Embed Size (px)
Citation preview

11/4/2006
WORK AND TALK:
INFORMATION PROVISION BY INFORMAL CONSULTING IN MEDICAL CLINICS *
DOUGLAS R. WHOLEY, PH.D†,‡
AMY R. WILSON, PH.D.†
WILLIAM RILEY , PH.D.†
DAVID KNOKE, PH.D§
November 4, 2006
* We thank Ward Godsall, David Yauch, John Schousboe, and Leif Solberg for their assistance and comments. We thank Jim Moody for assistance in using SPAN. Earlier versions of this paper were presented at the 6th Annual Health Care Organizations Conference at Boston University in June 2004, the Social Networks Seminar at the University of Minnesota, the National Primary Care Research and Development Centre at the University of Manchester, England, and the Department of Health Management and Policy at Harvard University. We thank the participants at these presentations and Tim Hoff, in particular, for valuable suggestions. We thank the University of Minnesota for its funding support.
† Division of Health Policy and Management, School of Public Health, University of Minnesota, MMC 729, 420 Delaware Street SE, Minneapolis, MN, 55455.
‡ Wholey contact information: Phone 612) 626-4682, Fax – 612-624-2196, Email; [email protected]
§ Department of Sociology, University of Minnesota, 939 Social Sciences, 267 19th Ave S, Minneapolis, MN 55455.

Work and Talk
1
WORK AND TALK:
INFORMATION PROVISION BY INFORMAL CONSULTING IN MEDICAL CLINICS
ABSTRACT
This paper examines the effect of work relationships on informal consulting within medical
clinics. A retrospective survey was used to measure individual characteristics and relationships
among all members of four clinics. Descriptive analyses describe informal consulting within
each clinic and multivariate analyses analyze the effect of work organization on informal
consulting in dyads. The analyses show that dyadic work relations, such as working with or
referring patients to others, and being members of the same work group increase information
sharing. Within work groups information sharing increases as density and occupational
heterogeneity increase. Information sharing tends to occur within similar professions (nurses
with nurses, physicians with physicians) and inter-occupational bridging occurs between
professionals central within their professional groups.
Key Words: Informal consulting, information sharing, knowledge management, opinion leaders,
medical clinics, professions.

Work and Talk
2
WORK AND TALK:
INFORMATION PROVISION BY INFORMAL CONSULTING IN MEDICAL CLINICS
How do work relationships affect informal consulting relations? Information sharing
within groups and teams is an important component of organizational performance. Information
sharing is particularly important in health care where information about patients, professional
knowledge, diagnostic tests, and many other pieces of information have to be blended. Because
of the diversity of information sources, the ambiguity of some types of information (e.g.,
symptoms), and variation in expertise within and between professions, managing information in
health care is a complex problem. One possible approach to managing these information needs
is formal tools such as medical records, both paper and electronic. But, encoding information
often leaves gaps. For example, a nurse entering patient information in a medical record may
not encode all the information a physician feels is relevant. This may occur because the nurse
has insufficient time or does not realize the relevance of a piece of information. Furthermore,
formal information gathering processes, such as patient referral to specialists, can be costly.
Talking with colleagues informally can resolve ambiguities quickly and provide reassurance,
resulting in improved quality of care and lower costs.
Informal consulting is a form of information sharing in organizations. This paper
contributes to this literature by showing how work-with relationships, patient referral
relationships, and structurally equivalent work groups pattern informal consulting within medical
clinics. In developing our arguments, we extend deductive analyses of information sharing by
building on inductive case studies of information sharing.
The information sharing literature can be broadly grouped into deductive and inductive
approaches. Bunderson describes three major deductive approaches, transactive memory,
distributed knowledge, expert influence, and develops an argument for a fourth, status
Work and Talk
2
characteristics (Bunderson 2003). Research in social networks provides a fifth approach. The
transactive memory approach shows that shared knowledge of who knows what and who can
do what within a group improves group performance (Austin 2003; Moreland and Myaskovsky
2000; Wegner et al. 1991). One source of shared knowledge is common training (Moreland and
Myaskovsky 2000). Distributed knowledge research suggests that explicit cues about who
knows what help groups integrate information from different sources (Stasser et al. 2000). The
expert influence argument is similar to an opinion leader argument, focusing on understanding
who is identified as an opinion leader and the effect of opinion leaders on integrating diverse
information. The status characteristics approach argues that status markers help individuals
recognize experts (Bunderson 2003). Status markers are either specific markers of an
individual‘s task-relevant expertise or diffuse general categories, such as gender and ethnicity.
Both specific and diffuse markers affect whether an individual is perceived as expert, with
specific markers having a larger effect in long-tenured, decentralized teams and diffuse markers
having a greater effect in lower-tenured, centralized teams (Bunderson 2003, 578). Groups with
specific status markers and influence alignment perform better. The social network knowledge
approach argues that information sharing is a function of knowing what others know, believing
what the other knows is useful and knowing the information is accessible quickly with low cost
(Borgatti and Cross 2003). The status characteristics and social networks approaches elaborate
the transactive memory, distributed knowledge, and expert influence approaches by seeking to
understand how information sharing is influenced by shared knowledge about the
characteristics of others.
A difficulty with the deductive approach is that it is not clear from where the transactive
memory, the explicit cues for distributed knowledge, the knowledge of expertise, the knowledge
of status, and knowledge of social networks comes. While teams can be trained in experimental
settings, in many medical clinics and professional settings teams and work groups are often

