Embed Size (px)
Citation preview
Department of Oncology and
Haematology Azienda Ospedaliera
Policlinico di Modena.
Novità nel campo della Genetica Medica

Genetic Helps us to Identify Patients at High Risk of Developing Breast and Ovarian Cancer
Genetics
• Genetics is the study of heredity
While genetics influence genomics, genetics is responsible for only 5-10% of breast cancer
• Genetics focuses primarily on the likelihood of developing cancer
• Genetic tests find mutations, not disease
Source: Understanding Cancer Series: Gene Testing, National Cancer Institute

Key point: whole body has the mutation
Knudson A, PNAS 1971
Two Hits Hypothesis
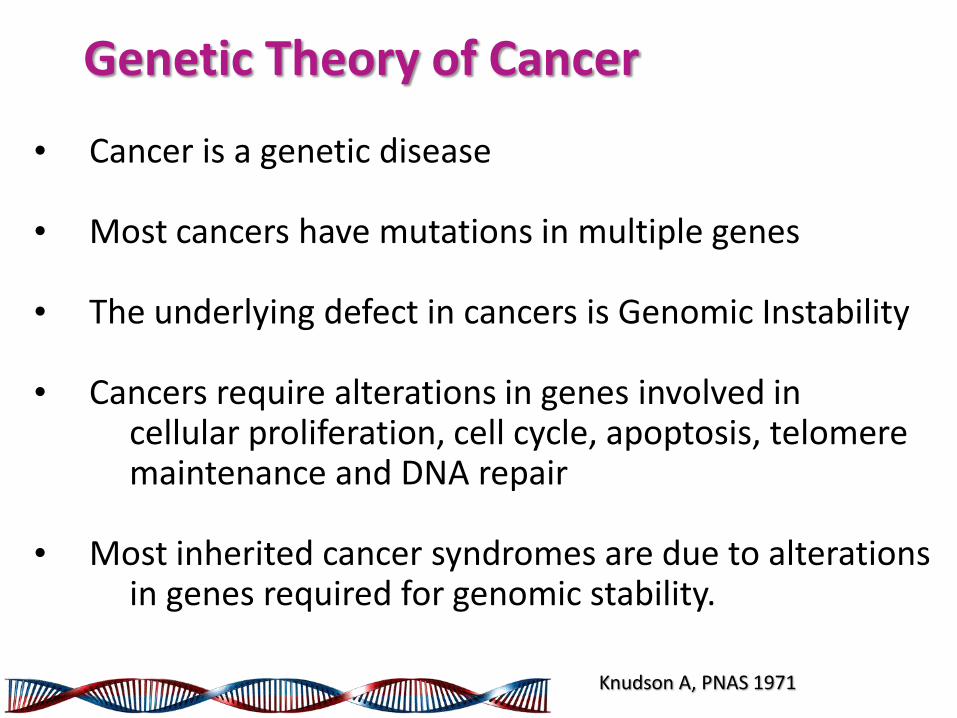
Genetic Theory of Cancer
• Cancer is a genetic disease • Most cancers have mutations in multiple genes • The underlying defect in cancers is Genomic Instability • Cancers require alterations in genes involved in
cellular proliferation, cell cycle, apoptosis, telomere maintenance and DNA repair
• Most inherited cancer syndromes are due to alterations in genes required for genomic stability. Knudson A, PNAS 1971
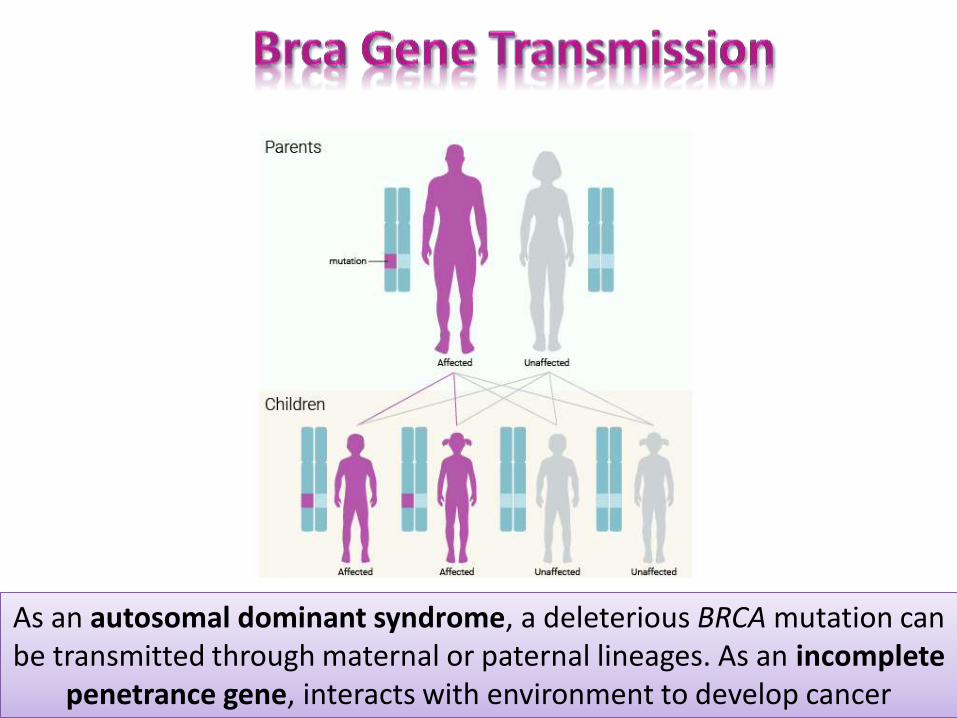
As an autosomal dominant syndrome, a deleterious BRCA mutation can be transmitted through maternal or paternal lineages. As an incomplete
penetrance gene, interacts with environment to develop cancer
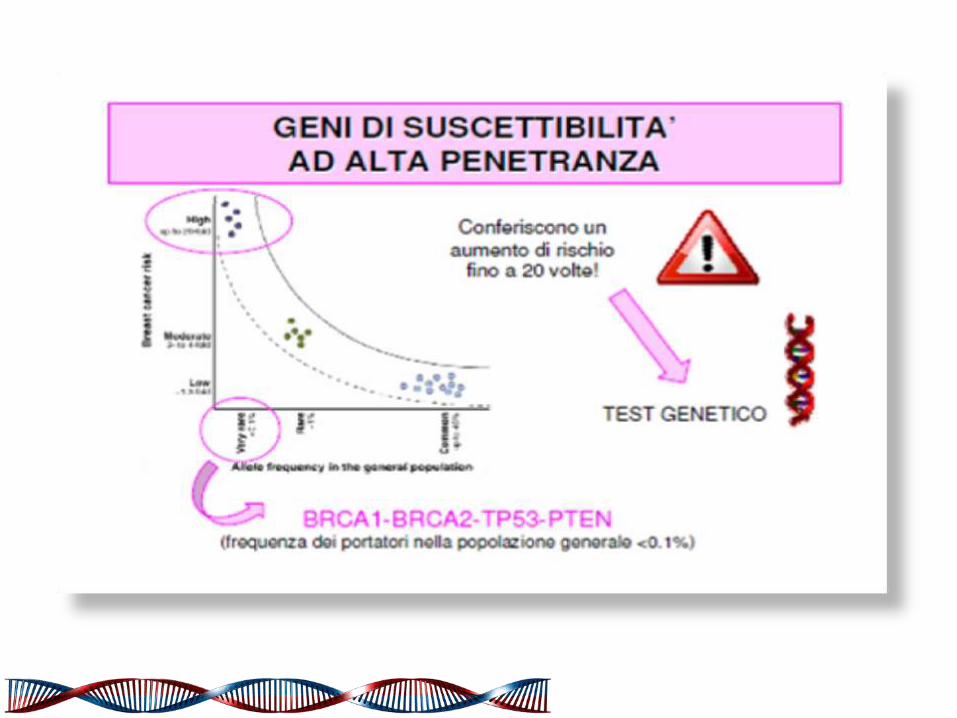


SYNDROME TUMORAL SPECTRUM TRANSMISSION GENES
BREAST/OVARY Breast, ovary, uterus, prostate,
stomach, colo-rectum, pancreas, bilious tract, melanoma
Dominant autosomal BRCA 1 BRCA2
LI-FRAUMENI Soft tissues, breast, bone, leukemya,
brain, adrenal Dominant autosomal P53
COWDEN Breast, tyroid, endometrium
(amartomes) Dominant autosomal
PTEN
Diffuse Gastric Cancer
Stomach, Lobular Breast Dominant autosomal CDH1
HNPCC (Lynch Syndrome)
Colo-rectum, ovary, endometrium, bladder, urinary tract, pancreas,
stomach, bilious tract, breast
Dominant autosomal
MLH1 MSH2 MSH6
PEUTZ-JEGHERS Colo-rectum, stomach, ovary, testis,
cervix, pancreas, breast Dominant autosomal
LKB1
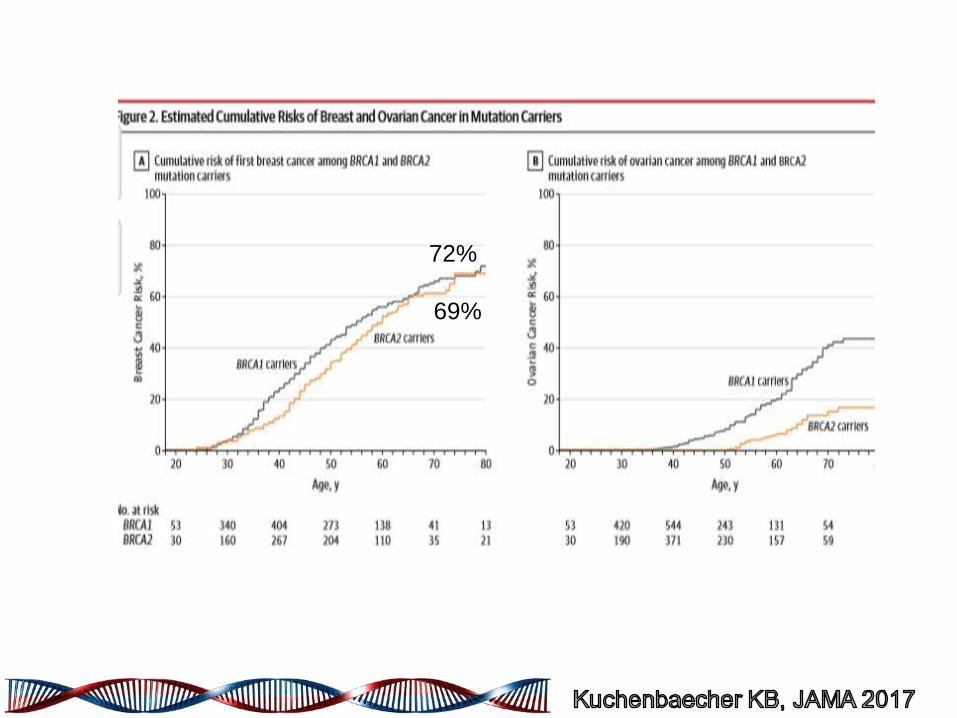
72%
69%
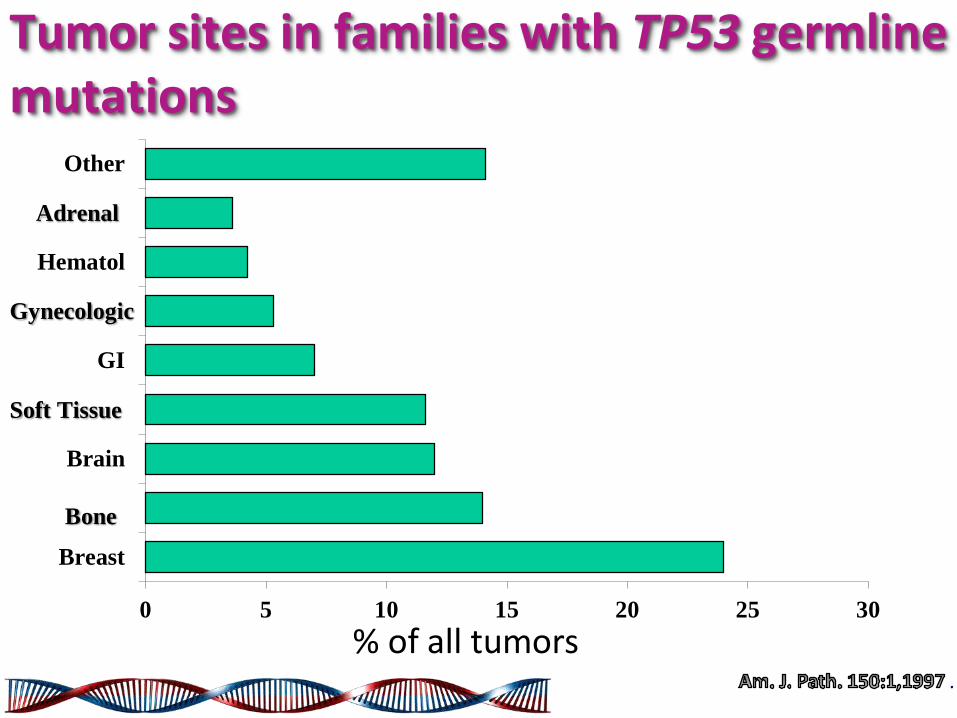
Tumor sites in families with TP53 germline mutations
% of all tumors 0 5 10 15 20 25 30
Breast
Brain
GI
Hematol
Other
Bone
Soft Tissue
Gynecologic
Adrenal
.

