Embed Size (px)
Citation preview

NRIMC
Endocrinology
HYPOPITUITARISMHYPOPITUITARISM
Dr Srikanth M.D., D.M.Dr Srikanth M.D., D.M.Associate ProfessorAssociate Professor
Dept. of EndocrinologyDept. of EndocrinologyNRIASNRIAS
Dr Sirisha M.D.Dr Sirisha M.D.Senior ResidentSenior Resident
Dept. of EndocrinologyDept. of EndocrinologyNRIASNRIAS

NRIMC
Endocrinology
HypopituitarismHypopituitarism
• Underdiagnosed entityUnderdiagnosed entity
• Diagnosis Requires Diagnosis Requires – High index of suspicionHigh index of suspicion
– Low threshold for investigationsLow threshold for investigations
– Availability of all dynamic endocrine investigations Availability of all dynamic endocrine investigations
– Endocrine expertise while carrying out investigationsEndocrine expertise while carrying out investigations
• Not so rareNot so rare

NRIMC
Endocrinology
..
A 26 year old male patient, a product ofA 26 year old male patient, a product of consangenous parentage presented with consangenous parentage presented with
Growth RetardationGrowth Retardation
Failure to develop secondary sexual charactersFailure to develop secondary sexual characters normallynormally
Decreased frequency of nocturnal erectionsDecreased frequency of nocturnal erections
Reduced exercise capacityReduced exercise capacity

NRIMC
Endocrinology
No H/o head injuryNo H/o head injury
No H/o Anosmia / Visual abnormalitiesNo H/o Anosmia / Visual abnormalities
No evidence of Chronic illness / Viral infectionNo evidence of Chronic illness / Viral infection
No H/o any drug abuseNo H/o any drug abuse

NRIMC
Endocrinology
..
• General ExaminationGeneral Examination::
PR – 88/minPR – 88/min
BP – 110/70 mm Hg without any postural variationBP – 110/70 mm Hg without any postural variation
WeightWeight – 42 Kg – 42 Kg HeightHeight – 152 Cm – 152 Cm• US – US – 65 cm 65 cm• LS LS _ _ 87 cm 87 cm• Arm spanArm span – 158 cms – 158 cms

NRIMC
Endocrinology
..
• Genital ExaminationGenital Examination::
Pubic Hair – P2Pubic Hair – P2
SPL – 10cmSPL – 10cm
Testes Volume – PrepubertalTestes Volume – Prepubertal
No facial hair & hair in other androgen dependent areas No facial hair & hair in other androgen dependent areas
Axillary hair – present but minimalAxillary hair – present but minimal Other systemic examination is normalOther systemic examination is normalAnosmia –ve, CNS - NormalAnosmia –ve, CNS - Normal

NRIMC
Endocrinology
Bone ageBone age
• Bone age -Bone age - 13 years13 years– DelayedDelayed– Chronological age – 26 yearsChronological age – 26 years– Epiphyses – still unfusedEpiphyses – still unfused

NRIMC
Endocrinology
Thyroid function testsThyroid function testsParameter Result Units Normal range
T3 0.92 ng/ml 0.8-1.81
FT3 2.38 pg/ml 0.92-11.25
T4 3.3 gm/dl 4.0 -12.6
FT4 0.29 ng/dl 0.89-1.76
TSH 11.34 IU/ml 0.35 -5.50
Comment Central Hypothyroidism / Primary hypothyroidism

NRIMC
Endocrinology
Gonadal axis evaluationGonadal axis evaluation
Parameter Result Units Comment
FSH 0.60 mIU/ml Low
LH 0.29 U/L Low
Testosterone 0.02 ng/ml Low
Impression Central Hypogonadism

NRIMC
Endocrinology
Growth AxisGrowth Axis
• IGF 1 IGF 1 – Active form of GHActive form of GH– < 25 ng/ml< 25 ng/ml– Normal range ( 116-358 ng/ml)Normal range ( 116-358 ng/ml)

NRIMC
Endocrinology
Adrenal axis evaluationAdrenal axis evaluation
• ACTH ACTH 27 pg/ml27 pg/ml NormalNormal
• Basal cortisolBasal cortisol 2.0 mcg/dl2.0 mcg/dl LowLow
Parameter Result Units Comment
ACTH 27 Pg/ml Normal
Basal Cortisol 2.0 g/dl 4.3- 22.4 Low
Stim cortisol Not done
Impression Central Hypocortisolism !

NRIMC
Endocrinology

NRIMC
Endocrinology
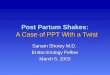
• Empty sella appearanceEmpty sella appearance

NRIMC
Endocrinology

NRIMC
Endocrinology
..
• A 42 year old Female Patient presented withA 42 year old Female Patient presented with
Recurrent episodes of facial puffiness of 10 years durationRecurrent episodes of facial puffiness of 10 years duration
Dryness of skin associated with scaling & itchingDryness of skin associated with scaling & itching
Amenorrhoea of 10 years durationAmenorrhoea of 10 years duration
Loss of pubic hair & axillary hairLoss of pubic hair & axillary hair
Weakness, fatiguability, depression & impaired memoryWeakness, fatiguability, depression & impaired memory
Previous H/o PPH and Lactation failurePrevious H/o PPH and Lactation failure

NRIMC
Endocrinology
..
• General ExaminationGeneral Examination
• Periorbital puffinessPeriorbital puffiness
• Skin – dry, coarse & scalySkin – dry, coarse & scaly
• No axillary and pubic hairNo axillary and pubic hair
• Breast atrophyBreast atrophy
• PR – 90/minPR – 90/min
• BP – 100/70 mm Hg without postural variationBP – 100/70 mm Hg without postural variation
• Other Systemic examination is NormalOther Systemic examination is Normal

