relevant Table for useful summary of CYP450 drug interactions.
© Fitzgerald Health Education Associates, Inc. 45
And perhaps DC a med that might have been the trigger to go on a PPI?
Source- http://www.uptodate.com/contents/bisphosphonates-in-the-management-of-osteoporosis-in-postmenopausal-
women?source=search_result&search=bisphosphonate+elderly&selectedTitle=1%7E150#H11271424
© Fitzgerald Health Education Associates, Inc. 46
Continuing Bisphosphonate Therapy
• For patients taking alendronate or risedronate for five years or who received zoledronic acid once yearly for three years, who have a stable BMD, no previous vertebral fractures, and who are at low risk for fracture in the near future, we suggest discontinuing the drug.
© Fitzgerald Health Education Associates, Inc. 47
Per Beers Criteria, Commonly Used Medication in Elder with Little
Evidence of Benefit
• Aspirin for primary prevention of cardiac events– Lack of evidence of benefit versus risk
in individuals aged≥80– Use with caution in adults aged≥80
© Fitzgerald Health Education Associates, Inc. 48
Avoid unneeded repeat therapy.
© Fitzgerald Health Education Associates, Inc. 49
72-year-old Woman with UTI and Mild Renal Insufficiency
• Sensitive– Nitrofurantoin– Ciprofloxacin
• Resistant– TMP-SMX– Ampicillin
© Fitzgerald Health Education Associates, Inc. 50
Urine culture results=100K colonies E. coliWhat is the best therapeutic option?
Antimicrobial Dose Adjustment in Renal Impairment: Nitrofurantoin
• If Cr Cl=>50 mg/dL (=>0.84 mL/s)– Standard dosing according to
indication
• If Cr Cl<50 mg/dL (<0.84 mL/s)– Avoid use
© Fitzgerald Health Education Associates, Inc. 51
Medications with Dose Adjustment Required in Renal Impairment
• Ciprofloxacin– Cr Cl=>30 mL per minute (0.5 mL/s):
No change with doses 250-750 mg BID
– Cr Cl<30 mL per minute (0.5 mL/s): Required dose q24h
© Fitzgerald Health Education Associates, Inc. 52
Medications with Dose Adjustment Required in Renal Impairment
(continued)
• TMP SMX (Bactrim®)– Cr Cl>30 ml/min (0.5 mL/s): No change,
1 DS tab BID– Cr Cl 15-30 ml/min (0.25-0.5 mL/s): 1
DS tablet 24h OR 1 SS tablet q12h– Cr Cl<15 ml/min (0.25 mL/s): Avoid if
possible or use 1 tablet SS or DS q24h
© Fitzgerald Health Education Associates, Inc. 53
True or false?
• In providing care for an older adult with mild renal impairment who is taking an ACEI with K+=5-5.5 mEq/L (5-5.5 mmol/L), aside from assuring adequate hydration, taking the once-daily ACEI dose in the morning should be considered so as to allow for overnight excretion of renal potassium to avoid hyperkalemia. – Source- Hou FF et al. Efficacy and Safety of Benazepril for Advanced Chronic
Renal Insufficiency. N Engl J Med 2006;354:131-40
© Fitzgerald Health Education Associates, Inc. 54
Medications Used in Alzheimer-type Dementia
• “Use of cholinesterase inhibitors is associated with increased rates of syncope, bradycardia, pacemaker insertion, and hip fracture in older adults with dementia. The risk of these previously under recognized serious adverse events must be weighed carefully against the drugs' generally modest benefits.”
– Source- Arch Intern Med. 2009;169:867-873.© Fitzgerald Health Education Associates, Inc. 55
And a Few Medications to Use with Caution in the Older Adult
© Fitzgerald Health Education Associates, Inc. 56
Azithromycin and the Risk of Cardiovascular Death
Wayne A. Ray, Ph.D., Katherine T. Murray, M.D., Kathi Hall, B.S., Patrick G. Arbogast, Ph.D., and C.
Michael Stein, M.B., Ch.B.N Engl J Med
Volume 366(20):1881-1890May 17, 2012
57 Fitzgerald Health Education Associates, Inc.
Background Information
• Azithromycin– Thought relatively free of cardiotoxic
effects noted with the other macrolides clarithromycin, erythromycin
– The FDA’s Adverse Event Reporting System includes at least 20 reports of torsades de pointes associated with azithromycin use.