Cowden Syndrome Cancer Risks
Tumor Site Risk
Pilarski R. JGC.2009;18:13-27
Risk
Tan et al. Clin Can Res. 2012;18(2):400-7
Breast 25-50% 85%
Thyroid 3-10% 35%
Endometrial 5-10% 28%
Renal Cell Unknown 34%
Melanoma Unknown 6%
Colon Unknown 9%
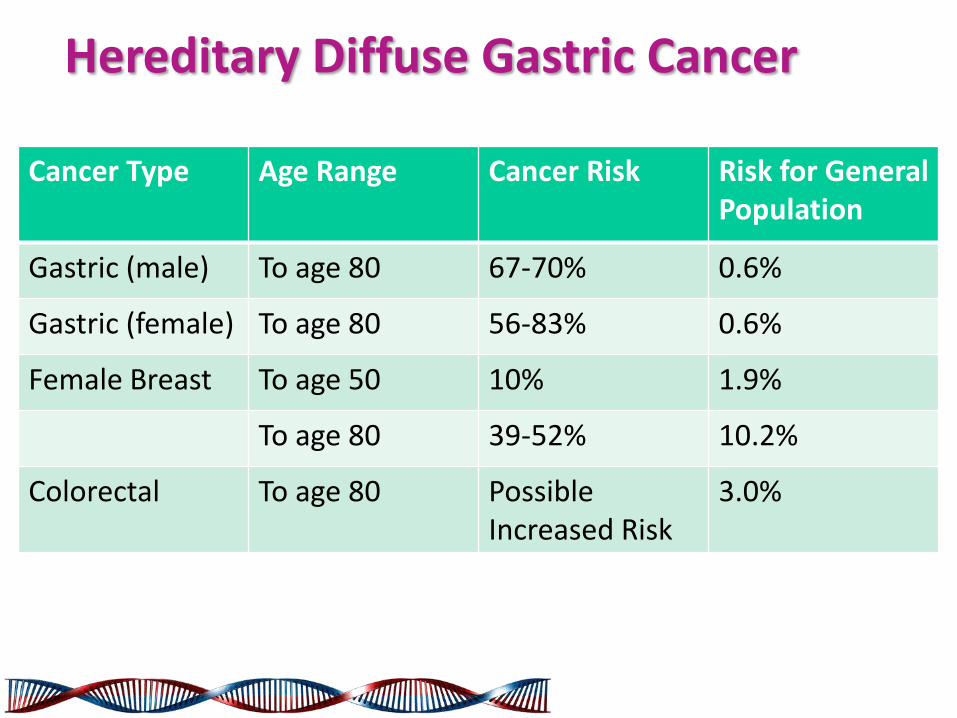
Cancer Type Age Range Cancer Risk Risk for General Population
Gastric (male) To age 80 67-70% 0.6%
Gastric (female) To age 80 56-83% 0.6%
Female Breast To age 50 10% 1.9%
To age 80 39-52% 10.2%
Colorectal To age 80 Possible Increased Risk
3.0%
Hereditary Diffuse Gastric Cancer

0
20
40
60
80
100
0 20 40 60 80
Colorectal
Endometrial
Stomach
Biliary tract
Urinary tract
Ovarian
78
43
19
18
10
9
%
Age (years)
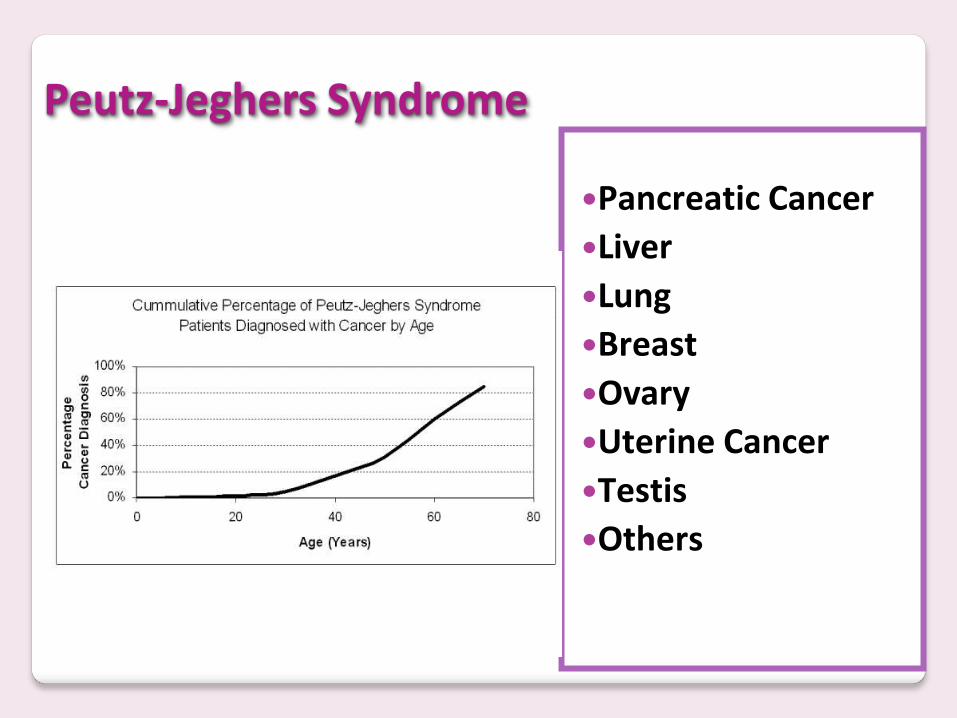
Peutz-Jeghers Syndrome
Pancreatic Cancer
Liver
Lung
Breast
Ovary
Uterine Cancer
Testis
Others

Website for BRCA classification ◦ BRCA exchange ◦ ClinVar ◦ BIC ◦ LOVD ◦ HCI ◦ A-GVGD
Website for functional analysis of BRCA
• BRCA Circos
• LOVD BRCA1
• LOVD BRCA2

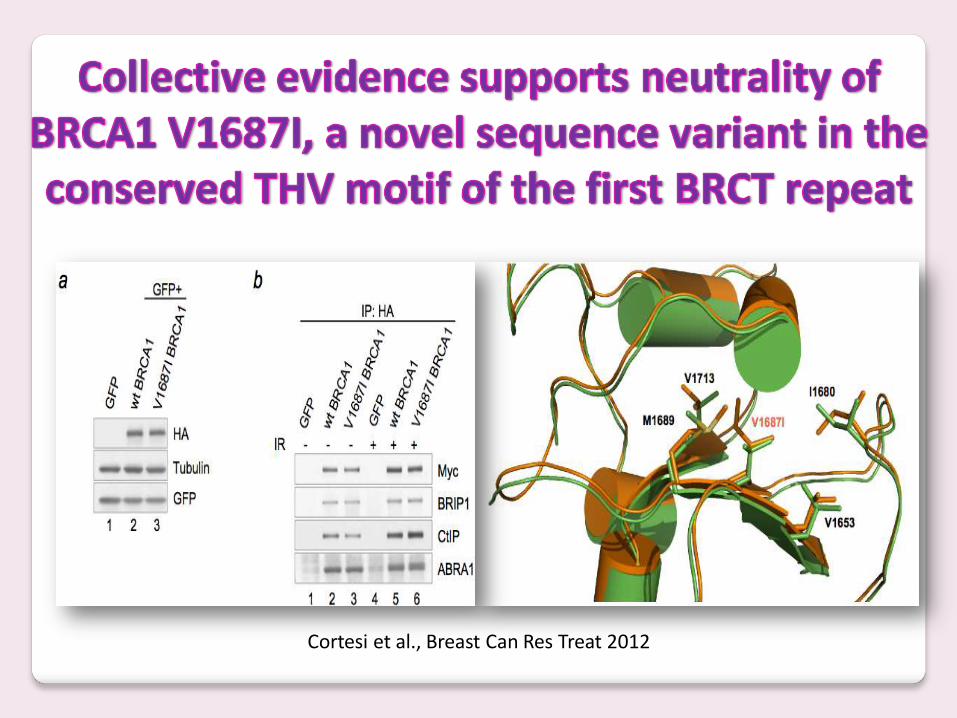
Cortesi et al., Breast Can Res Treat 2012

BRCA1 p.His1673del is a pathogenic mutation associated with a predominant ovarian cancer
phenotype
Zuntini et al., Oncotarget 2017

Prevention of tumorigenesis
DNA repair Protein Ubiquitination
Regulation of transcription
Regulation of cell cycle
Repair of double strand DNA breaks / DNA adducts
Mediates E2-dependent ubiquitination
Modulates gene expression in response to cell stress P21 DNA damage
Induces cell cycle arrest at the G1/S, S and G2/M checkpoints
Cellular function regulated by BrCa1
BRCA1 tumor suppressor protein

BRCA2
RAD51
DNA damaging RAD51 forms nucleoprotein filaments
RAD51 RAD51
RAD51
RAD51
RAD51
BRCA1
BRCA1 is a DNA damaging “detector”, blocks the transcription by cell cycle arrest at the G1/S, S and G2/M checkpoints and by ubiquitination of FANCD1
otherwise induces the DSB repair by chromatin remodelling
Chk2
ATM ATR
Toss & Cortesi, 2013
A
L
F
C
E
G
D1 Ub B
M
I

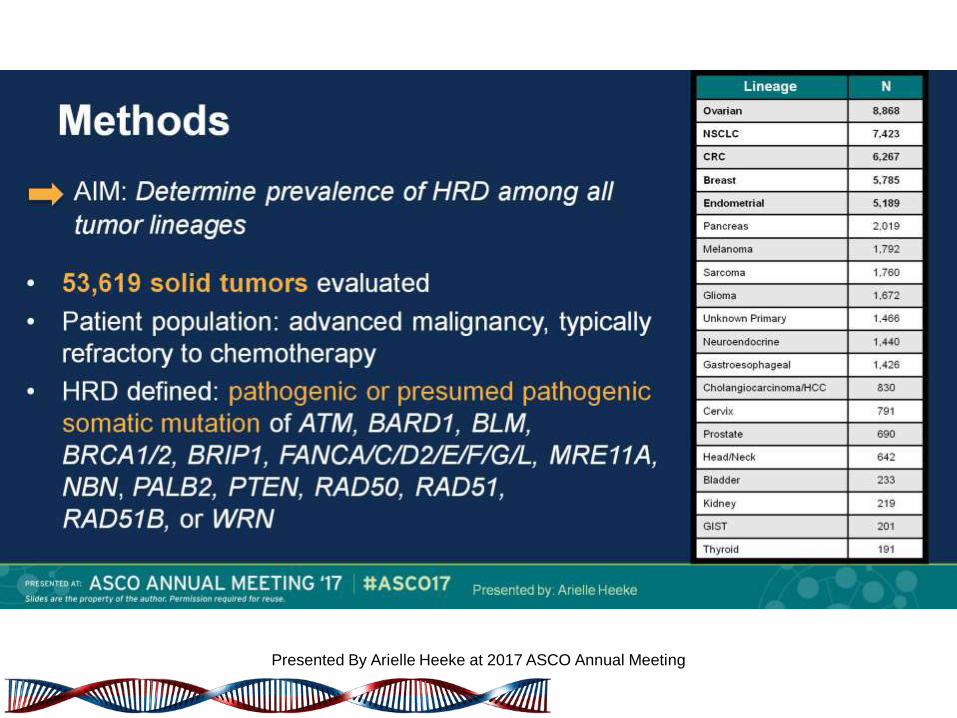
Methods
Presented By Arielle Heeke at 2017 ASCO Annual Meeting
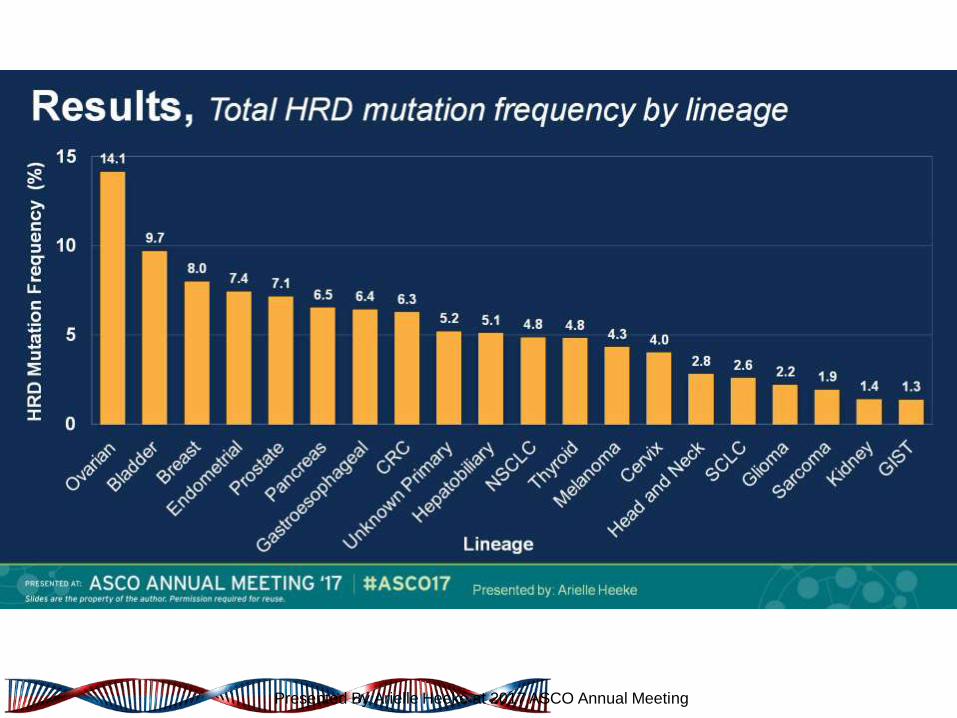
Results, Total HRD mutation frequency by lineage
Presented By Arielle Heeke at 2017 ASCO Annual Meeting

