Embed Size (px)
Citation preview

Role of Antidiuretic Hormone in the Abnormal
Water Diuresis of Anterior Hypopituitarism in Man
ZALMANS. AGUSand MARTINGOLDBERG
From the Renal-Electrolyte Section, Department of Medicine, University ofPennsylvania School of Medicine, Philadelphia, Pennsylvania 19104
A B S T R A C T To evaluate the role of antidiuretic hor-mone (ADH) in the defect in water excretion which ischaracteristic of glucocorticoid deficiency, the effects ofhydrocortisone and ethanol upon urinary dilution duringa sustained water load were studied in patients withanterior hypopituitarism. A spectrum of defects in uri-nary dilution was found in the seven patients with an-terior hypopituitarism, and the subjects were separableinto two groups. Four patients were unable to excrete aurine hypotonic to plasma (group I) while three dilutedthe urine (group II). In two of the group II patients,despite maintenance of hydration, urinary osmolalitylater rose to hypertonicity. Physiological doses of hy-drocortisone improved urinary dilution in all patients.Submaximal doses of oral hydrocortisone, when givento the group I patients, converted their response to hy-dration to one characteristic of the group II patients,i.e., an initial hypotonic urine followed by a secondaryrise to hypertonicity. Ethanol, a known inhibitor ofADH secretion, had no effect in the group I patients.When two of these patients were pretreated with sub-maximal doses of hydrocortisone, however, so that theywere able to transiently dilute the urine, ethanol pre-vented the secondary rise in urine osmolality. Similarly,the administration of ethanol to the untreated group IIpatients, when the urine was hypotonic, improved di-luting ability as characterized by a lowering of urinaryosmolality and an increased excretion of solute-free wa-ter in all three patients. Hydrocortisone did not improveurinary dilution in three patients with complete hypo-physeal diabetes insipidus and one with both anterior andposterior insufficiency receiving constant infusions ofvasopressin. These data suggest, therefore, that inap-propriately elevated levels of ADH play a major rolein the defect in water excretion of anterior hypopituitar-
A preliminary report of this work was published: 1962.Trans. Ass. Amer. Physicians Philadelphia. 75: 129.
Received for publication 7 December 1970 and in revisedform 16 February 1971.
ism. Glucocorticoids appear to be necessary for a normalneurohypophyseal response to inhibitory stimuli.
INTRODUCTIONA defect in the excretion of a water load and its cor-rection by glucocorticoid administration have been welldocumented in patients with hypopituitarism and adrenalinsufficiency (1-5), but the physiologic mechanismsunderlying these observations have not been completelyelucidated. While several mechanisms may contributeto the defect in water excretion in hypopituitarism, manyfeel that the major factor is insufficient impermeabilityto water of the distal tubular and collecting duct epi-thelium due either to a direct effect of glucocorticoiddeficiency or indirectly via elevated levels of circulatingantidiuretic hormone (ADH). The role of elevated lev-els of ADH, first suggested in 1949 (6) and supportedby the observations of Dingman and Despointes (5),has not as yet been definitively established. Bioassayshave shown both sustained high ADH levels (7) andundetectable ADH blood levels (8) in patients withglucocorticoid deficiency. Furthermore, the difficultyinherent in interpreting data derived from bioassay stud-ies of this problem is evident by the fact that neither ofthese observations has been confirmed by other investi-gators; also the results of one of these studies (8)could not be reproduced by the senior investigator work-ing in another laboratory (9).
The present study was undertaken in order to charac-terize further the defect in water excretion and to evalu-ate the role of elevated levels of ADH in patients withhypopituitarism. Patients with anterior and posteriorhypopituitarism were studied during a sustained waterload using standard clearance techniques, and the ef-fects of hydrocortisone and ethanol, a known inhibitorof ADHsecretion (10-12), upon urinary dilution wereevaluated. All patients with anterior hypopituitarismdemonstrated an abnormality in the ability to dilute the
1478 The Journal of Clinical Investigation Volume 50 1971

urine, but a wide spectrum of defects was found. Bothhydrocortisone and ethanol administration effected im-provement in urinary dilution in these patients whilehydrocortisone did not influence urinary dilution inpatients with posterior pituitary insufficiency receivinginfusions of vasopressin. The data suggest a major rolefor inappropriately elevated levels of ADH in the de-fect in water excretion of glucocorticoid-deficient man.
