Embed Size (px)
Citation preview

Nursing Management of Delirium
updated 2011 http://www.nursingplanet.com/pn/nursing_management_delirium.html
Sutisa Rengratsamee RN. 18 August 2011
Definition
According to The Diagnostic and Statistical Manual of Mental Disorders (DSM) IV TR
Delirium is characterized by a
disturbance of consciousness and a change in cognition that develop rapidly over a period of time.
Epidemiology
Delirium is a common problem in all health
care settings, with a prevalence of
0.4% in general population,
1.1% in general population aged >55 years,
9–30% in general hospital admissions,
5–55% in elderly general hospital admissions
Predisposing factors
2. Endocrine causes
3. Drugs
4. Nutritional deficiencies
5. Systemic infections
6. Intracranial causes
7. Miscellaneous
Delirium
1. Metabolic Causes
1. Metabolic causes
Hypoxia
Hypoglycemia
Hepatic Encephalopathy
Uremic Encephalopathy
Cardiac failure, Cardiac arrhythmias
Water and Electrolyte Imbalance
Metabolic Acidosis
Fever, Anemia, Hypovolemic Shock
2. Endocrine causes
Hypo-hyper pitutairism
Hypo-hyper –thyroidism
Hypo-hyper –parathyroidism
Hypo-hyper –adrenalism
3. Drugs
both ingestion and withdrawal causes delirium and polypharmacy
Digitalis, quinidine, anti-hypertensive’s
Alcohol, sedatives, hypnonitics
Tri cyclic antidepressants and antipsychotics
Anti convulsants –levo dopa
Salicylates, steroids, pencillin, insulin
Methyl alcohol, heavy metals
4. Nutritional deficiencies
Thiamin
Niacin
Pyridoxine
Folic acid
B12
5. Systemic infections:
Acute and chronic
e.g.
Septicemia
Pneumonia
Endocarditis
6. Intracranial causes
Epilepsy
Head injury, subarachnoid hemorrhage, sub dural hematoma
Intracranial infections e.g. meningitis, encephalitis cerebral malaria
Stroke, hypertensive encephalopathy
Focal lesions e.g. right parietal lesions

7. Miscellaneous
Multiple medical problems
Cognitive impairment, dementia
Perception impairment, visual impairment
Post operative states, Fractures
Fever, hypothermia
Sleep deprivation
Heat, electricity and radiation
Clinical features
Impairment of consciousness
Appearance and behavior
Mood
Speech
Perception
Cognition
Orientation
Concentration
Memory disturbances
Insight
The disturbance of sleep wake cycle
Diurnal variation
Diagnosis
According ICD 10, symptoms should be present in each one of the following areas.
Impairment of the consciousness and attention
Global disturbance of cognition
Psychomotor disturbances
Disturbance of sleep walk cycle
Emotional disturbances
The onset is usually rapid

