Embed Size (px)
Citation preview
ICP/HST/002
REGIONAL WORKSHOP ON
NATIONAL HEALTH INFORMATION SYSTEMS
Sponsored by the
WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR THE WESTERN PACIFIC
Kuala Lumpur, Malaysia 16-25 June 1980
REPORT
Not for Sale
Printed and Distributed
by the
Regional Office for the Western Pacific of the World Health Organization
Manila, Philippines October 1980
WHO/WPRO LlJ3RARY MANILA.I'IlTLlPPINES
1 0 JU ~l 2005
NOTE
The views expressed in this report are those of the consultant and participants in the workshop and do not necessarily reflect the policy of the World Health Organization.
CONTENTS
SUMMARY AND CONCLUSIONS vii
1. BACKGROUND AND OBJECTIVES 1
2. PRESENT STATUS OF HEALTH INFORMATION SYSTEMS IN THE REGION 3
2.1 Introduction ••••••••••••••••••••••••••••••••••..• 3 2.2 Present NHIS organization •••••••••••••••••••••••• 3 2.3 NHIS problems .•.•••••••.•••••••••••••••••••••••.• 4 2.4 NHIS development •• • • • • • • • . . • • • . . . . • . • • • • • • • • • • • • • 5 2.5 Summary and conclusions •••••••••••••••••••••••••• 5
3. HEALTH MANAGEMENT INFORMATION SYSTEMS (HMIS) -DEFINITION, BOUNDARIES, OBJECTIVES AND FUNCTIONS 5
3.1 3.2 3.3 3.4
Definitions Boundaries or scope of HMIS •••••••••••••••••••.•• Ob je ct i ves of HMIS •••••••••••••.••••••••••••••••• Functions of HMIS ...•.•••••••••••••••••••••••••••
5 6 7 7
4. HEALTH MANAGEMENT INFORMATION AND ITS RELATIONSHIP
5.
6.
TO THE HEALTH SYSTEM • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • . • • 8
4.1 4.2 4.3 4.4 4.5 4.6
Bas ic categor ies ••••••••••.••••••..•.•••.••.•...•• Population characteristics ••••••••••••••••..••.•.• Heal th status •••.••••.•••••••••••.••••••••••.••.•• Heal th resources . ,. ....... ,. ,. ........... ,. . ,. .. ,. ,. ,. ... ,. Health services utilization Summary and conclusions
SOURCES AND PRODUCERS OF HEALTH INFORMATION
5.1 5.2 5.3 5.4 5.5
Classification Rou tine sources ........ ,. ,. .. ,. ... ,. .. ,. . ,. ,. ...... ,. ,. . ,. . ,. Special and non-routine sources •••••••••••••...•.• Library and literature sources •••••••.•••••••..••• Summary and conc 1 us ions ••••.••••••••••••••••••••••
DECISION-MAKERS AND MANAGEMENT IN THE HEALTH SYSTEM
8 8 8
11 11 12
12
12 12 13 13 13
13
6.1 Data, information and decision-making ••.•.••••..•• 13 6.2 Decision-makers in the health system •.•••••••••••• 14 6.3 Types and levels of decision-making ••••••••••••••• 16 6.4 Summary and conclusions ........................... 18
7. BRIDGING THE GAP BETWEEN PRODUCERS AND USERS 19
7.1 The problem restated •...•••••••••••••••••••••••••• 19 7.2 A coordinating focus for HMIS •••••.••••••.•.•••••• 19 7.3 Options for a coordinating focus •••••••••••••••••• 19 7.4 Summary and conclusions •••••••••••••••••.•.....•.• 21
./
- 11 -
8. A FRAMEWORK FOR HMIS DEVELOPMENT
8.1 A programme approach •••••..••....••••••••.•••••••• 8.2 Advantages and disadvantages ..•.•.••.•.•...••....• 8.3 Priorities for service development •.••.••..••..... 8.4 Summary and conc 1 us ions •••.•.••.................••
9. THE PLACE OF INDICATORS IN HMIS
10.
9.1 Definitions and description ••••••••••••.•••••••... 9.2 Use of indicators •..•..••.•..•......•.•...••••••.• 9.3 Types of indicators .•.••......•..•.••••........... 9.4 Decision making and indicators .•.................. 9.5 Previous reports
STATISTICAL SUPPORT SERVICES
10.1 Function of statistical services •.••••••••••••... 10.2 Sources of statistical support .•••.•..•••••••.... 10.3 Training .••......••••••••••••.••••.•••••..•......
11. TECHNOLOGICAL SUPPORT SERVICES
12.
13.
14.
11.1 Definition and functions 11.2 Organization of information .•....••.....•••.•.... 11. 3 Types of technological support .••.••...•...•..... 11.4 Using computers in HMIS .•.....................••.
HMIS FOR PRIMARY HEALTH CARE
12.1 Importance of primary health care •............... 12.2 Information requirements for primary health care 12.3 Lay reporting •••••••••••••••••.•.••.............. 12.4 Primary health care and health for all •••••••••••. 12.5 Summary and conclusions ..•....••..•..••••••••••••
ORGANIZATIONAL DEVELOPMENT OF HMIS
13 .1 13.2 13.3 13.4
The need for organization of HMIS •••.•.••.•••...• A coordinating committee or group .••••••••.••.•.• Decentralized HMIS ••••••••••••.••••..••.......... Summary and conclusions
THE MALAYSIAN EXPERIENCE OF HMIS DEVELOPMENT
14.1 14.2 14.3 14.4
Background Development Test-run •.••.••..••••.•••••••••••••.••••.•••..•.• Important lessons which might be learned •.•.••••.
Pag,=
21
21 21 23 23
23
23 23 25 25 25
25
29 29 30
30
30 30 31 31
32
32 32 33 33 35
35
35 35 36 36
36
36 ,.
37 37 37
- iii -
15. CONDITIONS TO IMPLEMENT HMIS DEVELOPMENT AT COUNTRY LEVEL • • • • • • • • • • • • • • • • • . • . • • • • • . . • • • • • • • • . • • • 40
15.1
15.2 15.3 15.4 15.5 15.6 15.7 15.8 15.9 15.10 15.11 15.12
TABLE 1
Securing support of top management and policy-makers ••••••••.••.••••••••••••••••••••••• Strengthening national capabilities for HMIS Management development •••••••••••••••••••••••••• Organizational framework ..•••.••.••.•••••••.•••• Identification of user requirements •••••.••.•••• Coordination Des ign of HMIS Test-run ......................................................... .. Implementation .................................................................. .. Use of information ............................ .. Suggested steps •••••••••••••••••••••••.••••••••• Role of international agencies ••••••••••••••••••
LIST OF TABLES
CATEGORIES OF HEALTH MANAGEMENT INFORMATION: ILLUSTRATIVE INDICATORS AND SOURCES OF INFORMATION
TABLE 2 EXAMPLE OF DECISION LEVELS, DECISION AREAS AND ASSOCIATED INFORMATION NEEDS - HEALTH S ERVI CE S PROGRAMME • • • • • • • • • • • • • • • • • • • . . • • • . • • • •
TABLE 3 - EXAMPLE OF POSSIBLE STRATEGY FOR DEVELOPMENT
FIGURE 1
FIGURE 2
FIGURE 3
OF llMIS ................................................................................ ..
LIST OF FIGURES
GENERALIZED SYSTEMS MODEL OF THE VARIABLES AFFECTING THE SUPPLY, DISTRIBUTION AND UTILIZATION OF HEALTH SERVICES AND THE RELATIONSHIPS BETWEEN THEM •••••••..•..•••••••
SYSTEMS MODEL OF INFORMATION AND KNOWLEDGE AS INPUTS TO THE DECISION-MAKING PROCESS
POLICY PLANNING, MANAGEMENT CONTROL AND OPERATIONAL CONTROL AS MANAGEMENT FUNCTIONS IN RELATION TO HIGH, MIDDLE AND LOW LEVELS OF MAN'AGEMEN'T .................................................................... ..
40 41 41 41 41 42 42 42 42 43 43 43
9
26
45
10
15
17
- iv -
FIGURE 4 - SYSTEMS MODEL OF THE RELATIONSHIP BETWEEN SOURCES AND PRODUCERS OF INFORMATION; THE COORDINATING AND DEVELOPMENT FOCUS OF HMIS AND THE DECISION-MAKING PROCESS .•••••••••••••••••• 20
FIGURE 5 SYSTEMS MODEL OF A FRAMEWORK FOR HMIS BASED UPON-THE INTERRELATIONSHIPS BETWEEN PHC AND OTHER-SERVICES/PROGRAMMES ••••••••••••••••••••• 22
FIGURE 6 - DECISIONS, DECISION CENTRES AND INFORMATION NEEDS . • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • . • • 28
FIGURE 7 THE RELATIONSHIP BETWEEN THE DEMANDS OF HIGH COST HOSPITAL BASED CARE AND THE NEEDS OF THE WHOLE POPULATION FOR BASIC PRIMARY HEALTH CARE SERVICES • •• • • • • • • • • • • • • • • • • • • • • • • • • • • • • •• 34
FIGURE 8 - STRATEGIC STEPS IN DEVELOPMENT OF HEALTH
FIGURE 9
MANAGEMENT INFORMATION SYSTEM ................. TECHNICAL STEPS IN DEVELOPMENT OF HEALTH MANAGEMENT INFORMATION SYSTEM •••••••••••••••••
LIST OF ANNEXES
ANNEX 1.1 - OPENING ADDRESS BY DR L.R.L. VERSTUYFT, WHO PROGRAMME COORDINATOR, MALAYSIA, ON BEHALF OF THE REGIONAL DIRECTOR, WHO REGIONAL
38
39
OFFICE FOR THE WESTERN PACIFIC •••••••••••••••• 47
ANNEX 1.2 - CLOSING ADDRESS BY DR L.R.L. VERSTUYFT, WHO PROGRAMME COORDINATOR, MALAYSIA, ON BEHALF OF THE REGIONAL DIRECTOR, WHO REGIONAL OFFICE FOR THE WESTERN PACIFIC •.••••••••••••••••••••• 51
ANNEX 2.1 - OPENING ADDRESS BY Y.B. TAN SRI CHONG HON NYAN MINISTER OF HEALTH, MALAYSIA •••••••••••••••••• 53
ANNEX 2.2 - CLOSING ADDRESS BY
ANNEX 3
ANNEX 4
ANNEX 5
ANNEX 6
TAN SRI DATUK PROFESSOR R.P. PILLAY, DIRECTOR-GENERAL OF HEALTH, MALAYiIA ••...••••• 57
LIST OF PARTICIPANTS, OBSERVERS, TEMPORARY ADVISER, CONSULTANT AND SECRETARIAT •••••••••••
FINAL AGENDA AND LIST OF DOCUMENTS
BIBLIOGRAPHY • 10 ••••••••••••••••••••••••••••••••
SUMMARY OF EVALUATION ON THE REGIONAL WORKSHOP ON NATIONAL HEALTH INFORMATION SYSTEMS; Kuala Lumpur, Malaysia, 16-25 June 1980 •••••••
59
65
69
91
ANNEX 7
ANNEX 8
ANNEX 9
ANNEX 10
- v/vi -
QUESTIONNAIRE ON NATIONAL HEALTH INFORMATION SYSTEMS • . . . . . . . . . . • . • • • . • • • . . . . . . . • . . • • • • • . . • 113
- REPORT OF THE INTERREGIONAL CONSULTATION ON NATIONAL HEALTH INFORMATION SYSTEMS, San Jose, Costa Rica, 14-20 November 1979 119
CONCEPTUAL PHASE, HEALTH MANAGEMENT INFORMATION SYSTEM DEVELOPMENT PROJECT, MALAYSIA • . • • . . • . • 141
- TEST RUN STRATEGY AND ACTIVITIES 179
II I I
, i
- vii -
SUMMARY AND CONCLUSIONS
1. Health management information system (HMIS) development
(1) There are important national health information systems (NHIS) problems in all countries, especially the gap between producers and users of information. However, the situation in many countries seems favourable for NHIS development.
(2) A health management information system is that subsystem of NHIS which provides information to support the management process. Its objectives are to identify information sources and to link these to the specific requirements of management.
(3) Health management information may be categorized into population, health status, health resources and health services utilization. Understanding the relationship of these variables to sound health system management is fundamental to HMIS development.
(4) Traditional sources of health information tend to lack specificity for management purposes. They lack coordination and are isolated from decision-makers.
(5) Decision-making in management of the health system is complex in that it involves politicians, administrators, health professionals and the community. Appropriate information is required for all groups and at all levels. Developed countries tend to be weak on policy and planning while in developing countries, operational control is a critical weakness. These contrasting problems present important challenges to HMIS development.
(6) In order to bridge the gap between information producers and decision-makers, a coordinating focus is required which may be provided by a unit of a health ministry.
(7) Indicators have an important place in HMIS development. Indicators must be identified which are programme and user specific.
(8) Statistical services are an integral part of HMIS. Such services offer support with data collection, analysis and interpretation and must satisfy user requirements.
(9) A wide variety of technological support services are now available for HMIS development. Cost-effectiveness criteria and clearly defined output requirements should be critically applied to any decision to move into computerization of HMIS.
(10) Primary health care is an important and critical priority area for health services and hence for HMIS development.
(11) It is essential to have a "nerve centre" for HMIS development which is an integral part of a ministry. This centre should be under the control of a top-level committee of the Ministry.
- viii -
(12) The Malaysian experience of HMIS development suggests that toplevel and prolonged careful planning of HMIS with a test run in a selected area are essential steps prior to wider implementation.
2. International support for health management information syst~m development
The workshop concluded that, for the development of HMIS in many countries, the support of international agencies, particularly WHO, would be desirable and necessary in one or more of the following ways:
(1) technical support with the design of systems, standardization of statistical and other procedures, and advice on technological developments;
(2) information on intercountry developments, technical literature and availability of support services;
(3) consultant services on an intercountry basis;
(4) training of staff through intercountry semtnars and workshops, study visits and fellowships;
(5) promotion of health information systems through the developm~nt of regional and global policies;
(6) financial support to promote research and development programmes tn HMIS within countries.
1
1. BACKGROUND AND OBJECTIVES
Present trends and developments have underlined the increasing importance of national health information systems (NHIS). These include:
the need to relate health services more closely to the overall health problems of the community;
the need to find solutions to the organizational problems of escalating health costs, inefficiencies, inequalities, lack of coordination and accountability;
the growing awareness of the need for better management of health services;
increased demands for information from many sources;
the recognition of the importance of primary health care;
international commitment to the goal of health for all by the year 2000 and the need to express this goal and monitoring achievement of progress towards achievement of this goal in measurable terms.
World Health Assembly resolution WHA 31.20 urged the Member States to develop or strengthen their health information systems and requested the Director-General to develop principles for national health information system (NHIS) in close collaboration with Member States. Through resolution WHA 31.43, the World Health Assembly also stressed the need for a unified managerial process for national health development, including provision of adequate information support to the process as a whole and to each of its component parts. As a follow-up of these WHA resolutions, WHO embarked upon a programme of intercountry and interregional consultation and held regional meetings in New Delhi in December 1978, Washington in February 1979, and an interregional consultation meeting in San Jose, Costa Rica, in November 1979.
In the Western Pacific Region of the World Health Organization, the development and further improvement of health information systems to support planning and management of health programmes and subprogrammes has been a priority area for collaboration with Member States, particularly since 1976 when collaborative activities were undertaken with the Government of Malaysia to develop a dynamic, integrated and user-oriented health management information system for the Ministry of Health.
- 2 -
Associated events were the Regional Seminar on Indicators Relevant to Maternal and Child Health, held in Manila, Philippines, from 13 to 19 December 1978l/ and the Sixth SEAMIC Workshop on the Development of Operational, Performance and Impact Indicators with Special Reference to Community Health, held in Kuala Lumpur, Malaysia, from 13 to 19 February 1979~/.
As a part of these development activities, a regional workshop on National Health Information Systems was scheduled to be held in Kuala Lumpur, Malaysia from 16 to 25 June 1980 with participants from countries/areas in the Western Pacific Region of WHO.
The objectives of the workshop were;
(1) to exchange views and information on the present status of the health information systems in countries in the WHO Western Pacific Region;
(2) to identify problems related to existing health information systems supporting the planning, management and evaluation functions of ministries/departments of health;
(3) to establish a framework for a national health information system to serve managerial functions and to explore alternative strategies for its development;
(4) to consider the role of international agencies 1n the promotion and development of national health information systems.
The Workshop was formally opened on 16 June 1980 by the Honourable Minister of Health of the Government of Malaysia, Tan Sri Chong Hon Nyan. Annexes 1.1 and 1.2 give respectively the opening and closing addresses of Dr H. Nakajima, Regional Director of WHO Regional Office for the Western Pacific. Annexes 2.1 and 2.2 give respectively the opening address of the Honourable Minister of Health and closing address of the Director-General of Health, Malaysia.
There were in all 20 part1c1pants from 18 countries/areas of the Western Pacific Region of WHO (Annex 3). Participants included health managers and planners, statisticians, epidemiologists, and technicians. They represented a wide spectrum of involvement in health information systems from the perspective of both users and producers. Annex 4 gives the Final Agenda and List of Documents distributed to the participants. Annex 5 gives the Bibliography and Annex 6 gives a report on the evaluation of the workshop carried out by WHO.
The present report summarizes the background papers, results of the workshop discussions, and group consultations.
l/Document No. WPR/HST/80.14, Final Report of the Regional Seminar on Indicators Relevant to Maternal and Child Health, held in Manila, Philippines, from ]3-19 December 1978.
~/Document No. WPR/HST/80.15, Proceedings of the 6th SEAMIC Workshop -The Development of operational, performance and impact indicators with special reference to community health, South East Asian Medical Information Center, Tokyo, 1979.
- 3 -
It is hoped that its publication will lead, not only to a wider understanding of the theoretical and practical aspects of developing a health information system, but also to appropriate action in implementing some of the proposals in country situations.
2.1 Introduction
2. PRESENT STATUS OF HEALTH INFORMATION SYSTEMS IN THE REGION
In preparation for the workshop, a structured questionnaire was sent to all country participants seeking information on existing information systems, problems with such systems, and plans and procedures for review and development (see Annex 7). In addition to the questionnaire which was completed by 17 countries/areas, more detailed reports were provided by participants from a number of countries. These, together with the workshop discussions, provide the basis for this section of the workshop report.
2.2 Present NHIS organization
In all but one of the countries/areas, there is an identifiable organizational division/unit to provide data and information in support of planning and management of its health services. However, except for two countries where a single identifiable unit/division is responsible for health information service functions, others stated that there are two or more units/divisions/sections responsible for one or more components of the health information system!/. Since programmes function vertically, so do the health information services. In addition to some of the technical units responsible for programme areas and for planning, including research, and administration/management services, some institutions also provide health information services. The health information service as such appears to be structurally fragmented among different units/sections/ divisions of the ministry or department of health in some countries.
