Embed Size (px)
Citation preview

Nutrition: A Co-factor in
HIV Infection/AIDS Progression
Phara JourdanRosabelle CamposMarch 28, 2005

Outline Trends & Prevalence Overview of HIV Infection/AIDS Application of HAART AIDS Wasting Syndrome HIV-Associated Lipodystrophy Nutritional Interventions Case Study Summary Discussion
HIV/AIDS Worldwide
• 38 million people live with HIV/AIDS worldwide.
• Sub-Saharan Africa is home to 70% of the people living with HIV.
• 2.1 million children are infected with HIV/AIDS in the world

Top HIV/AIDS-Infected Countries
1. South Africa
2. Nigeria
3. Zimbabwe
4. Tanzania
5. The Congo
6. Ethiopia
7. Kenya
8. Mozambique
Source: Steinbrook R. The AIDS epidemic in 2004. NEJM. 2004;351:115-117.
9. United States
10. Russian Federation
11. China
12. Brazil
13. Thailand
Sub-Saharan Africa

AIDS Rates reported in 2002, US

Proportion of AIDS Cases, by Race/Ethnicity

AIDS = Acquired Immune Deficiency Syndrome
Acquired - because it's a condition one must acquire or get infected with, not something transmitted through the genes
Immune - because it affects the body's immune system, the part of the body which usually works to fight off germs such as bacteria and viruses
Deficiency - because it makes the immune system deficient
Syndrome - because someone with AIDS may experience a wide range of different diseases and opportunistic infections
Modes of Transmission
Unprotected intercourse
Injection drug use
Other unsafe injections
Blood transfusions
Direct blood contact
Mother to child
Sources: 2004 Report on the global AIDS epidemic. Geneva: Joint United Nations Program on HIV/AIDS, July 2004. Steinbrook R. The AIDS epidemic in 2004. NEJM. 2004;351:115-117.
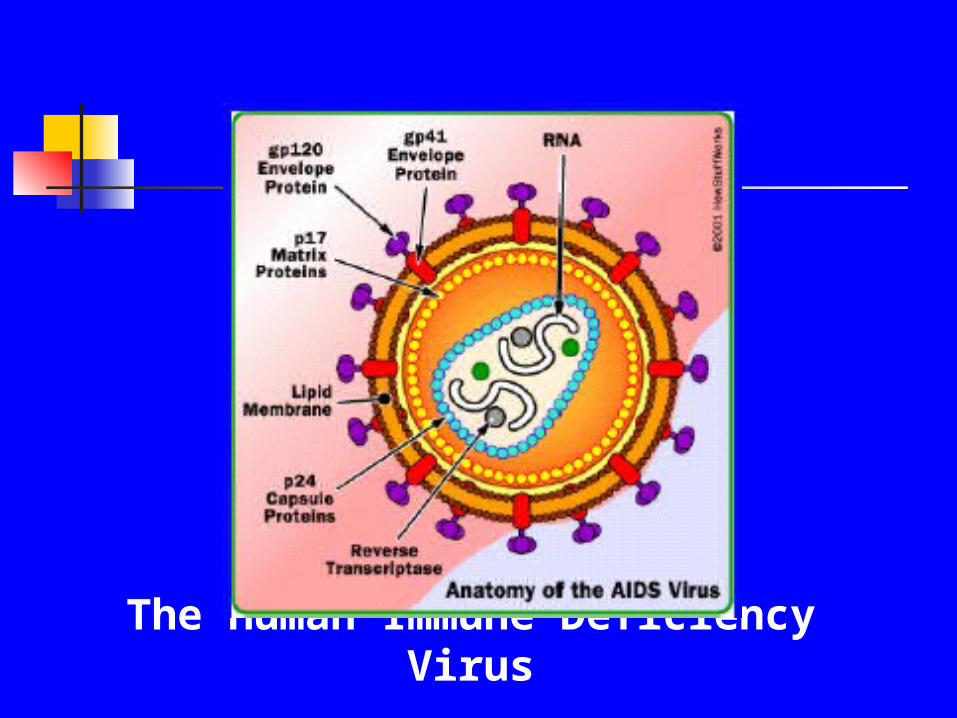
The Human Immune Deficiency Virus