Physical and laboratory examinations
Physical Examination & Mental Status
Consciousness, V/S
DSM-IV-TR diagnostic criteria for delirium
The Confusion Assessment Method (CAM)
Delirium Symptoms Interview (DSI)
Delirium Rating Scale (DRS)
The Memorial Delirium Assessment Scale (MDAS)
Nursing Delirium Screening Scale (Nu-DESC)
Physical and laboratory examinations
CBC
Electrolyte
Glucose
Renal and Lever Function Test
Thyroid Function Test
Urine Analysis
Urine and Blood Drug screen
http://emedicine.medscape.com/article/288890- workup,
online publication update Jan,3, 2011
Thiamine and vitamin B12 levels
Test for Bacteriological and Viral etiology
Sedimentation rate
Drug screen including alcohol level
HIV
Laboratory Examination
Other Tests
• Lumbar puncture
• Brain Computerized Tomography (CT)
• Magnetic Resonance Imaging (MRI)
• Electroencephalography (EEG)
The Diagnostic and Statistical Manual of Mental Disorders (DSM)
• Published by the American Psychiatric Association and provides a common language and standard criteria for the classification of mental disorders
• There have been five revisions since it was first published in 1952 The last major revision was the fourth edition (DSM-IV), published in 1994, although a "text revision" was produced in 2000.
• The fifth edition (DSM-5) is currently in consultation, planning and preparation, due for publication in May 2013
http://en.wikipedia.org/wiki/Diagnostic_and_Statistical_Manual_of_Mental_Disorders , last modified on 3 August 2011
DSM-IV-TR diagnostic criteria for delirium
• Disturbance of consciousness occurs, with reduce ability to focus, sustain, or shift attention
• Change in cognition; memory deficit, disorientation,
language disturbance, perceptual disturbance
• The disturbance develop over short period (usually hours to days) and tends to fluctuate during the course of day
• Evidence from history, physical examination, or laboratory finding, that indicates the disturbance is cause by direct physiologic consequence of general medicine condition, an toxicating substance, medication use, or more than one cause
http://emedicine.medscape.com/article/288890- clinical, online publication update Jan,3, 2011
Confusion Assessment Method
Best Tool: The Confusion Assessment Method (CAM) includes two parts.
• Part one is an assessment instrument that screens for overall cognitive impairment.
• Part two includes only those four features that were found to have the greatest ability to distinguish delirium or reversible confusion from other types of cognitive impairment.
http://www.medscape.com/viewarticle/481726
Delirium Symptoms Interview (DSI)
• Developed by an interdisciplinary group of investigators
• This interview had good validity and reliability. The sensitivity of the DSI = .90 and the specificity = .80 (compared with the clinical judgment of a psychiatrist and neurologist)
• Interrater reliability, using lay interviewers, was .90 for the detection of major symptoms of delirium.
• delirium_dsi.pdf
(J Geriatr Psychiatry Neurol 1992;5:14–21).

Delirium Rating Scale (DRS)
• A 10-item rating scale, each item has specific descriptors that can be scored from 0 to a maximum either of 2, 3, or 4 points, depending on the item
• The sum of all item scores comprises the total DRS score; the maximum possible score is 32 points, ranged from 12 to 30 in a sample of individuals that showed symptoms of delirium
• It is suggested that symptoms be rated over a 24-hour period because of the fluctuating nature of delirium symptom severity and to better detect the disruption of the sleepwake cycle
Delirium Rating Scale (DRS)
1. Temporal onset
2. Perceptual disturbances
3. Hallucinations
4. Delusions
5. Psychomotor behavior
6. Cognitive status 7. Physical disorder 8. Sleep-wake cycle disturbance 9. Lability of mood 10. Variability of
symptoms
The DRS is a 10-item rating scale
ขอ 1. ระยะเวลาทเรมมอาการ
ขอ 2. ความผดปกตดานการรบร
ขอ 3. ชนดของอาการประสาท หลอน
ขอ 4. อาการหลงผด
ขอ 5. พฤตกรรมการเคลอนไหว
ขอ 6. Cognitive status
ขณะท าการประเมน
Thai Delirium Rating Scale (TDRS)
ขอ 7. โรคทางกาย
ขอ 8. ความผดปกตของวงจรการหลบตน
ขอ 9. ความแปรปรวนดานอารมณ
ขอ 10. การเปลยนแปลงของอาการตาง ๆ
วารสารสมาคมจตแพทยแหงประเทศไทย 2543; 45(4):325-332.
The Memorial Delirium Assessment Scale (MDAS)
is specifically designed to quantify the severity of delirium symptoms.
• It is composed of 10 observer-rated 4-point items, summed for range of 0 – 30, cut-off score of 13 for delirium and 30 worst/ most severe
It integrates objective cognitive testing and evaluation of behavioral symptoms.
delirium_mdas.pdf
..\แนวทางการวนจฉยภาวะสมองเสอม (TMSE).doc
delirium_dsi.pdf

