Embed Size (px)
Citation preview
Psoriasis Therapies: Choosing the Correct Drug
Bruce Strober, MD, PhD
Professor and ChairDepartment of Dermatology
UConn Health CenterFarmington, CTJuly 30, 2017
DISCLOSURE OF RELEVANTRELATIONSHIPS WITH
INDUSTRY
Bruce Strober, MD, PhD
Consultant and Advisory Boards – AbbVie, Amgen, Astra Zeneca, Celgene, Dermira, Janssen, Leo, Eli Lilly, Cutanea-Maruho, Medac, Novartis, Pfizer,
Regeneron, Sanofi-Aventis, Sun Pharma, Boehringer Ingelheim, UCBInvestigator – AbbVie, Amgen, Boehringer Ingelheim, GlaxoSmithKline,
Novartis, Eli Lilly, Janssen, Merck, Sun Pharma, Celgene Scientific Director – CORRONA Psoriasis Registry
Grant Support to the University of Connecticut for Fellowship Program –AbbVie, Janssen
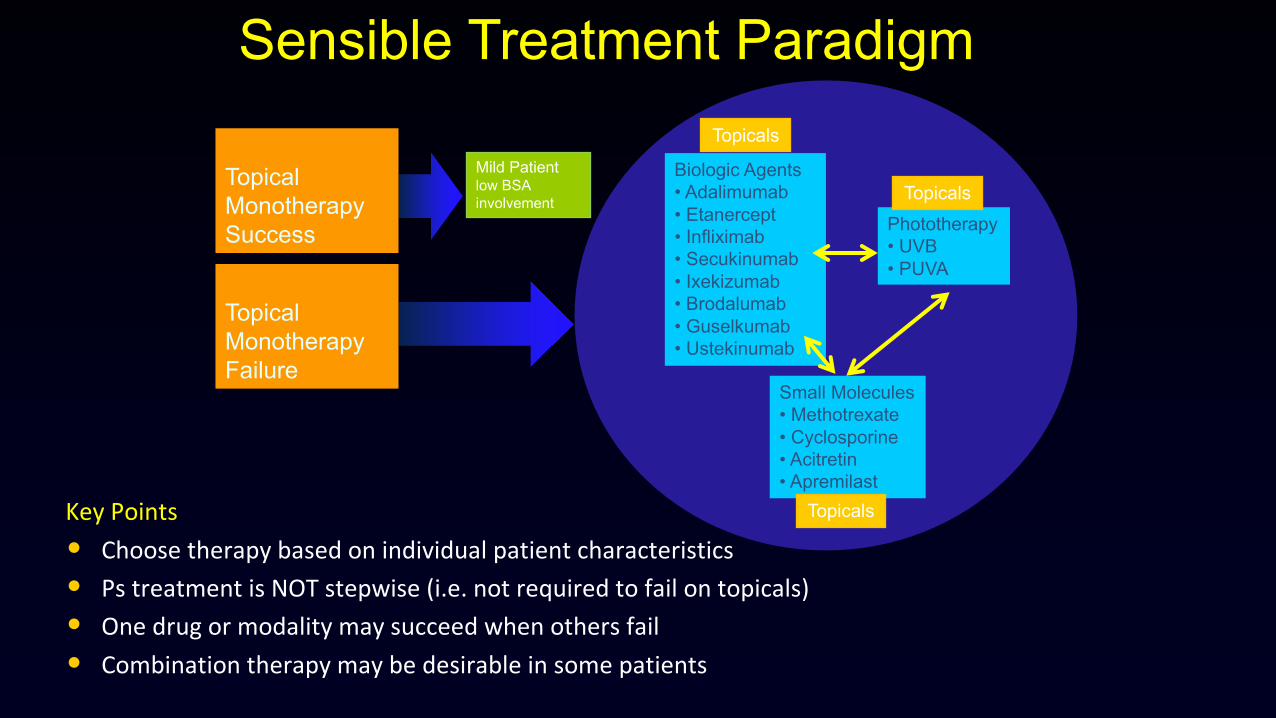
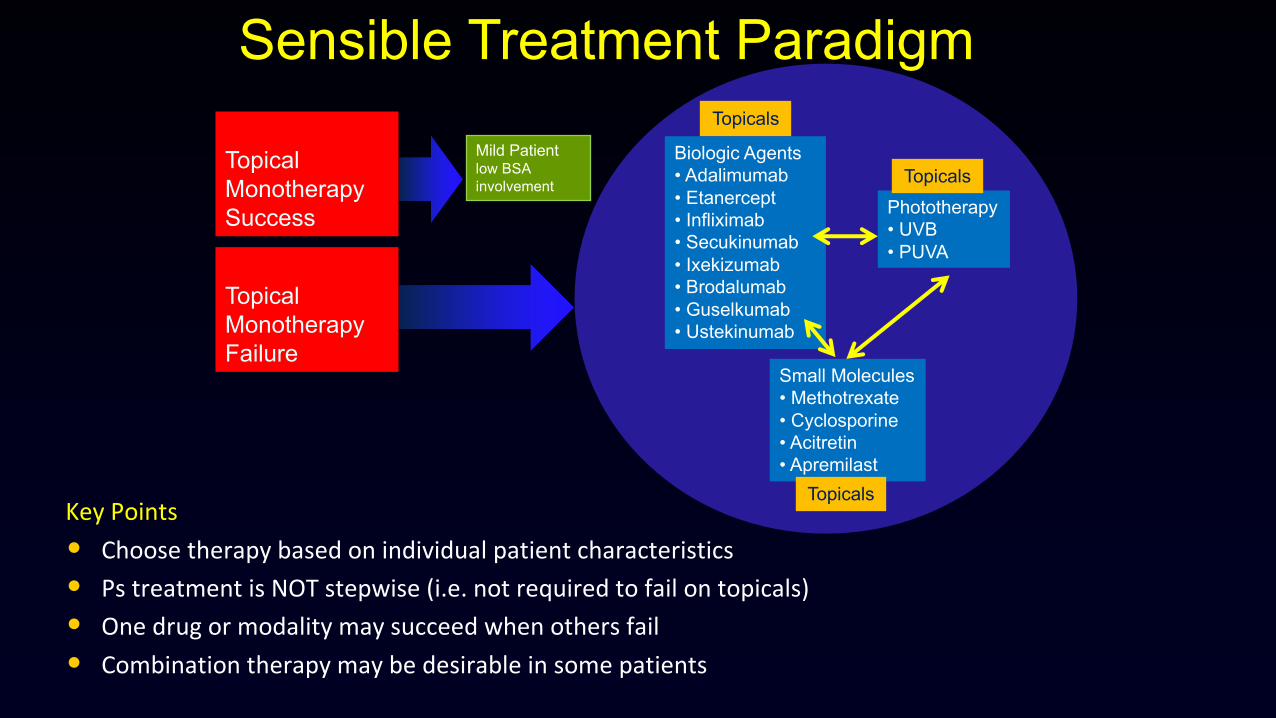
KeyPoints• Choosetherapybasedonindividualpatientcharacteristics• PstreatmentisNOTstepwise(i.e.notrequiredtofailontopicals)• Onedrugormodalitymaysucceedwhenothersfail• Combinationtherapymaybedesirableinsomepatients
TopicalMonotherapyFailure
Biologic Agents• Adalimumab• Etanercept• Infliximab• Secukinumab• Ixekizumab• Brodalumab• Guselkumab• Ustekinumab
Phototherapy• UVB• PUVA
Small Molecules• Methotrexate• Cyclosporine• Acitretin• Apremilast
Sensible Treatment Paradigm
Topicals
Topicals
Topicals
TopicalMonotherapySuccess
Mild Patient low BSA involvement

Baseline Week 12
PASI Score = 43.9 PASI Score = 0.4
Ultraviolet Phototherapy
• Effective and safe • No psoriatic arthritis• Practical for the patient
Why Do We Need to Know About Methotrexate and Cyclosporine?
