Embed Size (px)
Citation preview

Ob/Gyn & Women’s Health PerspectivesAn Update for Physicians from Cleveland Clinic’s Ob/Gyn & Women’s Health Institute
Winter 2010
Innovative Procedure Addresses Cancer of the Peritoneal Cavityp 6
AlsO In tHIs IssUe
Fetal Care Center teams
Up to treat Infant with
eye Anomaly
p 8
Gyn Office
Procedures expand
p 4
Gynecologic Oncologist
earns Prestigious Award
in China
p 11
trial Compares
traditional and Robotic
sacrocolpopexy
p 12
72222_CCFBCH_ACG.indd 1 11/15/10 2:40 PM

CONTENTS
3 Clinicians and Scientists Collaborate on Promising Breast Cancer Research
4 Gyn Office Procedures Expand
6 Innovative Procedure Addresses Cancer of the Peritoneal Cavity
7 Increased Education Required to Improve Maternal Influenza Vaccination
8 Fetal Care Center Teams Up to Treat Infant with Eye Anomaly
11 Cleveland Clinic Medical Students and Staff Provide Care in Peru
10 Gynecologic Oncologist Earns Prestigious Award in China
12 Trial Compares Traditional and Robotic-Assisted Laparoscopic Sacrocolpopexy
13 Selected Publications
Dear Colleagues & Friends:
This is an exciting time for Cleveland Clinic’s Ob/Gyn & Women’s Health Institute. Our commitment to clinical excellence, innovation, education and research has earned us recognition as the No. 4 program in the country, according to U.S.News & World Report. We are proud and humbled by the confidence our patients and colleagues have shown in our treatment of women, but we are not resting on our laurels. We continue to explore new approaches to obstetric and gynecologic care that will improve our outcomes.
While our main campus location has long been a national referral center for ob/gyn care, we are expanding throughout Northeast Ohio in regional hospitals and family health centers, bringing specialized care closer to home for our patients. Whether patients are referred from near or far, we work closely with their primary ob/gyn, offering treatment recommendations and follow-up care to the extent desired.
This issue of Ob/Gyn & Women’s Health Perspectives highlights several examples of our innovative work. Among the advancements featured in the following pages area promising approach to cancer of the peritoneal cavity, exciting progress toward developing a breast cancer vaccine, development of a robust menu of hysteroscopic office procedures and research that will help define the role of robotics. I also am pleased to share the work of our team members who are actively involved in interna-tional humanitarian efforts
For more information on our work, please take a look at the recently released edition of our Outcomes book, available online at clevelandclinic.org/quality/outcomes.
I hope you find this edition of Ob/Gyn & Women’s Health Perspectives valuable. I look forward to continued collaboration with you. As always, I welcome your comments and feedback.
Sincerely,
Tommaso Falcone, MD Professor & Chairman, Department of Obstetrics and Gynecology Chairman, Ob/Gyn & Women’s Health Institute
Cleveland Clinic’s gynecology program is ranked No. 4 in the nation by U.S.News & World Report.
72222_CCFBCH_ACG.indd 2 11/15/10 2:40 PM

3
Clinicians and Scientists Collaborate on Promising Breast Cancer Research
For more than 30 years, the search for an effective breast cancer vaccine has eluded scientists throughout the world.
However, a Cleveland Clinic researcher recently reported the development of a vaccine that provides safe and effective
protection against the growth of breast tumors in mouse models. Remarkably, this protection occurs in the complete
absence of any detectable side effects.
Scientists in the laboratory of Vincent Tuohy, PhD,
Department of Immunology in the Lerner Research Institute,
evaluated alpha-lactalbumin, a breast-specific protein
over-expressed in the majority of human breast tumors
but expressed only during lactation in the normal breast.
The research involved vaccination of mice with recombi-
nant mouse alpha-lactalbumin. The team then assessed
responses in normal mice and in several mouse breast
tumor models, including autochthonous tumors in
MMTV-neu and MMTV-PyVT transgenic mice, as well as
transplantable 4T1 tumors in BALB/c mice. The data show
a significant treatment effect when mice with established
breast tumors are vaccinated and also show a highly signifi-
cant inhibition of tumor growth when vaccination occurs
prior to the appearance of palpable autochthonous tumors
and prior to inoculation of 4T1 breast tumors.
“We are hopeful that this vaccine strategy will someday be
used to prevent breast cancer in adult women in the same
way that vaccines prevent polio and measles in children,”
Dr. Tuohy says.
Derek Raghavan, MD, PhD, Chairman of Taussig Cancer
Institute, expressed cautious optimism over Dr. Tuohy’s
findings.
“This work is intriguing and the science is impressive,” says
Dr. Raghavan. “If Dr. Tuohy’s early research is validated in
clinical studies, it could potentially reduce the incidence
of breast cancer. We’re currently designing trials here at
Cleveland Clinic to test the vaccine in humans, but we’re
five to 10 years away from being able to offer it to women.”
Financial support is now needed to continue the processes
involved in moving this from the lab to the research venue to
the patient. ◆
Dr. tuohy’s research is published in Nature Medicine, June 2010, “A prophylactic, autoimmune-mediated vaccination strategy for breast cancer,” and can be found at www.nature.com/nm/index.html.
3clevelandclinic.org /obgyn | 800.553.5056
72222_CCFBCH_ACG.indd 3 11/15/10 2:40 PM

Gyn Office Procedures Expand:
Recent research has confirmed that hysteroscopic
procedures such as sterilization and endometrial ablation
performed in an office setting are safe, efficient and
provide a high degree of patient satisfaction. With patient
demand increasing for these services, gynecologists
should be aware of important requirements that will
enable them to provide office hysteroscopic procedures.
In the November 2008 edition of Journal of Reproductive
Medicine, “Utility of in-office endometrial ablation: a pro-
spective cohort study of endometrial ablation under local
anesthesia” concluded that endometrial ablation can be
performed successfully in a physician’s office under local
anesthesia and oral anixolysis with low patient pain scores,
high tolerability and high patient satisfaction. The study
found 130 of 143 patients reported being very satisfied with
the office procedure, while 13 patients said they were satisfied.
Cleveland Clinic gynecologists have found no clear advan-
tage to performing hysteroscopic sterilization in a hospital
operating room versus performing the procedure in a physi-
cian’s office.
Patient satisfaction, safety and efficiency drive demand for office hysteroscopic procedures
CLEVELAND CLINIC OB/GyN & WOMEN’S HEALTH PERSPECTIVES | WINTER 20104
72222_CCFBCH_ACG.indd 4 11/15/10 2:40 PM

