Embed Size (px)
Citation preview

Journal of Cardiac Failure Vol. 18 No. 11 2012
Obesity and the Response to Intensified Diuretic Treatmentin Decompensated Heart Failure: A DOSE Trial Substudy
ACHAL GUPTA, MD,1 EUGENE BRAUNWALD, MD,2 STEVEN MCNULTY, MS,4 G. MICHAEL FELKER, MD,6
E. MICHAEL GILBERT, MD,1 RAMI ALHARETHI, MD,3 KERRY L. LEE, PhD,4 KEVIN J. ANSTROM, PhD,4
MARGARET M. REDFIELD, MD,5 STEVEN R. GOLDSMITH, MD,7 CHRISTOPHER M. O’CONNOR, MD,6 DAVID A. BULL, MD,1,8
JOSEF STEHLIK, MD, MPH,1,8 AND SHELDON E. LITWIN, MD1,8,9
Salt Lake City, Utah; Boston, Massachusetts; Durham, North Carolina; Rochester and Minneapolis, Minnesota; and Augusta, Georgia
From the 1DiviUtah; 2Division opital, Harvard Mediology, IntermouCoordinating CenCarolina; 5Divisio6Division of CardiCarolina; 7UniverCardiology, Salt LUtah and 9DivisioAugusta, Georgia.
ABSTRACT
Background: Obesity could attenuate diuretic effectiveness in treatment of acute decompensated heartfailure (HF).Methods and Results: The DOSE trial randomized 308 subjects with acute HF to low- versus high-intensification intravenous diuretic therapy. We tested for statistical interactions between obesity and dos-ing strategy across clinical end points. After 72 hours of treatment, obese subjects (body mass index O30kg/m2; n 5 173) had greater volume loss than nonobese subjects (n 5 119) but similar improvements indyspnea and freedom from congestion. Both groups had greater fluid loss with high-intensification treat-ment. Obese subjects had a higher incidence of worsening renal function (WRF) at 72 hours with low-intensification treatment, compared with nonobese subjects. In contrast, nonobese and obese subjectshad similar incidence of WRF with high-intensification treatment. There were no differences betweenobese and nonobese subjects in time to discharge and 60-day freedom from death, emergency departmentvisit, or rehospitalization.Conclusions: The incidence of WRF was greater in obese than in nonobese subjects with low-intensification treatment. However, the frequency of WRF was equivalent in obese and nonobese subjectswith high-intensification treatment. Additional studies are needed to assess whether obese patients withacute HF benefit from an initial high-intensification treatment strategy. (J Cardiac Fail 2012;18:837e844)Key Words: Obesity, congestive heart failure, diuretics, renal function, readmission.
The prevalence of obesity in most developed countrieshas approximately doubled over the past 2 decades.1,2 Obe-sity is a risk factor for the development of heart failure(HF).3,4 Mechanisms accounting for the association be-tween obesity and HF likely include premature and acceler-ated coronary atherosclerosis,5,6 hypertension,7,8 diabetes,9
sleep-disordered breathing, and atrial fibrillation.10 Ina large registry of patients with acute decompensated HF,38% of the patients were obese based on World Health Or-ganization criteria.11 Despite the very frequent coexistence
sion of Cardiology, University of Utah, Salt Lake City,f Cardiovascular Medicine, Brigham and Women’s Hos-dical School, Boston, Massachusetts; 3Division of Car-ntain Medical Center, Salt Lake City, Utah; 4Datater, Duke Clinical Research Institute, Durham, Northn of Cardiology, Mayo Clinic, Rochester, Minnesota;ology, Duke University Medical Center, Durham, Northsity of Minnesota, Minneapolis, Minnesota; 8Division ofake City Veterans Affairs Medical Center, Salt Lake City,n of Cardiology, Georgia Health Sciences University,
837
of these conditions, it is unknown whether the treatment forHF should be altered based on the presence of obesity.
Intravenous loop diuretics are the most commonly usedpharmacologic agents in the treatment of acute HF becauseof their rapid action in alleviating volume overload andconsequent symptoms. Some retrospective studies havesuggested that higher doses of diuretics are associatedwith harm,12,13 but the optimal dosing of intravenous loopdiuretics has not been rigorously studied. Despite uncertainclinical significance, it is common practice to stop or
Manuscript received May 9, 2012; revised manuscript received August8, 2012; revised manuscript accepted September 21, 2012.Reprint requests: Josef Stehlik, MD, University of Utah Health Sciences
Center, Division of Cardiology, 50 North Medical Drive, 4A100 SOM, SaltLake City, UT 84132. Tel: þ1 801 585 2340; Fax: þ1 801 581 7735.E-mail: [email protected]: National Heart, Lung, and Blood Institute.Drs. Litwin and Stehlik are coesenior authors.See page 843 for disclosure information.1071-9164/$ - see front matterPublished by Elsevier Inc.http://dx.doi.org/10.1016/j.cardfail.2012.09.005

838 Journal of Cardiac Failure Vol. 18 No. 11 November 2012
reduce the dosage of diuretics in the setting of worseningrenal function. There are theoretical reasons why obesitymight attenuate the response to intravenous diuretics or ex-acerbate worsening renal function during diuretic treat-ment: 1) Obese patients often have higher lean body massas well as fat mass, and therefore may have larger volumeof distribution of drugs14; 2) obese patients often haveincreased intra-abdominal pressure and/or increased renalvein pressure and therefore may have greater resistance toglomerular filtration15; and 3) obesity has been associatedwith a 3e4-fold increased lifetime risk of developingchronic renal failure, not all of which is attributable to di-abetic nephropathy.16e19 Few trials have directly examinedwhether obese subjects respond differently to treatment ofacute HF compared with nonobese subjects.
The Diuretic Optimization Strategies Evaluation (DOSE)trial showed that among subjects with acute decompensatedHF, there were no significant differences in subjects’ globalassessment of symptoms or in the change in renal functionwhen intravenous diuretic therapy was administeredwith the use of high- versus low-intensification strategy orwith bolus versus continuous infusion dosing.20 We testedthe hypothesis that obese subjects would require high-intensification diuretic treatment to achieve adequate volumeloss and symptomatic improvement, whereas nonobese sub-jects would improve in both the high- and low-intensificationtreatment arms. For the reasons described above, we also hy-pothesized that high-intensification diuretic treatment wouldbe associated with moreworsening of renal function in obesecompared with nonobese subjects.
