-
8/4/2019 Readmission report
1/51
Reducing Hospital Readmissionsin New York State:A Simulation
Analysis
of AlternativePayment Incentives
Sb 2011
Deborah Chollet
Allison BarrettTimothy Lake
athematica olicy esearch
-
8/4/2019 Readmission report
2/51
Contents
I. Introduction 1
II. Hospital eadmissions in New York State 4
III. Hospital Strateies to educe eadmissions 15
Factors that Contribute to Readmissions 15
Interventions to Reduce Readmissions 16
IV. ayment Incentives to educe eadmissions 19
Direct Costs 19
Indirect Costs 21
Financial Benefts 22
Pay or Perormance 22
Episode-Based Payments 23
V. ayment eorm Simulations 24
Hospital Response to P4P 25
Hospital Response to Episode-Based Payments 27
Eect on the Number o Readmissions 28
Eect on Hospital Payments 29
Direct Payment or Clinical Interventions 30
VI. Summary and Concludin emarks 33
eerences 34
echnical Appendix 36
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
-
8/4/2019 Readmission report
3/51
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
The authors are grateul to the New York State Health Foundation
and especially toSenior Vice President David R. Sandman. Dr.
Sandman provided valuable suggestions
and support throughout the process, and oered thoughtul comments
on early
drats o the research design, fndings, and report. His guidance
and insights are
evident in the report.
In addition, we would like to acknowledge Greg Peterson at
Mathematica Policy Research,
who helped to develop the literature review, and Donna Dorsey,
who produced the drat
and fnal manuscripts.
Support or this work was provided by the New York State Health
Foundation
(NYSHealth). The mission o NYSHealth is to expand health
insurance coverage,
increase access to high-quality health care services, and
improve public and community
health. The views presented here are those o the authors and not
necessarily those
o the New York State Health Foundation or its directors, ofcers,
and sta.
Acknowledgements
-
8/4/2019 Readmission report
4/51
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital readmissions are widely recognized as an important
source o avoidablehealth care costs and a potential marker or
unacceptable levels o hospital
acquired inections, premature discharge, ailure to reconcile
medications,
inadequate communication with patients and community providers
responsible or
post-discharge care, or poor transitional care. While not all
readmissions result rom problems
with patient care or management, strong evidence exists that
some specifc interventions at the
time o discharge can reduce readmissions or certain
conditions.
Conronting the urgent need to address health costs, some states
have begun to ocus
specifcally on such interventionsincluding adherence to
condition-specifc protocols shown
to reduce readmissions, restructuring hospital and post-hospital
discharge planning, and use
o standardized discharge orms to improve communication across
care settings. Similarly,
some integrated delivery systems and multi-stakeholder
collaboratives have begun to investin programs to provide
discharged patients with inormation and advice in order to
prevent
problems that might lead to readmissions. However, emerging
eorts to reduce readmissions
largely ocus on payment incentives.
In this study, we investigate two such incentives:
pay-or-perormance (P4P) and episode-based
payments. The P4P strategy we consider is similar to the New
York Medicaid programs current
P4P system and also similar to the P4P strategy Medicare will
develop as required by the Patient
Protection and Aordable Care Act. The episode-based payment
strategy we consider is similar
to a planned Medicare pilot program, bundling payments or
hospital and post-acute physician
services to encourage more eective coordination o services and
prevent avoidable readmissions.
Rssons n nw YoRk Cost nRY $4 Bon pR YR.In 2008, nearly 15% o all
initial (or index) hospital stays in New York resulted in a
readmission
within 30 days. These readmissions (nearly 274,000 hospital
stays in 2008) cost $3.7 billion,
accounting or 16% o total hospital costs (table s.1).
Readmissions or complications or
inections cost $1.3 billion, accounting or nearly 6% o total
hospital costs.
Ab S.1. Hospital eadmission ates and the Cost o eadmissions,
2008
ttAl
(tHuSANdS)
AdISSIN
At
pCNtAg
f
AdISSINS
ttAl
pAYNtS
($ bIllINS)
pCNtAg
f pAYNtS f
AdISSINS
pCNtAg
f ttAl HSpItAl
pAYNtS
ll admii 2,087.1 /a /a $23.4 /a 100.0%
ll idexadmii 1,872.6 /a /a $19.9 /a 85.2%
All AdISSINS
Fr ay reaihi 30 day 273.6 14.6% 100.0% $3.7 100.0% 16.0%
Frcmlicai rifeciihi 30 day 72.7 3.9% 26.6% $1.3 34.5% 5.5%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
Executive Summary
-
8/4/2019 Readmission report
5/51
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Executive Summary(continued)
Patients aged 65 or older accounted or more than hal o all
readmissions and readmission
costs in New York State in 2008. The rate and cost o
readmissions were highest or Medicareand Medicaid, but readmissions
were a source o signifcant cost or private payers as well.
Rsson Rts VRY wY, Vn just FoR Cs .Individual hospitals
readmission rates varied substantially in 2008. Nine percent o
hospitals
had unadjusted readmission rates that were at least 50% above
the statewide average.
Even adjusted or hospital case mix (that is, the prevalence o
more severely ill patients),
hospital experience varied. Six percent o hospitals had actual
readmission rates that were
at least three percentage points above their expected rates.
pRoVn sCR pRoCsss n post-sCR suppoRtCn RuC ospt Rssons BY
on-tR.At least our actors are widely viewed as important to eective
discharge planning:
(1) coordination between the hospital-based and primary care
physicians, (2) better
communication between the hospital-based physician and the
patient, (3) better education
and support or patients to manage their own conditions, and (4)
reconciliation o medications
at discharge or immediately aterward. While many o the most
promising interventions or
lowering readmission rates address some or all o these actors,
ew have been rigorously
evaluated using randomized controlled trials.
Two interventions that have been rigorously evaluated and ound
eective are the Care
Transitions Intervention (CTI) and Project Re-Engineered
Discharge (RED). Both interventions
engage specially trained nurse advocates who help patients
navigate the discharge process,
educating and coaching the patient to manage his or her disease
ater discharge. Both also
include a ormal reconciliation o medications ollowing discharge.
However, despite strongevidence that both interventions can reduce
30-day all-cause readmissions by 30 to 35%,
relatively ew hospitals have adopted these programs.
wn ConsRn ntRVntons to RuC Rssons,ospts BnC Costs n BnFts.When
hospitals are paid ee-or-service (FFS), each admission or day they
provide care
represents additional revenue. A hospital that is not paid more
when it reduces the probability
o readmissions loses revenue when it readmits ewer patients:
each readmission the hospital
avoids represents lost revenue. As a result, it is unsurprising
that hospitals might be reluctant
to adopt an intervention to reduce readmissions when they are
paid FFS, even when the
intervention is proven to be eective.Increasingly, Federal and
state policymakers are looking to payment incentives to
re-align
hospital incentives to improve quality on various metrics,
including their rates o readmission.
When deciding how to respond to payment incentives, a
revenue-maximizing hospital
-
8/4/2019 Readmission report
6/51
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
would compare the direct and indirect costs with the fnancial
beneft o reducing its rate
o readmission. Payment reorm aims to tip the scale by increasing
the fnancial beneftto hospitals that reduce their readmission
rates; however, little analysis has been done to
determine how eective dierent payment reorms might be.
The two payment reorms considered in this studyP4P and
episode-based payments
represent the two ends o a continuum o payment approaches
designed to reduce the perverse
incentives o FFS payment that encourage readmissions. The
versions o P4P and episode-
based payment we selected are clearly dierent rom one another,
but either could be modifed
in ways that would make them more similar (or example, by
integrating shared savings
between the payers and hospitals).
The P4P approach that we consider is similar to that recently
adopted by New Yorks Medicaid
program, and potentially like that which Medicare will implement
soon. P4P continues
to provide FFS payments or each readmission, but adds an
incentive or hospitals withmore readmissions than would be expected
(given their case mix) to work at lowering their
readmission rates. With P4P, payers can easily recoup savings:
not only do they beneft rom
reduced readmissions (resulting in reduced payments), but they
pay hospitals with high rates o
readmission less per admission.
In contrast, episode-based payments (which Medicare has piloted
but currently does not plan
to adopt more widely) would replace ee-or-service payment
entirely. Each hospital would be
paid more or an index stay by an amount equal to its expected
cost o readmissions, adjusted to
its case mix. Episode-based payments would provide an incentive
or everyhospital to reduce
its readmission rate by, in eect, putting the hospital at
fnancial risk or each readmission.
However, because hospitals would retain the savings associated
with reduced readmissions,
payers would beneft only as payments are benchmarked to lower
readmission rates over time.
pYnt nCntVs Cn RuC Rssons n Costs.Based on a simulation o
hospital responses to P4P and episode-based payments, we
estimated
that either would result in reduced readmissions and lower total
hospital payments. However,
both the magnitude o the response and the expected short-term
cost savings would vary,
depending on the payment incentive.
Specifcally, when conronted with P4P incentives, most hospitals
would ace no payment
reduction; and among the hospitals that would ace a payment
reduction, only some would act
to reduce readmissions. We estimate that 7% o hospitals in New
York would respond to P4P
by implementing an intervention known to reduce readmissions
(CTI or Project RED), resulting
in 1,200 to 2,000 ewer readmissions per year (a reduction o 0.5
to 1%). In contrast, hospitalswould be uniormly more responsive to
episode-based payments. We estimate that at least hal
o hospitals (and as many as 82%) would implement either clinical
intervention, resulting in
19,000 to 45,000 ewer readmissions per year (a reduction o 7 to
16%).
Executive Summary(continued)
-
8/4/2019 Readmission report
7/51
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Reducing the number o readmissions generates cost savingsbut the
savings to payers
depend on the type o payment incentive. When hospitals are paid
FFS, payers always capturethe cost savings rom ewer readmissions.