strong Demand
“Office endometrial ablation is very much in demand, and
hysteroscopic sterilization is growing in popularity as more
patients become aware of the common benefits of this
minimally invasive procedure,” says Cleveland Clinic ob/gyn
Jonathan Emery, MD. “Because demand for these services
is growing, it is recommended that gynecologists consider
certain steps that will help them establish safe and efficient
office hysteroscopic procedures for their patients.”
Dr. Emery is among several gynecologists who perform outpa-
tient hysteroscopic procedures at Cleveland Clinic locations
throughout Northeast Ohio.
To develop the necessary technical proficiencies, Dr. Emery
recommends that physicians perform at least 10 to 20 hystero-
scopic procedures in a hospital operating room.
“I also recommend a minimal amount of proctoring to guide
physicians through their first few cases in the office setting,
which can enhance their comfort and confidence level when
they begin to perform these procedures solo,” Dr. Emery
explains. “Moreover, the companies that offer outpatient
sterilization methods require some degree of proctoring
for physicians.”
new Methods
Two sterilization methods that can be used in a physician’s
office are Adiana and Essure. Adiana is a new hysteroscopic
sterilization procedure that was approved for use by the U.S.
Food and Drug Administration last year. This method utilizes
radio frequency energy and a polymer microinsert that
together result in tubal occlusion in the interstitial segment
of the fallopian tube. Essure sterilization, which has been
in use since 2002, is a coiled spring device that is inserted
through the uterine cavity into the tubal opening utilizing
a hysteroscope.
“These companies provide simulation training for physicians
so they can develop a thorough understanding about how
the methods work,” says Dr. Emery. “Following this training,
companies also encourage physicians to have a proctor to
guide them through the steps of one or two procedures in an
office setting.”
Newer methods of endometrial ablation enable gynecolo-
gists to perform the procedure without special training. The
methods utilize radiofrequency, freezing, heated fluid, heated
balloon or microwave energy.
“These global methods treat the whole lining of the uterus,
which theoretically provides a more uniform destruction of
the endometrial lining,” explains Dr. Emery. “These methods
are straightforward and have safety mechanisms, although
they are not without risks. However, if physicians follow the
prescribed recommendations and safety procedures, the
outcomes are positive in terms of decreasing the patient’s
menstrual cycle."
necessary Protocols
In addition to obtaining the necessary medical equipment
such as a hysteroscope, fluid management system and other
surgical tools, performing office hysteroscopic procedures
requires protocols that typically involve a paracervial block,
non-steroidal pain relievers and, in some cases, anti-anxiety
medications.
“It also is important to have a well-trained office staff. You
need a nurse or a medical assistant who can assist from the
technical side and from the patient management side,” says
Dr. Emery. “Although these procedures require only a local
anesthetic and medications for pain management during and
after the surgery, it may be helpful to train your staff to utilize
‘vocal local techniques’ to engage and distract the patient in
conversation, which can help lower anxiety.”
Patient selection Critical
“Not all patients are suitable candidates for an office hystero-
scopic procedure,” explains Dr. Emery. “For example, a patient
who can barely withstand a physical examination is clearly
not ideal. Of course, qualifying a patient also requires a com-
prehensive review of her medical history, including whether
she has had a C-sections or other prior surgeries or has an
unusual uterine anatomy that may make the procedure too
complex to perform in a physician’s office.”
In these cases, performing hysteroscopic procedures may be
more appropriate in a hospital operating room. ◆
to refer a patient to Dr. emery or to discuss office procedures, call 440.943.2500 or email [email protected].
5clevelandclinic.org /obgyn | 800.553.5056
72222_CCFBCH_ACG.indd 5 11/15/10 2:40 PM

Innovative Procedure Addresses Cancer of the Peritoneal Cavity
Cancer of the peritoneal cavity that originates from
primary colorectal cancer, ovarian cancer, gastric
cancer, appendiceal cancer, mesothelioma and
peritoneal carcinomatosis has been virtually incurable.
For patients diagnosed with Stage IV peritoneal
carcinomatosis, survival is approximately four months.
Surgical therapy is producing promising results for some
patients. Cytoreductive (debulking) Surgery (CS) and
Hyperthermic Intraperitoneal Chemotherapy (HIPEC)
are aggressive treatments that have been shown to increase
life expectancy for well-selected patients with advanced
abdominal cancers.
“Recently, a series of research studies has shown clear benefits
for patients who have undergone CS and HIPEC surgeries,”
says Cleveland Clinic hepato-pancreato-biliary and transplant
surgeon Sricharan Chalikonda, MD, who performs approxi-
mately four CS and HIPEC surgeries every month. “For the
right patients, we are starting to see survival rates increase
by years.”
CS is a complicated surgical procedure that takes up to 10 to
12 hours to perform. It involves the destruction and/or resec-
tion of visible tumors within the peritoneal cavity. Depending
on the size and location of the tumors, the procedure also
may involve the partial resection of various viscera, such as
the small bowel, large bowel, spleen and uterus.
Removing all visible tumors is crucial to the patient’s progno-
sis for long-term survival. The patient’s survival also depends
on the volume of tumors within the abdomen and the aggres-
siveness of the carcinoma. The patient’s survival outlook
decreases when all tumors cannot be eradicated or resected,
unless they are less than 2.5 millimeters.
HIPEC facilitates the destruction of very small tumors that
cannot be seen by the surgeon. HIPEC also eliminates cancer
cells that may be hiding or those that may have been released
during resections of visible tumors or when portions of
visceral organs have been removed. The HIPEC procedure
involves placing special catheters in the patient’s abdomen.
Once the chemotherapy agent is heated to 42 degrees Celsius,
it is distributed into the abdomen through the catheters for
100 minutes.
“HIPEC enables us to deliver higher concentrations of the
chemotherapy agent into the peritoneal cavity, which facili-
tates the destruction of remaining cancer cells,” explains
Cleveland Clinic gynecologic oncologist Pedro Escobar, MD,
Director of Robotic and Minimally Invasive Surgery, who
operates with Dr. Chalikonda on gyn cases.
HIPEC causes fewer side effects than IV chemotherapy
because of the peritoneal plasma barrier, which prevents
the high concentrations of the chemotherapy solution from
invading the bloodstream.
Patients who may be candidates for CS and HIPEC are those
with Stage IV cancer that is confined to the abdomen with no
evidence of hematagenous spread of the disease. Other fac-
tors include comorbidities, the type of cancer, surgical history
and the patient’s overall physical strength to withstand the
CS and HIPEC procedures. ◆
To make a referral or for more information, please contact Dr. Escobar at 216.445.8486 or Dr. Chalikonda at 216.445.0053.
Cover story
6 CleVeland ClInIC Ob/Gyn & WOmen’S HealtH PerSPeCtIVeS | WInter 2010
72222_CCFBCH_ACG.indd 6 11/22/10 10:28 AM