Pathophysiology of HIV/AIDS
A retrovirus unknown until early 1980s: 1. Cannot replicate outside of living host
cells 2. Contains only RNA; no DNA 3. Destroys the body’s ability to fight
infections and certain cancers4. Infects CD4 cells – the primary target of HIV infection
Patients infected with HIV are at risk for illness and death from:1. Opportunistic infections2. Neoplastic complications

CD4 Count in HIV infection
The CD4 cell , also known as "T4" or "helper T cell“ is responsible for signaling other parts of the immune system to respond to an infection.
Normal counts range from 500 to 1500 cells per cubic millimeter of blood
Initially in HIV infection there is a sharp drop in the CD4 count and then the count levels off to around 500-600 cells/mm3.
CD4 count is a marker of likely disease progression. CD4 percentage tends to decline as HIV disease progresses.
CD4 counts can also be used to predict the risks for particular conditions such as Pneumocystis carinii pneumonia, CMV disease or MAI disease.
Treatment decisions are often based on Viral Load and CD4 count.

Natural History of Untreated HIV Infection

Opportunistic Infections

Manifestations of HIV Infection
Primary Infection Clinical Latency Advanced Disease
often asymptomatic or overlooked
symptoms 1-6 weeks after infection
viral like syndrome: sore throat, fever, lymphadenopathy, rash
differential includes EBV, CMV, hepatitis, toxoplasmosis
antibody (ELISA, Western Blot) may not be detected
usually asymptomatic
lymph nodes site of ongoing viral latency
massive viral production
destruction of CD4 cells
a decrease in lean body mass without apparent total body weight change
vitamin B12 deficiency
increased susceptibility to food and water-borne pathogens.
Symptomatic
Plasma viremia begins to rise
CD4 cell count falls further
A decline in nutrient status or body composition
Opportunistic infections develop: fever, weight loss, lymphadenopathy, thrush, diarrhea, malignancies, wasting syndrome, neurologic syndrome including dementia

AIDS Defined
HIV positive with a CD4 cell count that is or has been less than 200 cells/mm3
HIV positive with a CD4 percent below 14%.
HIV positive and with an AIDS defining illness such as PCP, toxoplasmosis, MAC, Kaposi’s Sarcoma, etc. regardless of CD4 cell count

Antiviral Drug Therapy
Nucleoside/Nucleotide
Analogues
Nonnucleoside Reverse
Transcriptase Inhibitors
Protease Inhibitors
Fusion Inhibitors
Abacavir Didanosine Emtricitabine Lamivudine Stavudine Tenofovir Zalcitabine Zidovudine
Delavirdine Efavirenz Nevirapine
Amprenavir Atazanavir Fosamprenavir Indinavir Lopinavir/Ritonavir Nelfinavir Ritonavir Saquinavir
Enfuvirtide
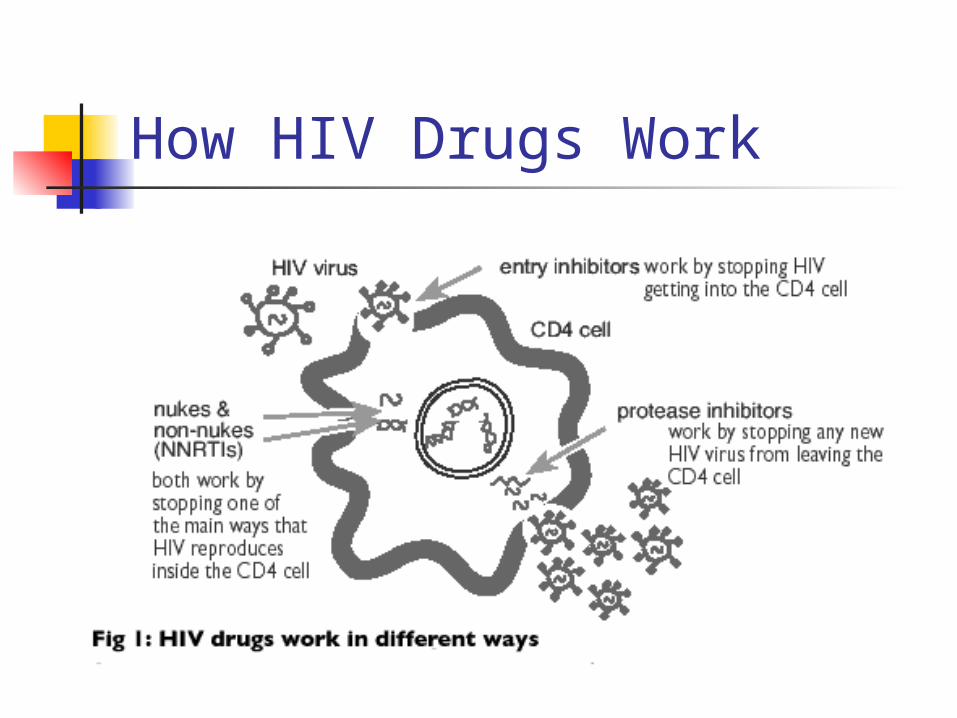
How HIV Drugs Work