While the P4P incentives we modeled would induce
less change in hospital behavior than episode-based payments,
payers would capture most o
the cost savings. As a result, simulated total payments to
hospitals (or all admissions) would
all by about $200 million (1%) (table s.2).
With episode-based payments, many more hospitals would respond
and, thereore,
readmissions would all more than they have under P4P; however,
because the hospitals would
be paid their risk-adjusted expected cost o readmissions
(reecting recent past perormance
statewide), the reduction in total payments would lag behind the
reduction in readmissions.
Under episode-based payments, simulated total payments would all
$188 to $286 million
(0.8 to 1.2%). Payers would save more over time as they rebased
episode-based payments to
reect lower rates o readmission, but in the short term,
hospitals would retain most o thesavingsand, thereore, have an
incentive to urther reduce readmissions.
Ab S.2. Simulated ayment eorm ects on Hospital ayments, 2008
ttAl pAYNtS
f All AdISSINS
($ bIllINS)
SIulAtd CHANg IN ttAl pAYNtS
dllAS
($ IllINS)
pCNtAg
CHANg
cal exeriece $23.4 /a /a
pay fr erfrmace
All HSpItAlS tHAt SpNd IplNt:
Ct $23.2 -$200.3 -0.9%
prjec R $23.2 -$205.3 -0.9%
ide-baed ayme
All HSpItAlS tHAt SpNd IplNt:
Ct $23.2 -$187.5 -0.8%
prjec R $23.1 -$285.5 -1.2%
SC: ahemaica plicy Reearch aalyi f ne Yr hial dicharge daa.
RCt pYnt FoR VnC-Bs sCR pRoCsssn post-sCR suppoRt Cou B oR
FFCtV.Under either payment incentives that we modeled, cost savings
were less than would have
occurred had more hospitals been induced to adopt CTI or Project
RED, or had payers been able
to retrieve all o the savings rom reduced readmissions
immediately. Payers might achieve
both greater change and immediate savings simply by paying
hospitals directly to implementevidence-based interventions. For
example, we estimate that New York Medicaid might have
spent $19.9 million to implement Project RED in all hospitals to
achieve a net savings o $116
million. I Medicare had paid directly or evidence-based
interventions to reduce readmissions,
Executive Summary(continued)
-
8/4/2019 Readmission report
8/51
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Executive Summary(continued)
it might have achieved even larger net savings: $427 million by
paying or the Project RED in all
New York hospitals. In the aggregate, commercial payers savings
would have been smaller, butcomparable to Medicaids and still
substantial.
Diverting rom payment incentives to direct payment or reducing
hospital readmissions would
be a signifcant step, especially in light o the P4P program that
New Yorks Medicaid program
already has implemented. However, the prospect o both greater
reduction in readmissions
and greater payer savings rom direct payment to hospitals to
adopt evidence-based discharge
procedures raises important questions about whether payers
should instead rely on payment
incentives or that purpose. This study demonstrates the need or
greater clarity and discussion
among payers and hospitals about how best to achieve the changes
that are needed to reduce
readmissions in New York.
-
8/4/2019 Readmission report
9/51
1
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital readmissions are widely recognized as an important
source o avoidablehealth care costs, as well as a potential marker
or problems that reduce the
quality o care.1 High rates o hospital readmissions can indicate
unacceptable
levels o hospital-acquired inections, premature discharge,
ailure to reconcile
medications, inadequate communication with patients and
community providers responsible or
post-discharge care, or poor transitional care. Indeed,
appropriate coordination and planning
or ollow-up care that should begin in the hospital appears oten
to be lacking: one study
ound that a large percentage o readmitted patients had not seen
a physician ater their initial
discharge (Jencks et al. 2009).
Early initiatives to reduce readmissions started with simply
educating providers and consumers
about the prevalence o readmissions, and many continue to rely
on this method. For example,
Medicare Quality Improvement Organizations use data on
readmissions to provide eedback tohospitals about their own
perormance. In addition, CMS hosts a Medicare Compare website
to help consumers make more inormed choices when selecting a
hospital or inpatient
care. Medicare Compare oers hospital-specifc inormation
comparing 30-day Medicare
readmissions or three conditions (heart attacks, heart ailure,
and pneumonia).2 At least eight
states (including New York) have data systems comparing
hospitals on potentially preventable
readmissions (3-M Health Inormation Systems 2011).3 The
Accountable Care Act (ACA) requires
the Department o Health and Human Services also to collect data
on readmission rates in
order to calculate and publicly report each hospitals
readmission rate.
While not all readmissions result rom problems with patient care
or management, there
is strong research evidence that some specifc interventions at
the time o discharge can
reduce readmissions or certain conditions (Gwadry-Sridhar et al.
2004, Phillips et al. 2004).Conronting the urgent need to address
health costs, some states have begun to ocus
specifcally on such interventionsincluding adherence to
condition-specifc protocols shown
to reduce readmissions, restructuring hospital and post-hospital
discharge planning, and use
o standardized discharge orms to improve communication across
care settings.4
Introduction
1 naially, ad i eleced ae here die f readmii have bee cdced, bh
he rae ad c f readmii areigica. Fr examle, early e-fh (19.1%) f
edicare aie dicharged frm he hial are readmied ihi 30 day,cig
edicare a eimaed $15 $18 billi er year (Cs 2011; jec e al. 2009;
edpC 2007). lg rig dy ipeylvaia acr all ayer fd ha early 20% f aie
admied fr ay f everal cmm rcedre r diage i 2007ere readmied ihi 30
day f dicharge. aa frm arylad hial fr 2007 fd ha arximaely 10% f
aie erereadmied ihi 30 day, cig a eimaed $657 milli er year, r 8% f
al iaie charge (sCRC 2011).
2 Fr each cdii, edicare Cmare rer each hial cae-mix-aded readmii
rae he aial average.
3 the yem develed by 3 ealh ifrmai syem i m cmmly ed meare
eially reveable hialreadmii. decrii f he yem i lace i vari ae i
available a
h://.mh.cm/wrh_aerial/peially%20preveable%20Readmii%20(ppR)%20Rer/texa%20ppR%20
ehdlgy%20overvie.df, acceed ril 22, 2011.
4 Fr examle, sae ci vidable Rehializai (stR) i rig ih fr ae
(aache, ichiga, ohi, adwahig) hel redce rehializai. stR aem egage
ayer, ae ad aial aehlder, aie ad heir
familie, ad caregiver imrve care crdiai befre ad fllig dicharge
(ee: h://aar.er.cm/archive/7/2010,acceed ay 22, 2011).
-
8/4/2019 Readmission report
10/51
2
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Introduction (continued)
Similarly, some integrated delivery systems or multi-stakeholder
collaboratives have begun
to invest in programs to provide discharged patients with
inormation and advice to preventproblems that might lead to
readmissions. For example, some pay specially trained nurses
or pharmacists to ollow up by telephone to confrm that the
patients or caregivers received
discharge instructions, the patient did not receive duplicate or
contraindicated prescriptions,
and that patients or caregivers understand what they need to do
(such as physician ollow-up
visits) to prevent uture problems or complications (Pittsburgh
Regional Health Initiative 2011;
Lake, Stewart, and Ginsburg 2011; Boutwell and Hwu 2009). Two
prominent approaches used in
many o these eorts, the Care Transitions Intervention and
Project Re-Engineered Discharge
(Coleman et al. 2006; Jack et al. 2009), are discussed in detail
in Chapter 3 o this report.
Seeking to expand hospitals eorts to reduce preventable
readmissions, both public and
private payers increasingly are turning to the use o fnancial
incentivesusing measures o
preventable or all-cause readmissions to select a hospital
network, give preerred status ina network, or determine payment
levels. For example, in New York, the Medicaid program
reduces payment to hospitals with a potentially preventable
readmission rate higher than
a statewide risk-adjusted benchmark or all admissions in the
ollowing year.5 In Maryland
(the only state with an all-payer system or establishing
hospital payment rates), planning to
incorporate P4P incentives in all-payer hospital rates is
underway in an eort to reduce rates
o potentially preventable readmissions (Feeney 2011). Under the
Accountable Care Act (ACA),
Medicare also will adjust payment to hospitals with relatively
high rates o readmissions or
selected high-volume or high-expenditure conditions, eective
October 1, 2012. As set out in
proposed regulations, the readmissions reduction program
initially will target acute myocardial
inarction (heart attack), heart ailure, and pneumonia.6
Designing appropriate payment incentives to reduce readmissions
raises important questions
related both to the potential eectiveness o payment incentives
and to their unintended
consequences. For example, ew hospitals may respond to payment
incentives i the magnitude
o incentives is insufcient. Someincluding those that
disproportionately serve disadvantaged
populationsmay not have the fnancial or sta resources to
respond. In either case, payment
incentives might produce less change that is desired and,
urther, might worsen the fnancial
condition o hospitals that serve disadvantaged populations
(Bhalla and Kalkut 2010).
This study investigates the potential or two alternative types o
payment incentives to
reduce rates o readmission in New York acute-care hospitals.
Microsimulation analysis is
used to estimate whether a revenue-maximizing hospital would
respond to, respectively, a
conventional P4P payment system or episode-based payments by
adopting either o two specifc
5 the sae blic healh la reqire ha rae f ayme fr iaie ervice be
redced ch ha e edicaid aymeaeide fall a lea $35 milli fr he erid
jly 1, 2010 hrgh arch 31, 2011, ad a lea $47 milli he ex year (ril
1, 2011hrgh arch 31, 2012).
6 the red mehdlgy ad crieria be ed i imlemeig chage he edicare
hial iaie recive aymereglai ere ied ril 19, 2010. the deii f
alicable hial ad he adme facr by hich ayme ill beredced ill be
addreed i he red rle fr FY 2 013 (Cs 2010).