Methods
The DOSE study design and primary outcomes have been re-ported previously.21 The study was conducted by a National Heart,Lung, and Blood Instituteefunded Heart Failure Clinical ResearchNetwork. Each of the subjects provided written informed consent.The trial was registered at ClinicalTrials.gov under number:NCT00577135.
Study Participants
Patients with history of chronic HF were eligible for enrollmentinto the trial if they were within 24 hours of hospital admissionwith acute decompensated HF.
Randomization and Treatment Assignments
Subjects were randomized to either a low-intensification strat-egy (total daily intravenous dose of 1.0� their daily oral furose-mide dose) or high-intensification strategy (a total dailyintravenous dose of 2.5� their daily oral dose) and to dosing eitherby intravenous bolus every 12 hours or by continuous intravenousinfusion. Because the main trial did not show differences betweencontinuous and intermittent dosing, in the present analysis we fo-cused only on high-intensification versus low-intensification di-uretic treatment. Blinded study treatment was continued for upto 72 hours, and subjects were followed for clinical events to60 days. All patients were recommended to receive standard HFmedications and a low-salt diet with fluid restriction.
End Points
The end points of this substudy were similar to those of themain DOSE trial. The primary efficacy end point was subject-reported global assessment of symptoms assessed with the useof a visual analog scale and quantified as the area under the curvefrom baseline to 72 hours. The primary safety end point was thechange in serum creatinine from baseline to 72 hours. Secondaryend points included: 1) subject-reported dyspnea; 2) changes innet fluid loss and body weight; 3) proportion of subjects freefrom congestion; 4) worsening renal function defined as an in-crease in serum creatinine of O0.3 mg/dL at any time from ran-domization to 72 hours; 5) worsening or persistent HF definedas the need for additional therapy between randomization and72 hours; 6) changes in cystatin C and N-terminal proeB-type na-triuretic peptide (NT-proBNP); and 7) composite of death, reho-spitalization, or emergency room visit within 60 days.
Statistical Analysis
All comparisons involving the different diuretic treatment strat-egies were based on ‘‘intention to treat.’’ Continuous variables arepresented as mean and standard deviation (SD) or median and in-terquartile range (IQR), and categoric variables are presented asfrequencies and percentages. The baseline characteristics of sub-ject groups defined by presence or absence of obesity were com-pared with the use of the Wilcoxon rank-sum test for continuousvariables and the chi-square test for categoric variables. The ef-fects of high-intensity diuretics and obesity regarding the primaryand secondary end points were estimated and assessed with theuse of a general linear model (continuous end points), logistic re-gression (binary end points), or Cox model and Kaplan-Meiercurves (event-time end points) as appropriate. A test for the pres-ence of an interaction between the treatment strategy and presenceof obesity was also performed within the statistical modelingframework appropriate for each individual end point, includingwhether the interaction was independent from other relevant clin-ical factors. Differences between groups were considered to bestatistically significant if the 2-sided P value was !.05.
Results
Subject Characteristics
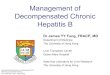
The DOSE study enrolled 308 subjects from March 2008to November 2009. Two hundred ninety-two subjectshad data available to calculate body mass index (BMI).Median BMI in subjects enrolled in the DOSE study was31.9 kg/m2 (IQR 25.6e34.7), and 59% of the subjectsmet World Health Organization criteria for obesity (BMIO30 kg/m2) at enrollment. Baseline characteristics forobese (median BMI 35.5 [IQR 32.8e40.6] kg/m2 and me-dian weight 236 [IQR 210e268] lb) and nonobese (medianBMI 25.7 [IQR 24.1e27.9] kg/m2 and median weight171 [151e190] lb) subjects are provided in Table 1. Obesesubjects were younger than nonobese subjects (median age66 vs 72 years; P ! .01). Obese and nonobese subjectshad similar sex distribution, etiology of HF, qualifying fu-rosemide dosage, number of HF hospitalizations in thepast 12 months, history of atrial fibrillation, and baselineserum creatinine. Obese subjects had a higher median leftventricular EF (31.5% [IQR 20%e55%] vs 25.0% [IQR
Table 1. Baseline Demographics and Clinical Characteristics
BMI O30 kg/m2 (n 5 173) BMI #30 kg/m2 (n 5 119) P Value
DemographicsAge !.01
Median (IQR) 66.0 (54.0e75.0) 72.0 (62.0e80.0)Mean 6 SD 64.3 6 13.5 69.7 6 13.1
White race 126 (72.8%) 94 (79.0%) .23Male 123 (71.1%) 89 (74.8%) .49Qualifying furosemide dose .64
Median (IQR) 120.0 (80.0e160.0) 120.0 (80.0e160.0)Mean 6 SD 132.3 6 52.4 128.9 6 51.3
HF hospitalization within 12 mo before randomization 130 (76.5%) 81 (68.1%) .11LVEF*
Median (IQR) 31.5 (20.0e55.0) 25.0 (20.0e45.0) .03Mean 6 SD 36.6 6 17.9 32.5 6 16.7$50% 52 (31.0%) 27 (22.9%) .13
Medical historyIschemic etiology 95 (54.9%) 77 (64.7%) .09Diabetes mellitus 106 (61.3%) 45 (37.8%) !.01Atrial fibrillation/flutter 90 (52.0%) 69 (58.0%) .31
Baseline medicationsACE or ARB 111 (64.2%) 72 (60.5%) .53Aldosterone antagonists 46 (26.6%) 38 (31.9%) .32Beta-blockers 143 (82.7%) 99 (83.2%) .91
Physical and laboratory findingsSystolic blood pressure !.01
Median (IQR) 119.0 (106.0e135.0) 112.0 (101.0e128.0)Mean 6 SD 121.3 6 20.7 114.2 6 16.6
Heart rate* .65Median (IQR) 76.0 (67.0e86.0) 76.0 (70.0e84.0)Mean 6 SD 78.3 6 17.2 78.3 6 13.5
Rales* 100 (58.1%) 69 (58.5%) .95JVP $8 cm* 147 (91.3%) 108 (93.1%) .58SPO2 (%)* .51
Median (IQR) 96.0 (94.0e98.0) 96.0 (94.0e99.0)Mean 6 SD 95.9 6 3.0 96.1 6 3.0
Serum creatinine (mg/dL) .95Median (IQR) 1.40 (1.11e1.82) 1.44 (1.08e1.85)Mean 6 SD 1.49 6 0.50 1.50 6 0.55
Serum cystatin C (mg/L) .53Median (IQR) 1.51 (1.16, 1.92) 1.45 (1.08, 1.89)Mean 6 SD 1.58 (0.56) 1.54 6 0.56
Sodium (mEq/L) !.01Median (IQR) 139.0 (137.0e141.0) 138.0 (135.0e140.0)Mean 6 SD 138.7 6 3.9 137.6 6 3.4
NT-proBNP (pg/mL)* !.01Median (IQR) 3,404.0 (2,005.0e6,929.0) 7,491.5 (4,190.0e14,374.0)Mean 6 SD 5,630.3 6 6,479.4 10,135.0 6 7,898.0
IQR, interquartile range; HF, heart failure; LVEF, left ventricular ejection fraction; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensinreceptor blocker; JVP, jugular venous pressure; NT-proBNP, N-terminal proeB-type natriuretic peptide.P values for continuous variables are based on Wilcoxon rank-sum test. P values for categoric variables are based on chi-square test.*Small number of responses missing; percentages are based on total known responses.