In all but one of the countries/areas, ministries and departments other than health also cater to the needs of the health system. Thus, ministries and departments dealing with census and statistics, education, labour, environment, family planning, central statistics system, and national planning and development analyse health data relevant to their functions.
!/Information system refers to the methods, materials, media, producers and recipients involved in an organized way to effect information transfer within a specific field, activity or organization and hence consists of a complex collection of information, persons who produce and use them, institutions which process them and a set of behaviour patterns, customs and traditions by which these persons and institutions interrelate.
Information service is a service for the regular and ad hoc provision of information. This may take the form of dissemination o~information or information transfer, including a query/answer service. An information service must be backed by at least one information system, and an information system may back several information services.
- 4 -
2.3 NHIS problems
Problems associated with data collection, analysis and utilization were identified both in country reports as well as in workshop discussions.
2.3.1 Data collection
There are many gaps in the collection of data, especially on finance and from the private sector. Delays occur in transmitting and collating data due to geographical constraints, organizational limitations and processing.
There is a lack of common definition in data collection with associated problems of validity and comparability. Motivation of health workers to accurately provide data is also a problem in spite of the judicious use of legislation to make collection mandatory. In some countries, reliance upon legislation alone is found to be ineffective but some believe it valuable to legitimate requests for data.
Data collection is not always coordinated. As a consequence there lS
duplication and redundancy. Requests for data often arise in an ad hoc way. Together these lead to excessive demands for data. The lac~o~ statistical coordinating agency is seen as a basic problem in the way of coordinating data collection.
2.3.2 Problems of analysis
Reliance on manual processing limits the potential for analysis. On the other hand, in some countries introduction of automatic data processing systems has created problems. Information is not always classified in a way which permits analysis in relation to health policy objectives. An example is the need to identify expenditure on urban and rural health services, when it is policy to increase spending in rural areas. Health indicators need to be developed for analysis of such information.
2.3.3 Problems of utilization
There was a general acceptance that a serious problem is a lack of utilization of available information. This is due to a lack of awareness of the value of information by managers and others involved in decision making. Available information tends to be unrelated to priorities of managers. There is a lack of coordination of information requirements. Information on services and programmes is often unrelated to financial information.
2.3.4 General problems
There are also some general problems. Lack of trained staff is a very common problem in all aspects of information systems. Another problem is resources devoted to research which does not address high priority health problems or result in information useful for management.
- 5 -
2.4 NHIS development
In seven countries/areas, activities have been initiated to further develop health information systems/services, such as computerized hospital discharge/vital statistics information system, standard health statistics system, health reporting system, use of computer technology to strengthen the health information system, private sector service information, manpower information, centralized management information system development. Since the technical support information component of NHIS contributes to the establishment of an information base for planning and management, it seems that the major area for development has been the management informatio~ system. Ministries and departments of health themselves have been responsible for initiating development activities in this area though the actual scope of these activities covers specific components only. It seems that different units/divisions take the initiative in developing an information system to cater for their programme requirements.
2.5 Summary and conclusions
There are NHIS problems in all countries relating to data collection, processing and utilization. There is an important gap between available and needed information on the one hand and available and used information on the other.
In some countries, national vital and health statistics committees exist. Through feedback mechanisms problems are being identified and efforts being made to solve these problems. However, these efforts are isolated and uncoordinated and lead to duplication and inefficiency.
An environment favourable to the development of a more comprehensive health information system is present in many countries. Time seems to be ripe to initiate more systematic approaches to the provision of information to programme development and management.
3.1 Definitions
3. HEALTH MANAGEMENT INFORMATION SYSTEMS (HMIS) - DEFINITION, BOUNDARIES,
OBJECTIVES AND FUNCTIONS
The workshop took as its starting point the Costa Rica Consultation definition of a National Health Information System (NHIS):
"A National Health Information System is a family of mechanisms and procedures primarily intended to acquire, analyse and provide within a country the information required (a) by all levels of health planners and managers for the planning, programming, budgeting, monitoring, control, evaluation and coordination of national health programmes, and (b) by other members of the health professions - specifically health care personnel (for example, medical and public health personnel, sanitary engineers, dental workers, pharmacists, and auxiliary personnel of all categories), health
- 6 -
research workers, and educators and trainers of health personnel - each in support of their respective roles in the national health programme. The system also provides specific health information to users outside the health sector, particularly national policy-makers, socioeconomic planner!! and the general public. ,,1
NHIS is thus seen as being inclusive of all health-related information required by both "health planners and managers" as well as "other members of the health professions". A third group is also identified - "users outside the health sector particularly national policy makers, socioeconomic planners and the general public". The full report of the Costa Rica Consultation Meeting is given as Annex 8.
That part of NHIS which provides information to support process is the health management information system (HMIS). subsystem of NHIS.
the management HMIS is thus a
3.2 Boundaries or scope of HMIS
The boundaries or scope of HMIS embrace information to be used in the management process associated with health programmes and services. The management process involves the control of health systems and subsystems. The process includes:
Planning:
Budgeting:
Monitoring:
Control:
Coordination:
Evaluation:
Planning and policy-making requires information about population, disease, service actIvIty, finance, training and manpower, facilities and supplies.
Budgeting requires information about the resource implications of policies, plans and programmes over a specified time period.
Monitoring requires information about progress and activity.
Control requires information to assess the current situation so that corrective action can be taken, if necessary.
Coordination requires reports about the actlvitles of associated agencies and reports to other agencies about health service activities.
Evaluation requires information to compare plans with achievements.
HMIS provides information to operational management, including information about the use of resources and logistics, as well as for central planning and policy making. HMIS should allow and promote the use of information by health care workers in the field (e.g. rural health clinics) to manage their own operational units.
lWorld Health Organization (1980). Report of the Interregional Consultation Meeting on NHIS, Costa Rica, 14-20 November 1979, Geneva (World Health Organization, NHIS/IR/80.l), p. 3.
- 7 -
HMIS does not include technical, professional or clinical information used by health care workers in the care of individual patients. Information about bio-medical research and related scientific literature is also excluded as is information specifically for education and training or public education. Technical and educational information are considered separate specialist components of NHIS.
Because of practical difficulties, health-related information collected by other government departments and information about private hospitals or private practitioners may be difficult to include in HMIS. Conceptually however all information relevant to management should be included in HMIS.
3.3 Objectives of HMIS
Having regard to problems, boundaries and relationships to the management process, the workshop identified the following objectives of HMIS.
To support management - planning, programming, budgeting, monitoring, control, coordination and evaluation - of the health system at all levels, by;
(a) identifying and coordinating all sources of information relevant to the management process and establishing links with other health-related information sources;
(b) efficiently acquiring, processing (including storage and retrieval) analysing and timely provision of relevant information;
(c) promoting training in all aspects of management information system development, especially utilization;
(d) working with management to identify changing requirements for health information;
(e) contributing to the development of NHIS.
3.4 Functions of HMIS
In order to achieve the above objectives, a wide range of functions and strategies are required which will be elaborated upon in subsequent sections. A brief list of the functions of HMIS is as follows:
identification of the information needs of management;
identification of all relevant sources of information and establishment of collaborative links between sources;
definition of data sources and setting up mechanisms for acquisition, processing, analysis, storage, retrieval and presentation of information to management;
training resource personnel to operate within HMIS and assist in the training of management in utilization of information.
- 8 -
4. HEALTH MANAGEMENT INFORMATION AND ITS RELATIONSHIP TO THE HEALTH SYSTEM
4.1 Basic categories
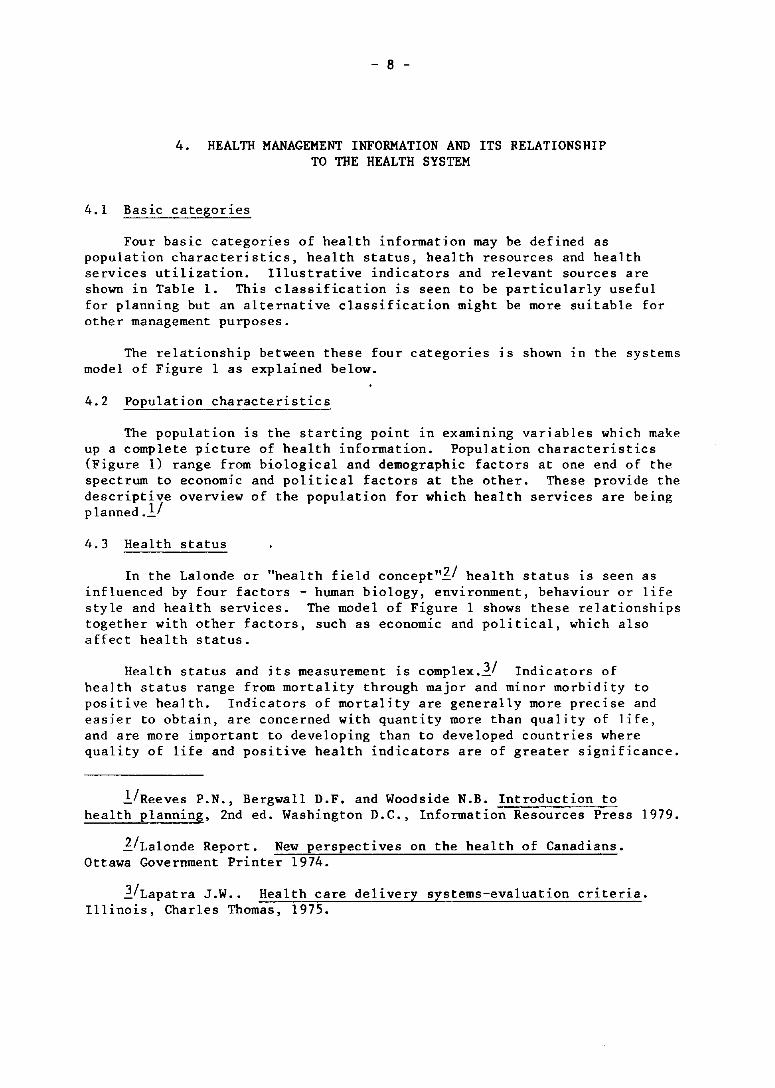
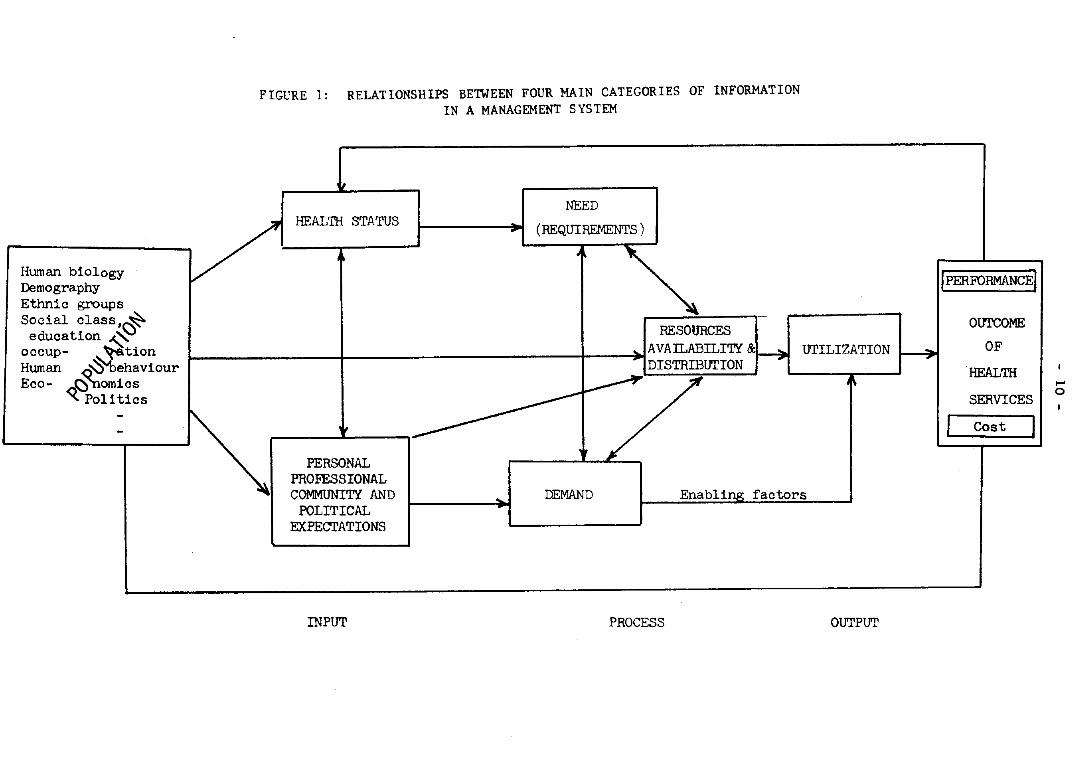
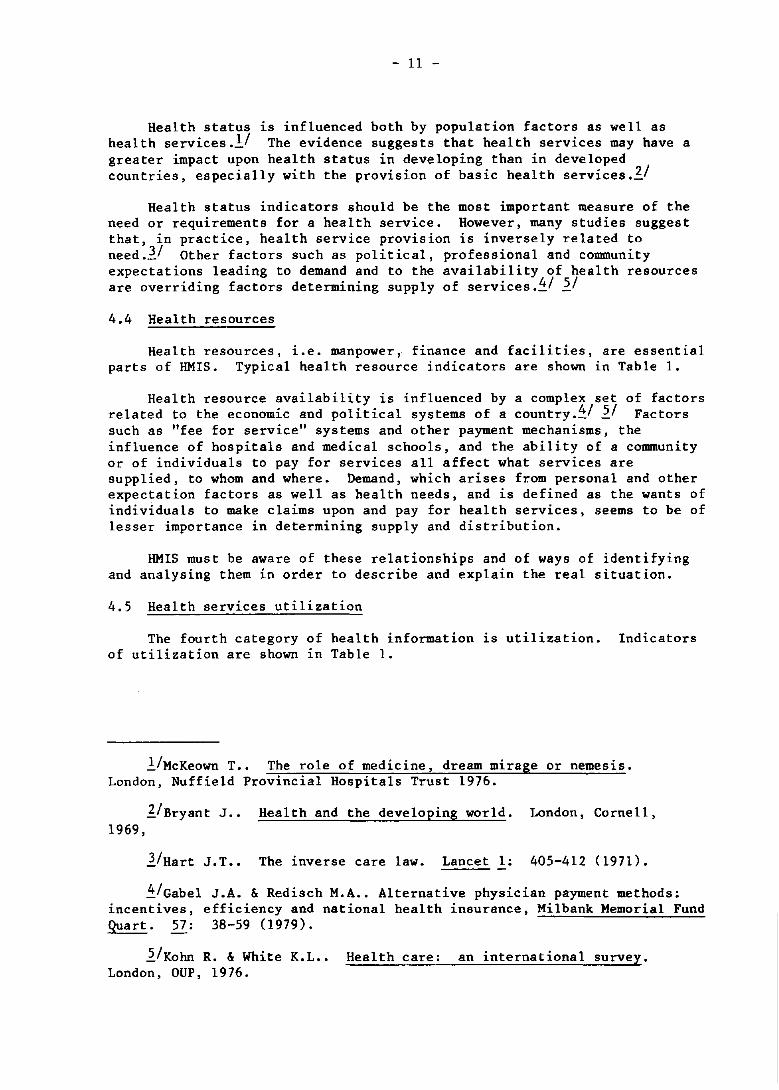
Four basic categories of health information may be defined as population characteristics, health status, health resources and health services utilization. Illustrative indicators and relevant sources are shown in Table 1. This classification is seen to be particularly useful for planning but an alternative classification might be more suitable for other management purposes.
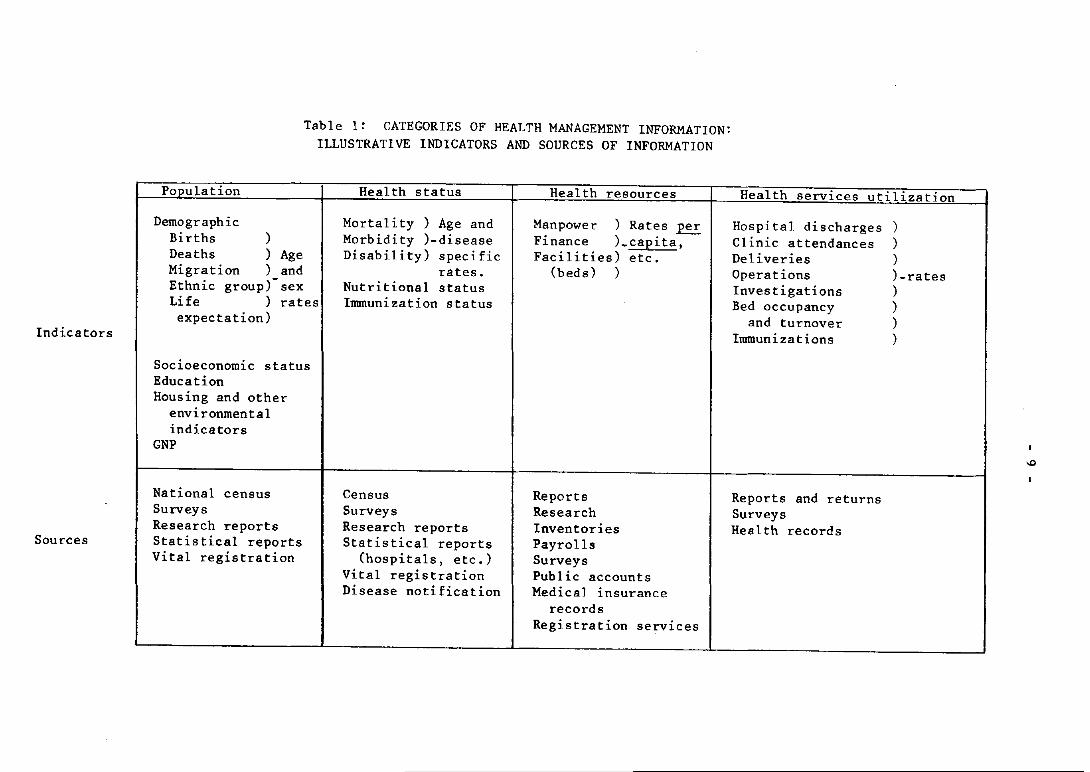
The relationship between these four categories lS shown ln the systems model of Figure 1 as explained below.
4.2 Population characteristics
The population is the starting point In examining variables which make up a complete picture of health information. Population characteristics (Figure 1) range from biological and demographic factors at one end of the spectrum to economic and political factors at the other. These provide the descriptive overview of the population for which health services are being planned.Y
4.3 Health status
In the Lalonde or "health field concept"ll health status is seen as influenced by four factors - human biology, environment, behaviour or life style and health services. The model of Figure 1 shows these relationships together with other factors, such as economic and political, which also affect health status.