Results, HRD mutation landscape by lineage
Presented By Arielle Heeke at 2017 ASCO Annual Meeting

Niraparib Plus Carboplatin in Patients with Homologous Recombination Deficient Advanced Solid Tumor Malignancies
Presented By Arielle Heeke at 2017 ASCO Annual Meeting


Multi-Gene (NGS) Panels
• Genetic tests to look at dozens of genes related to cancer
• Similar cost and turn around time as gene specific testing
• Higher risk of uncertain results



ACCE FRAMEWORK
Parameter Definition
Analytic Validity
How well test measures property or chracteristics it is intended to measure
Clinical Validity
Accuracy of the test in diagnosing or predicting risk for health condition (sensitivity, specificity, PPV, NPV)
ELSI
Ethical, Legal and Social Implication
ACTIONABILITY
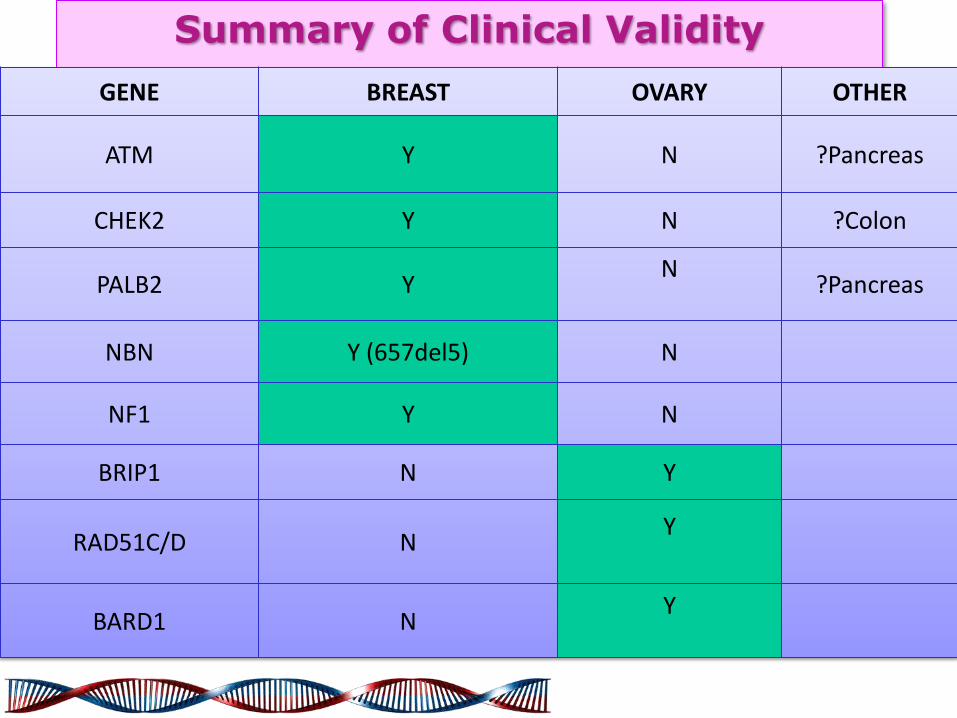
Summary of Clinical Validity
GENE BREAST OVARY OTHER
ATM Y N ?Pancreas
CHEK2 Y N ?Colon
PALB2 Y N
?Pancreas
NBN Y (657del5) N
NF1 Y N
BRIP1 N Y
RAD51C/D N Y
BARD1 N Y
Normal ATM protein Function
• A Serine-Protein Kinase as p53 or BRCA1
• Senses Double Stranded Breaks in DNA
• Activates cell cycle checkpoints
• Mutant ATM causes A-T, a genomic instability syndrome, which is lethal by age 20.
• Mutant ATM heterozygotes have increased risk of breast, leukemia, lymphomas and stomach cancer.

Gene Variant Tumor type
CHEK2 pI157T Br, CCR, Pr, Kidney, Bladder
CHEK2
c1000delC Br, CCR, Pr
CHEK2
pS428F Br
CHEK2
Cdel5395 Br, Pr
CHEK2
c.IVS2 + 1G > A Br, Pr, Tyr
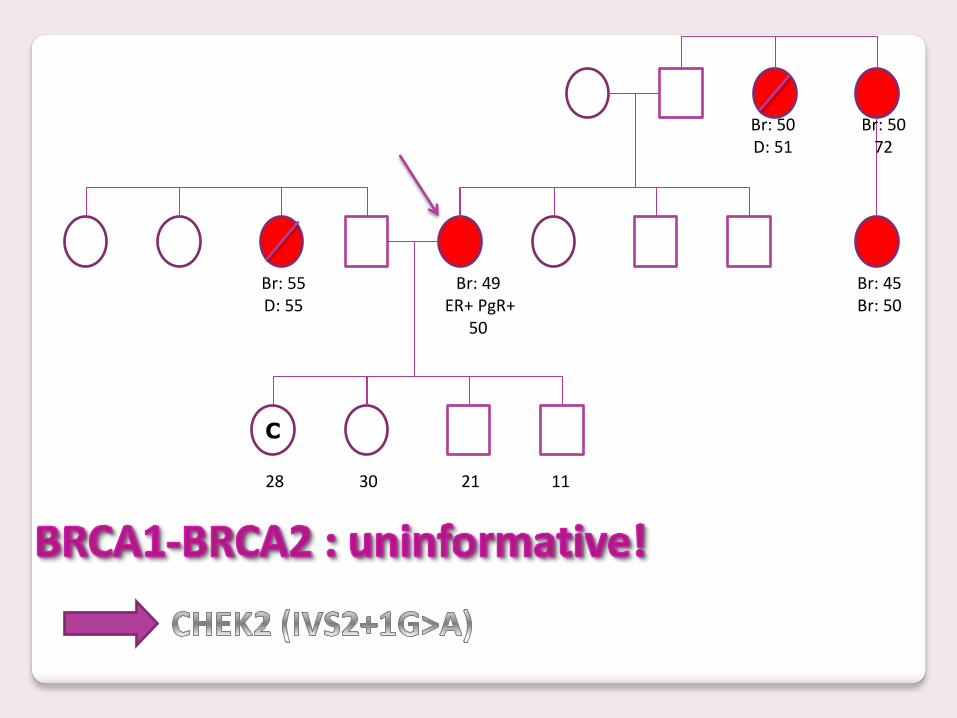
C
28 30 21 11
Br: 49 ER+ PgR+
50
Br: 45 Br: 50
Br: 50 D: 51
Br: 50 72
Br: 55 D: 55

PALB2 in BRCA1&2 negative pts

Cancer Type
Age Range Cancer Risk
Risk for General Population
Breast To age 80 Up to 30% 10.2%
Prostate To age 80 Increased Risk
10.9%
NBN Gene Mutation

46
NF1 Gene
NF1 is a tumor suppressor gene
NF1 is located on Chromosome 17 long arm
- NF2 on other hand is
located on Chromosome 22
NF1 gene encodes the protein Neurofibromin

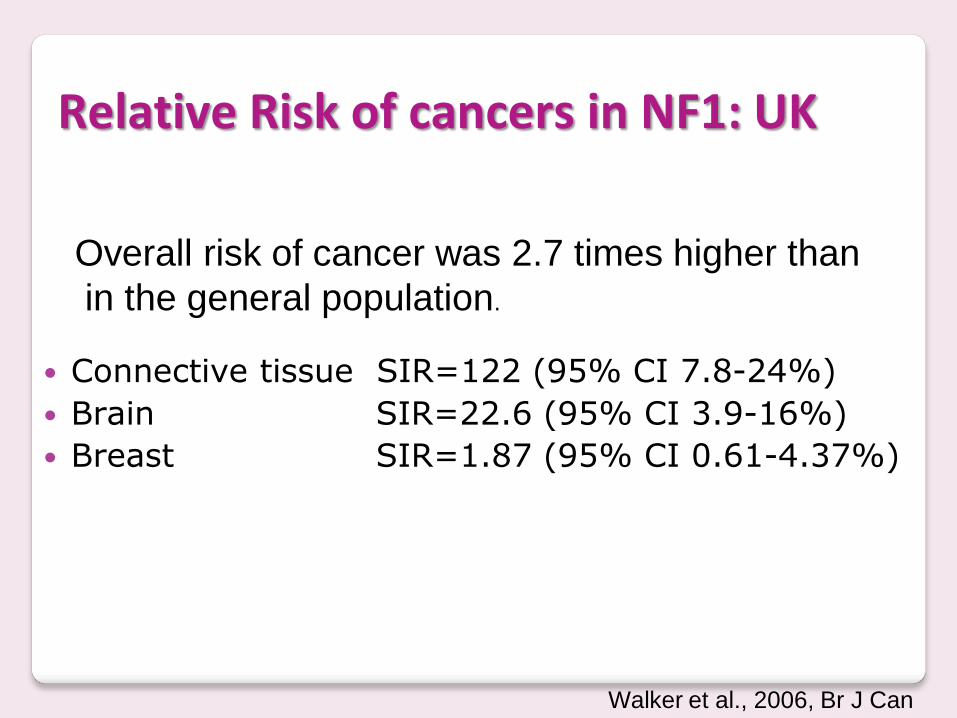
Relative Risk of cancers in NF1: UK
Overall risk of cancer was 2.7 times higher than
in the general population.
Connective tissue SIR=122 (95% CI 7.8-24%)
Brain SIR=22.6 (95% CI 3.9-16%)
Breast SIR=1.87 (95% CI 0.61-4.37%)
Walker et al., 2006, Br J Can

The transfer of multigene panel testing for hereditary breast and ovarian cancer to
healthcare: What are the implications for the management of patients and families?
Eliade M et al., Oncotarget 2017
ASCO supports the communication to patients of medically relevant incidental germline findings conducted in the clinical setting. Oncology providers should communicate the potential for incidental germline information to patients and should review the potential benefits, limitations, and risks before testing.
ASCO Policy Statement

NGS offers promise, but poses significant challenges for oncologists who are ill prepared to handle incidental findings that have clinical implications for at-risk family members. This report underscores the need for oncologists to develop a framework for pre- and post-communication of risks to patients undergoing routine multi-gene panels testing
Ready for Surprises?

