Embed Size (px)
Citation preview

Introduction to GIT and Stomach
To BDS 2nd year
Dr. Laxman Khanal
Assistant professor, Department of Human Anatomy
BPKIHS, Dharan
21-01-2018

Introduction
• Gastrointestinal tract (GIT) performs digestion (mechanical and chemical), absorption and excretion of waste products.
• Consists of mouth, esophagus, stomach, intestines and accessory organs.
• Medical specialty to study GIT is called as Gastroenterology.
56
8
2
1
3
7
4
5 6 821 3 74
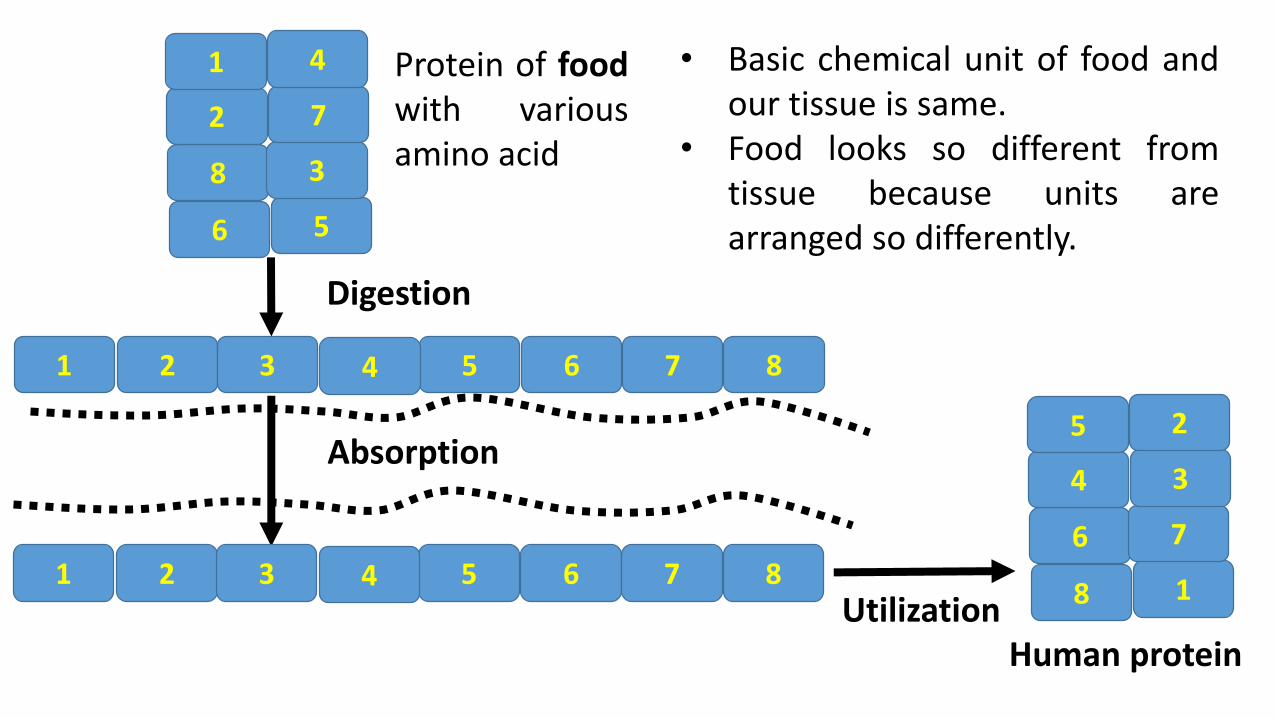
Protein of foodwith variousamino acid
Digestion
5 6 821 3 74
Absorption
18
6
4
5
7
3
2
Human protein
• Basic chemical unit of food andour tissue is same.
• Food looks so different fromtissue because units arearranged so differently.
Utilization

Gastrointestinal system1. GI tract• A continuous tube extends from
oral cavity to the anal canal.• It passes through the thoracic
cavity, abdominal cavity andpelvic cavity.
• 5-7 meter long (longer incadavers).
2. Accessory organs Consist of teeth, tongue and
glands. They helps in mechanical
digestion, swallowing and digestion.