METHODSSubjects
29 studies were performed on seven patients with anteriorhypopituitarism, three patients with complete central dia-
U OsmP
O A * * * a
betes insipidus off vasopressin therapy, and one with bothanterior and posterior pituitary insufficiency. The diagnosisof hypopituitarism was established by determinations of uri-nary gonadotrophins, 17-ketosteroids, 17-hydroxy steroids,response to ACTH and metyrapone, PBI, 'I uptake, andresponse to thyroid-stimulating hormone. Patients wereselected for study on the basis of availability before initiationof therapy and not because of the presence of hyponatremia.Posterior pituitary insufficiency was diagnosed by hyper-tonic saline infusion, water deprivation (urine osmolalityless than 100 mOsm/kg), and response to intravenous vaso-pressin (urine osmolality greater than 500 mOsm/kg). Allpatients were admitted to the Clinical Research Center ofthe Hospital of the University of Pennsylvania and placedon a constant sodium and potassium intake of approxi-
(A) GM0
K/e2ZZ~\ .G
=
340
V.&i 2s0
TIME mninubs)
R.C.
300 310
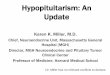
FIGURE 1 Response to a sustained water load in seven patients with anterior hypopituitarism,four of whom were unable to excrete a hypotonic urine (A) and three of whom were ableto excrete a hypotonic urine (B). In two of the patients in the latter group, urinary hypo-tonicity could not be sustained despite maintenance of the water load.
ADHand the Impaired Water Excretion of Anterior Hypopituitarism
6 110 180 2A0 300
(B)3.0'
2.01
.ILO.mP
0o60
IM2ULOW'
--~~~~~~~~wmmmm.
L
Oa7
1479

(A)LodE
UOs%
2.0iL0sm >-~~
_~~~~~~~~~~~~~~0 A
,=e0_ 20mg
60 120 180 240 300
(B)
3|0 L H1
1.-0_
W W ~40mg
0
60 120 1A0 AO 300
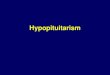
TIME(niinutes)FIGURE 2 The effect of the administration of graded doses of oral hydrocortisone1 hr before the initiation of a sustained water load in patients E. S. (A) andR. D. (B).
mately 100 and 40 mEq, respectively, for several days beforeperformance of the studies.
ProtocolsANTERIORHYPOPITUITARISMSustained water load. After 8-10 hr of hydropenia, 20
ml/kg of fluids was administered over 30-45 min either astap water by mouth or as intravenous 4% fructose in waterat 8-10 a.m.; during the entire experiment, the patient re-mained in the recumbent position. Subsequent fluids wereadministered in amounts equal to urine flow plus estimatedinsensible loss (40-50 ml/hr). Urine samples were collectedevery 30-60 min in most subjects by having the patientstand to void. In three patients, indwelling urinary catheterswere necessary to facilitate accurate collections. Informedconsent was obtained, and urine cultures 48 hr and 7 daysafter the studies revealed no growth. In order to minimize
the influence of noxious stimuli on the water diuresis, veni-punctures were not performed during the development orpeak of a water diuresis, but only 1 hr before the waterload was begun, at the end of the study, or after a definitedecrease in free water clearance or rise in urinary osmo-lality.
Hydrocortisone. In two patients, 100 mg of hydrocorti-sone was given intravenously during a sustained water loadat a time when the urine was hypertonic to plasma. Infive patients, hydrocortisone was given orally in doses of5, 10, 20, or 40 mg, 1 hr before initiation of a sustainedwater load. Fluid replacement, blood, and urine collectionswere obtained as above.
Ethanol. Ethyl alcohol was administered as 100 proofwhiskey diluted with small amounts of juice or carbonatedbeverage to five patients at varying times during a sustainedwater load as described above.
1480 Z. S. Agus and M. Goldberg

Ethanol plus hydrocortisone. In two patients, who failedto respond to alcohol alone, identical studies were per-formed after pretreatment with hydrocortisone in doses of10 and 20 mg. Ethyl alcohol was administered as previouslyduring a sustained water load, and blood and urine collec-tions were obtained as above.
POSTERIOR PITUITARY INSUFFICIENCYThree patients with complete central diabetes insipidus
and one with anterior and posterior pituitary insufficiencyreceived a sustained water load. Fluid maintenance, blood,and urine collections were performed as above. Simultane-ously with the water load, constant infusions of aqueousvasopressin providing 8-15 mU/hr were administered witha Harvard constant infusion pump. 100 mg of hydrocorti-sone was given intravenously during the study after a stableantidiuresis had been obtained.