• All BRCA1 and BRCA2 pathogenic variants regardless of tumor type (NCCN guideline)
• Founder mutations (ie. MSH2 exon 1-6 deletion, TP53 R337H)
• Uncommonly mutated genes (ie. CHEK2, PALB2)
Germline Finding Report

N° of UV in different genes for patients
Kurian AW et al., JCO 2014
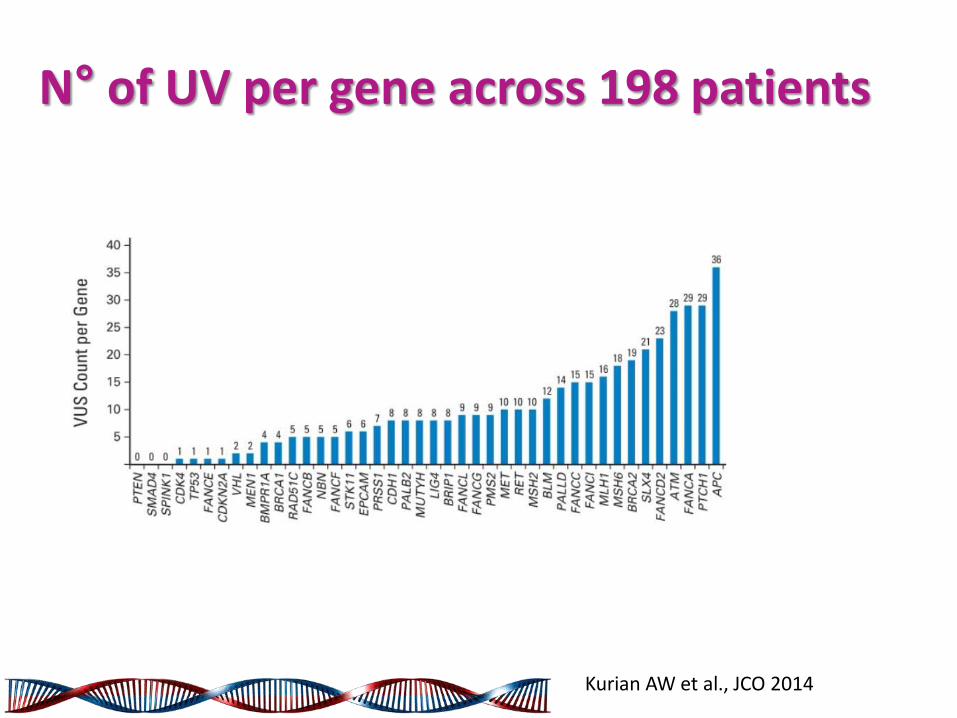
N° of UV per gene across 198 patients
Kurian AW et al., JCO 2014


Matsuzawa et al., Mol Cell 2014

BRCA1
BARD1
OLA1 ?
BRCA1
BARD1
OLA1
E168Q
?
OLA1
mutation BRCA1
mutation
BRCA1 I62V
BARD1
OLA1 ?
BRCA1
BARD1
V695L
OLA1 ?
BARD1
mutation
Modified by Chiba N

H.Chen et al., Scient Rep 2015

Genome-wide association analysis of more than 120,000 individuals identifies 15 new susceptibility loci for breast cancer
Michailidou, Nat Gen 2015

CONCLUSIONS
• Oncogenetic counselling as prediction of treatment response and mutation carrier
• HRD analysis by NGS for PARP-inhibitor using
• Role for MGPs in individuals who are negative for hereditary syndrome but with suggestion for susceptibility
• Refer results only for «actionable» genes
• A professional genetic expertise needs for MGPs
• GWA will be able to identify new susceptibility loci for BC

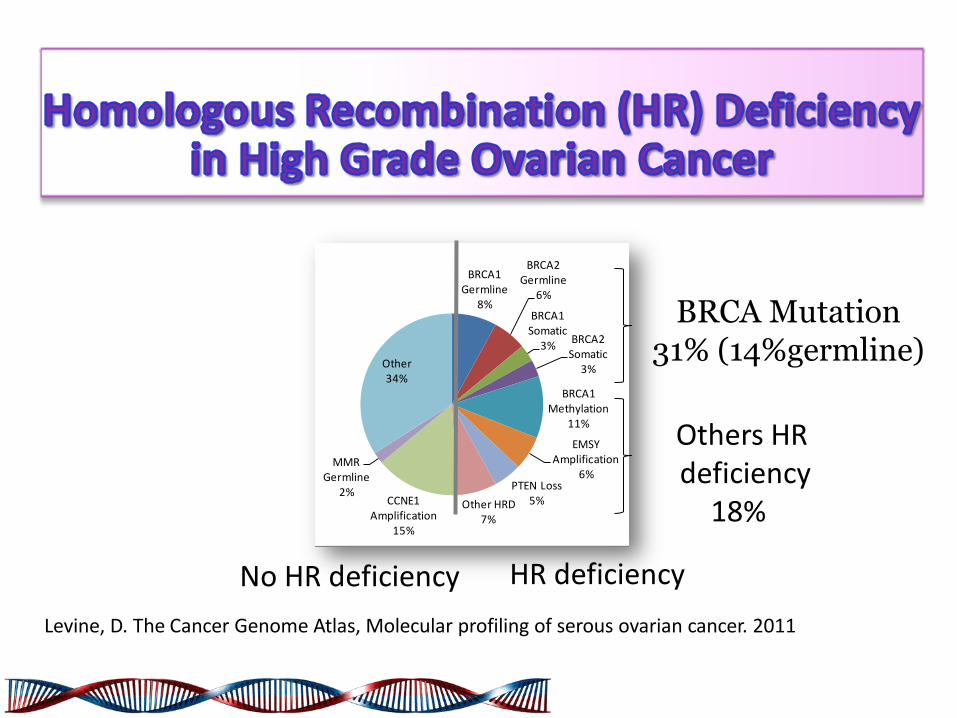
BRCA1 Germline
8%
BRCA2 Germline
6%
BRCA1 Somatic
3%BRCA2
Somatic3%
BRCA1 Methylation
11%
EMSY Amplification
6%PTEN Loss
5%Other HRD7%
CCNE1 Amplification
15%
MMR Germline
2%
Other 34%
HR deficiency No HR deficiency
Levine, D. The Cancer Genome Atlas, Molecular profiling of serous ovarian cancer. 2011
BRCA Mutation 31% (14%germline)
Others HR deficiency
18%

Gabai-Kapara E et al. ( 2014)
45 74 84
3% 50% 55%
45 74 84
1% 17% 65%

BRCA2
RAD51
DNA damaging RAD51 forms nucleoprotein filaments
RAD51 RAD51
RAD51
RAD51
RAD51
BRCA1
BRCA1 is a DNA damaging “detector”, blocks the transcription by cell cycle arrest at the G1/S, S and G2/M checkpoints and by ubiquitination of FANCD2
otherwise induces the DSB repair by chromatin remodelling
Chk2
ATM ATR
Toss & Cortesi, 2013
A
L
F
C
E
G
D2 Ub B
M
I

Santos-Pereira J. et al. Nat. Publ. Gr. (2015)

PARP
Inhibition of PARP-1 prevents recruitment of repair factors to repair SSB
XRCC1
LigIII
PNK 1
pol β
Replication (S-phase)
DNA DSB
DNA SSB
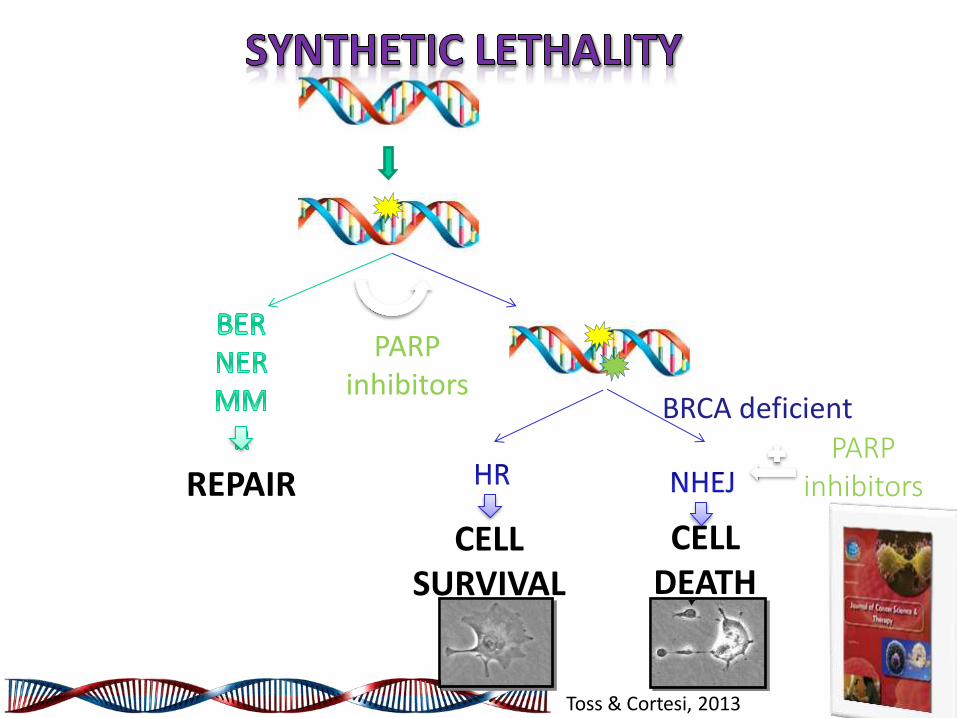
REPAIR
CELL SURVIVAL
CELL DEATH
BRCA deficient
PARP inhibitors
PARP inhibitors
Toss & Cortesi, 2013

Chemosensitivity/resistance
Tassone P. et al.; 2003:88; 1285-1291

N
N
O
N
O
N OF
IC50 on PARP-1 = 4.9 nM
IC50 on PARP-2 ≈ 5nM
IC50 on PARP-3 ≈ 50nM
IC50 on Tankyrase >1M
• Olaparib (AZD2281; KU-0059436) • Favorable PK • Good bioavailability across species • Tumor PK -Significant levels at 24 hrs following single oral dose
Menear et al. J Med Chem 2008
Olaparib: an Oral Inhibitor of Poly (ADP-ribose) Polymerase (PARP)

BRCA2 +/-
BRCA2 -/-
Wild type
Log surviving fraction
0 - 4
- 3
- 2
- 1
0
PARP inhibitor concentration (M)
10-9 10-8 10-7 10-6 10-5 10-4
Increased levels of chromosomal aberrations in PARP inhibitor
treated BRCA2 -/- cells
WT BRCA-/-
0
1
2
3
4
BRCA2-/-
+ PARPi WT
+ PARPi M
ean
nu
mb
er
of
ch
rom
ati
d
ab
err
ati
on
s p
er
cell
Chromatid
breaks
Complex
aberrations
Farmer et al. Nature 2005; 434:917-21
BRCA 1 & 2 -/- ES Cells are Very Sensitive to PARP Inhibition

Sono eleggibili al test BRCA tutte le pazienti con diagnosi di carcinoma epiteliale ovarico non mucinoso e non borderline, di carcinoma delle tube di Falloppio e di carcinoma peritoneale primitivo per completare la fase diagnostica molecolare in previsione di un eventuale utilizzo terapeutico e per favorire l’accesso ad una consulenza pre-test nell’ambito dei percorsi di prevenzione.