Health status and its measurement is complex.ll Indicators of health status range from mortality through major and minor morbidity to positive health. Indicators of mortality are generally more precise and easier to obtain, are concerned with quantity more than quality of life, and are more important to developing than to developed countries where quality of life and positive health indicators are of greater significance.
l/Reeves P.N., Bergwall D.F. and Woodside N.B. Introduction to health planning, 2nd ed. Washington D.C., Information Resources Press 1979.
l/Lalonde Report. New perspectives on the health of Canadians. Ottawa Government Printer 1974.
l/Lapatra J.W •• Health care delivery systems-evaluation criteria. Illinois, Charles Thomas, 1975.
Indicators
Sources
Table 1: CATEGORIES OF HEALTH MANAGEMENT INFORMATION: ILLUSTRATIVE INDICATORS AND SOURCES OF INFORMATION
P~ulation
) Demographic
Births Deaths ) Age Migration ) and Ethnic group) sex Life ) rates expectation)
Socioeconomic status Education Housing and other
environmental indicators
GNP
National census Surveys Research reports Statistical reports Vital registration
Health status
Mortality) Age and Morbidity )-disease Disability) specific
rates. Nutritional status Immunization status
Census Surveys Research reports Statistical reports
(hospitals. etc.) Vital registration Disease notification
Health resources
Manpower ) Rates per Finance )_capita. Facilities) etc.
(beds) )
Reports Research Inventories Payrolls Surveys Public accounts Medica) insurance
records Registration services
Health services utilization
Hospital discharges) Clinic attendances ) Deliveries Operations Investigations Bed occupancy
and turnover Immunizations
Reports and returns Surveys Health records
) )-rates ) ) ) )
>D
Human biology Demography Ethnic groups Social ClaSS.~
education ~ occup- ~tion Human ~'behaviour Eco- ~<::) arnics
Politics --
FIGVRE 1: RELATIONSHIPS BETWEEN FOUR MAIN CATEGORIES OF INFORMATION IN A MANAGEMENT SYSTEM
if
NEED
V HEALTH STATUS
(REQUIREMENTS)
~ RESOURCES
AVATI..ABILI'lY & .. DISTRIBUTION "7
~ ,---------PERSONAL
PROFESSIONAL
lJrILIZATION
1\
COMMUNI'lY AND . DEMAND Enabling factors POLITICAL
EXPECTATIONS , --
INPUT PROCESS OUTPUT
IPERFORMANCEI
OUTCOME
OF ~
HEALTH
SERVICES
I Cost I
,..... o
- 11 -
Health status is influenced both by population factors as well as health services.ll The evidence suggests that health services may have a greater impact upon health status in developing than in developed countries, especially with the provision of basic health services.~1
Health status indicators should be the most important measure of the need or requirements for a health service. However, many studies suggest that, in practice, health service provision is inversely related to need.ll Other factors such as political, professional and community expectations leading to demand and to the availability of health resources are overriding factors determining supply of services.~1 ~I
4.4 Health resources
Health resources, i.e. manpower,· finance and facilities, are essential parts of HMIS. Typical health resource indicators are shown in Table 1.
Health resource availability is influenced by a complex set of factors related to the economic and political systems of a country.~1 51 Factors such as "fee for service" systems and other payment mechanisms, the influence of hospitals and medical schools, and the ability of a community or of individuals to pay for services all affect what services are supplied, to whom and where. Demand, which arises from personal and other expectation factors as well as health needs, and is defined as the wants of individuals to make claims upon and pay for health services, seems to be of lesser importance in determining supply and distribution.
HMIS must be aware of these relationships and of ways of identifying and analysing them in order to describe and explain the real situation.
4.5 Health services utilization
The fourth category of health information is utilization. Indicators of utilization are shown 1n Table 1.
l/McKeown T.. The role of medicine, dream mirage or nemesis. London, Nuffield Provincial Hospitals Trust 1976.
~/Bryant J •• Health and the developing world. London, Cornell, 1969,
l/Hart J.T •• The inverse care law. Lancet I: 405-412 (1971).
~/Gabel J.A. & Redisch M.A •• Alternative physician payment methods: incentives, efficiency and national health insurance, Milbank Memorial Fund Quart. 57: 38-59 (1979).
~/Kohn R. & White K.L •• Health care: an international survey. London, OUP, 1976.
- 12 -
Factors already mentioned converge to influence supply which in turn is a most important determinant of utilization. Utilization is also influenced by enabling factors (price, time, distance, etc.).
Health service outputs have a feedback link to health status, while cost outputs produce feedback constraints through the various allocative and decision-making processes upon resource availability.
4.6 Summary and conclusions
Health management information may be usefully categorized into four groups: population, health status, health resources and health services utilization. These categories are made up of a wide range of information variables, which interact in various ways to influence the provision of health services and the functioning of the health system.
Such a categorization of those information variables and their relationships to sound management of the health system is an essential basis for the development of HMIS.
5. SOURCES AND PRODUCERS OF HEALTH INFORMATION
5.1 Classification
The previous section identified a number of sources of health information. These may be classified into routine producers, e.g. health and other statistical units, data processing programmes, inventories and reporting systems, and non-routine, e.g. research units, academic departments, special surveys and reports.
5.2 Routine sources
Most health departments/ministries/organizations maintain special statistical units, which receive and process routine information such as hospital discharges and general mortality, morbidity and service statistics, population statistics, financial and other resource information. Such units however tend to be isolated from and independent of the management process and their output, while providing general background information, tends to lack the specificity and timeliness required for many management decisions.
Electronic data processing has speeded up presentation but the problem of specificity remains, largely due to the failure of management to more precisely define its requirements.
This is also true of routine reports as information sources, which tend to continue to be produced long after they were first requested and their original purpose is lost sight of. Reports are often poorly coordinated and duplicated and not analysed or presented appropriately.
- 13 -
5.3 Special and non-routine sources
Much research carried out by special research units, either of departments/ministries or independent units, is unrelated to policy and management problems. This is also true of academic departments where the choice of research is determined more by the personal interest of the researcher than by its relevance to policy. Where policy research is undertaken, there are no mechanisms to introduce the results into the policy-making process. Health services research is still a relatively new concept lacking the skills, methodology and access which are essential if it is to make an effective contribution to the management process. Furthermore, the research process is often long drawn out and results are received too late to influence policy.
5.4 Library and literature sources
A further important source of health management information is health literature both in published form such as is found in libraries or unpublished reports of studies and surveys. These latter sources are often difficult to obtain or even find out about. Developing a coordinated literature and library service is another task for HMIS.
5.5 Summary and conclusions
In summary, therefore, traditional sources of health information tend to be isolated, to lack specificity and timeliness and to lack coordination and a general awareness of policy issues and management requirements. The key question facing HMIS development is "how can information sources be coordinated and linked to the management process?"
Before answering this question, however, it is necessary to examine the management process in the health system.
6. DECISION-MAKERS AND MANAGEMENT IN THE HEALTH SYSTEM
6.1 Data, information and decision-making
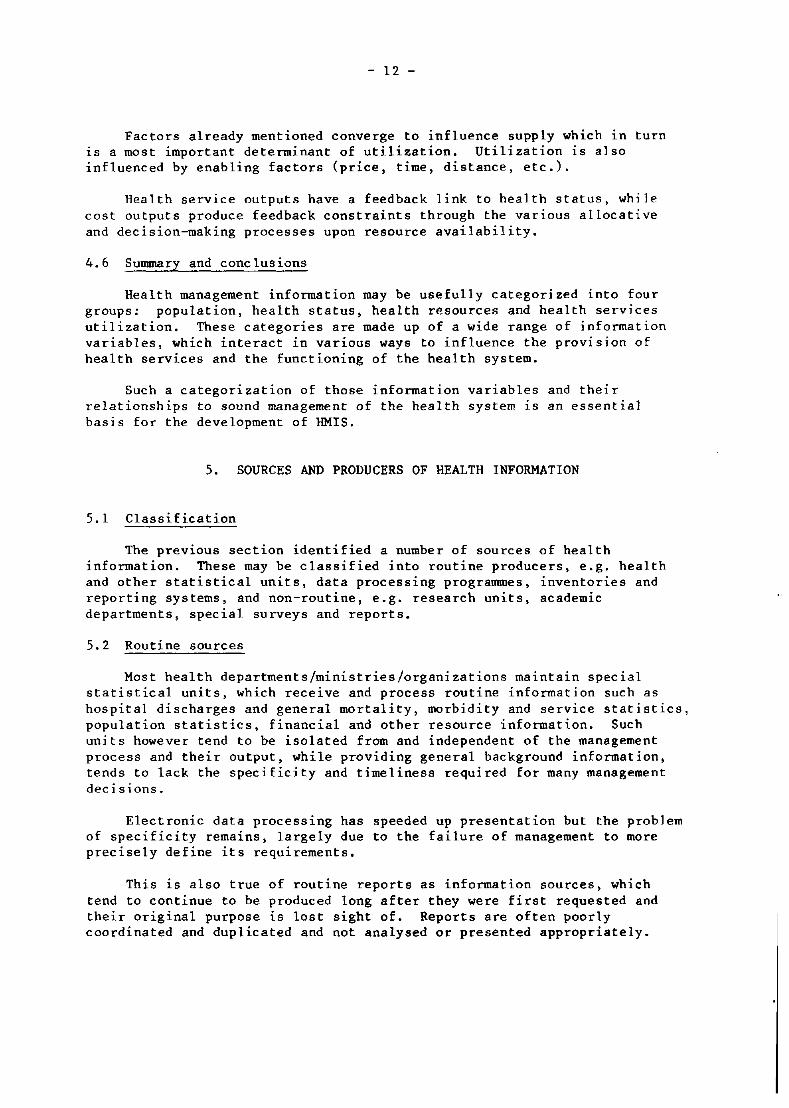
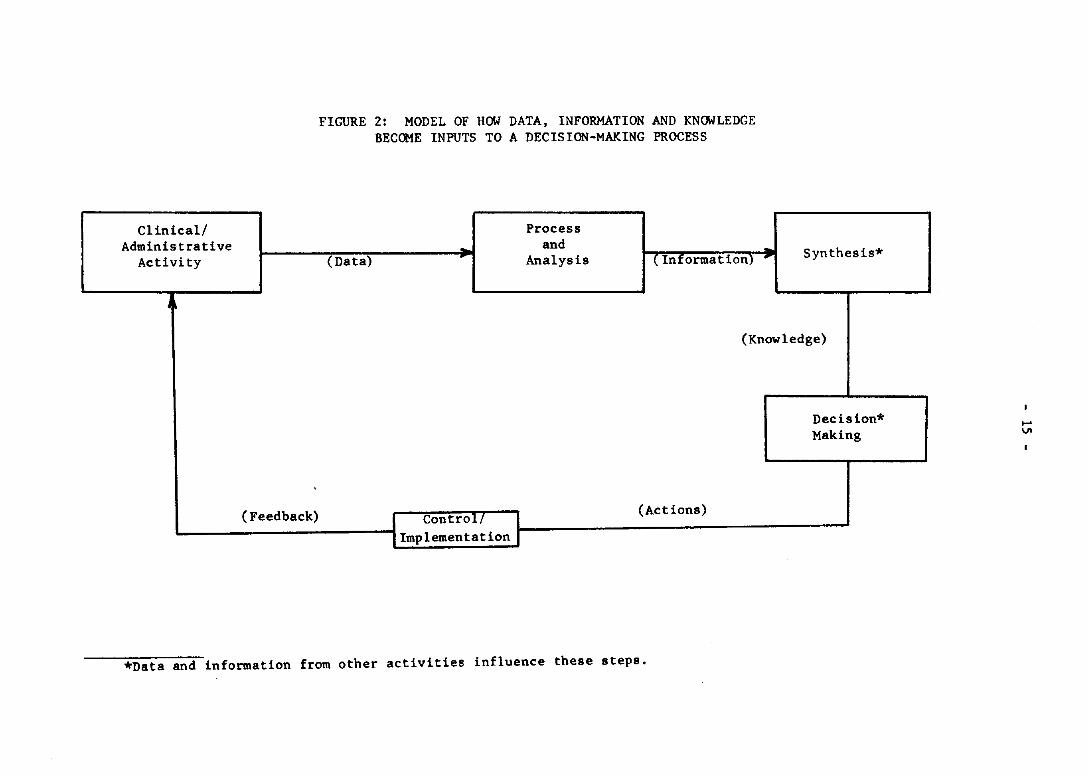
Data are the raw statements of fact derived from clinical and administrative activity and other sources. Data as an input are processed and analysed to produce the output information. This in turn, with relevant information from a variety of sources, is synthesized to produce knowledge.
Knowledge and information are inputs to the decision-making process, the output of which is decisions. Outcome of decisions in turn provide a feedback and control link to clinical and administrative activity completing the cycle of a systems model.
- 14 -
These interactions are shown in Figure 2. Information and knowledge are essential inputs to this decision-making process. Thus, in the design of an information system, the following sequence of questions must be asked;
What decisions are to be made and who should make them?
What information outputs are necessary in order to make such decisions and with what frequency?
What essential data inputs are required in order to provide such information and with what frequency?
Determining data inputs are the last in this sequence of questions.
6.2 Decision-makers in the health system
The management process in the health system is complex due to the variety of decision-makers involved and their differing interests and influences. These include the role of politicians, the influence of professionals, and the place of the consumer and the community. Other problems are the relative independence of the private and voluntary sector and the generally fragmented nature of the health system.
Top-level decision-making within the health system is political. Politicians are elected to represent community concerns but in making political or policy decisions are influenced by a wide range of interest groups. The quality of decision-making at this level will be enhanced by the provision of timely and relevant information which covers all aspects of the problem being considered.
Political decision-making closely interfaces with and overlaps administrative decision-making. The administrator has a particular role in structuring and supporting the management process at all levels, especially the political level.
Health professionals have an area of responsibility in influencing the management. This not only applies to their day-to-day decisions regarding patient management but also in their demands for resources and their influence over health policy. At the peripheral health centre level, health professionals have a direct management responsibility in addition to patient care.
Consumer and community decision-making is also important in the health system. Decisions to seek treatment and from what source, to comply with advice and treatment, and to behave in ways which critically affect health status all ultimately interact with and influence the management process in the health system. An important example is consumer behaviour in relation to hospital outpatients.
Clinical/ Administrative
Activity
,
FIGURE 2: MODEL OF HOW DATA, INFORMATION AND KNOWLEDGE BECOME INPUTS TO A DECISION-MAKING PROCESS
. (Data)
Process and
Analysis ( Information) , Synthesis*
(Knowledge)
Decision* Making
~ ______________________ -JI Control! I (Actions) . Implementation _~--------------------------------------~
(Feedback)
*Data and information from other activities influence these steps.
.... VI
- 16 -
Thus four levels of overlapping and interacting decision-making can be identified - political, administrative, health professional and consumer. This last directly influences political decision-making through the democratic process. HMIS is closely concerned with providing appropriate information to all aspects of this process which affects the management of the health system. These relationships are shown in Figure 3.
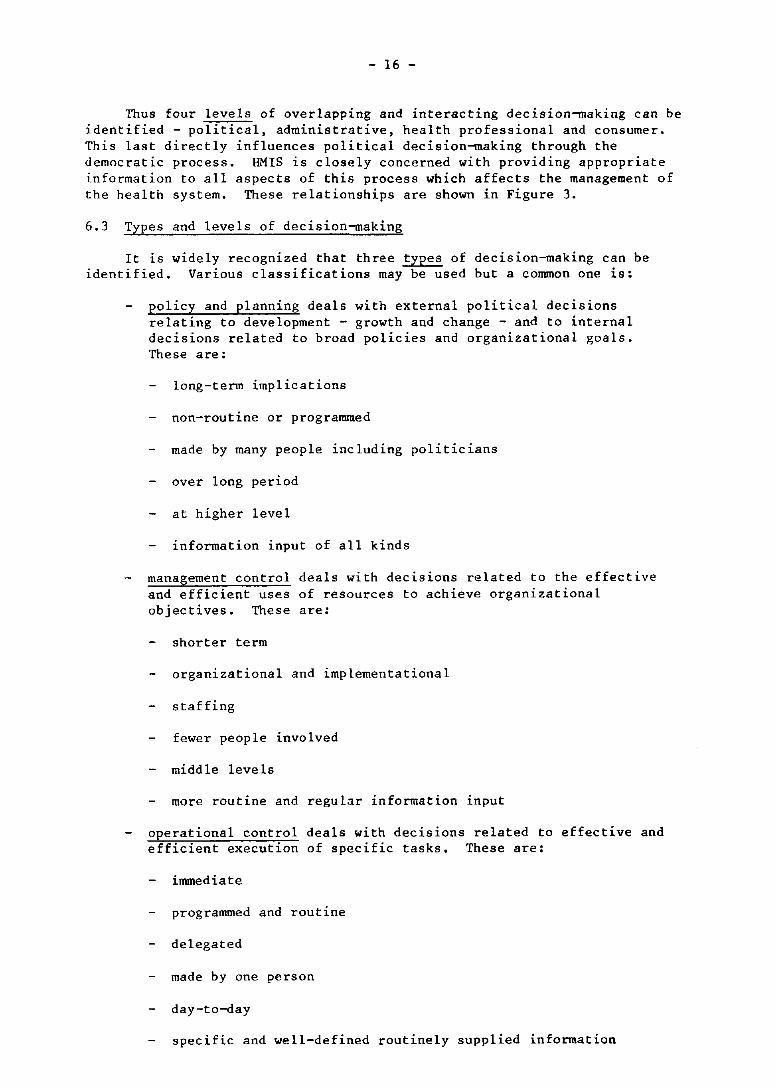
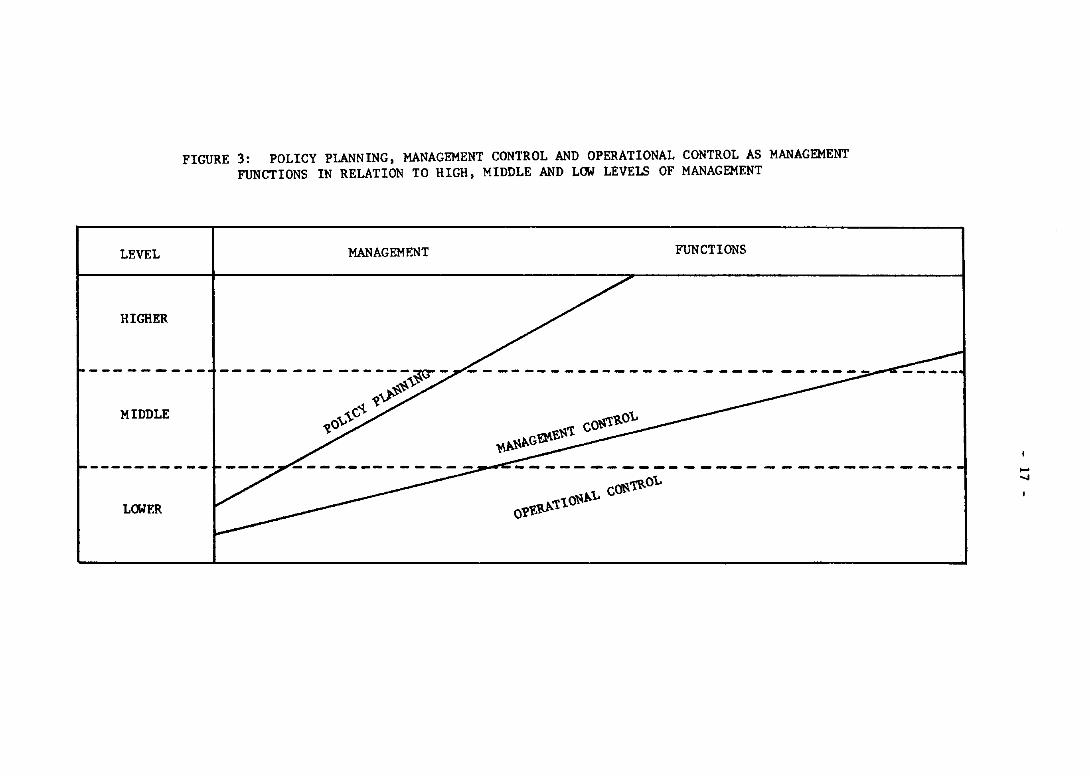
6.3 Types and levels of decision-making
It is widely recognized that three types of decision-making can be identified. Various classifications may be used but a common one is:
policy and planning deals with external political decisions relating to development - growth and change - and to internal decisions related to broad policies and organizational goals. These are:
long-term implications
non-routine or programmed
made by many people including politicians
over long period
at higher level
information input of all kinds
management control deals with decisions related to the effective and efficient uses of resources to achieve organizational objectives. These are:
shorter term
organizational and implementational
staffing
fewer people involved
middle levels
more routine and regular information input
operational control deals with decisions related to effective and efficient execution of specific tasks. These are:
immediate
programmed and routine
delegated
made by one person
day-to-day
specific and well-defined routinely supplied information
LEVEL
HIGHER
MIDDLE
LOWER
FIGURE 3: POLICY PLANNING, MANAGEMENT CONTROL AND OPERATIONAL CONTROL AS MANAGEMENT FUNCTIONS IN RELATION TO HIGH, MIDDLE AND LOW LEVELS OF MANAGEMENT
MANAGEMENT FUNCTIONS
¥)..l\t.G~f.l\'t COl\'!RO\"
~---------- ----- - ------------01'f.v..t.'t10l\t.\.. COll'tR°\"
...... .....