Foregut
Midgut
Hindgut
Derivatives of endodermal lined gut tube and blood vessels supplying them

Transpyloric plane
Intertubercular plane
Midclavicular planeHorizontal planesTranspyloric planePasses through lower border of L1 vertebra.Subcostal planePasses through upper border of L3 vertebra.Intertubercular planePasses through upper part of L5 vertebra.
Vertical planeMidclavicular planeMidpoint of clavicle to midinguinal point.
1 2
7
654
3
8 9
9 regions division of abdominopelvic region


Diaphragm
Pelvic inlet
Vertebral column
12 3
4
56
1. Skin2. Superficial fascia (camper’s fascia)3. Superficial fascia (scarpa’s fascia)4. Muscle layers5. Transversalis fascia6. Extraperitoneal CT7. Parietal peritoneum
7 Anteriolateralabdominal wall

Viscera of abdominal cavity
Intraperitoneal or peritoneal organ
Extra peritoneal organ
Mesentery During development1. Peritoneal organ2. Extraperitoneal organSecondary
Primary

Basic structure1. Lumen2. Mucosa3. Submucosa Meissner’s plexus4. Muscularis layer Outer longitudinal Myenteric plexus Inner circular5. Serosa

Regulation of GI functions
1. Neural regulation
a. Intrinsic neural regulation- enteric nervous system
b. Extrinsic neural regulation- autonomic nervous system
c. Reflex control (gastrointestinal reflexes)
2. Hormonal regulation
a. Intrinsic hormones- endocrine cells of GI tract
b. Extrinsic hormones- thyroxin & cortisol

Stomach
• Widest part of GIT• Most distensible part of GIT• Mostly J shaped• Developed from foregut• Position Epigastric region Umbilical region Left hypochondrium• Capacity At birth-30ml At puberty-1 liter In adults-1.5-2 liter
Greater omentum
Lesser omentum

Cardiac end
Cardiac notch(Below the nipple)
Pyloric end
Pyloric sphincter
Angular incisura
Fundus
Body Greater curvature
Lesser curvature
123Pyloric part1. Pyloric antrum2. Pyloric canal3. Pylorus (with orifice)
External features 2 ends 2 surfaces 2 curvatures

Location of stomach ?
Q. Which of the following is not true regarding position of stomach?a. Most of it lies in left hypochondrium regionb. It also occupies epigastric regionc. Most of it lies under left costal margin and left
lower ribs.d. Pylorus part almost always extends to hypogastric
region.

Peritoneal relationship of stomach
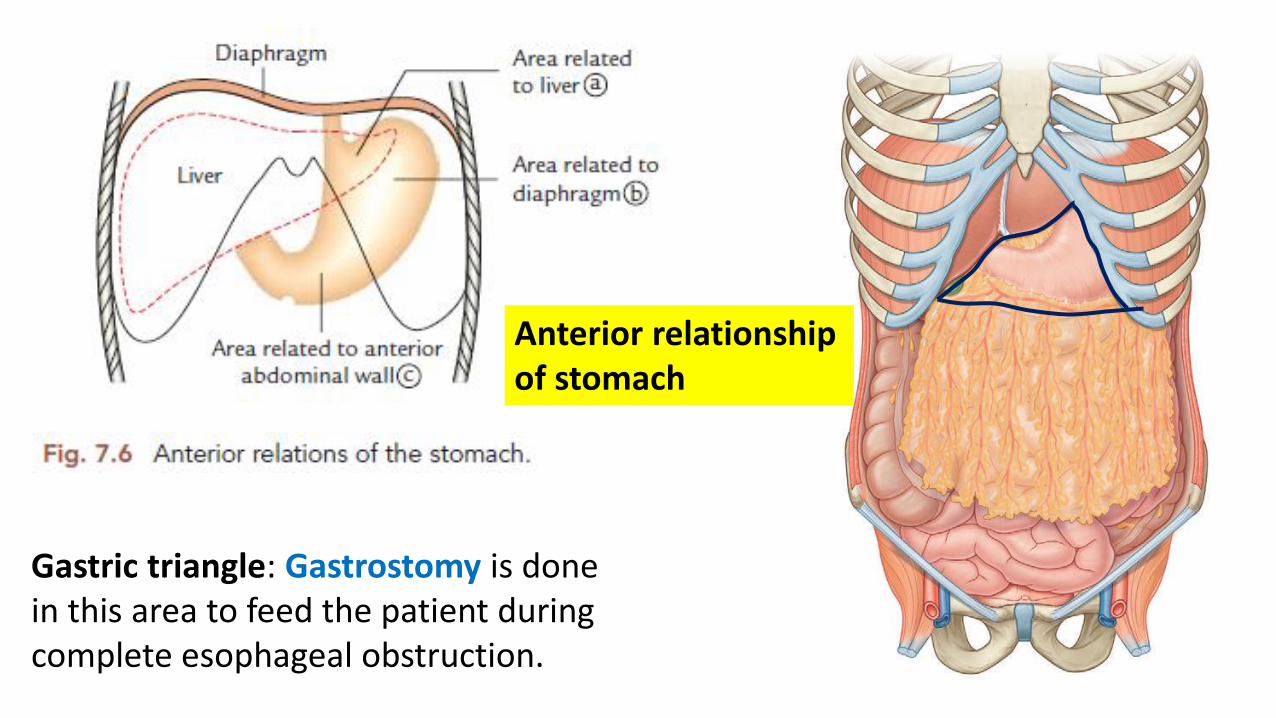
Gastric triangle: Gastrostomy is done in this area to feed the patient during complete esophageal obstruction.
Anterior relationship of stomach