• Effective and safe if used correctly• Cost-effective and FDA-approved for psoriasis• Not all patients can receive biologic therapy• Biologic therapies may fail as monotherapy, and
succeed in combination with traditional systemics• Rescue therapies in tough clinical scenarios
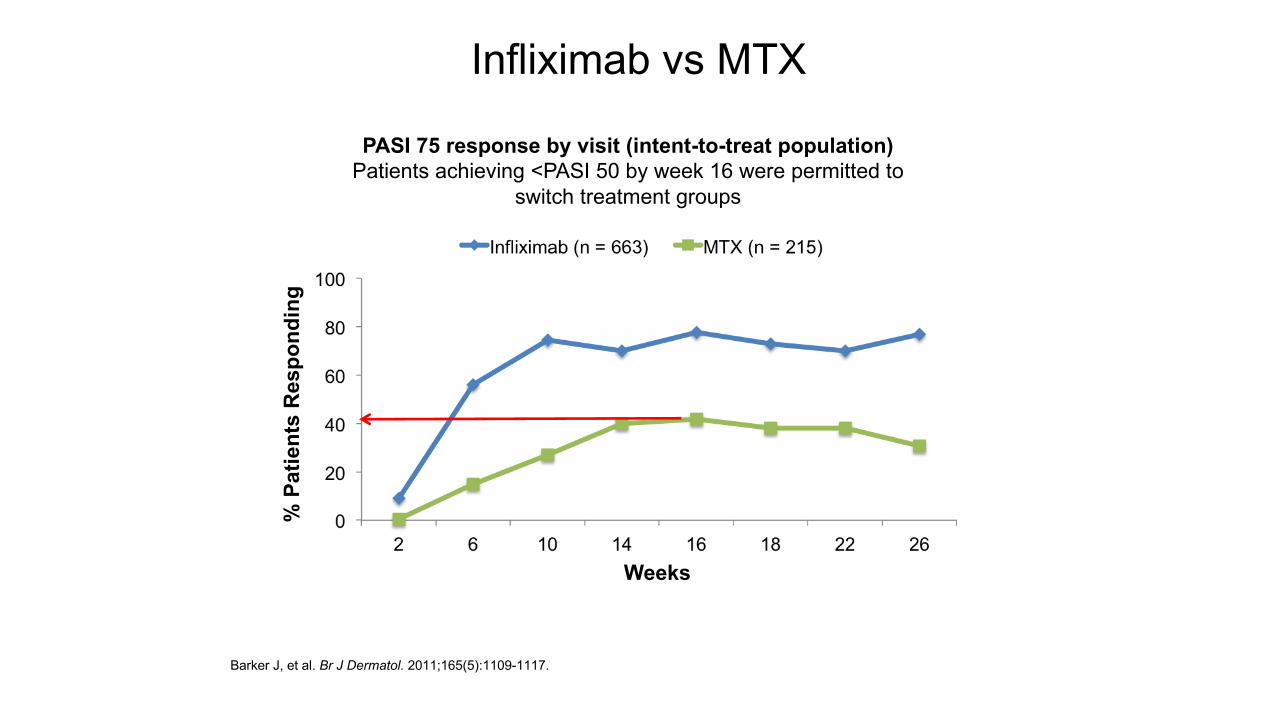
Infliximab vs MTX
Barker J, et al. Br J Dermatol. 2011;165(5):1109-1117.
PASI 75 response by visit (intent-to-treat population)Patients achieving <PASI 50 by week 16 were permitted to
switch treatment groups
% P
atie
nts
Res
pond
ing
Weeks
Methotrexate: When Do I Use It?
• Medicare patients• Lack of health insurance• Psoriatic arthritis• Pediatric psoriasis• Prior to a biologic therapy• Combined with a biologic therapy
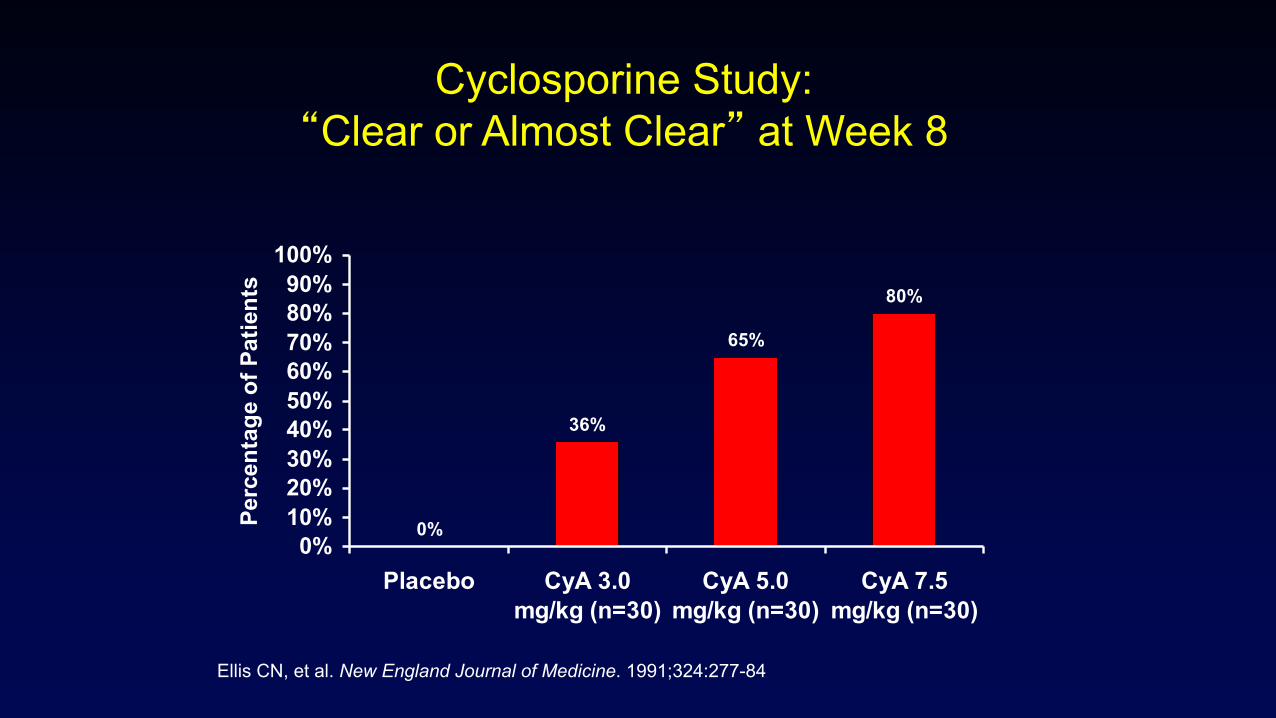
Ellis CN, et al. New England Journal of Medicine. 1991;324:277-84
Cyclosporine Study:“Clear or Almost Clear” at Week 8
0%
36%
65%
80%
0%10%20%30%40%50%60%70%80%90%
100%
Placebo CyA 3.0mg/kg (n=30)
CyA 5.0mg/kg (n=30)
CyA 7.5mg/kg (n=30)
Perc
enta
ge o
f Pat
ient
s
Cyclosporine: When Do I Use It?
• Severe patients in need of quick response• Pregnancy• Patients who fail other therapies• Prior to biologic therapies• Combined at lower doses with a biologic
therapy
EtanerceptTNF-α Blocker
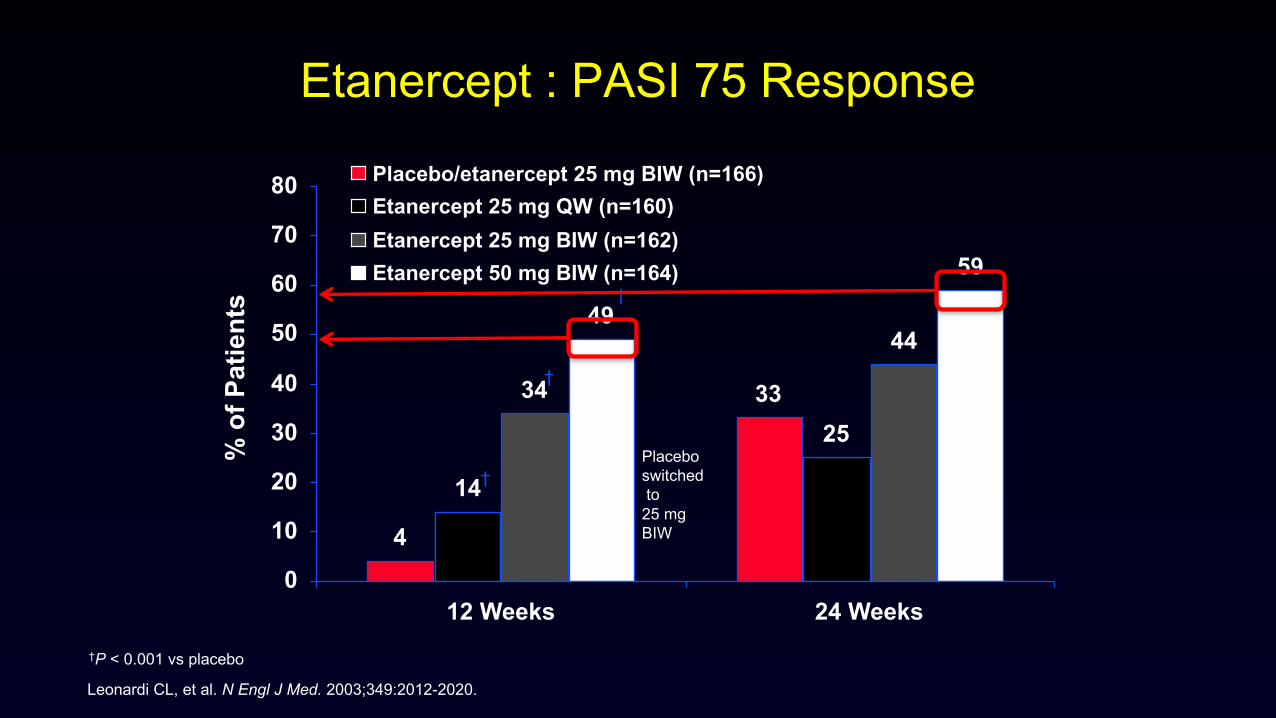
Etanercept : PASI 75 Response
†P < 0.001 vs placebo
Leonardi CL, et al. N Engl J Med. 2003;349:2012-2020.