In February 2010, Cleveland Clinic launched a study of vac-
cination compliance in pregnant women who received their
prenatal care in Cleveland Clinic outpatient clinics and
planned to receive intrapartum care at Hillcrest Hospital, a
busy (3600 deliveries per year) community hospital located
in the eastern suburbs of Cleveland. Patients were asked to
answer 18 questions while waiting for an office visit during
the month of February. The questionnaire involved both
seasonal and H1N1 vaccination. Descriptive statistics were
applied, and comparisons were made using appropriate tests.
A total of 328 questionnaires were collected at a gestational
age of 23.5 weeks.
The study indicated that the major reason for refusal of both
the seasonal and H1N1 vaccination was belief that the vac-
cines had not been studied enough. Despite reports from a
recent review of the safety of the inactivated influenza vaccine
verifying that no study has yet demonstrated an increased risk
of either maternal complications or adverse fetal outcomes,
the issue of vaccine safety remains an important barrier.
The next most frequent reason for refusal was related to the
fact that the patient’s ob/gyn provider neither discussed nor
recommended vaccination. When the ob/gyn provider dis-
cussed H1N1 vaccination, 69.1 percent of the patients received
the vaccination, compared to 33.3 percent who declined the
H1N1 vaccination (p<0.001). When the patient either strongly
agreed or agreed that the ob/gyn provider thought it was
important to get vaccinated against H1N1, the vaccination
rate increased from 34.2 percent to 75.7 percent (p<0.001).
When the ob/gyn provider did not recommend seasonal
vaccination, 92.7 percent refused vaccination, compared to
40.8 percent who refused when it was recommended by the
ob/gyn provider (p<0.001).
Increased Education Required to Improve Maternal Influenza vaccination
By elliot Philipson, MD, Jonathan emery, MD, and Benjamin nutter
While pregnant women represent just 1 percent of the U.S. population, they accounted for 5 percent of H1N1 flu
deaths in 2009, according to a study by the Centers for Disease Control and Prevention. H1N1 is about as deadly
as seasonal flu overall, but kills a higher proportion of those who are otherwise young and healthy, and is more deadly
for pregnant women.
The three factors that produced the highest vaccination rate
were having a discussion with the ob/gyn provider, the pro-
vider's recommendation, and the belief that the vaccine had
been studied enough.
It is clear from this study that to increase the vaccination
rate of both seasonal and H1N1 influenza during pregnancy,
there must be improvement in the information provided by
the obstetrical providers to their patients. In a climate where
more than 75 percent of the patients either strongly agreed
or agreed that the advice by their providers was important to
them, almost 30 percent reported that their ob/gyn providers
did not discuss influenza or vaccination with them.
More information and educational materials that are directed
to both patients and providers addressing barriers to vaccina-
tion should be considered. This type of interventional strategy
would improve antepartum care, have economic value and,
most important, decrease the severity of H1N1 influenza and
maternal deaths in this high-risk group. ◆
Drs. Philipson and emery recently presented their results at the annual meeting of the Central Association of Obstetricians and Gynecologists. For more information on the study, contact Dr. Philipson at 440.312.7774 or [email protected] or Dr. emery at 440.943.2500 or [email protected].
7clevelandclinic.org /obgyn | 800.553.5056
72222_CCFBCH_ACG.indd 7 11/15/10 2:40 PM

Fetal Care Center Teams Up to Treat Infant with Eye Anomaly
When a maternal or fetal problem threatens a pregnancy, Cleveland Clinic’s Fetal Care Center facilitates diagnosis,
offers counseling, and orchestrates delivery and immediate postnatal treatment to maximize patient outcomes.
Team members shift to meet the needs of each clinical
situation. In the following case, the center’s maternal-fetal
medicine specialists and neonatologists teamed with an
ophthalmic oncologist, ophthalmic geneticist, pediatric neu-
rosurgeon and fetal imaging specialist when an orbital cyst
was diagnosed in utero. The entire process was coordinated
by one of the center’s two advanced practice nurses, who also
provide constant communication and support to the family.
History: An ultrasound for an unrelated obstetric concern
revealed an orbital cyst in the fetus (at 27 weeks, 6 days esti-
mated gestational age) of a 28-year-old, G2P0 woman. The
4-cm x 2-cm cyst behind the right eye occupied the right orbit,
with a high likelihood of extensive damage within the eye.
The left orbit appeared normal. The mother and father were
advised of concerns about fetal brain development, although
ultrasound findings appeared normal. Upon hearing this, they
sought a second opinion in Cleveland Clinic’s Fetal Care Center.
Maternal-fetal medicine consult: The couple met the following
day, Sept. 17, 2008, with maternal-fetal medicine specialist
Jeffrey Chapa, MD, for a repeat ultrasound and consultation.
Imaging revealed the cystic mass posterior to the right eye;
however, the globe, including the lens and muscular attach-
ments, appeared to be intact. The eye was severely proptotic,
protruding from the orbit.
Cesarean section was planned to avoid potential trauma to
the globe during passage through the birth canal. Left eye
findings were unremarkable, as were intracranial anatomy
and the remaining fetal anatomy.
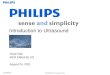
Fetal MRI: Ultrafast fetal MRI, obtained the following day in
our Fetal Imaging Center, showed an intraconal cyst involving
the right orbit that produced marked proptosis but minimal
globe deformity. Pediatric imaging specialists Janet Reid, MD,
and Stuart Morrison, MD, believed that location and appear-
ance suggested a lymphatic or venolymphatic malformation
or, less likely, a colobomatous cyst. Because the finding was
relatively recent, concerns were raised regarding rapid pro-
gression of the cystic structure. Follow-up MRI was planned
in two weeks.
Ophthalmology consult: After a follow-up visit with Dr. Chapa,
the couple had a prenatal consult on Sept. 23 with Arun Singh,
MD, Director of Ophthalmic Oncology in Cleveland Clinic’s
Ultrafast fetal MRI revealed intraconal cyst involving the right orbit, producing marked proptosis
Several stitches placed to protect what appeared to be the functional globe
Baby at 6 months of age growing and thriving
8 Cleveland CliniC Ob/Gyn & WOmen’s HealtH PersPeCtives | Winter 2010
72222_CCFBCH_ACG.indd 8 11/22/10 10:36 AM