-
8/4/2019 Readmission report
11/51
3
Introduction (continued)
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
evidence-based interventions to improve discharge procedures and
ollow-up with patients
ater discharge. In order to calculate the maximum potential
eectiveness o such paymentincentives, we assume that all
payersMedicare, Medicaid, and private insurance and employer
planssimultaneously adopt the same system o payment
incentives.
The rest o this report is organized as ollows. In Chapter 2,
estimates o hospital readmission
rates in 2008 are presented or all payers, measured rom New
Yorks hospital discharge
data. Chapter 3 includes a review o the research literature on
hospital interventions to
reduce readmissions, explaining the rationale or selecting two
specifc evidence-based
interventions or the purpose o this study. In Chapter 4, we
present the logic o a revenue-
maximizing hospitals business case or acting to reduce
readmissions in response to either
P4P or episode-based payments. We also present estimates o
hospital cost or each o the
two evidence-based interventions considered in this study. In
Chapter 5, the results o the
simulation analysis are presentedincluding the number and
proportion o hospitals thatimplement either intervention in
response to payment incentives, the change in the number and
rate o readmissions, and changes in the total cost o inpatient
care. Chapter 5 concludes with
an additional analysis investigating the net change in payments
or inpatient hospital care that
might occur i payers directly unded interventions to reduce
hospital readmission, rather than
relying on payment incentives.
-
8/4/2019 Readmission report
12/51
4
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Readmissions are common in New York hospitals, and they are
costly. In 2008, nearly
15% o initial (or index) hospital stays in New York resulted in
a readmission within
30 days (table .1). The cost o these readmissions totaled $3.7
billion, or about 16%
o total hospital costs that year.7
Ab II.1.Hospital eadmission ates and the Cost o eadmissions,
2008
ttAl
AdISSIN
At
ttAl pAYNtS
($ IllINS)
pCNtAg f ttAl
HSpItAl pAYNtS
ll admii 2,087,087 /a $23,391.1 100.0%
ll idex admii 1,872,564 100.0% $19,925.2 85.2%
INDEx ADMISSIONS FOLLOWED BY A READMISSION WITHIN 30 DAYS
Fr ay rea 273,575 14.6% $3,744.0 16.0%
Fr cmlicai r ifeci 72,656 3.9% $1,290.6 5.5%
INDEx ADMISSIONS FOLLOWED BY A READMISSION WITHIN 14 DAYS
Fr ay rea 175,766 9.4% $2,461.6 10.5%
Fr cmlicai r ifeci 48,079 2.6% $867.4 3.7%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
N: Readmii rae are calclaed a he erceage f idex admii flled by a
readmii ihi 30 r 14 day. Readmii raead c ere calclaed fr admii ha
ccrred beee jaary ad ocber 2008 (rered hrgh ecember 2008) ad he
aalized.the c f readmii i eimaed a he charge fr readmii mlilied by
he hial 2008 al c--charge rai.
More than one-ourth o readmissions in 2008 (equal to nearly 4% o
hospital stays) were
or complications or inections. On average, these readmissions
were disproportionately
expensivecosting nearly $1.3 billion or 5.5% o total hospital
costs in 2008.
Not all hospital stays are equally likely to be ollowed by a
readmission. In 2008, most index
stays in New York were or medical treatment (versus surgery,
behavioral health care, or
maternity care). Nearly 18% o medical stays resulted in a
readmission, accounting or 67% o
all readmissions and 69% o all readmission costs ($2.6 billion)
(table .2).8 Nearly 19% o all
readmissions were or complications or inections ollowing a
medical stay; these readmissions
were disproportionately costly, accounting or 24% o all
readmission costs ($913 million).
Hospital Readmissionsin New York State
7 oly idex admii are ed deermie he rri f ay ha rel i a readmii.
dex admii exclde ayhere he aie died, raferred aher healh care
faciliy, lef agai medical advice, r received reame fr a cdiiexeced
rel i a beqe readmii, ch a berical care rir l abr ad delivery r
reame fr a meaaiccacer. reaer deail decribig h idex admii ere deed
i rvided i he echical aedix hi r er.
8 ll admii ha did ivlve rgery, labr ad delivery, r meal healh r
bace abe reame ere caegrizeda medical ay.
-
8/4/2019 Readmission report
13/51
5
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
Ab II.2.Numer and Cost o 30-ay eadmissions y ype o Stay,
2008
Nub f
AdISSINS
AdISSIN
At
pCNtAg
f ttAl
AdISSINS
pAYNtS f
AdISSINS
($ IllINS)
pCNtAg
f ttAl
AdISSIN
CStS
READMISSIONS FOR ANY REASON WITHIN 30 DAYS
nmber f readmii 273,575 14.6% 100.0% $3,744.0 100.0%
tYp f INdx AdISSIN:
edical 182,839 17.9% 66.8% $2,568.6 68.6%
srgical 52,466 11.8% 19.2% $771.8 20.6%
Behaviral healh 33,026 21.5% 12.1% $372.1 9.9%
aeriy 5,243 2.1% 1.9% $31.4 0.8%
READMISSIONS FOR COMPLICATIONS OR INFECTIONS WITHIN 30 DAYS
nmber f readmii 72,656 3.9% 26.6% $1,290.6 34.5%
tYp f INdx AdISSIN:
edical 50,590 4.9% 18.5% $913.4 24.4%
srgical 21,043 4.7% 7.7% $362.9 9.7%
Behaviral healh 930 0.6% 0.3% $13.5 0.4%
aeriy 94 0.0% 0.0% $0.8 0.0%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
N: see table .1.
Surgical stays were less likely than medical stays to be ollowed
by a readmission. In 2008,
nearly 12% o surgical index stays resulted in a readmission
within 30 days, accounting or 19%
o all readmissions and nearly 21% ($772 million) in total
payments or readmissions. However,
more than 40% o readmissions ollowing a surgical index stay were
due to complications
or inections, a much higher proportion than or any other
admission type. Though less than
5% o all readmissions, these readmissions were
disproportionately expensive (similar to
readmissions or complications or inections ollowing a medical
stay), accounting or nearly
10% o all readmission costs ($363 million) in 2008.
Index stays or behavioral health were the most likely to be
ollowed by readmission. More than
21% o patients initially admitted or a behavioral health
diagnosis were readmitted within 30 days.
However, because behavioral health stays were less common in the
frst place (accounting or lessthan 10% o all stays), readmissions
ollowing a behavioral health accounted or a relatively low
share o all readmissions (12%) and a still lower share o
readmission costs (10%, or $372 million).
Admissions or labor and delivery were the least likely to be
ollowed by a readmission. Just 2%
o index admissions or maternity diagnoses were ollowed by a
readmission, accounting or
2% o total readmissions and less than 1% o all readmission
costs.
-
8/4/2019 Readmission report
14/51
6
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Readmission rates varied by patient age: older patients were
much more likely than
younger patients to be readmitted or any reason, and also more
likely to be readmitted orcomplications or inections (table .3).
Patients aged 65 or older accounted or more than hal
o all readmissions and readmission costs in New York State in
2008. More than one-third o all
readmissions or these patients were linked to complication and
inection, compared with 22%
o readmissions or patients aged 45 to 64 and 11% o readmissions
or patients aged 18 to 44.
Ab II.3. Numer and Cost o 30-ay eadmissions y atient Ae,
2008
Nub f
AdISSINS
AdISSIN
At
pCNtAg
f ttAl
AdISSINS
pAYNtS f
AdISSINS
($ IllINS)
pCNtAg
f ttAl
AdISSIN
CStS
READMISSIONS
FOR ANY REASON
WITHIN 30 DAYS
273,575 14.6% 100.0% $3,744.0 100.0%
pAtINt Ag:
1824 year ld 8,880 6.9% 3.2% $101.4 2.7%
2544 year ld 43,043 9.4% 15.7% $484.0 12.9%
4564 year ld 78,407 15.1% 28.7% $1,094.8 29.2%
65 r lder 143,245 18.7% 52.4% $2,063.8 55.1%
READMISSIONS
FOR COMPLICATIONS
OR INFECTIONS
WITHIN 30 DAYS
72,656 3.9% 26.6% $1,290.6 34.5%
pAtINt Ag:
1824 year ld 768 0.6% 0.3% $12.8 0.3%
2544 year ld 5,177 1.1% 1.9% $82.2 2.2%4564 year ld 17,550 3.4%
6.4% $323.1 8.6%
65 r lder 49,162 6.4% 18.0% $872.6 23.3%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
N: see table .1.
Given the strong association between age and readmission rate,
it is unsurprising that most
readmissions occurred ollowing stays or which Medicare paid
(table .4). Nearly 20% o
Medicare stays in 2008 resulted in a readmission, accounting or
58% o all readmissions
and 60% o all readmission costs ($2.3 billion). Nearly one-third
o readmissions ollowing a
Medicare stay were or complications or inections, accounting or
32% o all readmissions and
24% o all readmission costs ($909 million).
Readmissions were less common ollowing index stays paid by
either Medicaid or private
insurance. In 2008, 15% o Medicaid stays were ollowed by a
readmission, accounting or 20%
o readmission costs ($757 million). Just 8% o stays paid by
commercial insurance resulted
in a readmission, but on average these were more costly than
Medicaid readmissions, at least
Hospital Readmissions in New York State (continued)
-
8/4/2019 Readmission report
15/51
7
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
in part due to higher commercial payment rates or hospital care.
Readmissions ollowing a
private-pay stay accounted or 15% o all readmissions costs ($569
million) in 2008.