Obesity and Response to Diuretics � Gupta et al 839
20%e45%]; P5 .03). However, the proportions of subjectswith an ejection fraction $50% were not significantly dif-ferent between the 2 groups (31% vs 23%; P 5 .13). Therewas a significantly higher proportion of subjects with diabe-tes in the obese compared with the nonobese cohort (61 vs38%; P! .01). There was no difference in the use of essen-tial HF medications in obese vs nonobese subjects at enroll-ment. Although within the normal range in both groups,the median systolic blood pressure was higher in obesesubjects (median 119 [IQR 106e135] mm Hg vs 112[IQR 101e128] mm Hg; P ! .01). Admission medianNT-proBNP was significantly lower in obese than nonobesesubjects (median 3,404 [IQR 2,005e6,929] ng/mL vs 7,492[IQR 4,190e14,374] ng/mL; P ! .01).
Study Drug Administration and Randomization
The median time from presentation to randomization(14.3 h vs 15.5 h; P 5 .80), duration of study drug admin-istration (67.7 h vs 60.5 h; P 5 .10), and change in drugstrategy at 48 hours (57% vs 63%; P 5 .31) were similarin obese and nonobese subjects. The proportions of sub-jects randomized to high-intensification strategy amongobese and nonobese subjects were similar (49% vs 52%;P 5 .58).
Primary End Points
Obese subjects were not statistically different from non-obese subjects regarding overall symptoms at 72 hours as
840 Journal of Cardiac Failure Vol. 18 No. 11 November 2012
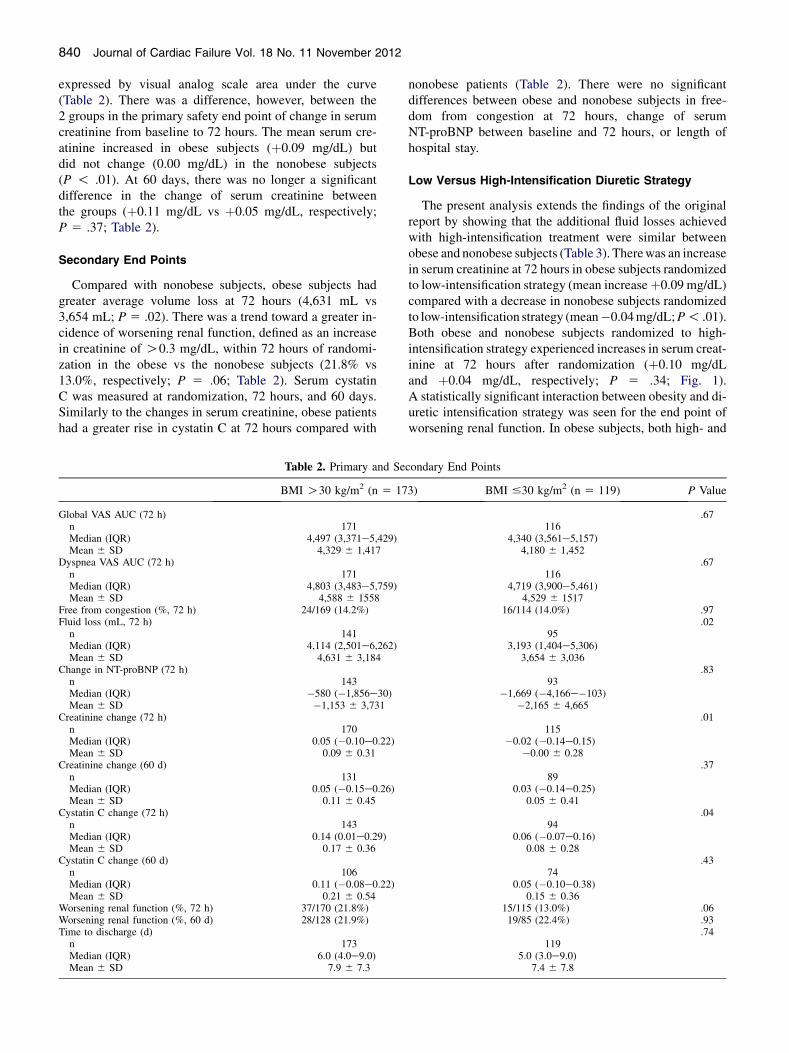
expressed by visual analog scale area under the curve(Table 2). There was a difference, however, between the2 groups in the primary safety end point of change in serumcreatinine from baseline to 72 hours. The mean serum cre-atinine increased in obese subjects (þ0.09 mg/dL) butdid not change (0.00 mg/dL) in the nonobese subjects(P ! .01). At 60 days, there was no longer a significantdifference in the change of serum creatinine betweenthe groups (þ0.11 mg/dL vs þ0.05 mg/dL, respectively;P 5 .37; Table 2).