Ashtabula County
Medical Center
2420 Lake Ave.
Ashtabula, OH 44004
440.997.6915
Beachwood Family Health
and surgery Center
26900 Cedar Road,
Suite 210 South
Beachwood, OH 44122
216.839.3100
elyria Family Health
and surgery Center
303 Chestnut
Commons Drive
Elyria, OH 44035
440.204.7400
Fairview Medical Center
18099 Lorain Ave.,
Suites 320/345
Cleveland, OH 44111
216.476.7144
Hillcrest Medical Office
6770 Mayfield Road,
Suite 426
Mayfield Heights, OH
44124
440.312.2229 (BABy)
Independence Family
Health Center
5001 Rockside Road,
Crown Center II
Independence, OH 44131
216.986.4130
lakewood Hospital
Community Health Center
1450 Belle Ave., Suite 310
Lakewood, OH 44107
216.529.2202
Westlake Medical Campus
850 Columbia Road,
Suite 320
Westlake, OH 44145
216.476.7144
strongsville Family Health
and surgery Center
16761 SouthPark Center
Strongsville, OH 44136
440.878.2500
Wooster Family
Health Center
1740 Cleveland Road
Wooster, OH 44691
330.287.4930
Expanded Maternal-Fetal Medicine Services
Cleveland Clinic has expert maternal-fetal medicine
services in several locations in Northeast Ohio.
Our high-risk pregnancy-related services include
preconception planning, pregnancy management
(primary or consultative) and delivery. Our goal is to
get patients in to be seen in a timely manner, while
keeping them close to home.
Cole Eye Institute. Dr. Singh discussed the ultrasound and
fetal MRI findings with them, describing potential diagnoses
and treatments for the orbital mass, based on the findings at
birth. The repeat fetal MRI on Sept. 30 showed relatively little
change, and surveillance continued via ultrasound for the
remainder of the pregnancy.
Orchestrating delivery: The Cesarean section was scheduled
for Dec. 1, 2008. Standing by were Dr. Chapa and maternal-
fetal medicine colleagues (to facilitate care for the mother)
and neonatologists Ricardo Rodriguez, MD, and Sabine Iben,
MD (to care for the newborn). Dr. Singh and his ophthalmic
surgical team, ophthalmic geneticist Elias Traboulsi, MD,
and pediatric neurosurgeon Mark Luciano, MD, were ready.
Side-by-side operating rooms were reserved. The father was
present for delivery, and the baby was promptly assessed.
The father then carried his daughter to the adjoining OR for
further assessment.
Prompt team assessment: Drs. Singh, Traboulsi and Luciano
were concerned that the proptosis worsened when the baby
cried. They quickly decided that further imaging was needed
to determine the cyst’s possible etiology prior to any invasive
procedure. Dr. Singh placed several stitches (a temporary
tarsorrhaphy) to protect what appeared to be the functional
left globe.
surgery and follow-up: Imaging revealed that the cyst had no
communication with any intracranial structures. Under the
care of Drs. Singh and Traboulsi, the baby underwent two
surgeries for partial cyst removal, with histopathologic con-
firmation of a benign squamous epithelial cyst.
By the time the baby reached 6 months of age, she was growing
and thriving. The cyst had not recurred, and she had good use
and function of her right eye. She required continued follow-
up to check for cyst recurrence and would likely need surgery,
including a procedure to shorten her right extra-ocular
muscles and cosmetic surgery for her eyelids. ◆
to refer families to Cleveland Clinic’s Fetal Care Center, please call coordinator Donna Patno, Rn, CnM, DnP, at 216.444.9706 or 866.864.0430.
9clevelandclinic.org /obgyn | 800.553.5056
72222_CCFBCH_ACG.indd 9 11/15/10 2:40 PM

Cleveland Clinic Medical Students and Staff Provide Care in Peru
CCLCM students Anna Brady, Jacqueline Chu, Alida Gertz,
Rachel Roth and Satoko Kanahara initiated the project.
They were accompanied by Tommaso Falcone, MD, Chairman,
Ob/Gyn & Women’s Health Institute, and retired staff member
Gita Gidwani, MD, as well as professionals from around
the country, including students and physicians from Yale,
Dartmouth, Mayo Clinic and Stanford.
The group was invited by the mayor and a local nonprofit
organization, Peruvian Hearts, to help the clinic become a
trusted and sustainable entity in the community. As team
members helped the clinic, they also soaked up many real-
life lessons.
“The level of teaching for the fourth-year students has been
great − we see patients on our own, present them with an
assessment and plan, have one of the doctors look over the
physical/history, and do some one-on-one teaching. Everyone
agrees they are learning a lot,” Roth wrote in her blog.
Participants saw the true value of simple human contact.
“Listening and reassuring them or directing them within the
medical system is the most important part of the medicine
we do here, and, indeed, medicine in general ... and (it) can
do as much for their state of mind as temporary fixes like
albendazole or Tylenol,” she wrote.
Kathleen Franco, Associate Dean of Admissions and Student
Affairs at CCLCM, says the faculty is very proud of the stu-
dents. “We are thrilled about what they did there and how
much of their free time they spent beforehand making sure it
went well,” she says.
Their preparation took place over about a year and a half
and included taking Spanish classes every Sunday, as well
as jumping legal hurdles and acquiring support, supplies
and advisers.
“They believed in it enough to make it happen,” Dr. Franco
says. “They were extremely respectful and concerned for those
who do not have the healthcare we receive in this country.”
Student Shares Snapshot
While the clinic was clean and spacious, it lacked some
key details. For example, it has a lead-lined room for X-rays
but no X-ray machine, and an operating room but no lights
or equipment.
Roth says the team expected a slow start the day it arrived
because local radio stations announced they were coming a
day later, but those expectations were soon cast aside. “We
were planning on getting organized in the morning and
starting to accept patients at 1 p.m. By 8:45 a.m., there was a
line,” Roth wrote in her blog. “As we watched people trickle in
steadily, it became obvious that the longer we waited to see
people, the longer we would be at the clinic.
“By 9:15, I was taking stitches out of a woman whose bull had
impaled her. It was only her leg, but there was an entry wound
and exit wound, and it was infected and ulcerated of course,
and why are the stitches still in three weeks later? Plus, do you
have any idea of the kind of logistics necessary to treat even
the smallest thing? First, just a place to sit. She sat in a spare
dentistry chair. I squatted on the floor. Second, light. We left
the door open for the hallway light, and I used my penlight
to spot the stitches amongst the scab and the healing tissue.
Third, water. Even if it was running somewhere in the clinic,
it’s not clean, so I used lots of iodine and alcohol ... she took
45 minutes. There were 10 people in the waiting room when I
came out at 10 a.m.”
A group of students and staff from Cleveland Clinic Lerner College of Medicine traveled to Peru’s impoverished area
of Lamay in the summer to staff a clinic established by the town’s mayor to attract medical personnel.
10 CLeveLAnd CLiniC Ob/Gyn & WOMen’s HeALtH PersPeCtives | Winter 2010
72222_CCFBCH_ACG.indd 10 11/22/10 10:29 AM