Bed of stomach• Diaphragm• Left kidney• Left suprarenal gland• Pancreas• Splenic artery• Left colic flexure• Transverse mesocolon
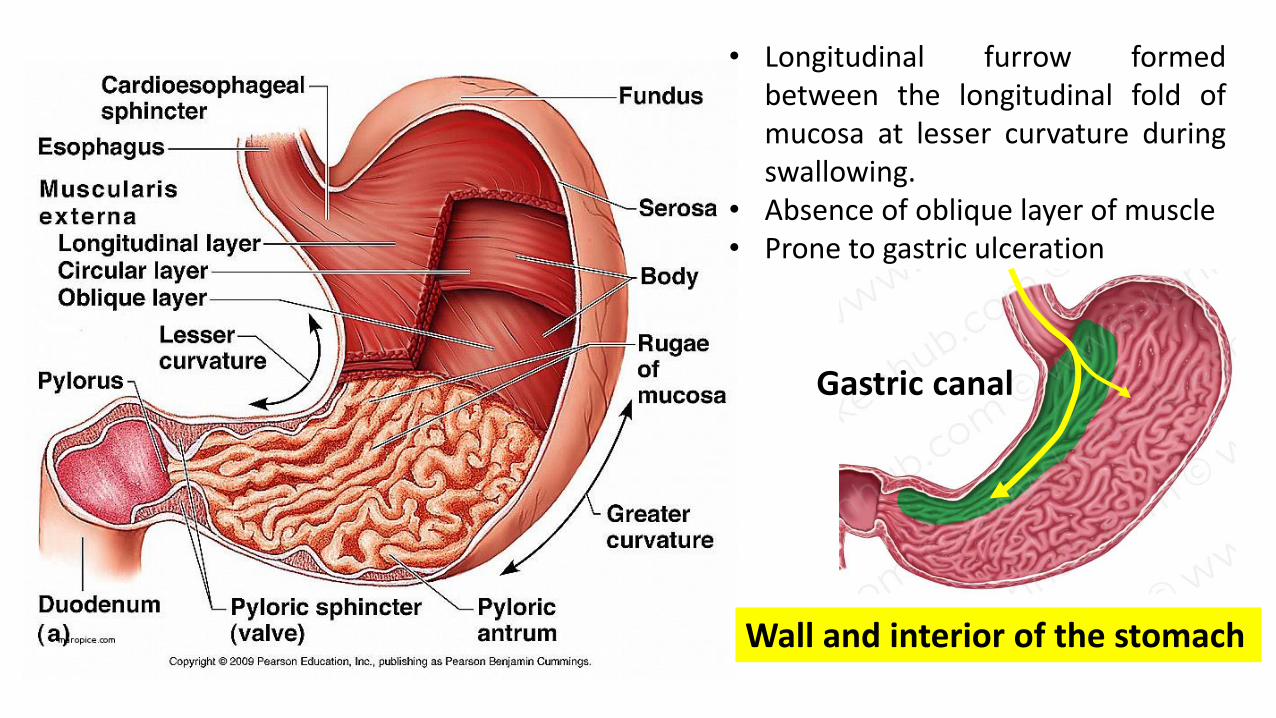
Wall and interior of the stomach
Gastric canal
• Longitudinal furrow formedbetween the longitudinal fold ofmucosa at lesser curvature duringswallowing.
• Absence of oblique layer of muscle• Prone to gastric ulceration

