Embed Size (px)
Citation preview
Novice to Expert A professional development model
for core team members
Presented by:
Gentiva Health Services Hospice Division
Lori H. Thompson, SPHR Director, Human Resources
David A. Eubanks, MSN, RN AVP, Clinical Development
Sally Parnell, MSN, RN DVP, Hospice
Charlotte Weaver, Ph.D, RN, FAAN Chief Clinical Officer

Learner Objectives
The Learner will: • Identify key concepts and components in the development of a clinical ladder program. • Be able to discuss the eligibility criteria for participating in the clinical ladder program. • Be able to describe the structure and process for application to the clinical ladder. • Be able to identify the criteria used for selection of a professional into the ladder and the reward and recognition associated with each level in the ladder.
Literature Review of Clinical Ladder
Retaining experienced nurses who provide direct clinical care is vital to improving quality care. (Benner 1982) To maintain a higher percentage of experienced nurses at the bedside nurse leaders must identify ways to increase nursing satisfaction. (Riley et al 2009) Only 32.2% of nurses surveyed felt they had opportunities for advancement at the clinical level. (Aiken 2001) A clinical advancement package is essential for recognizing excellence in clinical practice. The clinical ladder was developed to recognize the RN decisions to remain at the bedside and concentrate on expertise in clinical practice. (Zimmer 1972)

Literature Review of Clinical Ladder
Clinical ladder programs (CLP’s) are designed to reward nurses for specific criteria, such as education, research, clinical and leadership skills. (Riley et al 2009) Positive outcomes from clinical ladder programs are improvement of staff satisfaction, patient satisfaction, physician satisfaction, professional development, quantity of expert nurses, and healthcare expenditures.(Drenkard and Swartwout 2005) The literature reveals that the use of clinical ladders results in decreased cost, decreased use of nursing sick time, decreased turnover, and decreased use of agency nurses, as well as higher staff nurse satisfaction. (Drenkard and Swartwout 2005)
Clinical Ladder - Overview
• Intent of program is to provide a career path for direct care clinicians
• Created by team of clinical managers and clinicians in 2009 under direction of the Corporate Chief Clinical Officer
• Designed with Levels 1-6- with Level 6 being on par with a VP level salary
• Applications for Levels 1-3 are finalized; Levels 4-6 are in development
Founding Principals
• Promote highest standard of clinical practice
• Provide recognition/rewards/incentives
• Provide an alternative career path
Alternative to advancement only through management
• Promote loyalty and retention
• Encourage continued education (CE credits, advanced degrees, credentialing/certification)
• Promote active participation in Branch, Region or specialty area
Structure and Process
• National Advisory Board – comprised of divisional and regional leaders to promote the program and to provide guidance and oversight.
• Regional Clinical Council – promote clinical ladder program and review and approve applications twice yearly. Members serve a 3-4 year term.
Regional Clinical Council
• Co-Chairs – Regional Vice President of Clinical Operations and Regional Human Resources Leader
• Clinical Managers
• Quality Managers
• Clinical Educators
• Operational Leaders
Eligibility Requirements
• Be employed 30 hours or more per week, as a clinical associate working in a direct care capacity
• Have completed at least one full year of employment by the month the application is due
• Have a current performance evaluation rating of “meet expectations” or above on each performance standard for the last review period
• Meet company standards for case load and documentation requirements
• Not be currently involved in a disciplinary process
Reward and Recognition
• Certificate signed by company Chief Executive Officer
• Choice of Gift
• Recognition Plague
• Name Badge Designation
• Bonus – builds with each level advancement
Clinical Ladder Stats Summary
• Home Health Program began in 2009
– 583 applicants
– 384 recipients
• Therapists (%) outnumber nurses (70/30)
• Regional differences exist in number of applicants
• 3 yr retention rate of ~88% for CLP recipients staying with the company.