Work and Talk
3
amorphous, difficult to identify, and less likely to be accurately reflected in formal organizational
descriptions. Research suggests that even in a fairly well defined team environment, software
engineering, participants do not consistently agree on team membership (Mortensen 2004;
Mortensen and Hinds 2002). If it is difficult for teams to identify other team members and if
teams have ambiguous boundaries, from where does shared knowledge of who does what,
status, and social networks come? We propose that this knowledge flows from work
relationships, from the activities and relationships in which individuals engage to accomplish an
organization’s tasks.
The importance of work relationships as a cause of informal information sharing is well
established in the inductive approach to study information sharing. Blau examined information
sharing among agents who audited employers to determine compliance with federal laws (Blau
1963 (1955), Chapters 7, 8). Information sharing among agents had to be informal because it
was proscribed by formal rules. Blau found that proximity was a cause of asking for information.
Information requests for solving difficult problems were addressed to more expert agents, who
gained status as a consequence of providing help.1 While Blau showed how accomplishing work
is a key cause of information sharing, it is difficult to generalize his findings to work settings with
interdependent actors. In Blau’s study, agents were doing similar tasks in a situation of pooled
interdependence. Barley extended Blau’s work by examining how the introduction of new
scanning technologies affected roles and information sharing between technicians and
physicians (Barley 1986). The new technology provided a trigger for rearranging work activities
and information sharing practices. In early learning phases, these rearrangements were
idiosyncratic to small teams of technicians and physicians. Eventually arrangements evolved to
support the larger clinical environment and there was some convergence between the clinics. A
Work and Talk
4
key point is that role and information sharing arrangements emerged out of the necessity of
accomplishing the tasks at hand – namely scanning. Similarly, Barley studied the role of
technicians in work settings (Barley 1996). He found that technician roles took one of two work-
related forms, either brokering between patients and others or brokering between technology
and others. Bechky examined information sharing among three occupational communities at a
semiconductor firm (Bechky 2003). Engineers designed a product that was handed off to
technicians to make a prototype which assembly personnel used to develop a manufacturing
process. Because design, prototyping, and assembly were done by different groups, each had a
distinct occupational community. She found that information sharing was facilitated by
occupational communities coming to understand problems from each others’ perspective – by
“co-creating common ground.” Reddy and Dourish examined information sharing in Surgical
Intensive Care Units (SICUs) (Reddy and Dourish 2002) . Providers in the SICU must determine
when a patient recovering from an operation is stable enough to be transferred from the SICU to
the hospital. This transfer is necessary to open beds for patients who are completing their
operations. This decision requires integrating clinical information about a patient’s stability and
institutional information about bed availability. Reddy and Dourish argue that information
sharing, and decision-making, are temporally triggered by work-related rhythms, such as
medical rounds and the return of lab tests. For Reddy and Dourish, work rhythms create
common ground.
A broad, and very important, generalization from the inductive research is that
information sharing is rooted in accomplishing tasks, in getting work done. This is consistent
with the argument that organizations are goal-oriented systems, seeking to accomplish tasks
1 Blau’s causal order appears to differ from Bunderson’s, with Blau arguing that information provision increases specific status (“The consultant gains prestige” (Blau 1963 (1955), 130))while Bunderson argues that specific status increases information sharing.
Work and Talk
5
(Aldrich and Ruef 2006). A second broad generalization from the inductive approach is that
both emergent and formal work organization affects information sharing.
While the deductive and inductive approaches complement each other, it can be difficult
to synthesize their findings. When reading research taking the deductive approach, one may
conclude that research subjects have nothing to do other than seek information. Information
sharing is “inseparable from the work that it supports and generates. Information is not a
separate focus of concern, but is woven seamlessly into the work of the unit” (Reddy and
Dourish 2002, 347); thus, not accounting for work, either theoretically or as a control, may
result in biased or spurious estimates.
With the exception of the social networks approach, which determines emergent
information sharing subgroups within an organization, the deductive approaches take groups
and teams as given with defined boundaries. While research design means that experimental
research need not address group boundaries, organizational researchers must address this
issue because there is often significant boundary disagreement within teams - individuals who
are formally on a team do not agree on team membership (Mortensen 2004; Mortensen and
Hinds 2002). The result of boundary disagreement can be work groups within work groups that
affect patterns of information sharing.
We address these issues by examining the effect of work flows and relations on
information sharing in medical clinics. Next, we describe the study setting and then develop the
hypotheses. Methods, results and discussion follow.
THEORY
The argument focuses on the effect of work relations on information provision in dyads.
We focus on information provision because information provision is costly – information
providers take time away from more directly productive activities to assist the recipient (Myers
1984; Pearson et al. 1998; Reagans and McEvily 2003). There is also risk to the provider if she
Work and Talk
6
cannot provide a fully accurate answer. This may occur if all relevant details of the situation are
not known or there is not enough time to provide as complex answer as needed. While there
are costs to requesting information, such as loss of status or demonstrating ignorance (Blau
1963 (1955)), the risks and costs of providing information are greater. This implies that
information provision is a more conservative and reliable indicator of informal consulting than
information requesting or the existence of an information sharing relationship with another.
Following Reagans and McEvily, we expect that information transfer is more likely when
it is less costly to sender and receiver because shared common knowledge makes knowledge
transfer easier (2003). However, our argument differs from theirs because we focus on the
effects of work flows (referring patients to others) and work relationships (who works with
whom), on informal consulting. Work flows and relationships affect informal consulting in dyads
for two reasons. First, common work is a source of shared understanding. Second, when
relevant information is not transferred, such as contextual information, shared work relations
provide a readily available communication channel for informal consulting. We also argue that
work relations are often organized in groups that are settings of more intense informal
consultation.
DYADIC WORK FLOWS AND RELATIONS AND INFORMAL CONSULTING
Within medical clinics, there is extensive variation among patients and many problems
are difficult to analyze, making each clinic and each patient, unique (Berg 1997). The variation
and low analyzability increases uncertainty (Perrow 1967) which requires in information
provision to reduce. Within a clinic there are two key work relations that relate to information
provision: patient referral and work relationships.
Patient referral is typically organized in a centralized manner. Triage nurses or staff
greet patients and refer them to the appropriate provider. In a secondary set of referral
relationships, physicians refer patients to technicians for testing or, less frequently, to other
Work and Talk
7
physicians within the clinic. The work-with relationship shows who see each other as working
together to provide direct patient care.
Both relationships influence information provision. Individuals who refer patients to
others may have implicit knowledge that is not forwarded with the initial referral but can be
communicated later in an informal consultation. Stronger work-with relationships between
individuals lead to greater mutual availability for requesting, providing and receiving information.
During the care-giving process, for example, the informal consultation can be used to obtain
quick advice about diagnosis or treatment alternatives, assistance in interpretation, or
reassurance (Cross et al. 2001; Keating et al. 1998; Kuo et al. 1998).
Hypothesis 1: Referral and work-with relationships between individuals are associated
with greater information provision between those individuals.
WORK GROUPS, TEAMS, AND INFORMAL CONSULTING
It is likely that work groups, such as teams, affect informal consulting because they
create a boundary around a group of individuals who are working together. Teams are a special
form of a work group, usually being defined as having of at least two members who work
interdependently, share responsibility for a common task, and have a defined boundary (Cohen
and Bailey 1997; Hackman 2002; Salas et al. 2000). Interdependence implies a division of labor
among the team members.
In medical clinics, and in many other professional settings, there are two major
difficulties with using the typical analytic approach of using formal designations of teams or
grouping individuals in a common area (e.g., all senior managers constitute a top management
team). First, in professional settings there can be significant disagreement over team
boundaries (Mortensen 2004; Mortensen and Hinds 2002). Second teams can emerge from
interaction, as individuals find others with whom they are comfortable working or are collocated.
Group emergence may be an unintended consequence of organizational decisions. For
Work and Talk
8
example, in a medical clinic emergence could be due to the physical placement of nurse
stations and physician offices, which affects proximity which in turn affects who works with
whom.
We use structurally equivalent groups identified using work relations to identify work
teams. We argue that membership in these work groups affects information sharing. Since work
teams have a common boundary and work on a similar task, members of a work team have
similar relationships with other actors in an organization. Having similar relationships with others
in the organizations is the definition of structurally equivalent groups (Boorman and White 1976;
White et al. 1976a). This approach to defining group boundaries differs from commonly used
techniques based on, for example, departments or formally defined teams. This definition of
work groups suggests a minimal criterion for a work team – it should consist of actors who are
structurally equivalent in work relationships with others in the organization.
But, not all structurally equivalent groups are teams. Definitions of teams typically
include the ideas of interdependence and a division of labor (Cohen and Bailey 1997; Hackman
2002; Salas et al. 2000). Interdependence means that the individuals see themselves as
working together. The more often actors in a structurally equivalent work group report working
together, the more likely they are a team. The division of labor requirement suggests that the
greater the diversity of occupations among the members of a structurally equivalent group, the
more the group is a work team.
Examples illustrate the argument. In a medical clinic, the medical records staff is a group
that relates to others in the clinic in a similar manner. The staff organizes the medical records,
providing them as needed. The interdependence among the medical records staff is pooled,
with staff simply being collocated and going about their jobs independently. In contrast, a care
team consists of a reciprocally interdependent physician and rooming nurse.

Work and Talk
9
We expect that actors in structurally equivalent groups are more likely to interact within
the group, either because they share an identity that is formed because of similar relationships
(Tajfel 1982) or because they share a common task.
Hypothesis 2: Informal consulting is greater within structurally equivalent work groups
than between structurally equivalent work groups.
Second, within groups, we expect that the degree to which the work group is a team
affects informal consulting. Following the arguments about work group work relationship density
(working together) and occupational diversity, we expect that greater density and diversity
increase informal consulting. Information provision occurs because social cohesion based in
density affects interaction in a dyad through reputational consequences for individuals who are
uncooperative (Reagans and McEvily 2003). Greater cohesion, or work-with density, increases
observability of information provision and adverse reputational effects from not providing
information.2
Hypothesis 3: Increased the work group density leads to greater information provision
within the group.
Occupational heterogeneity also increases information provision. As a work group
becomes more occupationally heterogeneous, the sharing of information becomes less
occupationally based and more based on the work group’s shared tasks. Information provision
increases to assist the group in functioning in their particular environment (van Knippenberg et
al. 2004).
Hypothesis 4: Increased occupational heterogeneity within a group leads to greater
information provision within the group.
2 Note that the shard understanding effect is captured by the dyadic effect of working together.