Coeliac trunk1. Splenic artery2. Left gastric artery3. Common hepatic artery
Splenic artery• Short gastric arteries• Left gastroepiploic artery
Left gastric artery
Common hepatic artery
Right gastric artery
Gastroduodenal artery• Sup pancreaticoduodenal artery• Right gastroepiploic artery
Hepatic artery proper Arteries of stomach
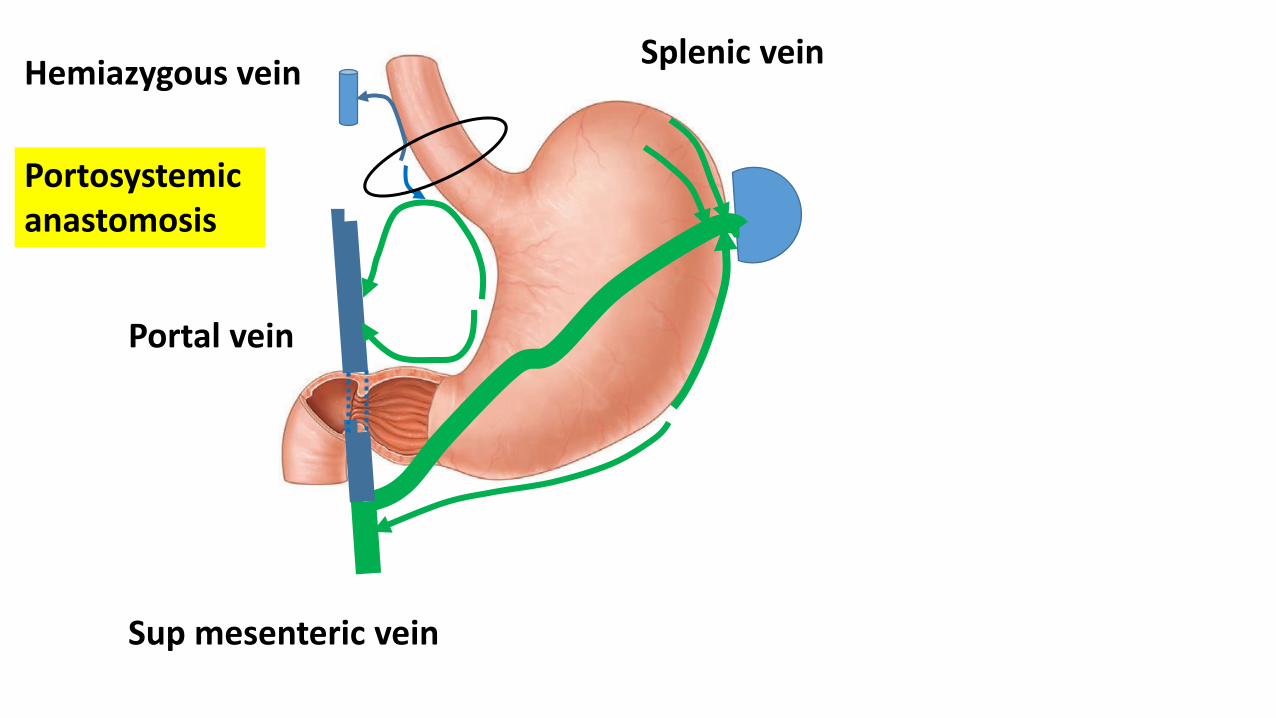
Sup mesenteric vein
Splenic vein
Portal vein
Hemiazygous vein
Portosystemic anastomosis


