Embed Size (px)
Citation preview
1
Timothy J. Wiegand, MD, FACMTAssociate Professor of Emergency Medicine
Director of Toxicology University of Rochester Medicine
Rochester, New York, USA
ASAM Disclosure of Relevant Financial Relationships
Content of Activity: ASAM Review Course 2014
Name Commercial Interests
Relevant Financial
Relationships: What Was Received
Relevant Financial
Relationships: For What Role
No Relevant Financial
Relationships with Any
Commercial Interests
Timothy J. Wiegand Purdue Pharmaceuticals
Honorarium Manuscript preparation related to Research Abuse and Addiction Related Surveillance (RADARS) data for Butrans® patch
Suggested Reading
• Principles of Addiction Medicine 5th Edition:– Section 2
• Chapter 6: Pharmacokinetic and Pharmacodynamic Principles: pages 85‐99.
• Section 14
– Chapter 112: The Science and Clinical Uses of Drug Testing: pages 1717‐1724.
– Sidebar: Workplace Drug Testing and the Role of the Medical Review Officer (MRO): pages 1725‐1729.
– Principles of Addiction Medicine: The Essentials (handbook):– Section 2
» Pharmacokinetic and Pharmacodynamic Principles: pages 27‐31
» Section 14
» Clinical and Legal Considerations in Drug Testing: pages 593‐598.
Objectives & Areas of Focus
Part 1.) Principles of Pharmacology A.) Define pharmacokinetics and pharmacodynamics
B.) Provide basic definitions and clinical applicability of pharmacologic terms including: bioavailability, Area Under the Curve (AUC), Cmax, Tmax, etc.
C.) Provide examples of the dose‐response relationship and how this relates to the reinforcing potentials of a substance with regard to route of administration.
D.)
Pharmacology
• The Study of drugs, their sources, their nature, their properties pharmacology is the study of the bodies reaction to drugs– Includes kinetics: What the body does to the drug– And dyanmics: What the drug does to the body
• Pharmacon – “poison” in classic Greek but “drug” in modern Green
• Logia –to know or “the study of”
Toxicology
• Toxicology is a branch of pharmacology, with roots in biology, chemistry and medicine. It is the study of adverse effects of the drug, of the poisoning of people.
• Toxicos or ‘toxicon’ – poison or earlier from bow and poison (poison dipped‐arrows)