Ab II.4. Numer and Cost o 30-ay eadmissions y rimary ayer,
2008
Nub f
AdISSINS
AdISSIN
At
pCNtAg
f ttAl
AdISSINS
pAYNtS f
AdISSINS
($ IllINS)
pCNtAg
f ttAl
AdISSIN
CStS
READMISSIONS
FOR ANY REASON
WITHIN 30 DAYS
273,575 14.6% 100.0% $3,744.0 100.0%
xpCtd pAY f INdx AdISSIN:
edicare 157,566 19.6% 57.6% $2,261.6 60.4%
edicaid 57,949 15.0% 21.2% $756.7 20.2%
Cmmercial irace 45,102 8.4% 16.5% $568.9 15.2%
self-ay (ired) 8,288 8.7% 3.0% $101.4 2.7%
ll her 4,669 9.2% 1.7% $55.5 1.5%
READMISSIONS
FOR COMPLICATIONS
OR INFECTIONS
WITHIN 30 DAYS
72,656 3.9%% 26.6% $1,290.6 34.5%
xpCtd pAY f INdx AdISSIN:
edicare 51,050 6.3% 32.4% $909.1 24.3%
edicaid 7,696 2.0% 4.9% $158.9 4.2%
Cmmercial irace 11,478 2.1% 7.3% $183.9 4.9%
self-ay (ired) 1,274 1.3% 0.8% $22.7 0.6%
ll her 1,158 2.3% 0.7% $16.0 0.4%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
N: see table .1.
Readmission rates were higher in some regions o the state than
in others. In particular,
stays at hospitals in the New York City metropolitan area or
Capital District were more likely
to result in a readmission than stays at hospitals in the
western or central regions o the
state (table .5). Readmissions associated with hospital stays in
the New York Metro areaaccounted or 72% o readmissions statewide
and nearly 80% o all readmissions costs, roughly
proportionate to its share o total stays and total hospital
costs.
Readmission rates showed little variation by type o hospital.
Readmission rates associated
with stays in major teaching hospitals and hospitals serving a
disproportionate number o low-
Hospital Readmissions in New York State (continued)
-
8/4/2019 Readmission report
16/51
8
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
income patients were somewhat higher than or other hospitals,
but readmission rates among
these hospital types averaged at most approximately one
percentage point higher than thatamong other hospitals. Reecting
their large share o all admissions and their generally more
complex case mix (an issue addressed below), major teaching
hospitals accounted or 43 o all
readmissions and nearly hal (49%) o all readmission costs.
Disproportionate share hospitals
many o them also teaching hospitalsaccounted or a large majority
o readmissions (72%)
and readmission costs (75%) in 2008.
Ab II.5.Numer and Cost o 30-ay eadmissions y the ocation
o the Index-Admission Hospital, 2008
Nub f
AdISSINS
AdISSIN
At
pCNtAg
f ttAl
AdISSINS
pAYNtS f
AdISSINS
($ IllINS)
pCNtAg
f ttAl
AdISSIN
CStS
READMISSIONS
FOR ANY REASON
WITHIN 30 DAYS
273,575 14.6% 100.0% $3,744.0 100.0%
lCAtIN f tH INdx AdISSIN HSpItAl:
ne Yr Ciy 127,496 15.2% 46.6% $2,051.1 54.8%
oher ne Yr era 69,515 14.5% 25.4% $941.2 25.1%
weer Regi 36,112 13.6% 13.2% $358.7 9.6%
Ceral 20,446 13.6% 7.5% $208.0 5.6%
Caial iric 20,006 14.5% 7.3% $185.0 4.9%
READMISSIONS
FOR COMPLICATIONS
OR INFECTIONS
WITHIN 30 DAYS
72,656 3.9% 26.6% $1,290.6 34.5%
lCAtIN f tH INdx AdISSIN HSpItAl:
ne Yr Ciy 30,780 3.7% 42.4% $682.3 18.2%
oher ne Yr era 19,501 4.1% 26.8% $338.3 9.0%
weer Regi 10,674 4.0% 14.7% $130.0 3.5%
Ceral 5,957 4.0% 8.2% $74.6 2.0%
Caial iric 5,744 4.2% 7.9% $65.3 1.7%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
N: see table .1.
a clde g lad ad ne Rchelle.
-
8/4/2019 Readmission report
17/51
9
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
Ab II.6.Numer and Cost o 30-ay All-Cause eadmissions y ype o
Index-Admission Hospital, 2008
Nub f
AdISSINS
AdISSIN
At
pCNtAg
f ttAl
AdISSINS
pAYNtS f
AdISSINS
($ IllINS)
pCNtAg
f ttAl
AdISSIN
CStS
READMISSIONS
FOR ANY REASON
WITHIN 30 DAYS
273,575 14.6% 100.0% $3,744.0 100.0%
TYPE OF INDEx ADMISSION HOSPITAL:
wNSHIp:
n fr r 237,373 14.6% 86.8% $3,090.9 82.6%
ll her 36,202 14.9% 13.2% $653.1 17.4%
tACHINg StAtuS:
ajr eachighial
118,642 14.8% 43.4% $1,819.4 48.6%
oher eachighial
96,185 14.4% 35.2% $1,278.9 34.2%
n-eachig 56,380 14.5% 20.6% $645.7 17.2%
dISpptINAt SHA HSpItAl:
Ye 196,450 14.9% 71.8% $2,793.4 74.6%
n 74,664 13.8% 27.3% $903.2 24.1%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
NS: see table .1 e. -icme edicare beeciarie receivig lemeal
ecriy icme (ss) ad l-icme edicaidbeeciarie acc fr a high rri f iaie
day i hial deigaed a dirriae hare hial. l 2008,55% f all ace-care
hial i ne Yr sae (129 f 234 i al) ere dirriae hare hial.
-
8/4/2019 Readmission report
18/51
10
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
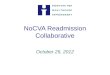
nVu ospt VRton n Rsson Rts
Despite relatively little variation between dierent types o
hospitals, there was substantialvariation among individual
hospitals readmission rates in 2008. While nearly one-third o
hospitals (31%) had readmission rates o 14 to 15%, nearly 13% o
hospitals had readmission
rates o 10% or less. Nine percent o hospitals had readmission
rates o 20% or moreat least
50% above the statewide average (Figre .1).
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
1.3%
0.4%
1.3% 1.3%1.7%
0.4%0.9%
2.6%3.0%
5.6%
7.8%8.2%
9.5%
fIg II.1. istriution o Hospitals y 30-ay All-Cause eadmission
ates, 2008
10.3%
15.5%15.9%
3.4%
2.2% 2.2%
3.4%3.0%
0% 1% 2% 3% 4% 5% 6% 7% 8% 9% 10% 11% 12% 13% 14% 15% 16% 17%
18% 19% 20% 21% 22%or
more
18%
10%
12%
14%
16%
4%
2%
8%
6%
0%
perceage f hial
30-ay ll-Cae Readmii Rae
-
8/4/2019 Readmission report
19/51
11
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
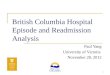
Individual hospitals also perormed very dierently with respect
to their rates o readmission or
complications or inections (Figre .2). One-third o all hospitals
(33%) had 30-day readmissionrates o 4% associated with
complications and inectionsapproximately the statewide average.
But in 9% o hospitals, readmission rates or complications and
inections were 6% or more, and
in 2% o hospitals, they were 8% or moreat least twice the
statewide average.
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
4.7%3.0%
11.6%
22.4%
33.2%
16.4%
5.6%
1.3% 1.7%
fIg II.2. istriution o Hospitals y 30-ay eadmission ates
orComplications and Inections, 2008
perceage f hial
0% 1% 2% 3% 4% 5% 6% 7% 8%
35%
15%
20%
25%
30%
10%
5%
0%
30-ay Readmii Rae fr Cmlicai ad feci
-
8/4/2019 Readmission report
20/51
12
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
Some o the variation in readmission rates between hospitals may
be because o dierences
in hospital case mix. Across all hospitals, index admissions or
some conditionsparticularlyor certain chronic conditionswere much
more likely to be ollowed by a readmission.
Approximately 28% o index admissions or heart ailure were
ollowed by a readmission within
30 days in 2008 (table .7). Similarly, at least 25% o index
admissions or septicemia and
disseminated inections, alcohol or opioid abuse and dependence,
or renal ailure were ollowed
by a readmission.
Ab II.7.hirty-day All-Cause eadmission ates y Index-Admission
ianosis, 2008
ttAl INdx
AdISSINS SultINg
IN A AdISSIN
AdISSIN
At
pCNtAg
f All
AdISSINS
ALL INDEx ADMISSIONS273,575 14.6% 100.0%
INdx-AdISSIN Ap-dgS wItH tH HIgHSt AdISSIN AtS:a
ear failre 15,059 28.3% 5.5%
Chric brcive lmarydieae (Cop)
9,540 22.9% 3.5%
seicemia & diemiaed ifeci 7,793 26.7% 2.8%
oher emia 7,440 16.9% 2.7%
schizhreia 6,506 23.1% 2.4%
lchl abe ad deedece 5,363 25.1% 2.0%
oiid abe ad deedece 5,082 25.9% 1.9%
Real failre 5,582 25.1% 2.0%
Cardiac arrhyhmia ad cdcidirder 5,456 15.9% 2.0%
percae cardivaclarrcedre
5,317 13.9% 1.9%
Bilar dirder 4,373 20.2% 1.6%
kidey & riary rac ifeci 4,766 17.2% 1.7%
gia ecri ad craryahercleri
4,490 17.5% 1.6%
ajr dereive dirder& her ychi
3,959 17.6% 1.4%
Celllii ad her bacerial iifeci
4,068 12.5% 1.5%
iabee 3,599 17.0% 1.3%
ll her pR-R 175,181 12.6% 64.0%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
NS: see table .1 e.
a dex ay ere claied ig ll paie Reed iagi Relaed r (pR-R), hich
gr hial ay fr imilardiage ad everiy f ille.