Home Health Division
Hospice Division Pilot
• SE Region team developed and tested extension of Clinical Ladder Program
• Started February 2012 and developed criteria for Levels I, II and III
• Included 7 roles
• September application cycle
Disciplines Eligible - Hospice Ladder
• Registered Nurse
– Admission
– RN Case Manager
– IPU RN
– On-call RN
• Medical Social Worker
• Spiritual Care Coordinator/Chaplain
• Bereavement Coordinator
Hospice Clinical Ladder Program
Level 3
Level 2
Level 1
Each Level builds upon the Criteria/Eligibility of the previous Level.
Example: A Registered Nurse must have BSN to be eligible for Level 3.
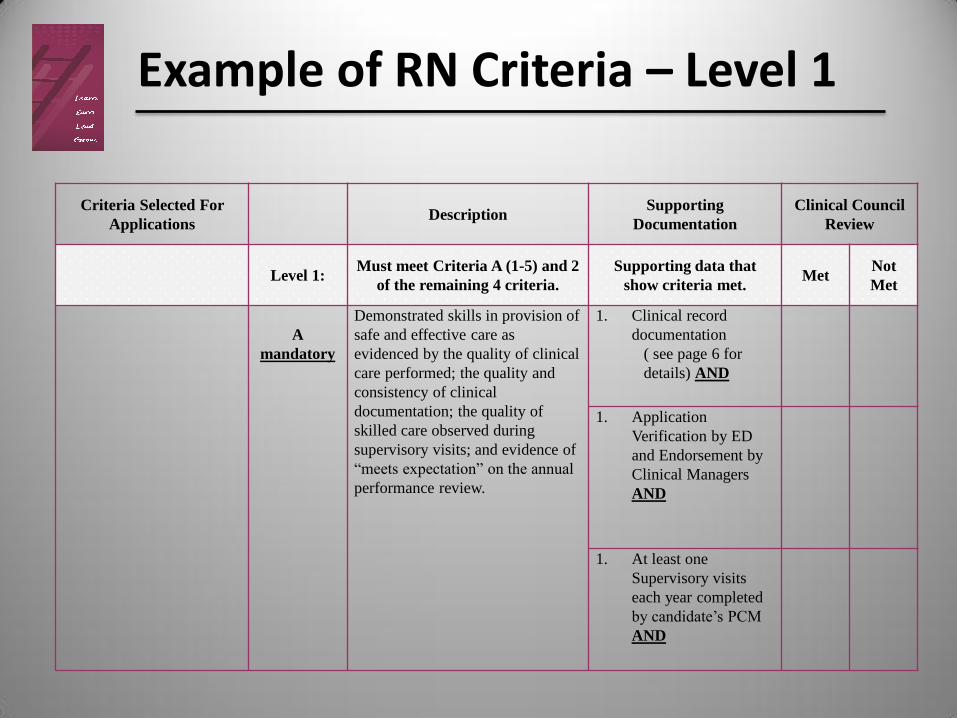
Criteria Selected For
Applications Description
Supporting
Documentation
Clinical Council
Review
Level 1: Must meet Criteria A (1-5) and 2
of the remaining 4 criteria.
Supporting data that
show criteria met. Met
Not
Met
A
mandatory
Demonstrated skills in provision of
safe and effective care as
evidenced by the quality of clinical
care performed; the quality and
consistency of clinical
documentation; the quality of
skilled care observed during
supervisory visits; and evidence of
“meets expectation” on the annual
performance review.