4
33
14
25
34
4449
59
0
10
20
30
40
50
60
70
80
12 Weeks 24 Weeks
Placebo/etanercept 25 mg BIW (n=166)Etanercept 25 mg QW (n=160)Etanercept 25 mg BIW (n=162)Etanercept 50 mg BIW (n=164)
% o
f Pat
ient
s †
†
†Placebo switchedto
25 mg BIW
EtanerceptTNF-α Blocker
Pros• Well-tolerated and effective
(PI: PASI 75 45-54%)• Self-injectable; SC• Treats PsA• Pregnancy safe• Extensive post-marketing experience• Pediatric indication • No contraindication in IBD• May benefit patients with CV co-morbidity risks
EtanerceptTNF-α Blocker
Cons• Lowest Ps efficacy of the 3 approved TNF-α inhibitors• Step down dosing (50 mg BIW to 50 mg QW) results in loss of
response• Fixed dose loses response over time• Lower efficacy in heavier patients (>100 kg)• Slight risk of TB reactivation – test for latent/active TB required• Contraindicated in CHF, MS, active infection• Very rare lupus-like syndrome
EtanerceptTNF-α Blocker
Who gets this drug:• Any patient with moderate-to-severe psoriasis, though lower
efficacy moves it down list• 1st line drug
• Psoriatic arthritis• Pediatric (children and adolescents) à should be first biologic
chosen for this group• No personal history of MS or severe CHF

AdalimumabTNF-α Blocker
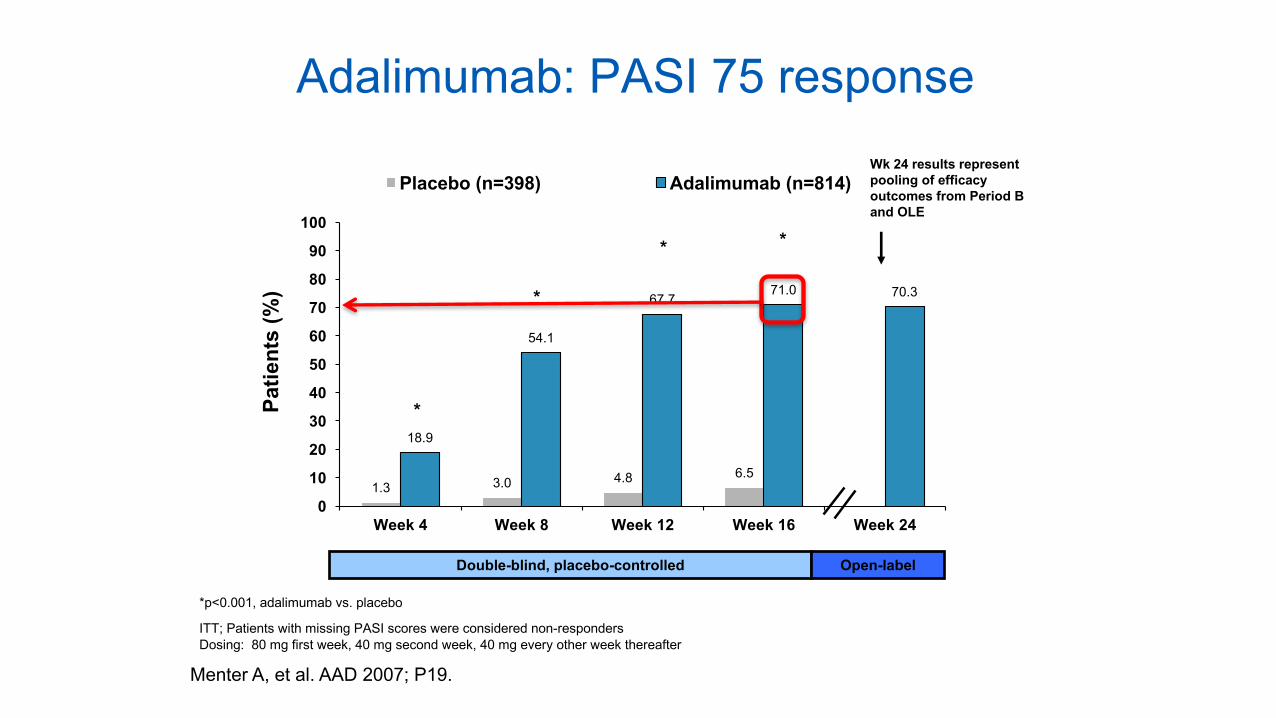
1.3 3.0 4.8 6.5
18.9
54.1
67.771.0 70.3
0
10
20
30
40
50
60
70
80
90
100
Week 4 Week 8 Week 12 Week 16 Week 24
Placebo (n=398) Adalimumab (n=814)
*
* *
*
Wk 24 results represent pooling of efficacy outcomes from Period B and OLE
*p<0.001, adalimumab vs. placebo
ITT; Patients with missing PASI scores were considered non-respondersDosing: 80 mg first week, 40 mg second week, 40 mg every other week thereafter
Menter A, et al. AAD 2007; P19.
Double-blind, placebo-controlled Open-label
Patie
nts
(%)
Adalimumab: PASI 75 response
AdalimumabTNF-α Blocker
Pros• Well-tolerated and highly effective SC; QOW; (PI: PASI 75 71%)• Treats PsA • Pregnancy safe• Extensive post-marketing experience• Pediatric indication for JIA (PI: > 4 years) and for psoriasis in
Europe• No contraindication in IBD• May benefit patients with CV co-morbidity risks
AdalimumabTNF-α Blocker
Cons• Fixed dose loses response over time; higher immunogenicity
• Mitigated by concomitant MTX
• Some loss of efficacy in heavier patients (>100 kg)• Elevated risk of TB reactivation - test for latent/active TB
required• Contraindicated in patients with CHF, MS, active infection• Very rarely lupus-like syndrome
AdalimumabTNF-α Blocker
Who gets this drug:• Any patient with moderate-to-severe psoriasis
• 1st line drug
• Psoriatic arthritis• Pediatric (children and adolescents)• No personal history of MS or severe CHF
InfliximabTNF-α Blocker
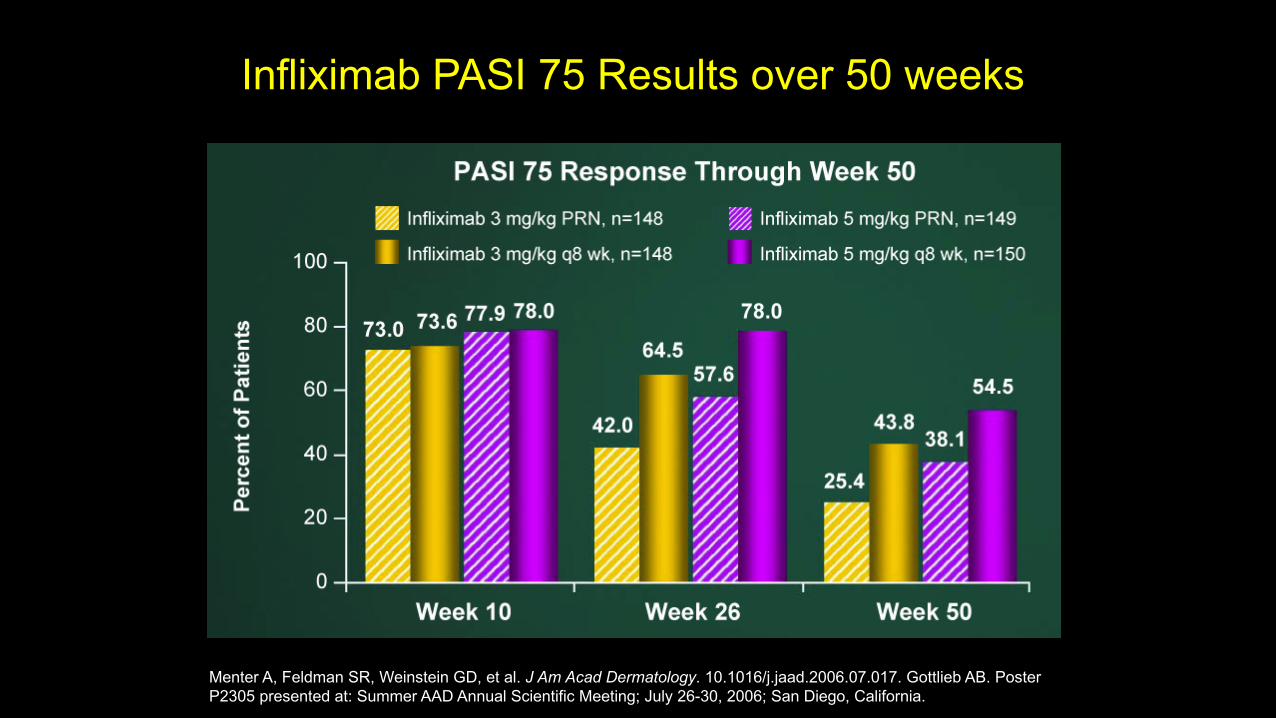
Infliximab PASI 75 Results over 50 weeks
Menter A, Feldman SR, Weinstein GD, et al. J Am Acad Dermatology. 10.1016/j.jaad.2006.07.017. Gottlieb AB. Poster P2305 presented at: Summer AAD Annual Scientific Meeting; July 26-30, 2006; San Diego, California.
