Embed Size (px)
Citation preview
A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
AgendaTopic Speaker Welcome/ Overview Karline Roberts, NYSPFP
NYSPFP Readmission Collaborative Karline Roberts, NYSPFP • Goals, Measurement
IPRO Readmission Project Sara Butterfield, RN, BSN, IPRO Donna DeGarmo, RN, MSN, Bassett Healthcare Network Laurie Neander, RN, MS, Bassett Healthcare Network Diane Judson, RN, BSHA, Wingate Healthcare
Next Steps Karline Roberts, NYSPFP • Preparing for In- person Meeting • Capabilities Assessment
Calendar of Events Karline Roberts, NYSPFP
Question and Answer Forum All participants
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
NYSPFP Readmissions Initiative Overview
o Domain I: Patient- and caregiver-centric discharge processes
o Domain II: Improving care transitions between the acute care setting and skilled nursing facilities (SNFs) o Objectives: To assist New York State hospitals inreducing their readmission rates by improving thetransitions of care between acute care providers andSNFs
o Goal: CMS goal of reducing readmissions by 12% from a 2014 baseline
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Approach
o Identify hospital and SNF partners with high readmission rates among shared patients
o Identify readmission champions and interdisciplinary team members in hospitals and SNFs
o Establish recurrent face-to-face collaborative meetings
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Why the Collaborative Approach? o Systematic approach to quality improvement whereby health care organizations come together to: o Identify, test, and measure evidence-based practiceinnovations
o Share experience to accelerate learning and disseminate innovations
o Create a framework for sustaining improvement
February 28, 2017

NYS PARTNERSHIP FOR PATIENTS
NYSPFP Support NYSPFP support will include: o Facilitation of regional collaborative meetings o Hands-on quality improvement support o Assessment tools to identify gaps in current practice o Action planning assistance to drive improvement o Ongoing activities to inform, educate, train, and share
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Benefits of Participating o Support in addressing challenging areas in the transitions of care process
o Resolve outstanding inter-facility issues o Avoid Medicare Reimbursement Reductions:
o Value Based Purchasing o Hospital Readmission Reduction (HRR) Program
February 28, 2017

NYS PARTNERSHIP FOR PATIENTS
Hospital Readmissions Reduction (HRR) Program
o Part of Affordable Care Act o Program links what hospitals are paid to the quality of the care they provide - not just quantity of the services provides
o The HRR Program provides financial incentives to hospitals to reduce costly and unnecessary hospital readmissions
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
The Skilled Nursing Facility Value-Based Purchasing Program (SNFVBP) o What is it?
o The program rewards skilled nursing facilities with incentive payments forthe quality of care they give to people with Medicare.
o When does it start? o Fiscal year 2019 for 2017 calendar year data
o Why is it important? o It promotes better clinical outcomes o Data to be publically reported starting Oct. 2017 on Nursing Home
Compare https://www.medicare.gov/nursinghomecompare/search.html o How will the program work?
o Participating facilities will be paid for their services based on the qualityof care, not just quantity of the services they provide in a givenperformance period.
