-
Professional Case Management Vol. 18 , No. 5 , 246 -254
Copyright 2013 Wolters Kluwer Health | Lippincott Williams &
Wilkins
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.246 Professional Case
Management Vol. 18/No. 5
CE
There have been numerous studies attempting to defi ne case
management roles, responsibilities, and essential functions (Tahan
& Campagna, 2010). Given the diversity of settings, case
manage-ment models, and organizational idiosyncrasies, most studies
tend to produce vague, overgeneralized fi nd-ings and one-size-fi
ts-all assertions. Responses to survey questions often refl ect
research bias, given the tendency to provide socially desirable
responses. The American Nurses Credentialing Center (ANCC)
conducted an extensive Nursing Case Management Role Delineation
Study, identifying 66 work activities ranked hierarchically by
overall criticality (ANCC, 2011, p. 6). The ANCC (2011) states,
Role delin-eation or job analysis studies are typically carried out
at the national level with the goal of describing current practice
expectations, performance require-ments, and environments. ANCC has
a current goal of conducting a study of each specialty
approxi-mately every three years in order to capture changes in
work activities and the knowledge and skill areas required to
perform those activities. The fi ndings are used to update the
content of its respective certifi ca-tion examination (p. 5). But
do role and function studies actually capture the day-to-day
involvement, interests, and struggles of hospital case
managers?
Hospital case managers have been described as professionals in
the hospital setting who ensure that
patients are admitted and transitioned to the appropri-ate level
of care, have an effective plan of care and are receiving
prescribed treatment, and have an advocate for services and plans
needed during and after their stay (Wikipedia, n.d., para. 3). Key
roles associated with hospital case management include variance
analy-sis, care coordination, optimal patient and hospital
out-comes, quality of care, effi cient resource utilization, and
reimbursement for services (Wikipedia, n.d., para. 3). Phaneuf
(2008) provides an extensive overview of the nursing case
management role. However, the overview fails to capture the present
inordinate emphasis on Cen-ters for Medicare and Medicaid Services
(CMS) compli-ance and utilization review. One study reports, Almost
two thirds of case managers say that patient satisfaction is the
number one factor they consider when evaluat-ing a case managers
performance (Health Law and Regulation, 2010, para. 3). Others
stress, Case manag-ers freed from the need to perform routine chart
reviews can work with physicians to manage progression of
Address correspondence to John J. Reynolds, BA, LCSW, Care
Management & Patient Access, Saint Vincents Medical Center, 47
Long Lots Rd., Westport, CT 06880 ( [email protected] )
The author reports no confl icts of interest.
A B S T R A C T
Purpose of the Study: The purpose of this study was to identify
the roles, functions, and types of activities that hospital case
managers engage in on a day-to-day basis and that leverage the most
amounts of time. Previous studies superimpose a priori categories
on research tools. Practice Setting: Hospital case management.
Methodology and Sample: This study analyzes 4,064 spontaneous,
unstructured list serve postings from the American Case Management
Association Learning Link list serve from August 15, 2011, to
August 18, 2012. The study group was a cross section of 415 case
management professionals. Implications for Practice: The data
suggest that hospital case managers time is inordinately leveraged
by issues related to observation status/leveling of patients and
the Centers for Medicare and Medicaid Services compliance. The data
also suggest that hospital case management has taken a conceptual
trajectory that has deviated signifi cantly from what was initially
conceived (quality, advocacy, and care coordination) and what is
publicly purported. Case management education and practical
orientation will need to be commensurate with this emerging
emphasis. Case management leadership will need to be adept at
mitigating the stresses of role confusion, role confl ict, and role
ambiguity.
Key words: compliance , functions , role confl ict , roles
Another Look at Roles and Functions Has Hospital Case Management
Lost Its Way?