InfliximabTNF-α Blocker
Pros• Superlatively effective TNF inhibitor (PI: PASI 75 78%)• Treats PsA • Dosed by weight, comparable efficacy for all weights• Pregnancy safe• Extensive post-marketing experience• No contraindication for IBD and has pediatric indication for Crohn’s
disease • May benefit patients with CV co-morbidity risks
InfliximabTNF-α Blocker
Cons• Intravenous; must monitor for infusion reactions• Loss of efficacy over time (mitigated by concomitant MTX)• Monitor LFTs• Higher risk of TB reactivation – test for latent/active TB required• Contraindicated in patients with CHF, MS and active infection• Very rarely lupus-like syndrome
InfliximabTNF-α Blocker
Who gets this drug:• Any patient with moderate-to-severe psoriasis, likely having
failed at least 2 other biologics, and previous response to 2 TNF-inhibitors who then lost response
• Obese patients who require weight-based dosing• Psoriatic arthritis• Pediatric (children and adolescents) who have failed multiple
other modalities• No personal history of MS or severe CHF
UstekinumabIL-12/23 inhibitor
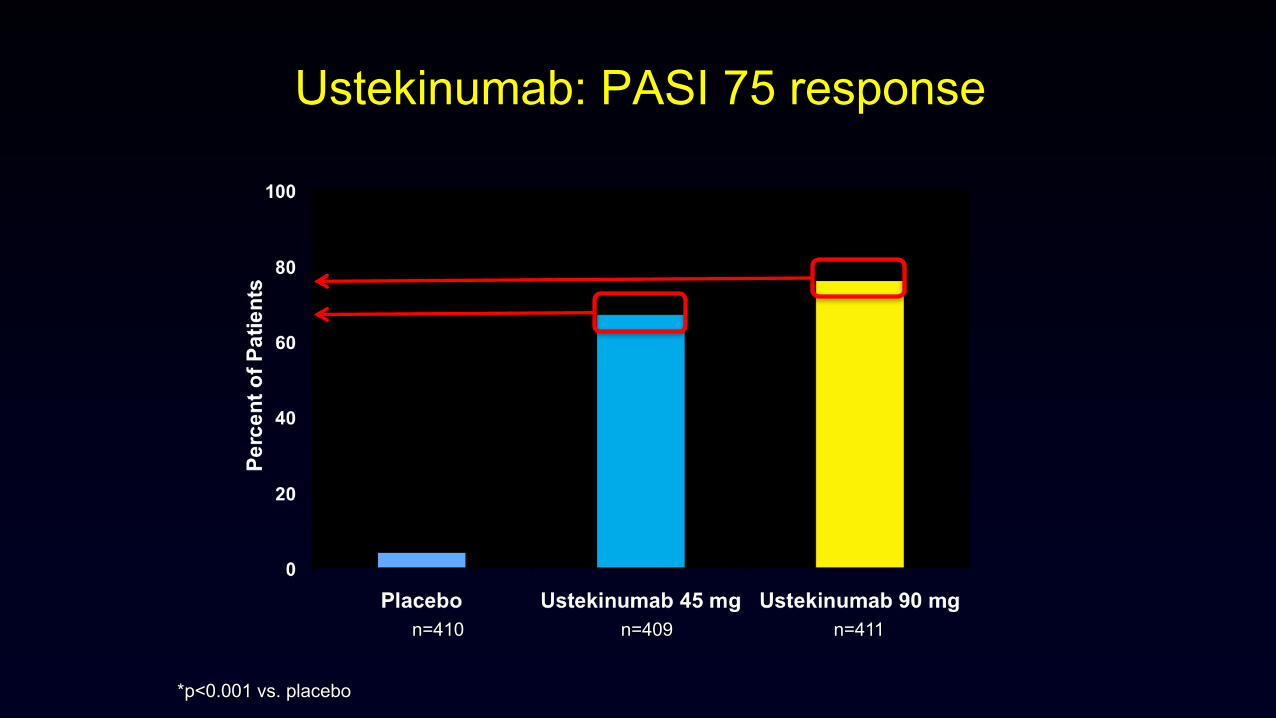
Ustekinumab: PASI 75 response
*p<0.001 vs. placebo
n=410 n=409 n=411
UstekinumabIL-12/23 Blocker
Pros• Well tolerated and highly effective• Infrequently dosed• No contraindication in CHF, MS, or IBD• Low risk of TB reactivation• Unpredictable positive effect on psoriatic arthritis
• Likely less effective than TNF-inhibitors, and, perhaps, IL-23 & IL-17 inhibitors
Cons• Lower efficacy in psoriatic arthritis• Dosing optimal for all patients?