…Si sottolinea la necessità di definire percorsi aziendali in cui vengano indicate in modo chiaro per le pazienti ed i loro familiari, le funzioni e le responsabilità dell’equipe oncologica, del laboratorio e dell’equipe di genetica clinica oncologica nelle varie fasi del percorso individuato….
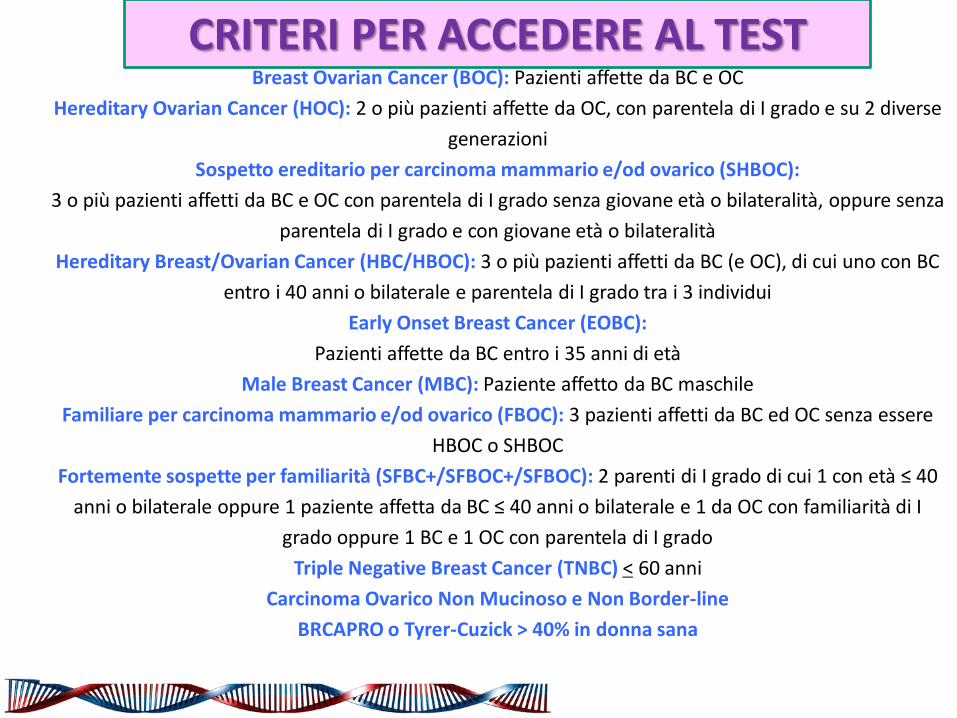
Breast Ovarian Cancer (BOC): Pazienti affette da BC e OC
Hereditary Ovarian Cancer (HOC): 2 o più pazienti affette da OC, con parentela di I grado e su 2 diverse
generazioni
Sospetto ereditario per carcinoma mammario e/od ovarico (SHBOC):
3 o più pazienti affetti da BC e OC con parentela di I grado senza giovane età o bilateralità, oppure senza
parentela di I grado e con giovane età o bilateralità
Hereditary Breast/Ovarian Cancer (HBC/HBOC): 3 o più pazienti affetti da BC (e OC), di cui uno con BC
entro i 40 anni o bilaterale e parentela di I grado tra i 3 individui
Early Onset Breast Cancer (EOBC):
Pazienti affette da BC entro i 35 anni di età
Male Breast Cancer (MBC): Paziente affetto da BC maschile
Familiare per carcinoma mammario e/od ovarico (FBOC): 3 pazienti affetti da BC ed OC senza essere
HBOC o SHBOC
Fortemente sospette per familiarità (SFBC+/SFBOC+/SFBOC): 2 parenti di I grado di cui 1 con età ≤ 40
anni o bilaterale oppure 1 paziente affetta da BC ≤ 40 anni o bilaterale e 1 da OC con familiarità di I
grado oppure 1 BC e 1 OC con parentela di I grado
Triple Negative Breast Cancer (TNBC) < 60 anni
Carcinoma Ovarico Non Mucinoso e Non Border-line
BRCAPRO o Tyrer-Cuzick > 40% in donna sana
CRITERI PER ACCEDERE AL TEST

Il test BRCA deve essere richiesto per la ricerca di varianti patogenetiche costituzionali e va valutata l’eventuale fattibilità del test BRCA somatico. Per un’adeguata esecuzione del test è necessaria per i laboratori una comprovata validazione ed un controllo di qualità esterno del test proposto

Mafficini A et al,. Oncotarget. 2016 Jan 12;7(2):1076-83
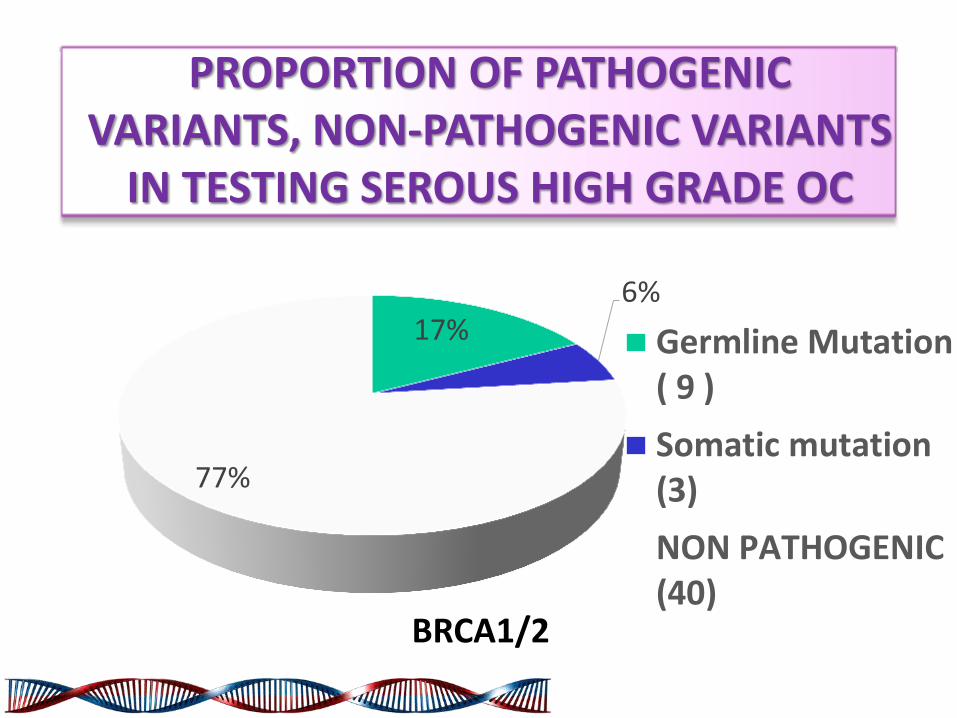
17% 6%
77%
Germline Mutation( 9 )
Somatic mutation(3)
NON PATHOGENIC(40)
PROPORTION OF PATHOGENIC VARIANTS, NON-PATHOGENIC VARIANTS
IN TESTING SEROUS HIGH GRADE OC
BRCA1/2

Stili di vita e prevenzione dei tumori

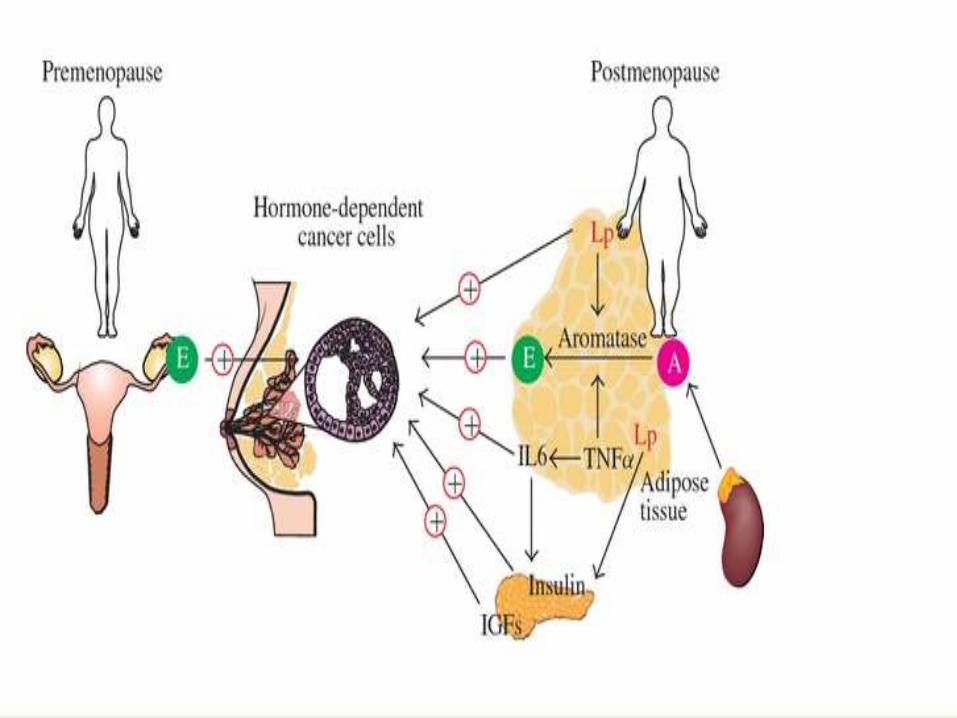
Biosintesi degli Estrogeni
20,22-Lyase
11b-Hydroxylase
18-Hydroxylase
17,20 Lyase
Pharmacological Target
Cholesterol
Pregnenolone
Progesterone
11-Deoxycorticosterone
Corticosterone
17a-Hydroxylase
21a-Hydroxylase
11-Deoxycortisol
Testosterone
Dehydroepiandrosterone
Androstenedione
Cortisol
Aldosterone
AROMATASI
Oestrone Oestradiol
(intermediate)
(intermediate)
17a- Hydroxypregnenolone
17a- Hydroxyprogesterone

Attività dell’ enzima aromatasi
ANDROGENS OESTROGENS
P-450 Aromatase + NADPH-cytochrome P-450 reductase
(Testosterone, androstenedione,
16-OH-testosterone)
(Oestradiol, oestrone)
tumour growth

Breast Cancer Tumorigenesis

Situazione nutrizionale – pool di Asl
2009-12 (n=149.823) Popolazione in eccesso ponderale
Sovrappeso* 31,4 %
Obeso** 10,5 %
Consigliato di perdere peso da un medico o operatore sanitario***
Sovrappeso 43,6%
Obesi 77,8 %
*sovrappeso = indice di massa corporea (Imc) compreso tra 25 e 29,9 **obeso = indice di massa corporea (Imc) ≥30 ***tra coloro che sono stati dal medico negli ultimi 12 mesi
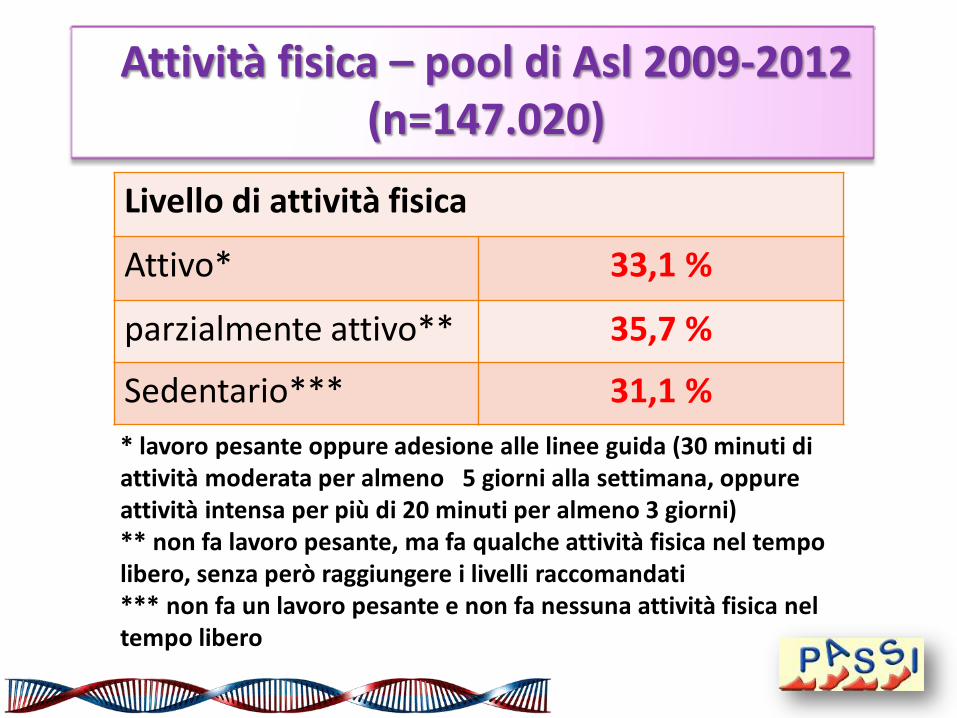
Attività fisica – pool di Asl 2009-2012 (n=147.020)
* lavoro pesante oppure adesione alle linee guida (30 minuti di attività moderata per almeno 5 giorni alla settimana, oppure attività intensa per più di 20 minuti per almeno 3 giorni) ** non fa lavoro pesante, ma fa qualche attività fisica nel tempo libero, senza però raggiungere i livelli raccomandati *** non fa un lavoro pesante e non fa nessuna attività fisica nel tempo libero
Livello di attività fisica
Attivo* 33,1 %
parzialmente attivo** 35,7 %
Sedentario*** 31,1 %
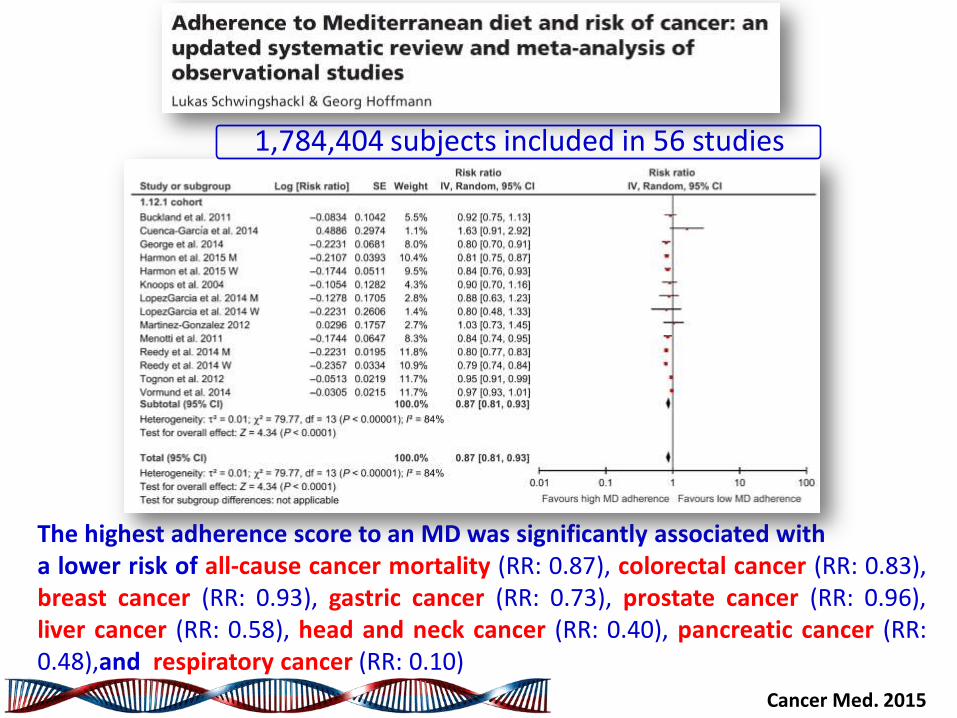
The highest adherence score to an MD was significantly associated with a lower risk of all-cause cancer mortality (RR: 0.87), colorectal cancer (RR: 0.83), breast cancer (RR: 0.93), gastric cancer (RR: 0.73), prostate cancer (RR: 0.96), liver cancer (RR: 0.58), head and neck cancer (RR: 0.40), pancreatic cancer (RR: 0.48),and respiratory cancer (RR: 0.10)
Cancer Med. 2015
1,784,404 subjects included in 56 studies