NRIMC
Endocrinology

NRIMC
Endocrinology
HemogramHemogram
• Hb 10.6 gm%Hb 10.6 gm%
• WBC count – 4200WBC count – 4200
• Platelets – 2.1 lakhPlatelets – 2.1 lakh
• DC – normalDC – normal
• Mild normocytic normocytic anemiaMild normocytic normocytic anemia

NRIMC
Endocrinology
BiochemistryBiochemistry
• CreatinineCreatinine :: 1.1 1.1 mg% (mg% (• BilirubinBilirubin :: 0.40.4 mg%mg%• SGOTSGOT :: 115115 U/LU/L• SGPTSGPT :: 4646 U/LU/L• SAPSAP :: 8787 U/LU/L• Total proteinTotal protein :: 7.97.9 gm/dlgm/dl• AlbuminAlbumin :: 4.04.0 gm/dlgm/dl• GlobulinGlobulin :: 3.93.9 gm/dlgm/dl• NaNa :: 126126 meq/lmeq/l• KK :: 2.62.6 meq/lmeq/l
Parameter Result Normal range

NRIMC
Endocrinology
Thyroid function testsThyroid function tests
Parameter Result Units Normal range
T3 < 0.01 ng/ml 0.8-1.81
FT3 1.03 pg/ml 0.92-11.25
T4 < 0.01 gm/dl 4.0 -12.6
FT4 0.11 ng/dl 0.89-1.76
TSH 2.38 IU/ml 0.35 -5.50
Comment Central Hypothyroidism

NRIMC
Endocrinology
Gonadal axis evaluationGonadal axis evaluation
Parameter Result Units Comment
FSH 1.98 mIU/ml Low
LH < 0.07 U/L Low
Estradiol 28.30 pg/ml Low
Impression Central Hypogonadism

NRIMC
Endocrinology
Adrenal axis evaluationAdrenal axis evaluationParameter Result Units Comment
ACTH 10 Pg/ml Low
Basal Cortisol 2.0 g/dl 4.3- 22.4 Low
Stimulated cortisol- 0 min 1.2 g/dl > 20 g/dl Low
Stimulated cortisol- 45 min 12.8 g/dl > 20 g/dl Low
Stimulated cortisol- 60 min 10.4 g/dl > 20 g/dl Low
Stimulated cortisol- 90 min 8.0 g/dl > 20 g/dl Low
Stimulation test was done by insulin tolerance test (0.15 U /Kg)
Impression Central Hypocortisolism

NRIMC
Endocrinology
Growth Hormone axis evaluationGrowth Hormone axis evaluationParameter Result Units Comment
IGF -1
Basal GH < 0.5 ng/ml Low
Stimulated GH - 0 min < 0.5 ng/ml > 10 ng/ml Low
Stimulated GH - 45 min < 0.5 ng/ml > 10 ng/ml Low
Stimulated GH - 60 min < 0.5 ng/ml > 10 ng/ml Low
Stimulated GH - 90 min < 0.5 ng/ml > 10 ng/ml Low
Stimulated GH - 120 min < 0.5 Ng/ml > 10 ng/ml Low
Stimulation test was done by insulin tolerance test (0.15 U /Kg) Peak GH response of > 10 ng/ml is considered normal response
Impression Adult Growth Hormone deficiency

NRIMC
Endocrinology
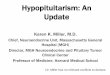
Radiological evaluation
MRI of pituitary is suggestive of partial empty sella
Minimal pituitary tissue is present at floor of sella

NRIMC
EndocrinologyHypopituitarism
Hypothyroidism Hypogonadism Hypocortisolism GH deficiency Low Prolactin
1. Puffiness 2. Lethargy3. Coma4. Weakness5. Infertility6. Cramps7. Can not
tolerate LT4
1. Pubertal delay2. Infertility3. Amenorrhea
* Primary * Secondary4. Loss of libido5. Breast
atrophy6. Osteoporosis
1. Weakness2. Weight loss3. Lethargy4. Hypotension5. Postural
hypotension6. Giddiness7. Vomitings8. Diarrhea9. Pain
abdomen10. Refractory
shock11. Hyponatremia
Children1.Growth failure2.Shortstature
Adults
1.Adult growth hormone deficiency
Lactational failure
No symptoms in male

NRIMC
Endocrinology
Causes of Hypopituitarism
• Heriditory Pituitary Hormone deficiency ( Pit 1, Prop 1, LHX 3, HESX1)
• Acquired Pituitary hormone deficiency– Infections - rare– Infiltrative
• Primary Hypophysitis ( Lymphocytic, Granulomatous, Xanthomatous)• Secondary Hypophysitis ( Histiocytosis X, sarcoidosis )
– Neoplastic• Pituitary Tumor and parasellar tumors• Craniopharyngioma etc• Post Pituitary surgery
– Trauma• Radiation, surgical resection, brain trauma
– Vascular• Apoplexy, pregnancy related ( post partum pituitary necrosis), Hypotension

NRIMC
Endocrinology
Summary• High index of suspicion is required
• Low threshold of investigations
• Seek for endocrine consultation where ever there is a doubt
• Treatment is difficult– Life threatening hypocortisolemia / hypothyroid coma can occur
– Multiple pituitary hormone replacement is needed in physiological manner
– Stress advise regarding the steroid replacement is mandatory
– Iatrogenic cushings is possible
– Constant reinforcement is needed for good complaince
– Fertility needs special protocols both in males and females