John J. Reynolds , BA, LCSW
DOI: 10.1097/NCM.0b013e31829c8aa8
NCM200342.indd 246NCM200342.indd 246 7/30/13 7:24 PM7/30/13 7:24
PM
-
Vol. 18/No. 5 Professional Case Management 247
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.
managers are immersed in, the author conducted a content
analysis of 4,064 list serve postings on the American Case
Management Association (ACMA) Learning Link, from August 18, 2011,
to August 18, 2012. ACMAs Learning Link is described as a vast
electronic network that connects members through an e-mail list
serve. Members ask questions and share their experiences, tools,
resources, successes, and per-spectives. When you have a question
or challenge, over 2,500 case management professionals are only an
e-mail away. Learning Link is provided as a Mem-ber benefi t of the
American Case Management Asso-ciation (ACMA website, n.d.; Learning
Link: Whos in Your Network? para. 2 and 3). Also, it should be
noted, ACMA accepts no responsibility for the opin-ions and
information posted on this site by others. ACMA disclaims all
warranties with regard to infor-mation posted on this site, whether
posted by ACMA or any third party (ACMA website, n.d., Learning
Link Disclaimer & Legal Rules, para. 1).
Postings were placed by 415 hospital case man-agers and
physicians. Postings were categorized by subject heading and
assessment of content for salient themes. Subject categories are
not mutually exclusive, because postings might cross-reference
other catego-ries. As with all studies, data interpretation rests
on certain assumptions. These data assume that the case managers
postings on the ACMA Learning Link are a representative sample of
hospital case management professionals and medical consultants.
Therefore, the fi ndings are subject to multiple interpretations.
Figures 1 to 3 are accompanied by a glossary that operationally
defi nes the fi gure categories.
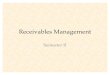
FINDINGS
The data illustrate that the issues related to the CMS
compliance, 719 posts (18%), and specifi cally observa-tion status
and the accurate leveling of patients, and 935 posts (23%), have
emerged as an intractable lever-age of time for hospital case
managers ( Figure 1 ). It is surprising that observation status was
identifi ed as a problem area in 1994, with the Health Care
Financing Administration publishing rules for appropriate
utili-zation of observation status in 1996, followed by the
inclusion of observation status in the Offi ce of Inspector General
Work Plan in 1998 (HCPro Inc, 2008). Utiliza-tion review committees
have been authorized to change patients status from inpatient to
outpatient since 2004 (Center for Medicare Advocacy, n.d.).
Nonetheless, despite more than 18 years of grappling with the
issue, hospital case managers seem shackled to observation status
and the appropriate leveling of patients.
Discharge planning/care transitions ranks a dis-tant third with
579 posts (14%), and best practice/quality only (6%),
metrics/outcomes 77 posts (2%).
care from hospital to community (Daniels & Frater, 2011,
para. 3). In The Gestalt of Case Management, Powell (2012) notes
the following job titles encompass-ing case management: care
coordinator; case manager; care manager; clinical resource
coordinator; guided care nurse; health coach; medical home care
coordina-tor; patient navigator; patient motivator; resource
coor-dinator; resource manager; transition coach; utilization
manager; and discharge planner.
The Case Management Society of America (2010) promulgates the
following standard for case manage-ment: Case management is a
collaborative process of assessment, planning, facilitation, care
coordination, evaluation, and advocacy for options and services to
meet an individuals and familys comprehensive health needs through
communication and available resources to promote quality cost
effective outcomes (p. 8).
The Case Management Society of America 2010 standards (p. 7)
assert that their standards refl ect many changes in the industry,
which resonate with current practice today. Some of these changes
include the following:
Minimizing fraxgmentation in the health care system
Incorporating adherence guidelines and other standardized
practice tools
Using evidence-based guidelines in practice Expanding the
interdisciplinary team in planning
care for individuals Navigating transitions of care Improving
patient safety
The underlying premise of case management is based in the fact
that, when an individual reaches the optimum level of wellness and
functional capability, everyone benefi ts: the individuals being
served, their support systems, the health care delivery systems,
and the various reimbursement sources. Case management serves as a
means for achieving client wellness and autonomy through advocacy,
communication, education, identifi cation of service resources, and
service facilitation. Case management services are best offered in
a climate that allows direct communication between the case
manager, the client, and appropriate service personnel, in order to
optimize the outcome for all concerned. (Case Management Society of
America, 2010, p. 9)
Although laudatory, do these high-level rhetori-cal statements
of standards resonate with actual hos-pital case management
activity?