MethodsUrine and serum electrolytes were determined by flame
photometry and creatinine as previously described (13).Osmolalities were determined with a Fiske osmometer andcorrected for ethanol concentration. Ethanol concentrationsof blood and urine were estimated by the microdiffusionmethod of Conway and Nolan, modified after Winnick (14).Solutions of known concentration of ethanol in serum were
checked both by chemical analysis and osmometry. Endoge-nous creatinine clearance was determined in the usual man-
ner. Osmolar clearance (Cosm) and free water clearance(CH2o) were calculated by the following formulas:
Cosm = Uosm/Poum X Vand CHE2o = V -Co.m
where Posm = osmolality of the serum (milliosmols perkilogram) and V urine flow (milliliters per minute).
(A)
HydrocortisoneW1mg
3.0
2.0
U Osmp
300
(B)Hydrocortisone20mg
11 2-0 -
u Osmp
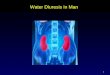
FIGURE 3 The effect of the administration of oral hydrocortisone 1 hr beforethe initiation of a sustained water load in patients M. M. (A) and J. D. (B).
ADHand the Impaired Water Excretion of Anterior Htipopituitarism
LflZ0 LOau'_
120 180TIME(minutes)
IH20
1481

RESULTSAnterior hypopituitarismResponse to sustained water load. The normal re-
sponse to a sustained water load of comparable dura-tion has been previously published (15) and is charac-terized by maintenance of urine hypotonicity and a urine/plasma (U/P) osmolal ratio of less than 0.3 throughoutthe study. In all seven patients in the present study,there was a defect in water excretion manifested by aninability to dilute maximally the urine in response to astandard water load. The response, however, was vari-able, and the patients could be divided into two groups.Group I, as shown in Fig. 1 (A), included four pa-tients who were unable to excrete a dilute urine andmaintained a U/P osmolal ratio of greater than 1throughout the study. Three of the four patients (J. D.,E. S., and M. M.) manifested hyponatremia, rangingfrom 120 to 130 mEq/1 before the institution of the
(A)
studies. Group II, as shown in Fig. 1(B), consisted ofthree patients who were able to excrete a urine hypo-tonic to plasma. In two, J. S. and G. R., this was notsustained, and the U/P ratio gradually rose to hyper-tonic levels despite maintenance of the water load. Thethird patient, P. C., had a very mild defect recognizableonly when compared with the studies obtained after hy-drocortisone and alcohol as will be shown below. None ofthe group II patients mainfested hyponatremia duringtheir course.
Response to hydrocortisone. The administration ofhydrocortisone in all patients produced a rapid improve-ment in the ability to excrete a water load. The effectsof hydrocortisone given orally 1 hr before the institutionof the water load in the group I patients are shown inFigs. 2 and 3. The response to glucocorticoid administra-tion appeared to be dose related. Thus, in E. S., as shownin Fig. 2A, the oral administration of 5, 10, and 20 mg
IH2u LOaW
Hydrocortisone 100mg I.v.
(B) Irr2V H o n 0 v
Hydrocortisone 100mi l.v.
0I,
TIME(mlnutes)
FIGURE 4 The effect of intravenous hydrocortisone given at a time whenthe urine was hypertonic upon urinary dilution in patients J. S. (A) andG. R. (B) during a sustained water load.
1482 Z. S. Agus and M. Goldberg

TABLE I
Response to Hydrocortisone
Before therapy* After hydrocortisone*
Patient Ccr Min. Uosm CH20 COsm Dose Ccr Min. U0am CH20 COsm
ml/min mOsm/kg ml/min mil/min mg ml/min mOsm/kg mi/min mi/minM. M. 74 709 -0.8 1.71 10 74 213 0.5 3.6R. D. 125 494 -0.8 1.7 40 115 66 8.0 2.5E. S. 48 391 -0.35 1.03 20 69 50 9.2 2.31J. D. 60 330 -1.0 4.0 20 83J. S. 106 83 3.5 1.4 100 118 51 7.4 1.6G. R. 57 90 2.9 1.5 100 65 42 6.1 1.5P. C. 95 75 4.1 1.6 20 66 61 8.3 2.3
Cc", CH2o, and Cosm = clearance of creatinine, solute-free water, and osmols, respectively. Min. UOsm= minimal urinary osmolality.