The team adjusted quickly, though, and two days later
saw about 80 patients in the same amount of time that
40 were seen the day before.
Future Directions
Surprised by the number of domestic violence prob-
lems it saw, the team initiated plans for a women’s
health clinic and domestic violence shelter, as none
in the region allows women to stay with their children.
(The children are sent to orphanages.) The mayor is
developing a rehabilitation and education program for
alcoholics to complement this effort. The team hopes
to repeat the trip annually for Cleveland Clinic and
Case Western Reserve University students as an elective
clinical rotation. ◆
To learn more, visit http://www.lamayclinic.org/ or email [email protected].
Gynecologic Oncologist Earns Prestigious Award in China
Jerome L. Belinson, MD, professor of surgery
in Cleveland Clinic Lerner College of Medicine
and founding director of Preventive Oncology
International, recently received the esteemed
Friendship Award from the People’s Republic
of China. Chinese Vice Premier Zhang Dejiang
recognized Dr. Belinson in a ceremony during this
year’s National Day celebrations in Beijing.
The Friendship Award, established in 1991, is China’s
highest award given to a foreign expert who has made
outstanding contributions to China’s economic and
social progress.
For more than 14 years, Dr. Belinson has worked to
bring gynecologic cancer screening integrated with
clinical trials to rural China, an area of the world with
a high prevalence of female cancers. Through his efforts
and the work of his POI colleagues, almost 40,000
women who participated in the studies received screen-
ing for cervical cancer, often for the only time in their
lives. Dr. Belinson and his team have been recognized
for their careful adherence to human values and the
proper conduct of studies involving human subjects in
the Third World.
“After more than 30 years in the full-time practice of
gynecologic oncology, my work in China has been the
highlight of my professional life,” said Dr. Belinson.
“Our mission is far from done, and it is my sincere hope
that this award will draw attention to the continuing
need for support for our efforts.” ◆
clevelandclinic.org /obgyn | 800.553.5056 11
72222_CCFBCH_ACG.indd 11 11/22/10 10:30 AM

Trial Compares Traditional and Robotic-Assisted Laparoscopic Sacrocolpopexy
Cleveland Clinic Director of Urogynecology and Reconstructive Pelvic Surgery Marie Fidela Paraiso, MD, recently
reported results from the first randomized clinical trial comparing traditional laparoscopic sacrocolpopexy to robotic-
assisted laparoscopic sacrocolpopexy. The study was the largest randomized controlled study comparing the two surgical
approaches in any field to date. While the primary outcome measured was operating time from incision to closure, the
trial also addressed other operative parameters, anatomic, functional and quality-of-life outcomes.
Dr. Paraiso’s team enrolled 76 patients, 67 of whom were
randomized and underwent surgery (32 traditional, 35
robotic-assisted). Inclusion criteria included post-hysterec-
tomy vaginal apex prolapse at POPQ stages 2-4; age over 21
years; and a desire for laparoscopic surgical management.
Patients were excluded based on contraindication for general
anesthesia; history of prior sacrocolpopexy; suspicious
adnexal masses or other factors that could increase risk of
pelvic malignancy; history of pelvic inflammatory disease;
morbid obesity (BMI over 40); or history of prior or concomi-
tant need of rectopexy for rectal prolapse. There were no
differences in demographic and preoperative anatomic and
functional data between groups.
Surgical experience (analyzed per surgeon) showed that there
was no significant association between the number of cases a
surgeon performed and any of the surgical times recorded.
“Both approaches led to significant improvement in anatomic
outcome and pelvic floor function at six months,” says Dr.
Paraiso, an internationally recognized pioneer in laparo-
scopic sacrocolpopexy. “We found no differences in length
of stay, hospital pain medication requirement, or pelvic floor
six-month functional or anatomic outcomes between groups.”
However, total operating room time, anesthesia time, total
procedure time, total sacrocolpopexy time and total sutur-
ing time were all significantly longer in the robotic-assisted
group. Similarly, the robotic group reported significantly
higher pain scale scores at rest and with activity during weeks
three through six after surgery and required non-steroidal
anti-inflammatory drugs longer (19.5 vs. 9.5 days).
Dr. Paraiso says that although robotic surgery greatly
improves surgeon dexterity and ergonomics and has enabled
surgeons to overcome some of the limitations of conventional
laparoscopy, this study provides valuable insight regarding
future application of the technology.
“One of the barriers to widespread adoption of robotics is the
lack of high-quality data such as this. Certainly, insurance
companies are asking for this kind of quantifiable data to
determine reimbursement,” she says. Her team currently is
engaged in a similar study of conventional vs. robotic-assisted
laparoscopic hysterectomy with Brigham and Women’s
Hospital in Boston. ◆
Dr. Paraiso specializes in laparoscopic surgery, vaginal reconstructive surgery, prolapse and incontinence in the Ob/Gyn & Women’s Health Institute and the Glickman Urological & Kidney Institute. Physicians may contact her at 216.444.3428 or [email protected].
Laparoscopic vental rectopexy with sacral colpoperineopexy
12 ClevelanD CliniC Ob/Gyn & WOMen’S HealTH PeRSPeCTiveS | WinTeR 2010
72222_CCFBCH_ACG.indd 12 11/29/10 12:17 PM