Work and Talk
10
STUDY SETTING
We test the hypotheses by studying information sharing in medical clinics. This section
describes informal consulting in medical care and reviews the research on it. Work in medical
clinics relies on well coordinated work among diverse occupations. Because of technological
and professional developments, technicians and professionals have proliferated, creating new
roles and changing existing roles (Barley 1986; Barley 1990). For example, nurses and
physician assistants increasingly serve as buffers between patient and physician, and
technicians may function as brokers between equipment and physician (Barley 1996). The
changing health care environment creates new demands for coordination. Population aging
results in greater prevalence of chronic rather than acute conditions, requiring care provision by
different professionals. Managing patient care, particularly for those with chronic conditions,
increasingly requires integrating buffering roles, nurses regularly monitoring patient conditions,
and brokering roles, technicians measuring disease progress (Bodenheimer et al. 2002a;
Bodenheimer et al. 2002b). Care management also requires integrating a rapidly expanding
evidence base. Integrating knowledge about best practice and patient conditions requires
extensive information sharing.
Information sharing through informal consulting is recognized as important in practice. It
is "an informal process whereby a physician obtains information or advice from another
physician to assist in the management of a particular patient. The consultant neither reviews
the patient's record nor examines the patient and does not document his/her recommendations"
(Kuo et al. 1998, 905-906). Informal consulting facilitates the expeditious diagnosis and
treatment of patients (Wrobel et al. 2003) and is a “survival skill” of busy health care
professionals. “From the perspective of the requesting physician, the consultation may be more
efficient than searching the literature, it imposes no costs on patient or physician, it can
minimize the number of additional consultants in a complicated case, and it can help physicians
Work and Talk
11
keep current with medical information, … be intellectually stimulating, it may facilitate future
formal consultations, and it may disseminate knowledge of local experts” (Golub 1998, 929).
Informal consulting provides a variety of benefits, such as solutions to problems, pointers
to related information, problem reformulation, action validation, and legitimation (Cross et al.
2001; Cross and Sproull 2004). A study of questions asked in informal consultations of
infectious disease specialists showed that most questions involved solutions and pointers to
related information - determining the correct treatment, selecting a prophylaxis, interpreting
laboratory reports, and providing antibiotic information (Leblebicioglu et al. 2003). Similarly,
another study showed that informal consultation was frequently used to obtain diagnostic and
treatment information. Myers (1984) reported that about one-third of informal consults involved
straightforward questions which were covered in standard texts and training programs.
Age, specialty, and setting are associated with the frequency with which informal
consulting occurs (Kuo et al. 1998),. Older generalists are less likely to seek information (Kuo
et al. 1998). Generalists are more likely to request information than specialists, and specialists
are more likely to receive requests than generalists (Keating et al. 1998). Physicians in group
settings are more likely to request and provide information (Keating et al. 1998), which is
consistent with a proximity effect (Kuo et al. 1998). Similarly, physicians are most likely to
informally consult with readily available colleagues (Rappolt 2002). Physicians who see more
patients are more likely to request information, which is consistent with the argument that
informal consulting is an efficient, shortcut way of gathering information in a busy day (Keating
et al. 1998). Incentives and managed care also influence informal consulting. Physicians who
are capitated for health care services (i.e., paid a fixed sum per patient per period of time) are
more likely to request and provide information (Keating et al. 1998; but see Kuo et al. 1998).
Physicians employed by a health maintenance organization are more likely to consult informally
(Kuo et al. 1998). The capitation and managed care effects are consistent with the argument
Work and Talk
12
that physicians who share an incentive to minimize health care costs avoid formal consultation
costs through informal consults.
Physicians strongly approve of informal consulting, with generalists expressing a more
positive attitude than specialists, who worry about incomplete information from the requestor
and incomplete answers (Kuo et al. 1998). Both generalists and specialists feel that informal
consulting “saved money for the patient and third-party payer and that these consultations were
an important way for physicians to stay current with medical knowledge” (Kuo et al. 1998, 907).
DATA AND METHODS
SAMPLE AND SURVEY
Study data come from surveys of all members of four clinics (referred to here as A, B, C,
and D). Clinics A, B, and C are part of a large multi-specialty medical group that focuses on
highly integrated primary care, namely internal medicine, pediatrics, and obstetrics/gynecology.
The overall group has over 130 providers with 22 medical and surgical specialists. While the
clinics were not randomly sampled, they were chosen to provide contrasts: (A) a small
pediatrics practice; (B and C) two similar family practice clinics from the same medical group;
and (D) a clinic specializing in caring for patients with chronic conditions and extensive co-
morbidities.
Clinic A is a pediatrics service consisting of 6 pediatricians, 1 nurse practitioner, 6
medical assistants (MAs), 2 registered nurses (RNs) and 2 receptionists. The pediatrics
department is supported by administrative staff from the larger clinic. The administrative staff
from the surrounding clinic was not included in the survey. In this clinic (unlike the other 3
clinics in this study), the formal staffing model is functional. Nurses and physicians are
organized into separate occupational pools and assigned to work together on a rotating basis.
Clinic B is a freestanding family practice clinic consisting of 8 primary care providers (5
adult physicians, 1 pediatrician, 1 obstetrician, and 1 osteopath), 2 RNs, 2 LPNs, 4 CMAs, 4

Work and Talk
13
medical records staff, and 4 receptionists. Physicians and nurses or CMAs are assigned to
work together on a regular basis as a team.
Clinic C is a freestanding family practice clinic consisting of 11 primary care specialists
(7 internal medicine, 1 pediatrician, 1 obstetrician, 1 nurse practitioner, and 1 counselor), 2 RNs,
4 LPNs, 3 CMAs, 6 receptionists, and 4 medical records staff. Physicians and nurses or CMAs
are assigned to work together on a regular basis as a team.
Clinic D is a specialty clinic within a large multi-specialty medical group. This clinic has 5
physicians, 8 nurses, 6 staff, and 4 technicians. The physicians practice predominantly at the
specialty clinic, but also regularly practice in the medical group’s family practice clinics. As in
clinics B and C, teams of mixed occupations are the staffing practice in clinic D.
METHODS
All personnel at each clinic, including physicians, nurses, technical staff, and
administrative staff, were asked to fill out surveys. The members of each clinic were identified
by the clinic administrator and physician leaders, who also identified a convenient day for clinic
members to fill out the questionnaire and informed clinic members about the survey. During
survey administration, the research team was available to answer questions about the survey.
Overall clinic response rates ranged from 75% to 91%. Response rates among physicians and
nurses ranged from 85% to 94%.
The survey asked about demographics, roles, work, and relationships. The
demographic measures included birth year, gender, ethnicity, education, certification, and
licensing. Role- and work-related measures included number of years practicing at the clinic,
number of days per week, hours worked in most recent workweek, average number of patient
contacts per day, primary occupation in clinic (e.g., physician, nurse, staff, technician), and
clinical role (e.g., medical director, triage nurse, receptionist, medical supplies clerk). Other
measures included percent of time by activity in a week for: patient care (including activities

Work and Talk
14
such as ordering tests, calling in prescriptions, talking with patients on phone); clinic
administration; medical group administration; staying current professionally (e.g., continuing
medical education); and resolving health insurance issues.
The survey measured four different types of relationships. Relationships were measured
with items that listed all clinic members by name down the page in rows and relationships
across columns. The respondent answered the following questions for each person in the clinic
(i.e., for every row): For those people you know, how much do you interact with them in each of
the following relationships): (a) work-with to provide patient care; (b) refer patients to; (c) provide
information to in informal consults; and (d) receive information from in informal consults.
Definitions provided to respondents were:
• Work-with means that you and the other are interdependent when caring for patients –
your actions affect each other. It does not refer to the situation where you and the other
contribute separately to clinic performance because you work in the same location.
Please consider all others, such as physicians, rooming nurses, staff, laboratory
technicians, and receptionists, with whom you work when delivering patient care.
• Refer patients to means referring a patient to another provider in your clinic, such as a
physician, triage nurse, or patient education.
• Informal consultation refers to obtaining or providing information about caring for a
patient without formally consulting with the patient, formally reviewing the patient’s
record, or formally documenting the consultation.
• Patient care means all patient care activity, including activities such as direct patient
contact, ordering prescriptions, managing laboratory and radiology testing.
MEASURES
The dependent variable, provide information, was constructed using respondents’
answers to the questions on provide and receive information in informal consults. Responses
Work and Talk
15
from these two questions formed two matrices. In one matrix, each respondent indicates to
which colleagues and with what frequency she provides information. In the other matrix, each
respondent indicates from whom and with what frequency she receives information. The matrix
entries consist of 0 (“Never”), 1 (“A little”), 2 (“Some”), or 3 (“A lot”). Transposing the “receive
information” matrix and combining it with the “provide information” matrix by taking the minimum
of corresponding cells forms the analysis matrix. For example, if person A reports providing
information to B “A lot” (3) and person B reports receiving information from A “Some” (2), the A
provides information to B cell in the analysis matrix is coded as “Some” (2). This procedure
both confirms the existence of the relationship – both provider and receiver report the
relationship – and provides a conservative estimate of its frequency, increasing measurement
reliability. Note that the resulting matrix is asymmetric – A can report providing information to B
while B does not report providing information to A. For all relationships studied, the analysis
includes only those individuals who responded.
For testing Hypothesis 1 about the effect of referral relationships, refer patients was
measured using the patient referral relationship question. Like the information provision
relationship, the refer patient to relationship may be asymmetric and is thus represented by two
dyads for every pair of individuals (e.g., A may refer patients to B and B may not refer patients
to A). Values ranged from 0 (None) to 3 (A lot). A confirmation procedure, such as that used
for information provision, was not used for this relationship because receivers of patient referrals
may not always be aware of who sent the patient.
For testing Hypothesis 1 about the effect of the work-with relationship, the work-with
relationship was measured using the responses to the work-with question. The entries are
valued 0 (None) to 3 (A lot). Because the work-with relationship is symmetric (if A reports
working with B, B should report working with A), every pair of individuals is represented by a
single dyad. The matrix value for that dyad was constructed by taking the minimum value of A’s