- 18 -
In general policy and planning, decisions are made at the higher levels of an organization while operational control is delegated to lower levels. However, there is some overlap as is shown in Figure 3. Higher levels of management are largely concerned (or should be) with policy and planning, to a lesser extent with management control, and only to a slight extent with day-to-day management. On the other hand, lower levels are largely operational.
In practice, however, there are important differences in health management from this model. Developed countries generally give a low priority to policy and planning, with top management tending to be heavily involved in routine control. By contrast, developing countries tend to be well-developed in policy and planning but are weaker in implementation and operational control. This latter problem is widely seen as the critical problem in management in developing country situations.
In HMIS development, therefore, policy and planning information is an important priority for developed countries while operational control information is critical for developing countries.
In a national health system, three or more levels of management may be defined - national, subnational (regional, district, province) and local or peripheral (health centre). Types of decision-making, decision-makers, and categories of information vary with different levels. At national level, policy and planning decisions, though largely political, are in need of information related to population, health status and health resources. At the peripheral level, operational control is exercised by the health professionals, taking into account the utilization pattern by the local community, and hence information related to resource distribution and health services utilization is of great importance.
6.4 Summary and conclusions
In designing HMIS, information required for decision-making at all echelons of the ministry/department of health should determine the essential data inputs.
The decision-making in the health system is complex in that it involves politicians, administrators, health professionals and the consumer and community. Appropriate information is required for all groups.
Management ranges from policy and planning to operational control. In general, this relates to the levels of decision-making within an organization. Developed countries, however, tend to be weak in decision-making in the areas of policy and planning. By contrast, this aspect is a strength in developing countries but operational control is a critical weakness. These contrasting problems present important challenges to HMIS development.
- 19 -
7. BRIDGING THE GAP BETWEEN INFORMATION PRODUCERS AND MANAGEMENT
7.1 The problem restated
The key problem facing HMIS identified throughout the preceding sections is how to bridge the gap between producers of information and those who should use it in decision-making. This section examines ways of building this bridge and achieving the objectives of HMIS as stated in section 3.3. In doing so, it proposes that HMIS must have a central coordinating focus if it is to achieve its objectives.
7.2 A coordinating focus for HMIS
A system may be defined as a set of elements or components with strong relationships between and among them and having an orientation towards an identifiable goal. HMIS may be viewed as such a system.
In summary, the objectives of HMIS were identified as being concerned with establishing coordination and communication between all sources of information and processing this into outputs relevant to management.
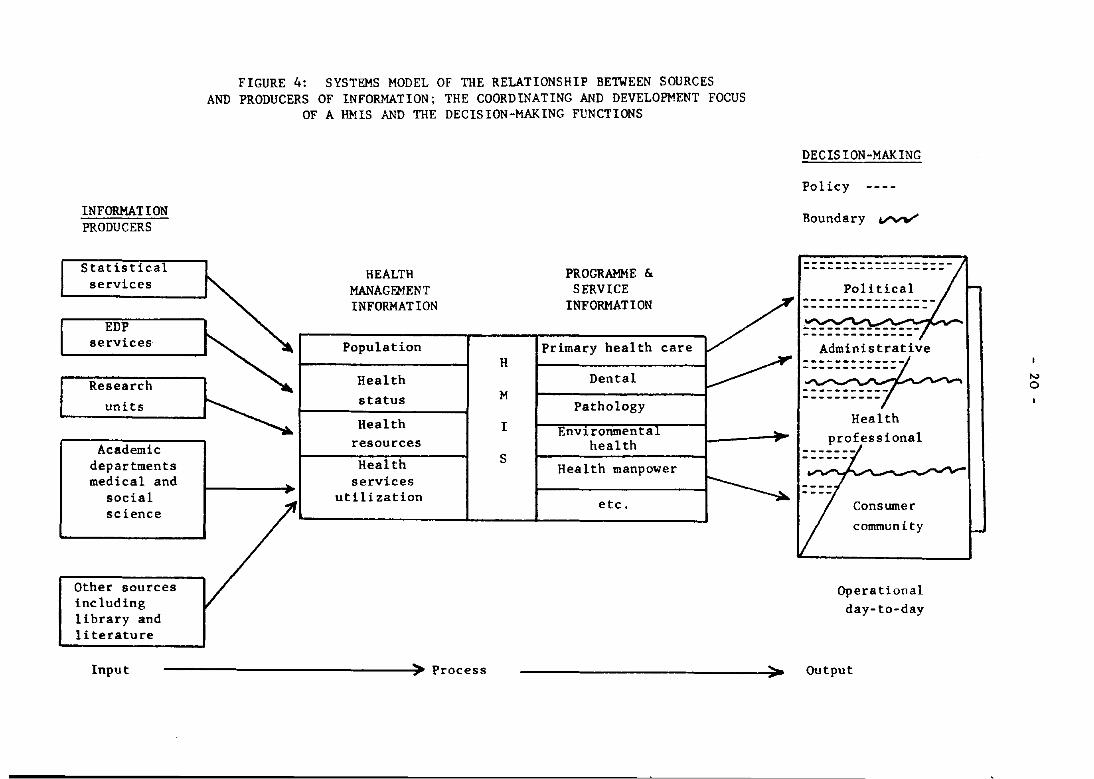
In order to achieve these objectives, it is necessary that HMIS must have a coordinating focus or responsibility centre, which identifies sources, develops indicators and other information, processes this into a programme or service framework, and presents this to decision-makers in the various levels which have been described. A systems model of these relationships is shown in Figure 4. This shows how a HMIS coordinating focus would receive health management information from different sources and process this within a programme or service framework as described in the next section and link it into various levels and types of decision-making. Thus, it would assist in the coordination of different information sources, assist in specifying relevant outputs and identify and support policy-relevant research by research units and academic departments. On the user side, it would provide information support to specific user groups and promote and train such groups in the use of information. An example of this would be support to user groups for planning services, for primary health care, maternal and child health or for alcoholism programmes.
An analogy of the way in which this coordinating focus would operate :LS the central nervous system of the body - a "nerve centre" receiving and processing information and sending it out to all parts of the body to ensure overall functioning and coordination between all systems.
7.3 Options for a coordinating focus
These would include a special unit or group established for this particular purpose. It could be located in a planning unit or division of a health department/ministry. It could also be part of a common service agency providing a variety of support services. Choice of such a focus will vary with different country situations.
INFORMATION PRODUCERS
Statistical services
EDP services
departments medical and
social science
Other sources including library and literature
FIGURE 4: SYSTEMS MODEL OF THE RELATIONSHIP BETWEEN SOURCES AND PRODUCERS OF INFORMATION; THE COORDINATING AND DEVELOPMENT FOCUS
OF A HMIS AND THE DECISION-MAKING FUNCTIONS
HEALTH PROGRAMME & MANAGEMENT SERVICE INFORMATION INFORMATION
Population Primary health care H
Health Dental
status M Pathology
Health I Envlronmenta resources health Health S
Health manpower services
uti 11 zation etc.
Input ------------------------------~)o Process -
DECISION-MAKING
Policy
Boundary vvV'
-------------------------------------Pol! tical
Health professional
Consumer community
Operational day-to-day
Output
N o
- 21 -
7.4 Summary and conclusions
In order to bridge the gap between producers of information and decision-makers, a coordinating focus is proposed which would function in relation to the health system as a kind of central nervous system. Options for such a focus would be a functionally integrated but structurally separate unit or agency or as part of a planning unit or division of a health ministry.
8. A FRAMEWORK FOR HMIS DEVELOPMENT
8.1 A programme approach
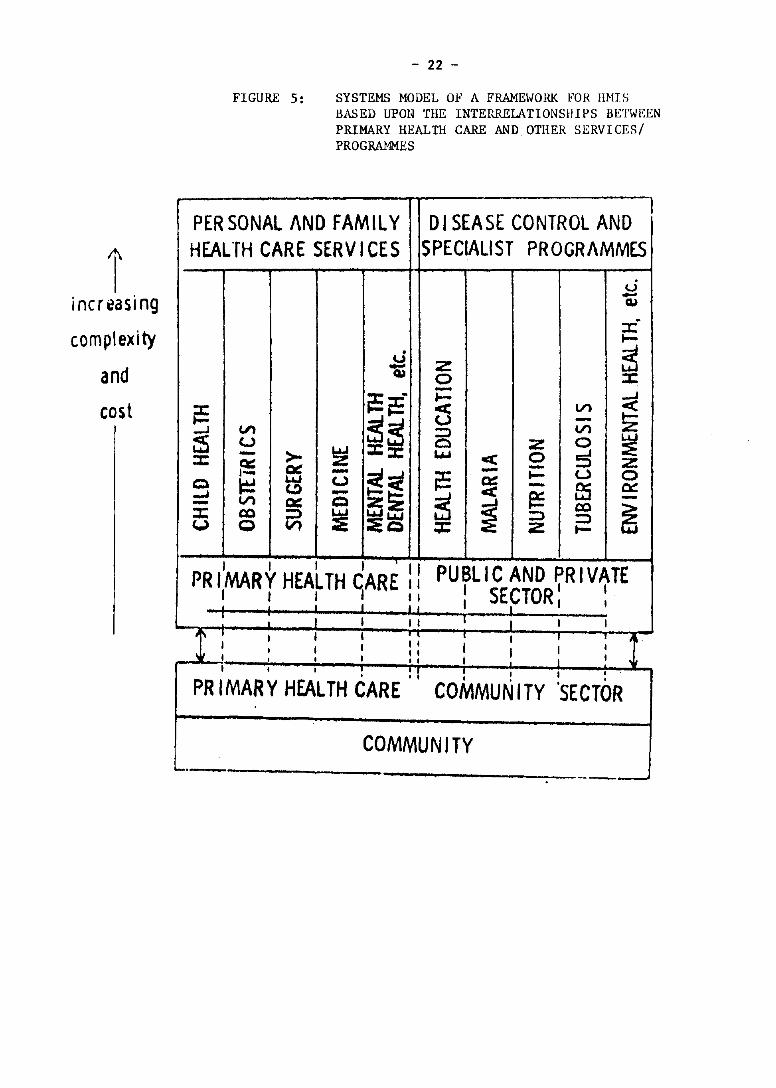
Reference has already been made to the need for HMIS to provide relevant, specific and timely information to users. It is suggested that relevant and specific information must relate to specific subsystems or functional programmes of the health system. As adopted in the Malaysian approach and as is now emerging in a number of countries, programme or service planning, based upon a systems perspective, is user-specific and seems to provide important solutions to a number of organizational problems including the approach to HMIS. The word "programme" as used in this section also encompasses a service approach as is used in some countries.
A model the Reyional Healtlt/.
of this approach is shown in Figure 5 taken from the report on Seminar on Indicators Relevant to Maternal and Child
The system may be divided into primary health care and personal specialized health care programmes integrating preventive and curative functions. It also includes disease control and other specialist programmes and (but not shown in the model) support programmes such as diagnostic, administrative, resource and personnel.
Information classified into this programme framework then becomes meaningful to programme planners and managers in that it conforms to a planning, programming and budgeting systems approach (PPBS). Finance and other resource information should be linked with programme information although this may be difficult to achieve at the operational control level.
8.2 Advantages and disadvantages
Advantages of this framework include the link between health problems and resource development, and flexibility and facilitation of analysis. It
!/Document No. WPR/HST/80.l4, Final Report of the Regional Seminar on Indicators Relevant to Maternal and Child Health, held in Manila, Philippines, from 13-19 December 1978.
I increasing
complexity
and cost
- 22 -
FIGURE 5: SYSTEMS MODEL OF A FRAME~IORK FOR IIMIS BASED UPON THE INTERRELATIONSHIPS BETWEEN PRIMARY HEALTH CARE AND OTHER SERVICES/ PROGRAMMES
1 PER SONAl AND FAMll Y OJ SEASE CONTROL AND HEALTH CARE SERV ICES SPECIALIST PROGRAMMES
u -~ ;r; I-
U Z ~ -~ 0 ::r: -~~. I- ~ ~ 5 Vl
~~ - I--J Vl :::) Vl Z
~ U 0 :z 0 ~ ::c: - >- ~ :e::r: t.J..I < 0 5 Q:: IX - Z 1- - ~cl i:= - I- U 0
Q ~ ~ u ~ - as 0:::: -' - ~ r= Vl CIC Q z!Z
~ -- co ~ ::x: co ::> :e L.i.JL..I.I :::) :::)
(,.) (;) Vl :5Q :;c Z to-
PR ,'MARY HEALTH CARE: I PUBLIC AND PRIVATE I I , I I 1 I SECTOR' I I I , I • I I I ' I
I I I 1 I I I 1
! : 1 I I ; : I I I I ~.
I 1 I I I I I 1 I
I I I I I 1 I I I I I ! : I : I I I
PR IMARY HEALTH CARE COMMUNITY ,
'SECTOR
COMMUNITY 0....- ._--
- 23 -
is user-specific in that it provides information of direct relevance to programme planners and managers. It promotes accountability for use of resources, matches complexity of problems to appropriate solutions, facilitates coordination at operational, policy-making and international levels and allows the user to see the total situation.
Disadvantages on the other hand may be the problem of disaggregating information to cater to specific requirement of operational management, of service units providing care, and of various programmes.
8.3 Priorities for service development
Within a programme framework, criteria suggested for determining priorities for the development of information systems include the public health importance of the problem related to the programme, the extent to which the health problem is amenable to programme intervention, costs of the programme in both overall expenditure and the costs of information development, demand for information by programme managers, and feasibility for information system development.
In general, primary health care, together with an appropriate management information system, was seen as the programme for priority development. This will be discussed in section 12.
8.4 Summary and conclusions
A programme/service framework following a systems approach is a logical way of classifying HHIS which is user-specific and relevant. It also provides a clear role for primary health care development as a subsystem of the health system and promotes a relationship between a programme and its resource components.
9. THE PLACE OF INDICATORS IN HHIS
9.1 Definition and description
While HHIS contains information that is both qualitative or descriptive and quantitative or measurable, that part of the information which is quantitative or quantifiable and expresses a measure of statuB or progress of a given event or entity is referred to as "indicators". They generally express or are used to express a particular relationship and reflect, singly or in combination, the basic phenomenon to be measured, for example, the rate of vaccination coverage as indicative of problem reduction. Other examples are set out in section 4.
Indicators together with other information of a less quantitative nature are essential in the management process at all levels.
9.2 Use of indicators
Indicators as stated in section 4 are used at all stages of planning and management. Population, health status and resource indicators are important in planning, while operational or service indicators are important in monitoring and control to compare targets with performance.