Selected Publications From Cleveland Clinic’s Ob/Gyn & Women’s Health Institute
Journal Publications
Abdelhafez FF, Desai N, Abou-Setta AM, Fal-cone T, Goldfarb J. Slow freezing, vitrification and ultra-rapid freezing of human embryos: a systematic review and meta-analysis. Reprod Biomed Online. 2010 Feb;20(2):209-222.
Aft R, Naughton M, Trinkaus K, Watson M, ylagan L, Chavez-MacGregor M, Zhai J, Kuo S, Shannon W, Diemer K, Herrmann V, Dietz J, Ali A, Ellis M, Weiss P, Eberlein T, Ma C, Fracasso PM, Zoberi I, Taylor M, Gillanders W, Pluard T, Mortimer J, Weilbaecher K. Effect of zoledronic acid on disseminated tumour cells in women with locally advanced breast cancer: an open label, randomised, phase 2 trial. Lancet Oncol. 2010 May;11(5):421-428.
Belinson JL, Hu S, Niyazi M, Pretorius RG, Wang H, Wen C, Smith JS, Li J, Taddeo FJ, Burchette RJ, Qiao yL. Prevalence of type-specific human papillomavirus in endocervical, upper and lower vaginal, perineal and vaginal self-collected specimens: Implications for vaginal self-collection. Int J Cancer. 2010 Sep 1;127(5):1151-1157.
Bradley CS, Rahn DD, Nygaard IE, Barber MD, Nager CW, Kenton KS, Siddiqui Ny, Abel RB, Spino C, Richter HE. The questionnaire for urinary incontinence diagnosis (QUID): valid-ity and responsiveness to change in women undergoing non-surgical therapies for treatment of stress predominant urinary incontinence. Neurourol Urodyn. 2010 Jun;29(5):727-734.
Chen CCG, Korn A, Klingele C, Barber MD, Paraiso MFR, Walters MD, Jelovsek JE. Objec-tive assessment of vaginal surgical skills. Am J Obstet Gynecol. 2010 Jul;203(1):79.e1-79.e8.
Desai N, AbdelHafez F, Drazba J, Goldfarb J, Falcone T. A simple and efficient method for preparation of isolated ovarian follicles for transmission electron microscopy. J Assist Reprod Genet. 2010 Feb;27(2-3):97-101.
Desai N, Sabanegh E Jr, Kim T, Agarwal A. Free radical theory of aging: implications in male infertility. Urology. 2010 Jan;75(1):14-19.
Diwadkar GB, Jelovsek JE. Measuring surgical trainee perceptions to assess the operating room educational environment. J Surg Educ. 2010 Jul-Aug;67(4):210-216.
du Plessis SS, Cabler S, McAlister DA, Sa-banegh E, Agarwal A. The effect of obesity on sperm disorders and male infertility. Nat Rev Urol. 2010 Mar;7(3):153-161.
du Plessis SS, McAllister DA, Luu A, Savia J, Agarwal A, Lampiao F. Effects of H(2)O(2) exposure on human sperm motility parameters, reactive oxygen species levels and nitric oxide levels. Andrologia. 2010 Jun;42(3):206-210.
Escobar PF, Bedaiwy MA, Fader AN, Falcone T. Laparoendoscopic single-site (LESS) surgery in patients with benign adnexal disease. Fertil Steril. 2010 Apr;93(6):2074.e7-2074.e10.
Escobar PF, Starks DC, Fader AN, Barber M, Rojas-Espalliat L. Single-port risk-reducing salpingo-oophorectomy with and without hysterectomy: surgical outcomes and learn-ing curve analysis. Gynecol Oncol. 2010 Oct;119(1):43-47.
Fader AN, Cohen S, Escobar PF, Gunderson C. Laparoendoscopic single-site surgery in gynecology. Curr Opin Obstet Gynecol. 2010 Aug;22(4):331-338.
Falcone T. Adnexal masses: when to observe, when to intervene, and when to refer. Obstet Gynecol. 2010 Apr;115(4):680-681.
Farley J, Rose PG. Trial design for evaluation of novel targeted therapies. Gynecol Oncol. 2010 Feb;116(2):173-176.
Firoozi F, Ingber MS, Goldman HB. Pure trans-vaginal removal of eroded mesh and retained foreign body in the bladder. Int Urogynecol J Pelvic Floor Dysfunct. 2010 Jun;21(6):757-760.
Firoozi F, Goldman HB. Transvaginal excision of mesh erosion involving the bladder after mesh placement using a prolapse kit: a novel tech-nique. Urology. 2010 Jan;75(1):203-206.
French DB, Sabanegh ES, Jr., Goldfarb J, Desai N. Does severe teratozoospermia affect blastocyst formation, live birth rate, and other clinical outcome parameters in ICSI cycles? Fertil Steril. 2010 Mar 1;93(4):1097-1103.
Frick AC, Walters MD, Larkin KS, Barber MD. Risk of unanticipated abnormal gynecologic pathology at the time of hysterectomy for uterovaginal prolapse. Am J Obstet Gynecol. 2010 May;202(5):507.e1-507.e4.
Gill BC, Moore C, Damaser MS. Postpartum stress urinary incontinence: Lessons from ani-mal models. Expert Rev Obstet Gynecol. 2010 Sep;5(5):567-580.
Gill IS, Advincula AP, Aron M, Caddedu J, Canes D, Curcillo PG, II, Desai MM, Evanko JC, Falcone T, Fazio V, Gettman M, Gumbs AA, Haber GP, Kaouk JH, Kim F, King SA, Ponsky J, Remzi F, Rivas H, Rosemurgy A, Ross S, Schauer P, Sotelo R, Speranza J, Sweeney J, Teixeira J. Consensus statement of the consor-tium for laparoendoscopic single-site surgery. Surg Endosc. 2010 Apr;24(4):762-768.
Kader A, Choi A, Sharma RK, Falcone T, Agarwal A. Effect of varying equilibration time in a two-step vitrification method on the post-warming DNA integrity of mouse blastocysts. Fertil Steril. 2010 May 15;93(8):2640-2645.
Kader A, Falcone T, Sharma RK, Mangrola D, Agarwal A. Slow and ultrarapid cryopreserva-tion of biopsied mouse blastocysts and its effect on DNA integrity index. J Assist Reprod Genet. 2010 Aug;27(8):509-515.
Kader A, Sharma RK, Falcone T, Agarwal A. Mouse blastocyst previtrification interventions and DNA integrity. Fertil Steril. 2010 Mar 15;93(5):1518-1525.
Liu Z, Belinson SE, Li J, yang B, Wulan N, Tresser NJ, Wang C, Mohr M, Zhang L, Zhou y, Weng L, Wu R, Belinson JL. Diagnostic effi-cacy of real-time optical coherence tomography in the management of preinvasive and invasive neoplasia of the uterine cervix. Int J Gynecol Cancer. 2010 Feb;20(2):283-287.
Mahfouz RZ, du Plessis SS, Aziz N, Sharma R, Sabanegh E, Agarwal A. Sperm viability, apop-tosis, and intracellular reactive oxygen species levels in human spermatozoa before and after induction of oxidative stress. Fertil Steril. 2010 Feb;93(3):814-821.
Moore HCF, Budd GT, Sikon A, Rim A, Chell-man-Jeffers M, Crowe J. Sorting through the recent controversies in breast cancer screening. Cleve Clin J Med. 2010 Feb;77(2):76-79.
Muffly TM, Boyce J, Kieweg SL, Bon-ham AJ. Tensile strength of a surgeon's or a square knot. J Surg Educ. 2010 Jul-Aug;67(4):222-226.
13clevelandclinic.org /obgyn | 800.553.5056
72222_CCFBCH_ACG.indd 13 11/15/10 2:40 PM