Secondary End Points
Compared with nonobese subjects, obese subjects hadgreater average volume loss at 72 hours (4,631 mL vs3,654 mL; P 5 .02). There was a trend toward a greater in-cidence of worsening renal function, defined as an increasein creatinine of O0.3 mg/dL, within 72 hours of randomi-zation in the obese vs the nonobese subjects (21.8% vs13.0%, respectively; P 5 .06; Table 2). Serum cystatinC was measured at randomization, 72 hours, and 60 days.Similarly to the changes in serum creatinine, obese patientshad a greater rise in cystatin C at 72 hours compared with
Table 2. Primary and Se
BMI O30 kg/m2 (n 5 17
Global VAS AUC (72 h)n 171Median (IQR) 4,497 (3,371e5,429)Mean 6 SD 4,329 6 1,417
Dyspnea VAS AUC (72 h)n 171Median (IQR) 4,803 (3,483e5,759)Mean 6 SD 4,588 6 1558
Free from congestion (%, 72 h) 24/169 (14.2%)Fluid loss (mL, 72 h)
n 141Median (IQR) 4,114 (2,501e6,262)Mean 6 SD 4,631 6 3,184
Change in NT-proBNP (72 h)n 143Median (IQR) �580 (�1,856e30)Mean 6 SD �1,153 6 3,731
Creatinine change (72 h)n 170Median (IQR) 0.05 (�0.10e0.22)Mean 6 SD 0.09 6 0.31
Creatinine change (60 d)n 131Median (IQR) 0.05 (�0.15e0.26)Mean 6 SD 0.11 6 0.45
Cystatin C change (72 h)n 143Median (IQR) 0.14 (0.01e0.29)Mean 6 SD 0.17 6 0.36
Cystatin C change (60 d)n 106Median (IQR) 0.11 (�0.08e0.22)Mean 6 SD 0.21 6 0.54
Worsening renal function (%, 72 h) 37/170 (21.8%)Worsening renal function (%, 60 d) 28/128 (21.9%)Time to discharge (d)
n 173Median (IQR) 6.0 (4.0e9.0)Mean 6 SD 7.9 6 7.3
nonobese patients (Table 2). There were no significantdifferences between obese and nonobese subjects in free-dom from congestion at 72 hours, change of serumNT-proBNP between baseline and 72 hours, or length ofhospital stay.
Low Versus High-Intensification Diuretic Strategy
The present analysis extends the findings of the originalreport by showing that the additional fluid losses achievedwith high-intensification treatment were similar betweenobese and nonobese subjects (Table 3). Therewas an increasein serum creatinine at 72 hours in obese subjects randomizedto low-intensification strategy (mean increaseþ0.09 mg/dL)compared with a decrease in nonobese subjects randomizedto low-intensification strategy (mean�0.04mg/dL;P! .01).Both obese and nonobese subjects randomized to high-intensification strategy experienced increases in serum creat-inine at 72 hours after randomization (þ0.10 mg/dLand þ0.04 mg/dL, respectively; P 5 .34; Fig. 1).A statistically significant interaction between obesity and di-uretic intensification strategy was seen for the end point ofworsening renal function. In obese subjects, both high- and
condary End Points
3) BMI #30 kg/m2 (n 5 119) P Value
.67116
4,340 (3,561e5,157)4,180 6 1,452
.67116
4,719 (3,900e5,461)4,529 6 1517
16/114 (14.0%) .97.02
953,193 (1,404e5,306)
3,654 6 3,036.83
93�1,669 (�4,166e�103)
�2,165 6 4,665.01
115�0.02 (�0.14e0.15)
�0.00 6 0.28.37
890.03 (�0.14e0.25)
0.05 6 0.41.04
940.06 (�0.07e0.16)
0.08 6 0.28.43
740.05 (�0.10e0.38)
0.15 6 0.3615/115 (13.0%) .0619/85 (22.4%) .93
.74119
5.0 (3.0e9.0)7.4 6 7.8
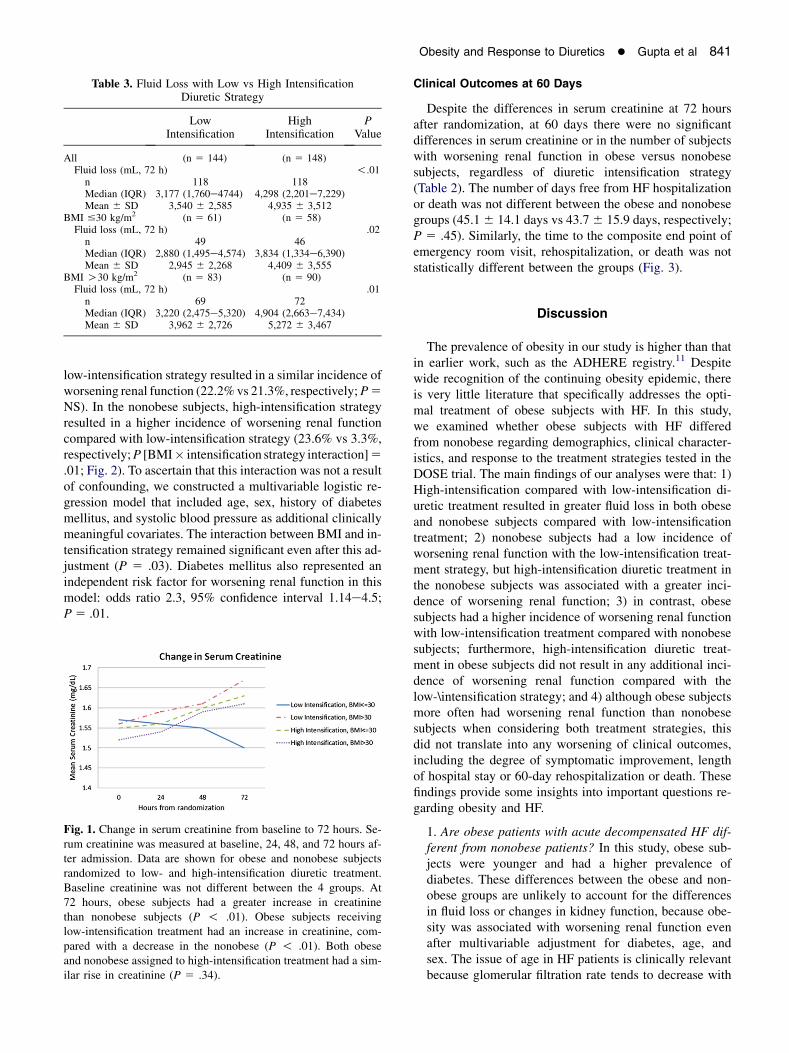
Table 3. Fluid Loss with Low vs High IntensificationDiuretic Strategy
LowIntensification
HighIntensification
PValue
All (n 5 144) (n 5 148)Fluid loss (mL, 72 h) !.01
n 118 118Median (IQR) 3,177 (1,760e4744) 4,298 (2,201e7,229)Mean 6 SD 3,540 6 2,585 4,935 6 3,512
BMI #30 kg/m2 (n 5 61) (n 5 58)Fluid loss (mL, 72 h) .02
n 49 46Median (IQR) 2,880 (1,495e4,574) 3,834 (1,334e6,390)Mean 6 SD 2,945 6 2,268 4,409 6 3,555
BMI O30 kg/m2 (n 5 83) (n 5 90)Fluid loss (mL, 72 h) .01
n 69 72Median (IQR) 3,220 (2,475e5,320) 4,904 (2,663e7,434)Mean 6 SD 3,962 6 2,726 5,272 6 3,467
Obesity and Response to Diuretics � Gupta et al 841