Work and Talk
16
response about working with B and B’s response about working with A. The work-with
relationship is confirmed.
Hypotheses 2 through 4 concern work group effects. Work groups were sets of
individuals identified as structurally equivalent using the work-with relationship (Wasserman and
Faust 1994; White et al. 1976b) and the CONCOR structural equivalence algorithm in SPAN
(Moody 2000), a social network analysis package for SAS.3
Hypothesis 2, that informal consulting is greater among members of a work group, was
tested by estimating a model that contained an indicator for being members of a common work
group. Hypotheses 3 and 4 were tested by adding measures for work group density,
occupational heterogeneity, and their interaction to the first model. Work group density was
measured as the density of the work with relationship within the group. Occupational
heterogeneity is measured using a Herfindahl index of the sum of the squared proportions of
each occupation within the group. The interaction of work group density with occupational
heterogeneity was included to allow for moderation effects. Work group size is included as a
control variable because density often varies with group size.
CONTROLS
We control for occupational similarity because it is likely to affect informal consulting for
two reasons. First, individuals with similar occupational backgrounds are more likely to provide
information to each other because of similar training (e.g., Reagans and Zuckerman 2001). We
initially control for this effect by estimating a model with a single indicator for occupational
similarity. Because the length of training affects the amount of shared knowledge and strength
3 The SPAN algorithm to identify structurally equivalent work groups was used, with the number of splits was set to 3 and the convergence criteria to .001. Because of clinics A and D smaller size, the group partitions at the third level were used. Because of clinics B and C’s larger size, group partitions at the fourth level were.
Work and Talk
17
of status hierarchies,4 we also estimate models that control for occupational similarity by
occupational pairs (e.g., physicians-physicians, nurses-nurses, physicians-nurses).
The measure of occupational similarity was coded based on degrees and roles (MD/OD,
RN, CMA/LPN, technicians, and staff). Degrees were used for medical staff because of the
homogeneity of degrees and training. Roles were used for staff and technicians because of the
heterogeneity of degrees and training .5 Technicians were coded in a separate category if
enough technicians in the clinic responded to make individuals unidentifiable when clinic-
specific graphs were viewed by clinic members; otherwise they were included with staff. For
each pair of individuals within a clinic, an indicator was set to one if both individuals had the
same occupation. Occupational similarity-specific indicators (MD to MD, N to N, etc.) were used
to control for differences across occupations in the likelihood of informal consulting.
Similarity in gender and age were included as control variables. An indicator was set to
one if both individuals were the same gender, and the absolute value of the age difference was
calculated.
METHODS
For the multivariate analysis, each row of data was a unique dyad and data was pooled
across clinics to obtain more efficient estimates.6 Since the unit of analysis is the dyad, each
individual is included in the analysis multiple times as an information provider and as an
4 The strong status hierarchy in medicine is strongly correlated with specific status markers of expertise in tasks. While there is an incentive to approach high status individuals because of their expertise (Bunderson 2003), the costs of approaching them are higher because of the higher value of their time.
5 In the graphs, nurses include registered nurses, licensed practical nurses, and certified medical assistants to maintain confidentiality when the graphs are viewed by clinic members. Similarly, physicians included family practitioners, pediatricians, obstetricians, and osteopaths.
6 Models estimated separately for each clinic that included the group characteristics did not converge in three of the four clinics. Separate models estimated for each clinic that included work with, patient referral, occupational similarity, gender similarity, age difference, and whether the individuals in a dyad were in the same work group and did not include work group characteristics did converge. The results from these models were similar to the estimates from the pooled
Work and Talk
18
information receiver. This can result in correlated errors. This problem has been approached in
a variety of ways by network researchers. Some use a quadratic assignment procedure (QAP)
(Krackhardt 1987) while others include an indicator variable for each sender and receiver (e.g.,
Reagans and McEvily 2003). Neither of these approaches fit the information provision data
well. Among all dyads, the frequencies for level of information provision from 0 to 3 were 1,701,
181, 90, and 14, respectively. A linear model fails to take into account this highly skewed
response distribution. An ordered logit model is more appropriate because it assumes a
continuous underlying distribution for information provision but estimates cut-points for each
category. The inclusion of indicators for each receiver and sender resulted in the loss of data
associated with six individuals because of collinearity and the model did not converge. So, the
Ologit procedure (ordinal logit) using the bootstrap option with 1,000 iterations in Stata 9 was
used to estimate the model for dyads for information provision. The bootstrap procedure
estimates the model using resamples with replacement from the original data. The
bootstrapped standard errors are not dependent on distributional assumptions (Stata Press
2005).
Five models were estimated. The first two models tested Hypothesis 1. Model 1
measures occupational similarity using an indicator to measure whether two individuals were
the same occupation. Model 2 generalizes this model by allowing the effect of occupational
similarity/difference to vary across occupations. Model 3 adds the measures of work group
characteristics that are necessary to test Hypotheses 2 through 4. Model 4 extends this model
to see how work centrality in an occupation affects information provision. Model 5 examines the
special case of reciprocated information provision, the minimum level of information provision in
a dyad. Blau (1963 (1955), 131) found that reciprocity in informal consultation was a special
analysis with the exception that individuals in different work groups were less likely to provide information.