• Q12 weeks is too great an interval for many patients
• Effects on comorbidities unclear
UstekinumabIL-12/23 Blocker
Who gets this drug:• Any patient with moderate-to-severe psoriasis
• 1st line drug
• Patients with minimal or no psoriatic arthritis• Pediatric (children and adolescents, off label)• Patients who cannot self-inject
UstekinumabIL-12/23 Blocker
GuselkumabIL-23 inhibitor
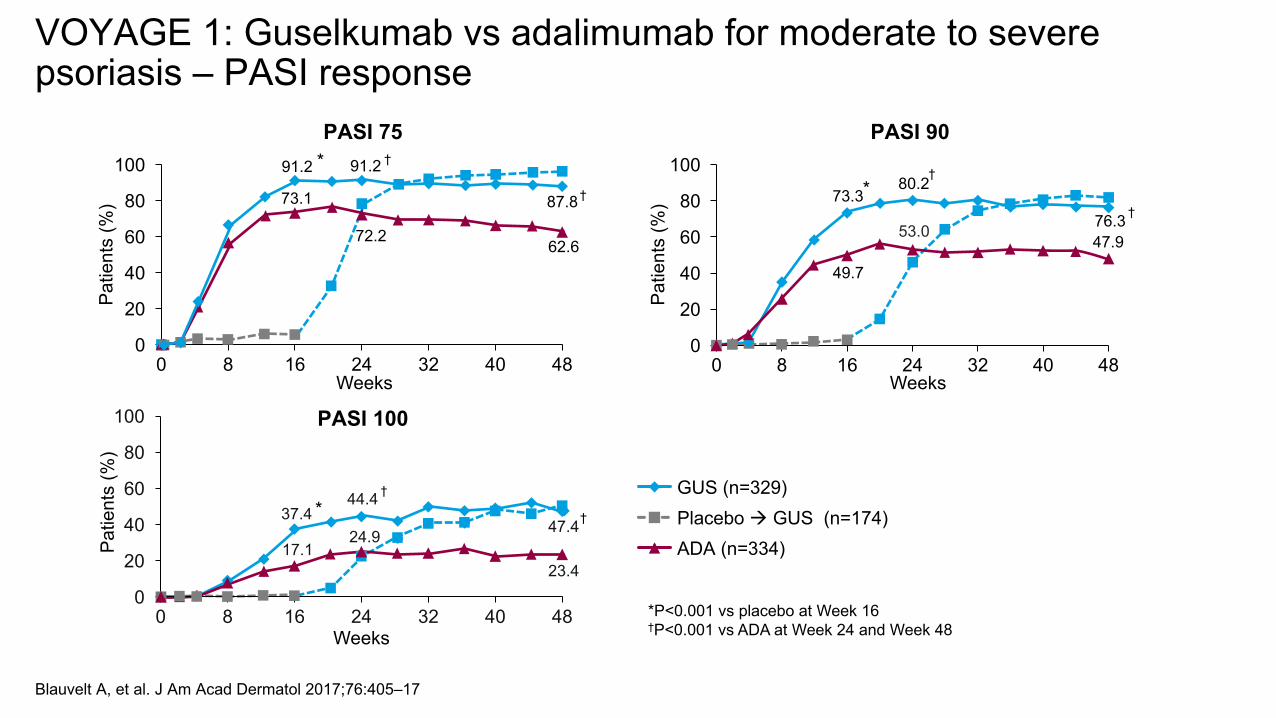
Blauvelt A, et al. J Am Acad Dermatol 2017;76:405–17
VOYAGE 1: Guselkumab vs adalimumab for moderate to severe psoriasis – PASI response
GUS (n=329)
ADA (n=334)Placebo à GUS (n=174)
PASI 7591.2 91.2
87.873.1
72.2 62.6
0
20
40
60
80
100
0 8 16 24 32 40 48
Patie
nts
(%)
Weeks
* †
† 73.380.2
76.3
49.7
53.0 47.9
0
20
40
60
80
100
0 8 16 24 32 40 48
Patie
nts
(%)
Weeks
PASI 90
†
†*
37.444.4
47.417.1
24.9
23.4
0
20
40
60
80
100
0 8 16 24 32 40 48
Patie
nts
(%)
Weeks
PASI 100
†
†*
*P<0.001 vs placebo at Week 16†P<0.001 vs ADA at Week 24 and Week 48
GuselkumabIL-23 Blocker
Pros• Well tolerated and superlatively effective• Infrequently and appropriately dosed every 2 months• No contraindication for CHF, MS or IBD• Low risk of TB reactivation• Likely very effective in psoriatic arthritis
Cons• Effects on comorbidities unclear• Long-term safety not fully established
GuselkumabIL-23 Blocker
Who gets this drug:• Any patient with moderate-to-severe psoriasis
• 1st line drug
GuselkumabIL-23 Blocker
IL-17 inhibitors
IL-17 inhibitors: Secukinumab
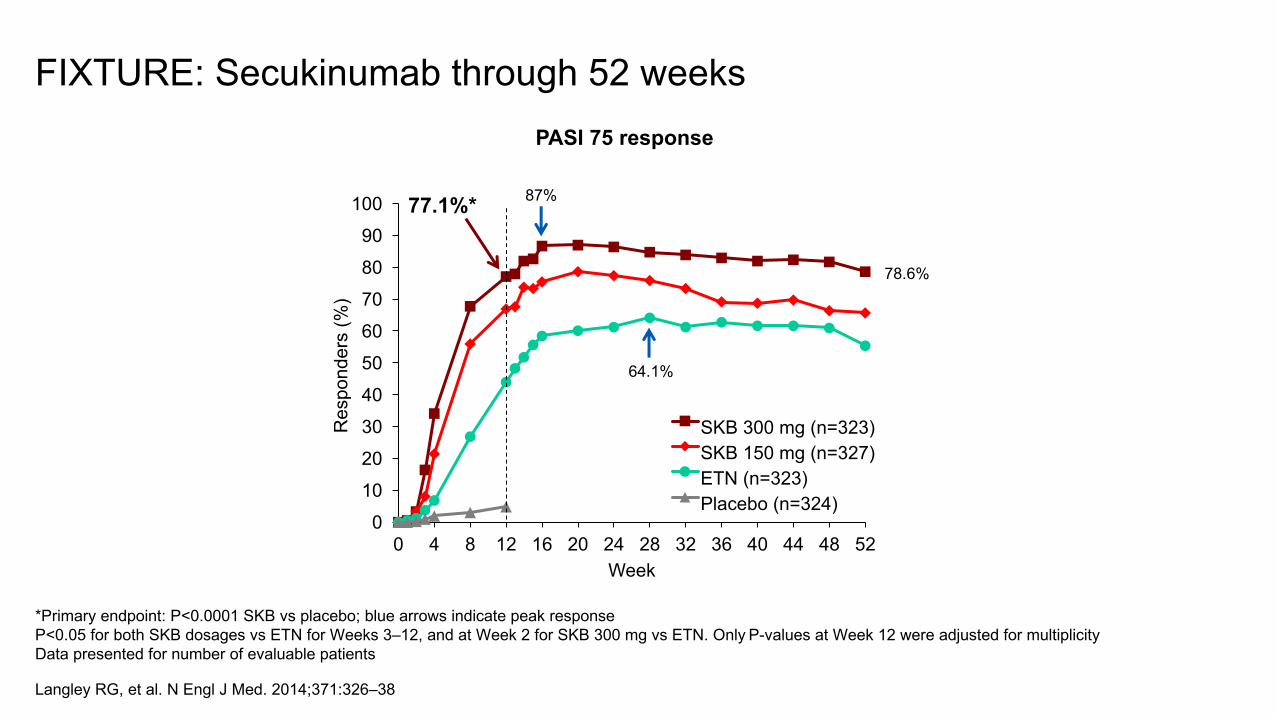
*Primary endpoint: P<0.0001 SKB vs placebo; blue arrows indicate peak responseP<0.05 for both SKB dosages vs ETN for Weeks 3–12, and at Week 2 for SKB 300 mg vs ETN. Only P-values at Week 12 were adjusted for multiplicityData presented for number of evaluable patients
Langley RG, et al. N Engl J Med. 2014;371:326‒38