Adverse Drug Effects
Mitochondrialdysfunction
Metabolic abnormalities
Hematologiccomplications
Allergic reactions
Lactic acidosis
Hepatic toxicity
Pancreatitis
Peripheral neuropathy
LipodystrophyFat accumulationLipoatrophy
Hyperlipidemia/ ? Premature CAD
Hyperglycemia
Insulin resistance/DM
Bone disorders: oesteoporosis and osteopenia
Bone marrowsuppression
Hypersensitivityreactions
Skin rashes

Medication Side Effects
Anorexia Sore/dry/painful mouth Swallowing difficulties Constipation/Diarrhea Nausea/Vomiting/Altered Taste Depression/Tiredness/Lethargy

Pathogenesis of Malnutrition
in HIV Infection

Malnutrition can...
√ Contribute to impaired immune response√ Result in more rapid disease progression
& shortened survival√ Contribute to increased frequency and
severity of infections√ Result in fatigue, loss of appetite, sense
of taste and smell, and decreased quality of life
√ Decrease tolerance to therapy and lessen medication efficacy

Weight Loss: Independent Predictor of Mortality Weight loss and wasting have been predominant features of HIV
disease progression since the beginning of the HIV/AIDS epidemic and have long been established as strong predictors of morbidity and mortality in patients infected with HIV.
Several studies in the pre-HAART era showed that HIV-related wasting was strongly associated with more rapid disease progression and increased mortality in HIV-infected patients.
With the advent of HAART and prophylaxis for opportunistic infections, many AIDS-defining illnesses that were previously frequent are now rarely seen in successfully treated patients.
So the prevalence of HIV-related wasting syndrome has greatly diminished ; however, several studies have concluded that patients treated with HAART were still at risk for wasting.
Wanke et al. found that ~1/3 of HIV-infected patients in the NFHL study who were treated with HAART were still at risk for wasting. Thus weight loss, regardless of treatment status, remains a strong predictor of death.

‘The Wasting Syndrome’ The wasting syndrome is defined as weight loss
>10% of baseline body weight with chronic fever, weakness, or diarrhea in the absence of other related illnesses contributing to the weight loss.
‘unexplained weight loss’ believed to be due to the HIV virus
The wasting syndrome is so common in HIV infection that it is classified according to the Center for Disease Control (CDC 1987) as a diagnostic indicator of AIDS.

Pathophysiology AIDS Wasting
Oxidative Stress Micronutrient Deficiency
Malabsorption/Dysphagia
Dietary Intake
Negative EnergyBalance
Intestinal Parasites
Protein Loss
Fat Loss
HIV
OpportunisticInfectionImmune Function
Pro-inflammatory Cytokines (TNF alpha)
Anorexia
Metabolic Rate
Endocrine Disorder
Skeletal Protein BreakdownJ AIDS 1988

Potential Mechanisms of AIDS Wasting
1) Increased energy expenditure
2) Decreased energy intake
3) Altered metabolism4) Hormonal Alterations

Energy Expenditure
A review of the literature shows: Increased REE depending on the stage of immunodeficiency
(denoted by the CD4 count) and the presence of active infections—measured by indirect calorimetry.
Elevated REE in asymptomatic subjects A direct relationship between REE and plasma HIV viral
burden Compared with healthy controls, pts with AIDS and active
infections had a 34% increase in BMR; stable pts with AIDS were found to have 21% increase.
Melchior JC, et al, Mulligan et al

Calculating Energy Needs BWH standard is BMR x AF x SF +
weight gain (if applicable)
Injury/Stress Factors: HIV = 8-15% AIDS = 20-30% AIDS with secondary infection = 30%
Protein: 1.2 – 1.8g/kg (depending on clinical status)

Nutritional Problems
Decreased appetite may result from fever, pain, fatigue, emotional stress, and altered sensations of taste and smell due to medication side effects.
Lactose intolerance is an early effect of HIV on the intestinal tract due to the loss of lactase. The HIV infection changes the structure of the gut wall, resulting in a decreased lactase level. Intolerance results in fermentation causing abdominal cramping and a bloated feeling.
Oral Lesions, caused by Candida albicans, herpes, or Kaposi’s sarcoma can make chewing and swallowing difficult and painful.