METHODOLOGY
In an attempt to cast light on the actual day-to-day roles,
tasks, functions, and issues that hospital case
NCM200342.indd 247NCM200342.indd 247 7/30/13 7:24 PM7/30/13 7:24
PM
-
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.248 Professional Case
Management Vol. 18/No. 5
Utilization review has a primary goal that is adminis-trative in
nature, that is, to place patients in the proper status and fulfi
ll our obligation to provide assistance as to the optimal
utilization of resources and patient care. It is stated at the
outset that these issues are marked by potential confl ict between
patient care and plac-ing barriers to that care (p. 263). Daniels
and Reece (2007) state, Because their work was heavily centered on
utilization review tasks, nurses became the chart police and the
instruments for growing chart review activities, such as core
measure abstracting, medi-cal documentation review, concurrent
coding assign-ments, safety indicators, and numerous other
perfor-mance improvement projects. The idea of resource
appropriateness, advocacy, and navigation through the episode of
care, cost reductions, and improved qual-ity vanished, except for
an obligatory mention in the job description (para. 3). The 4,064
ACMA Learn-ing Link postings call into question the initial vision
of case management. With the big picture perspec-tive, the hospital
case manager harnesses the collective wisdom of the clinical team
to assess, plan, and con-tinuously evaluate the patients post-acute
experience (Phoenix Medical Management, n.d., para. 6).
Figure 2 integrates the combined impact of CMS com-pliance
issues and distinct compliance and revenue integrity issues related
to observation status account-ing for 1,654 (41%) of all postings.
If we were to consider the revenue implications of compliance and
observation and combine those categories with Bill-ing, Utilization
Review Criteria, Physician Advisor, and Denials, Figure 3
illustrates a combined impact of 2,348 (58%). This is signifi cant,
because case manag-ers often fi nd that organizational business
imperatives often confl ict with other facets of their professional
identity, such as patient advocate. Of note is that Team Building
received less than 1% of the overall postings. This may suggest
that Team Building has been satisfactorily addressed by
organizations or that other activities preclude team building
activities.
DISCUSSION
The frequency distribution among categories suggests that
hospital case management is strategically posi-tioned to impact
revenue and manage risk. However, has it done so at the opportunity
cost of commitment to quality and patient advocacy? Cohen (2012)
notes,
FIGURE 1 Hospital case management role and function as refl
ected by American Case Management Association Learning Link posts
from August 15, 2011, to August 18, 2012 (n = 4,064). ADM =
admission; DCP = discharge planning; DOC = documentation; ED =
emergency department; JD = job description; OBS = observation; OP =
outpatient.
935
719579
259 236 202 179 163 156 122 116 106 77 76 74 30 190
100200300400500600700800900
1000
OBS/A
DM ST
ATUS
COMP
LI
DCP/T
RANS
BEST
PRAC
STFF
NG
CRITE
RIA
DENIA
LS
BILLN
G
SOFT
WARE JD ED
READ
M
OUTC
OMES
PHYA
DV DOC OP
TEAM
Post
s
b
a
MISC0%
TEAM0%
OP1%
DOC2%
PHYSADV2%
METRICS2%READM
3% ED3%JD3%
SOFTWARE4%
BILLNG4%
DENIALS4%
CRITERIA5%STFFNG
6% BESTPRAC6%
DCP/TRANS14%
COMPLI18%
OBS/ADM STATUS23%
OBS/ADM
STATUSCOMPLIDCP/TRANSBESTPRACSTFFNGCRITERIADENIALSBILLNGSOFTWAREJDEDREADMMETRICSPHYSADVDOCOPTEAMMISC
NCM200342.indd 248NCM200342.indd 248 7/30/13 7:24 PM7/30/13 7:24
PM
-
Vol. 18/No. 5 Professional Case Management 249
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.
FIGURE 2 American Case Management Association Learning Link
posts. DCP = discharge planning; ED = emergency department; OP,
outpatient.
FIGURE 3 American Case Management Association Learning Link
posts by major category and percent.