Nursing Delirium Screening Scale (Nu-DESC)
• The Nu-DESC is a five symptoms rating scale and the screening score is 0-2, high score mean severe delirium
• It is easy to use, time-efficient (1 minute/ 1 patient), and accurate, and could lead to prompt delirium recognition and treatment
• useful concomitant delirium research tool, allowing continuous screening, symptom monitoring, and severity rating
Journal of Pain and Symptom Management, Vol. 29 No. 4 April 2005

Nursing Delirium Screening Scale (Nu-DESC)
Features and description Symptoms Rating (0-2)
Time Period Symptom
Midnight – 8 AM
8 Am – 4 AM
4 AM - Midnight
1. Disorientation Verbal or behavioral manifestation of not
being oriented to time or place or misperceiving persons in the environment
2. Inappropriate behavior Behavior inappropriate to place and/or for
the person; e.g., pulling at tubes or dressing, attempting to get out of bed when that is contraindicated, and the like (Gaudreau, Gagnon, Harel, Tremblay, and Roy, 2005)
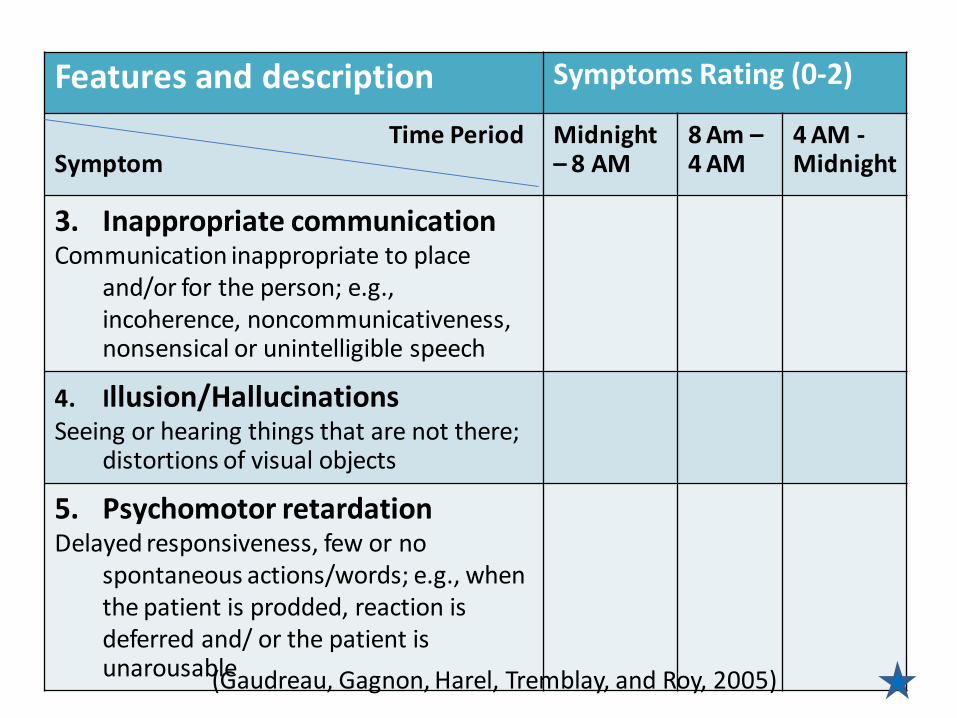
Features and description Symptoms Rating (0-2)
Time Period Symptom
Midnight – 8 AM
8 Am – 4 AM
4 AM - Midnight
3. Inappropriate communication Communication inappropriate to place
and/or for the person; e.g., incoherence, noncommunicativeness, nonsensical or unintelligible speech
4. Illusion/Hallucinations Seeing or hearing things that are not there;
distortions of visual objects
5. Psychomotor retardation Delayed responsiveness, few or no
spontaneous actions/words; e.g., when the patient is prodded, reaction is deferred and/ or the patient is unarousable (Gaudreau, Gagnon, Harel, Tremblay, and Roy, 2005)
Document
• All Examination Tools can be used to document the cognitive impairment and to provide a base line from which to measure the patient’s clinical course
• Don’t forget to document
all exiting results in to
patient file