Toledo et al. JAMA Internal Medicine 2015
The multivariable-adjusted hazard ratios vs the control group were 0.32 (95%CI, 0.13-0.79) for the Mediterranean diet with extra-virgin olive oil group
and 0.59 (95% CI, 0.26-1.35) for the Mediterranean diet with nuts group
4282 women Follow up: 4,8 ys

Soy isoflavones consumption was inversely associated with risk of breast cancer incidence
(RR = 0.89, 95% CI: 0.79–0.99)
The protective effect of soy was only observed among studies conducted in Asian populations
(RR = 0.76, 95% CI: 0.65–0.86) but not in Western populations (RR = 0.97, 95% CI: 0.87–1.06)
Jia-Yi Dong • Li-Qiang Qin. Breast Cancer Res Treat (2011)

Soy intake consistent with a traditional Japanese diet (2-3 servings daily, containing 25-50 mg isoflavones) appears safe for breast
cancer survivors
While there is NO clear evidence of harm, better evidence confirming safety is required before use of high dose (≥ 100mg) isoflavones can
be recommended for breast cancer patients
MODERATE soy consumption appears to be safe and possibly beneficial for most women
Heidi Fritz. PLOS ONE. November 2013
Soy consumption may be associated with reduced risk of breast cancer incidence, recurrence, and mortality
Cancer 2017
a higher dietary intake of isoflavone was associated with reduced all-cause mortality
A 21% decrease was observed in all-cause mortality for women who had the highest versus lowest quartile of
dietary isoflavone intake (>1.5 vs<0.3mg daily: HR, 0.79; 95% CI, 0.64-0.97; Ptrend
5.01)
6235 women with BC F-up approx. 9.4 ys1224 deaths documented

WCRF / AICR. CUP: Diet, Nutrition, Physical Activity and Breast Cancer Survivors. 2014

Linee guida sulla nutrizione
e l’attività fisica per la prevenzione dei
tumori. American Cancer
Society
© 2012 American Cancer Society
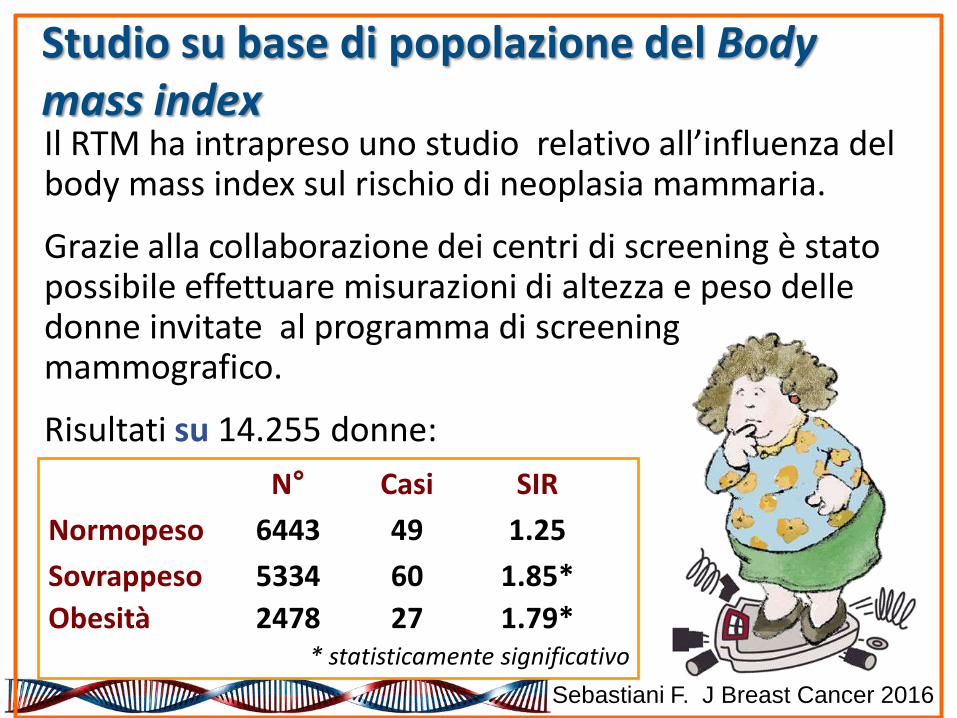
Studio su base di popolazione del Body mass index Il RTM ha intrapreso uno studio relativo all’influenza del body mass index sul rischio di neoplasia mammaria.
Grazie alla collaborazione dei centri di screening è stato possibile effettuare misurazioni di altezza e peso delle donne invitate al programma di screening mammografico.
Risultati su 14.255 donne:
N° Casi SIR
Normopeso 6443 49 1.25
Sovrappeso 5334 60 1.85*
Obesità 2478 27 1.79* * statisticamente significativo
Sebastiani F. J Breast Cancer 2016

Increased incidence and poor prognosis of breast cancer in postmenopausal women with high Body Mass Index
attending to the Mammography Screening Program in the province of Modena (Italy)
Normal weight
Overweight
Obesity
Normal weight Over weight Obesity
Sebastiani F. J Breast Cancer 2016
J Clin Oncol 2010
Obesity is an independent prognostic factor for developing distant metastases and for death as a result
of breast cancer
On a long-term basis, adjuvant therapy seemed to be less effective for patients with breast cancer and obesity.

After 10 years, both chemotherapy and endocrine therapy seemed
to be less effective in patients with BMIs of 30 kg/m2 or greater
HR for death (all causes) in relation to follow-up time, BMI, and adjuvant treatment
J Clin Oncol 2010
J Clin Oncol 2010
ATAC study: 9366 postmenopausal women with early-stage breast cancer randomly assigned to
oral daily anastrozole alone, tamoxifen alone, or the combination in a double-blind fashion

There is a significantly greater risk of recurrence in
overweight women receiving anastrozole
women with a high BMI at baseline had more recurrences than those women with a low BMI (adjusted HR, 1.39) and
significantly more distant recurrences (adjusted HR, 1.46)
Is estrogen suppression with anastrozole complete in obese women?
J Clin Oncol 2010
LISTA DEGLI INVESTIGATORI
Sperimentatore principale Massimo Federico¹ Co-sperimentatore di riferimento Federica Sebastiani¹ Co-sperimentatori e collaboratori Nino Battistini¹, Silvia Toni¹ ¹ Dipartimento di Medicina Diagnostica, Clinica e di Sanità Pubblica. Università di Modena e Reggio Emilia

Programma di educazione alimentare e al movimento rivolto alle donne operate per carcinoma della mammella Obiettivi: valutare l’ efficacia di un programma di educazione alimentare e al movimento su: parametri antropometrici (BMI, peso corporeo) Livello di attività fisica Miglioramento della qualità di vita
OBIETTIVI
Analisi attività ambulatoriale Gen 2010-Mag 2016
Variabili considerate
BODY MASS INDEX (Kg/m2)
ATTIVITÀ FISICA PROGRAMMATA (ore/settim)
ANALISI STATISTICA Anova per misure ripetute
Campione
N°donne sottoposte alla prima visita: 442
N°donne con un follow-up di 24 mesi: 442

* differenza statistica con p<0.05
Campione: donne (n=442) con un f-up mediano di 24 mesi
Analisi per strato di BMI
103
170 169
103
150
130
103
150
125
103
135
115
Normopeso Sovrappeso Obese
P=0.74 P<0.001*
P<0.001*
103 donne
170 donne
169 donne
BM
I (kg
/m2)
Base
6 M
12 M
24 M

0,00
0,50
1,00
1,50
2,00
2,50
3,00
3,50
BASELINE 6 MESI 12 MESI 24 MESI
* differenza statistica con p<0.05
ore
/se
ttim
P<0.001*
Attività fisica media
Campione: donne (n=442) con un f-up mediano di 24 mesi

Conclusioni
• L’analisi preliminare dei dati raccolti in 6 anni di
attività dimostra come una corretta alimentazione ed
un regolare esercizio fisico possono favorire una
significativa riduzione del peso corporeo
• Il controllo del peso e del livello di attività fisica
attraverso strategie di intervento sullo stile di vita
dovrebbe rappresentare parte integrante del follow
up delle pazienti con tumore della mammella

Costi sanitari pubblici
Trattamenti e cure
Prevenzione
Ogni investimento in prevenzione produce, nel corso degli anni successivi, un risparmio triplo in trattamenti e cure
Prof. Cascinu Stefano
Dr. Cortesi Laura
Dr. Toss Angela
Dr Spaggiari Federica
Dr. Razzaboni Elisabetta
Dr. Marchi Isabella
Dr. Medici Veronica
Dr. Venturelli Marta
Inf. Bevini Paola
Prof. Pietro Torricelli
Dr. Rachele Battista
Dr. Barbara Canossi
Dr. Annarita Pecchi
Dr. Dal Molin Chiara
Dr. Antonella Drago
Dr. Giovanni Grandi
Programmi di screening di popolazione
Gratuiti, ad invito
Indicazioni dell’Unione Europea e del Ministero della Salute
Donne fra i 45 ed i 74 anni
Mammografia annuale in due proiezioni dai 45 ai 50 anni poi biennale

Learning Objectives
• To distinguish between role of Genetics and Genomics in clinical practice
• Focus on Hereditary Breast Cancer Syndromes and Multi-Gene Panels
• To explain the clinical meaning of Moderate Gene Risk and VUS
• To identify the patients for whom the Oncotype DX assay has been clinically validated
• To identify the patients for whom the Mammaprint assay could spare the chemotherapy
• To describe the most frequent mutated genes in sub-type breast cancer and resistance mechanisms by NGS

Examples of Genetic and Genomic Tests Genetic Test • BRCA1 and BRCA2
• The genetic make up of patients is tested for BRCA1 and BRCA2 mutations. Patients with those mutations have higher chances of developing breast cancer.
Genomic Test
• Oncotype DX® Breast Cancer Assay • The expression level of 21 genes is measured in tumor tissue from patients that have already been diagnosed with breast cancer. This assay evaluates if a patient is going to recur (prognostic) and predicts benefit from chemotherapy and hormonal therapy (predictive)
• Mammaprint assay • Breast Cancer Index