o Measure o 30-day all cause unexpected potentially preventable readmission rate
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
NYSPFP Readmissions Measurement Strategy
o Overall Outcome Measure o 30 day potentially preventable readmission rate (PPR) o All Condition, All Cause Readmissions Rate o Medicare, All Cause Readmission Rate
o Overall Process Measure o HCAHPS: “Care Transitions” and “Discharge Information” scores
o Aligns with patient/family engagement efforts o No manual data entry o Provides meaningful and actionable data
o Domain II Measures o Medicare SNF readmission rate will be analyzed as databecomes available
o Process and outcome measures within each collaborative will be determined by the collaborative teams
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Website Resources https://www.nyspfp.org/Members/Initiatives/Readmissions/Overview.aspx
February 28, 2017
Transitional Care Partnerships: Aligning Forces for Improved Communication & Care Coordination Across the Healthcare Continuum
IPRO Coordination of Care Initiative
Sara Butterfield RN, BSN, CPHQ, CCM Senior Director, Healthcare Quality Improvement
February 28, 2017
A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
in collaboration with IPRO
1
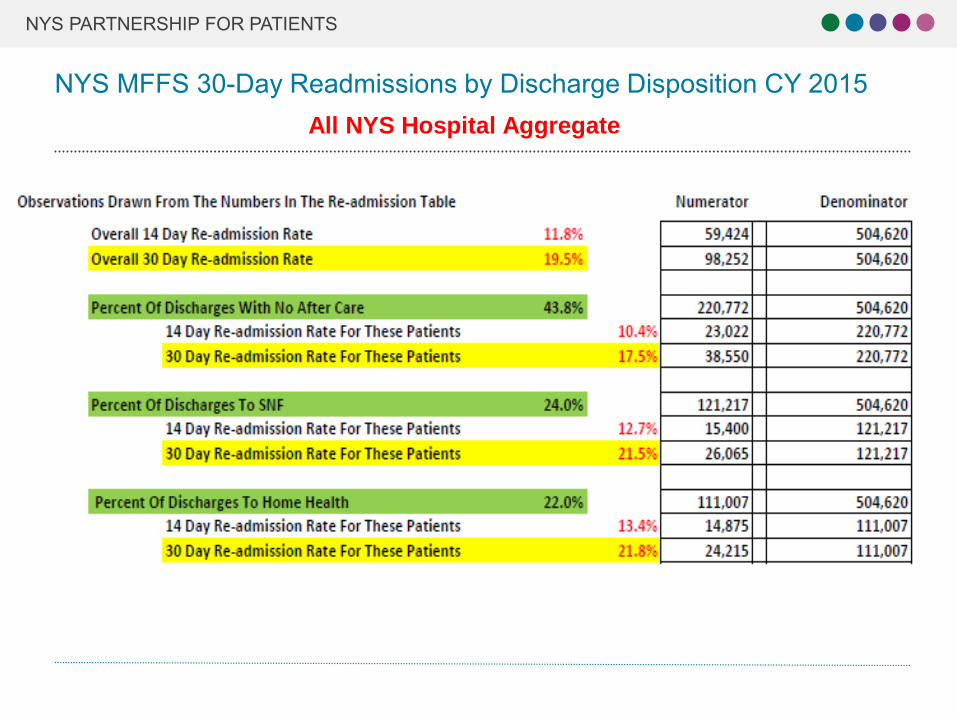
Source: CMS FFS Medicare Claims Data (In hospital deaths and transfers to another acute facility were not counted)
NYS PARTNERSHIP FOR PATIENTS
NYS MFFS 30-Day Readmissions by Discharge Disposition CY 2015
All NYS Hospital Aggregate
2
NYS PARTNERSHIP FOR PATIENTS
Approach o Regional cross-setting community coalitions
● Hospitals, Home Health, Nursing Homes, Assisted Living Facilities, Physician Practices, Hospice, RHIO, Office for Aging, County-based services, community service providers, EMS, Community Pharmacies, Key Stakeholders
o Community Based Root Cause Analysis
o Adoption of Evidence Based Interventions
o Assistance in monitoring & measuring impact
o Building collaborative partnerships to support sustainability
3
NYS PARTNERSHIP FOR PATIENTS
Approach
o Identify common goals & shared missions acrosssettings
o Identify cultural & procedural differences across settings o Each partner has a unique perspective to identify &address issues associated with failed transitions
o Deal with one or two problems at a time, beginning with the easier issues
o Move out of the silo(s)
4
NYS PARTNERSHIP FOR PATIENTS
Building Capacity o Cross-Setting Collaboration is key to success!