Management
Four key steps in management of delirium are
1. Addressing the underlying causes
2. Maintaining behavioral control
3. Preventing complications
4. Supporting functional needs
The management strategies include both nonpharmacologic and pharmacologic interventions

Nursing management
Assessment
Physical assessment Nursing
diagnoses
Nursing management
Assessment
Physical assessment Nursing
diagnoses
Assessment
Client history: Nurses should assess the following areas of concern
Orientation to person, place, date and situation
Cognitive changes such as problems with attention, thinking process, personality and behavioral changes
Type, frequency, and severity of mood swings
Catastrophic emotional reactions
Appropriateness of social behavior
Language difficulties

Assessment (Cont.)
History
Full drugs history
Substance abuse; alcohol, recreational drugs
Previous delirium
Sensory deficits and or aids; hearing aids, glasses)
History by proxies
Journal of Psychosomatic Research, 62, (2007): 371-383
Nursing management
Assessment
Physical assessment Nursing
diagnoses
Physical assessment
Assessment should focus on two main areas
1. Signs of damage to the nervous system
2. Evidence of diseases of other organs

Nursing management
Assessment
Physical assessment Nursing
diagnoses
Nursing diagnoses
1. Risk for trauma related to impairment in cognitive and psychomotor function
Outcome criteria:
Client will not experience injury
Interventions:
Arrange furniture and other items in the room to accommodate clients disabilities
Store frequently used items within easy access
Nursing diagnoses
Interventions:
Do not keep bed in elevated position
Assist the client with ambulation
Keep a dim light on at night
Frequently orient the client to place, time and situation
Soft restraints may be required if client is very disoriented and hyperactive

2. Disturbed thought process related to cerebral degeneration as evidenced by disorientation, confusion, memory deficits and inaccurate interpretation of the environment
Outcome criteria:
client will interpret the environment accurately and maintain reality orientation to the best of his or her cognitive ability
Nursing diagnoses

Interventions:
Frequently orient the client to reality: clock and
calendars with large numbers that are easy to read
Notes and large bold signs may be used as reminders
Keep explanation simple
Discourage rumination of delusional thinking
Talk about real people and real events
Monitor for medication side effect
Nursing diagnoses
3. Self care deficit related to disorientation, confusion and memory deficits as evidenced by inability to fulfill the ADL
Outcome criteria:
Client will accomplish the ADLs to the best of his or her ability
Unfulfilled activities may be kept by caregivers
Nursing diagnoses
Interventions:
Identify the self care deficits and provide assistance as required
Provide guidance and assistance for independent actions
Provide a structured schedule of activities that does not change from day to day
Provide for consistency in assignment of daily caregivers
Nursing diagnoses
Interventions:
Perform ongoing assessment of clients ability to fulfill nutritional needs ,ensure personal safety ,follow medication regimen and communicate need for assistance with activities that she or he cannot accomplish independently
Involve the family members in the care of the patient conclusion
Nursing diagnoses