Work and Talk
19
case of informal consultation since it “virtually eliminated the danger of rejections as well as the
status threat implicit in asking for help, since the roles questioner and consultant were
intermittently reversed.” Because of the lower threat, Blau further argues that reciprocal
relations support seeking reassurance. And, it seems reasonable to argue that reciprocity may
be more likely to serve a social role than other forms of informal consultation. Since there is only
a single-valued dependent variable for each dyad, only half the dyads are included in the
analysis and the indicator for a physician-nurse dyad was set to one if the dyad was a
physician-nurse pair.
We also estimated an individual-level model to examine the individual correlates of being
an opinion leader. The sums of all send and receive information measures for each individual
were regressed on measures of individual characteristics. Because the sum is positive, the
QLIM procedure in SAS was used to estimate a Tobit model.
RESULTS
DESCRIPTIVE STATISTICS
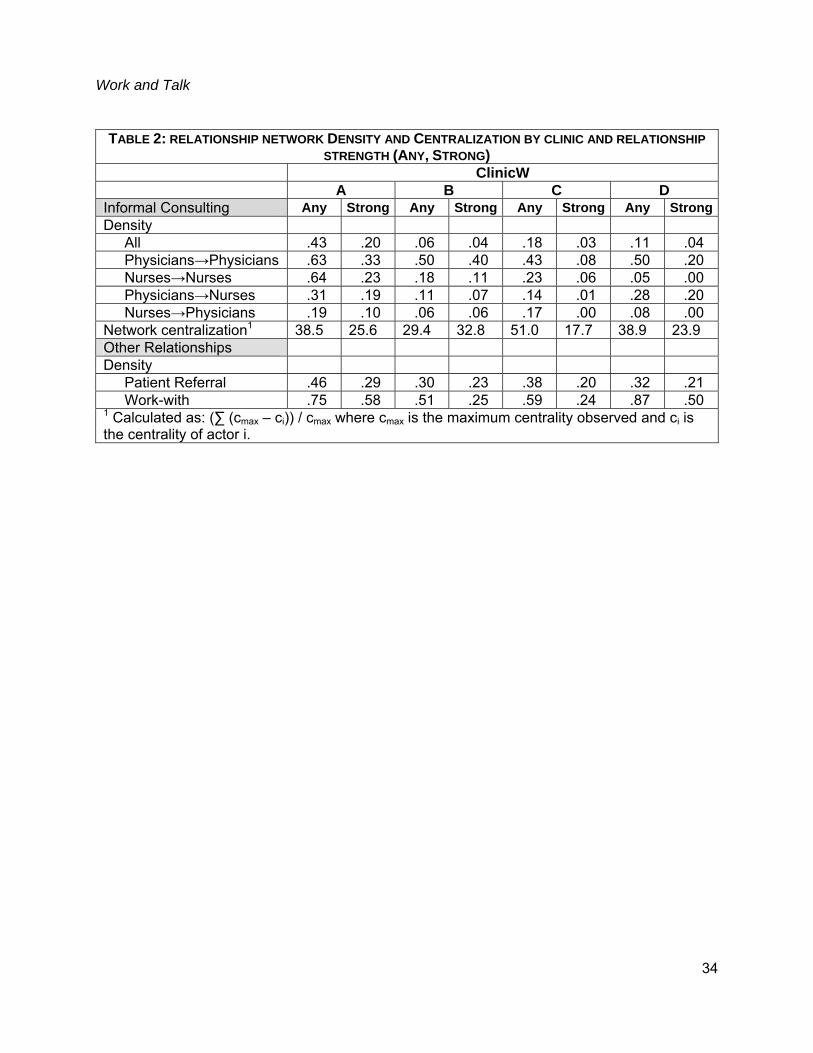
Table 1 shows descriptive statistics. Table 2 shows network density and centralization
for the informal consulting relationships, and the densities of the work-with and patient referral
relationships. Density is calculated both by relationship strength and by occupational
characteristics. Relationships are classified as “any” (A little, Some, A lot) or strong (Some, A
lot). Relationships can be between any two occupations, or defined by the occupations of the
participants. The density measures show that information provision tends to occur intra-
occupationally, and more often among physicians. Inter-professional information provision
tends to occur from physicians to nurses. Interestingly, the highest levels of strong information
provision among physicians occur in clinics B and A, even though the work group organization
differs significantly between the two. Clinic A’s small size, focus on pediatrics, and staffing from
pools may encourage dense, decentralized information provision among physicians (Figure 1).

Work and Talk
20
Clinic B’s dense informal consulting among physicians appears to be associated with MD23’s
central role. The network centralization measures for the strong informal consulting relationship
support this argument as Clinic B has the most centralized informal consulting network.
MULTIVARIATE ANALYSES
Table 3 shows the results of the multivariate analysis of the determinants of information
provision. Models 1 and 2 support Hypothesis 1 for referral relationships and not for work-with
relationships. Individuals who refer patients to others are more likely to provide information.
Model 2 refines this analysis and checks whether the finding is an artifact of having a single
indicator for occupational similarity by allowing the effect of occupational similarity to vary
across occupations. The referral effect is still significant. In contrast to nurses providing
information to each other, LPN/CMAs and other pairs are less likely to provide information.
Models 1 and 2 also test Hypothesis 2 that individuals within the same work group are
more likely to interact. This is demonstrated by a negative effect of working in different work
groups on information provision. This means that actors in structurally equivalent relationships
are more likely to interact with each other. This effect is consistent: the presence of a boundary,
either formal or emergent.
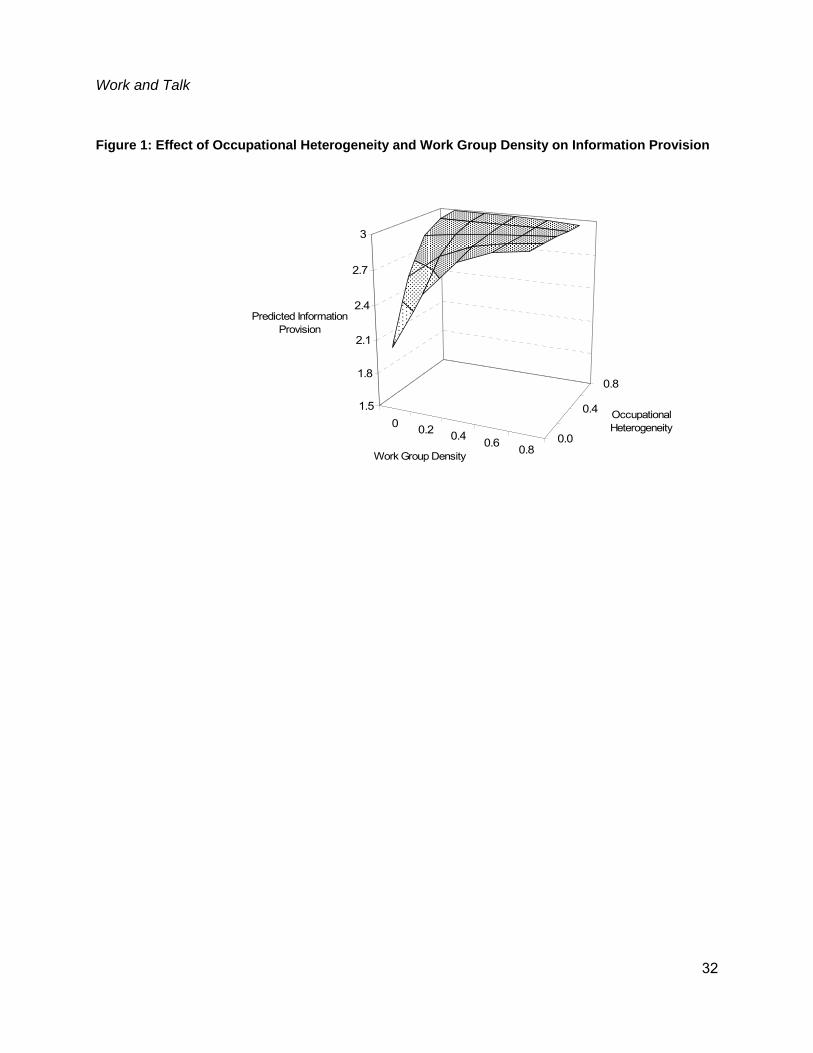
Model 3 tests Hypotheses 2 through 4 by adding the work group measures. These
hypotheses are supported. Within work groups, higher levels of work relationship density and
occupational heterogeneity are associated with higher levels of information provision. The
negative interaction of density and heterogeneity reflects a very slight attenuation of the effects
at high levels (Figure 5). Interestingly, once characteristics of work groups are included, Model
3 also suggests that work group size is positively associated with information provision.
Perhaps in larger work groups there are more opportunities for finding a similar other with whom
to interact (Gibson and Vermeulen 2003).