o All healthcare settings, community service providers andcommunity partners who have a stake in improving caretransitions need to be involved in Coalition efforts to impact readmission drivers: Hospitals Home health SNF’s Hospice High Volume Physician Offices EMS Community Based Organizations Federal Qualified Health Centers Area Aging and Human Service Providers Medical Homes Assisted Living
5
NYS PARTNERSHIP FOR PATIENTS
The True Key to Success: Building Capacity
Communication Collaboration Partnerships
NYS PARTNERSHIP FOR PATIENTS
Bassett Healthcare Network
Laurie Neander RN, MS President / At Home Care
Donna D. Anderson, RN, MSN, CENP Senior Director for Care Management
Transition Partnerships
A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association
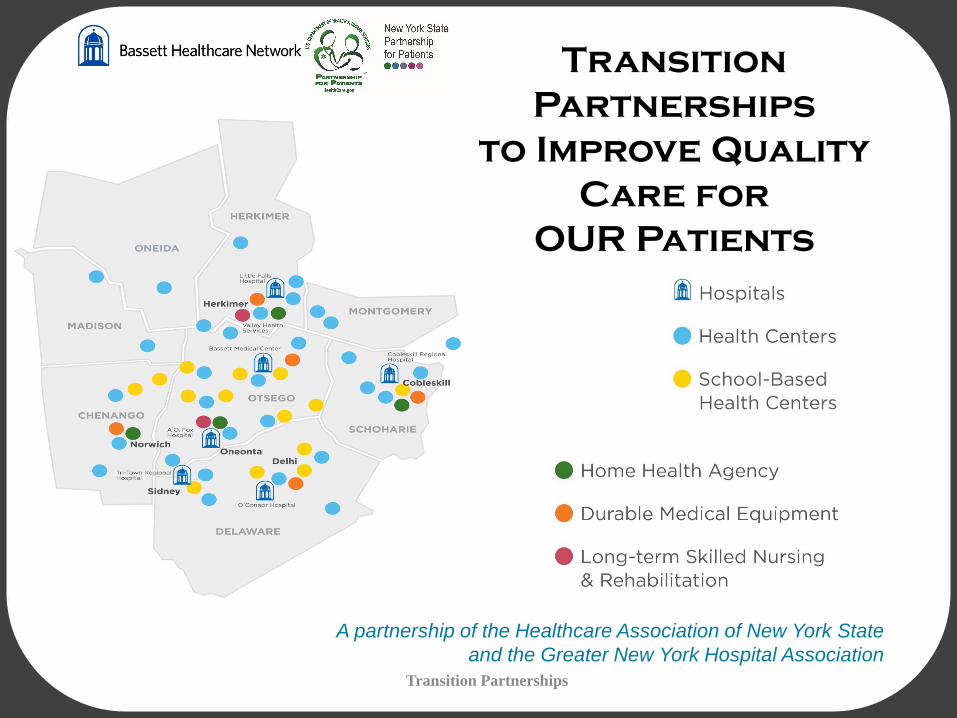
Transition Partnerships
to Improve Quality Care for
OUR Patients
Transition Partnerships

NYS PARTNERSHIP FOR PATIENTS
Adopt a Standardized Risk Assessment Tool
Adopt a Standardized Risk Assessment Tool
Institute for Healthcare Improvement: How-to Guide: Improving Transitions from the Hospital to Home Health Care to Reduce Avoidable Rehospitalizations http://0104.nccdn.net/1_5/1fe/228/023/VNAABP_IHI-Risk-Assessment.pdf