Clinical Nursing Practice Guideline
การสรางแนวปฏบตการพยาบาลเพอปองกนภาวะ Delirium ของผสงอายโรงพยาบาลศรราช (สวรรณา สกประเสรฐ, พรทตา วศาจารย, และภรภา แสงจนทร, 2549)
• การศกษานไดท าการสบคนและคดเลอกงานวจยทมความเกยวของมา 7 เรอง และ Guideline 2 เรอง
• น ามาวเคราะห และสรปขอเสนอแนะ เพอปองกนภาวะ Delirium ของผสงอายในโรงพยาบาล ดงน
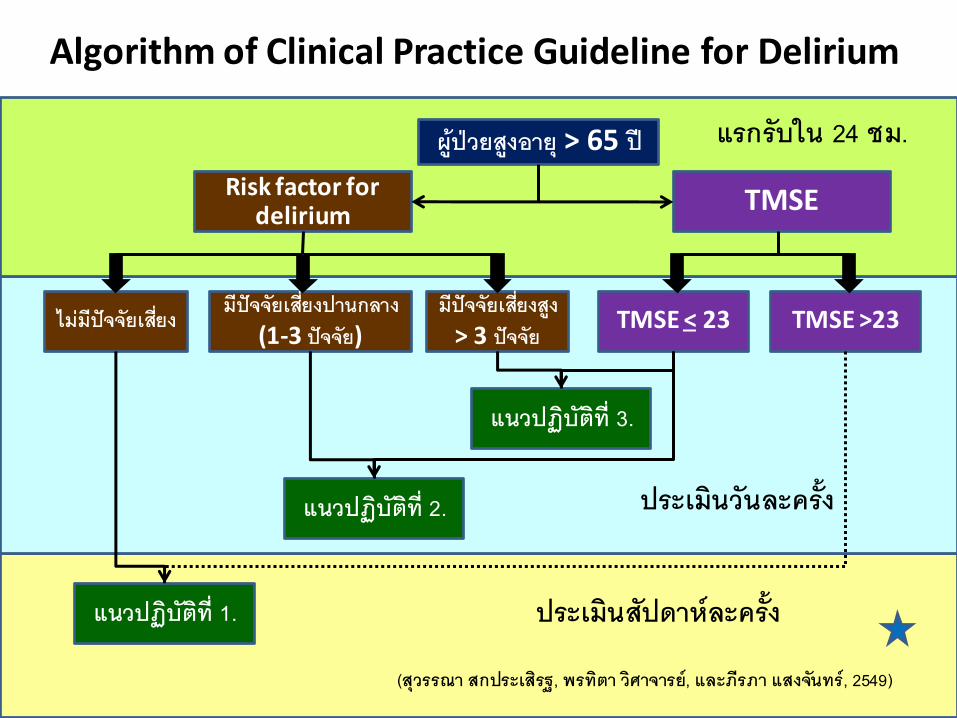
Algorithm of Clinical Practice Guideline for Delirium
ผปวยสงอาย > 65 ป
TMSE Risk factor for delirium
แนวปฏบตท 3.
มปจจยเสยงปานกลาง (1-3 ปจจย)
มปจจยเสยงสง > 3 ปจจย
TMSE < 23 ไมมปจจยเสยง TMSE >23
แนวปฏบตท 2.
แนวปฏบตท 1.
แรกรบใน 24 ชม.
ประเมนวนละครง
ประเมนสปดาหละครง
(สวรรณา สกประเสรฐ, พรทตา วศาจารย, และภรภา แสงจนทร, 2549)
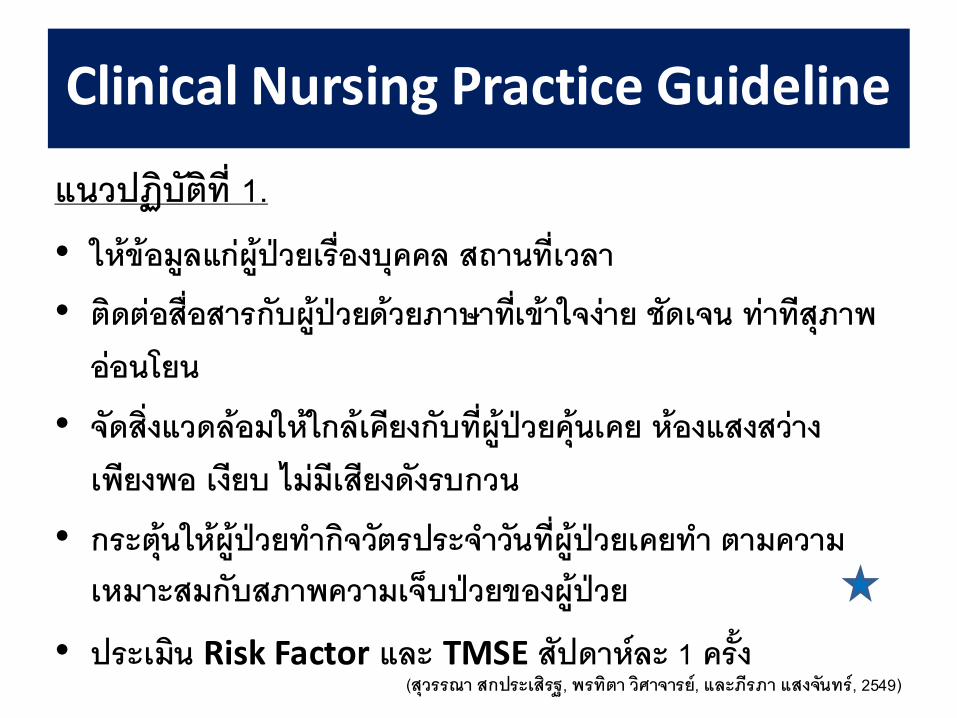