* Values represent the mean of two to three consecutive periods at a time of minimal urinary osmolalityduring a standard water load. In -five patients, the values were obtained in two separate studies. Thecontrol values were obtained during a standard water load and the hydrocortisone values during a studypreceded by an oral dose of hydrocortisone. In two patients, J. S. and G. R., hydrocortisone was givenintravenously during the study, and the values given represent the mean of two to three consecutiveperiods at a time of minimal urinary osmolality before and after hydrocortisone infusion.
of hydrocortisone produced a graded improvement inthe response to a water load. It is also apparent in Figs.2 and 3 that submaximal doses of hydrocortisone con-verted the severe defect of three of the four group Ipatients to the milder defect of group II, i.e., the excre-tion of urine which was transiently hypotonic, but fol-lowed by a secondary rise in urinary osmolality. Theeffects of intravenous administration of 100 mg of hy-drocortisone in two group II patients, J. S. and G. R.,given as the U/P osmolal ratio was rising, are shown inFig. 4. Approximately 30-60 min after administration,urine osmolality fell to levels below those previously ob-tained at any time during the water load and wassustained.
The response to hydrocortisone of all seven patientsis summarized in Table I. In the group I patients (E. S.,R. D., J. D., and M. M.) in association with the markedfall in minimal urine osmolality there occurred sub-stantial increases in free water excretion. Accurateclearance values for J. D. after the administration ofhydrocortisone were not available because of a leakaround the urinary catheter. There were no consistentchanges in either osmolar or creatinine clearance. Inthe group II patients (J. S., G. R., and P. C.) hydro-cortisone produced a marked fall in urine osmolality anda rise in free water clearance in all three and reversedthe secondary rise in urinary osmolality in J. S. andG. R.
Response to ethanol. The administration of ethanolduring a water diuresis to two of the patients in groupI (J. D. and E. S.) while the urine was hypertonic,produced no response in either urinary osmolality or free
water excretion, and the data were identical with thosedepicted in Fig. 1. In group II, however, the administra-tion of ethanol produced a fall in urinary osmolality, ifgiven at a time when the urine was hypotonic. Fig. 5depicts this phenomenon in J. S. When the ethanol wasgiven to J. S. after the rise in urinary osmolality hadreached hypertonicity, there was no demonstrable effect(Fig. 5A). The administration of 30 g of ethanol twice,as urine osmolality began to rise, but was still hypo-tonic, produced a fall in urine osmolality, a rise in freewater excretion, and prevented the development of hy-pertonicity (Fig. 5B). Qualitatively similar responses toethanol occurred in the other group II patients G. R. andP. C. (Fig. 6). When administered while the urine washypotonic, ethanol either reversed the late secondary risetoward hypertonicity (Figs. 1 and 6A) or improvedboth Uo0m and free water excretion (Fig. 6B).
Responses of group I patients to ethanol plus hydro-cortisone. The lack of response to ethanol in the groupI patients might be due either to the absence of elevatedlevels of ADHor decreased sensitivity of the neurohy-pophysis to the inhibitory effects of ethanol. To assessthese possibilities, two patients, J. D. and E. S., werepretreated with submaximal doses of hydrocortisone be-fore the study. As shown in Fig. 7, after initial hydro-cortisone doses of 20 and 10 mg, respectively, J. D. andE. S. were able to produce a dilute urine which, how-ever, could not be sustained as previously documentedin Figs. 3 and 4. While urinary osmolality was risingbut was still hypotonic, the oral administration was as-sociated with a response identical with that of the groupII patients, i.e., a fall in urinary osmolality and preven-
ADHand the Impaired Water Excretion of Anterior Hypopituitarism 11483

tion of the secondary rise to hypertonicity in bothpatients.
Posterior hypopituitarismIn order to study the action of hydrocortisone on
ADH-induced antidiuresis in subjects unable to reduceADH secretion, three patients with diabetes insipidusreceiving a water load were given a constant infusion ofvasopressin, designed to achieve levels of urinary os-molality comparable with those obtained in the group Ipatients. Fig. 8 demonstrates the rise in U/P osmolalitywith vasopressin infusion. The administration of 100 mgof hydrocortisone intravenously during the antidiuresishad no demonstrable effects. To eliminate the possibilitythat glucocorticoid deficiency was a prerequisite to atubular action of hydrocortisone, the identical studywas performed in a patient with combined anterior andposterior pituitary insufficiency. Fig. 9 demonstrates thatin this patient, the administration of intravenous hydro-
(A) IH20LoadI
cortisone had not effect upon the vasopressin inducedantidiuresis. Table II is a summary of the effect of in-travenous hydrocortisone upon osmolar clearance, freewater excretion, and creatinine clearance in these fourpatients receiving both a water load and vasopressin in-fusion. Free water excretion continued to fall in allwith hydrocortisone administration.
DISCUSSIONInability to excrete a water load in hypopituitarism iswell documented, and hyponatremia has been recognizedas a frequent manifestation (1-5). The defect has beenshown to be correctable by glucocorticoid administration(2, 3, 5), but the pathophysiologic mechanisms involvedremain controversial and incompletely understood. Inthe present study, seven patients with anterior hypo-pituitarism were studied, and in all there was a defectin water excretion. The defect was quite variable, and
(B) 1H20 LoadI
2.0.