2
Toxicology and dose/response
• "All substances are poisons; there is none which is not a poison. The right dose differentiates a poison…." Paracelsus (1493‐1541)
– ‐The dose that makes the poison‐‐
This stuff is important!!!
Reinforcement by route/speed
• The more rapidly a drug is delivered to its site of action in the CNS the greater the reinforcing effect.
Drug Absorption
• Drugs may be administered in a variety of ways– Oral administration one of the most common routes
• The amount of unchanged drug reaching systemic circulation after administration is the bioavailability (F).
• The amount of drug reaching the general circulation (bioavailability) depends upon various factors– Route of administration– Physical properties of the drug– Presence and type of food in the stomach and rate of emptying– Interactions with other drugs (i.e. grapefruit juice)– First‐pass metabolism
Routes of Administration
• Oral• SL or buccal• Intranasal• Inhalational
(smoked/freebase)• Transdermal• Rectal• IM or SC• IV• Intrathecal
Dose‐Response, Cmax and AUC
3
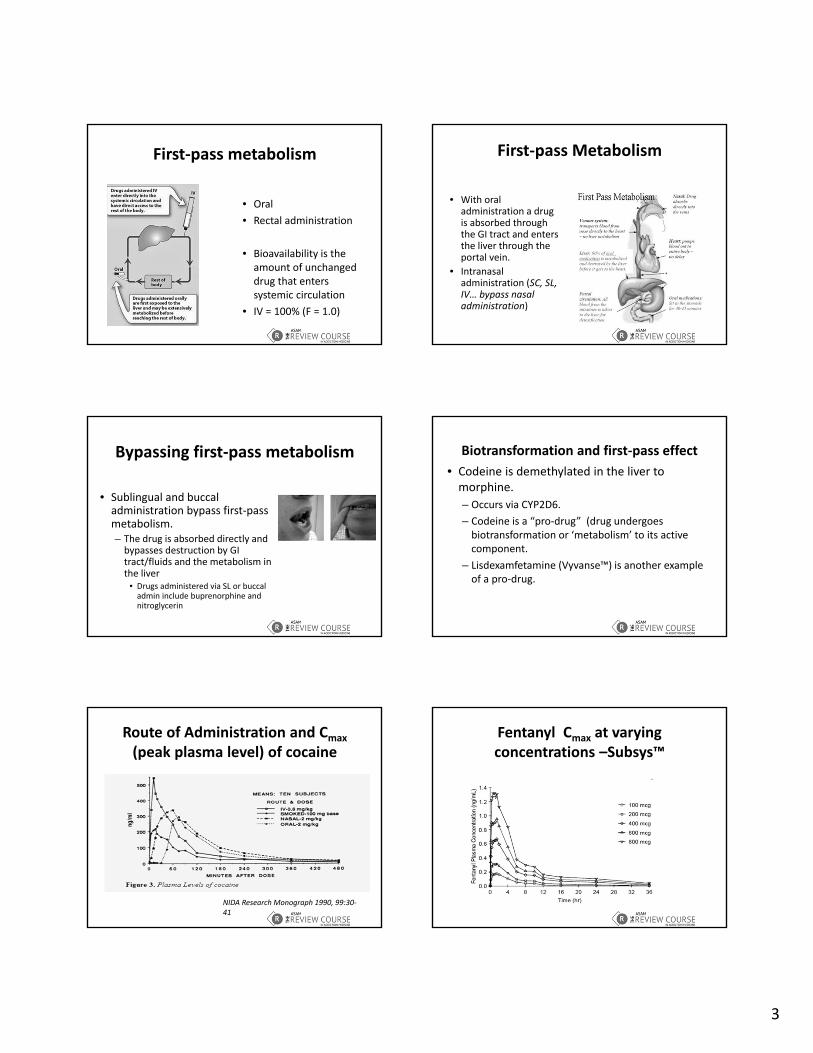
First‐pass metabolism
• Oral
• Rectal administration
• Bioavailability is the amount of unchanged drug that enters systemic circulation
• IV = 100% (F = 1.0)
First‐pass Metabolism
• With oral administration a drug is absorbed through the GI tract and enters the liver through the portal vein.
• Intranasal administration (SC, SL, IV… bypass nasal administration)
Bypassing first‐pass metabolism
• Sublingual and buccaladministration bypass first‐pass metabolism.– The drug is absorbed directly and bypasses destruction by GI tract/fluids and the metabolism in the liver
• Drugs administered via SL or buccaladmin include buprenorphine and nitroglycerin
Biotransformation and first‐pass effect
• Codeine is demethylated in the liver to morphine.
– Occurs via CYP2D6.
– Codeine is a “pro‐drug” (drug undergoes biotransformation or ‘metabolism’ to its active component.
– Lisdexamfetamine (Vyvanse™) is another example of a pro‐drug.
Route of Administration and Cmax
(peak plasma level) of cocaine
NIDA Research Monograph 1990, 99:30‐41
Fentanyl Cmax at varying concentrations –Subsys™