1654
831 694492 358
16190
200400600800
10001200140016001800
COMP
LIANC
E
CARE
TRAN
S
DENI
ALS
BEST
PRAC
STFF
NGTE
AM MISC
MISC0.4%
TEAM0.5%STFFNG
9%
BESTPRACT12%
DENIALS17%
CARE TRANS20%
COMPLIANCE41%
COMPLIANCECARE TRANSDENIALSBESTPRACTSTFFNGTEAMMISC
a
b
NCM200342.indd 249NCM200342.indd 249 7/30/13 7:24 PM7/30/13 7:24
PM
-
250 Professional Case Management Vol. 18/No. 5
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.
no admitting privileges, write transitional orders that are
confused with admission orders. The confl uence of these forces
creates massive amounts of re-work that case managers are held
accountable to unravel at the back end. Compliance offi cers,
Departments of Revenue Integrity, too often take a step back,
defer-ring to case managers who then assume responsibil-ity and
liability for any missteps in what is the conver-gence of several
volatile issues, leaving hospital case managers as the repositories
for risk assumption.
A review of legal and regulatory issues seems to focus
exclusively on Protected Health Informa-tion ( Muller, 2012 ,
2013). This is consistent with the 2010 ANCC Role Delineation Study
Overview sur-vey fi ndings, which ranked, maintains clients con-fi
dentiality as the number one work area relative to overall
criticality for hospital case managers (ANCC, 2011, p. D2).
However, the slippery slope of case managements entry into billing
compliance, admis-sion status determination, revenue integrity, and
interpretation of CMSese as it explains, or tries to, CMS
regulatory stipulations for billing and take backs have received
little attention as a professional practice issue. In fact, the
ANCC survey question, Reviews level of care based on utilization
review cri-teria, did not rank in the surveys top-20 work items
relative to overall criticality (ANCC, 2011, pp. 12).
There has been a consistent failure to capture this shift as a
professional practice issue and to offer guid-ance as how to
navigate the changing landscape. Per-haps the 2011 American Case
Management Associa-tion National Hospital Survey (pp. 3233; this
survey is available to ACMA members only) is instructive, while
noting a statistically signifi cant increase in the number of case
management departments reporting to operations and other
departments, whereas the number of departments reporting to
nursing/patient care services is almost equal to the number
reporting to fi nance. This fi nding is again refl ected in the
2013 ACMA National Hospital Case Manage-ment Survey (p. 23). Role
confusion, role ambiguity, role confl ict, and role tension have
emerged as central themes in defi ning case management integrity as
a practice specialty. There is evidence to suggest that, in varying
degrees, these practice strains have not only job satisfaction and
job effectiveness implications but mental health ramifi cations
relative to burnout
Does the dominance of CMS compliance, patient assignment, and/
or leveling signify a risk that would fragment the unifi ed skill
set of case management into individual elements creating the
biggest threats to case management to building recognition of, and
consistency in, the professional practice of case man-agement? (
Powell, 2012 , p. 228). I believe that the implications of the
issue are exquisitely expressed in Smiths (2011) treatment of role
ambiguity, role con-fusion, and role confl ict in hospital case
managers.
Although less overt than in the past and ample rhetoric to the
contrary, many health care organizations continue to harbor a
culture of blame. Because hospi-tal operating margins continue to
shrink, determining patient status and the concomitant compliance
and operational implications have engendered increasing amounts of
audit anxiety and undermine team cohe-sion. I have seen the
abdication of other disciplines rel-ative to Observation and
patient leveling create a void that case managers have been
compelled to fi ll. From the framework of thermodynamic theory,
entropy is a measure of a systems energy that is unavailable for
work or of the degree of a systems disorder or trend toward
disorder (Entropy, n.d.). I would argue that the inordinate
reliance on Case Management Assignment Protocols and other fi
rst-level review screening meth-odologies signify hospital case
managers confronting a state of organizational and physician
entropy. Because there is not a suffi cient energy contribution by
other sources, hospital case managers compensate for a mul-titude
of organizational systemic defi cits on the road to professional
burnout.