low-intensification strategy resulted in a similar incidence ofworsening renal function (22.2%vs 21.3%, respectively;P5NS). In the nonobese subjects, high-intensification strategyresulted in a higher incidence of worsening renal functioncompared with low-intensification strategy (23.6% vs 3.3%,respectively;P [BMI� intensification strategy interaction]5.01; Fig. 2). To ascertain that this interaction was not a resultof confounding, we constructed a multivariable logistic re-gression model that included age, sex, history of diabetesmellitus, and systolic blood pressure as additional clinicallymeaningful covariates. The interaction between BMI and in-tensification strategy remained significant even after this ad-justment (P 5 .03). Diabetes mellitus also represented anindependent risk factor for worsening renal function in thismodel: odds ratio 2.3, 95% confidence interval 1.14e4.5;P5 .01.
Fig. 1. Change in serum creatinine from baseline to 72 hours. Se-rum creatinine was measured at baseline, 24, 48, and 72 hours af-ter admission. Data are shown for obese and nonobese subjectsrandomized to low- and high-intensification diuretic treatment.Baseline creatinine was not different between the 4 groups. At72 hours, obese subjects had a greater increase in creatininethan nonobese subjects (P ! .01). Obese subjects receivinglow-intensification treatment had an increase in creatinine, com-pared with a decrease in the nonobese (P ! .01). Both obeseand nonobese assigned to high-intensification treatment had a sim-ilar rise in creatinine (P 5 .34).
Clinical Outcomes at 60 Days
Despite the differences in serum creatinine at 72 hoursafter randomization, at 60 days there were no significantdifferences in serum creatinine or in the number of subjectswith worsening renal function in obese versus nonobesesubjects, regardless of diuretic intensification strategy(Table 2). The number of days free from HF hospitalizationor death was not different between the obese and nonobesegroups (45.16 14.1 days vs 43.76 15.9 days, respectively;P 5 .45). Similarly, the time to the composite end point ofemergency room visit, rehospitalization, or death was notstatistically different between the groups (Fig. 3).
Discussion
The prevalence of obesity in our study is higher than thatin earlier work, such as the ADHERE registry.11 Despitewide recognition of the continuing obesity epidemic, thereis very little literature that specifically addresses the opti-mal treatment of obese subjects with HF. In this study,we examined whether obese subjects with HF differedfrom nonobese regarding demographics, clinical character-istics, and response to the treatment strategies tested in theDOSE trial. The main findings of our analyses were that: 1)High-intensification compared with low-intensification di-uretic treatment resulted in greater fluid loss in both obeseand nonobese subjects compared with low-intensificationtreatment; 2) nonobese subjects had a low incidence ofworsening renal function with the low-intensification treat-ment strategy, but high-intensification diuretic treatment inthe nonobese subjects was associated with a greater inci-dence of worsening renal function; 3) in contrast, obesesubjects had a higher incidence of worsening renal functionwith low-intensification treatment compared with nonobesesubjects; furthermore, high-intensification diuretic treat-ment in obese subjects did not result in any additional inci-dence of worsening renal function compared with thelow-\intensification strategy; and 4) although obese subjectsmore often had worsening renal function than nonobesesubjects when considering both treatment strategies, thisdid not translate into any worsening of clinical outcomes,including the degree of symptomatic improvement, lengthof hospital stay or 60-day rehospitalization or death. Thesefindings provide some insights into important questions re-garding obesity and HF.