Lymphatic drainage of stomach
Rt gastric
Lt gastric
Pyloric LN Rt gastroepiploic LN
Pancreaticosplenic LN
Hepatic LN
Coeliac Node

Rt & Lt Vagus nerve
Parasympathetic supply
Post & Ant Vagal trunk
Sympathetic supply: T6-T9 segment
Nerve supply of stomachT6T7T8T9
Coeliac plexus
+
-
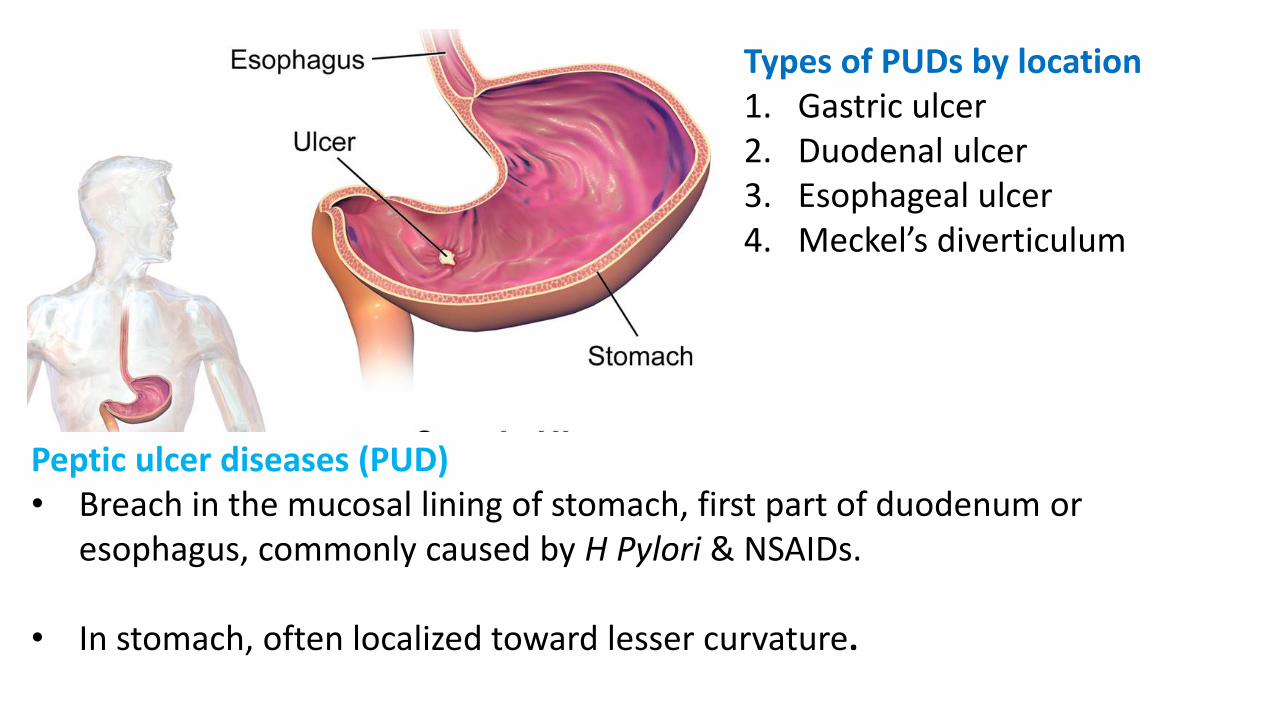
Peptic ulcer diseases (PUD)• Breach in the mucosal lining of stomach, first part of duodenum or
esophagus, commonly caused by H Pylori & NSAIDs.
• In stomach, often localized toward lesser curvature.
Types of PUDs by location1. Gastric ulcer2. Duodenal ulcer3. Esophageal ulcer4. Meckel’s diverticulum

Virchow’s LN (signal LN)• LN of the left supraclavicular fossa• Enlarged during gastric cancer
(Troisier’s sign)
Vagotomy:• Removal of part of Vagus nerve to
reduce its secretion in PUD.• Potential side effect: Vit B12
deficiency
