4
Subjective ‘high’ (0‐100) by route for cocaine (highest for smoked IV)
NIDA Research Monograph 1990, 99:30‐41
Intoxication vs plasma concentration (cocaine) ‐tolerance
NIDA Research Monograph 1990, 99:30‐41
Intoxication vs concentration –smoking (dash line) vs IV (solid line)
NIDA Research Monograph 1990, 99:30‐41
Clinical Pharmacology & Drug Design
Cmax and elimination of 10, 20, 40, 80 and 160 mg formulations OxyContin™
Route of Administration and Absorption

5
Bioavailability –how much unchanged drug is delivered to the systemic circulation. IV = 100%
Cmax and Tmax depend on route of administration
T1/2 (half‐life) is the time for Cmax to drop in half
Toxicity varies by route of administration
• IV administration of opioids may result in concentration above the respiratory depression threshold compared to other routes (i.e. IN, oral, SL, PR, IM…)

6
Tolerance shifts dose‐response to right
• Tolerance and Sensitization reflect changes in the way the body responds to a drug when it is used repeatedly.
• Tolerance is the reduction in response to a drug after its repeated administration.
• Tolerance shifts the dose‐response curve to the right –requires higher doses than initial doses to achieve the same effect.
Tolerance as modifier of euphoria
Tolerance develops to geater extent for some effects compared to others
• Tolerance develops to euphoria from opiates after repeated administration.
• Tolerance does NOT develop to opioid‐induced constipation or miosis.
SensitizationShifts dose‐response curve to left
• Indicates an increase in drug response after repeated administration.
• Shifts the dose‐response curve to the left so that repeated doses cause a greater effect than initial dose
Sensitization develops more rapidly to some effects than others
• Animal models of sensitization include increases in locomotor response to intermittent doses of cocaine or amphetamine.
• Rats given repeated daily intraperitoneal doses of cocaine had higher levels of dopamine detected by microdialysis on the 7th day than on the first day.
• Sensitization may underlie chronic stimulant psychosis as well as alcohol‐withdrawal seizures.
Cocaine self administration and tolerance to various effects
• Tolerance to various effects of cocaine in repeated self‐administration vs control

7
Fentanyl administration and tolerance
• Tolerance to the conscious‐sedating effects of fentanyl in
– Open circle –naïve rats
– Filled square –saline admin rats
– Dashed line/diamond –fentanyl infusion (60 mcg/kg) rats
Types of tolerance
• Pharmacokinetic tolerance –occurs as a consequence of increased metabolism after a drug is repeatedly administered –results in less being available at the receptor for drug activity. From: Ethanol Metabolism ‐Elsevier
Induction of MEOS can lead to accelerated metabolism of other drugs
Learned Tolerance
• Refers to a reduction in the effects of a drug because of compensatory mechanisms that are learned.
• Example –roofers and workers at heights that are able to walk in a straight line despite motor impairment from alcohol intoxication.
Conditioned Tolerance
• Conditioned tolerance is a subset of ‘learned’ tolerance –environmental cues (sights, sounds, smells) paired with drug administration lead to expectation –the drug effect experienced before drug administered
• Rats died after being given a dose of opiates to which they had been previously tolerant. The deaths occurred when the rats were put in an unusual environment instead of usual drug‐admin cage.
Cross Tolerance
• Occurs when tolerance to the repeated use of a specific drug in a given category is generalized to other drugs with the same structural/mechanistic category.
• Cross tolerance occurs between:– Ethanol
– Barbiturates
– Benzodiazepines
– Zolpidem (GABAA agonists)

8
Physical Dependence
• A state that develops as a result of adaptation and the resetting of homeostatic mechanisms.
• Can arrive from both addictive and non‐addictive use of drugs
• Withdrawal syndrome can occur in physically dependent person when the drug is abruptly stopped
Non‐addictive tolerance, physical dependence and withdrawal
• Individuals who take prescribed medicines for appropriate medical indications can show tolerance, physical dependence and withdrawal
– Propranolol
– Clonidine
– Appropriate use of opioid‐analgesics for pain
Alcohol and Drug Testing
• Clinical and Legal Considerations in Drug Testing– Testing identifies recent use it does NOT identify addiction.– Great utility in treatment of substance use disorders because denial is a feature of addiction
– Drug users may not be able to identify which drugs they have ingested (Rx/illicit/adulteration)
• Workplace drug testing may include on‐site testing (immunoassay) and more formal testing including Gas chromatography (GC) (or liquid chromatography (LC) ) and mass spectroscopy (MS)
ASAM White Paper on Drug Testing
• “Drug testing is primary prevention and diagnostic monitoring tool.”
“ABCs of drug testing”
• A – adulterant• “An adulterant is defined as any
substance that, when added to a urine specimen, alters it in such a way to yield a negative result (aka a "false negative"). Common adulterants like bleach, Visine, or glutaraldehyde, as well as many chemical oxidants such as nitrates (e.g. Whizzies, Klear), are screened for by the drug testing industry and are readily identifiable. Nevertheless, "spiking" a sample still remains a viable option for those who are willing to risk it, as there is no shortage of new, alternative adulterants promising to "beat" a urine test while avoiding the watchful eye of the drug testers”
Drug detection windows
• In general drug and metabolites can detected 1‐3 days after single use.
• Heavy use of some drugs (in particular cannabis) can detected longer (up to weeks)
• Detection time depends on limit of detection and cut‐off levels (e.g. longer for GC/MS)