O0
Ethanol Ethanol
L h6.0
4.0.
2.0
00
2001
100'
60 180 300TIME (minutes)
420 540 50 150 250
TIIME(minutes)
FIGURE 5 The effects of ethanol upon urinary dilution, solute-free water excretion, andcreatinine clearance during a sustained water load in J. D. (A) 30 g ethanol administeredorally when the urine was hypertonic. (B) 30 g ethanol administered orally twice when theurine was hypotonic.
1484 Z. S. Agus and M. Goldberg
4.0.cM2
2.0.(m6min)
0-TcH2o
2.0'
100'CCrL/min)
350 450
IV* ftmft*o NOUN==*
*a
III

) O dLoad
Ethanol
NI.
\_
100'
70 210 350TMEininutes)
490 630 70 210 350TIME(minutes)
FIGURE 6 The effect of the oral administration of 30 g ethanol upon urinary dilution, solute-free water excretion, and creatinine clearance in patients G. R. (A) and P. C. (B). Theethanol was given at a time when the urine was hypotonic.
a spectrum of responses was found ranging from totalinability to dilute the urine to an almost normal re-
sponse. The patients were divided into two groups basedupon their ability to respond. Four patients were unableto excrete a dilute urine while three excreted a hypo-tonic urine. The response to oral glucocorticoids ap-peared to be dose related within the physiologic range.The administration of submaximal doses to patients withthe most severe defect (group I) converted their re-
sponse into one characteristic of the milder defect(group II), i.e., transient dilution of the urine followedby a secondary rise to hypertonicity.
Ethyl alcohol has been previously shown to preventthe antidiuresis of dehydration and hypertonic salineadministration and to have no effect upon urine flowwhen given at the height of water diuresis or to dogswith diabetes insipidus. On the basis of these observa-tions, ethyl alcohol is considered to be an inhibitor ofADH secretion. The administration of ethanol to thepatients with the most severe defect in our studies re-
sulted in no significant change in diluting ability.However, when administered to those with the milderdefect, ethanol effected an improvement in dilutingability as characterized by a lowering of urinary osmo-
lality and increased excretion of solute-free water. Thisresponse was seen only when the ethanol was given ata time when the urine was still hypotonic. When pa-tients in group I had been pretreated with submaximaldoses of glucocorticoids so that they were now able todilute transiently the urine, the administration of ethanolat a time when the urine was hypotonic, produced as inthe group II patients a fall in urinary osmolality anda rise in solute-free water excretion. The lack of re-
sponse to ethanol when the urine was hypertonic, i.e.at a time when ADH secretion was maximal, is com-
patible with previously published data. Thus, ethanolis able to block the antidiuretic response to hypertonicsaline when given simultaneously with the initiation ofsaline infusion, but has no effect when superimposedupon a hypertonic saline antidiuresis (10). Our data sug-
ADHand the Impaired Water Excretion of Anterior Hypopituitarism
Ethanol
I,2.0'
AOsmp
Oa
6.0.CH20
4.0'(ml/min)
2.0.
TCH20
100'
Ccr(ml/mln)
O .490 .
(8) jH2oLmwL(A)
1485

(A) Ai20LoHydrocortisone 10mg
I 1.52
ICH20So
(nml/n)0
TH205T s~,
100*
CCr
(mi/mi.)
(B) H20Load_Hydrocortisone 20mg
2.0a
2.0
100'
50 150 250TUME(mlnutes)
350 450
FIGuRE 7 The effect of the oral administration of 30 g ethanol in two patients, E. S. (A)and J. D. (B), after treatment with oral hydrocortisone 1 hr before the initiation of thesustained water load. Ethanol administration to these two patients without pretreatment withhydrocortisone had no effect upon urinary dilution (see text).
gest, therefore, that elevated levels of ADHplay an im-portant role in the defect in water excretion charac-teristic of hypopituitarism. In the most severely af-fected patients, the neurohypophysis responds neitherto changes in plasma osmolality nor to ethanol adminis-tration while the less severely affected responded to both.The role of glucocorticoids is seen as a permissive one
(5). Thus, the administration of submaximal doses ofglucocorticoid, while not completely correcting the de-fect, permits sufficient suppression of ADHto allow theformation of dilute urine and a further response toethanol.