1. Are obese patients with acute decompensated HF dif-ferent from nonobese patients? In this study, obese sub-jects were younger and had a higher prevalence ofdiabetes. These differences between the obese and non-obese groups are unlikely to account for the differencesin fluid loss or changes in kidney function, because obe-sity was associated with worsening renal function evenafter multivariable adjustment for diabetes, age, andsex. The issue of age in HF patients is clinically relevantbecause glomerular filtration rate tends to decrease with
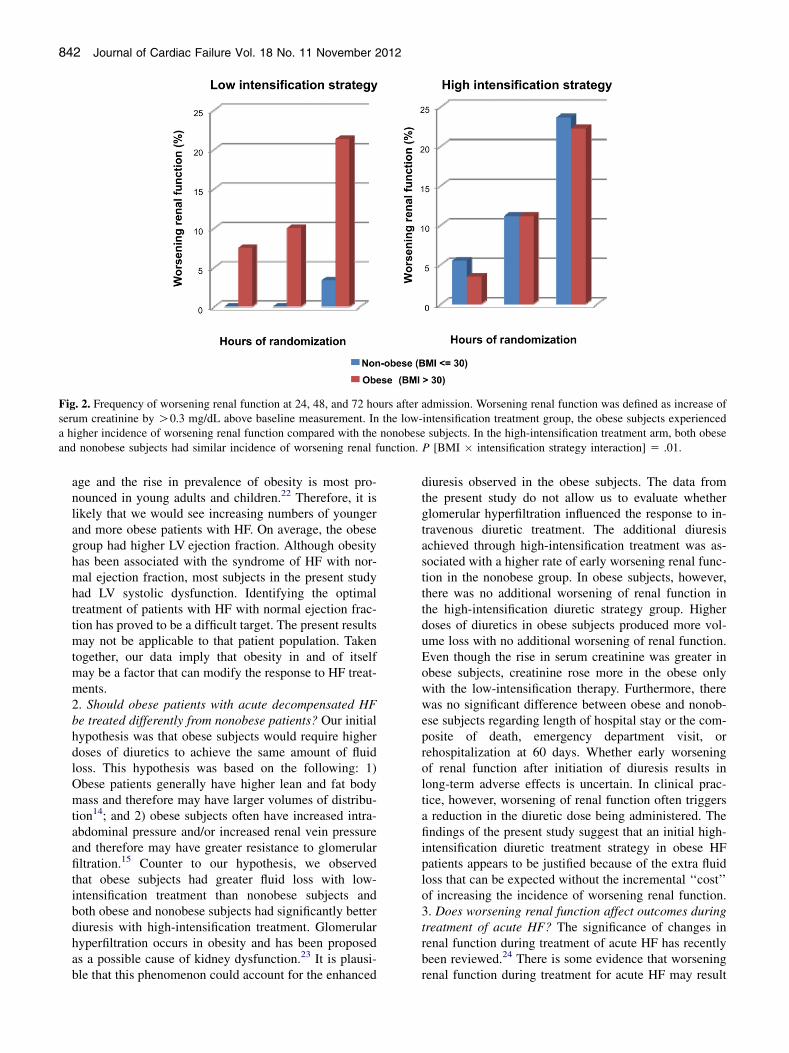
Fig. 2. Frequency of worsening renal function at 24, 48, and 72 hours after admission. Worsening renal function was defined as increase ofserum creatinine by O0.3 mg/dL above baseline measurement. In the low-intensification treatment group, the obese subjects experienceda higher incidence of worsening renal function compared with the nonobese subjects. In the high-intensification treatment arm, both obeseand nonobese subjects had similar incidence of worsening renal function. P [BMI � intensification strategy interaction] 5 .01.
842 Journal of Cardiac Failure Vol. 18 No. 11 November 2012
age and the rise in prevalence of obesity is most pro-nounced in young adults and children.22 Therefore, it islikely that we would see increasing numbers of youngerand more obese patients with HF. On average, the obesegroup had higher LV ejection fraction. Although obesityhas been associated with the syndrome of HF with nor-mal ejection fraction, most subjects in the present studyhad LV systolic dysfunction. Identifying the optimaltreatment of patients with HF with normal ejection frac-tion has proved to be a difficult target. The present resultsmay not be applicable to that patient population. Takentogether, our data imply that obesity in and of itselfmay be a factor that can modify the response to HF treat-ments.2. Should obese patients with acute decompensated HFbe treated differently from nonobese patients? Our initialhypothesis was that obese subjects would require higherdoses of diuretics to achieve the same amount of fluidloss. This hypothesis was based on the following: 1)Obese patients generally have higher lean and fat bodymass and therefore may have larger volumes of distribu-tion14; and 2) obese subjects often have increased intra-abdominal pressure and/or increased renal vein pressureand therefore may have greater resistance to glomerularfiltration.15 Counter to our hypothesis, we observedthat obese subjects had greater fluid loss with low-intensification treatment than nonobese subjects andboth obese and nonobese subjects had significantly betterdiuresis with high-intensification treatment. Glomerularhyperfiltration occurs in obesity and has been proposedas a possible cause of kidney dysfunction.23 It is plausi-ble that this phenomenon could account for the enhanced
diuresis observed in the obese subjects. The data fromthe present study do not allow us to evaluate whetherglomerular hyperfiltration influenced the response to in-travenous diuretic treatment. The additional diuresisachieved through high-intensification treatment was as-sociated with a higher rate of early worsening renal func-tion in the nonobese group. In obese subjects, however,there was no additional worsening of renal function inthe high-intensification diuretic strategy group. Higherdoses of diuretics in obese subjects produced more vol-ume loss with no additional worsening of renal function.Even though the rise in serum creatinine was greater inobese subjects, creatinine rose more in the obese onlywith the low-intensification therapy. Furthermore, therewas no significant difference between obese and nonob-ese subjects regarding length of hospital stay or the com-posite of death, emergency department visit, orrehospitalization at 60 days. Whether early worseningof renal function after initiation of diuresis results inlong-term adverse effects is uncertain. In clinical prac-tice, however, worsening of renal function often triggersa reduction in the diuretic dose being administered. Thefindings of the present study suggest that an initial high-intensification diuretic treatment strategy in obese HFpatients appears to be justified because of the extra fluidloss that can be expected without the incremental ‘‘cost’’of increasing the incidence of worsening renal function.3. Does worsening renal function affect outcomes duringtreatment of acute HF? The significance of changes inrenal function during treatment of acute HF has recentlybeen reviewed.24 There is some evidence that worseningrenal function during treatment for acute HF may result
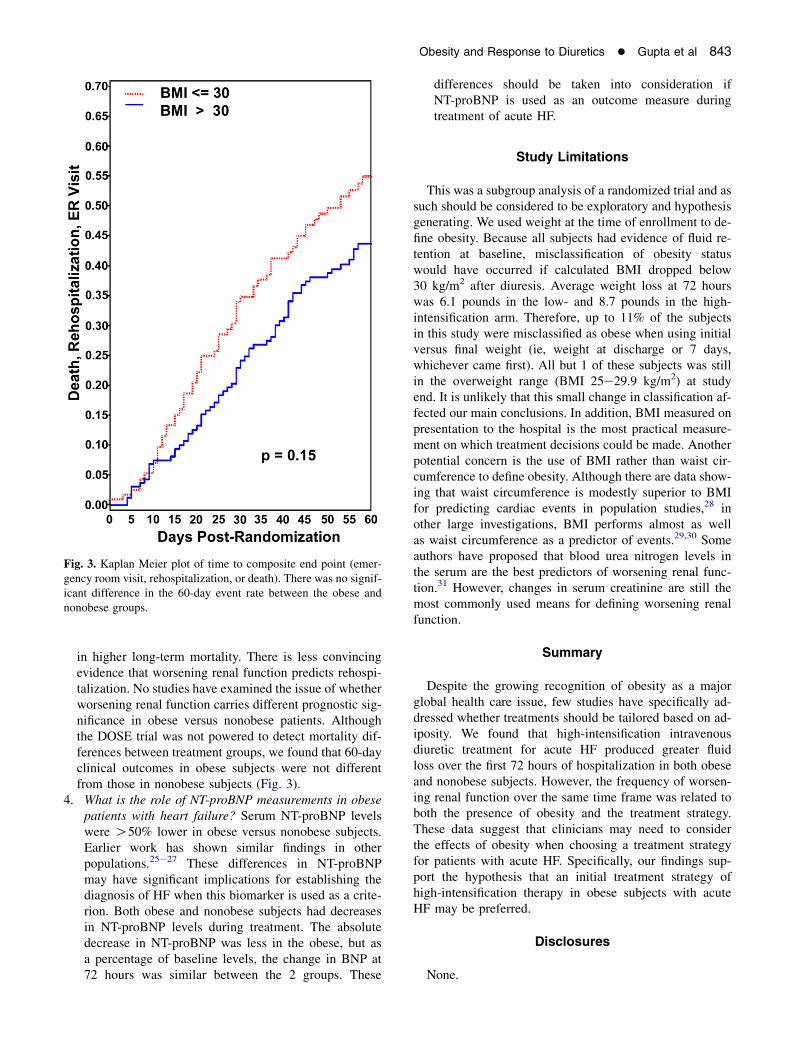
