-
8/3/2019 Nurological Emergencies .
1/54
Non-traumatic neurologic emergenciesRadiology
Edith Nielsen
rhus University Hospital
Denmark
Stroke
Ischemic stroke
Thromboembolic
Vasculitis Dissection
Post anoxic ischemia
-
8/3/2019 Nurological Emergencies .
2/54
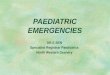
Ischemic stroke
Earliest signs are demonstrated on CT after 6-12hours
Faint loss of discrimination between grey andwhite matter
Loss of well defined sulci
High density may be seen in occluded arteries
Loss of discrimination and sulci
-
8/3/2019 Nurological Emergencies .
3/54
High density vessels
Ischemic stroke
Perfusion CT shows areas with no flow or reducedflow
-
8/3/2019 Nurological Emergencies .
4/54
Occlusion of MCA after coil treatment
Ischemic stroke
After 6-12 hours low density changes are seen
Mass effect due to edema peaks between day 3-5
Mass effect is gone in 2-4 weeks
-
8/3/2019 Nurological Emergencies .
5/54
Low density
Edema
-
8/3/2019 Nurological Emergencies .
6/54
Day 1 Day 4
Ischemic stroke
Blood-brain barrier breaks after 3 days
Enhancement may be seen for a few weeks
Enhancement is gyriform in cortical infarcts Enhancement is ring
like in central parts of the
brain
-
8/3/2019 Nurological Emergencies .
7/54
Enhancement
Ischemic stroke
After weeks to months a loss of substancedevelops
The defect is filled with CSF A secondary enlargement of the
ventricles may be
seen
-
8/3/2019 Nurological Emergencies .
8/54
Loss of substance
Ischemic stroke
Earliest signs of ischemia on MR can be seenwithin a few
minutes
On DWI high signal is seen after a few minutes.The signal
decreases during the next week
ADC is low at first and increases over weeks
-
8/3/2019 Nurological Emergencies .
9/54
Infarct 1-2 hours
DWI ADC T2
Nonischemic causes for decreased ADC
Abscess
Lymphoma and other tumors
Multiple sclerosis Metabolic diseases (Canavans)
Seizures
Severe hypoglycemia
Trauma
-
8/3/2019 Nurological Emergencies .
10/54
Ischemic stroke
On PWI a reduced flow can be seen
A hypoperfused area surrounding the DWI lesionmay be seen the
penumbra
The penumbra is the potentially salvageable tissue
Perfusion diffusion mismatch
CBV CBF MTT
DWI
T2 +7 mdr
CBV CBF MTT
DWI
T2 +7 months
-
8/3/2019 Nurological Emergencies .
11/54
Ischemic stroke
On T2WI a high signal is seen after 6-8 hours.
The signal increases over weeks until water valuesare reached
when the tissue resorption is complete
On T1WI low signal develops after 6-8 hours. Thesignal decreases
until water values are reached
High signal on T2WI og DWI
-
8/3/2019 Nurological Emergencies .
12/54
Ischemic stroke
On MRA a large vessel occlusion can be seen
Vessel occlusion
-
8/3/2019 Nurological Emergencies .
13/54
Ischemic stroke
Vasculitis :
CT may show poorly demarcated low densityareas
MR shows high signal changes on T2WI andFLAIR often in more than
one area
MRA is most often normal
Low density
-
8/3/2019 Nurological Emergencies .
14/54
High signal on T2WI og DWI
High signal on T2 and FLAIR
-
8/3/2019 Nurological Emergencies .
15/54
Narrowing af vessels
Takayasu Before treatment
After treatment
-
8/3/2019 Nurological Emergencies .
16/54
Ischemic stroke
Dissection :
Can cause stenosis or pseudoaneurisms
Can give ischemic changes or hemorrhages
On MRI thrombus can be seen in the vessel wall
Normal flow void is not seen in the vessel or part
of the vessel
Dissection
-
8/3/2019 Nurological Emergencies .
17/54
Dissection
Ischemic stroke
Post anoxic changes
Affects globus pallidus
Can affect other areas
-
8/3/2019 Nurological Emergencies .