Another possible explanation of amelioration of thedefect by glucocorticoids in the presence of elevatedADH levels is antagonism of the peripheral action ofADHat the renal tubular level (6). Thus the absence ofglucocorticoids would be associated with an increasedsensitivity to ADH, and glucocorticoid administration
would decrease tubular permeability to water thus al-lowing maintenance of dilute urine and free water ex-
cretion. In order to study this possibility, patients withdiabetes insipidus were given a constant infusion ofvasopressin during a sustained water load. The ad-ministration of hydrocortisone intravenously had no
effect upon urinary diluting ability which suggests thatthe beneficial action of glucocorticoids in hypopituitarismis not a direct tubular effect but rather is related to theability to reduce circulating ADH levels. In order torule out the possibility that glucocorticoid deficiency was
a prerequisite for this phenomenon, an identical studywas performed in a patient with both anterior and pos-
terior pituitary insufficiency with identical results. Thus,glucocorticoids are effective in lowering urinary os-
molality during a water load in the face of elevated levelsof ADH only when the elevated levels are producedendogenously.
1486 Z. S. Agus and M. Goldberg
Ethanol
50 150 250TIME(manuts)
350 450
I
M.
-Jmr.

The role of ADH in the defect in water excretion ofglucocorticoid deficiency has been a source of controversysince Gaunt in 1947 first postulated a biological antago-nism between ADH and glucocorticoids (6). Attemptsto quantitate ADH levels directly by bioassay haveyielded conflicting results, both confirming (7) anddenying (8) the presence of elevated levels in this syn-drome. More recently, Davis, Bloom, Field, and Mintz(16) described a patient with hypopituitarism and hypo-natremia in whom urinary osmolality responded toethanol administration when pretreated with dexametha-sone similar to the patients described here. Green, Har-rington, and Valtin (17) showed that they could inducea defect in the response to a water load in adrenalecto-mized rats with diabetes insipidus which suggests thatthe presence of ADHwas not a prerequisite to the syn-drome. However, when the rats were replaced withmineralocorticoids, the impairment in urinary osmo-lality was ameliorated even though a defect in totalwater excretion persisted. Thus, they could not demon-strate a defect in urinary dilution when the adrenalec-tomized rat with diabetes insipidus was given mineralo-corticoids. As our patients with anterior hypopituitarismare able to secrete ADHand presumably maintained theability to secrete mineralocorticoid (18), but still mani-fest a defect in urinary dilution, our conclusion that ele-vated levels of ADHare important in this syndrome areconsistent with the data of Green et al. (17).
The reason for elevated levels of ADH in the face ofhypoosmolality in patients with glucocorticoid deficiencyis not clear from our data. Gill, Gann, and Bartter (19)presented data suggesting that volume repair of gluco-corticoid-deficient patients led to an improvement infree water excretion, and implied that hypovolemia wasthe stimulus to ADH release. Share and Travis (20)demonstrated elevated ADH levels in adrenalectomizeddogs and showed that this elevation could be preventedby a high salt intake. In our studies, however, the ra-pidity with which the defect could be corrected by in-travenous glucocorticoid administration and the absenceof a consistent fall in osmolar clearance after eitheroral or intravenous administration would argue againstvolume repletion as a major mechanism in the actionof glucocorticoid to improve urinary-diluting ability.
In addition to elevated levels of ADH, two other ex-planations have been suggested for the defect in waterexcretion of glucocorticoid deficiency. A decrease indelivery of glomerular filtrate to the diluting sites inthe loop of Henle and distal tubules due to changes inglomerular filtration rate and/or proximal tubular reab-sorptive rates could lead to a decrease in the excretionof free water and an increase in urinary osmolality (19,21). Previous studies in the literature (22) have shownthat increasing glomerular filtration rate alone in pa-
tients with glucocorticoid deficiency does not correctthe defect in water excretion. In our studies glucocorti-coids produced an improvement in urinary dilution in
(A)
2.0
AI Osmp
1.0
0
(B)
2A
.I Osmp
01
(C ) 5.1
Up
3.'osn
1.1
Vasopressin BmLlhrl Vasopressin l5mU/hr IWater intake = Urine Flow+ Insensible Loss
Hydrocortisone 100mg i.v.
0s owMead
;;/ ' 0
200 400 600
Vasopressin-8m ZZhrWater Intake = Urine Flow+ Insensible Loss
Hydrocortisone 100 mg i.v.
I 0
100 200 300
10 Water Intake -Urine Flow + Insensible Loss
Hydrocortisone 100mg i.v.
I .*eeo#f0_-_o 0
n~~0~~~~
100 200 300TEVE(minutes)
FIGURE 8 The effect of intravenous hydrocortisone uponurinary dilution in three patients with complete central dia-betes insipidus receiving a constant infusion of vasopressin.