FIXTURE: Secukinumab through 52 weeksPASI 75 response
0
10
20
30
40
50
60
70
80
90
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Res
pond
ers
(%)
Week
SKB 300 mg (n=323) SKB 150 mg (n=327) ETN (n=323) Placebo (n=324)
87%77.1%*
64.1%
78.6%
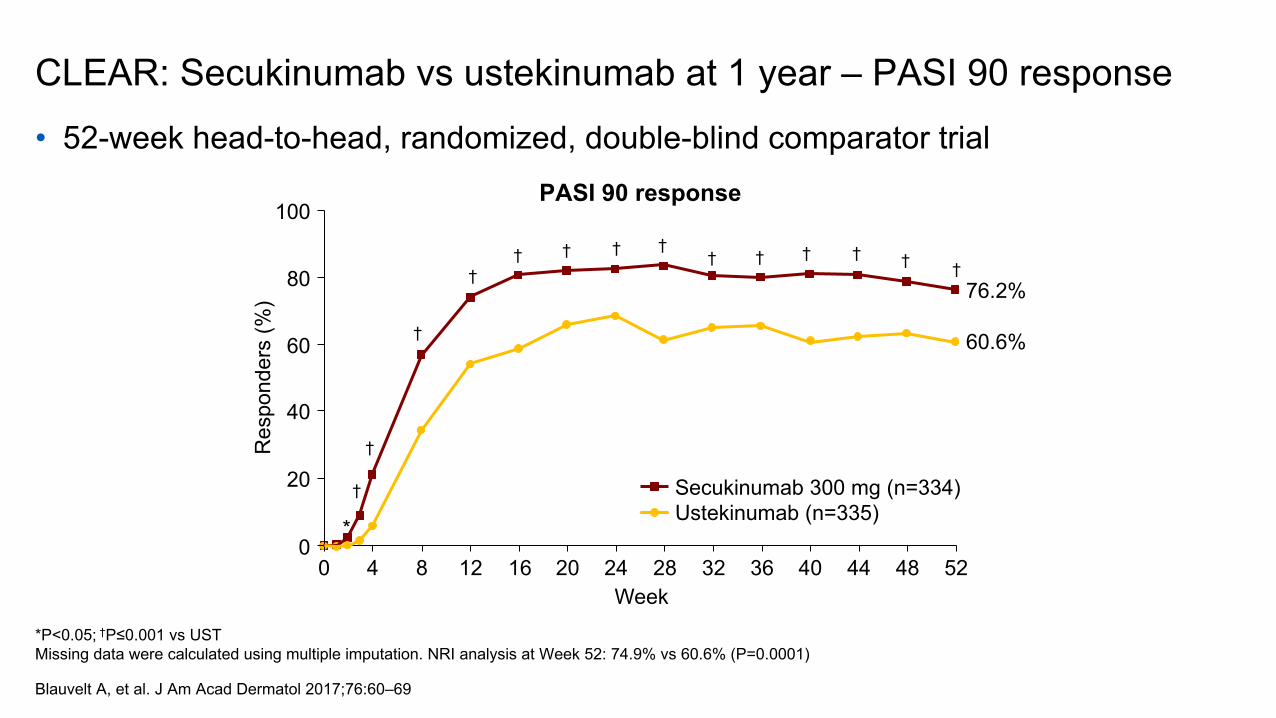
CLEAR: Secukinumab vs ustekinumab at 1 year – PASI 90 response• 52-week head-to-head, randomized, double-blind comparator trial
*P<0.05; †P≤0.001 vs USTMissing data were calculated using multiple imputation. NRI analysis at Week 52: 74.9% vs 60.6% (P=0.0001)
Blauvelt A, et al. J Am Acad Dermatol 2017;76:60–69
Secukinumab 300 mg (n=334)Ustekinumab (n=335)
Res
pond
ers
(%)
0
Week0
100
20
4 248 32
40
60
80
12 2016 5228 48444036
76.2%
60.6%
†
*
†
†
†† † † †
† † † † † †
PASI 90 response
IL-17 inhibitors: Ixekizumab
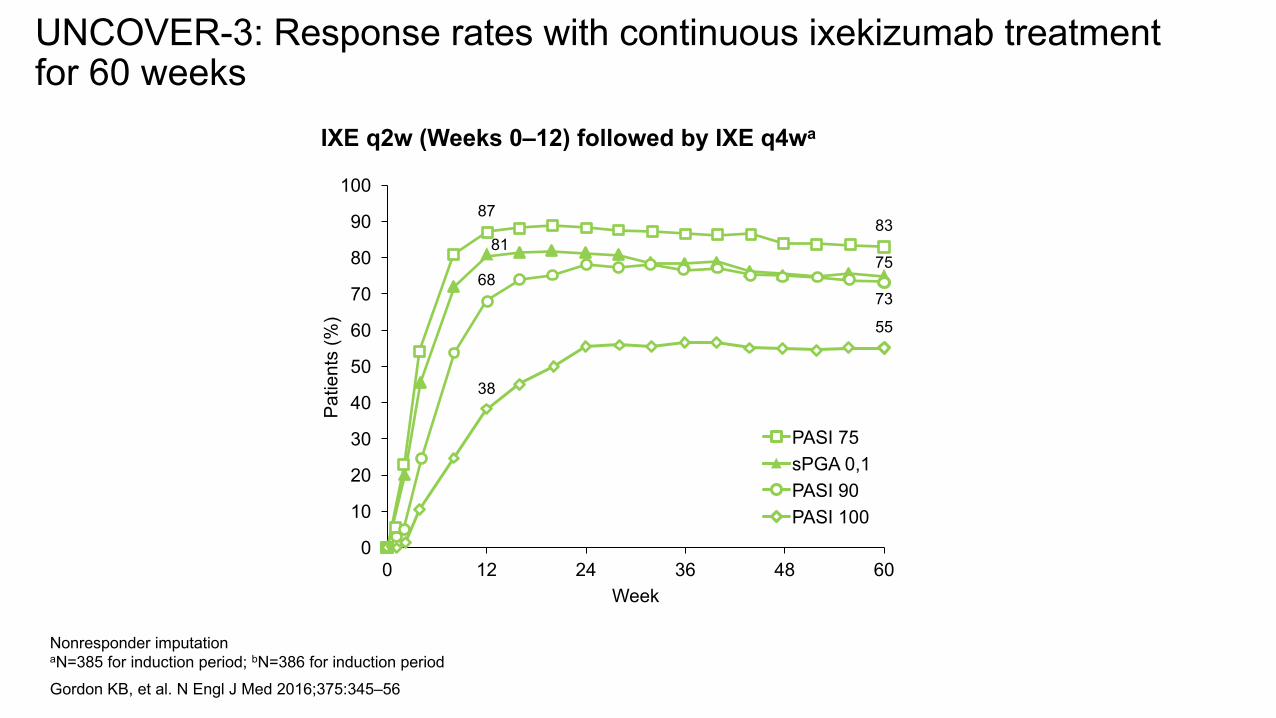
Nonresponder imputation aN=385 for induction period; bN=386 for induction periodGordon KB, et al. N Engl J Med 2016;375:345–56
UNCOVER-3: Response rates with continuous ixekizumab treatment for 60 weeks
8783
8175
6873
38
55
0
10
20
30
40
50
60
70
80
90
100
0 12 24 36 48 60
Patie
nts
(%)
Week
PASI 75sPGA 0,1PASI 90PASI 100
IXE q2w (Weeks 0–12) followed by IXE q4wa
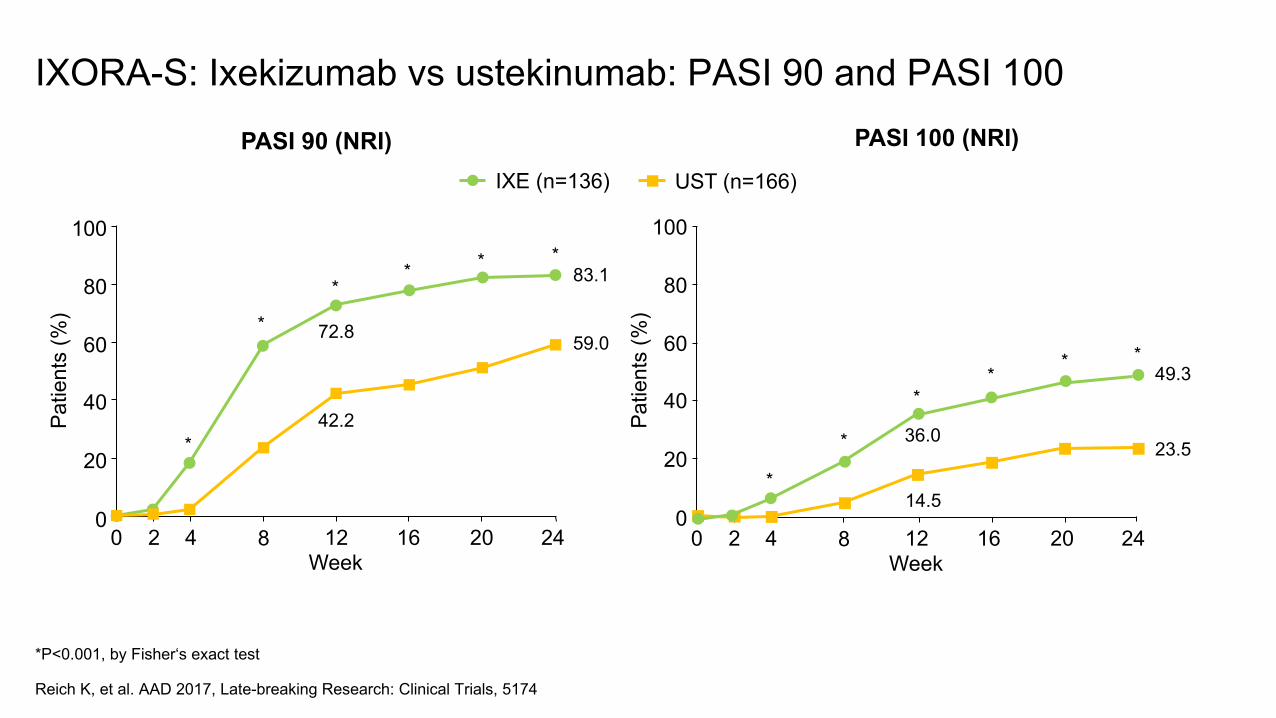
*P<0.001, by Fisher‘s exact test
Reich K, et al. AAD 2017, Late-breaking Research: Clinical Trials, 5174
IXORA-S: Ixekizumab vs ustekinumab: PASI 90 and PASI 100
IXE (n=136) UST (n=166)
Patie
nts
(%)
0
Week0
100
20
2 4
40
60
80
8 2412 2016
49.3
23.5*
*
**
* *
14.5
36.0
PASI 100 (NRI)
Patie
nts
(%)
0
Week0
100
20
2 4
40
60
80
8 2412 2016
83.1
59.0
*
*
** * *
42.2
72.8
PASI 90 (NRI)
IL-17 inhibitors: Brodalumab
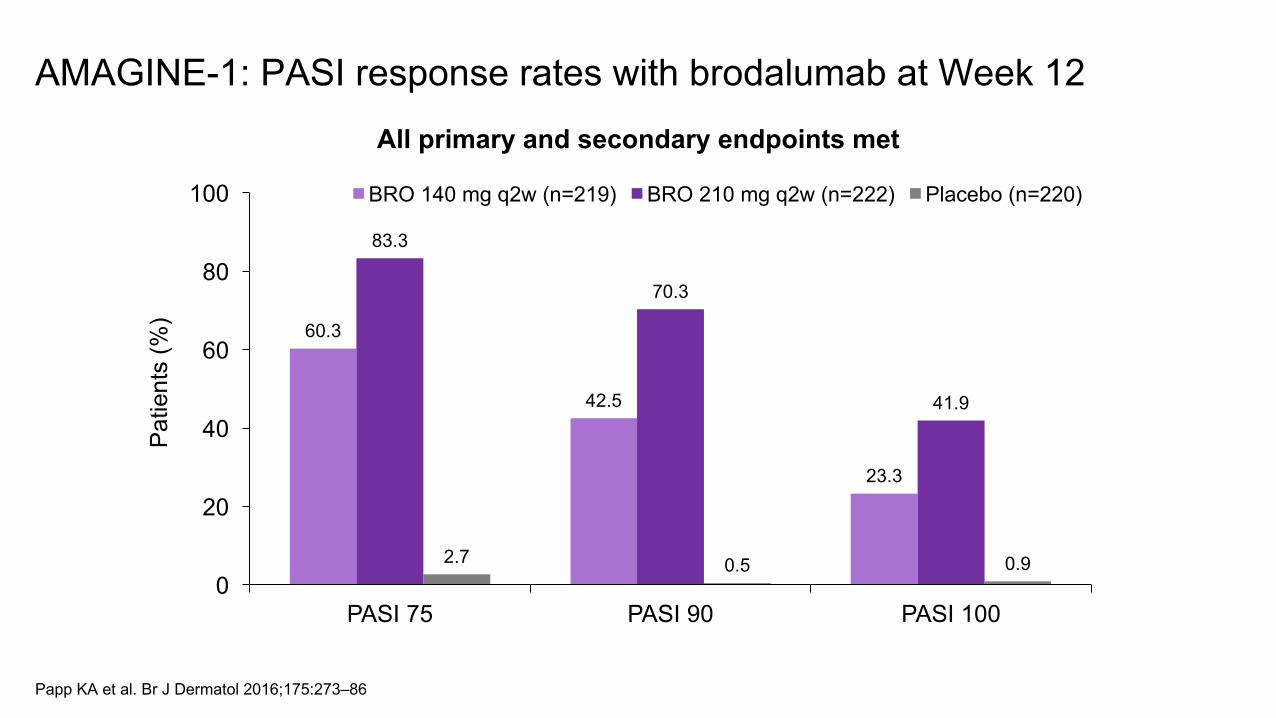
60.3
42.5
23.3
83.3
70.3
41.9
2.7 0.5 0.90
20
40
60
80
100
PASI 75 PASI 90 PASI 100
Patie
nts
(%)
BRO 140 mg q2w (n=219) BRO 210 mg q2w (n=222) Placebo (n=220)