9
Interpretation and Clinical Utilization of Drug Testing
• Not incorporated into standard medical training.
• Clinicians often have little understanding of false‐positive/false‐negative results.
• Clinicians are unaware of types of testing available, limitations by testing type, drug metabolism and windows of detection.
• Medical Review Officers (MROs) are specialized clinicians with certification in drug testing and interpretation.
Drug testing ‐Immunoassay
Detector molecule
Detector site
Target molecules
Immunoassay testing
• Inexpensive• Overall fairly
accurate although false positive and negative can occur
• Historically, false positives limited usefulness –current rate much less *
Immunoassay tests –”POC tests” (Point of Care testing)
• Initial screening is POC/Immunoassay• False negatives can be common with immunoassay (history of use with negative detection*)
• Confirmation by GC/MS• POC testing primary method in:
– Emergency Departments– Drug Treatment Programs*– Criminal Justice System– Home drug testing kits
Drug testing considerations
• Specific Gravity (or urine creatinine level)
• Temperature of specimen
• Directly observed
• pH and volume of sample
• In forensic testing second sample (B sample) saved for GC‐MS (confirmatory testing)
Defining the extent of false‐negatives• Split samples (one Sample divided into Sample A and Sample B) and send B for confirmatory analysis.
• Perform urine testing on proportion of oral tests (lower amounts of drug found in saliva make it easier for false‐negatives to occur for many drugs).
10
Specimen Validity Testing (SVT)
• SVT is performed to assess whether substitution, adulteration or dilution occurred.– Substitution is submission of a specimen that is not human urine or
is from another person (a ‘clean’ specimen). Temperature, creatinine and specific gravity help determine whether a specimen has been substituted or not.
– Adulteration is the addition of chemicals to a urine specimen that will mask or destroy drugs or their metabolites (nitrates, acids, oxidizing/reducing agents)
– Dilutionmay be intentional (drinking large amounts of water before providing a specimen) or the result of physiologic conditions (i.e. diabetes)
Drug testing confirmation –GCMS (or LCMS)
• GC – MS testing includes chromatographic separation and analysis
Mass spectroscopy
• Provides a ‘fingerprint’ as a chemical is heated and broken apart –(e.g. methcathinone vs ephedrine)
Drug testing by matrix ‐urine
• Easy to collect and most drugs and metabolites are easy to detect for longer periods of time than blood or saliva.
• Drugs and metabolites are concentrated in urine.• Ideally sampling is directly observed. Need same sex observer/collector.• Creatinine determination can be used to normalize drug concentrations for dilute urine.
• Federal government 5 drug test –SAMHSA ‐5– Marijuana– Cocaine– PCP – Amphetamines (and methamphetamine)– Opiates (codeine and morphine and by it’s metabolism to morphine,
heroin)
Drug testing by matrix –oral fluid
• Can be analyzed both by point‐of‐care (immunoassay) tests and GC/MS (confirmatory) testing.
• Drugs are found in much lower concentrations in saliva (compared to urine)
• Highly resistant to cheating (easy to observe)• Relatively insensitive to marijuana (THC in
very low concentrations in the body) in particular POC tests.
• Used for post‐accident or ‘reasonable’ suspicion testing. If sensitivity improves may be future standard.
Drug testing by matrix ‐hair
• Drugs and metabolites incorporated into hair as it is being formed.
• Hair grows ½ an inch/month and average hair is 1.5 inches –detection is typically over 90 days.
• It takes 7 days for hair to grow from base of follicle to point it can be snipped –hair does not detect use in preceding week
• Concentrations of drugs low with sporadic use and may go undetected (use < than 2 x/week of marijuana is often missed).
• Codeine and morphine from poppy seeds not enough to be detected in hair (compared to urine + for opiates).
• No on‐site testing methods.

11
Drug testing by matrix ‐sweat
• Sweat testing patches are similar to nicotine replacement patches.
• Patch usually removed after 1‐2 weeks.• Testing is prospective compared to other matrices.• No on‐site method for sweat testing• Resistant to cheating as the patch ‘puckers’ if
removed and reapplied.• High interindividual (and intraindividual patch)
variability • Contamination possible (external and internal)
Drug testing by matrix –blood
• Invasive testing. Not part of screening.
• Forensic and legal (post accident/injury).
• Results may be used to help interpret impairment in certain situations.
• Used for acute use during intoxication.
• More expensive than urine testing
Drug testing by matrix ‐breath
• Breath alcohol is prototype.
• Drugs of abuse are present in breath as well (albeit at very low concentrations).
• If technology advances appropriately may eventually be gold standard – Easier to collect than urine, saliva
or other matrices.
– Resistant to cheating
Advancing Technology
• “Breathometer™ can transform your smartphone into a breathalyzer within seconds — helping you monitor your alcohol consumption, giving you the power to make smarter decisions when drinking. A combination of a sleek and portable device that connects to your smartphone and an easy‐to‐use app estimates your blood alcohol level.”
Matrix Summary• Blood and breath levels may correlate with impairment for alcohol testing in particular.
• Urine and hair testing indicate test for use or exposure NOT addiction or dependence.
• Oral fluid testing indicates recent use –levels low and drugs such as THC only detected 24‐48 hours from use.
• Sweat patch testing prospective –contamination possible
Drug Detection Times by matrixTable 112‐1 in The ASAM Principles of Addiction
Medicine 5th edition: page 1722