In my own experience, with rare exception, the physician
community has taken the stance that the leveling of patients is an
administrative, nonclinical issue. Medical coders who have their
own creden-tialing and practice guidelines consistently ask case
managers how they should code on the basis of what the physician
has (or has not) documented. Organi-zational goal misalignment
manifests as Emergency Departments move patients out at a rate of
accel-eration that precludes hospitalists accurately leveling a
patient at the point of entry. Emergency department registration
processes frequently do not cohere to clin-ical/regulatory
requirements by using the colloquial of Admit and Observation and
create a web of confusion. Emergency department physicians,
with
In an effort to justify and prove our organizational worth,
perhaps case management leaders inadvertently contribute to the
myriad confl uence of varied roles and
expectations that are assumed and consequently required of
staff. Or, maybe as helping professionals, we are all too willing
to have our capacity to care exploited as
we compensate for organizational and leadership voids.
NCM200342.indd 250NCM200342.indd 250 7/30/13 7:24 PM7/30/13 7:24
PM
-
Vol. 18/No. 5 Professional Case Management 251
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.
containment and fi nancial issues; some perceived this
expectation as confl icting with their role as patient advocate and
created tension as well as decreased job satisfaction and
self-confi dence. Also was noted the participants perception of not
being aware of the aspects of the case management role and of not
being prepared for the role and not aware of the aspects of case
management that would be problematic (Smith, 2011, p. 184). Gray,
White, and Brooks-Buck (2013) astutely note, it is clear that role
confl ict and role ambiguity are important intervening variables
that mediate the effects of various organizational practices on
individual and organizational outcomes (p. 69). The authors also
found that many responses indicate that there is role confusion and
confl ict and ambigu-ity related to the areas of time, resources,
capabilities, and the multiplicity of roles and responsibilities.
Nurse case managers are held to different sets of stan-dards that
could be at odds with each other (p. 72).
It is true that case managers are a unique segment of the
healthcare workforce, therefore, their unique role needs to be
clearly articulated if the specialty is to gain industry-wide
recognition and standardiza-tion (Gray et al., 2013, p. 72).
However, there is a good reason to believe that case management has
become the Swiss Army Knife of health care, engaged in quality,
utilization management, denial man-agement, family intervention,
discharge planning, compliance, etc. (see Figure 4 ). Although a
seeming organizational convenience, the Swiss Army Knife
as hospital case managers endeavor to reconcile the many roles
and expectations in a manner that is pro-fessionally
acceptable.
In an effort to justify and prove our organiza-tional worth,
perhaps case management leaders inadvertently contribute to the
myriad confl uence of varied roles and expectations that are
assumed and consequently required of staff. Or, maybe as helping
professionals, we are all too willing to have our capac-ity to care
exploited as we compensate for organiza-tional and leadership
voids. Smith (2011) has written insightfully about role ambiguity
and role confu-sion for nurses transitioning from bedside to
nursing case management. Specifi cally, within the business culture
and fi nancial objectives theme, participants revealed feelings of
confl ict and being at odds with the employer regarding the
expected focus on cost
FIGURE 4 Hospital case management and role confusion case
management as the Swiss Army Knife of health care. HIM =health
information management; RAC = recovery audit contractors.
John J. Reynolds
Utilization management
Quality improvement Risk
management
Discharge planning
Outcomes monitoring
Tracking variances
Regulatory compliance
Pt./Family advocacy
Teamleader
Observation/inpatient only
Billing
HIM consultant
RAC take backs
Care progression
Core measures
The frequency distribution among categories suggests that
hospital case
management is strategically positioned to impact revenue and
manage
risk. However, has it done so at the opportunity cost of
commitment to
quality and patient advocacy?
NCM200342.indd 251NCM200342.indd 251 7/30/13 7:24 PM7/30/13 7:24
PM
-
252 Professional Case Management Vol. 18/No. 5
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.
and update where needed. Revise departmental orientation as
indicated.
Use relevant articles and case vignettes at staff meetings to
support staff and foster the coordi-nation and integration of
specialties.
Utilize guest speakers who are subject-matter experts to support
training and departmental curriculum development.