- 24 -
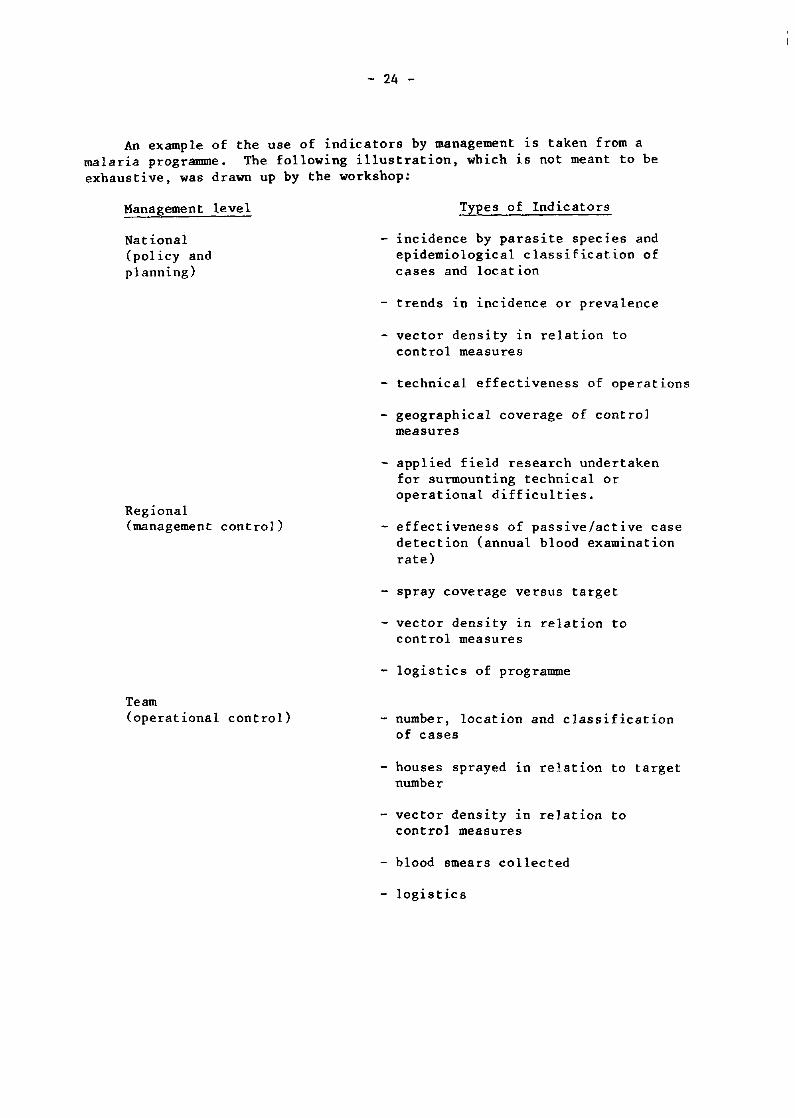
An example of the use of indicators by management is taken from a malaria programme. The following illustration, which is not meant to be exhaustive, was drawn up by the workshop:
Management level
National (policy and planning)
Regional (management control)
Team (operational control)
Types of Indicators
- incidence by parasite species and epidemiological classification of cases and location
- trends 1n incidence or prevalence
- vector density in relation to control measures
technical effectiveness of operations
- geographical coverage of control measures
- applied field research undertaken for surmounting technical or operational difficulties.
- effectiveness of passive/active case detection (annual blood examination rate)
- spray coverage versus target
vector density in relation to control measures
- logistics of programme
- number, location and classification of cases
houses sprayed in relation to target number
- vector density in relation to control measures
- blood smears collected
- logistics
I I
- 25 -
9.3 Types of indicators
Examples of types of indicators have been listed in section 4. At the policy/planning level, ~ffect or impact indicators quantifying a particular c~ncern or problem are lmportant. These include infant mortality rates, blrth rates, etc. At the operational level on the other hand, output or performance indicators are more important and relate to the measurement of a particular programme target.
Criteria for determining the value of an indicator identified are;
- related to operational objectives and targets;
- easily understood, interpreted and reliable;
- readily available and comparable;
- related to programme planning and management and hence user specific;
- sensitive and critical as measures of effect, impact and output of performance;
- non-redundant and not duplicating other indicators.
9.4 Decision-making and indicators
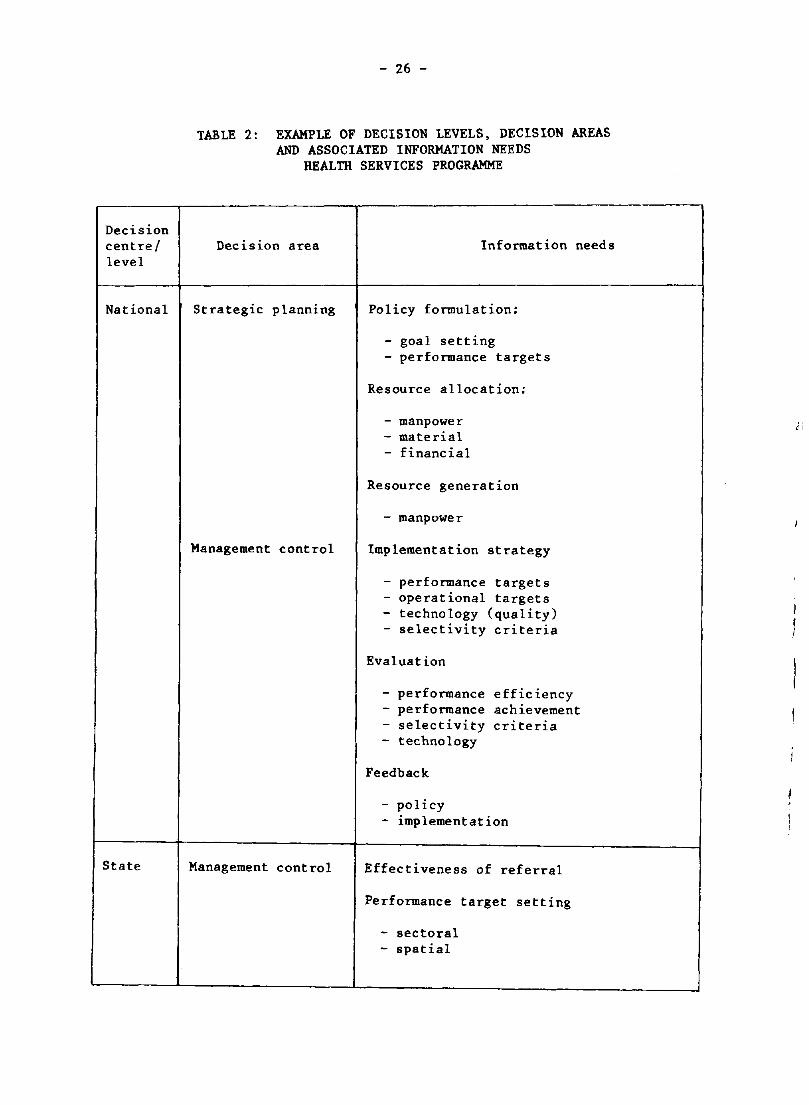
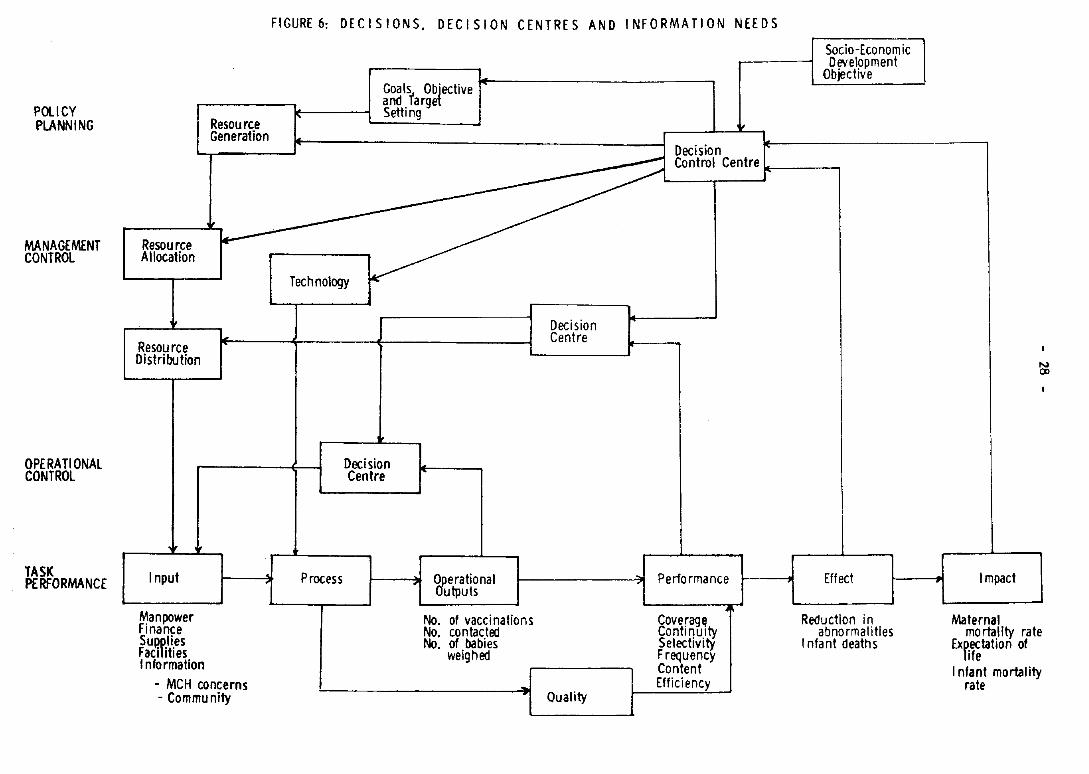
At different levels of decision-making in the Department/Ministry of Health, information requirements will vary. Level of aggregation and types of indicators will be determined by the decision-making authority and decision-implementation responsibility at these levels. An example of relationship between decision-making levels and information needs is given in Table 2 and Figure 6.
9.5 Previous reports
The workshop noted the reports on previous seminars/workshops referred to in the introduction as useful documents on indicators relevant to the development of a HMIS.
10. STATISTICAL SUPPORT SERVICES
Statistical services provide the major quantitative input to HMIS. The basis of this support is the requirements of management. As discussed in the section on indicators, the main information requirement of management should be expressed in the form of indicators. Once indicators have been defined the function of the statistical services is to collect, compile, analyse and interpret the data in relation to the indicators.
Decision centre! level
National
State
- 26 -
TABLE 2: EXAMPLE OF DECISION LEVELS, DECISION AREAS AND ASSOCIATED INFORMATION NEEDS
HEALTH SERVICES PROGRAMME
Decision area Information needs
Strategic planning Policy formulation:
- goal setting - performance targets
Resource allocation:
- manpower - material - financial
Resource generation
- manpower
Management control Implementation strategy
- performance targets - operational targets - technology (quality) - selectivity criteria
Evaluation
- performance efficiency - performance achievement - selectivity criteria - technology
Feedback
- policy - implementation
Management control Effectiveness of referral
Performance target setting
- sectoral - spatial
t i
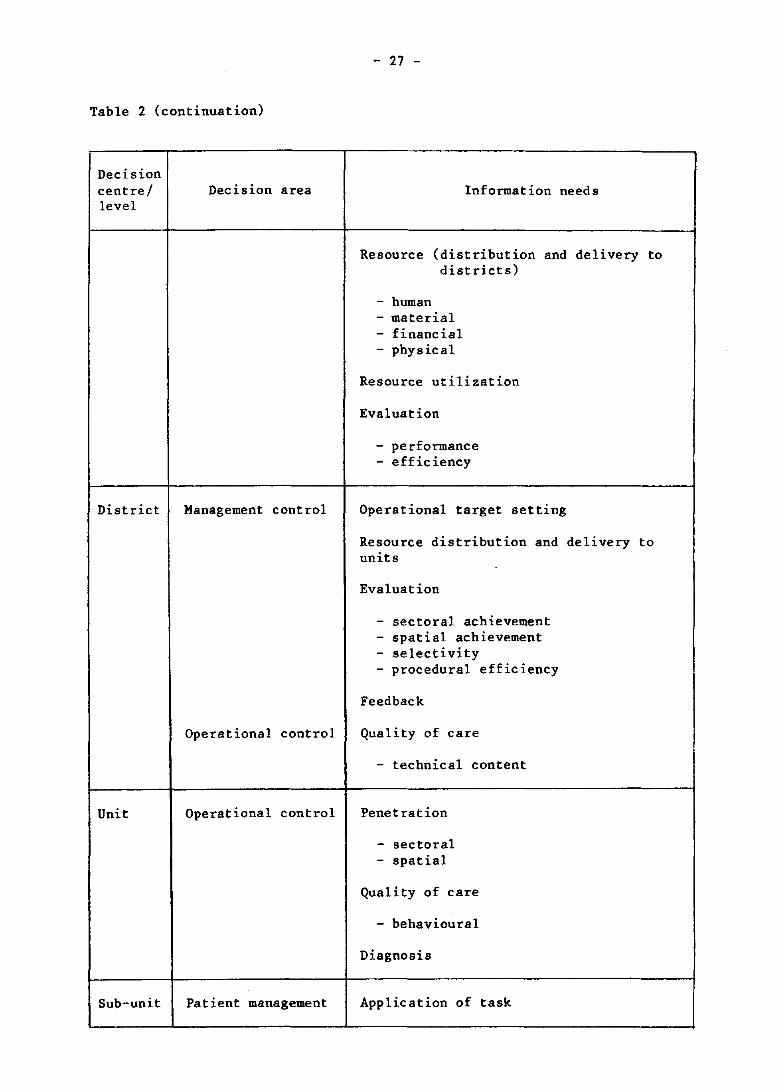
Table 2 (continuation)
Decision centre/ level
District
Unit
Sub-unit
Decision area
Management control
Operational control
Operational control
Patient management
- 27 -
Information needs
Resource {distribution and delivery to districts}
- human - material - financial - physical
Resource utilization
Evaluation
- performance - efficiency
Operational target setting
Resource distribution and delivery to units
Evaluation
- sectoral achievement - spatial achievement - selectivity - procedural efficiency
Feedback
Quality of care
- technical content
Penetration
- sectoral - spatial
Quality of care
- behavioural
Diagnosis
Application of task
POll CY PLANNING
MANAGEMENT CONTROL
OPE RA TI ONAl CONTROL
TASK PERFORMANCE
Resource Allocation
j,
Resource Distribution
Input
Manpower Finance SUlHllies Facilities Information
,
Resource Generation
~
- MCH concerns - Community
FIGURE 6: DECISIONS. DECISION CENTRES AND INFORMATION NEEDS
I'
Goals,. Objective and larget Setting
Decision
Socia-Economic Development
Objective
Control Centre ... ,, ___ ~
Technology
" Process
Decision Centre
Decision Centre
'T Qperational Outputs
I-------?t;,f Perfo rmance
No. of vaccinations No. contacted No. of babies
weighed
Quality
Coveragfl ContinUity Selectivity Frequency Content Efficiency
Effect
Reduction in abnormalities
I nfa nt death s
Impact
Maternal
.." CD
mo rtallty rate Expectation of
life I nfant mortal ity
rate
- 29 -
10.1 Function of statistical services
The workshop noted that in the development of HMIS, a number of statistical support services activities should be planned with due attention to the following functions:
Collection of data. A decision is needed on the amount of data to be collected. Even though the management plan with its need for indicators should determine all the basic data needs, in practice more data are collected than are needed to meet this requirement. This is due to planning for increased management needs and also anticipating information requirements from sources outside the Ministry of Health, for example, WHO. All of these factors must be considered in a data collection decision. The collection plan includes the design of forms. This is a very critical step and much care should be taken to ensure that;
(1) procedures are standardized,
(2) terms are defined,
(3) filling follows the sequence of operations/services given, and
(4) forms are tested before implementation.
Compilation. The compilation function involves reporting and transmission considerations. The workshop noted that due care must be taken to ensure that reporting meets the information needs for indicators at the various levels. A procedural concern of this function involves duplication of recording and the communication process to ensure timely reports. It was noted that supervision is very important to ensure that the reports reflect the basic data that are collected. It was also noted that a criterion for reporting is how critical is the information; for example, infectious disease reports need to be communicated through the system more quickly than others.
Analysis/interpretation. The workshop expressed the opinion in relation to this function that analysis must be closely carried out with the users. It was noted that in the past some statistical units were performing complex statistical analysis using analytical tools which were not intelligible to the managers. It is clearly the responsibility of the statistical unit to examine data with high standards of quality control. On the other hand, if the tools used cannot be understood by management, a compromise must be made. The analysis function provides a good opportunity to work with management and to assist in developing their analytical skills.
10.2 Sources of statistical support
The workshop noted that the information required to support HMIS is available from sources in many ministries and agencies of the government, e.g. population, education, economic, insurance, research, financial,.etc. This means that many types of statistical.sources are possib~e to.sat~sfy the HMIS requirement and those selected w1ll depend on the s1tua~1on.1n each country. The workshop noted, however, that a central ~00rd1na~1ng. committee or a coordinating unit for HMIS is desirable. Th1S coord1nat1ng activity - preferably at a high level in the minist:y - would regu~arlY review statistical collections, approve new collect10ns, and e~ped1te ~he communication of information between the various users of the 1nformat10n.
- 30 -
10.3 Training
On many occasions tra1n1ng was cited by the workshop as a key area In any strategy for HMIS development. It is particularly important in relation to statistical support services. The best form, report and communication design will not work if people are not trained to use it. It was further noted that training must involve all levels of HMIS development and most likely will involve a great deal of effort on the part of the HMIS unit. Training and supervision are very closely related. Training alone is not enough and supervision should be considered a part of training.
11. TECHNOLOGICAL SUPPORT SERVICES
11.1 Definition and functions
Technological support provides the procedures and equipment required to process and transmit information needed by HMIS in an efficient and timely manner. Technological support services should provide the following functions:
- store, collate and retrieve information;
- process and transmit information;
- assist with analysis, particularly when large volumes of data or complex analysis are involved; and
- assist with the presentation of information.
11.2 Organization of information
The experiences shared during the workshop clearly indicate that effective support to HMIS involves functions quite different from the support provided by a traditional health statistics unit. These new functions involve a wider scope of information which must be coordinated and, a more flexible format of information, and must be more responsive to changing requirements for information from the managers of the health delivery system.
A tool to assist in defining the appropriate technology as well as coordinating the information in a technological support service is a data/information organization procedure. In order to determine the needs for specific technological support, the situation of the data must be clearly known. This is essentially making a situational analysis of the HMIS data base. In the previous sections, ways of determining the specific information requirements of HMIS were discussed. Once these are known, the support services must define procedures and equipment to perform the functions of storing, retrieving, processing and presenting the required information. A data/information organization is mainly a detailed descrip~ion of where and with what frequency the data originates, what it looks l1ke (format), who works with it, how it is moved and who uses it. These detailed descriptions on the basic data of HMIS will be useful not onl~ in determ~ning the most appropriate technological support but also in mak1ng correct10ns to the support services to meet changing needs.
- 31 -
11.3 Types of technological support
Technological support includes all kinds of devices which assist jn collecting, processing, transmitting, analysing and presenting information. Such devices range in complexity from the abacus to satellite communication systems. Technology should support and not dominate HMIS development. It was noted that there are many examples of successes and failures in computerized health information systems. It was further noted that the recent significant advances in communication technology now enable many more users to have low-cost, reliable and robust equipment which is fairly simple to operate. Computerization therefore need not imply large central installations, requiring massive investments and highly skilled operators.
The workshop noted that the variety of technological support equipment available today probably made it more difficult rather than easier to make decisions on type of technological support needed. A key consideration is the organization and complete knowledge about the data in HMIS and the detailed procedures on how the information must be collected, transmitted, processed, presented. etc. Once these steps are well determined, the equipment part of technological support decisions can most often be made without much difficulty.
11.4 Using computers in HMIS
The workshop considered that computers could make and have been makjng many valuable contributions as an effective technological support to HMIS development. Computers - either the expansion or introduction - in HMIS, need to be justified on the basis of cost-effectiveness. The indication of effectiveness will be the measurable improvement in current functions or any new functions that can be performed. The most likely areas where a computer will improve effectiveness include:
volume of workload (collection, processing of data and preparing reports);
accuracy and reliability (reducing clerical errors and providing mechanical editing);
timeliness;
standardization (both in collection and reporting procedures);
analysis (being able to handle large volumes of data and complex manipulations).