Work and Talk
21
Some of the effects from Models 1 and 2 change when work group characteristics are
included in Model 3. The effect of working in different work groups becomes positive, suggesting
that bridging occurs across work groups. This is consistent with the arguments that within group
information provision focuses on direct task-related information and information seeking across
groups involves less task-specific knowledge. And, the effect for occupational similarity among
physicians becomes significant. This also suggests a bridging effect across groups among
physicians.
Model 4 extends Model 3 by adding the interaction of occupational centrality for the two
members of the dyad. The strong positive effect and the decrease of the effect of working in
different groups suggest that bridging occurs between individuals who are occupationally
central. The effect of the work relationships becomes significant and positive, which supports
Hypothesis 1, and the effect of occupational similarity among physicians increases.
Model 5 examines the determinants of reciprocity - individuals in a dyad sharing
information with each other. The results are similar to Models 3 and 4 but the effect of physician
similarity increases yet again. And, the effect of the work-with relationship increases relative to
Model 4. This suggests that reciprocity is strongly influenced by work relationships, and by
status equality, either due to being in a high status occupation or being central in one of a
medical clinic’s occupational group.
Table 4 explores the correlates of being an opinion leader. The dependent variable is the
sum of all the information provision measures, either as a sender or receiver, for an individual.
The analysis suggests that nurses, physicians, and technicians who refer patients to others
within the clinic are active in informal consulting. For technicians, this may be may be
associated with their buffering role; they act as an intermediary between technology and others
(Barley 1996). For physicians and technicians, a high refer-in degree is positively associated
with informal consulting. This may be associated with requests to follow up on the referral.
Work and Talk
22
Interestingly, technicians are less likely than staff (the contrast category) to be involved in
informal consulting. Perhaps technicians only become involved in information provision when
they are involved in a patient referral arrangement. Finally, physicians who are central in work
networks are more likely to be informally consulted. This may be due their having a broader
perspective on clinic operations than other physicians and being more likely to be able to
provide information. Higher technician’s work-with centrality is associated with a decrease in
the likelihood of being consulted. The lower informal consulting by technicians who are central
in work relationships may be due to lack of work centrality being associated with less clear
communication.
DISCUSSION
We have shown that work relationships influence information sharing. Inductive case
studies show similar strong effects. This point may seem obvious. But, if it is so obvious, its
absence in of information sharing studies is striking. Not controlling for work relationships can
result in spurious findings. In a work environment with diverse expertise, completing work
requires interaction among diverse individuals. Because it is difficult to convey all relevant
information, contextual and otherwise, in professional work such as patient care, work
relationships are accompanied by informal consulting. And, during this interaction, individuals
come to know who has what expertise. This results in a spurious correlation between knowing
who knows what and informal consulting, which are both caused by working together. Since not
controlling for work flows and work relationships runs the strong risk of generating spurious
findings, our research provides a foundation from which to build other models of information
sharing.
Our finding that occupational diversity increases information sharing contradicts
Bunderson and Sutcliffe’s finding that occupational diversity decreased information sharing
(Bunderson and Sutcliffe 2002). This difference may be caused by the way team boundaries
Work and Talk
23
were identified. Bunderson and Sutcliffe included all individuals in top management teams,
which had an average size of 11 members. Subgroups can easily form in larger groups.
Perhaps the negative effect that Bunderson and Sutcliffe observed was caused by subgroups
forming within top-management teams with high levels of information sharing within subgroups
and low levels between subgroups. Further research is necessary to determine if this occurred.
But, our results suggest that accounting for sub-group formation within larger groups (clinics, top
management teams) is important for analyzing information sharing.
An important contribution of this paper is examining the relationship between work
networks and information provision. We found that work flows, such as patient referral and
work-with relationships, and work group characteristics increase information provision. We
argued that the reason for the work relationship effects is that information transmitted with work,
particularly in medical clinics, may be often summarized and not fully contain all the sender’s
observations. Further research is necessary to examine this assumed theory of information
summary within clinics.
A second important contribution is demonstrating that structurally equivalent work
groups based on work relationships affect information provision. Individuals in structurally
equivalent work groups have higher levels of information sharing. Information sharing is more
likely when work-with density and occupational heterogeneity are high. This suggests that
information sharing increases as groups take on team like characteristics.
Our approach of using structurally equivalent work groups is a promising approach to
identifying and measuring work groups and teams in ambiguous environments. Typically,
teams are identified and measured using formal organizational structures, such as identifying all
software development teams. Formal teams are often relatively durable with an assigned
mission. In dynamic professional environments, teams may not have such clear boundaries
and team characteristics may be emergent. In extreme cases, teams may be temporary,

Work and Talk
24
assembled and disbanded quickly (Chilingerian and Glavin 1994). Identifying groups of
structurally equivalent actors based on a self-reported work-with relationship, provides a
method to identify groups and teams that may be particularly valuable in settings where teams
are emergent.
There are two arguments supporting the approach of using structural equivalence to
identify work groups. First, the results in this paper are consistent with our arguments about
teams and work groups. Second, other organizational research supports such an approach.
Research shows that structural equivalence affects the diffusion of innovations (Burkhardt and
Brass 1990; Burt 1987). Research on common membership in a work group shows that
common work team membership affects shared meanings (Klein et al. 2001), common
departmental membership does not influence shared meaning (Young and Parker 1999), and
that membership in work-based interaction groups affects shared meanings (Rentsch 1990;
Rentsch and Klimoski 2001; Totterdell et al. 2004; Young and Parker 1999). These interaction
groups have been measured as employee groups consisting of individuals who have structurally
equivalent work relationships. It seems reasonable to expect that the shared work environment,
because of equivalence in work relations and interaction, results in common information flows
that result in shared beliefs.
Further research is required, however, to more completely examine our approach to
identifying and measuring work groups. One test would be to compare teams identified through
work relations with formally identified teams or departments. Another test would be to compare
teams identified through work relations with the teams of which individuals subjectively report
themselves to be members.
A significant limitation of this study is that it is based on four clinics. The social network
methods used here required a very high response rate. This in turn required extensive
interaction and preliminary work to gain access to the clinics. The results do suggest that we

Work and Talk
25
can draw some generalizations, such as the effect of work relationships and social similarity on
information provision. We cannot yet explain why the appearance of each clinic’s informal
consulting network differed so greatly.
A second limitation is that we studied information provision only within clinics.
Individuals could obtain information from others outside their clinic. The research could be
extended by including boundary-spanning relationships and examining how externally acquired
information is shared within a clinic. Understanding when external sources function as
substitutes for internal sources and when external sources provide knowledge that is shared
within a clinic may be a key to understanding which clinics are more successful at implementing
evidence-based care and becoming a learning organization.
In conclusion, this paper extends organizational research on information sharing by
showing how work relationships affect information provision and how work groups and work
group structures affect information provision. Given the centrality of work and work relationships
in instrumental work organization, it is reasonable to argue that these models of the effect of
work relationships on information provision should be the baseline model for testing other
theories about information provision.

Work and Talk
26
REFERENCES
Aldrich, Howard and Martin Ruef. 2006. Organizations Evolving. London: Sage Publications.
Austin, John R. 2003. "Transactive memory in organizational groups: The effects of content,
consensus, specialization, and accuracy on group performance." Journal of Applied
Psychology 88:866-878.
Barley, Stephen R. 1986. "Technology as an occasion for structuring: Evidence from
observations of CT scanners and the social order of radiology departments."
Administrative Science Quarterly 31:78-108.
—. 1990. "The alignment of technology and structure through roles and networks."
Administrative Science Quarterly 35:61-103.
—. 1996. "Technicians in the workplace: Ethnographic evidence for bringing work into
organization studies." Administrative Science Quarterly 41:404-441.
Bechky, Beth A. 2003. "Sharing Meaning Across Occupational Communities: The
Transformation of Understanding on a Production Floor." Organization Science 14:312-
330.
Berg, M. 1997. Rationalizing Medical Work. Cambridge, MA: The MIT Press.
Blau, Peter M. 1963 (1955). The Dynamics of Bureaucracy: A Study of Interpersonal Relations
in Two Government Agencies. Chicago: University of Chicago Press.
Bodenheimer, T., E. H. Wagner, and K. Grumbach. 2002a. "Improving primary care for patients
with chronic illness." Journal of the American Medical Association 288:1775-9.
—. 2002b. "Improving primary care for patients with chronic illness: the chronic care model, Part
2." Journal of the American Medical Association 288:1909-14.
Boorman, Scott A. and Harrison White, C. 1976. "Social structure form multiple networks: II.
Role structures." American Journal of Sociology 81:1384-1447.
Borgatti, Stephen P. and Rob Cross. 2003. "A Relational View of Information Seeking and
Learning in Social Networks." Management Science 49:432-445.