Fitzgerald Health Education Associates, Inc. 58
Torsades de Ponte
Fitzgerald Health Education Associates, Inc. 59
Study Conclusion
• As compared with amoxicillin, there were 47 additional cardiovascular deaths per 1 million courses of azithromycin therapy. For patients in the highest decile of baseline risk of cardiovascular disease, there were 245 additional cardiovascular deaths per 1 million courses.
Fitzgerald Health Education Associates, Inc. 60
For Additional Information, http://www.qtdrugs.org
• True or false?– The risk of torsades
de pointe with erythromycin or clarithromycin is greater in females than in males.
Fitzgerald Health Education Associates, Inc. 61
Citalopram and QT Prolongation
• For all, not recommended above 40 mg/d– Causes too large
an effect on QT interval and confers no additional benefit
© Fitzgerald Health Education Associates, Inc. 62
Citalopram and QT Prolongation (continued)
• Use not recommended– With congenital long QT syndrome,
bradycardia, hypokalemia, or hypomagnesemia, recent acute MI, or uncompensated heart failure
– In patients who are taking other drugs that prolong the QT interval
© Fitzgerald Health Education Associates, Inc. 63
• Do not exceed 20 mg per day– Age>60 years, hepatic impairment,
CYP2C19 poor metabolizers, or patients who are taking concomitant cimetidine (Tagamet®) or another CYP2C19 inhibitor including many PPIs
© Fitzgerald Health Education Associates, Inc. 64
Citalopram and QT Prolongation (continued)
Citalopram and QT Prolongation (continued)
• In patients who are found to have persistent QTc measurements exceeding 500 ms, citalopram should be discontinued.
– Source-http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm297624.htm
© Fitzgerald Health Education Associates, Inc. 65
While polypharmacy is a concern, keep in mind underutilized vaccines.
© Fitzgerald Health Education Associates, Inc. 66
Per ACIP Adults with DM
• HBV vaccination be given to unvaccinated adults with diabetes mellitus who are ages 19 to 59.
• For older patients with diabetes, vaccination can be administered at clinician’s discretion based on the risk of acquiring HBV and likelihood of adequate immune response to vaccination.
© Fitzgerald Health Education Associates, Inc. 67
Why this recommendation?
• Outbreaks of HBV infection in patients with assisted blood glucose monitoring, particularly in LTC facilities– Viable HBV can be found on surfaces for
protracted periods even when blood not visible
– Also HBV note in insulin pen reservoirs, pen sharing not recommended
© Fitzgerald Health Education Associates, Inc. 68
General Pharm Rule in Prescribing for the Elder: Start low, go slow, but get to goal.
Do not put patient in situation of perhaps having some of the
adverse effects but none of the benefit of a give medication.
© Fitzgerald Health Education Associates, Inc. 69
End of PresentationThank you for your time and attention.
Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC
www.fhea.com, e-mail: [email protected]
70© Fitzgerald Health Education Associates, Inc.
References
• Katzung, BG. (2012) Basic and Clinical Pharmacology (12th ed.) New York: Lange Medical Books/McGraw-Hill.
• Stringer, J. (2011) Basic Concepts in Pharmacology: All you need to know for each drug class (4th edition). New York: McGraw-Hill.
71© Fitzgerald Health Education Associates, Inc.
Stage 1 HypertensionSBP 140-159 mmHg or DBP 90-99 mmHg
ACEI, ARB, CA, diuretic, or combination
Stage 2 HypertensionSBP≥160 mmHg or DBP≥100 mm Hg
Majority will require≥2 drugs to reach goal if ≥20 mmHg above target. Initial combinations should be considered. The combination of amlodipine with an RAAS blocker may be preferred to a diuretic combination, though either is acceptable.
Compelling Indication• Heart failure• Post MI• CAD or high CVD risk• Angina pectoris• Aortopathy/AAA• Diabetes• Chronic kidney disease• Recurrent stroke prevention • Early dementia
Initial Therapy OptionsSee following slides. Multiple drug therapy usually needed, dictacted by tolerance, comorbidity.
Optimize dosages or add additional drugs until goal BP is achieved. Refer to a clinical hypertension specialist if unable to achieve control.
Not at target BP
Lifestyle Modifications
Initial Drug Choices
Not at Target BP
With Compelling IndicationsWithout Compelling Indications
32






![Assessing drug synergy in combination therapies...Comprehensive [Drug A] [Drug B] Practical for pairs only. Most insightful data: Reveals drug interactions at all ratios between drugs](https://img.pdfslide.us/doc/110x75/612fa09d1ecc51586943922e/assessing-drug-synergy-in-combination-therapies-comprehensive-drug-a-drug.jpg)