-
8/4/2019 Readmission report
21/51
13
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
To account or dierences in readmission rates related to
dierences in hospital case mix,
we calculated the dierence between each hospitals actual
readmission rate and its expectedreadmission rate. A hospitals
expected readmission rate is the readmission rate that would
have occurred had it achieved the statewide average readmission
rate or its case mix. In 2008,
about one-third o all hospitals (37%) had an actual readmission
rate within one percentage
point o their expected rates (Figre .3). All other hospitals
either outperormed their expected
rates by more than a percentage point (40%) or underperormed by
the same margin (23%).
Six percent o hospitals had actual readmission rates that were
at least three percentage points
above their expected rates.
e ha -7 -4 -3 2 3 6 7-6 -5 0 1-2 -1 4 5 8 r mre
-7 -6 -1 0-5 -4 1 2 5 6-3 -2 3 4 7 8
1.7% 1.7% 1.3% 1.7%2.6%
12.1%
19.0% 19.4%
9.9%
7.3%
1.3%
2.6%
0.4% 0.4% 0.4%0.9%
17.2%
fIg II.3. istriution o Hospitals y the ercentae-oint ierence
etweenActual and xpected eadmission ates, 2008
perceage f hial20%
12%
14%
16%
18%
10%
6%
4%
2%
0%
8%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
NS: negaive vale idicae a hial acal readmii rae a bel (beer ha)
i execed rae, give i cae mix f idexadmii. piive vale idicae a hial
acal readmii rae a abve (re ha) i execed rae.
perceage pi ifferece Beee he ial' cal ad xeced Readmii Rae
-
8/4/2019 Readmission report
22/51
14
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Readmissions in New York State (continued)
While major teaching hospitals showed, on average, just a
slightly higher rate o actual
readmissions in 2008, they were much more likely to have actual
readmission rates above theirexpected rates. In 2008, nearly 40% o
major teaching hospitals had actual rates o readmission
more than a percentage point higher than their expected rates,
compared with 17 to 18%
o other teaching and nonteaching hospitals (table .8).
Disproportionate share hospitals
also were much more likely to have readmission rates above their
expected rates than other
hospitals (30% versus 14% among other hospitals), although their
actual average readmission
rate was only moderately higher.
In the ollowing chapter we describe strategies to reduce rates o
hospital readmissions and
the research evidence supporting their eectiveness. We select
two o these strategies with
arguably the strongest empirical evidence o eectiveness or the
microsimulation analysis that
comprises the balance o this report.
Ab II.8.Actual and xpected eadmission ates y ype o Hospital,
2008
Nub
f
HSpItAlS
ACtuAl AdISSIN At CpAd wItH
tH HSpItAlS xpCtd At
ACtuAl
AdISSIN
At
btt
(AdISSIN At
wAS At lASt N
pCNtAg pINt
blw xpCtd)
Abut quAl
(AdISSIN At
wAS wItHIN +/- 1
pCNtAg pINt
f xpCtd)
wS
(AdISSIN At
wAS At lASt N
pCNtAg pINt
AbV xpCtd)
ALL HOSPITALS 232 14.6% 40.1% 36.6% 23.3%
wNSHIp:
n-fr-r 205 14.6% 39.5% 37.6% 22.9%
oher 27 14.9% 44.4% 29.6% 25.9%tACHINg StAtuS:
ajr teachig 53 14.8% 20.8% 39.6% 39.6%
oher teachig 69 14.4% 44.9% 36.2% 18.8%
n-eachig 108 14.5% 47.2% 35.2% 17.6%
dISpptINAt SHA HSpItAl:
Ye 129 14.9% 34.9% 34.9% 30.2%
n 100 13.8% 47.0% 39.0% 14.0%
SC: ahemaica plicy Reearch aalyi f ne Yr spRCs hial dicharge
daa.
NS: see table .1. t f he 234 ace-care hial ideied i hi dy had ay
qalifyig a idex admii,ad are iclded i he hial-ecic able ad gre.
-
8/4/2019 Readmission report
23/51
15
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Strategies toReduce Readmissions
The growing body o research investigating actors that contribute
to hospital
readmissions has led to broad agreement among clinical experts
and other
stakeholders that improving the discharge process and providing
support
immediately post-discharge are essential to reducing the number
o readmission
(Minott 2008). In turn, a number o clinical interventions have
been piloted or populations
most at-risk or readmissions (such as older patients and
patients with congestive heart
ailure), and some have been ound to be eective in reducing the
likelihood o readmission.
This chapter briey reviews the literature evaluating these
interventions.
FCtoRs tt ContRBut to RssonsFragmentation o care across settings
is a major contributor to readmissions. Over the past two
decades, patients have become less likely to see their primary
care physicians when hospitalized,
and more likely to see a hospitalist (a physician who provides
care only to hospitalized patients).
This trend has created a heightened need or care coordination
and inormation sharing o among
providers as patients are admitted and discharged rom hospitals,
beyond the limits o a typical
discharge process (Bodenheimer 2008). Instead, hospitals
discharge processes and timelines
generally are oriented toward documentation (not notifcation)
and implicitly assume that patients
primary care physicians were involved with their inpatient care.
Fewer than one in fve primary
care physicians report being routinely notifed when their
patients are discharged rom a hospital
(Kripalani et al. 2007). Moreover, even when the primary care
physician receives a discharge
summary, it oten lacks key inormation about the patients
discharge diagnosis, test results,
medications prescribed, or plans or ollow-up care.
When primary care physicians are not notifed about an admission
through the discharge
process, patients themselves become the primary source o
inormation about their hospital
stay. But patients oten do not understand their condition and
treatment plan as well as
hospital-based physicians may assume. One study ound that, while
nearly 90% o physicians
believed patients understood key inormation about the side eects
o their medications and
when to resume normal activity ollowing discharge, less than 60%
o their patients actually
said they understood (Calkins et al. 1997). Such poor
communication oten leaves patients
and amily members abruptly expected to manage problems
encountered ater discharge
with little preparation (Coleman and Berenson 2004).
Unknowledgeable about their condition
and conused about who is responsible or their care immediately
ollowing discharge, many
patients may return to the hospital when they experience
problems that might have beentreated successully without
readmission.
Poor communication between physicians and patients, or between
dierent physicians treating
the same patient in dierent settings, can also generate
medication errors. One study ound that
nearly 13% o discharged patients suered an injury caused by
medication errors; many required
-
8/4/2019 Readmission report
24/51
16
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Hospital Strategies to Reduce Readmissions (continued)
re-admission (Foster et al. 2003). Poor communication among the
hospitalist, the patient, and the
patients primary care physician was identifed as a contributing
actor in most cases.
Medication errors oten occur when the prescribing physician has
incomplete inormation about
the patient. In one study, 94% o patients discharged rom an ICU
were ound to have medication
errors that the treating physician corrected when presented with
current inormation about
the patients other prescriptions and allergies (Provonost et al.
2003). Medication errors also
occur when patients ail to correctly take the medications that
were prescribed during their
stay ater leaving the hospital. At least 14% o recently
discharged patients may not comply with
the medications specifed in their discharge instructionsoten
because the instructions are
illegible or incomplete, contain conicting inormation about what
kind o medicine or dosage to
take, or duplicate older prescriptions without inorming the
patient that previously-prescribed
drugs must be discontinued (Moore et al. 2003, Coleman et al.
2005).
ntRVntons to RuC RssonsAt least our actors are widely viewed as
important to eective discharge planning: (1)
coordination between the hospital-based and primary care
physician, (2) better communication
between the hospital-based physician and the patient, (3) better
education and support or
patients to manage their own condition, and (4) reconciliation o
medications at discharge or
immediately aterward (Kripalani et al. 2007). While many o the
most promising interventions
or lowering readmission rates address some or all o these
actors, relatively ew have been
rigorously evaluated (Minott 2008).
However, the interventions that have been have been rigorously
evaluated, based on one
or more randomized controlled trials (RCTs), are summarized in
Table III.1. Most o these
interventions have ocused on enhancing the discharge process or
educating patients aboutsel-management o their condition (Boutwell
and Hwu 2009). The intervention oten included
ormal review or reconciliation o medications as part o the
discharge process or immediately
ater discharge. One meta-analysis o 18 dierent interventions
targeting older patients with
congestive heart ailure ound that comprehensive discharge
planning plus post-discharge
support reduced the probability o readmission by 25% (Phillips
et al. 2004). More intensive post-
discharge services did not appear to be more eective than less
intensive services: a single home
visit, multiple home visits, and requent telephone ollow-ups
were all eective in reducing the
likelihood o readmissions.
Several o the tested interventions targeted older adults, who
typically experience the highest
rates o readmission. One such intervention, the Transitional
Care Model, was evaluated or
older patients with congestive heart ailure or respiratory
inection, or who underwent cardiac
surgery, orthopedic surgery, or bowel procedures. An advanced
practice nurse (APN) visited
each patient regularly during the hospital stay to evaluate
patient and caregiver needs, develop
an individualized discharge plan, and educate the patient about
sel-care ater discharge. The
APN also provided post-discharge support in the orm o home
visits and telephone calls. In three
dierent RCTs, this model was shown to signifcantly reduce
readmissions over periods ranging
rom 2 to 52 weeks ater discharge (Naylor et al. 1994; Naylor et
al. 1999; Naylor et al. 2004).
-
8/4/2019 Readmission report
25/51
-
8/4/2019 Readmission report
26/51
18
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Three interventions targeted patients o all ages. Project
Re-Engineered Discharge (RED) uses
a nurse advocate to assist patients in navigating the discharge
process, as well as a clinicalpharmacist who telephones the patient
2 to 4 days ater discharge to reconcile medications.
Project RED was shown to reduce 30-day all-cause readmissions by
32% (Jack et al. 2009).