- 32 -
The cost of a computer system can be determined from:
number of new staff;
training of staff;
preparation and establishment of new procedures (new forms and collection methods may be required);
the computer equipment and the instructions which are needed to perform these specific tasks;
new supplies.
The task of performing a cost-effectiveness analysis for a computerized HMIS support is not always the most straightforward process. This is due partly to the difficulty in assessing improvements anticipated and partly from determining the costs (particularly new procedures). The workshop noted that ministries considering the introduction of computers may wish to seek advice from at least two independent referees before making a final decision.
12. HMIS FOR PRIMARY HEALTH CARE
12.1 Importance of primary health care
Primary health care has already been identified as a priority area for development, both as a service and in its related information needs.
From the model of Figure 5, primary health care has certain important features which make it the cornerstone in the management of the health system. It is the link between the community and its various self-help and self-reliant movements and, through the public and private sector, the specialist services. Thus the management of primary health care is a critical element in ensuring both the development of basic health services and their impact on specialist services and is also influenced by the socio-economic development of the community. Furthermore, primary health care integrates all specialist services at the basic or community level and has an important role in promoting community involvement in these services.
The weakness of management at the primary health care level has already been mentioned as a critical problem in developing countries. This is also true of developed countries where primary health care is fragmented, uncoordinated and lacks any organizational or managerial focus.
12.2 Information requirements for primary health care
As primary health care operates at the peripheral health centre level, the type of information needed relates to resource and health services utilization for operational management involving health professionals and the local community.
- 33 -
Information needs must therefore be simple, meaningful and related to day-to-day management. Information on finance, supplies, unit performance compared to similar units may be useful. Modern technology can allow primary health care management access to low-cost but reliable dataprocessing equipment and a sound manual system needs to be developed first.
Reports from primary health care level to higher levels need to be kept to a minimal level consistent with adequate management. Reports will include immediate reports on outbreaks of illness, routine reports on service act1v1ty, e.g. attendances, referrals, deliveries, home visits, immunizations, reports on health status, e.g. malnutrition, incidence of infectious disease, reports of resource use, expenditure and inventory and report of environmental/community health status, e.g. sanitation, water supply and community activities.
Ad hoc reports may include special reports on a particular disease or problem as-it occurs at the time or on other topics of special interest.
Reliability of data collection is an important question for supervision and needs constant attention. Training of staff in reporting and use of information is essential.
12.3 Lay reporting
Lay reporting includes reports from not only the general public but also traditional health workers and those working at a more peripheral level than health centres. Such information is required to give a more complete picture of health and other problems in the community including an insight into the community's knowledge, attitudes and practices in health matters. Its development should be given careful study.
Such information is important at the health centre level to ensure adequate management and supportive supervision of such health workers but its value for mortality and morbidity information at a higher level is questionable. In many cases lay reporting is also relevant to the outpatient clinics in hospitals.
12.4 Primary health care and health for all
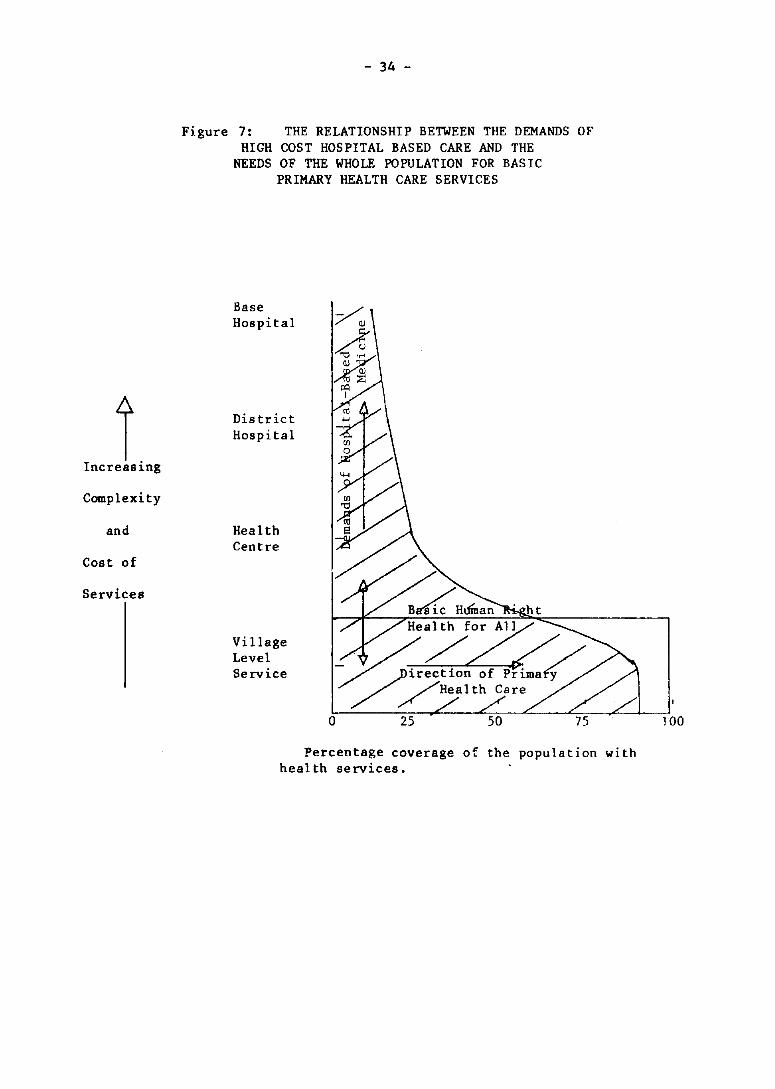
An ongoing tension in the health system is the demand for high status, hospital based, technologically orientated medicine on the one hand and the need to provide a basic level of health services to the whole population on the other. A continuing imbalance exists in almost all countries in favour of the former.
An improved primary health care service providing a basic level of care to all the population is an important challenge to management if the goal of Health for all by the year 2000 is to be achieved.
Figure 7 presents this challenge in a visual form. The shaded area represents the limited resources available to the health services. The horizontal axis indicates the percentage coverage of the population by health services ranging from 0-100%. The vertical axis indicates the increasing complexity and cost of services ranging from base level workers (aid post orderlies, "barefoot doctors", village midwives) to expensive base hospitals.
t Increas~ng
Complexity
and
Cost of
Services
- 34 -
Figure 7: THE RELATIONSHIP BETWEEN THE DEMANDS OF HIGH COST HOSPITAL BASED CARE AND THE
NEEDS OF THE WHOLE POPULATION FOR BASIC PRIMARY HEALTH CARE SERVICES
Base Hospital
District Hospital
Health Centre
Village Level Service
Percentage coverage of the population with health services.
100
- 35 -
Movement of resources in a vertical direction means retraction of services from rural areas. The line entitled "basic human right" and "health for all" is an attempt to delineate that minimal level of health services which a population should receive as a priority before higher level services are provided.
Finding appropriate indicators to measure and to manage the achievement of this priority care is an important challenge to primary health care services and to HMIS.
12.5 Summary and conclusions
Primary health care is an important and critical component in the management of the health system. Its information requirements are therefore critical to effective management. Priority must be given to ways of devising an appropriate HMIS for primary health care, including reporting from the community level.
13. ORGANIZATIONAL DEVELOPMENT OF HMIS
13.1 The need for organization of HMIS
The previous sections have referred to a number of important problems and needs in the development of HMIS. These now converge upon the issue of what organizational arrangements are required if HMIS is to function effectively. These concern:
(1) lack of utilization of information due to
gap between available information and decision making needs;
fragmented state of information services.
(2) need for an organizational focus
to determine priority areas for HMIS development;
to be responsible for achievement of overall and specific objectives of HMIS.
(3) need to reorient or develop appropriate statistical and technological support services
the responsibility for the achievement of identified objectives of HMIS.
13.2 A coordinating committee or group
In order to meet these problems and needs, a top level coordinating or steering committee of heads of divisions of ministries/departments is an essential step in HMIS development. This would ensure that all representative interests, including producers and managers, are brought
- 36 -
together to determine what kind of HMIS would be appropriate to the country and how it could be implemented. It would also ensure that, wherever the proposed coordinating focus or responsibility centre/unit is located, its rather powerful position as an information centre of the organization 1S
not subject to anyone division.
A central focus/unit for HMIS would report to such a committee but could be appropriately located within a planning or information unit - a separate semi-independent body or agency which could provide statistical, computing and research services to all levels of the health system.
13.3 Decentralized HMIS
Arrangements would be needed to provide for planning/information support units at subnational/regional/district level to promote HMIS development for regional management. Such a unit could be a sub-unit of the national unit or be more directly under the regional management. In any case communication both laterally and vertically is essential to ensure compatibility, standardization of procedures and close links between regional management and the central body.
13.4 Summary and conclusions
In order to meet the needs and problems and achieve the objectives of HMIS development, a top-level coordinating/steering committee is proposed. This would establish a coordinating unit responsible for the promotion and development of HMIS. Decentralized units would also be required at subnational/regional levels.
14. THE MALAYSIAN EXPERIENCE OF HMIS DEVELOPMENT
14.1 Background
The workshop was fortunate to be able to share in the practical steps already taken by the Malaysian Ministry of Health to implement a national HMIS.
The need for a better information system and the role of information in the better management of health services arose out of an operations research study of rural health services, conducted in the early 1970s. The lack of appropriate information to formulate five-year development plans and the awareness of the lack of health information among the rural population highlighted the improvement of the existing information system as a priority area for development. Exchange of experience and information is one of the ways by which HMIS development can be promoted. Through such an exchange of information, it should be possible for the managers to study and understand possible ways by which available information can be better understood and utilized.
- 37 -
14.2 Development
Preliminary work began in 1975 with technical support from WHO and a protocol was prepared in June 1976 on Health Management Information System Development. Figure 8 gives the strategic steps in development of Health Management Information System and Figure 9 gives the technical steps in development of Health Management Information System. A top-level Steering Committee was formed by Directors of Divisions of the Ministry, chaired by the Director-General and responsible for all aspects of HMIS development.
The Steering Committee was assisted by an Information System Development Group (ISDG), which consisted of full-and part-time staff seconded from various divisions to survey information needs and problems, to design a conceptual framework, to identify user needs and to design, test-run and evaluate HMIS.
A prolonged planning and developmental phase then followed. HMIS was designed on the basis of systems and subsystems which are closely related to existing divisions and programmes of the Ministry (see Annex 9). A wide range of data forms were designed and tested.
14.3 Test-run
A test-run in the State of Penang was commenced in 1979. The purpose of this was to test the applicability of basic documents in the field, to test instruction manuals and to identify any other problems including training needs, resource requirements and communication flows.
Roles and responsibilities of participants were defined and a series of worksho~s conducted to train and involve staff in implementation. A State coordinator was appointed together with a focal group in the State equivalent to ISDG.
It was proposed that the test-run continue for one year at which time feedback and evaluation procedures would determine the feasibility of the system for national implementation.
Details of the test-run strategies and activities are provided 1n Annex 10.
14.4 Important lessons which might be learned
(1) There is a need for top-level understanding and commitment before embarking upon a national HMIS.
(2) A working group of seconded or full-time staff is required to undertake a situational analysis, to define problems and needs, and to design the system in consultation with both top management and users.
(3) Technical consultancy support from international agencies may almost certainly be required.
(4) Careful and prolonged design of the system is required before anything is implemented. Design should be based on programmes and services and certainly involve users. Output information requirements must precede input data design.
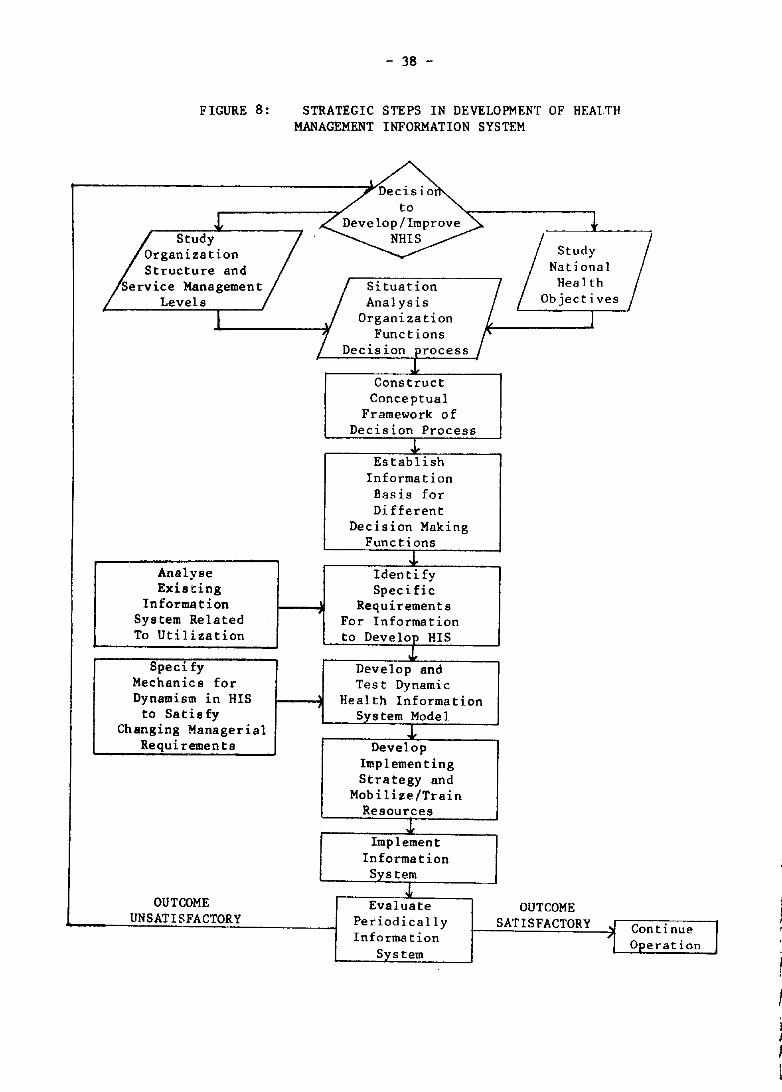
FIGURE 8:
J,
- 38 -
STRATEGIC STEPS IN DEVELOPMENT OF HEALTH MANAGEMENT INFORMATION SYSTEM
I .. /Declslo
to Develop/Improve ~ p "Ud
Y
/
NHIS Organization /8<U
d
Y
/ Structure and National
Service Management Situation Health
Levels Analysis Objectives
I \, Organization I
1 Funct ions " Decision process
J, Construct
Conceptual Framework of
Decision Process J,
Establish Information Basis for Different
Decision Making Functions
J. Analyse Identify Existing Specific
Informs t ion Requirements System Related For Information To Utilization to Deve lop HIS
J, Speci fy Develop and
Mechanics for Tes t Dynamic Dynamism in HIS Health Information
to Satisfy Sys tern Mode 1 Changing Managerial J.
Requi remen ts Develop Implementing Strategy and
Mobilize/Train Resources
J. Implement
Information System
.t OUTCOME Evaluate OUTCOME
UNSATISFACTORY Periodically SATISFACTORY " Continue Information 1 O~eration System I
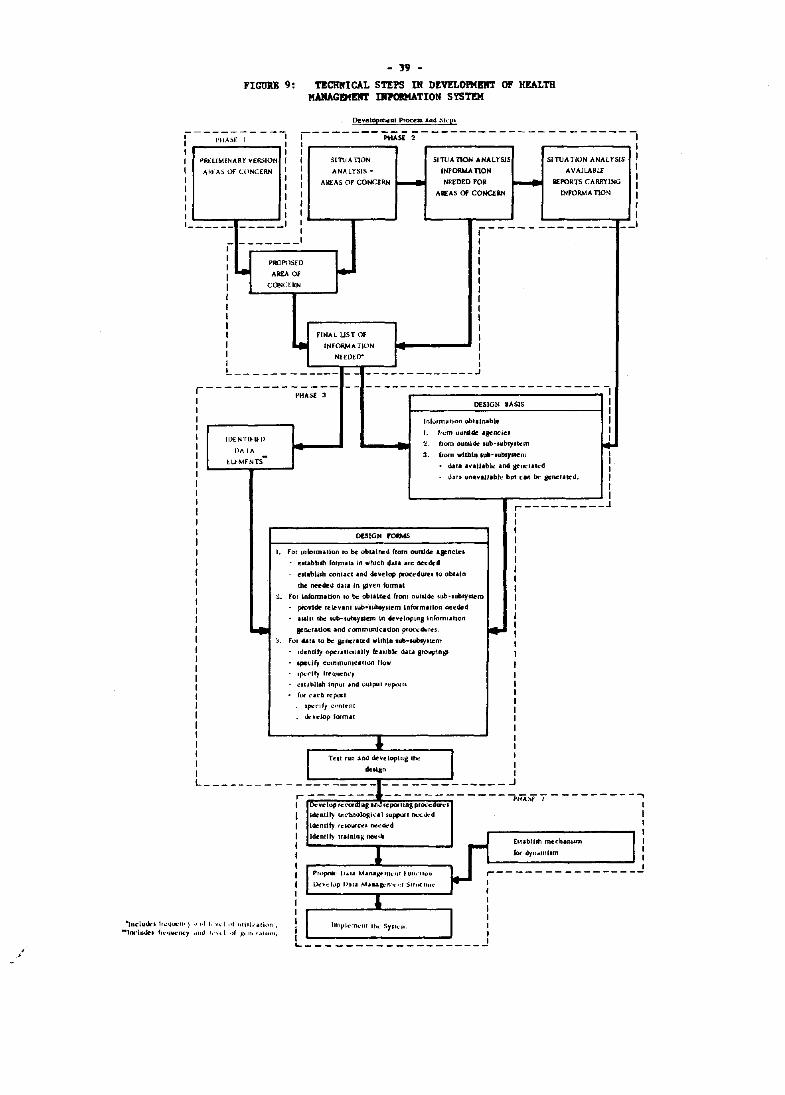
- 19 -FIGUU 9: TECHNICAL STEPS IN DEVl!LOl'KBlI'r OF HEALTH
!WIAGEIIE1IT DI7OIIIATION SYST!H
[)uelopmcnl Proaa alld !il<·e~
f--~;;;;:;;-;-----' r-------~~2---------------------1 I I I I
~RHIMINARY vt::IbION 1 1 SlnrA nON SlroA nON ANALl"SJS S(nJAliON ANALYSiS
AfII:"A:) or U1NC£RN I 1 ANALYSIS ~ INFORMAnON AVAILABL£ I I I-- I--I 1 ARfAS OF CONCERN NEEDED FOR REPORTS CARRYING
I 1 AREAS Of CONCERN INFORMATION
I I 1 1
1
1 1
I 1 I 1 1 1 I ------ _____ 1
1 ,-------------- --
"IncluQ.:, fr""..,II' ) -Ioil"luoir. f"'~lWnc:y
, - ______ 1 , I ,
PROPOSED I , Le ~ I A ..... Of I
I I CONCEIlN , r I , I , I r I , FINAL UST Of I I • INFORM A nON I I NHDErr I I I L ____________
- -_ ____________ .J
,-------------- - - --------------------------1 I PHAS.E :1 DESIGN BASIS I
1 I I lol ... rmOltloo obl.ln.ble I I I , I. IfOm t1I11U:tde 'jenele.
Im:NT[tll:[) 2. from 0I.Iu,14e sub-subsyltcm ~ P ..... I/\ 3. (rom wlml_ .ub-IUbsJ11em
lUMFNTS-1
- d.l' ..... II.ble nd grocrllo:d I 1
,bra un.v.JJ.bk but Call bt" aeBCfaklJ. I I I
r---------.l I I
DESIGN rOOMS I I
I. For Lnformllioo 10 be obtained ftom outside aFnciei r utabb.h formus 1n which d.l. illfe metdd
, ell.blbn COnllel and develop proc:~dure, 10 obl.ln I
I the ne-edeli dall In given kllmal ,
". For Inbmuion 10 be: obuloed frorn ouul4e sLlb'lubryctem I pIOY'de re~v.nllub"lubsyJtem Intt-mltlon ne~cSed 1
I .Mln tht IUb-1ubty~ In .~eloplnllnromlluon I I ... gener.don .1nd ("omrnunl~.uon pruc\:4unn, • I 'I. For dall Ie be- FRer.ted Wllhlll ,ub-subly'leffl
I Identify operulonally It •• lble d.l.1 groupln" I 'PCu(y cummunlufh>n fklw I I Ipt!rlfy fr"l.I~nry , 4:1I~bllab Inpul .nd output rcpOUI , for "icb repall , Ipo:"lly ':"f'llfnl
I &veJop formll I I I 1 r Tell fun.and dt ... eloplng lhe I I lIIc"'g"
L _______ - - - ~ ------::.=-t---- ____ -:::::: ____________ I IJot:ovelopfeCOfdlUllnJrc:potllngproccQI\lrCI PUA,\f I
I l.nU~ lecbnologh:'\ suppon no:o:ok'd , Identify rc50U";~1 nccdt-d , ldentl~ tralmn& nc.:t.4 I
ElI,blhh mccham.m
1 1 kif dyu,ulI,.m , , P'''poIi' 0.11 M.n.jltPIII. "I • UIf,'lIulI ,---------------, 1)e\lt:I ... p I'ill. M ... a.all'"'l-n' S,r'I£IUr .. I
1 1
I , I
I I , 1 "".I I, ....... [ ", IjIUI(lIiofl .