12
Special Considerations• Student drug testing –athletics, private schools, clubs/other
‘after‐hours groups’. • Drug tests identify far more use than self report.• Primary goal of testing is prevention.• In pediatric/adolescent patients some clinicians feel
involuntary testing is violation of patient‐physician relationship however may test in cases of: – Depression– Learning problems– Accidents– Suicidal ideation or attempts
Medical Review Officer• “MRO is an impartial gatekeeper and advocate and integrity of a workplace drug testing program.”
– Verify chain‐of‐custody documentation
– Interpret and verify laboratory confirmed results
– Receives test results before they go to the individual or organization requesting the test.
– Establishes if there was acceptable explanation for non‐negative results
MRO certification and MOC1.) Must be licensed physician with experience in, “controlled substances abuse disorders.”
2.) Certified by a nationally recognized certifying board (Medical Review Officer Certification Counsel or the American Association of Medical Review Officers)
3.) Initial and refresher training is required.
MRO –contracts and regulation
1.) Contract between organization of employment and MRO before review process begins.2.) Medical Review is only part of a drug‐free workplace program –MRO can provide other components or direct employer to them.3.) MRO is prohibited from having a financial relationship with the laboratories whose tests they review.
MRO and collection processWhen working with DHHS (SAMHSA) 5 tests the MRO should work with a laboratory certified under the DHHS rules regarding credentials and performance testing for blind proficiency specimens.
With non‐urine specimens review of laboratory credentials and quality control is critical.
MRO and specimen collection• MRO is required to check each chain‐of‐custody form for signatures and collection remarks.
• For non‐negative tests the chain of custody should be confirmed as ‘not‐broken.’
• MRO also needs to evaluate ‘shy bladder’ (which is not automatically a cause for inferring ‘positive’)
• Issues of dilution, substitution, adulteration or other ‘interferences’ with laboratory testing techniques need evaluation.
• Verifies that correctable errors are corrected if possible.

13
MRO and Results• Negative results require review of the Custody Control Form (CCF) for confirmation specimen is not diluted, the temperature was in correct range along with other specimen integrity checks.
• Positive results require confirmation the correct specimen was tested, analysis was accurate and no acceptable/legitimate medical condition explains the result.
MRO and Non‐Negative Results• Differences in testing (types of drugs) between DHHS‐5 drug testing
programs and other (i.e. Physician Health Programs). • Each employee with laboratory confirmed non‐negative test offered
an interview:– MRO reviews collection paperwork from laboratory collection site.– MRO may speak with designated employee representative and
individual who collected the urine, laboratory personnel, the employees physician and pharmacy.
– On occasion the MRO may request an Independent Medical Exam (IME) of employee.
– Reanalysis of the specimen can be requested (or additional testing –i.e. conformational testing of d and l isomers of methamphetamine)
MRO and Invalid Tests• Some specimens cannot be tested
– Too dilute
– Too concentrated
– Contain an interfering substance
– pH to high/low
• Adulterants and some medications can interfere with analysis
• If laboratory cannot ID interfering substance results reported to MRO as “invalid” –reported as “test cancelled” after MRO reviews and interviews although if legitimate explanation (i.e. medication responsible) than repeat may not be necessary.
Additional Reading• 1.) ASAM White paper –Press release and link to full paper:
http://www.asam.org/docs/default‐source/pressreleases/asam‐press‐release‐on‐drug‐testing‐white‐paper.pdf?sfvrsn=0
• 2.) Substance Abuse and Mental Health Services Administration (SAMHSA) , Division of Workplace Programs: http://workplace.samhsa.gov/Dtesting.html