Develop presentations for professional work-shops and
conferences that address the changing landscape and related skill
sets while focusing on maintaining a commitment to core values.
The multitude of titles, functions, and activities that hospital
case managers fi nd themselves engaged in is testament to case
managements organizational value. It is no wonder that hospital
case managers report role strain, role ambiguity, role confl ict,
and feelings of burnout. Nonetheless, hospital case man-agement
cannot be allowed to become a victim of its own aspirations and its
own success.
Operational Defi nitions
Best practice/quality: Standards of care for spe-cifi c disease
states, professional articles, certifi ca-tion, The Joint
Commission compliance.
Billing: Non-RAC, billing-related issues. Compliance:
CMS-related guidance and regula-
tory adherence. Observation: Admission status orders, RAC,
pre-
payment reviews, utilization management plans. Care Transition:
Diffi cult discharges, discharge
assistance programs, discharge resources, trans-fer centers;
readmissions; emergency department; outpatient.
Denials: Non-CMS utilization review activity, denial management,
criteria
Documentation: Issues related to clinical docu-mentation
improvement and other charting issues.
Emergency department: Issues related to emer-gency department
functioning, including staffi ng, coverage, job descriptions.
Outcomes: Issues related to benchmarking, tar-gets, acuity
systems.
Job descriptions (nonemergency department): Issues related to
various job descriptions, including case management, utilization
review, transfer center.
Outpatient: Issues related to outpatient proce-dures, billing,
and outpatient staff roles.
Physician advisor/physician roles: Issues related to physician
advisor, attending physician, medical director roles.
Readmissions: Issues related to readmission pre-vention,
tracking.
as an All in One solution is not a sustainable tool ( Fry, 2007
; Reynolds, 2004). It is meant as a stop-gap measure, not as a
long-term solution because each application is a substitute for a
full size, enduring, more effi cacious specialty instrument.
Many organizations fail to recognize that hos-pital case
managers provide direct care to patients. Although not necessarily
at the bedside, they are direct care workers. The integration of
case and manager as a job title creates a distortion of what case
managers do. First, case manager implies an inordinate and
misleading amount of control in the face of a multiplicity of
organizational and external forces. Second, manager implies a
nondirect care function with inherent hierarchical authority. I
have been astounded at the amount of committee time direct
care/case management staff spend in meetings, thus vitiating their
direct patient service activities and creating time constraints
relative to their numerous other activities.
What Can Be Done?
Case management practice education and departmen-tal leadership
will need to address the actual day-to-day operational and clinical
emphasis on CMS com-pliance and the interface of professional
practice and organizational business imperatives and the impact on
the integrity of hospital case manages role bound-aries, role confl
ict, and role ambiguities.
Case management is what I call a lynchpin practice specialty
with numerous spokes emanat-ing out to other departments. Heeding
Powells cau-tion that case management functions need not become
independent titles, I do believe that there does need to be some
acknowledgment of both the specialty skill and its link to the core
case management role. A com-promise nomenclature might be as
follows:
Case management utilization specialist. Case management
compliance/recovery audit con-
tractors specialist. Case management quality specialist. Case
management discharge planning/care transi-
tion specialist. If job descriptions cannot be specialized,
stipu-
late to new recruits what percentage of time is expected in each
function/activity.
Create clear reporting relationships with other departments.
Orientation : Guarantee that each function receives the
requisite amount and type of training/preceptorship to engender
confi dence and com-petence.
Use staff meetings to explore whether current job descriptions
refl ect current departmental practice
NCM200342.indd 252NCM200342.indd 252 7/30/13 7:24 PM7/30/13 7:24
PM
-
Vol. 18/No. 5 Professional Case Management 253
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.
case management/utilization review software, electronic medical
records, meaningful use, etc.
Compliance: CMS-related guidance and regula-tory adherence.
Observation: Admission status orders, RAC, pre-payment reviews,
utilization management plans.
Discharge planning/care transitions: Diffi cult dis-charges,
discharge assistance programs, discharge resources, transfer
centers.
Denials: Non-CMS utilization review activity, denial management,
criteria.
Physician advisor/physician roles: Issues related to physician
advisor, attending physician, medi-cal director roles.