I In1f'1<'m"lIr 1110' SY'ICJlI I _ .. ,,, kH'1 .• , x. 'I! <.1110111. 1 I I '-------
I I I I I I I I I
.., I I 1 , I 1 1
..!
- 40 -
(5) Choose a test-run or pilot area as representative as possible of the country but where cooperation can be assured. Begin small and gradually expand as problems are identified.
(6) Train and retrain staff at all levels and all stages of the process.
(7) Define clear lines of responsibility and uniformity of action.
(8) Provide adequate feedback to all levels to ensure full understanding and involvement.
(9) Provide non-technical support to undertake clerical and other recording duties.
15. CONDITIONS TO IMPLEMENT HMIS DEVELOPMENT AT COUNTRY LEVEL
A number of practical conditions and steps were identified which might form part of HMIS development.
The priority and sequence of steps will vary between different countries according to circumstances; not all those identified will be necessary in all countries and additional steps may be important in some countries.
15.1 Securing support of top management and policy-makers
High level commitment to HMIS is important. This might be promoted through:
management education and development activities
recommendations of government, parliamentary and other official inquiries
regional meetings of WHO and the World Health Assembly
professional bodies, community planning agencies, consumer groups, etc.
demonstration of the value of information in decision-making, particularly in relation to high-cost services
promotion of pilot schemes.
- 41 -
15.2 Strengthening national capabilities for HMIS
It might be important to strengthen national capability in components of HMIS which are weak. For example, in different countries health statistics services, data processing, staff training, or financial information services might need to be upgraded.
WHO might assist such efforts for the establishment of common standards or definitions and the consultancy services to individual countries.
15.3 Management development
General development of managerial and organization skills can assist development by HMIS through:
management education and training schemes;
decentralization of management responsibility, which may create a demand for information;
practical demonstration of usefulness of information in decision-making.
15.4 Organizational framework
If effective health management information systems are to be established in the individual countries, it is essential that, as part of the system, some office, service or centre should have the role of providing an overall vision and dynamism, keeping relevant existing and forthcoming information under constant review, noting omissions and imbalances, helping to plan future information collection and studies, encouraging adjustments in statistical compilations which are being planned and made, working on data collection methods and indicators for the country concerned, relating information to policy needs and bringing it to the attention of policy-makers, helping to organize and prepare regular reports for use by policy-makers and public health managers and administrators at different echelons in the Ministry or Department of Health or similar bodies as well as for general dissemination. In this respect, an early step may be to identify organizations/units already concerned with components of HMIS. Alternatives for the formal organization of HMIS, whether centralized or decentralized, within the Ministry of Health, or another agency, and other possibilities need to be evaluated. In the development of HMIS, a whole system needs to be considered, in all aspects, which will include how information will be used.
15.5 Identification of user requirements
To identify user requirements for information, it may be necessary to systematically analyse policy objectives and functions of programmes. Such analysis will suggest what indicators need to be developed and what information should be collected.
- 42 -
15.6 Coordination
Development of information coordination between private, public or voluntary groups providing similar services and between health-related agencies may be important. It may be helpful to work out and agree on a formal protocol for mutual assistance and communication. In some situations a formal national coordinating body may be desirable.
15.7 Design of HMIS
In the design of the system, it 1S important:
to define objectives;
to establish a budget;
to carry out a cost-effectiveness analysis;
to establish priorities;
to establish national norms and standards;
to consider methods of presentation;
to include consideration of a management reporting system.
15.8 Test-run
In an arrangement for a test-run:
(1) There needs to be flexibility in the system to allow it to be modified after evaluation.
(2) It needs to be tested in a variety of areas and conditions.
(3) Sites for the test-run should be chosen which are representative of conditions in the country, sufficiently manageable and compact.
(4) The test project should be small enough for control, but complex enough to bring out critical problems which may be associated with implementation of any system.
15.9 Implementation
In implementation:
(1) It is important to have arrangements for regular monitoring.
(2) A user-committee can be useful.
(3) The process of implementation needs to be fully documented.
(4) Attention to staff education and training is important.
(5) Requirements of implementation need to be taken account of in design of the system.
_ 43/44 -
15.10 Use of information
Promoting the use of information may be necessary at a very early stage in development of HMIS. Making relevant information available to managers at appropriate times can create the demand for more information. Managers may need to be trained in numerical methods in order to interpret information. An understanding of concepts such as probability, statistical significance, "best fit", or stochastic processes are essential to the interpretation of numerical information.
15.11 Suggested steps
A possible series of steps in the development of HMIS was suggested for illustration (Table 3). It was emphasized that this example was for illustration only, and the steps appropriate in anyone country would vary according to the country's circumstances.
15.12 Role of international agencies
International agencies might assist countries 1n the development of HMIS by:
Development of international standards, definitions and classifications
Consultancy advice to individual countries
Dissemination of expert opinion and technical literature
Promoting concept of HMIS through formal meetings of representatives from Member States, such as regional meetings or the World Health Assembly
Promoting exchange of experience between countries and training
Resource support
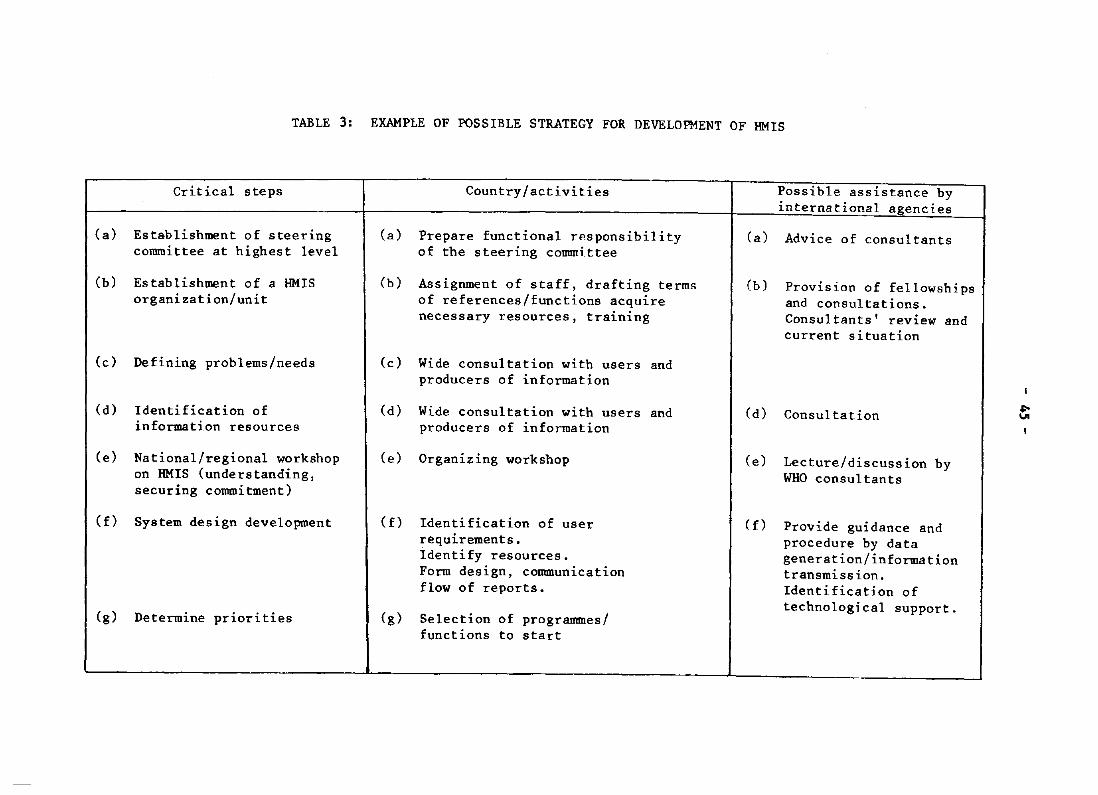
TABLE 3: EXAMPLE OF POSSIBLE STRATEGY FOR DEVELOPMENT OF HMIS
Critical steps
(a) Establishment of steering committee at highest level
(b) Establishment of a HMIS organization/unit
(c) Defining problems/needs
(d) Identification of information resources
(e) National/regional workshop on HMIS (understanding, securing commitment)
(f) System design development
(g) Determine priorities
Country/activities
(a) Prepare functional responsibility of the steering committee
(b) Assignment of staff, drafting terms of references/functions acquire necessary resources, training
(c) Wide consultation with users and producers of information
(d) Wide consultation with users and producers of information
(e) Organizing workshop
(f) Identification of user requirements. Identify resources. Form design, communication flow of reports.
(g) Selection of programmes/ functions to start
Possible assistance by international agencies
(a) Advice of consultants
(b) Provision of fellowships and consultations. Consultants' review and current situation
Cd) Consultation
(e) Lecture/discussion by WHO consultants
Cf) Provide guidance and procedure by data generation/information transmission. Identification of technological support.
~
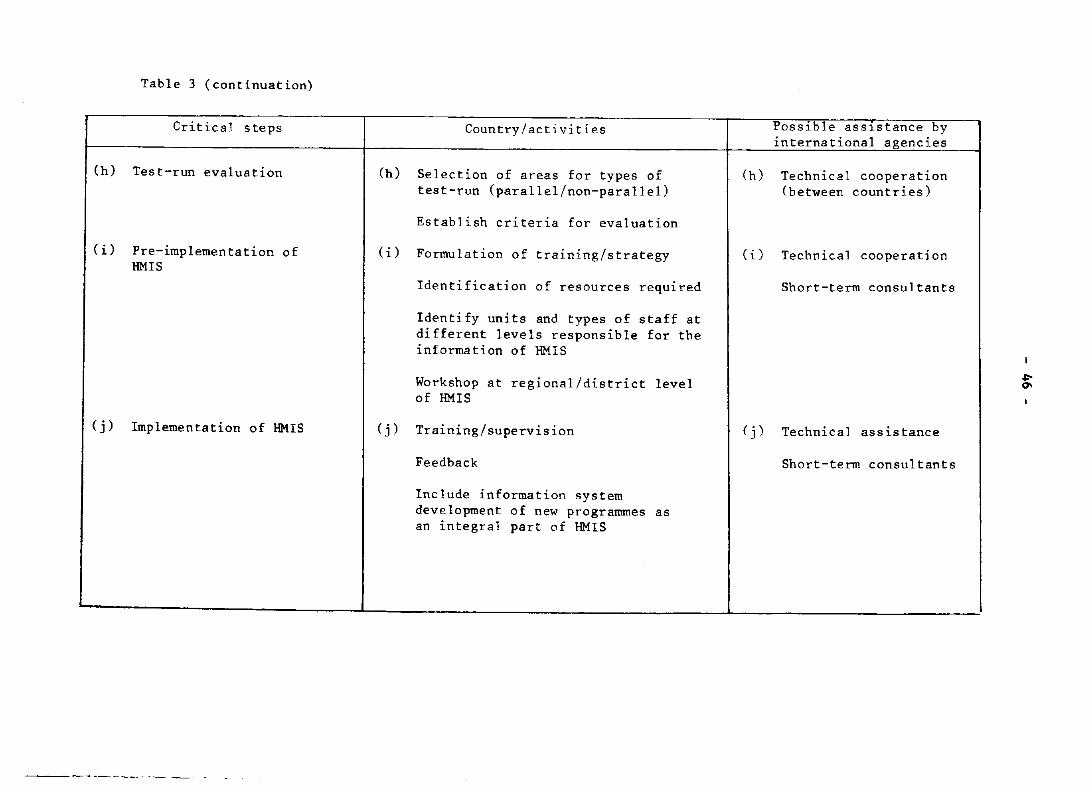
Table 3 (continuation)
Critical steps
(h) Test-run evaluation
(i) Pre-implementation of HMIS
(j) Implementation of HMIS
Country/activities
(h) Selection of areas for types of test-run (parallel/non-parallel)
Establish criteria for evaluation
(i) Formulation of training/strategy
Identification of resources required
Identify units and types of staff at different levels responsible for the information of HMIS
Workshop at regional/district level of HMIS
(j) Training/supervision
Feedback
Include information system development of new programmes as an integral part of HMIS
Possible asslstance by international agencies
(h) Technical cooperation (between countries)
(i) Technical cooperation
Short-term consultants
(j) Technical assistance
Short-term consultants
.I:-0\
- 47 -
OPENING ADDRESS BY DR L.R.L. VERSTUYFT, WHO PROGRAMME COORDINATOR, MALAYSIA, ON BEHALF OF THE REGIONAL DIRECTOR,
WHO REGIONAL OFFICE FOR THE WESTERN PACIFIC
Honourable Minister of Health, Tan Sri Chong Hon Hyan, Honourable Deputy Minister of Health, Dr Sulaiman Daud, Secretary General of Health, Dato' Alwi Jantan, Director General of Health, Tan Sri Professor Dr R.P. pillay, Organizing Chairman of Workshop, Dr Lim Ewe Seng, WHO Operational Officer of Workshop, Mr M. Subramanian,
ANNEX 1.1
On behalf of the Regional Director of the WHO Western Pacific Region, Dr H. Nakajima, I wish to welcome you all to this Regional Workshop on the National Health Information System.
The subject of this Workshop is of great interest and concern to both the Member States and WHO. As you all know, the Member States of the World Health Organization resolved at the Thirtieth World Health Assembly in 1977 to achieve the goal of health for all by the year 2000. They have been engaged since then in formulating strategies and developing procedures to manage the implementation of those strategies and to achieve that goal within the given time frame. As organizational and functional modifications to ensure the efficient management and effective achievement of the health development objectives of Member States under this goal are formulated, the importance of information as an essential ingredient in the decision-making process becomes obvious.
The first thing about information systems that strikes me is that one gets too much information. This flood of information crosses and criss-crosses the desks of managers with a great deal of data. Much of it is only partly comprehensible and digested and much of it is irrelevant. Managers have to go through reams of reports and try to determine for themselves which are the most critical pieces of information contained in the reports so that they can take appropriate action and correct any problems before they become public issues and get politicized. In the turbulent world of today which offers an impressive range of technological possibilities for coping with the basic health and other related problems, information requirements relate more to support for the manoeuvering of uncertainty than for the administration of certainty. The timely availability of relevant information, selected and extracted for its significance from a mass of data and presented in a meaningful format for the decision-makers at different echelons, is of tremendous importance. And as information becomes inseparable from the management process and the need for further improvement of the information system in support of management functions is recognized, we are witnessing also an explosion in the volume of data available, the number of computers available to process these data, newer and more powerful teChniques to extract useful information from the data, and various forms and methods of presenting
- 48 -
Annex 1.1
information to management so that it can be understood and used. The use of all these possibilities, either singly or in combination, to develop II
dynamic and effective information system which will enable management to recognize and respond to existing management problems or to adapt quickly to changes in the environment or to exploit changes arising in technology, ~s therefore highly complex.
The information system, as an organized and standardized system to manage the flow of information in a proper time frame, is essential for collecting, converting, communicating and maintaining the flow of information from producers - mainly service personnel - to users - mainly managers at different echelons - and for providing feedback to them. But however good an information system is, it is not a substitute for good management. To be effective, an information system has need not only of readily available information when required but also of managers competent to utilize it and an organizational environment providing managers with the authority and responsibility to implement the decisions taken. Given that we operate under conditions of increasing uncertainty, our expectations from an information system may be attenuated or affected by these factors but we cannot forego it entirely. The management information system as a priority component of the national health information system has to be recognized and activities must be initiated now.
Concerned with the possible problems that Member States may face, the World Health Organization has been undertaking a number of activities at country and intercountry levels to further develop information systems in support of health development, programme development and management. The present Regional Workshop on National Health Information System is one such activity. The objective of the Workshop is to formulate an overall health information system development strategy, to develop guidelines to adapt this strategy to the country context, and to outline practical steps for its implementation. I hope the Workshop will examine with equal emphasis the dual problems of information availability and the capability for its use.
An information system is country specific and, to be relevant and meaningful, must be developed in the country context. It is significant therefore that we are holding this Regional Workshop in one of the Member States of the Western Pacific Region. I wish to thank the Government of Malaysia for acting as host to this Workshop in Malaysia - a country already engaged in the development of the health information system for the Ministry of Health.