NYS PARTNERSHIP FOR PATIENTSAdopt a Risk Management Strategy
Adopt a Risk Management Strategy
Institute for Healthcare Improvement: How-to Guide: Improving Transitions from the Hospital to Home Health Care to Reduce Avoidable Rehospitalizations http://0104.nccdn.net/1_5/1fe/228/023/VNAABP_IHI-Risk-Assessment.pdf
Transition Partnerships
NYS PARTNERSHIP FOR PATIENTS
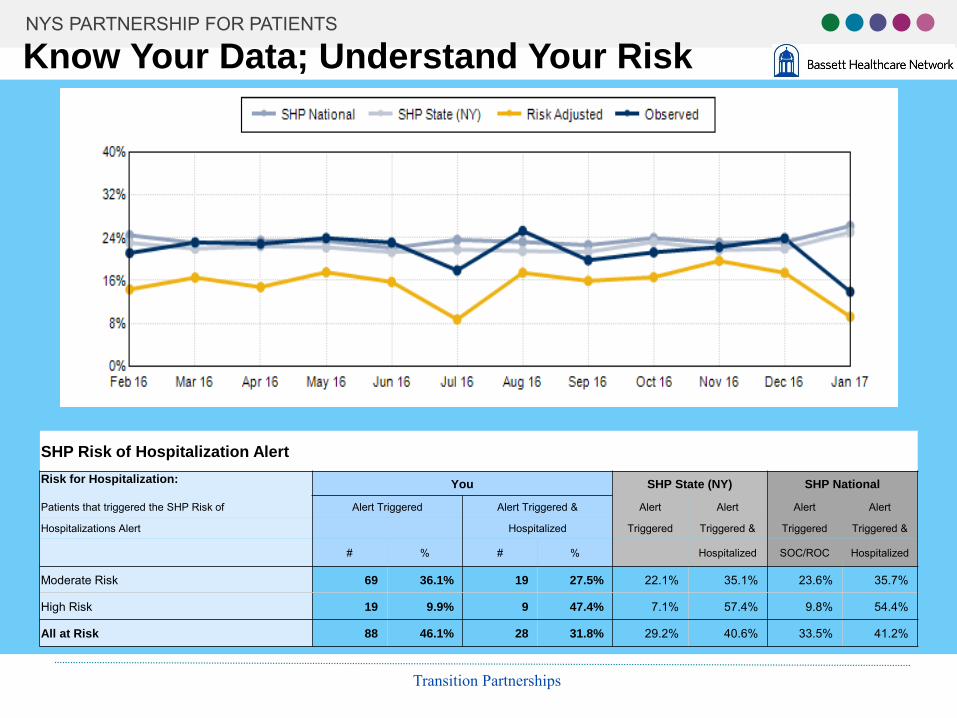
Know Your Data; Understand Your Risk
SHP Risk of Hospitalization Alert Risk for Hospitalization: You SHP State (NY) SHP National
Patients that triggered the SHP Risk of Alert Triggered Alert Triggered & Alert Alert Alert Alert
Hospitalizations Alert Hospitalized Triggered Triggered & Triggered Triggered &
# % # % Hospitalized SOC/ROC Hospitalized
Moderate Risk 69 36.1% 19 27.5% 22.1% 35.1% 23.6% 35.7%
High Risk 19 9.9% 9 47.4% 7.1% 57.4% 9.8% 54.4%
All at Risk 88 46.1% 28 31.8% 29.2% 40.6% 33.5% 41.2%
Transition Partnerships
NYS PARTNERSHIP FOR PATIENTS
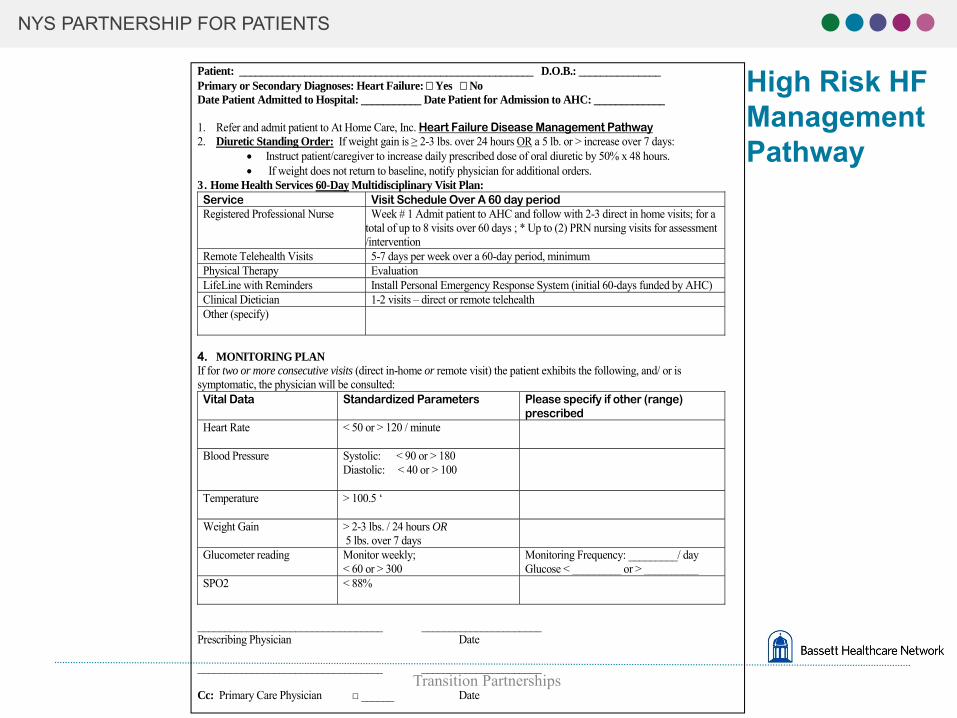
Disease Management Pathways Supported by Telehealth Technology: The Underpinning of A High-Risk Strategy
• Evidence based (American College Cardiology; AHA; ADA; COPD GoldStandard, etc.)