ADHand the Impaired Water Excretion of Anterior Hypopituitarism 1
El
m 0 -0-L
1487

Vasopressin lOmU/hrWater Intake= Urine Flow + Insensible Loss
TIM E (minutes)
FIGURE 9 The effect of intravenous hydrocortisone upon urinary dilution ina patient with combined anterior and posterior pituitary insufficiency receivinga constant infusion of vasopressin.
all patients with anterior hypopituitarism without anassociated consistent change in endogenous creatinineclearance. An increase in proximal tubular sodium reab-sorption has been demonstrated in the glucocorticoid-deficient rat (23) but this has been attributed to a de-creased glomerular filtration rate and perfusion pressure,and is not a direct effect of glucocorticoid deficiency.Another explanation proposed for the defect in waterexcretion in glucocorticoid deficiency is a change in thepermeability to water of the distal tubules and collect-ing duct epithelium leading to increased back diffusion ofwater (22) in the absence of ADH. Evidence in favor ofthis concept is twofold. First, administration of gluco-corticoids to normal man will produce an improvement inboth Uomi and CHso in the absence of hemodynamicchanges (24, 25), and secondly, glucocorticoids willrestore to normal the enhanced water permeability ofthe distal tubule of the adrenalectomized rat (26).
Both of these observations, however, require severaldays of glucocorticoid therapy while the response inour studies was an immediate one. In addition, in threepatients with diabetes insipidus and one with anteriorpituitary insufficiency and diabetes insipidus, the intra-venous administration of glucocorticoid had no effectupon either urinary osmolality or solute-free water ex-cretion when pitressin was simultaneously infused.Thus, while changes in renal hemodynamics and distaltubular water permeability may contribute to the defectin water excretion in hypopituitarism, elevated levels ofADH secondary to glucocorticoid deficiency would ap-pear to play a major role in this syndrome.
ACKNOWLEDGMENTSWe acknowledge the technical assistance of Mrs. JeanElias, and are grateful to Lidia Kosolopovs and LeonidKosolopovs for the laboratory analysis. We also wish to
TABLE I IEffects of Hydrocortisone in Patients with Diabetes Insipidus Receiving Constant Infusion of Vasopressin
Before hydrocortisone* Hydro- PosthydrocortisonetVasopressin cortisone
Patient dose COmm Ccr CH20 dose COmm Ccr CH20
mU/hr mg
A. B. 8 0.67 70.1 0.12 100 1.09 152 -0.42T. H. 10 2.53 86.1 -1.72 100 2.7 87.1 -1.98G. M. 15 0.95 30.0 -0.33 100 0.85 34.7 -0.39P. R. 10 1.20 94.3 -0.3 100 1.37 114 -0.63
Abbreviation as in Table I.* Values represent the mean of three consecutive periods of 10-25 min duration before infusion of hydro-cortisone.t Values represent the mean of three to four consecutive periods of 10-30 min duration beginning 30-45 minafter infusion of hydrocortisone.
1488 Z. S. Agus and M. Goldberg

thank Miss Cordelia Shute and the nursing staff of theClinical Research Center, Hospital of the University ofPennsylvania for their cooperation.
This project was supported in part by U. S. PublicHealth Service grants HE-00340, HE-07284, Clinical Re-search Center Grant 5MO1 RR40-10, Training grant AM05634, and a Research Career Development Award AM18,582.
REFERENCES1. Slessor, A. 1951. Studies concerning the mechanism of
water retention in Addison's disease and in hypopitui-tarism. J. Clin. Endocrinol. Metab. 11: 700.
2. Oleesky, S., and S. W. Stanbury. 1956. Effect of oralcortisone on water diuresis in Addison's disease andhypopuituitarism. Lancet. 2: 664.
3. Garrod, O., and R. A. Burston. 1952. The diuretic re-sponse to ingested water in Addison's disease and pan-hypopituitarism and the effect of cortisone thereon.Clin. Sci. (London). 11: 113.
4. Bethune, J. E., and D. H. Nelson. 1965. Hyponatremiain hypopituitarism. N. Engl. J. Med. 272: 771.
5. Dingman, J. F., and R. Despointes. 1960. Adrenalsteroid inhibition of vasopressin release from the neuro-hypophysis of normal subjects and patients with Addi-son's disease. J. Clin. Invest. 39: 1851.
6. Gaunt, R., J. H. Birnie, and W. J. Eversole. 1949.Adrenal cortex and water metabolism. Physiol. Rev.29: 281.
7. Abdul, B., J. Ahmed, B. C. George, C. Gonzalez-Auvert,and J. F. Dingman. 1967. Increased plasma argininevasopressin in clinical adrenocortical insufficiency and itsinhibition by glucosteroids. J. Clin. Invest. 46: 111.