1. Clinical record
documentation
( see page 6 for
details) AND
1. Application
Verification by ED
and Endorsement by
Clinical Managers
AND
1. At least one
Supervisory visits
each year completed
by candidate’s PCM
AND
Example of RN Criteria – Level 1
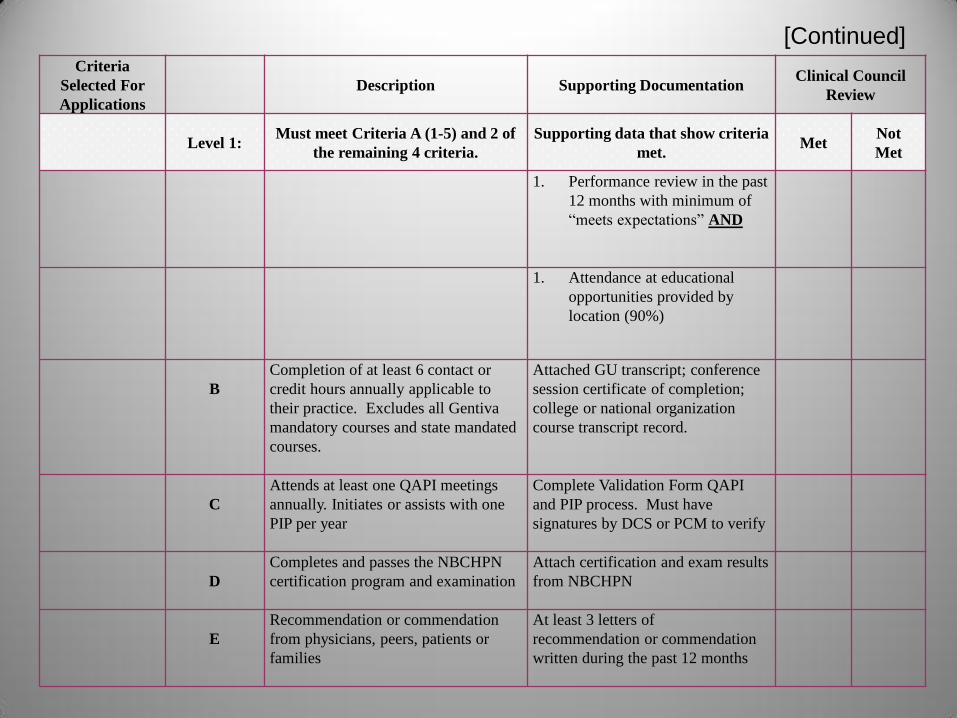
Criteria
Selected For
Applications
Description Supporting Documentation Clinical Council
Review
Level 1: Must meet Criteria A (1-5) and 2 of
the remaining 4 criteria.
Supporting data that show criteria
met. Met
Not
Met
1. Performance review in the past
12 months with minimum of
“meets expectations” AND
1. Attendance at educational
opportunities provided by
location (90%)
B
Completion of at least 6 contact or
credit hours annually applicable to
their practice. Excludes all Gentiva
mandatory courses and state mandated
courses.
Attached GU transcript; conference
session certificate of completion;
college or national organization
course transcript record.
C
Attends at least one QAPI meetings
annually. Initiates or assists with one
PIP per year
Complete Validation Form QAPI
and PIP process. Must have
signatures by DCS or PCM to verify
D
Completes and passes the NBCHPN
certification program and examination
Attach certification and exam results
from NBCHPN
E
Recommendation or commendation
from physicians, peers, patients or
families
At least 3 letters of
recommendation or commendation
written during the past 12 months
[Continued]
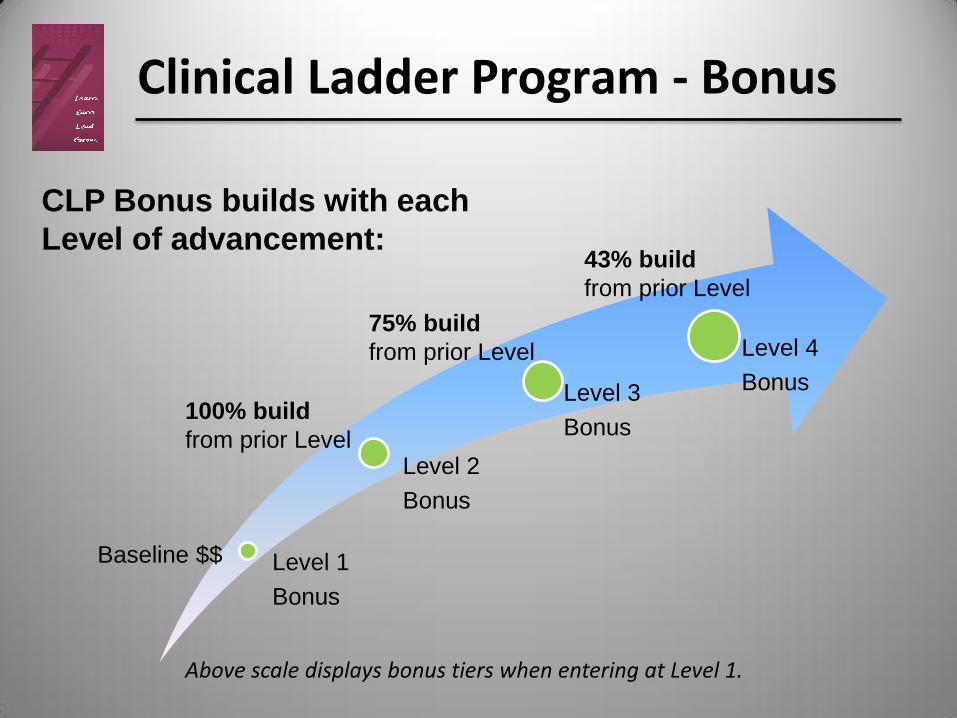
Clinical Ladder Program - Bonus
Level 1
Bonus
Level 2
Bonus
Level 3
Bonus
Level 4
Bonus
CLP Bonus builds with each
Level of advancement:
Baseline $$
100% build
from prior Level
75% build
from prior Level
43% build
from prior Level
Above scale displays bonus tiers when entering at Level 1.
Hospice Clinical Ladder Program
Example: • RN making $28.00/hour
• Accepted into the Clinical Ladder Program Level 1
• CLP Bonus would be paid out every pay period for the following 3 years
• In this example, the CLP Bonus would be a 6.7% increase for the RN
Special Incentive
RN to BSN Tuition Reimbursement Offering:
100% reimbursement for an on-line, in-state tuition from a public university program and would carry a required B grade average and an employment commitment of three years post-program completion. To be eligible for this special incentive a clinician must:
• Be accepted into the Ladder at Level 1 or 2 • Continue to remain in the Ladder during the course of the BSN program • Maintain a “meets expectations” performance review rating throughout the duration of their program • Continue to work as a full-time employee • Agree to continue employment with the company for three years after degree completion
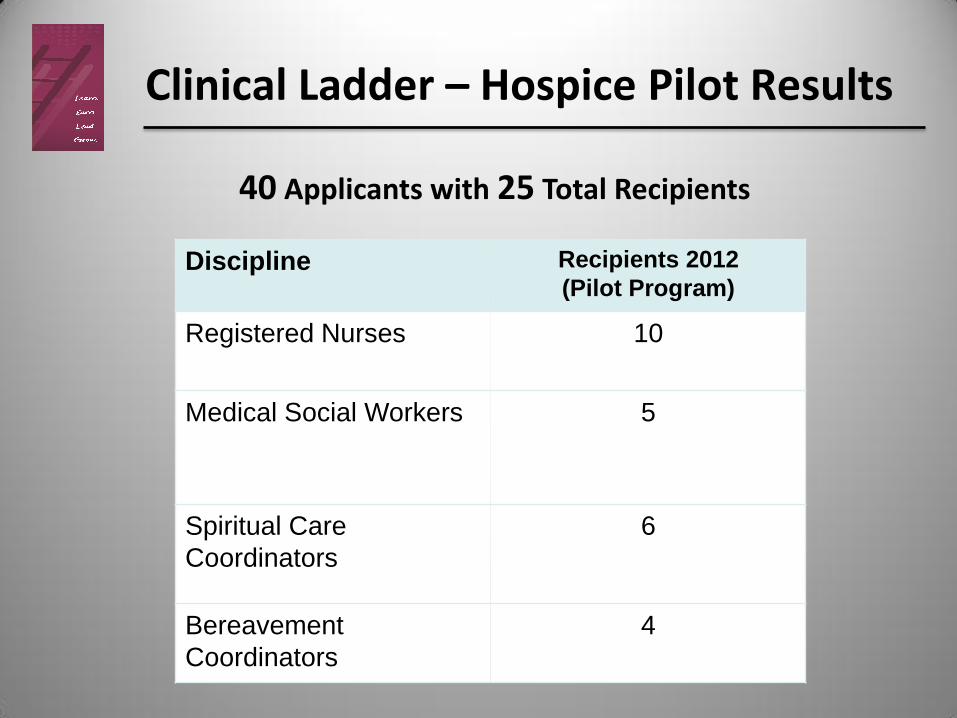
Clinical Ladder – Hospice Pilot Results
Discipline Recipients 2012
(Pilot Program)
Registered Nurses
10
Medical Social Workers
5
Spiritual Care
Coordinators
6
Bereavement
Coordinators
4
40 Applicants with 25 Total Recipients

Applicant Notification
Value Added Feedback for each applicant: • Timely feedback following council review
• Notification Call with the following: council co-chairs, assigned application reviewers, CLP program director, and direct supervisor present with applicant during the call
• Thorough and specific reasons provided for acceptance or deferment
• Collaborative discussion with each applicant
Application Review Cycle
• Semi-annual application cycle for 2013 March 15th and September 13th
• An applicant may enter the Ladder at any level that he/she qualifies for
• Once admitted to a Clinical Ladder level, that level status is
in effect for three years. At the end of the 3-year period, the clinician has three choices: Reapply to stay in the Clinical Ladder at the same Level Apply for advancement to the next Level or above Opt not to reapply and leave the Clinical Ladder
22
Conditions for Losing CLP Status
A CLP recipient may lose status and/or stipend if:
• Promotion to a manager level position
• Change in status from full time to per diem (less than 30 hours)
• Disciplinary action
• Medical or family leave of absence (temporary suspension of
bonus payments; reinstatement upon return to work)
23

The Documentation Challenge