Work and Talk
27
Bunderson, J. Stuart. 2003. "Recognizing and Utilizing Expertise in Work Groups: A Status
Characteristics Perspective." Administrative Science Quarterly
Administrative Science Quarterly J1 - Administrative Science Quarterly 48:557-591.
Bunderson, J. Stuart and Kathleen M. Sutcliffe. 2002. "Comparing Alternative
Conceptualizations Of Functional Diversity In Management Teams: Process And
Performance Effects." Academy of Management Journal 45:875-893.
Burkhardt, Marlene E. and Daniel J. Brass. 1990. "Changing patterns or patterns of change: the
effects of a change in technology on social network structure and power." Administrative
Science Quarterly 35:104-.
Burt, Ronald S. 1987. "Social Contagion and Innovation: Cohesion Versus Structural
Equivalence." American Journal of Sociology 92:1287-1335.
Chilingerian, J. A. and M. P. Glavin. 1994. "Temporary firms in community hospitals: elements
of a managerial theory of clinical efficiency." Medical Care Research and Review
51:289-335.
Cohen, Susan G. and Diane E. Bailey. 1997. "What makes teams work: Group effectiveness
research from the shop floor to the executive suite." Journal of Management 23:239-290.
Cross, Rob, Stephen P. Borgatti, and Andrew Parker. 2001. "Beyond answers: Dimensions of
the advice network." Social Networks 23:215-235.
Cross, Rob and Lee Sproull. 2004. "More Than an Answer: Information Relationships for
Actionable Knowledge." Organization Science 15:446-462.
Gibson, Cristina and Freek Vermeulen. 2003. "A Healthy Divide: Subgroups as a Stimulus for
Team Learning Behavior." Pp. 202-239 in Administrative Science Quarterly, vol. 48.
Golub, R. M. 1998. "Curbside consultations and the viaduct effect." Journal of the American
Medical Association 280:929-30.
Hackman, J. Richard. 2002. Leading Teams: Setting the Stage for Great Performances. Boston,
MA: Harvard Business School Press.
Work and Talk
28
Keating, N. L., A. M. Zaslavsky, and J. Z. Ayanian. 1998. "Physicians' experiences and beliefs
regarding informal consultation." Journal of the American Medical Association 280:900-
904.
Klein, Katherine J., Amy Buhl Conn, D. Smith, and Joann Speer Sorra. 2001. "Is everyone in
agreement? An exploration of within-group agreement in employee perceptions of the
work environment." Journal of Applied Psychology 86:3-16.
Krackhardt, David. 1987. "QAP partialling as a test of spuriousness." Social Networks 9.
Kuo, D., D. R. Gifford, and M. D. Stein. 1998. "Curbside consultation practices and attitudes
among primary care physicians and medical subspecialists." Journal of the American
Medical Association 280:905-9.
Leblebicioglu, H., A. Akbulut, S. Ulusoy, M. Sunbul, K. Aydin, M. F. Geyik, S. Esen, and C.
Eroglu. 2003. "Informal consultations in infectious diseases and clinical microbiology
practice." Clinical Microbiology and Infection 9:724-6.
Moody, James. 2000. "SPAN: SAS Programs for Analyzing Networks." Columbus, OH: James
Moody.
Moreland, Richard L. and Larissa Myaskovsky. 2000. "Exploring the Performance Benefits of
Group Training: Transactive Memory or Improved Communication?*1." Organizational
Behavior and Human Decision Processes 82:117-133.
Mortensen, Mark. 2004. "Antecedents And Consequences Of Team Boundary Disagreement."
Academy of Management Proceedings:M1-M6.
Mortensen, Mark and Pamela Hinds. 2002. "Fuzzy teams:Boundary disagreement in distributed
and colocated teams." Pp. 281-308 in Distrtibuted Work, edited by P. J. Hinds and S.
Kiesler. Cambridge, MA: MIT Press.
Myers, J. P. 1984. "Curbside consultation in infectious diseases: a prospective study." Journal
of Infectious Diseases 150:797-802.

Work and Talk
29
Pearson, S. D., R. Moreno, and Y. Trnka. 1998. "Informal consultations provided to general
internists by the gastroenterology department of an HMO." Journal of General Internal
Medicine 13:435-8.
Perrow, Charles. 1967. "A framework for the comparative analysis of organizations." American
Sociological Review 32:194-208.
Rappolt, S. 2002. "Family physicians' selection of informal peer consultants: Implications for
continuing education." The Journal of Continuing Education in the Health Professions
22:113-20.
Reagans, Ray and Bill McEvily. 2003. "Network Structure and Knowledge Transfer: The Effects
of Cohesion and Range." Pp. 240-267 in Administrative Science Quarterly, vol. 48:
Administrative Science Quarterly.
Reagans, Ray and Ezra W. Zuckerman. 2001. "Networks, Diversity, and Productivity: The
Social Capital of Corporate R&D Teams." Organization Science 12:502.
Reddy, Madhu and Paul Dourish. 2002. "A finger on the pulse: temporal rhythms and
information seeking in medical work " Pp. 344-353 in Proceedings of the 2002 ACM
conference on Computer supported cooperative work. New Orleans, Louisiana, USA
ACM Press.
Rentsch, J.R. 1990. "Climate and Culture: Interaction and Qualitative Differences in
Organizational Meanings." Journal of Applied Psychology 75:668-681.
Rentsch, Joan R. and Richard J. Klimoski. 2001. "Why do 'great minds' think alike? Antecedents
of team member schema agreement." Journal of Organizational Behavior 22:107-120.
Salas, Eduardo, C. Shawn Burke, and Janis A. Cannon-Bowers. 2000. "Teamwork: Emerging
principles." International Journal of Management Reviews 2:339-356.
Stasser, Garold, Sandra I. Vaughan, and Dennis D. Stewart. 2000. "Pooling Unshared
Information: The Benefits of Knowing How Access to Information Is Distributed among

Work and Talk
30
Group Members*1." Organizational Behavior and Human Decision Processes 82:102-
116.
Stata Press. 2005. Stata Release 9, Users Manual, Reference K-Q. College Station, Texas:
Stata Press.
Tajfel, Henri. 1982. "Social Psychology of Intergroup Relations." Annual Review of Psychology
33:1-39.
Totterdell, Peter, Toby Wall, David Holman, Holly Diamond, and Olga Epitropaki. 2004. "Affect
Networks: A Structural Analysis of the Relationship Between Work Ties and Job-Related
Affect." Journal of Applied Psychology 89:854-867.
van Knippenberg, Daan, Carsten K. W. De Dreu, and Astrid C. Homan. 2004. "Work Group
Diversity and Group Performance: An Integrative Model and Research Agenda." Journal
of Applied Psychology 89:1008-1022.
Wasserman, Stanley and Katherine Faust. 1994. Social network analysis : Methods and
applications. Cambridge ; New York: Cambridge University Press.
Wegner, Daniel M., Paula Raymond, and Ralph Erber. 1991. "Transactive Memory in Close
Relationships." Journal of Personality & Social Psychology 61:923-929.
White, Harrison C., Scott A. Boorman, and Ronald L. Breiger. 1976a. "Social Structure from
Multiple Networks. I. Blockmodels of Roles and Positions." American Journal of
Sociology 81:JAN, 730-780.
—. 1976b. "Social Structure from Multiple Networks. I. Blockmodels of Roles and Positions."
American Journal of Sociology 81:730-780.
Wrobel, J. S., M. P. Charns, P. Diehr, J. M. Robbins, G. E. Reiber, K. M. Bonacker, L. B. Haas,
and L. Pogach. 2003. "The relationship between provider coordination and diabetes-
related foot outcomes." Diabetes Care 26:3042-7.
Work and Talk
31
Young, Scott A. and Christopher P. Parker. 1999. "Predicting collective climates: Assessing the
role of shared work values, needs, employee interaction and work group membership."
Journal of Organizational Behavior 20:1199-1218.
Work and Talk
32
Figure 1: Effect of Occupational Heterogeneity and Work Group Density on Information Provision
0 0.2 0.4 0.6 0.80.0
0.4
0.8
1.5
1.8
2.1
2.4
2.7
3
Predicted Information Provision
Work Group Density
Occupational Heterogeneity