Nutrional Problems (cont) Diarrhea and malabsorption can result from direct HIV
infection in the intestine but are more often caused by other pathogens such as bacteria, Crytosporidium, or herpes simplex that take advantage of the depressed immune system.
Medications can interfere with eating by causing GI discomfort, nausea, vomiting, diarrhea, and altered taste
Depression often leads to isolation, apathy, neglect of self-care, and diminished appetite – all which can affect immunocompetence
Socioeconomic factors play an important role in whether the patient can afford adequate and nutritious food.

Altered Metabolism Early studies documented weight loss and
protein depletion in untreated patients
The application of HAART has led to a decreased incidence of malnutrition
Syndrome of altered body fat distribution has emerged (lipodystrophy) associated with PIs
Hypertriglyceridemia, hypercholesterolemia, and insulin resistance are commonly seen in patients treated with HAART therapy.

HIV-Associated Lipodystrophy
Fat Fat atrophyatrophy
Fat Fat accumulationaccumulation
HyperlipidemiaHyperlipidemia Insulin resistanceInsulin resistance

What Causes Lipodystrophy? Syndrome most likely has a multi-factorial etiology
Most patients who have lipodystrophy started noticing symptoms while they were on triple-drug therapy.
Lipodystrophy was first reported among patients taking combinations of drugs that included a protease inhibitor (PI).
There are also some patients who have experienced one or more symptoms of lipodystrophy without taking any anti-HIV drugs at all.
It's still not clear what role these anti-HIV drugs play in the development of lipodystrophy.

What does Lipodystrophy look like?

Hormonal Factors Testosterone deficiency: Testostereone levels have
been found to be markedly reduced in some HIV-infected patients and a reduction in free serum testosterone levels correlates closely with loss of BCM.
Growth hormone resistance or deficiency: Many HIV-infected patients with hypogonadism or malnutrition display functional GH resistance.
Anabolic/Anti-catabolic agent Important in maintaining protein balance and muscle
mass

Nutritional Supplements in HIV Infection to
counteract AIDS Wasting
•MVI•Glutamine•Carnitine•Appetite Stimulant•Hormone Therapy•Resistance Training

Role of Micronutrients in the Pathogenesis of HIV infection Micronutrients play important roles in
maintaining immune function and neutralizing the reactive oxygen intermediates produced by activated macrophages and neutrophils in their response to microorganism
Micronutrient deficiencies are common among HIV infected persons.
Micronutrient deficiency has been associated with further immunopression, oxidative stress, subsequent acceleration of HIV replication and CD4+ T-cell depletion. (semba)

Fawzi et al. Study: Randomized controlled trial of multivitamin
supplementation among HIV-infected pregnant women in Tanzania.
Subjects: n=1078, 2 yr study Method: Compared supplementation consisting of
multivitamins alone, vitamin A alone, or both with placebo Results: Women who were randomly assigned to receive
multivitamin supplementation were less likely to have progression to advance stages of HIV
disease, had better preservation of CD4+ T-cell counts and lower viral
loads had lower HIV-related morbidity and mortality rates Vitamin A appeared to reduce the effect of multivitamins and,
when given alone, had some negative effects Conclusion: Multivitamin supplementation could reduce the
risk of or delay HIV-associated disease and mortality.
New England Journal Medicine, 2004

Glutamine Application in HIV/AIDS
Glutamine is the most abundant amino acid in the body and is considered a conditionally essential amino acid during periods of catabolism.
During periods of increased metabolic stress, glutamine is released freely from the skeletal muscle, and intracellular glutamine concentrations fall by more than 50%
Increased de novo synthesis of glutamine in the skeletal muscle often results in muscle-wasting syndrome
Glutamine synthesis cannot keep up with the higher requirements during stress.
Individuals deficient in glutamine manifest changes in gut morphology including increased membrane permeabilitiy resulting in bacterial translocation, malabsorption, and diarrhea
Lack of support to immunocytes and fibroblasts cause immunosuppression and impaired wound healing