Another intervention that had a pharmacist placing a telephone
call to reconcile medications
in the days ater discharge also decreased readmission rates
substantially, but the change
was not statistically signifcant (Dudas et al. 2001). An
intervention that involved a redesigned
discharge orm, but no ormal reconciliation o medications or
additional patient education and
coaching, did not reduce readmissions (Balaban et al. 2008).
Some o the evaluations described above also compared the direct
costs o the intervention
to the costs savings due to lower readmissions. In most cases,
the amounts that would
have been paid or readmissions were larger than the direct costs
o the intervention; even
relatively intense and expensive interventions reduced net
medical spending. However,in practice the savings rom lower
readmissions accrue to payersMedicare, Medicaid,
commercial health insurance companies, and the patients
themselveswhile hospitals
shoulder the direct costs o the intervention. When paid per
admission, hospitals would also
ace a revenue loss rom ewer readmissions.
The next chapter explores this problem o incentives or hospitals
to invest in reducing
readmissions and reviews changes in payment methods that might
cause hospitals to invest
in reducing readmissions. We consider hospital decisions to
adopt either o two clinical
interventions described above: CTI or Project RED. Both models
have been rigorously evaluated
and tested on a range o patients with dierent diagnoses, and
estimates o their resource costs
are public inormation.
Hospital Strategies to Reduce Readmissions (continued)
-
8/4/2019 Readmission report
27/51
19
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Policymakers have long been concerned about the lack o
incentives or providers to
improve health care quality under a ee-or-service payment
system, which provides
ew i any apparent incentives or quality o care and probably
contributes to service
overuse and cost (Leatherman et al. 2003). These concerns have
motivated some
payers to develop payment reorms that modiy or replace
ee-or-service payment.
In this chapter, we consider the decision process o a hospital
whose business model is simply
to maximize revenues. Such a hospital would weigh the direct and
indirect costs o reducing
readmissions with the likely fnancial benefts, and proceed to
invest in reducing readmissions
only i the expected fnancial benefts outweigh the costs. The
basic cost components o this
calculus are discussed below with reerence to two alternative
clinical interventions that weredescribed in Chapter 3: the Care
Transitions Intervention (CTI) and Project Re-Engineered
Discharge (RED). The fnancial benefts are discussed with
reerence to two alternative payment
reorms, pay-or-perormance (P4P) and episode-based payments, each
structured to encourage
hospitals to reduce readmissions. Because each cost component
could dier according to a
hospitals particular circumstances, dierent hospitals could make
dierent decisions to invest in
reducing readmissions when conronted with the same payment
incentives.
RCt CostsClinical interventions to reduce readmissions entail
both labor and capital costs. Labor costs
are incurred to manage transitions rom the hospital to home or
other settings. Capital costs,
at least with respect to the clinical interventions that have
been rigorously evaluated in theresearch literature, are minimal.
Potentially they include only the opportunity cost o unds
allocated to fnance labor.
As described in Chapter 3, CTI targets patients with any o 11
high-risk conditions. CTI entails
use o an advanced practice nurse who serves as an advocate or
these patients during the
discharge process, helps them coordinate post-discharge care,
and ormally reconciles their
medications during an initial home visit. Estimated or 2008 and
calculated regionally or New
York State, these costs per discharge would have varied or
hospitals across the state due to
regional dierences in labor costs and by the number o patients
per year the advance practice
nurse manages. Hospitals in nonmetropolitan southwest New York
State would have paid as
little as $198 per discharge to implement CTI, while hospitals
in the New York-White Plains-
Wayne metropolitan area would have paid as much as $348 (table
V.1).
In contrast, Project RED targets all patients discharged rom a
medical stay. It uses a nurse
advocate to assist patients in navigating the discharge process,
as well as a clinical pharmacist
who telephones the patient to reconcile medications. This
intervention is less costly per admission
than CTI because it does not entail home visits. In 2008, the
cost o implementing Project RED
Payment Incentivesto Reduce Readmissions
-
8/4/2019 Readmission report
28/51
20
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Incentives to Reduce Readmissions (continued)
would have ranged rom as little as $111 per discharge or
hospitals in the nonmetropolitan
Capital/Northern New York area to $132 per discharge or
hospitals in Nassau-Suolk(table V.2). However, because Project RED
is not as narrowly targeted (it would apply to all
patients discharged rom the hospital to home, not only those
with selected high-risk diagnoses),
the total cost o implementing it can be higher depending on the
hospitals case mix.
Ab IV.1.xpected Cost o CI per Admission y eion o New York State,
2007
AVAg ANNuAl CpNSAtIN
f A gIStd NuS
xpCtd AVAg CSt
f A CA tANSItINS INtVNtIN
p AdISSIN
AVAg ANNuAl
wAg
ttAl AVAg
ANNuAl
CpNSAtIN lw StIAt HIgH StIAt
tplItAN AAS
lbay-scheecady-try $56,040 $73,300 $218 $255
Bigham $52,350 $68,474 $204 $238
Bffal-niagara Fall $56,180 $73,483 $219 $255
lmira $48,140 $62,967 $187 $219
le Fall $54,410 $71,168 $212 $247
haca $52,020 $68,042 $203 $236
kig $55,280 $72,306 $215 $251
naa-sffl, erliaivii
$73,440 $96,060 $286 $334
ne Yr-whie plai-waye $78,920 $103,227 $307 $358
pgheeie-nebrgh-iddle $65,810 $86,079 $256 $299
Rcheer $54,860 $71,757 $214 $249
syrace $52,770 $69,023 $205 $240
uica-Rme $52,290 $68,395 $204 $237
NN-tplItAN AA S
Caial/nrher ne Yr $52,170 $68,238 $203 $237
Ceral ne Yr $52,970 $69,285 $206 $241
a-ceral ne Yr $53,720 $70,266 $209 $244
she ne Yr $48,540 $63,490 $189 $220
SCS: ahemaica plicy Reearch. verage aal age are frm eropolia rea
Cro-dury imae, ay 2007 (Brea f abrsaiic). the erceage f al cmeai
her ha age i he aial average fr hial-baed re, frm mployer Co
for
mployee Compeaio, table 14, je 2007 (Brea f abr saiic).NS: the
eimae ame ha he raii crdiar i a Rn h i aid he lcal average aal age
ad maage 288 aie (higheimae) 336 aie (l eimae) er year, baed a
blihed evalai f he Ct demrai (Clema e al. 2006). tal cmeaic iclde
he c f all -age cmeai (FC, aid leave, healh irace, reireme bee, ad
lemeal ay); agecmeai averaged 30.8 erce f al cmeai fr hial-baed Rn
aially i 2007.
-
8/4/2019 Readmission report
29/51
21
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Incentives to Reduce Readmissions (continued)
Ab IV.2.xpected Cost o roject per Admission y eion o New York
State, 2007
ggApHIC
AA
AVAg ANNuAl CpNSAtIN
f A pHYSICIAN ASSIStANt
AVAg ANNuAl CpNSAtIN
f A pHAACISt xpCtd CSt
f pjCt d
INtVNtIN
p AdISSIN
AVAg
ANNuAl wAg
ttAl
CpNSAtIN
AVAg
ANNuAl wAg
ttAl
CpNSAtIN
tplItAN AAS
lbay-scheecady-try
$80,300 $104,711 $90,900 $118,534 $104
Bigham /a /a $89,000 $116,056 $103
Bffal-niagara Fall $74,900 $97,670 $96,470 $125,797 $101
lmira /a /a $102,010 $133,021 $107
le Fall $84,740 $110,501 $88,100 $114,882 $107
haca /a /a $98,000 $127,792 $106
kig /a /a $98,450 $128,379 $106
naa-sffl,erlia ivii
$87,630 $114,270 $102,690 $133,908 $115
ne Yr-whieplai-waye
$85,880 $111,988 $94,690 $123,476 $110
pgheeie-nebrgh-iddle
$82,270 $107,280 $103,510 $134,977 $110
Rcheer $76,700 $100,017 $108,490 $141,471 $106
syrace $75,810 $98,856 $100,110 $130,543 $103
uica-Rme $84,380 $110,032 $103,470 $134,925 $112
NN-tplItAN AA S
Caial/nrher neYr
$71,630 $93,406 $91,730 $119,616 $96
Ceral ne Yr $85,860 $111,961 $94,230 $122,876 $110
a-ceral ne Yr $86,360 $112,613 $106,500 $138,876 $115
she ne Yr $72,250 $94,214 $99,630 $129,918 $99
SCS: ahemaica plicy Reearch. verage aal age are frm erlia rea
Cr-dry imae, ay 2007 (u.s. Brea fabr saiic). the erceage f al cmeai
her ha age i he aial average fr hial-baed rfeial, frm mlyerC fr
mlyee Cmeai, table 14, je 2007 (u.s. Brea f abr saiic).
NS: the eimaed c er idex admii ame 0.5 hr f harmaci ime ad 1.5
hr f -hyicia rvider ime er aie(jac e al. 2009). tal cmeai iclde he
c f all -age cmeai (FC, aid leave, healh irace, reireme bee,
adlemeal ay) fr -Rn hial-baed rfeial, hich averaged 30.4% f al
cmeai aially i 2007; /a idicae haeimae are available.
nRCt CostsIn considering whether to intervene to reduce
readmissions, a revenue-maximizing hospital
presumably would also consider its indirect costs. With
ee-or-service payment (even when
hybridized to include P4P incentives), hospitals receive
additional revenue when they readmit
a patientand conversely, they lose revenue when they readmit
ewer patients. Plainly stated,
-
8/4/2019 Readmission report
30/51
22
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Incentives to Reduce Readmissions (continued)
a hospital whose business model is to maximize inpatient
revenues might not make an eort
to reduce readmissions, all else equalregardless o the level o
direct costs the eort wouldrequire. Each readmission it avoids
would simply represent revenue oregone.