Work and Talk
33
TABLE 1: DESCRIPTIVE STATISTICS FOR RESPONDENTS BY CLINIC Clinic A (N=14) MEAN STD Age 45.00 15.51 Gender (Female=1) 0.79 0.43 Physician (=1) 0.43 0.51 Nurse (=1) 0.57 0.51 Staff (=1) 0.00 0.00 Technician (=1) 0.00 0.00 Percent of time direct patient care 71.64 34.78 Days per week 4.39 1.06 Patients per day 17.92 9.69 Years at clinic 9.20 6.83 Clinic B (N=29) Age 45.38 9.70 Gender (0 = Male, 1 = Female) 0.72 0.45 Physician (=1) 0.21 0.41 Nurse (=1) 0.31 0.47 Staff (=1) 0.41 0.50 Technician (=1) 0.07 0.26 Percent of time direct patient care 40.48 34.88 Days per week 3.75 1.67 Patients per day 27.38 26.21 Years at clinic 5.14 4.33 Clinic C (N=26) Age 48.15 7.94 Gender (0 = Male, 1 = Female) 0.73 0.45 Physician (=1) 0.42 0.50 Nurse (=1) 0.42 0.50 Staff (=1) 0.13 0.34 Technician (=1) 0.04 0.20 Percent of time direct patient care 47.88 35.70 Days per week 4.06 1.61 Patients per day 27.94 14.63 Years at clinic 9.25 7.44 Clinic D (N=19) Age 49.00 10.32 Gender (0 = Male, 1 = Female) 0.74 0.45 Physician (=1) 0.26 0.45 Nurse (=1) 0.26 0.45 Staff (=1) 0.32 0.48 Technician (=1) 0.16 0.37 Percent of time direct patient care 46.42 37.86 Days per week 4.68 0.67 Patients per day 21.23 28.41 Years at clinic 6.87 6.14
Work and Talk
34
TABLE 2: RELATIONSHIP NETWORK DENSITY AND CENTRALIZATION BY CLINIC AND RELATIONSHIP STRENGTH (ANY, STRONG)
ClinicW A B C D Informal Consulting Any Strong Any Strong Any Strong Any StrongDensity All .43 .20 .06 .04 .18 .03 .11 .04 Physicians→Physicians .63 .33 .50 .40 .43 .08 .50 .20 Nurses→Nurses .64 .23 .18 .11 .23 .06 .05 .00 Physicians→Nurses .31 .19 .11 .07 .14 .01 .28 .20 Nurses→Physicians .19 .10 .06 .06 .17 .00 .08 .00 Network centralization1 38.5 25.6 29.4 32.8 51.0 17.7 38.9 23.9 Other Relationships Density Patient Referral .46 .29 .30 .23 .38 .20 .32 .21 Work-with .75 .58 .51 .25 .59 .24 .87 .50 1 Calculated as: (∑ (cmax – ci)) / cmax where cmax is the maximum centrality observed and ci is the centrality of actor i.

Work and Talk
35
TABLE 3: DETERMINANTS OF INFORMATION PROVISION
MODEL 1: BASE MODEL 2:
OCCUPATIONS MODEL 3: WORK
GROUPS MODEL 4: ACTOR
CENTRALITY MODEL 5:
RECIPROCITY OBS BTS OBS BTS OBS BTS OBS BTS OBS BTS
COEFF ERR. COEFF ERR. COEFF ERR. COEFF ERR. COEFF ERR. WORK RELATIONS Refer patients to (Max in Mdl 5) 0.65* 0.07 0.52* 0.07 0.54* 0.07 0.51* 0.08 0.73* 0.13 Work-with 0.19 0.07 0.35 0.07 0.33 0.08 0.23* 0.08 0.46* 0.13 Occupational Centrality of Sender * Occupational Centrality of Receiver 2.63* 0.46 2.89* 0.80 OCCUPATIONAL RELATIONSHIPS Same degree 0.76* 0.15 Nurse to Nurse (Contrast) Physician to Physician 0.57 0.41 0.94* 0.40 1.26* 0.38 1.64* 0.63 LPN/CMA to LPN/CMA -1.54* 0.61 -1.36* 0.55 -1.57* 0.55 -1.69 7.26 Physician to Nurse (Phys-Nrs pair, mdl 5) 0.18 0.49 0.71 0.47 0.86† 0.46 0.62 0.69 Nurse to Physician -0.93 0.50 -0.39 0.52 -0.23 0.49 Other to Other -1.33* 0.41 -1.18 0.38 -1.16* 0.37 -0.92 0.62 DEMOGRAPHIC SIMILARITY Same Gender 0.17 0.15 0.39 0.15 0.42* 0.16 0.45* 0.17 0.58* 0.28 Age Difference -0.03* 0.01 -0.02* 0.01 -0.02* 0.01 -0.02* 0.01 -0.01 0.01 WORK GROUPS Different Work Groups -0.89* 0.17 -1.04* 0.17 7.70* 2.03 6.59* 2.02 7.76* 3.15 Group Size 0.60* 0.14 0.66* 0.15 0.76* 0.26 Work Group Density 8.34* 2.42 6.24* 2.33 7.73* 3.69 Occupational Heterogeneity 10.07* 3.53 8.52* 3.47 12.36* 5.62 Occupational Heterogeneity * Work Group Density -16.24* 4.64 -13.79* 4.53 -20.67* 7.41 CLINIC EFFECTS Clinic 1 (Contrast) Clinic 2 -3.29* 0.24 -2.67* 0.25 -2.30* 0.28 -2.19* 0.28 -3.14* 0.54 Clinic 3 -1.93* 0.21 -1.52* 0.21 -1.12* 0.23 -0.89* 0.23 -1.02* 0.40 Clinic 4 -2.57* 0.26 -2.08* 0.26 -1.69* 0.30 -1.97* 0.32 -2.63* 0.63 ORDERED LOGISTIC CUTPOINTS Cut 1 -0.23 0.32 -0.61 0.47 8.73 2.10 7.99 2.10 10.89 3.25 Cut 2 1.11 0.32 0.83 0.47 10.23 2.12 9.51 2.12 12.49 3.26 Cut 3 3.31 0.36 3.13 0.51 12.56 2.11 11.83 2.11 15.05 3.24 Pseudo R-squared 0.18 0.22 0.24 0.26 0.31
* - p < .05; † < .10. Estimated using OLogit in Stata 9 with bootstrap option for errors.

Work and Talk
36
TABLE 4: OCCUPATIONAL AND WORK FLOW DETERMINANTS OF INDIVIDUAL INFORMAL CONSULTING LEVELS†
OCCUPATION (STAFF CONTRAST) EST. T EST. T Physician 11.74* 3.05 2.36 0.27 Nurse 5.52 1.81 6.74 0.98 Technician 4.35 0.90 -89.38* -7.94 WORK RELATIONS Refer Out Degree 15.58* 3.39 * Physician 33.11* 3.52 * Nurse 17.79* 3.23 * Technician 190.22* 4.83 * Staff 0.32 0.04 Refer In Degree 27.54* 2.39 * Physician 34.48* 2.15 * Nurse 23.23 1.59 * Technician 555.82* 32.06 * Staff 43.60 1.42 Work-with Degree Centrality 13.29* 2.03 * Physician 24.11* 2.82 * Nurse 6.82 0.87 * Technician -176.27* -5.94 * Staff 18.22 1.36 DEMOGRAPHICS Age (> 53 Contrast) Less than 40 -1.33 -0.45 0.59 0.21 40 to 48 -1.84 -0.64 1.19 0.43 48 to 53 -0.66 -0.22 0.54 0.19 Female (Male Contrast) 4.17 1.41 4.90 1.73 CLINIC (CLINIC A CONTRAST) Clinic B -11.76* -2.48 -13.21* -2.80 Clinic C -6.63 -1.58 -7.51 -1.78 Clinic D -15.31* -3.90 -18.51* -4.90 Intercept -5.32 -0.89 -4.74 -0.55 Sigma 8.38* 10.56 7.37* 10.51 †Estimated using SAS Proc QLIM Tobit Implementation. Dependent variable is the sum of the number of times an individual is mentioned as providing or receiving information. N = 88. * - p < .05.
![Introduction: Curating Feeling - COnnecting REpositories · 2017-11-06 · Introduction: Curating Feeling Victoria Mills I am [. . .] wholey unable to surport myself and child and](https://img.pdfslide.us/doc/110x75/5edb927aad6a402d6665db54/introduction-curating-feeling-connecting-repositories-2017-11-06-introduction.jpg)