Fig. 3. Kaplan Meier plot of time to composite end point (emer-gency room visit, rehospitalization, or death). There was no signif-icant difference in the 60-day event rate between the obese andnonobese groups.
Obesity and Response to Diuretics � Gupta et al 843
in higher long-term mortality. There is less convincingevidence that worsening renal function predicts rehospi-talization. No studies have examined the issue of whetherworsening renal function carries different prognostic sig-nificance in obese versus nonobese patients. Althoughthe DOSE trial was not powered to detect mortality dif-ferences between treatment groups, we found that 60-dayclinical outcomes in obese subjects were not differentfrom those in nonobese subjects (Fig. 3).
4. What is the role of NT-proBNP measurements in obesepatients with heart failure? Serum NT-proBNP levelswere O50% lower in obese versus nonobese subjects.Earlier work has shown similar findings in otherpopulations.25e27 These differences in NT-proBNPmay have significant implications for establishing thediagnosis of HF when this biomarker is used as a crite-rion. Both obese and nonobese subjects had decreasesin NT-proBNP levels during treatment. The absolutedecrease in NT-proBNP was less in the obese, but asa percentage of baseline levels, the change in BNP at72 hours was similar between the 2 groups. These
differences should be taken into consideration ifNT-proBNP is used as an outcome measure duringtreatment of acute HF.
Study Limitations
This was a subgroup analysis of a randomized trial and assuch should be considered to be exploratory and hypothesisgenerating. We used weight at the time of enrollment to de-fine obesity. Because all subjects had evidence of fluid re-tention at baseline, misclassification of obesity statuswould have occurred if calculated BMI dropped below30 kg/m2 after diuresis. Average weight loss at 72 hourswas 6.1 pounds in the low- and 8.7 pounds in the high-intensification arm. Therefore, up to 11% of the subjectsin this study were misclassified as obese when using initialversus final weight (ie, weight at discharge or 7 days,whichever came first). All but 1 of these subjects was stillin the overweight range (BMI 25e29.9 kg/m2) at studyend. It is unlikely that this small change in classification af-fected our main conclusions. In addition, BMI measured onpresentation to the hospital is the most practical measure-ment on which treatment decisions could be made. Anotherpotential concern is the use of BMI rather than waist cir-cumference to define obesity. Although there are data show-ing that waist circumference is modestly superior to BMIfor predicting cardiac events in population studies,28 inother large investigations, BMI performs almost as wellas waist circumference as a predictor of events.29,30 Someauthors have proposed that blood urea nitrogen levels inthe serum are the best predictors of worsening renal func-tion.31 However, changes in serum creatinine are still themost commonly used means for defining worsening renalfunction.
Summary
Despite the growing recognition of obesity as a majorglobal health care issue, few studies have specifically ad-dressed whether treatments should be tailored based on ad-iposity. We found that high-intensification intravenousdiuretic treatment for acute HF produced greater fluidloss over the first 72 hours of hospitalization in both obeseand nonobese subjects. However, the frequency of worsen-ing renal function over the same time frame was related toboth the presence of obesity and the treatment strategy.These data suggest that clinicians may need to considerthe effects of obesity when choosing a treatment strategyfor patients with acute HF. Specifically, our findings sup-port the hypothesis that an initial treatment strategy ofhigh-intensification therapy in obese subjects with acuteHF may be preferred.
Disclosures
None.
844 Journal of Cardiac Failure Vol. 18 No. 11 November 2012
References
1. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends
in obesity among us adults, 1999e2008. JAMA 2010;303:235e41.2. Howel D. Trends in the prevalence of obesity and overweight in en-
glish adults by age and birth cohort, 1991e2006. Public Health Nutr
2011;14:27e33.
3. Kenchaiah S, Gaziano JM, Vasan RS. Impact of obesity on the risk of
heart failure and survival after the onset of heart failure. Med Clin
North Am 2004;88:1273e94.
4. Baena-Diez JM, Byram AO, Grau M, Gomez-Fernandez C, Vidal-
Solsona M, Ledesma-Ulloa G, et al. Obesity is an independent risk
factor for heart failure: Zona Franca cohort study. Clin Cardiol
2010;33:760e4.
5. Berenson GS, Srinivasan SR. Emergence of obesity and cardiovascu-
lar risk for coronary artery disease: the Bogalusa heart study. Prev Car-
diol 2001;4:116e21.