All primary and secondary endpoints met
Papp KA et al. Br J Dermatol 2016;175:273–86
AMAGINE-1: PASI response rates with brodalumab at Week 12
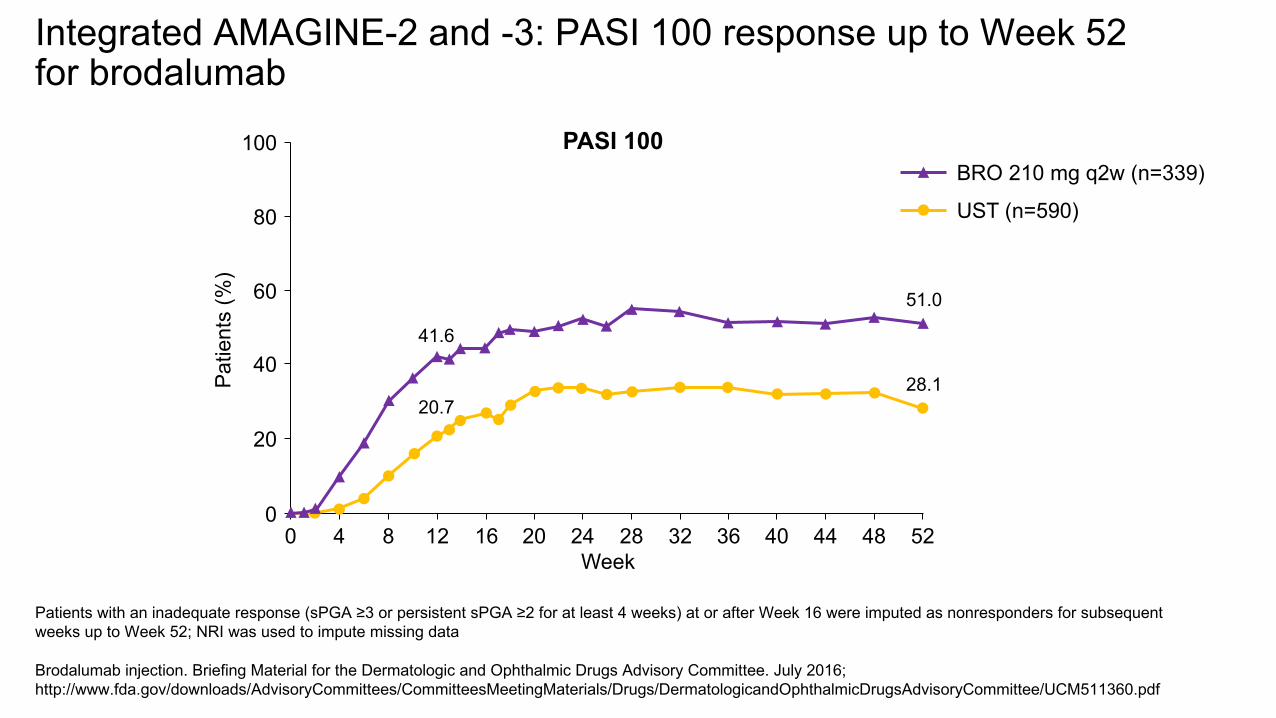
Patients with an inadequate response (sPGA ≥3 or persistent sPGA ≥2 for at least 4 weeks) at or after Week 16 were imputed as nonresponders for subsequent weeks up to Week 52; NRI was used to impute missing data
Brodalumab injection. Briefing Material for the Dermatologic and Ophthalmic Drugs Advisory Committee. July 2016; http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/DermatologicandOphthalmicDrugsAdvisoryCommittee/UCM511360.pdf
Integrated AMAGINE-2 and -3: PASI 100 response up to Week 52 for brodalumab
PASI 100
Patie
nts
(%)
0
Week0
100
20
4 248 32
40
60
80
12 2016 5228 48444036
51.0
28.1
41.6
20.7
UST (n=590)
BRO 210 mg q2w (n=339)
Brodalumab injection. Briefing Material for the Dermatologic and Ophthalmic Drugs Advisory Committee. July 2016. http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/DermatologicandOphthalmicDrugsAdvisoryCommittee/UCM511360.pdf
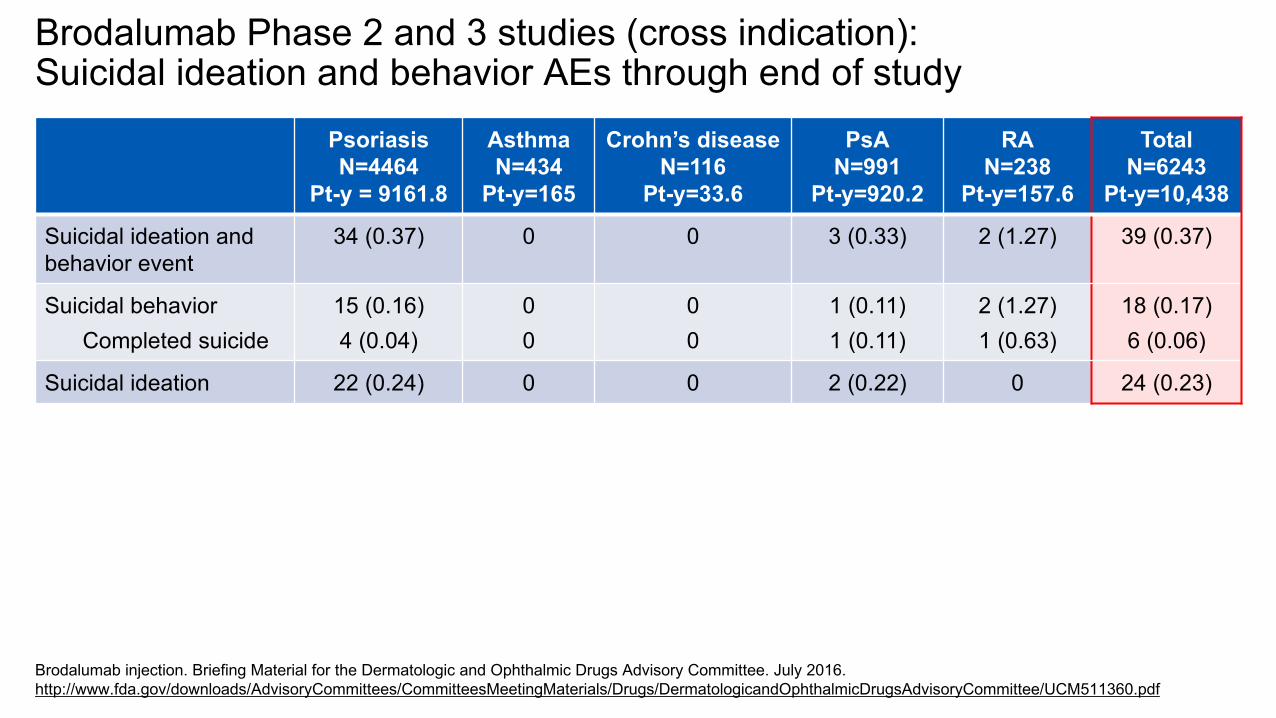
Brodalumab Phase 2 and 3 studies (cross indication): Suicidal ideation and behavior AEs through end of study
PsoriasisN=4464
Pt-y = 9161.8
AsthmaN=434
Pt-y=165
Crohn’s diseaseN=116
Pt-y=33.6
PsAN=991
Pt-y=920.2
RAN=238
Pt-y=157.6
TotalN=6243
Pt-y=10,438
Suicidal ideation and behavior event
34 (0.37) 0 0 3 (0.33) 2 (1.27) 39 (0.37)
Suicidal behaviorCompleted suicide
15 (0.16)4 (0.04)
00
00
1 (0.11)1 (0.11)
2 (1.27)1 (0.63)
18 (0.17)6 (0.06)
Suicidal ideation 22 (0.24) 0 0 2 (0.22) 0 24 (0.23)
IL-17 inhibitors
Pros• Well tolerated and superlatively effective• No contraindication in CHF or MS• Low risk of TB reactivation• Effective for psoriatic arthritis
Cons• Dosing optimal for all patients?