Documentation: Issues related to clinical doc-umentation
improvement and other charting issues; Billing : Non-RAC,
billing-related issues.
Emergency department: Issues related to emer-gency department
functioning, including staffi ng, coverage, job descriptions.
Outpatient : Issues related to outpatient proce-dures, billing,
and outpatient staff roles.
Readmissions: Issues related to readmission pre-vention,
tracking.
Staffi ng: Issues related to roles/responsibilities,
departmental structure, policies, staff ratios, mis-sion.
Job descriptions (nonemergency department): Issues related to
various job descriptions, includ-ing case management, utilization
review, transfer center.
Team building: Issues related to interdisciplinary team building
and huddles.
Misc.: All other issues (see Figure 3 ).
REFERENCES American Case Management Association.
(2010-2011).
National hospital case management survey [Published Results].
Little Rock, AR: Author.
American Case Management Association. (2012-2013). National
hospital case management survey [Published Results]. Little Rock,
AR: Author.
American Case Management Association . (n.d.). Learn-ing link
disclaimer & legal rules . Retrieved March 10, 2013, from
http://www.acmaweb.org/section.asp?sID = 10&mn = mn5&sn =
sn5&wpg = ll.
American Nurses Credentialing Center . ( 2011 , March). 2010
role delineation study: Nursing Case Manage-ment National Survey
results . Silver Spring, MD : Author .
Case Management Society of America . ( 2010 ). Standards of
practice . Little Rock, AR : Author .
Case Management Society of America . (n.d.). Defi nition of case
management . Retrieved March 24, 2013, from
http://www.cmsa.org/Home/CMSA/WhatisaCaseManager/tabid/224/Default.aspx
Staffi ng: Issues related to roles/responsibilities,
departmental structure, policies, staff ratios, mis sion.
Software/IT: Issues related to discharge plan ning, case
management/utilization review software, elec-tronic medical
records, meaningful use, etc.
Team building : Issues related to interdisciplinary team
building and huddles.
Misc.: All other issues (see Figure 1 ). Best practice/quality:
Standards of care for spe-
cifi c disease states, professional articles, certifi ca-tion,
The Joint Commission compliance.
Compliance: CMS-related guidance and regulatory adherence.
Observation: admission status orders, RAC, pre-payment reviews,
utilization management plans.
Discharge planning/care transitions: Diffi cult dis charges,
discharge assistance programs, dis-charge resources, transfer
centers.
Denials: Non-CMS utilization review activity, denial management,
criteria.
Physician Advisor/Physician Roles: Issues related to physician
advisor, attending physician, medi-cal director roles.
Documentation: Issues related to clinical docu-mentation
improvement and other charting issues; Billing : Non-RAC,
billing-related issues.
Emergency department : Issues related to emer-gency department
functioning, including staffi ng, coverage, job descriptions.
Outcomes: Metrics : Issues related to benchmarking, targets,
acuity systems; Information technology/software : Issues related to
discharge planning, case management/utilization review software,
electronic medical records, meaningful use, etc.
Outpatient: Issues related to outpatient proce-dures, billing,
and outpatient staff roles.
Readmissions: Issues related to readmission pre-vention,
tracking.
Staffi ng: Issues related to roles/responsibilities,
departmental structure, policies, staff ratios, mis sion.
Job descriptions (nonemergency department): Issues related to
various job descriptions, includ-ing case management, utilization
review, transfer center.
Team building: Issues related to interdisciplinary team building
and huddles.
Misc.: All other issues (see Figure 2 ). Best practice/quality:
Standards of care for spe-
cifi c disease states, professional articles, certifi ca-tion,
The Joint Commission compliance.
Outcomes: Issues related to benchmarking, tar-gets, acuity
systems; Information technology/software : Issues related to
discharge planning,
NCM200342.indd 253NCM200342.indd 253 7/30/13 7:24 PM7/30/13 7:24
PM
-
254 Professional Case Management Vol. 18/No. 5
Copyright 2013 Lippincott Williams & Wilkins. Unauthorized
reproduction of this article is prohibited.