Glutamine Application in HIV/AIDS (cont…) Data suggest that glutamine supplementation
offers the potential to limit skeletal muscle wasting, reduce diarrhea and malabsorption, enhance immune host defense, and reduce the incidence of opportunistic infections associated with HIV infection and AIDS Shabert J et al. Med Hypotheses. 1996;46:252-256

Glutamine: ↑body BCM in AIDS patients with Weight Loss
Double-blind, placebo-controlled trial N=26 patients with >5% weight loss since disease onset
Subjects received GLN-antioxidants (40g/d) in divided doses or glycine (40g/d) as the placebo for 12 wks.
Result: Over 3 mos, the GLN-antioxidant group gained 2.2kg in body weight (3.2%), whereas the control group gained 0.3kg (0.4%) P=0.04 for difference between groups.
The GLN-antioxidant group gained 1.8kg in body cell mass, whereas the control group gained 0.4kg (P=0.007.)
Intracellular water increased in the GLN-antioxidant group but not in the control group.
In conclusion, GLN-antioxidant supplementation can increase body weight, body cell mass, and intracellular water when compared with placebo supplementation.
Shabert J, Winslow C. et al. Nutrition 1999;15:860-864

L-Carnitine in HIV Infection Carnitine is a conditionally essential amino acid found
predominantly in red meat. It is also found in milk (human and cow’s), pork, lamb, tempeh, and supplements.
It is conditionally essential because the body can make it from lysine and methionine with assistance from Vitamin C and other compounds produced in the body.
Carnitine is synthesized in the Kidney and stored in the muscles.
Carnitine’s function is to shuttle long-chain fatty acids into the mitochondria to be utilized as fuel.
HIV/AIDS is a risk factor for carnitine deficiency
Carnitine cont’d (Morretti, et al.)
Small study (n=11), Italy Pt’s refusing ART, normal Carnitine levels, stable weight,
declining CD4 counts, asymptomatic 6 g intravenous Carnitine Qday times 150 days By second week, all subjects report increased feeling of well-
being CD4 cell counts significantly increased by day 90 and 150,
but there was an evident (non-significant) positive trend at day 15 and 30 compared to baseline.
Overall upward trend in CD8 cell counts as well Only moderate changes in plasma viral load No toxicity was reported at this level Authors conclude that carnitine targets immune system
rather than virus Authors propose possibility that carnitine’s antiapoptotic
effect could be due to antioxidant activityMorretti, et al. Effect of L-Carnitine on Human Immunodeficiency Virus-1 Infection-Associated Apoptosis: A
Pilot Study, Blood, Vol 91, No. 10, May 15, 1998: pp 3817-3824

Appetite Stimulant: Dronabinol
Derived from delta-9-tetrahydrocannabinol (major active component of Marijuana)
Useful in decreasing nausea and increasing appetite Insignificant gains or even loss of total BW May induce central nervous system events such as
anxiety, confusion, emotional lability and hallucinations, possibly addictive.
Treatment Guidelines for HIV Associated Wasting, Mayo Clinic Proceedings, April 2000

Appetite Stimulant: Megestrol Acetate (Megace) A synthetic derivative of the natural steroid hormone,
progesterone. Improved appetite in a number of studies Takes two weeks for effect. Considerable increases in BW, although mostly in body fat May be due to testosterone lowering effect, not reversed by
supplementation w/testosterone May induce or exacerbate DM, cause adrenal insufficiency
when abruptly discontinued after long-term use
Treatment Guidelines for HIV Associated Wasting, Mayo Clinic Proceedings, April 2000

Testosterone & Testosterone Analogues About half of men with advanced HIV have androgen deficiency. May contribute to muscle wasting. May be due to effects of undernutrition, chronic illness, or medications such as
Megesterol acetate’s effect on gonadotropin secretion. 25% have primary hypogondadism most often idiopathic but may be due to OI,
malignant infiltration of testes, or testicular effects of HIV infection or medication.
Most studies have shown IM testosterone supplementation to result in wt gain, increased LBM, overall feeling of well-being.
Studies of testosterone analogues show varied efficacy in improving nutritional status but may carry risks for hepatic toxic effects:
Nandrolone decanoate 100mg/mL IM q 2wks = increased BW, LBM and quality of life.
Oxymethalone 150 mg/day found to have similar results Testosterone cypionate 200mg IM q 2wks for 3 mos, no result except for
increased quality of life.
Treatment Guidelines for HIV Associated Wasting, Mayo Clinic Proceedings, April 2000