Selected Publications From Cleveland Clinic’s Ob/Gyn & Women’s Health Institutecontinued
Muffly TM, Barber MD. Insertion and removal of vaginal mesh for pelvic organ prolapse. Clin Obstet Gynecol. 2010 Mar;53(1):99-114.
Muffly TM, Penick ER, Tang F, Bonham AJ, Smith RP, Hill RFC, Blandon RE. Factors used by female pelvic medicine and reconstructive surgery fellowship directors to select their fel-lows. Int Urogynecol J Pelvic Floor Dysfunct. 2010 Mar;21(3):349-352.
Mukhopadhyay D, Varghese AC, Pal M, Baner-jee SK, Bhattacharyya AK, Sharma RK, Agarw-al A. Semen quality and age-specific changes: a study between two decades on 3,729 male partners of couples with normal sperm count and attending an andrology laboratory for infertility-related problems in an Indian city. Fertil Steril. 2010 May 1;93(7):2247-2254.
Novara G, Artibani W, Barber MD, Chapple CR, Costantini E, Ficarra V, Hilton P, Nilsson CG, Waltregny D. Updated systematic review and meta-analysis of the comparative data on colposuspensions, pubovaginal slings, and midurethral tapes in the surgical treatment of female stress urinary incontinence. Eur Urol. 2010 Aug;58(2):218-238.
O'Flynn O'Brien KL, Varghese AC, Agarwal A. The genetic causes of male factor infertility: a review. Fertil Steril. 2010 Jan;93(1):1-12.
Park AJ, Barber MD, Bent AE, Dooley yT, Dancz C, Sutkin G, Jelovsek JE. Assessment of intraoperative judgment during gynecologic surgery using the Script Concordance Test. Am J Obstet Gynecol. 2010 Sep;203(3):240-246.
Powell MA, Filiaci VL, Rose PG, Mannel RS, Hanjani P, Degeest K, Miller BE, Susumu N, Ueland FR. Phase II evaluation of pa-clitaxel and carboplatin in the treatment of carcinosarcoma of the uterus: a Gynecologic Oncology Group study. J Clin Oncol. 2010 Jun 1;28(16):2727-2731.
Ragheb AM, Sabanegh ES, Jr. Male fertility-implications of anticancer treatment and strate-gies to mitigate gonadotoxicity. Anticancer Agents Med Chem. 2010 Jan 1;10(1):92-102.
Richter HE, Burgio KL, Brubaker L, Nygaard IE, ye W, Weidner A, Bradley CS, Handa VL, Borel-lo-France D, Goode PS, Zyczynski H, Lukacz ES, Schaffer J, Barber M, Meikle S, Spino C. Continence pessary compared with behavioral therapy or combined therapy for stress incon-tinence: a randomized controlled trial. Obstet Gynecol. 2010 Mar;115(3):609-617.
Rose PG, Ali S, Whitney CW, Lanciano R, Stehman FB. Impact of hydronephrosis on outcome of stage IIIB cervical cancer patients with disease limited to the pelvis, treated with radiation and concurrent chemotherapy: a Gynecologic Oncology Group study. Gynecol Oncol. 2010 May;117(2):270-275.
Rose PG, Tian C, Bookman MA. Assessment of tumor response as a surrogate endpoint of survival in recurrent/platinum-resistant ovarian carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2010 May;117(2):324-329.
Sajadi KP, Goldman HB. Percutaneous tibial nerve stimulation and overactive bladder. Curr Urol Rep. 2010 Sep;11(5):293-295.
Samplaski MK, Agarwal A, Sharma R, Sa-banegh E. New generation of diagnostic tests for infertility: review of specialized semen tests. Int J Urol. 2010 Oct;17(10):839-847.
Sikon A, Batur P. Profile of teriparatide in the management of postmenopausal osteoporosis. Int J Women Health. 2010;2(1):37-44.
Sikon A, Bronson DL. Shared medical ap-pointments: challenges and opportunities. Ann Intern Med. 2010 Jun 1;152(11):745-746.
Siraj ES, Abacan C, Chinnappa P, Wojtowicz J, Braun W. Risk factors and outcomes associated with posttransplant diabetes mellitus in kidney transplant recipients. Transplant Proc. 2010 Jun;42(5):1685-1689.
Skaznik-Wikiel ME, Jelovsek JE, Andrews B, Bradley LD. Accuracy of endometrial thickness in detecting benign endometrial pathology in postmenopausal women. Menopause. 2010 Jan;17(1):104-108.
Staskin D, Kay G, Tannenbaum C, Goldman HB, Bhashi K, Ling J, Oefelein MG. Trospium chloride has no effect on memory testing and is assay undetectable in the central nervous sys-tem of older patients with overactive bladder. Int J Clin Pract. 2010 Aug;64(9):1294-1300.
Swartz M, Vasavada S, Goldman H. Reply [Perioperative management of patients under-going sling surgery: A survey of US urologists]. Urology. 2010 Aug;76(2):318.
Swartz M, Ching C, Gill B, Li J, Rackley R, Va-savada S, Goldman HB. Reply [Risk of infection after midurethral synthetic sling surgery: are postoperative antibiotics necessary?]. Urology. 2010 Jun;75(6):1309.
Swartz M, Ching C, Gill B, Li J, Rackley R, Vasavada S, Goldman HB. Risk of infection after midurethral synthetic sling surgery: are postoperative antibiotics necessary? Urology. 2010 Jun;75(6):1305-1308.
Swartz M, Vasavada S, Goldman H. Periopera-tive management of patients undergoing sling surgery: a survey of US urologists. Urology. 2010 Aug;76(2):314-317.
von Gruenigen VE, Huang HQ, Gil KM, Gib-bons HE, Monk BJ, Rose PG, Armstrong DK, Cella D, Wenzel L. A comparison of quality-of-life domains and clinical factors in ovarian cancer patients: a Gynecologic Oncology Group study. J Pain Symptom Manage. 2010 May;39(5):839-846.
Wang C, Michener CM, Belinson JL, Vaziri S, Ganapathi R, Sengupta S. Role of the 18:1 lysophosphatidic acid-ovarian cancer immunoreactive antigen domain containing 1 (OCIAD1)-integrin axis in generating late-stage ovarian cancer. Mol Cancer Ther. 2010 Jun;9(6):1709-1718.
Wulan N, Rasool N, Belinson SE, Wang C, Rong X, Zhang W, Zhu y, yang B, Tresser NJ, Mohr M, Wu R, Belinson JL. Study of the diag-nostic efficacy of real-time optical coherence tomography as an adjunct to unaided visual inspection with acetic acid for the diagnosis of preinvasive and invasive neoplasia of the uterine cervix. Int J Gynecol Cancer. 2010 Apr;20(3):422-427.
Books
Falcone T, Goldberg JM. Basic, Advanced, and Robotic Laparoscopic Surgery. Philadelphia, PA: Saunders/Elsevier, 2010.
Le T, Bhushan V, Sheikh-Ali M, Abu Shahin F. First Aid for the USMLE Step 2 CS. 3rd ed. New york, Ny: McGraw-Hill, 2010.
Walters MD, Barber MD. Hysterectomy for Benign Disease. Philadelphia, PA: Saunders Elsevier, 2010.
14 CLEVELAND CLINIC OB/GyN & WOMEN’S HEALTH PERSPECTIVES | WINTER 2010
72222_CCFBCH_ACG.indd 14 11/15/10 2:40 PM