Muller , L. S. ( 2013 ). Editors commentary . Professional Case
Management , 18 ( 1 ), 36 40 .
Phaneuf , M. ( 2008 ). The roles and qualities required of a
case manager . Retrieved November 24, 2012, from http://www.infi
ressources.ca/fer/Depotdocument_anglais/The_Roles_and_Qualities_Required_of_a_Case_Manager.pdf
Phoenix Medical Management . (n.d.). Best practice con-sulting
services . Retrieved March 31, 2013, from
http://www.phoenixmed.net/best-practice-consulting-services.html
Powell , S. K. ( 2012 ). The gestalt of case management .
Professional Case Management , 16 ( 5 ), 227228 .
Reynolds , J. ( 2004 , July). Case management and discharge
planning along the continuum staff presentation . New York, NY :
St. Lukes-Roosevelt Hospital .
Smith , A. C. ( 2011 ). Role ambiguity and confl ict in nurse
case managers: An integrative review . Professional Case Management
, 16 ( 4 ), 182 196 .
Tahan , H. A. , & Campagna , V. ( 2010 ). Case manage-ment
roles and functions across various settings and professional
disciplines . Professional Case Manage-ment , 15 ( 5 ). Retrieved
March 26, 2013, from
http://www.nursingcenter.com/prodev/ce_article.asp?tid =
1067978
Wikipedia . (n.d.). Case management (USA health system).
Hos-pital case management . Retrieved April 13, 2013, from
http://en.wikipedia.org/wiki/Case_management_
(USA_health_system)
John Jude Reynolds, CCM, CPHM, LCSW, has been a CCM since 1996
and a health care manager for 24 years. He has published numer-ous
articles for the American Hospital Association and most recently in
the American Journal of Nursing. John is currently the Director of
Care Management & Patient Access at St. Vincents Medical
Center, Westport Campus, Westport, CT.
Center for Medicare Advocacy . (n.d.). Retrieved Septem-ber 8,
2012, from
http://www.medicareadvocacy.org/medicare-info/observation-status/
Cohen , D. H. ( 2012 ). Hospital status admission
determina-tion: The use of Boolean logic, set theory, and
infor-mation theory to improve accuracy . Professional Case
Management , 17 ( 6 ), 258 264 .
Daniels , S. , & Frater , J. ( 2011 , August). Hospital case
man-agement and progression of care . Healthcare Financial
Management , 65 ( 8 ), 108 113 . Retrieved September 8, 2012, from
http://www.hfma.org/GSASearch.aspx?id = 4482&searchterms =
progression%20of%20care.
Daniels , S. , & Reece , R. ( 2007 ). The business case for
hospi-tal case management for health leaders news . Retrieved
September 8, 2012, from
http://phoenixmed.net/best-practice-consulting-services.html
Entropy . (n.d.). In Merriam-Websters online dictionary .
Retrieved March 30, 2013, from
http://www.merriam-webster.com/dictionary/entropy
Fry , J. ( 2007 , March 26). All in one? Technology compa-nies
dream of one device that can do it all. Now if only consumers would
get on board . The New York Times , p. R6 .
Gray , F. C. , White , A. , Brooks-Buck , J. ( 2013 ). Exploring
role confusion in nurse case management . Professional Case
Management , 18 ( 2 ), 6676 .
HCPro, Inc . ( 2008 ). Observation status: A guide to compli-ant
level of care determinations (2nd ed.) . Retrieved September 3,
2012, from
http://www.hcmarketplace.com/supplemental/6325_browse.pdf
Health Law and Regulation . ( 2010 ). The changing role of the
healthcare case manager . Retrieved September 8, 2012, from
http://www.hin.com/sw/healthLaw_regulation122710_case_manager_hospital_discharge_primary_care_ROI_ER.html
Muller , L. S. ( 2012 ). The ever changing legal landscape .
Professional Case Management , 17 ( 1 ), 33 36 .
For more than 38 additional continuing education articles
related to Case Management topics, go to NursingCenter.com/CE.
NCM200342.indd 254NCM200342.indd 254 7/30/13 7:24 PM7/30/13 7:24
PM