• Define patient specific biometric data ranges-actual vs. self-report • Patient Activation: real time data facilitates an understanding of the relationship
between unhealthy behaviors and poor health – teach self care • Identify a defined set of patient-centered services and interventions to reduce risk
of ED or ACH
Example: • Diuretic Standing Order: If weight gain is ≥ 2-3 lbs. over 24 hours OR a 5 lb. or
> increase over 7 days: • Instruct patient/caregiver to increase daily prescribed dose of oral diuretic by 50%
x 48 hours. • If weight does not return to baseline, notify physician for additional orders.
Transition Partnerships
NYS PARTNERSHIP FOR PATIENTS
Patient: ______________________________________________________ D.O.B.: _______________ Primary or Secondary Diagnoses: Heart Failure: � Yes � No High Risk HF Date Patient Admitted to Hospital: ___________ Date Patient for Admission to AHC: _____________
1. Refer and admit patient to At Home Care, Inc. Heart Failure Disease Management Pathway Management2. Diuretic Standing Order: If weight gain is ≥ 2-3 lbs. over 24 hours OR a 5 lb. or > increase over 7 days:
• Instruct patient/caregiver to increase daily prescribed dose of oral diuretic by 50% x 48 hours. Pathway• If weight does not return to baseline, notify physician for additional orders.
3. Home Health Services 60-Day Multidisciplinary Visit Plan: Service Visit Schedule Over A 60 day period Registered Professional Nurse Week # 1 Admit patient to AHC and follow with 2-3 direct in home visits; for a
total of up to 8 visits over 60 days ; * Up to (2) PRN nursing visits for assessment /intervention
Remote Telehealth Visits 5-7 days per week over a 60-day period, minimum Physical Therapy Evaluation LifeLine with Reminders Install Personal Emergency Response System (initial 60-days funded by AHC) Clinical Dietician 1-2 visits – direct or remote telehealth Other (specify)
4. MONITORING PLAN If for two or more consecutive visits (direct in-home or remote visit) the patient exhibits the following, and/ or is symptomatic, the physician will be consulted: Vital Data Standardized Parameters Please specify if other (range)
prescribed Heart Rate < 50 or > 120 / minute
Blood Pressure Systolic: < 90 or > 180 Diastolic: < 40 or > 100
Temperature > 100.5 ‘
Weight Gain > 2-3 lbs. / 24 hours OR 5 lbs. over 7 days
Glucometer reading Monitor weekly; < 60 or > 300
Monitoring Frequency: _________/ day Glucose < _________ or > __________
SPO2 < 88%
__________________________________ ______________________ Prescribing Physician Date
__________________________________ ______________________ Transition Partnerships
Cc: Primary Care Physician □ ______ Date
NYS PARTNERSHIP FOR PATIENTS
Challenges…and, Opportunity • Health and IT system silos effective use of information technologies is key • Understanding data – including what matters to patients (loss of work, loss of
independence, etc.) • Enabler to reengineer care processes. To understand effective coordination of
longitudinal care and services across all care settings and across all patient conditions
• Level of risk and most appropriate response – cost and care efficient for the full cycle of care
• Supported by a risk stratification assessment, home health care providers design collaborative transitions’ programs to coordinate with primary care/ health home, navigation, remote monitoring technology, care managers …. And, in lieu of ED or ACH, referral of high risk individuals to a traditional Medicare Certified home health program
• A work in progress – knowledge continues to evolve
2/27/2017 Transition Partnerships
NYS PARTNERSHIP FOR PATIENTS
Collaborative Care Patient Centered Care Redesigned Delivery of Care Quality-Adjusted Care Cost-Adjusted Car
NYS PARTNERSHIP FOR PATIENTS
Wingate Healthcare
Diane Judson, RN Regional Director of Network Integration Post Acute Services
Transition Partnerships
NYS PARTNERSHIP FOR PATIENTS
A Transitional Care Model Provider integration moving toward:
Value Based Care Readmission Reduction
& Consistent Patient Engagement
NYS PARTNERSHIP FOR PATIENTS
One Year - 2 Pilot Programs Hospital/SNF/VNS/PCP Areas of Focus: ▪ Organization Capabilities/Process mapping ▪ Communication system development:
→ Provider to Provider → Emergency Room utilization → Hospital Units to SNF Units → Primary and Specialty Care providers → Community Based Providers
Goals: ▪ Care Paths/Risk Stratification ▪ Patient/Caregiver identification, engagement, education and support

NYS PARTNERSHIP FOR PATIENTS
Transitional Care Interdisciplinary Team
○ SNF RN Care Manager (new)
○ Hospital Case Managers
○ Admission Liaisons
○ Specialty Care/Hospitalists
○ Community Based Care Managers/Providers
○ Primary Care Physicians:
○ ACOs/Independent/Small practices

NYS PARTNERSHIP FOR PATIENTS
Blended Models Implemented
▪ Greater New York Hospital Association IMPACT(Readmission Reduction Collaborative)
▪ Geisinger Transitional Care Model
▪ INTERACT
▪ Harold Freeman Care Navigation
▪ Coleman/Naylor
NYS PARTNERSHIP FOR PATIENTS
Key Elements
• Care Management Integration • Physician/Care Manager Engagement• Capabilities Enhancement
• Communication systems: • Warm handoffs • Medication reconciliation • Parallel care paths • Sustained partnerships
NYS PARTNERSHIP FOR PATIENTS
How well did the pilots work?