Indeed, with ee-or-service payment, the fnancial incentives
associated with hospitals indirect
costs are strongly perverse, as long as the hospital expects to
at least break even on the next
readmission. A hospitals indirect costs would be highest (and,
thereore, its ee-or-service
incentives to reduce readmissions would be lowest) when a
relatively high share o its revenue
comes rom readmitting patients it had previously discharged.9
Moreover, the more eective
the intervention, the greater this hospitals indirect cost would
beand, thereore, the less
likely the hospital would be to implement it.
FnnC BnFts
For a revenue-maximizing hospital to make an eort to reduce
readmissions, it would needto anticipate a fnancial reward or
reducing readmissions o sufcient magnitude to oset its
cost disincentives. We consider two payment reorms intended to
oer such a reward: P4P and
episode-based payments. Each is discussed below.
ay or erormance
P4P is a particular instance o a broader set o payment reorms
called value-based purchasing
(Rosenthal et al. 2006, Rosenthal 2009, Miller 2009). P4P
initiatives typically use evidence-
based measures o quality, eectiveness, and efciency to classiy
or select providers, and to
determine how much they are paid. Commercial P4P systems oten
use hybrid approaches,
combining ee-or-service payment with payment bonuses or
withholds that reect provider
perormance on specifc measures o quality or patient satisaction
(Bernstein et al. 2010).
Evidence o the eects o P4P systems is mixed, in no small part
because o the difculty o
discerning their impact on care delivery, costs, or outcomes.
However, many may simply oer too
little fnancial incentive or providers to invest in quality
improvement (Rosenthal et al. 2005).
A P4P system intended to reduce readmissions, when hybridized
with ee-or-service, would
pay hospitals with low case-mix-adjusted readmission rates more
than it would pay hospitals
with high case-mix-adjusted readmission rates. To invest in
reducing readmissions, a revenue-
maximizing hospital would need to see a fnancial beneft that
outweighs its direct and indirect
costs. That is, the hospital would need to succeed in increasing
its P4P payment rate enough
to oset both its higher cost per discharge and its revenue loss
due to lower patient volume.
Whether any one hospital would see such a net beneft is not
immediately obvious. Indeed, the
hospitals response would depend both on its own circumstances
and on the particular P4P
strategy used. All else equal, a hospital that expects a larger
reduction in its readmission ratewould be less inclined to invest
in reducing readmissions, even when paid less per admission.
9 ial al receive revee by readmiig aie dicharged frm her hial.
Fr he re f hi aalyi, e ameha a hial decii a heher imleme a iervei
redce readmii i made ideedelyha i, eachhial cider ly he acial
ceqece i migh rdce he acig ale.
-
8/4/2019 Readmission report
31/51
23
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Incentives to Reduce Readmissions (continued)
For payers, a potential advantage o P4P is the opportunity to
retrieve savings immediately,
even i hospital behavior does not change. Payers are most likely
to retrieve P4P savingso the top by paying low-perorming hospitals
less, while making little or no adjustments
to payment rates or high-perorming hospitals. This practice
limits high-perorming hospitals
incentives to urther reduce readmissions, although it might be
efcient i currently low-
perorming hospitals oer the greatest potential or reducing
aggregate readmissions.
pisode-based aymentsEpisode-based payments would eliminate
payments or some or all readmissions within some
interval ater discharge, removing muchi not allo the perverse
incentive associated with
ee-or-service payments. For each index admission, the hospital
would receive an increase in
payment equal to the expected cost o readmissions. Each
readmission would represent wholly
unreimbursed cost.
With episode-based payment, every hospital would see a fnancial
beneft rom reducing
readmissions regardless o how low its readmission rate might
already be. However, a revenue-
maximizing hospital would choose to invest in reducing
readmissions only i its expected
savings (that is, the expected change in its costs or
readmissions) exceeded the direct cost o
the intervention.
Thus, the hospitals decision to invest in reducing readmissions
hinges on the same general
actors as those that come into play or P4P, but the hospital
considers them dierently.
All else equal, a hospital that expects a greater reduction in
its readmission rate would be more
inclined to invest in reducing readmissions.
For payers, the downside o episode-based payments would be their
inability to retrieve
immediate savings. I payments are set equal to the expected
value o current payments oradmissions plus expected
(case-mix-adjusted) readmissions, aggregate payments in the
short
term would change very little, i at all. The only signifcant
opportunity to retrieve savings would
occur over time, as hospitals succeeded in reducing readmissions
and payers re-benchmarked
payments to a lower expected rate o readmissions.
In the next chapter, we estimate hospital responses to P4P and
episode-based payment
reorms, using a simulation modeling approach. We estimate
whether hospitals in New York
would adopt either CTI or Project RED under either payment reorm
and examine the resulting
eects on statewide readmission rates and payments or hospital
care.
-
8/4/2019 Readmission report
32/51
24
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Reform Simulations
In this chapter, we present the results o our payment reorm
simulations and theresulting eects on readmissions and aggregate
hospital payments. We estimate
hospitals adoption o either CTI or Project RED in response to
two alternative payment
incentivesP4P and episode-based payments. The simulations assume
that each
hospital would compare its cost o implementing either
intervention to its expected fnancial
beneft rom reducing readmissions. A hospital would implement an
intervention to reduce
readmissions only i its expected beneft exceeded its expected
cost.
The frst payment reorm we simulated is a P4P approach similar to
those recently adopted
by New York Medicaid and soon to be implemented by Medicare.
Under this P4P approach,
hospitals with readmissions exceeding an expected rate o
readmissions, reerred to as
excess readmissions, would have their overall payments per
admission reduced in an amount
roughly equal to payments or those excess readmissions.
The second payment approach is an episode-based payment model,
in which hospitals no
longer receive incremental payments or each readmissionas under
ee-or-servicebut
instead are paid an additional amount or each initial index stay
intended to cover the expected
costs o any readmissions that may occur. Thus, hospitals are at
fnancial risk or each
readmission, with no incremental revenue received or actual
readmission costs.
These two payment approaches represent the two ends o a
continuum o reorms designed to
modiy hospitals incentives under ee-or-service (FFS) to increase
the volume o admissions
including readmissions. On the one hand, P4P would continue to
pay hospitals or each
readmission, but it would reduce the level o payment to
hospitals that have relatively high rates o
readmissions. Since P4P retains FFS payment, ewer readmissions
result in lower total payments.
Payers, thereore, can immediately recoup the savings associated
with lower rates o readmission.
In contrast, episode-based payments remove all ee-or-service
incentives or hospitals to
readmit the patients they discharge. However, in the short-term,
hospitals retain the savings
associated with reduced readmissions, so there is less immediate
beneft to payers.
Variants o these payment reorms all along a continuum in terms o
how strongly they alter
the existing FFS incentives (MedPAC 2007). For example, P4P
approaches might incorporate
stronger fnancial incentives that aect a greater number o
hospitals, not only those with
above-average rates o readmission. They might also reduce,
though not eliminate, FFS
payments or each readmission.
We observe very dierent hospital responses to P4P and
episode-based payments. Each would
result in reduced readmissions and total hospital payments, but
both the magnitude o theresponse and the expected cost savings in
the short term vary. As described in the concluding
section, directly paying hospitals to undertake one o the
evidence-based interventions to
reduce readmissions (Project RED) might yield both more change
in hospital processes o care
and more savings to payers than instituting payment
incentives.
-
8/4/2019 Readmission report
33/51
25
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Reform Simulations (continued)
ospt Rspons to p4p
The P4P simulation assumed that each hospital would receive
reduced payment in 2008 iits readmissions in 2007 exceeded a
benchmark rate. The benchmark rate or each hospital
was calculated as the statewide average readmission rate in
2006, adjusted or the hospitals
case mix. For each payer, the amount o the potential payment
reduction was calculated as
the sum o payments or excess readmissions (that is, the number o
readmissions above
the benchmark rate) divided by total payments or all admissions
to that hospital. Thus, i 1%
o payments to a hospital in 2007 were or excess readmissions,
then the payment per
admission or all stays in 2008 would be reduced by 1%.
The simulation conronted each hospital with deciding whether to
implement an intervention
to reduce readmissions in 2007 in order to avoid reduced
ee-or-service payments the
ollowing year. I the hospitals expected reduction in total
payments in 2008 exceeded the sum
o its direct costs or the intervention in 2007 plus its indirect
costs (lost revenue rom reducedreadmissions) in 2007, then it would
implement the intervention to reduce readmissions.
We assumed that any hospital that chose to implement the
intervention in 2007 would continue
the intervention into 2008.
Based on this calculation, we ound that relatively ew hospitals
would undertake the cost o
an intervention to reduce readmissions: 7% o hospitals in New
York would have implemented
CTI in 2007, and 3% would have implemented Project RED (table
V.1).10
Ab V.1.Simulated Adoption o vidence-based Interventions
under
Alternative ayment Incentives, 2007
pAYNt
INCNtIV
All
HSpItAlS
HSpItAlSSubjCt
t pAYNt
INCNtIVS
HSpItAlS tHAt wuldIplNt CtI
HSpItAlS tHAt wuldIplNt pjCt d
Nub pCNtAg Nub pCNtAg
pay-fr-erfrmace
238 82 17 7.1% 6 2.5%
ide-baedayme
238 238 194 81.5% 121 50.8%
SC: ahemaica plicy Reearch aalyi f ne Yr hial dicharge daa.
Under P4P, most hospitals would decline to invest because their
2007 readmission rates were
below their benchmark expected readmission rates. These
hospitals would have aced no
payment reduction under P4P and, thereore, no beneft or reducing
readmissionsonly directand indirect costs. Among the 82 hospitals
that would have aced a payment reduction, only
a small raction would have acted to reduce readmissions.