• Every month may be too infrequent for secukinumab and ixekizumab (after week 13 step down); brodalumab has most optimal dosing schedule at every 2 weeks
• Some fall-off in efficacy for heavier patients• Contraindicated in IBD• Ixekizumab often has painful injections and some hypersensitivity reactions• Secukinumab requires 2 injections per dose, yet injections are painless• REMS program with make brodalumab will be the most challenging to
prescribe• Effects on comorbidities unclear
IL-17 inhibitors
Who gets these drugs:• Any patient with moderate-to-severe psoriasis
• secukinumab and ixekizumab are 1st line drugs• brodalumab will be used in patients who have failed other
medications, and likely, more than one MOA
• Patients with psoriatic arthritis
IL-17 inhibitors
ApremilastPDE4 inhibitor
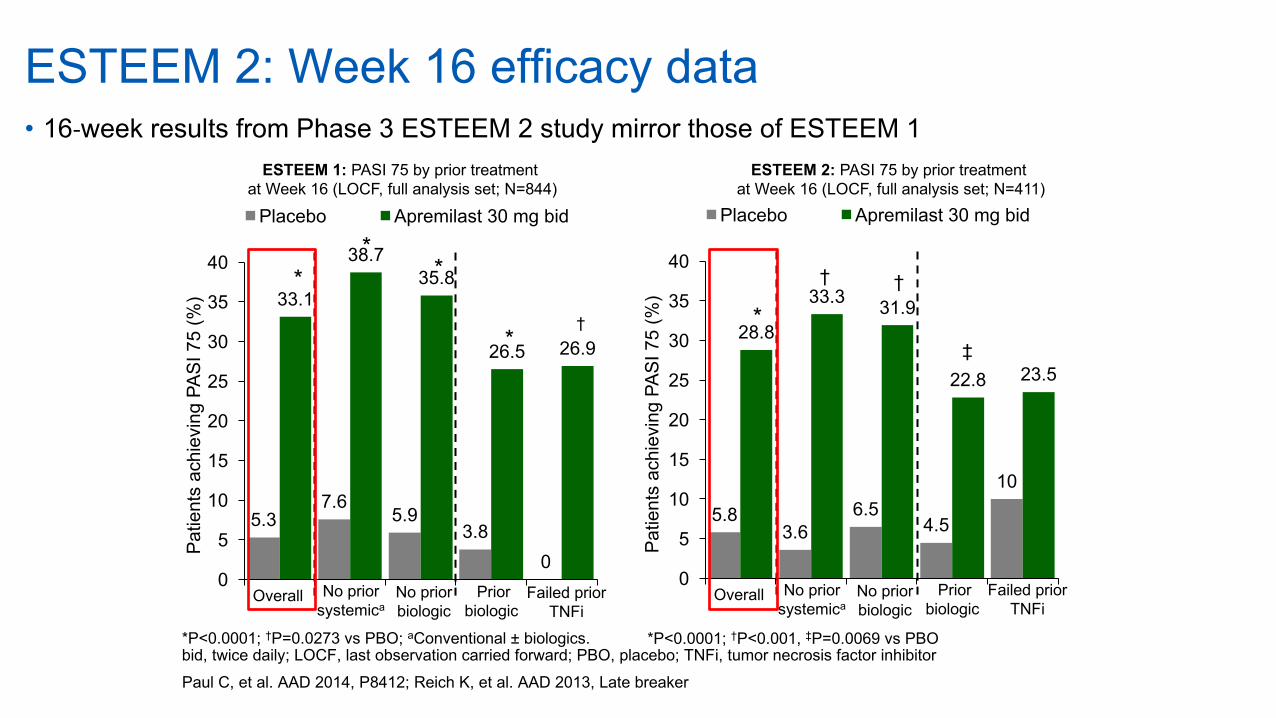
ESTEEM 2: Week 16 efficacy data• 16-week results from Phase 3 ESTEEM 2 study mirror those of ESTEEM 1
Paul C, et al. AAD 2014, P8412; Reich K, et al. AAD 2013, Late breaker
*P<0.0001; †P=0.0273 vs PBO; aConventional ± biologics. bid, twice daily; LOCF, last observation carried forward; PBO, placebo; TNFi, tumor necrosis factor inhibitor
ESTEEM 1: PASI 75 by prior treatment at Week 16 (LOCF, full analysis set; N=844)
5.37.6
5.93.8
0
33.1
38.735.8
26.5 26.9
0
5
10
15
20
25
30
35
40
Patie
nts
achi
evin
g PA
SI 7
5 (%
)Placebo Apremilast 30 mg bid
**
*
*†
No prior systemica
Overall No prior biologic
Prior biologic
Failed prior TNFi
ESTEEM 2: PASI 75 by prior treatment at Week 16 (LOCF, full analysis set; N=411)
5.83.6
6.54.5
10
28.8
33.3 31.9
22.8 23.5
0
5
10
15
20
25
30
35
40
Patie
nts
achi
evin
g PA
SI 7
5 (%
)
Placebo Apremilast 30 mg bid
*
† †
‡
No prior systemica
Overall No prior biologic
Prior biologic
Failed prior TNFi
*P<0.0001; †P<0.001, ‡P=0.0069 vs PBO
ApremilastPDE4 Blocker
Pros• Oral medication• No monitoring requirements• No contraindication in CHF, MS or IBD• Low risk of TB reactivation• Weight loss might be a positive
Cons• Low efficacy for both skin and arthritis• Effects on comorbidities unclear• Poor tolerability in some patients
• Diarrhea, nausea
• Rare mood disorders (depression)• Weight loss might be a negative
ApremilastPDE4 Blocker
Who gets this drug:• Any patient with moderate-to-severe psoriasis• Patients who fail higher efficacy biologics
• I have a preference for higher efficacy biologic therapies
• No ability to self-inject and stronger preference for oral medication
ApremilastPDE4 Blocker
KeyPoints• Choosetherapybasedonindividualpatientcharacteristics• PstreatmentisNOTstepwise(i.e.notrequiredtofailontopicals)• Onedrugormodalitymaysucceedwhenothersfail• Combinationtherapymaybedesirableinsomepatients
TopicalMonotherapyFailure
Biologic Agents• Adalimumab• Etanercept• Infliximab• Secukinumab• Ixekizumab• Brodalumab• Guselkumab• Ustekinumab
Phototherapy• UVB• PUVA
Small Molecules• Methotrexate• Cyclosporine• Acitretin• Apremilast
Sensible Treatment Paradigm
Topicals
Topicals
Topicals
TopicalMonotherapySuccess
Mild Patient low BSA involvement