Moderate Risk Genes
Cancer risks may not be very high
◦ How high does risk need to be before we pursue surgery or medications?
Cancer risks may be unclear
◦ How do we make medical decisions when we don’t know the risks?
We’re still learning
◦ The recommendations you get today may be different in 5 years
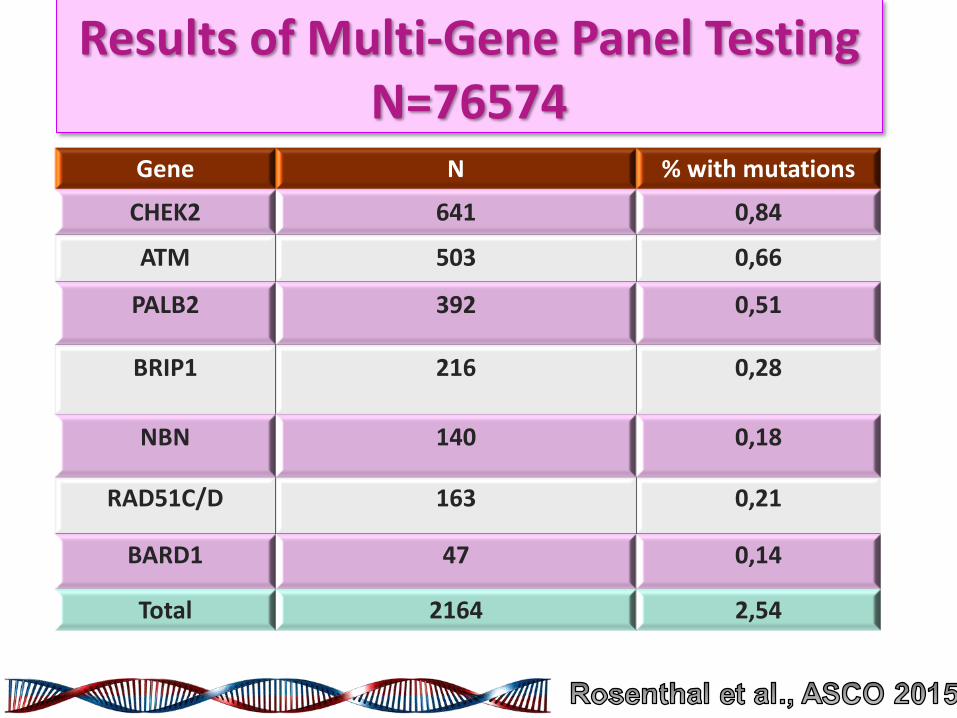
Results of Multi-Gene Panel Testing N=76574
Gene N % with mutations
CHEK2
641
0,84
ATM
503
0,66
PALB2
392
0,51
BRIP1
216
0,28
NBN
140
0,18
RAD51C/D 163 0,21
BARD1 47 0,14
Total 2164 2,54
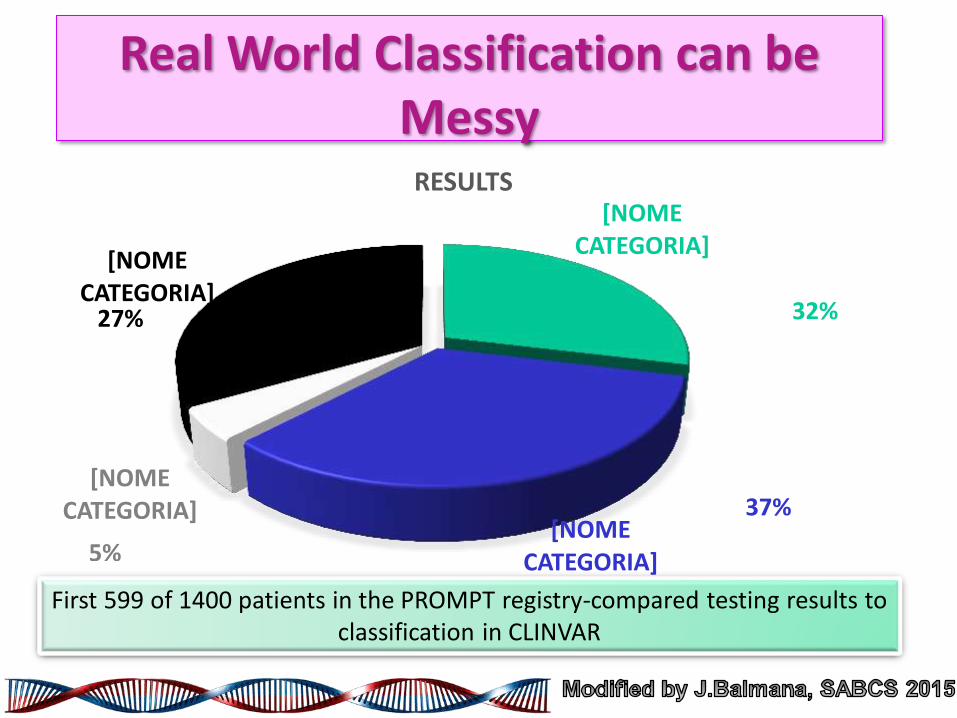
Real World Classification can be Messy
[NOME CATEGORIA]
[NOME CATEGORIA]
[NOME CATEGORIA]
[NOME CATEGORIA]
RESULTS
32%
37%
5%
27%
First 599 of 1400 patients in the PROMPT registry-compared testing results to classification in CLINVAR
Development of Functional Assays
• Most variants of uncertain significance have only been observed in a small number of families
• These VUS will not be readily classified by epidemiological approaches
• Functional assays offer a useful option for evaluating these VUS
• Must use assay associated with risk associated protein activity
• Sensitivity and specificity are required

Br: 33 49
47
Stomach: 54


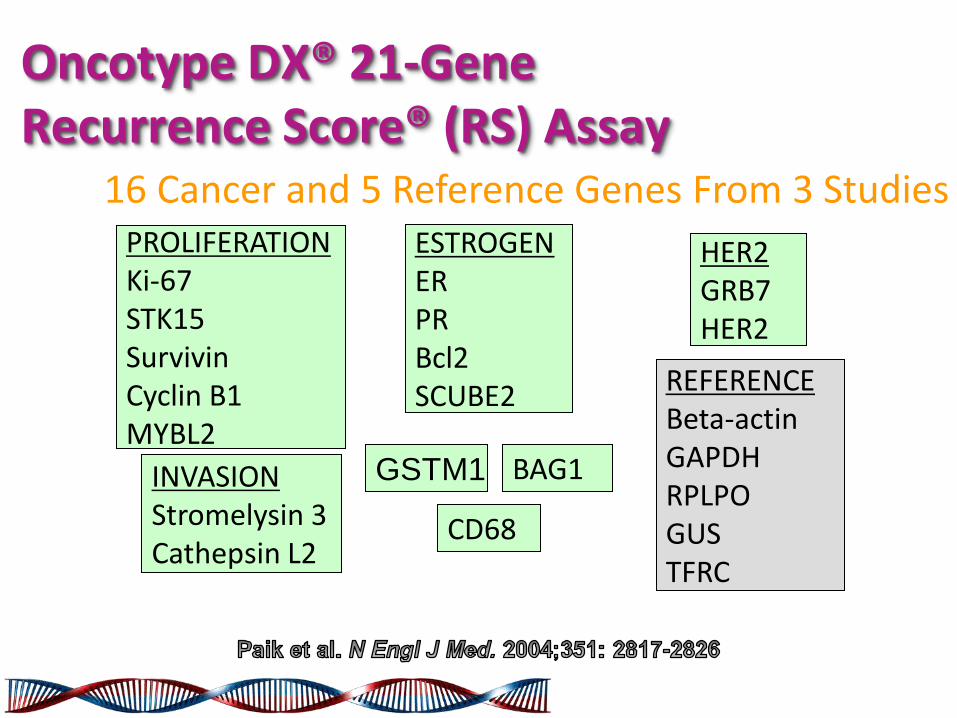
Oncotype DX® 21-Gene Recurrence Score® (RS) Assay
PROLIFERATION Ki-67 STK15 Survivin Cyclin B1 MYBL2
ESTROGEN ER PR Bcl2 SCUBE2
INVASION Stromelysin 3 Cathepsin L2
HER2 GRB7 HER2
BAG1 GSTM1
REFERENCE Beta-actin GAPDH RPLPO GUS TFRC
CD68
16 Cancer and 5 Reference Genes From 3 Studies

Oncotype DX® 21-Gene Recurrence Score® (RS) Assay
RS = Coefficient x Expression Level + 0.47 x HER2 Group Score - 0.34 x ER Group Score + 1.04 x Proliferation Group Score + 0.10 x Invasion Group Score + 0.05 x CD68 - 0.08 x GSTM1 - 0.07 x BAG1
Calculation of the Recurrence Score Result
Category RS (0-100)
Low risk RS <18
Int risk RS ≥18 and <31
High risk RS ≥31
The Trial Assigning Individualized Options for Treatment (TAILORx)
This trial was designed to further validate and refine the clinical usefulness of the 21-gene assay (Oncotype DX Recurrence Score, Genomic Health) in a specified low-risk cohort of women with hormone-receptor–positive, HER2-negative, axillary node–negative invasive breast cancer.

Node N-, ER+ Breast Cancer
RS <10 Hormone Therapy Registry
RS 11-25 Randomize
Hormone Rx vs
Chemotherapy + Hormone Rx
RS >25 Chemotherapy
+ Hormone Rx
Oncotype DX® Assay Register
Specimen banking
Primary study group
TAILORx Schema

Invasive Disease–free Survival
5-year event rate in cancers with recurrence scores 10 or less they did not receive chemotherapy
Freedom from Recurrence of Breast Cancer at Distant Site
Freedom from Recurrence at Any Site
Overall Survival

Among patients with hormone-receptor-positive, HER2-negative, axillary node-negative breast cancer who met established guidelines for the recommendation of adjuvant chemotherapy on the basis of clinicopathologic features, those with tumors that had a favorable gene-expression profile had very low rates of recurrence at 5 years with endocrine therapy alone.

The Winners are…
1.
2.
3.
4.
5.
N+ 2.86 0.004
T>2 1.55 0.003
GIII 1.43 0.005
HER21.56 0.001
ER 1.43 0.007
HR p

0.00
0.25
0.50
0.75
1.00
159 61 21 25/7378 195 75 73-4
1549 914 343 320/2Number at risk
2 5 8 10
0/2
3-4
5/7
A
0.00
0.25
0.50
0.75
1.00
88 42 8 25/7210 108 26 13-4675 372 113 80/2
Number at risk
2 5 8 10
0/2
3-4
5/7
B
Cu
mu
lativ
e r
ela
pse
pro
ba
bili
ty
Follow-up, years
Tumor size, node status, grading, HER2 and estrogen receptor status still retain a strong value in patients with operable breast cancer diagnosed in recent years
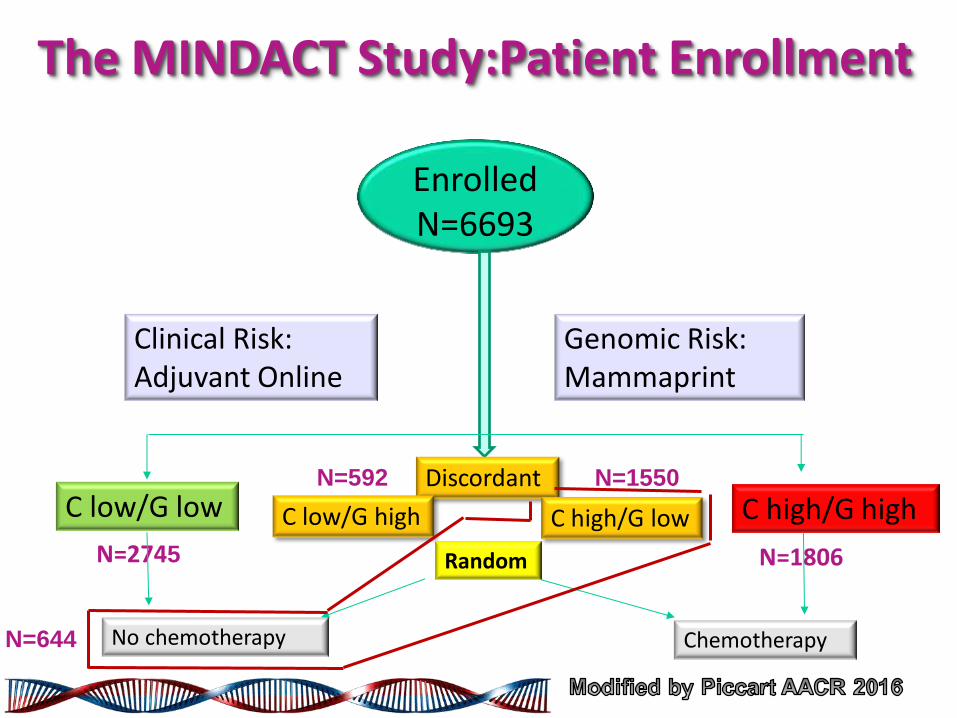
The MINDACT Study:Patient Enrollment
Enrolled N=6693
Clinical Risk: Adjuvant Online
Genomic Risk: Mammaprint
C low/G low
N=2745
Discordant N=592 N=1550
C low/G high C high/G low C high/G high
N=1806 Random
No chemotherapy Chemotherapy N=644

Clinical Outcome at 5-y Median Follow-up: Concordant Risk Group
cL/gL 97.6% (96.9-98.1)
cH/gH 90.6% (89.0-92.0)
92.8% (91.7-93.7)
85.3% (83.4-87.0)
98.4% (97.8-98.9)
94.7% (93.4-95.7)

The MINDACT Population: CT according Clinical or Genomic Strategy
Whole Population: N=6693
N=2745 cLow/gLow
N=1806 cHigh/gHigh
Discordant
N=592 cLow/gHigh
N=1550 cHigh/gLow
Clinical Strategy CT=1550+1806=3356
Genomic Strategy CT=592+1806=2398
14% CT reduction

• MINDACT study provide a level 1A of evidence of the clinical utility of Mammaprint for assessing the lack of CT benefit in cHigh Risk population
• cHigh/gLow patients have a 5-y DMFS rate of excess of 94% regardless CT
• In the whole population genomic strategy leads to a 14% CT reduction compared with clinical strategy
• Among the cHigh Risk patients the clinical use of Mammaprint is associated with a 46% CT reduction

HOXB13/IL17BR (H/I), is a prognostic biomarker in both untreated and tamoxifen-treated early-stage ER+ breast cancer patients.
Expression of H/I within primary tumors was determined by reverse-transcription polymerase chain reaction with a prespecified cutpoint. The predictive ability of H/I for
ascertaining benefit from letrozole was determined using multivariable conditional logistic regression including standard clinicopathological factors as covariates.