10 we amed rae f ime referece i hi decii. ad hial diced rer i
2008, relaive he c f iveig i2007, i i ible ha ill feer hial ld have
derae he iveme ad imac readmii ld have bee illle ha e imlaed.
-
8/4/2019 Readmission report
34/51
26
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Reform Simulations (continued)
Among adopters and non-adopters o the CTI intervention, the
average readmission rate
was almost identical (17%), as were the average direct and
indirect costs o the intervention(table V.2). However, the cost o
excess readmissions among hospitals that would choose
to adopt CTI ($3.2 million) was nearly twice as large as or
non-adopters ($1.5 million). As a
result these hospitals would have aced much larger potential
payment reductions in 2008.
Ab V.2.Simulated Costs and benets o educin eadmissions or
Hospitals facin
ayment eduction under 4, 2007
Nub
fHSpItAlS
AVAg
AdISSINAt IN 2007
AVAg CSt
f xCSS
AdISSINS
IN 2007($ IllINS)
AVAg
ptNtIAl
pAYNt
duCtIN
IN 2008($ IllINS)
AVAg
pAYNt
duCtIN
AVIdd
IN 2008 If 2007
AdISSINS
A duCd($ IllINS)
AVAg
INdICt CStS
f duCINg
AdISSINS
IN 2007($ IllINS)
AVAg
dICt CStS
f duCINg
AdISSINS
IN 2007($ IllINS)
CtI
der 17 17% $3.2 $3.4 $1.8 $1.2 $0.5
n-ader
66 17% $1.5 $1.4 $0.9 $1.0 $0.4
pjCt d
der 6 23% $2.0 $2.0 $1.8 $1.2 $0.3
n-ader
77 17% $1.8 $1.7 $1.7 $3.4 $0.6
SC: ahemaica plicy Reearch aalyi f ne Yr hial dicharge daa.
Reecting the dierent populations and conditions that each
intervention targeted and
the dierence in the costs o each intervention, the hospitals
that would choose to adopt CTI
were (with just two exceptions) not the same hospitals that
would adopt Project RED (data not
shown). Hospitals that would adopt CTI expected to reduce the
incidence o the most expensive
readmissions, bringing down the cost o excess readmissions aster
than the number o
readmissions.11 In contrast, Project RED targets all medical
admissions (not only conditions
with high-cost or high-likelihood readmissions) and is
cost-eective under P4P only or hospitals
with high readmission rates across all types o medical
admissions. Hospitals that would adopt
Project RED had higher readmission rates (23% versus 17% among
non-adopters) and also aced
much lower direct and indirect costs to achieve the same beneft
as non-adopters.
Among hospitals that would decide to invest in reducing
readmissions, the business case
or doing so was generally strong. Calculated across all
hospitals that would implement CTI,
the estimated rate o return was 41% on an average intervention
cost o $464,000 per hospital.
11 Cmared ih prec R, he Ct iervei i mre exeive er dicharge b
arge a maller mber f high-c,high-readmii cdii ch a cgeive hear
failre. the imlai rel migh chage if readmii erfrmaceder hee p4p
refrm ere baed umberf readmii abve he execed mber raher ha c f
readmiiabve he execed c.
-
8/4/2019 Readmission report
35/51
27
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Reform Simulations (continued)
The estimated rate o return or hospitals that would implement
Project RED was still greater:
112% on an average intervention cost o $292,000 per hospital
(table V.3).
Ab V.3.Simulated Hospital Costs and benets o Implementin
vidence-based Interventions under
Alternative ayment Incentives, 2007
HSpItAlS tHAt wuld IplNt CtI
HSpItAlS tHAt wuld IplNt
pjCt d
pAYNt INCNtIV
Nub f
HSpItAlS
AVAg
dICt CSt
($ tHuSANdS)
AgggAt
At
f tuN
Nub
f
HSpItAlS
AVAg
dICt CSt
($ tHuSANdS)
AgggAt
At
f tuN
pay-fr-erfrmace 17 $463.7 41% 6 $291.9 112%
ide-baed ayme 194 $415.0 111% 121 $711.4 75%
SC: ahemaica plicy Reearch aalyi f ne Yr hial dicharge daa.
NS: verage dllar am are rered er hial. the average rae f rer der
ay-fr-erfrmace i calclaed a he dicedredci i he ayme ealy i 2008, e
f l readmii revee ad iervei c, a a erceage f he iervei c. the rae
frer der eide-baed ayme i he redci i reimbred readmii a a erceage f
iervei c.
ospt Rspons to pso-Bs pYntsWe expect that revenue-maximizing
hospitals would be uniormly more responsive to episode-
based payments than to P4P (as we modeled these approaches).
Under episode-based
payments, hospitals would receive an enhanced payment or a
patients initial admission, but no
payments or any subsequent readmission within 30 days. The
enhanced payment is equivalent
to the hospitals current ee-or-service payment or the initial
stay, plus an additional payment
intended to cover the average cost and likelihood o readmission
or any reason.12 Hospitals that
successully reduce readmissions to below the average statewide
rate retain the dierence.
In each subsequent year, episode-based payments would be rebased
to the current statewidereadmission rate, reecting hospital
responses to episode-based payment incentives.
Because hospitals do not lose revenue rom reducing readmissions
(they are no longer paid
ee-or-service or each readmission), they undertake investment i
the beneft o avoiding an
unreimbursed readmission costs exceeds the cost o the
intervention. In addition, all hospitals
stand to beneft rom reducing readmissions under episode-based
payment, not only those
hospitals with relatively high case-mix-adjusted readmission
rates.
Consistent with hospitals universal exposure to episode-based
payment incentives, our out o
fve hospitals (82%) would implement CTI, and more than hal (51%)
would implement Project
RED (table V.1). As was the case under pay-or-perormance, more
hospitals making a cost-
beneft calculation would adopt CTI (which targets high-cost,
high-readmission conditions),
despite the higher average cost o CTI compared with Project
RED.
12 the lielihd f readmii fr ay rea ihi 30 day i baed he aeide
average readmii rae fr he R. a rel,hial ih ler-ha-execed readmii
rae give heir cae mix ld receive higher ayme ha hey crrely d derhe
FFs yem, hile hial ih ler-ha-execed readmii rae ld exeriece ayme
redci cmared hecrre ayme yem.
-
8/4/2019 Readmission report
36/51
28
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Reform Simulations (continued)
As under P4P, the hospitals that would implement either CTI or
Project RED under episode-
based payments generally had a strong business case or doing so.
The estimated rate oreturn among hospitals that would implement CTI
was 111% on an average intervention cost
o $415,000 (table V.3). Among those that would implement Project
RED, the estimated rate o
return was 75% on an average intervention cost o $711,444.
FFCt on t nuBR oF RssonsThe simulations assumed hospitals would
succeed in reducing all-cause readmissions at
about the same rate as reported in the research literature when
they adopted CTI (35%) or
Project RED (30%) (Kanaan 2009; Jack et al. 2009). Assuming that
all payers adopt P4P, New
York hospitals would have readmitted an estimated 1,000 to 2,000
ewer patients (depending on
the intervention)0.5 to 1% ewer readmissions than actually
occurred in 2008. The hospitals
that would fnd it cost-eective to implement Project RED were
mostly small hospitals with
relatively ew stays; in contrast, three times as many hospitals
would fnd it cost-eective to
implement CTI. Consequently, statewide readmissions would have
allen less with the adoption
o Project RED (by about 1,000 stays in 2007 and 2008) than with
the adoption o CTI (by 2,000
stays), notwithstanding CTIs ocus on a narrower range o
diagnoses (table V.4). Assuming that
hospitals that invest in reducing readmissions in 2007 would
continue that investment in 2008,
the percentage reductions in readmissions would have been
similar in both years.
Ab V.4. Simulated ects o ayment Incentives on eadmission ates,
20072008
Nub f AdISSINS
(IN tHuSANdS)
CHANg IN AdISSINS
Nub (IN tHuSANdS) pCNtAg
ACTUAL ExPERIENCE:
2007 263.1 /a /a
2008 273.6 /a /a
PAY FOR PERFORMANCE:
CA tANSItINS INtVNtIN (CtI)
2007 261.1 -2.0 -0.8%
2008 271.5 -2.0 -0.7%
pjCt d INtVNtIN
2007 261.9 -1.2 -0.5%
2008 272.3 -1.3 -0.5%
EPISODE-BASED PAYMENTS:
CA tANSItINS INtVNtIN (CtI)
2007 244.4 -18.7 -7.1%
2008 254.3 -19.2 -7.0%
pjCt d INtVNtIN
2007 220.1 -43.0 -16.3%
2008 228.9 -44.7 -16.3%
SC: ahemaica plicy Reearch aalyi f ne Yr hial dicharge daa.
N: ial ha imlemeed he iervei i 2007 are amed cie imlemeai i
2008.
-
8/4/2019 Readmission report
37/51
29
Reducing Hospital Readmissions in New York State: A Simulation
Analysis of Alternative Payment Incentives
Payment Reform Simulations (continued)
Because many more hospitals would respond to episode-based
payments, the reduction
in readmissions in 2007 and 2008 would have been substantially
greater. Depending on theintervention, the reduction in
readmissions under episode-based payments would have ranged
rom 19,000 ewer readmissions (7%) i hospitals had considered
adopting CTI, to 45,000 ewer
readmissions (16%) i they had considered adopting Project
RED.
FFCt on ospt pYntsReducing the number o readmissions generates
cost savingsbut depending upon the
payment method used, either payers or hospitals may realize
those savings in the short
term. When hospitals are paid FFS, payers immediately capture
the cost savings rom ewer
readmissions. Unless modifed (or example, by P4P) FFS oers
hospitals no fnancial reason
to help patients avoid readmission. In contrast, when hospitals
assume ull risk (as would occur
with episode-based payments) they capture nearly all o the
short-t