6. Rao SV, Donahue M, Pi-Sunyer FX, Fuster V. Results of expert meet-
ings: obesity and cardiovascular disease. Obesity as a risk factor in
coronary artery disease. Am Heart J 2001;142:1102e7.
7. Reisin E, Jack AV. Obesity and hypertension: mechanisms, cardio-
renal consequences, and therapeutic approaches. Med Clin North
Am 2009;93:733e51.8. Lakoski SG, Cushman M, Siscovick DS, Blumenthal RS, Palmas W,
Burke G, Herrington DM. The relationship between inflammation,
obesity and risk for hypertension in the Multi-ethnic Study of Athero-
sclerosis (MESA). J Hum Hypertens 2011;25:73e9.9. Abdullah A, Peeters A, de Courten M, Stoelwinder J. The magnitude
of association between overweight and obesity and the risk of diabe-
tes: a meta-analysis of prospective cohort studies. Diabetes Res Clin
Pract 2010;89:309e19.
10. Gami AS, Hodge DO, Herges RM, Olson EJ, Nykodym J, Kara T,
Somers VK. Obstructive sleep apnea, obesity, and the risk of incident
atrial fibrillation. J Am Coll Cardiol 2007;49:565e71.11. Fonarow GC, Srikanthan P, Costanzo MR, Cintron GB, Lopatin M.
An obesity paradox in acute heart failure: analysis of body mass
index and inhospital mortality for 108,927 patients in the Acute De-
compensated Heart Failure national registry. Am Heart J 2007;153:
74e81.
12. Klein L, O’Connor CM, Leimberger JD, Gattis-Stough W, Pina IL,
Felker GM, et al. Lower serum sodium is associated with increased
short-term mortality in hospitalized patients with worsening heart fail-
ure: results from the Outcomes of a Prospective Trial of Intravenous
Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-
CHF) study. Circulation 2005;111:2454e60.13. Cooper HA, Dries DL, Davis CE, Shen YL, Domanski MJ. Diuretics
and risk of arrhythmic death in patients with left ventricular dysfunc-
tion. Circulation 1999;100:1311e5.
14. Hanley MJ, Abernethy DR, Greenblatt DJ. Effect of obesity on the
pharmacokinetics of drugs in humans. Clin Pharmacokinet 2010;49:
71e87.
15. Mullens W, Abrahams Z, Skouri HN, Francis GS, Taylor DO,
Starling RC, Paganini E, Tang WH. Elevated intra-abdominal pressure
in acute decompensated heart failure: a potential contributor to wors-
ening renal function? J Am Coll Cardiol 2008;51:300e6.
16. Ejerblad E, Fored CM, Lindblad P, Fryzek J, McLaughlin JK,
Nyren O. Obesity and risk for chronic renal failure. J Am Soc Nephrol
2006;17:1695e702.
17. Cirillo M, Senigalliesi L, Laurenzi M, Alfieri R, Stamler J, Stamler R,
et al. Microalbuminuria in nondiabetic adults: relation of blood pres-
sure, body mass index, plasma cholesterol levels, and smoking: The
Gubbio population study. Arch Intern Med 1998;158:1933e9.
18. Fox CS, Larson MG, Leip EP, Culleton B, Wilson PW, Levy D. Pre-
dictors of new-onset kidney disease in a community-based population.
JAMA 2004;291:844e50.
19. Hsu CY,McCulloch CE, Iribarren C, Darbinian J, GoAS. Bodymass in-
dex and risk for end-stage renal disease.Ann InternMed2006;144:21e8.
20. Felker GM, O’Connor CM, Braunwald E. Loop diuretics in acute de-
compensated heart failure: Necessary? Evil? A necessary evil? Circ
Heart Fail 2009;2:56e62.
21. Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW,
Goldsmith SR, et al. Diuretic strategies in patients with acute decom-
pensated heart failure. N Engl J Med 2011;364:797e805.
22. Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Preva-
lence of high body mass index in us children and adolescents,
2007e2008. JAMA 2010;303:242e9.23. Griffin KA, Kramer H, Bidani AK. Adverse renal consequences of
obesity. Am J Physiol Renal Physiol 2008;294:F685e96.
24. Butler J, Chirovsky D, Phatak H, McNeill A, Cody R. Renal function,
health outcomes, and resource utilization in acute heart failure: a sys-
tematic review. Circ Heart Fail 2010;3:726e45.
25. Mehra MR, Uber PA, Park MH, Scott RL, Ventura HO, Harris BC,
Frohlich ED. Obesity and suppressed B-type natriuretic peptide levels
in heart failure. J Am Coll Cardiol 2004;43:1590e5.
26. Rogers RK, Stoddard GJ, Greene T, Michaels AD, Fernandez G,
Freeman A, et al. Usefulness of adjusting for clinical covariates to im-
prove the ability of b-type natriuretic peptide to distinguish cardiac
from noncardiac dyspnea. Am J Cardiol 2009;104:689e94.
27. Kevin Rogers R, Stehlik J, Stoddard GJ, Greene T, Collins SP,
Peacock WF, et al. Adjusting for clinical covariates improves the abil-
ity of B-type natriuretic peptide to distinguish cardiac from noncardiac
dyspnoea: a sub-study of HEARD-IT. Eur J Heart Fail 2009;11:
1043e9.
28. Whitlock G, Lewington S, Sherliker P, Clarke R, Emberson J,
Halsey J, et al. Body-mass index and cause-specific mortality in 900
000 adults: collaborative analyses of 57 prospective studies. Lancet
2009;373:1083e96.
29. Litwin SE. Which measures of obesity best predict cardiovascular
risk? J Am Coll Cardiol 2008;52:616e9.
30. Gelber RP, Gaziano JM, Orav EJ, Manson JE, Buring JE, Kurth T.
Measures of obesity and cardiovascular risk among men and women.
J Am Coll Cardiol 2008;52:605e15.
31. Testani JM, Cappola TP, Brensinger CM, Shannon RP, Kimmel SE.
Interaction between loop diuretic-associated mortality and blood
urea nitrogen concentration in chronic heart failure. J Am Coll Cardiol
2011;58:375e82.