แนวปฏบตท 1. • ใหขอมลแกผปวยเรองบคคล สถานทเวลา
• ตดตอสอสารกบผปวยดวยภาษาทเขาใจงาย ชดเจน ทาทสภาพออนโยน
• จดสงแวดลอมใหใกลเคยงกบทผปวยคนเคย หองแสงสวางเพยงพอ เงยบ ไมมเสยงดงรบกวน
• กระตนใหผปวยท ากจวตรประจ าวนทผปวยเคยท า ตามความเหมาะสมกบสภาพความเจบปวยของผปวย
• ประเมน Risk Factor และ TMSE สปดาหละ 1 ครง
Clinical Nursing Practice Guideline
(สวรรณา สกประเสรฐ, พรทตา วศาจารย, และภรภา แสงจนทร, 2549)
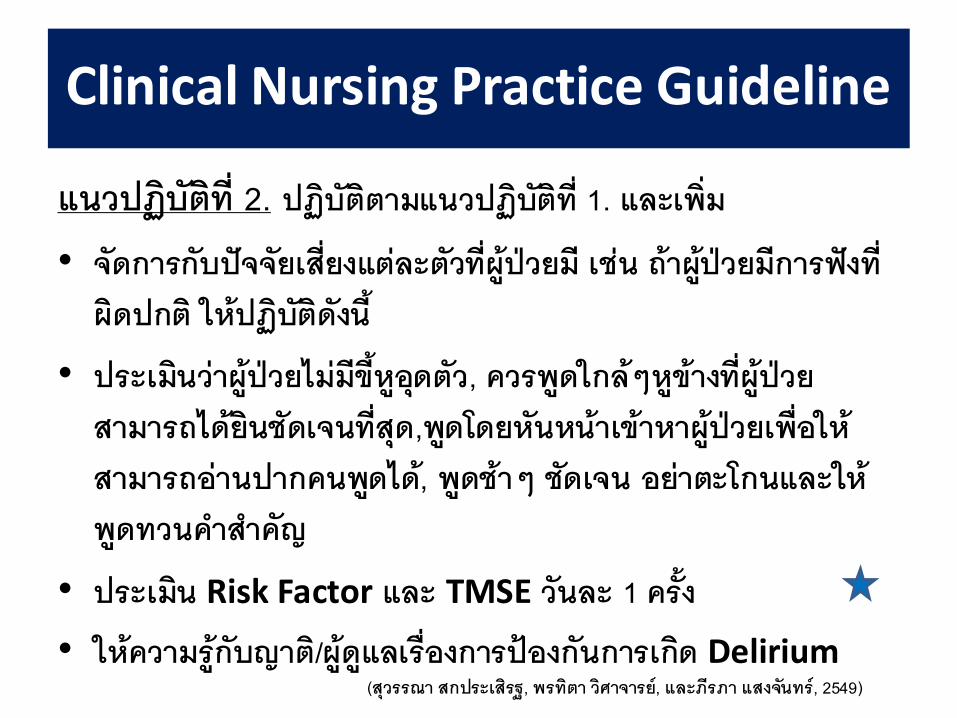
แนวปฏบตท 2. ปฏบตตามแนวปฏบตท 1. และเพม
• จดการกบปจจยเสยงแตละตวทผปวยม เชน ถาผปวยมการฟงทผดปกต ใหปฏบตดงน
• ประเมนวาผปวยไมมขหอดตว, ควรพดใกลๆ หขางทผปวยสามารถไดยนชดเจนทสด,พดโดยหนหนาเขาหาผปวยเพอใหสามารถอานปากคนพดได, พดชาๆ ชดเจน อยาตะโกนและใหพดทวนค าส าคญ