Growth Hormone AIDS pts may be growth hormone resistant. In studies of GH in AIDS pts,
doses used are significantly higher than those required for replacement. GH has been shown to increase LBM and protein synthesis and reduce urinary
nitrogen excretion. GH costs ~$18,000/yr but Medicaid has approved reimbursement, making this
therapy more accessible. Short-term use of growth hormone (12 wks) has effects on wt gain that persist
after therapy is discontinued. Using GH for short periods when required, rather than as continuous therapy
will minimize costs while maximizing patient nutritional status. Indicated for use when all other methods have failed and pt has normal
testosterone levels or on replacement testosterone for at least 4-6 wks. Contraindicated if pt has malignancyTreatment Guidelines for HIV Associated Wasting, Mayo Clinic Proceedings, April 2000

Resistance Training Supervised exercise training is a promising anabolic
strategy for pts with AIDS. Studies of exercise training have shown increased
muscle function, wt gain, strength, LBM. Effects of resistance training alone in AIDS wasting pts
remains unknown. However, use of resistance training with testosterone
and oxandralone has been shown to be effective in AIDS pts with AIDS wasting.
Journal of the American Medical Association, April 14 199, Volume 281(14), pp 1282-1290.The New England Journal of Medicine, June 3 1999
Resistance Training (cont) Strawford, et al studied 24 eugonadal men with HIV associated
wt loss. All subjects received supervised progressive resistance exercise with physiologic IM testosterone replacement 100 mg/wk to suppress endogenous testosterone for 8 weeks.
Randomization was between anabolic steroid, oxandralone, 20 mg/day and placebo.
Measured: LBM, nitrogen balance (10d met ward measure), body wt, muscle strength, and androgen status
Result: 22 completed the study (11per group). Both showed sig increase in N retention, LBM, wt, and strength. The mean gains were sig greater in oxandrolone group than in placebo, greater strength gains for upper/lower body muscle groups by max wt lifted, and dynomometry. Mean HDL cholesterol dropped sig in oxandrolone group. Protease inhibitors made no difference in outcome.
Conclusion: moderate androgen regimen (with oxandrolone) substantially increased lean tissue, strength gains from PRE, compared to testosterone replacement alone.
Journal of the American Medical Association, April 14 1999

Summary HIV/AIDS remains an epidemic worldwide Malnutrition is a complication in HIV related morbidity and
mortality Weight loss is an independent predictor of mortality Despite HAART, patients remain at risk for AIDS wasting
syndrome Contributors of AIDS wasting syndrome include increased
energy expenditure, decreased energy intake, altered metabolism, and hormonal factors
Multivitamin supplementation could reduce the risk of or delay HIV-associated disease and mortality.
Data suggest glutamine supplementation may help limit skeletal muscle wasting and increase BCM in patients with weight loss

Summary (cont) Pts have been found to be deficient in Carnitine, may benefit
from supplementation since it may have antiapoptic effect through antioxidant activity.
Appetite Stimulants may result in wt gain, but mostly in fat and may also have some negative side effects.
Testosterone deficiency may lead to wasting, supplementation may be beneficial leading to improved sense of well being, strength, etc, however Testosterone analogues may be hepatotoxic.
Correction of Growth Hormone resistance may help reverse wasting, but it is a costly intervention if pt does not have Medicaid. Short term use has been shown to be beneficial.
Resistance training has been shown to increase wt and LBM, but one study found that training plus oxandralone was most beneficial.

Discussion
Questions?