Physician Resources
Medical editor Majan Attaran, MD
Managing editorMarjie Heines
Art DirectorAnne Drago
PhotographersDon Gerda, Russell Lee, Tom Merce, Steve Travarca
IllustrationJoe Pangrace, Mark Sabo
Marketing Lori Schmitt, RN, Melissa Raines
Ob/Gyn & Women’s Health Perspectives is written for physicians and should be relied upon for medical education purposes only. It does not provide a complete overview of the topics covered, and should not replace the independent judgment of a physician about the appropriateness or risks of a procedure for a given patient.
© The Cleveland Clinic Foundation 2010
PHysICIAn DIReCtORy View all Cleveland Clinic staff online at
clevelandclinic.org/staff. To request a printed version of the Ob/Gyn directory,
call Susan Anton at 216.448.1020.
CRItICAl CARe tRAnsPORt WORlDWIDe Cleveland Clinic’s critical care
transport team serves critically ill and highly complex patients around the globe.
Critical care transport is available for children and adults.
To arrange a transfer for STEMI (ST elevated myocardial infarction), acute stroke,
ICH (intracerebral hemorrhage), SAH (subarachnoid hemorrhage) or aortic
syndromes, call 877.379.CODE (2633). For all other critical care transfers,
call 216.444.8302 or 800.553.5056.
IMPROveD COMMUnICAtIOn, IMPROveD CARe DrConnect offers secure
access to your patient’s treatment progress at Cleveland Clinic. To establish a
DrConnect account, visit clevelandclinic.org/drconnect or email [email protected].
ReMOte COnsUlts Request a remote medical second opinion from
Cleveland Clinic. MyConsult is particularly valuable for patients who wish to
avoid the time and expense of travel. Visit clevelandclinic.org/myconsult, email
[email protected] or call 800.223.2273, ext. 43223.
OUtCOMes DAtA AvAIlABle Our Outcomes books contain clinical outcomes
data and information on volumes, innovations, research and publications.
To view Outcomes books for many Cleveland Clinic institutes, visit
clevelandclinic.org/quality/outcomes.
General Patient Referral
24/7 hospital transfers or physician consults
800.553.5056
Obstetrics & Gynecology
Appointments/Referrals
216.444.6601 or 800.223.2273, ext. 46601
On the Web at
clevelandclinic.org/obgyn
stay Connected to Cleveland Clinic
Health Care Quality Innovation SummitOptimizing value and securing a Future of Innovation and Quality
May 11–13, 2011
InterContinental Hotel and Bank of
America Conference Center,
Cleveland, Ohio
ReGIsteR tODAy! www.ccfcme.org/Quality11
15clevelandclinic.org /obgyn | 800.553.5056
72222_CCFBCH_ACG.indd 15 11/15/10 2:40 PM

The Cleveland Clinic Foundation 9500 Euclid Avenue / AC311 Cleveland, Ohio 44195
10-OBG-008
New!
Healthcare Executive Education Programs
“I encourage you to join us for this unique educational opportunity. you will emerge enlightened, invigorated and ready to meet the business challenges of our time.”
– Delos M. “toby” Cosgrove, MD, CeO and President, Cleveland Clinic
Cleveland Clinic is launching two healthcare executive education programs that focus on the challenges of leadership, management and innovation in today’s highly competitive healthcare landscape.
“One of the unique aspects of our executive education programs
is peer learning. Attendees will learn directly from those involved
in the daily business of healthcare excellence,” says James K.
Stoller, MD, MS, a pulmonologist and critical care medicine
physician and Chairman of Cleveland Clinic’s Education Institute.
The Executive Visitors’ Program is an intensive two-day program,
designed for busy executives. The Samson Global Leadership
Academy is a two-week immersion program that offers, among
other things, a mentoring opportunity that continues after the
program is over.
The programs are open to healthcare executives, including
physicians, nurses and administrators. CME credit is available.
to learn more, visit clevelandclinic.org/executiveeducation.
16
CLEVELAND CLINIC OB/GyN & WOMEN’S HEALTH PERSPECTIVES | WINTER 2010 clevelandclinic.org /obgyn
72222_CCFBCH_ACG.indd 16 11/15/10 2:40 PM