8. Kleeman, C. R., J. W. Czaczkes, and R. Cutler. 1964.Mechanisms of impaired water excretion in adrenal andpituitary insufficiency. IV. Antidiuretic hormone in pri-mary and secondary adrenal insufficiency. J. Clin. Invest.43: 1641.
9. Vorherr, H., C. R. Kleeman, and M. Hoghoughi. 1968.Factors influencing the sensitivity of rats under ethanolanesthesia to antidiuretic hormone (ADH). Endocrinot-ogy. 82: 218.
10. Kleeman, C. R., M. E. Rubini, E. Lamdin, and F. H.Epstein. 1955. Studies on alcohol diuresis II. The evalua-tion of ethyl alcohol as an inhibitor of the neurohy-pophysis. J. Clin. Invest. 34: 448.
ll. Van Dyke, H. B., and R. G. Ames. 1951. Alcohol diure-sis. Acta Endocrinol. 7: 110.
12. Eggleton, M. G. 1943. The diuretic action of alcohol inman. J. Physiol. (London). 101: 172.
13. Goldberg, M. 1962. Studies of the acute renal effectsof hemolyzed red blood cells in dogs, including estima-
tions of renal blood flow with krypton'. J. Clin. Invest.41: 2112.
14. Conway, E. J. 1957. Microdiffusion Analysis and Volu-metric Error. Crosby Lockwood & Son Ltd., London.4th edition. 248-251.
15. Goldberg, M., D. K. McCurdy, E. L. Foltz, and L. W.Bluemle, Jr. 1964. Effects of ethacrynic acid (a newsaluretic agent) on renal diluting and concentratingmechanisms: evidence for site of action in the loop ofHenle. J. Clin. Invest. 43: 201.
16. Davis, B. B., M. E. Bloom, J. B. Field, and D. H.Mintz. 1969. Hyponatremia in pituitary insufficiency.Metab. (Clin. Exp.). 18: 821.
17. Green, H. H., A. R. Harrington, and H. Valtin. 1970.On the role of antidiuretic hormone in the inhibition ofacute water diuresis in adrenal insufficiency and, theeffects of Gluco- and mineralocorticoids in reversing theinhibition. J. Clin. Invest. 49: 1724.
18. Garcia, Llaurado, J. G. 1957. Aldosterone excretion fol-lowing hypophysectomy in man: relation to urinaryNa/K ratio. Metab. (Clin. Exp.) 6: 556.
19. Gill, J. R., Jr., D. S. Gann, and F. C. Bartter. 1962.Restoration of water diuresis in Addisonian patients byexpansion of the volume of extracellular fluid. J. Clin.Invest. 41: 1078.
20. Share, L., and R. H. Travis. 1970. Plasma vasopressinconcentration in the adrenally insufficient dog. Endocrin-ology. 86: 196.
21. Berliner, R. W., and D. G. Davidson. 1956. Productionof hypertonic urine in absence of pituitary antidiuretichormone. J. Clin. Invest. 35: 690.
22. Kleeman, C. R., M. H. Maxwell, and R. E. Rockney.1958. Mechanisms of impaired water excretion in adrenaland pituitary insufficiency I. The role of altered glomeru-lar filtration rate and solute excretion. J. Clin. Invest.37: 1799.
23. Hierholzer, K., and H. Stolte. 1969. The proximal anddistal tubular action of adrenal steroids on Na reab-sorption. Nephron. 6: 188.
24. Raisz, L. E., W. F. McNeeley, L. Saxon, and J. D.Rosenbaum. 1957. The effects of cortisone and hydro-cortisone on water diuresis and renal function in man.J. Clin. Invest. 36: 767.
25. Kleeman, C. R., J. Koplowitz, M. H. Maxwell, R. Cutler,and J. T. Dowling. 1960. Mechanisms of impaired waterexcretion in adrenal and pituitary insufficiency II. In-terrelationships of adrenal cortical steroids and anti-diuretic hormone in normal subjects and in diabetes in-sipidus. J. Clin. Invest. 39: 1472.
26. Stolte, H., F. P. Brecht, M. Wiederholt and K. Hier-holzer. 1968. Einfluss von adrenalektomie und glucocor-ticoiden auf die Wasserpermeabilitat corticaler nephro-abschnitte der rattenniere. Pfluegers Arch. 299: 99.
ADHand the Impaired Water Excretion of Anterior Hypopituitarism 11489