References Semba RD, Tang AM. Micronutrients and the pathogenesis of human
immunodeficiency virus infection. Br J Nutrition 1999;81:181-9. Fawzi WW, Msamanga GI, Spiegelman D, et al. A randomized trial of
multivitamin supplements and HIV disease progression and mortality. N Engl J Medicine 2004;351:23-32.
Melchior JC, Niyongabo T, Henzel D, et al. Malnutrition and wasting, immunodepression, and chronic inflammation as independent predictors of survival in HIV-infected patients. Nutrition 1999; 15:865-9
Suttmann U, Ockenga J, Selberg O, et al. Incidence and prognostic value of malnutrition and wasting in human immunodeficiency virus-infected outpatients. J Acquir Immune Defic Syndrome Hum Retrovirol 1995;8:239-46.
Silva M. Skolnik PR, Gorbach Sl, et al. The effect of protease inhibitors on weight and body composition n HIV-infected patients. AIDS 1998; 12:1645-51.
Wanke CA, Silva M, Knox TA, et al. Weight loss and wasting remain common complications in individuals infected with human immunodeficiency virus in the era of highly active antiretroviral therapy. Clin Infect Dis 2000; 31:803-5
Tang, Alice M. et al. Weight loss and survival in HIV-Positive Patients in the Era of Highly Active Antiretroviral Therapy. JAIDS 2002;31:230-236
Mittendorfer B, Gore D, Herndon D, et al. Accelerated glutamine synthesis in critically ill patients cannot maintain normal intramuscular free glutamine concentration. J Parenter Enteral Nutri. 1999;23:243-252.

References Kotler, Donald P. Nutritional Alterations Associated with HIV infection. JAIDS
2000;25:81-87 Ott M, Lambke B, Fischer H, et al. Early changes of body composition in
human immunodeficiency virus-infected patients: tetrapolar body impedance analysis indicates significant malnutrition. Am J Clin Nutr 1993;57:15-19
Melchior JC, Salmon D, Rigaud D, et al. Resting energy expenditure is increased in stable, malnourished HIV-infected patients. AM J Clin Nutr 1991;53:437-41
Rivera S, Briggs W, Qian D, et al. HIV RNA levels correlate with prior weight loss.
Mulligan k, Tai VW, Schambelan M. Energy expenditure in human immunodeficiency virus infection. N engl J Med 1997; 336:70-1.
HIV Prevalence in the United States, 2000. 9th Conference on Retroviruses and Opportunistic Infections, Seattle, Wash., Feb. 24-28, 2002. Abstract 11.
Centers for Disease Control and Prevention (CDC). HIV and AIDS - United States, 1981-2001. MMWR 2001;50:430-434.4
Centers for Disease Control and Prevention (CDC). HIV Prevention Strategic Plan Through 2005. January 2001.5.
Centers for Disease Control and Prevention (CDC). HIV/AIDS Surveillance Report 2002;14:1-40.
Gerrior, Jul. Nutritional Challenges in HIV Infection. Tufts University School of Medicine Nutrition Infection Unit

References Morretti, et al. Effect of L-Carnitine on Human Immunodeficiency
Virus-1 Infection-Associated Apoptosis: A Pilot Study, Blood, Vol 91, No. 10, May 15, 1998: pp 3817-3824
Treatment Guidelines for HIV Associated Wasting, Mayo Clinic Proceedings, April 2000, Volume 75(4), pp 386-394.
Drug Therapy: Treatments for Wasting in Patients with the Acquired Immunodefeciency Syndrome, The New England Journal of Medicine, June 3 1999, Volume 340(22), pp 1740-50.
Strawford, et al. Resistance Exercise and Supraphisilogic Androgen Thearpy in Eugonadal Men with HIV-Related Weight Loss: A Randomized Controlled Trial, Journal of the American Medical Association, April 14 1999, Volume 281(14), pp 1282-1290.
Shabert J, Winslow C, Lacey JM. Wilmore DW. Glutamine-antioxidant supplementation increases body cell mass in AIDS patients with weight loss: a randomized, double-blind controlled trial. Nutrition 1999;15:860-864.
Shabert JK, Wilmore DW. Glutamine deficiency as a cause of human immunodeficiency virus wasting. Med Hypotheses 1996;46:252-256.




![H120 SILVER - mobile.livejumping.itmobile.livejumping.it/ShowJumping/AR19028/Classifica1.pdf · 103aw41 (14) cast. bay mipa robine/(ennio ii) [own.:jourdan camilla] camilla jourdan](https://img.pdfslide.us/doc/110x75/5b76e6067f8b9ad2498ba393/h120-silver-103aw41-14-cast-bay-mipa-robineennio-ii-ownjourdan-camilla.jpg)