• ประเมน Risk Factor และ TMSE วนละ 1 ครง
• ใหความรกบญาต/ผดแลเรองการปองกนการเกด Delirium
Clinical Nursing Practice Guideline
(สวรรณา สกประเสรฐ, พรทตา วศาจารย, และภรภา แสงจนทร, 2549)
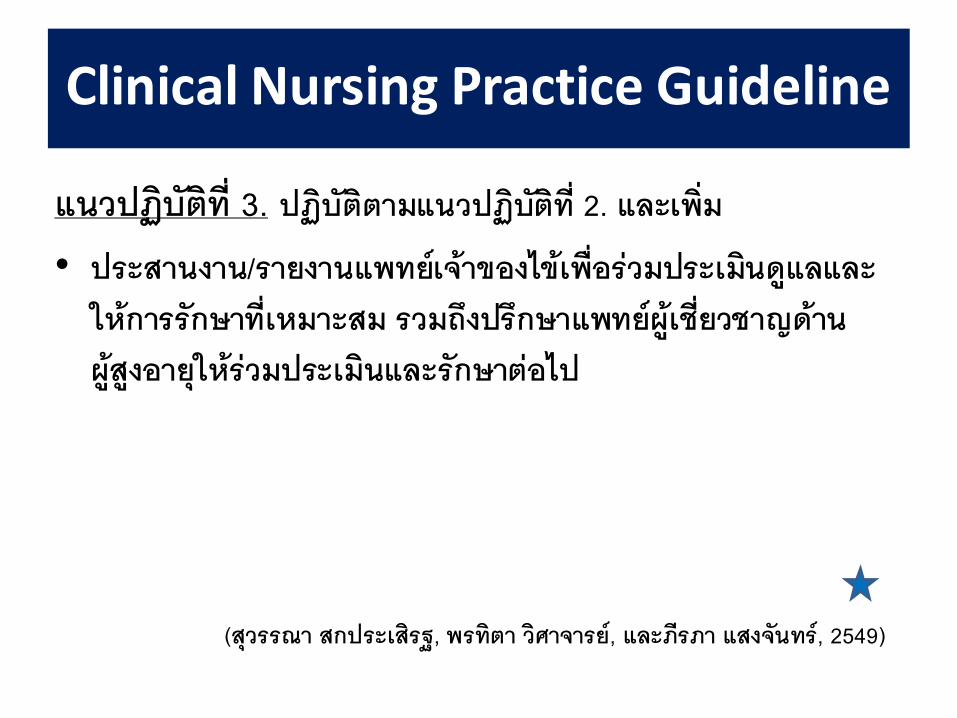
แนวปฏบตท 3. ปฏบตตามแนวปฏบตท 2. และเพม
• ประสานงาน/รายงานแพทยเจาของไขเพอรวมประเมนดแลและใหการรกษาทเหมาะสม รวมถงปรกษาแพทยผเชยวชาญดานผสงอายใหรวมประเมนและรกษาตอไป
Clinical Nursing Practice Guideline
(สวรรณา สกประเสรฐ, พรทตา วศาจารย, และภรภา แสงจนทร, 2549)
Suggestions
Delirium or acute confusional state is a medical emergency associated with increased morbidity and mortality rates
Early diagnosis and resolution of symptoms are correlated with the most favorable outcomes

Thank You
For Your Attention...