18/54
Post anoxic changes
Drowning CO
Post anoxic changes
Global ischemia
-
8/3/2019 Nurological Emergencies .
19/54
Stroke
Hemorrhagic stroke
Intraparenchymal hematoma
Hemorrhagic infarctions
Venous thrombosis
Subarachnoid hemorrhage
Hemorrhagic stroke
Intraparenchymal hemorrhage :
High density on CT images increases duringday 1-3
A surrounding low density rim consist of serum
During the following days an edema develops
Resorption starts in the periphery of the clot
After a month resorption is complete
Often very little is seen after resorption, a loss
of substance may be seen
-
8/3/2019 Nurological Emergencies .
20/54
Intraparenchymal hemorrhage
Hemorrhagic stroke
Intraparenchymal hemorrhage :
Hyper acute : T2 hyperintens, T1 hypointense
Acute : T2 hypointense, T1 iso-hypointense Early subacute : T2
hypointense, T1
hyperintense
Late subacute : T2 and T1 hyperintense
Chronic : T2 and T1 hypointense
-
8/3/2019 Nurological Emergencies .
21/54
Intraparenchymal hemorrhage
2 hours
Intraparenchymal hemorrhage
13 days
-
8/3/2019 Nurological Emergencies .
22/54
Intraparenchymal hemorrhage
3 months
Intraparenchymal hemorrhage
Cavernoma AVM
-
8/3/2019 Nurological Emergencies .
23/54
Hemorrhagic stroke
Hemorrhagic infarction :
Reperfusion in infarct
Occurs 6-12 hours after the initial stroke, butcan be seen a
week or more after ictus
Hemorrhage is often patchy
Hemorrhagic infarction
-
8/3/2019 Nurological Emergencies .
24/54
Hemorrhagic infarction
3 weeks
Hemorrhagic stroke
Venous thrombosis :
Flow void in veins are replaced by clots
The signal in the clots depends on the age of theclot
Normal veins are subject to individual variations
Infarcts or hemorrhages are often bilateral andsubcortical
-
8/3/2019 Nurological Emergencies .
25/54
Venous thrombosis
Venous thrombosis
Acute 4 weeks later
-
8/3/2019 Nurological Emergencies .
26/54
Venous thrombosis
Venous thrombosis
-
8/3/2019 Nurological Emergencies .
27/54
Hemorrhagic stroke
Intratumoral hemorrhage :
Degradation of blood is often slower than insimple hematomas
Blood will often obscure tumor as well asenhancement
Intratumoral hemorrhage
Meningeoma
-
8/3/2019 Nurological Emergencies .
28/54
Intratumoral hemorrhage
Metastasis
Intratumoral hemorrhage
Pituitary adenoma
-
8/3/2019 Nurological Emergencies .
29/54
Hemorrhagic stroke
Subarachnoid hemorrhage :
CT shows blood in subarachnoid space, in theventricles or a
hematoma
CTA or MRA can demonstrate the aneurysm inmost cases
The final diagnosis is made by conventional angio Most aneurysms
can be treated with coils
Subarachnoid hemorrhage
-
8/3/2019 Nurological Emergencies .
30/54
Subarachnoid hemorrhage
Subarachnoid hemorrhage
CTA
-
8/3/2019 Nurological Emergencies .
31/54
Subarachnoid hemorrhage
-
8/3/2019 Nurological Emergencies .
32/54
Infections
Subdural empyema
Meningitis
Cerebritis
Abscess
Ventriculitis
Herpes simplex encephalitis
Subdural and epidural empyemas
Extracerebral fluid collection
Enhancement of membranes
10% develops venous thrombosis Can spread to brain parenchyma as
cerebritis
-
8/3/2019 Nurological Emergencies .
33/54
Subdural empyema
Meningitis
A clinical diagnosis not a radiological diagnosis
Radiological examinations are performed only
when complications are suspected Most patients have normal
scans
Some have meningeal enhancement
Some will get complications hydrocephalus orinfectious
involvement of the brain
-
8/3/2019 Nurological Emergencies .
34/54
TB meningitis
Cerebritis
Early phase of abscess formation
Low signal on T1WI and high signal on T2WI and
FLAIR No enhancement
-
8/3/2019 Nurological Emergencies .