Clinical record must demonstrate: • Safe and effective care meeting regulatory standards
• Skilled care pertinent to your discipline
• Medical necessity
• Interventions and treatments and patient response to both
• Specific goal statements and progress towards goals
24
The Documentation Challenge
Common reasons for deferment:
• Inadequate/incomplete care planning
• Failure to follow the plan of care (visit frequency)
• Inadequate documentation of reason/criteria for change in level of care
• “Scanty” notes (visit notes, IDG notes)
• Failure to document communication and coordination with other disciplines
25
Hospice Division-Wide Rollout
• Southeast Regional Council met after the pilot to determine program modifications needed prior to Division-wide rollout
• Implemented changes after discussion/approval from Advisory Board
• Trained each Region VP, Clinical Affairs and HR Leader on process to begin their Region Councils
• Division-wide Rollout January 1, 2013
References
• Aiken, LH, Clark SP, Sloane DM, et al. Nurses’ report on hospital care in five countries. Health Affairs. 2001; 20(3): 43-53.
• Benner P. From novice to expert: the Dreyfus model of skill acquisition. American Journal of Nursing. 1982; 82(3):402-407.
• Benner P. From Novice to Expert: Excellence and Power in Clinical Nursing Practice. Menlo Park, CA; Addison-Wesley; 1984
• Drenkard K. and Swartwout, E. Effectiveness of a clinical ladder program. Journal of Nursing Administration 2005; 35(11) 502-506
• Zimmer M. J. Rationale for a ladder for clinical advancement in nursing. Journal of Nursing Administration 1972; 2(6) 18-24
• Riley, J. K., Rolband, D. H., James, D. and Norton, H. J. Clinical ladder: Nurses Perceptions and Satisfiers 2009; 39(4): 182-188.
Thank you!
![The Journey from Novice to Expert - Infection control1]Barbara [Compatibility... · The Journey from Novice to Expert ... • To Discuss the Benner Model of Novice to ... • Published](https://img.pdfslide.us/doc/110x75/5acfaaac7f8b9ac1478d13cb/the-journey-from-novice-to-expert-infection-1barbara-compatibilitythe-journey.jpg)




