• Improved quality of care ○ Communication Systems Design ○ Increased clinical capabilities related to plans of care
• Improved physician satisfaction with care○ Primary Care referral and involvement
• Improved patient/family satisfaction ○ Would you recommend? Increased: 78% → 96%
• Reduced Caregiver strain ○ Early engagement in care planning ○ Ongoing communication/education/support

NYS PARTNERSHIP FOR PATIENTS
Most importantly….
• Readmission reduction – Skilled Nursing facility
• from 28%/month to 9%/month within 3 months of implementation
– PCP Group • reported 48% reduction within 3 months of implementation
– LOS in SNF reduced from average of 60 -100 days to 7-21 days – VNS partnership in readmission reduction (blended participants)
▪ SNF placement within 30 days post hospital discharge ▪ Coordinated ER utilization and discharge
Next Steps
NYS PARTNERSHIP FOR PATIENTS
Step I: Building Relationships o Obtain Leadership support o Identify readmission champion and interdisciplinary team members o Complete contact form o Hospital to work with NYSPFP to confirm SNF partners and invite team to meetings
February 28, 2017

NYS PARTNERSHIP FOR PATIENTS
Step 2: Assessing Current Practices and Clinical Capabilities
o Capabilities Survey o Nursing Home Capabilities Survey/Checklist
o To assist hospital emergency rooms, hospitalists, and case managers with decisions about hospital admissions or return to the nursing home
o Hospital Emergency Department (ED) CapabilitiesSurvey/Checklisto To assess the current workflow and practice in the ED to better inform nursing homes
o NYSPFP Participants: Complete the survey o NYSPFP staff will review and aggregate the information to inform of the next steps of the collaborative
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Calendar of Events 2017 o Watch for NYSPFP announcements and dates for upcoming 2017 events: o April/May
o Launch of hospital site in-person sessions o Action planning and goal setting
o June/July o Follow-up coaching calls
o September o Idealized Model Process Mapping Webinar
o October/November o Hospital Site in-person session to tailor process mapping with“idealized practices”
o December o ED/Observation Webinar
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Understand Hospital-SNF Data and Issues
o Analyze your high readmissions by DRG o Compare discharge DRG to readmission DRG
o Conduct audits o Consider interviewing 5 patients who are readmitted to explore issues
o What are the top reasons for the readmissions
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Roadmap to Success o Participate fully – make significant improvementstogether o Commit to improvements and to staff education
o Maintain communication with partners o Maintain reliable contact lists
o Understand each other’s regulatory/site specific issues. o The hospital approach does not equal the nursing homeapproach
o Open communication between facilities o Understand community resources available o Understand or develop innovative best practices o Involve the patient, family, and health care advocate
February 28, 2017
NYS PARTNERSHIP FOR PATIENTS
Develop an AIM Statement and Action PlanAdministrative Champion Team Lead________________
Lead Physician Nurse Lead
Data Lead Other Team Member(s) ________________
AIM STATEMENT
Consider each process change or key strategy below, and complete the worksheet components for implementing them. Add other strategies as appropriate for your hospital.
Process Change/Key
Strategy*
List Next Steps (How will you implement process
change/key strategy?)
Resources/Stakeholders available/needed? (Which Depts/Staff
will be involved?) Owner(s)
CompletionDate(If Not in
Place)
Measurement Strategy (What data will be used to monitor progress/track impact of changes?)
February 28, 2017
Question and Answer