35/54
Cerebritis
Abscess
Enhancing rim, often thin and regular
Considerable edema
High signal on DWI and low on ADC
-
8/3/2019 Nurological Emergencies .
36/54
Abscess
T1 +C ADCDWI
Tumor
T1 +C ADCDWI
-
8/3/2019 Nurological Emergencies .
37/54
Ventriculitis
Enhancement of ependyma
Enlargement of ventricles
Zones of low density around ventricles on CT
Zones of high intensity around the ventricles onT2WI and
FLAIR
Ventriculitis
-
8/3/2019 Nurological Emergencies .
38/54
Herpes simplex encephalitis
Located in the temporal lobes, insula, theorbitofrontal region
and cingulate gyrus
Low density on CT
High signal on T2WI and FLAIR
Enhancement may be seen
Herpes simplex encephalitis
-
8/3/2019 Nurological Emergencies .
39/54
Herpes simplex encephalitis
-
8/3/2019 Nurological Emergencies .
40/54
Hydrocephalus
Colloid cyst
Aquaductal stenosis
Tumor
Hematoma or infarct
Infection, hemorrhage, carcinomatosis
Colloid cyst
Located anterior in the third ventricle
Signal on MR varies with protein content of cyst
Often high signal on T1WI High density on CT
-
8/3/2019 Nurological Emergencies .
41/54
Colloid cyst
Aquaductal stenosis
Dilatation of lateral and third ventricle withnormal fourth
ventricle
Can be diagnosed on CSF flow imaging
-
8/3/2019 Nurological Emergencies .
42/54
Aquaductal stenosis
Tumor
Pineal gland
Tectum
Posterior fossa
-
8/3/2019 Nurological Emergencies .
43/54
Tumor
AstrocytomaPineoblastoma
Tumor
Medulloblastoma
-
8/3/2019 Nurological Emergencies .
44/54
Hematoma or infarct
Compression of third ventricle, aqueduct andfourth ventricle
Complication of posterior fossa infarcts
Infarct in posterior fossa
-
8/3/2019 Nurological Emergencies .
45/54
Infection, hemorrhage, carcinomatosis
Due to disturbance of resorption of CSF inarachnoid villi
Caused by infection, SAH, carcinomatosis
Infection and hemorrhage
Ventriculitis SAH
-
8/3/2019 Nurological Emergencies .
46/54
Diseases of the spine
Disc herniation
Diskitis and osteomyelitis
Epidural abscess Metastasis
Infarcts
AVM
-
8/3/2019 Nurological Emergencies .
47/54
Degenerative diseases
Disc herniation :
Large herniations may affect the cauda equina
A free fragment (sequestered) can migrate
Disc herniation
-
8/3/2019 Nurological Emergencies .
48/54
Infections
Diskitis and osteomyelitis:
High signal in disc and vertebrae on T2WI andlow on T1WI
Enhancement in vertebrae and surrounding softtissue
Diskitis and osteomyelitis
-
8/3/2019 Nurological Emergencies .
49/54
Diskitis and osteomyelitis
Infections
Epidural abscess :
Often located in the dorsal epidural space
Low signal on T1WI and high on T2WI Enhancement of granulation
tissue
No enhancement in the center of an abscess
-
8/3/2019 Nurological Emergencies .
50/54
Epidural abscess
Tumors
Metastasis :
Normal high signal in vertebrae on T1WI is
replaced by low signal High signal on T2WI
Tumor masses may compress the spinal cord
-
8/3/2019 Nurological Emergencies .
51/54
Metastasis
Metastasis
-
8/3/2019 Nurological Emergencies .
52/54
Vascular lesions
Infarct :
High signal in spinal cord
Differential diagnosis includes MS and transversemyelitis
Infarct
-
8/3/2019 Nurological Emergencies .
53/54
Vascular lesions
AVM :
Can give rise to SAH
High signal in spinal cord on T2WI due to highpressure in
veins
Dilated vessels are often seen surrounding the
spinal cord
Dural fistula
-
8/3/2019 Nurological Emergencies .
54/54