• Patients with High H/I had a 5yr absolute benefit of 16.5% from extended endocrine therapy with Letrozole (p=0.007)
• Patients with Low H/I had no significant benefit from extended endocrine therapy with Letrozole (p=0.35)
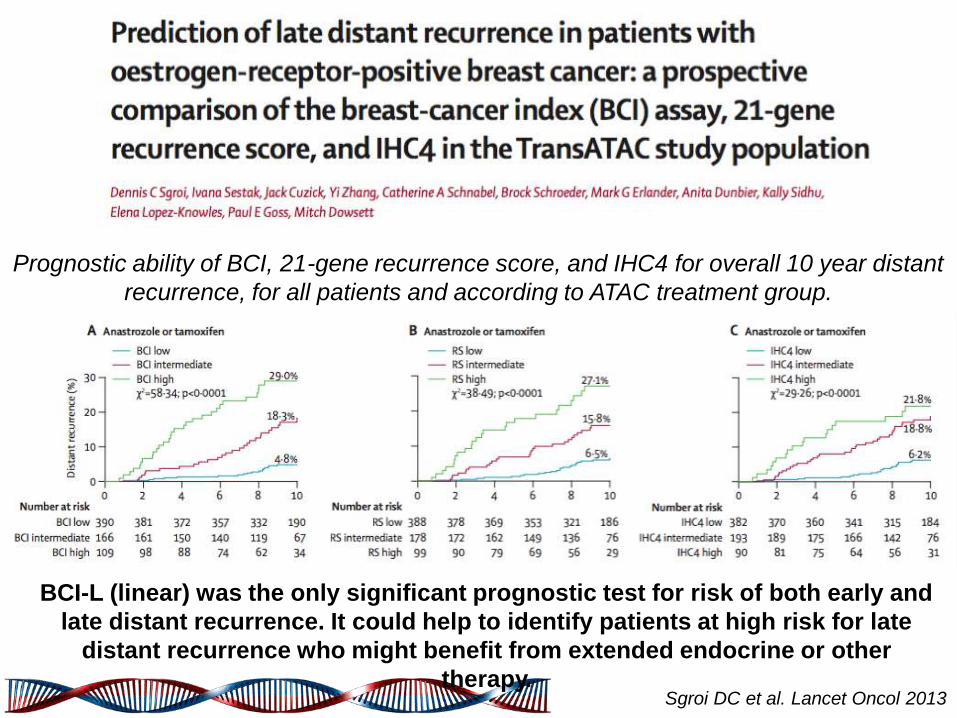
Prognostic ability of BCI, 21-gene recurrence score, and IHC4 for overall 10 year distant
recurrence, for all patients and according to ATAC treatment group.
BCI-L (linear) was the only significant prognostic test for risk of both early and
late distant recurrence. It could help to identify patients at high risk for late
distant recurrence who might benefit from extended endocrine or other
therapy. Sgroi DC et al. Lancet Oncol 2013
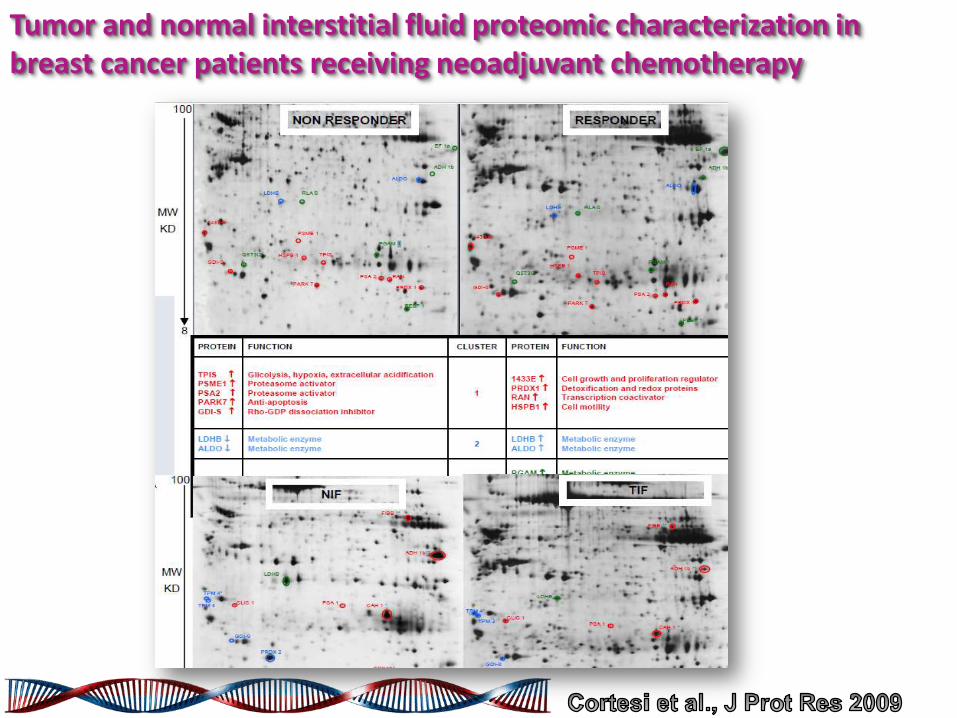
Tumor and normal interstitial fluid proteomic characterization in breast cancer patients receiving neoadjuvant chemotherapy

NGS meta-analysis: most frequently mutated genes in each molecular subtype
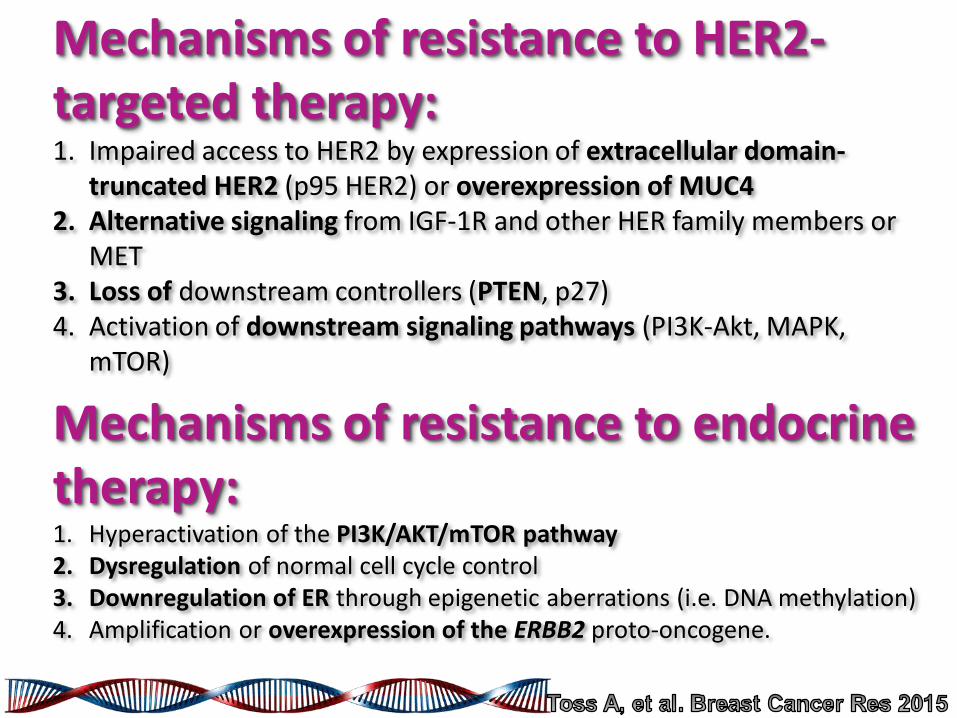
Mechanisms of resistance to HER2-targeted therapy: 1. Impaired access to HER2 by expression of extracellular domain-
truncated HER2 (p95 HER2) or overexpression of MUC4 2. Alternative signaling from IGF-1R and other HER family members or
MET 3. Loss of downstream controllers (PTEN, p27) 4. Activation of downstream signaling pathways (PI3K-Akt, MAPK,
mTOR)
Mechanisms of resistance to endocrine therapy: 1. Hyperactivation of the PI3K/AKT/mTOR pathway 2. Dysregulation of normal cell cycle control 3. Downregulation of ER through epigenetic aberrations (i.e. DNA methylation) 4. Amplification or overexpression of the ERBB2 proto-oncogene.
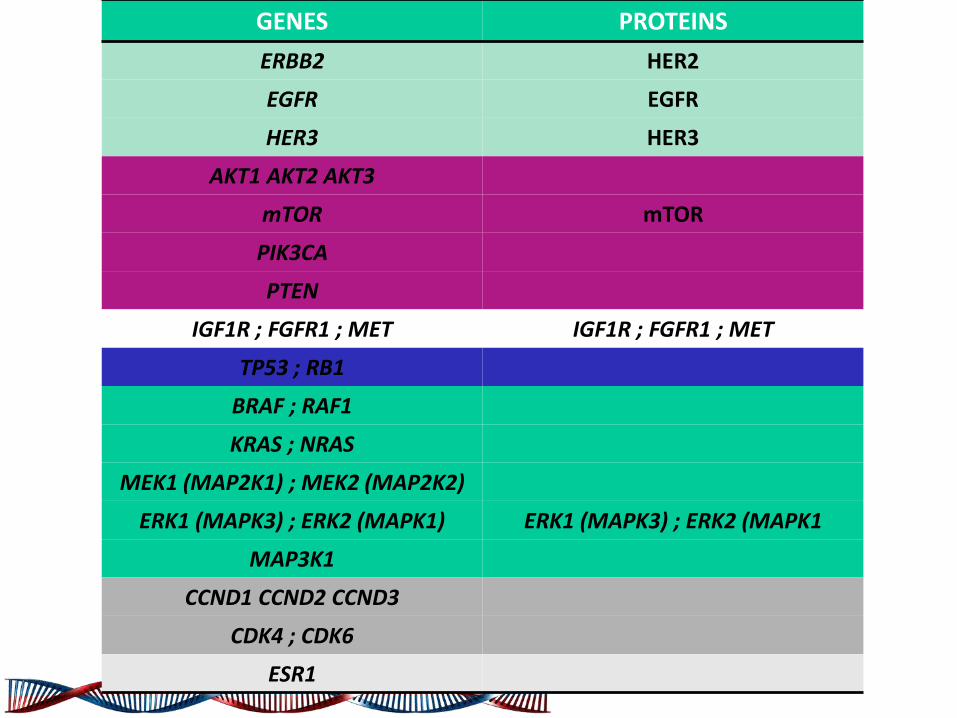
GENES PROTEINS
ERBB2 HER2
EGFR EGFR
HER3 HER3
AKT1 AKT2 AKT3
mTOR mTOR
PIK3CA
PTEN
IGF1R ; FGFR1 ; MET IGF1R ; FGFR1 ; MET
TP53 ; RB1
BRAF ; RAF1
KRAS ; NRAS
MEK1 (MAP2K1) ; MEK2 (MAP2K2)
ERK1 (MAPK3) ; ERK2 (MAPK1) ERK1 (MAPK3) ; ERK2 (MAPK1
MAP3K1
CCND1 CCND2 CCND3
CDK4 ; CDK6
ESR1






![Genetica Medica 6ed - Thompson & Thompson[1] - …lghm.ufpa.br/ppgbm/site/material_conteudo_programatico_3.pdf · Title: Genetica_Medica_6ed_-_Thompson_&_Thompson[1].pdf Author: Mara](https://img.pdfslide.us/doc/110x75/5ba9bad709d3f28b6f8cc1f1/genetica-medica-6ed-thompson-thompson1-lghmufpabrppgbmsitematerialconteudoprogramatico3pdf.jpg)