My sincere thanks are due to Dr Lim Ewe Seng for agreeing to serve as Workshop Director.
I would like to welcome Dr Laurence Malcolm and to express my s~ncere thanks for his readiness to help us in his capacity as consultant.
The significance and interest of this Workshop to WHO can be judged by the presence of the two directors concerned with information system areas in WHO/Headquarters. I wish to welcome Mr K. Uemura, Director, Division of Health Statistics, and Dr S.H. Mandil, Director, Information Systems Programme, and to thank them for taking time off to be with us to participate in this Workshop.
- 49/50 -
Annex 1.1
I note that you have a heavy agenda ahead of you. The group sessions in particular call for patience and effort on the part of all of you. I am sure you will find this a very useful and rewarding experience, and I wish the Workshop every success.
- 51 -
CLOSING REMARKS OF DR L.R.L. VERSTUYFT, WHO PROGRAMME COORDINATOR, MALAYSIA, ON BEHALF OF THE REGIONAL DIRECTOR,
WHO REGIONAL OFFICE FOR THE WESTERN PACIFIC
Director-General of Health Tan Sri Dr R.P. Pillay, Ladies and gentlemen,
ANNEX 1.2
Ten days have passed so quickly. I understand you shared my concern on the lack of an effective information support to management of health services and, with considerable effort and perseverance, approached the problem in its entirety to formulate appropriate ways by which solutions can be developed. I concur fully with your emphasis on the need to develop solutions in the country context taking into account political environment and operational constraints.
As I mentioned in my opening remarks, information is becoming more and more one of the critical areas for the betterment of the future. This workshop is one of the activities to bridge the gap between technological possibilities for improvement of health development and management on the one hand and information explosion we are presently witnessing on the other.
Knowledge of current situation to tell managers what resources and obligations he has, how these resources are committed and used, how the usage is contributing to the overall health development objective and, to a great degree, what freedom of action is now open to him are some of the specific issues to be answered in the context of a twenty-year horizon under the "heal th for all by the year 2000" goal. In many cases, I don I t think we know enough but how well or how poorly we are doing and I don't think we know it soon enough. It is thus appropriate that you have dealt with the need for an effective, efficient and dynamic information system to satisfy the requirements of significance and vitality, reliability, timeliness, understanding and comparison of results.
Your deliberations and hard work has laid the ground work to reduce guessing and assuming and to increase our ability, to a certain extent, to measure precisely how the health serVices function.
I notice you have agreed on the objective of a good Health Management Information System. You have also identified some of the critical steps to be taken towards its development. The basis you have established for selected transmission of relevant information in a timely manner and in a comprehensible format should help in reviewing and reorienting the existing health information in your respective countries to satisfy priority user requirements. We shall be glad to consider favourably proposals for follow-up in your respective countries for activities emanating from the workshop you have just concluded.
The visit to the Health Management Information System Development project test-area would have shown you not only the beauty of the host country but also the practical implementation problems and details associated with any HMIS development in a country.
- 52 -
Annex 1.2
This workshop is more of a part1c1patory learning type than of an essentially training one. I wish to thank you for sharing your experience with us. I assure you the Secretariat has learnt much from this workshop.
I wish to thank the Government of Malaysia for hosting and for making excellent arrangements for the workshop. My sincere thanks to Dr Lim Ewe Seng who has ably directed the workshop and effectively steered the deliberations to achieve the workshop objectives. My thanks are also to Dr Laurence Malcolm for providing valuable guidance to the workshop and to Mr K. Uemura, Director, Health Statistics Division and Dr S.H. Mandil, Director, Information Systems Programme with WHO/Headquarters for their contributions and for being with us during the entire duration of the workshop.
Finally, I wish to offer my very best wishes for success 1n your work and a pleasant journey home.
- 53 -
OPENING ADDRESS BY Y.B. TAN SRI CHONG HON NYAN MINISTER OF HEALTH, MALAYSIA
ANNEX 2.1
It is my pleasure once again to see the Ministry of Health associated with the World Health Organization in sponsoring this Regional Workshop on a National Health Information System. I thank the Regional Director and the Representative of the Western Pacific Region for their continued concern in all matters pertaining to health care in this Region. I welcome all our distinguished participants and consultants to this Workshop, especially those who have come from distant lands and islands in the Pacific.
You will have opportunity enough to discuss in broad outline and in detail the ingredients that must go into a National Health Information System as this must obviously be framed with your individual needs in mind. All I would like to do here is to touch a little upon our Malaysian experience, limited as it is, so that our weaknesses may be thoroughly examined and our merits, where there exist, can perhaps be adapted for use by others. Like many other developing countries, we inherited a health system, as we have inherited other administrative, social and professional systems, from a colonial heritage. We have consciously tried however, in the 23 years since our independence to make all these systems truly reflect our own needs and aspirations since then and are still in the process of evolution where our health care is concerned.
There are those however in this country, particularly professional associations, who are quick to criticize such systems that are now evolving as if mdre sophisticated models gleaned from advanced countries can be transplanted on us with immediate effect and as if there are also instant cures that can be advocated. There are gaps in our information system just as much as there are gaps in any other country. "Garbage in, garbage out" is a truism that is held dear by our computer programmers and analysts. This is equally true of information systems. What we devise for ourselves must pass the test whether the information is useful to managers of our health system. What is equally vital to appreciate, however, is whether operatives on the ground, possibly far removed from the managers and analysts themselves, realise the need and urgency for them to provide such inputs with accuracy, clarity and promptitude.
I have seen some of these procedures on the ground as we have initiated, a planned development of such a system in 1975, with assistance from the World Health Organization, just as you will see for yourselves how things are going on in our test-run area of Penang, during the course of your Workshop here. I have noted in a typical case, a young, newly-graduated doctor in one of our outpatient clinics, carefully and painstakingly ticking off appropriate boxes in his information sheet while surrounded, as many of our hard-pressed outpatient doctors are, by squalling infants and anxious mothers whose sole concern is that their
/
\
- 54 -
Annex 2.1
children should be examined - and examined quickly. I am certain that our doctors in turn are equally anxious to treat their patients urgently and if our input systems are going to be too cumbersome, complex or timeconsuming, then these are not likely to reflect any great degree of accuracy if filled in by harrassed personnel, pressurized as they often are by the sheer number of patients, all demanding immediate attention at the same time.
I trust, therefore, that when systems are devised in the rather detached atmosphere of workshops and planning committee, the human element is not glossed over - and this applies equally to the private sector. We have been accused by our critics of separating the health care system in this country too rigidly into the public and private sectors, leaving the latter severely alone as it were, and disregarding their sensitivities. Private sector doctors in this country are concerned mainly with curative medicine and we would certainly like to fill in gaps in our overall health information system with their contributions. Our experience however, which may be common with other countries, is that sometimes the enthusiasm of professional associations to assist is not shared by their members operating busy clinics and hospitals on their own. Filling forms is timeconsuming which means earning opportunities lost in that period. Certain private practitioners who are requested to provide health planning and management agencies with vital information on the incidence of certain types of cases they treat, have even suggested that they be paid for filling up periodic questionnaires. It would be a sad day for us if health services were to be so commercialized that we can only obtain information on health trends by commissioning market surveys and paying market rates for them.
While we can try to perfect our systems and our techniques therefore -and nobody denies the value of precise, up-to-date and relevant information for modern management and planning - I trust that even as we devise these systems that we do not lose sight of the need for the man on the ground to recognize the value of his particular input as well. He sees one piece of the crossword puzzle; this piece alone is meaningless, showing as it does uneven edges and features that are not distinct or relevant on its own. If he has to shape the piece, he may shape it in any way he likes. Unhappily, however, if he does this, then his piece will not fit in with those shaped by others who may be as independently-minded. Part of our problem will thus be to ensure that the objectives of whatever system we devise are understood by not only the planners, but also by the contributors towards this sytem who will willingly and with promptitude supply such information as is sought. Otherwise however well-intentioned we may be, we shall be embarking on exercise in futility - to the exasperation of all.
I am certain that all of us gathered here are anxious to have modern tools of management and relevant data is one of such tools. We are faced now with a rising volume of reports, statistics and data that can only bewilder and confuse, unless they are put into coherent shape and size that can be digested by managers and those who frame policies. Policy-makers may not be necessarily trained in the particular profession for whose services they are responsible to the public. It is as much to help the policy-maker as the professional, therefore, that we need an information system that is relevant to resolve problems.

- 55/56 -
Annex 2.1
How then to reduce these various sources of information and statistics to an understandable format that can contribute towards policy-making, is both your challenge and your vocation. It will take research and time to collate and coordinate facts and figures that may lie with various specific administrative divisions within a particular organization itself. So long as we work along such vertical divisions, so long will there be an inherent tendency to collect relevant data pertaining to that activity alone, unless there is a conscious effort to coalesce this information with others to form a whole.
I am confident that in a Workshop like this, the methodology and approach to the pooling of information in a cohesive manner will be better understood after your discussions. I look forward to the evolution of our own Health Information System when it can serve as a ready instrument for policy decision as well as for day-to-day management. We must dispel the notion that still lingers on in certain quarters that professionals should practise their skills but management should be left to others. You can and must do both if we are to ensure health delivery systems to achieve better health for all in our countries and our region.
- 57 -
ANNEX 2.2
CLOSING ADDRESS BY TAN SRI DATUK PROFESSOR R.P. PILLAY DIRECTOR-GENERAL OF HEALTH, MALAYSIA
Mr Chairman, Dr L.R.L. Verstuyft, WHO Programme Coordinator, Mr M. Subramanian, WHO Operational Officer of the Workshop, Ladies and Gentlemen,
It is with great pleasure that I accepted this invitation to come and say a few words during the closing session of this workshop. Although I have not been able to be with you during your daily discussions, this topic on health information is of great interest to me. As most of you are aware, I have just assumed the post of Director-General of my Ministry barely a month ago and everyday in my work I have been requesting for information of one category or another whether it pertains to planning, service delivery, personnel or financial matters of the Ministry. In a sense, being new to my job, I hunger for information that will assist me in the performance of my duty and I definitely appreciate the situation when information can be presented to me in a clear and concise manner and straight to the point.
The holding of this workshop is very timely in the context of Malaysia. We ourselves, with the assistance of WHO in the person of Mr Subramanian, have been engaged in developing a health management information system for the past few years. We have gone through the conceptual phase, the situational analysis, and the design phase. Currently, the project is being field-tested in Penang. I understand you have had a chance to see for yourselves our efforts in Penang over the weekend when you were there. As expected, we had our teething problems but these, to a great extent, are being gradually overcome and I am confident that, before the end of this year, we should have overcome most of them. Barring any unforseen circumstances, we should be completing our test run soon. It is my fervent hope that we shall be able to launch upon a wider application of the test run activities and hence on to a nationwide adoption.
I hope this workshop has given all of you an ample opportunity over the past 10 days to exchange your experience as well as resolve some of the problems. I understand that you have had very lively discussions and the papers that have been presented have been of a very high order. Credit must be given to the WHO consultant and staff members for having given such valuable advice and guidance and for ensuring that high standards are maintained. Credit must also go to the participants themselves for having persisted through this taxing and tiring exercise and come up with the findings. We in Malaysia have definitely benefitted from the workshop and I hope, this will give us the added stimulus to continue and complete our own project.
- 58_
Annex 2.2
Before I conclude, I must give my personal thanks to WHO for its continued leadership and for choosing Kuala Lumpur for the venue of this workshop. I wish to thank the organizing committee also for shouldering its responsibilities in making the workshop run as smoothly as possible.
For those of you who have come from afar, I hope you have had a very pleasant stay and found time to sample a bit of traditional Malaysian hospitality, if not, I hope you come aga1n. You can rest assured that Malaysia will always welcome you.
Now, without further ado, I declare this workshop closed and wish all of you a safe return home. Thank you.
American Samoa
Australia
- 59 -
List of Participants, Observers, Temporary Adviser, Consultant and Secretariat
1. PARTICIPANTS
(1) Dr Julia L. Grach-Lyons Acting Director of Health,
ANNEX 3
Director of Maternal and Child Hea1th/ Crippled Children Services Program LBJ Tropical Medical Centre Pago-pago American Samoa 96799
(2) Mr John Cooper Assistant Commissioner (Planning) South Australian Health Commission 52 Pirie St. Adelaide 5000 Australia
People's Republic of China (3) Dr Enmei Zhang
Cook Islands
Statistics Division Planning and Finance Bureau Ministry of Public Health Beijin¥ People s Republic of China
(4) Dr Weixia Shen Institute of Parasitic Diseases Chinese Academy of Medical Sciences Shanghai People's Republic of China
(5) Mr Ngari Munokoa Health Statistics Officer Ministry of Health P.O. Box 300 Rarotonga Cook Islands
Annex 3
Guam
Hong Kong
Japan
Malaysia
New Hebrides
New Zealand
- 60 -
(6) Mrs Priscilla T. Maanao Deputy Administrator Guam Health Planning and Development Agency Suite 205 GCIC Bldg. Agana Guam 96911
(7) Mr Bernard Hung-sum Wong Senior Statistician Medical and Health Department Lee Gardens Hysan Avenue Hong Kong
(8) Dr Hisashi Ohmichi Medical Officer and Deputy Director Office of Medical Service System Development Medical Affairs Bureau Ministry of Health and Welfare 1-2-2 Kasumigaseki Chiyoda-ku Tokyo Japan
(9) Mr Yok Ching Chong Mathematician (Operations Research) Planning and Development Division Ministry of Health K-13, Jalan Duta Kuala Lumpur Malaysia
(10) Dr Chin Seang Chee Deputy Director (Health) Office of the Medical and Health Director Penang Malaysia
(11) Dr Frank Spooner Director of Health Ministry of Health Port-Vila New Hebrides
(12) Mr H.D. Evans Chief Executive Officer Review and Development Department of Health P.O. Box 5013 Wellington New Zealand
Papua New Guinea
Philippines
Republic of Korea
Singapore
Socialist Republic of Viet Nam
Tonga
Trust Territory of the Pacific Islands
- 61 -
Annex 3
(13) Dr B.D. Taukuro Assistant Secretary-Planning and Research Department of Health P.O. Box 2084 Konedobu Papua New Guinea
(14) Dr Teresita M. Bonoan Officer-in-Charge Division of Epidemiology Disease Intelligence Center Ministry of Health San Lazaro Compound Sta. Cruz Manila
(15) Miss So-Young Ahn Statistical Officer Division of Statistics Ministry of Health and Social Affairs 77 Sejong-Ro, Jongro-Gu Seoul Republic of Korea
(16) Mr Wai Him Tham Statistical Officer Medical Records Department Singapore General Hospital Singapore 0316 Republic of Singapore
(17) Dr Dinh duc Tien Director Institute of Medical Information Ministry of Health 13 Le Thanh Tong Hanoi Socialist Republic of Viet Nam
(18) Mr Penaia Moa Health Statistics Officer Ministry of Health Nuku'alofa Tonga
(19) Mr Rokucho F. Billy Public Health Statistician Bureau of Health Services Trust Territory of the Pacific Islands Government Headquarters Saipan CM 96950 Trust Territory of the Pacific Islands
Annex 3
Western Samoa
Workshop Director
- 62 -
(20) Mr Tipasa Me Health Planning and Information Officer Health Department Apia Western Samoa
2. OBSERVERS
Mr Mohd. Isa Mohd. Samat Information Scientist Tun Ismail Atomic Research Centre, 6, Jalan I/3K, Bandar Baru Bangi Selangor
Lt Kol (Dr) Long Seh Chin Armed Forces Hospital Terendak Melaka Malaysia
3. TEMPORARY ADVISER
Dr Ewe Seng Lim Deputy Director Division of Planning and Development Ministry of Health Jalan Duta Kuala Lumpur Malaysia
4. CONSULTANT
Dr Laurence A. Malcolm Principal Medical Officer (Research) and Head, Health Planning and Research Unit Department of Health Christchurch New Zealand
- 63/64 -
Annex 3
5. SECRETARIAT
Mr M. Anderson Technical Officer (Programme Management) Intercountry project on Health Planning and Management c/o The WHO Programme Coordinator P.O. Box 113 Suva Fiji
Mrs L.E. Brasilefto Secretary Health Information Unit WHO Regional Office for the Western Pacific P.O. 2932 Manila
Dr S.H. Mandil Director Information Systems Programme WHO Headquarters Geneva Switzerland
Dr K.M. Patwary Statistician, Intercountry project on Research Promotion and Development Institute of Medical Research Kuala Lumpur Malaysia
Mr M. Subramanian Operational Officer Regional Adviser in Health Information WHO Regional Office for the Western Pacific P.O. Box 2932 Manila
Mr K. Uemura Director Division of Health Statistics WHO Headquarters Geneva Switzerland
- 65 -
ANNEX 4
FINAL AGENDA AND LIST OF DOCUMENTS
AGENDA ITEM
No. Description
1 OPENING CEREMONY
2 SITUATIONAL ANALYSIS
2.1 Country situation
DOCUMENT
No. Title
WPR/HST/80.l Agenda
WPR/HST/80.1 Add.l Draft Agenda and List of Documents
WPR/HST/80.2
WPR/HST / 80 . 3
WPR/HST/80.4
Time Schedule
Objectives of the Workshop
List of Participants, Temporary Adviser, Consultant and Secretari a t
Health Information Systems for the Management of Health Services - questionnaires and/or country papers
WPR/HS'r/80.5-AMS American Samoa
WPR/HST/80.5-AUS Australia
WPR/HST/80.5-CHN China
WPR/HST/80.5-COK Cook Islands
WPR/HST/80.5-GUM Guam
WPR/HST/80.5-HOK Hong Kong
WPR/HST/80.5-JPN Japan
Annex 4
No.
2.2
3
3.1
AGENDA ITEM
Description
Regional Situation
NATIONAL HEALTH INFORMATION SYSTEMS (NHIS)
Overview
- 66 -
DOCUMENT
No. Title
WPR/HST/80.5-MAA Malaysia
WPR/HST/80.5-NEZ New Zealand
WPR/HST/80.5-PNG Papua New Guinea
WPR/HST/80.5-PHL Philippines
wPR/HST/80.5-KOR Republic of Korea
WPR/HST/80.5-SMA Western Samoa
WPR/HST/80.5-SIN Singapore
WPR/HST/80.5-TON Tonga
WPR/HST/80.5-PTT Trust Territory of the Paci fic Islands
WPR/HST/80.5-VTN Viet Nam
WPR/HST/80.6
WPR/HST/80.7
Health Information ln the Western Pacific Region -
. A Review
Report of the Interregjonal Consultation on NHIS, held ln San Jose, Costa Rica, 14-20 November 1979
No.
3.2
4
5
AGENDA ITEM
Description
.. 67 ..
No.
WPR/HST/80.8
WPR/HST/80.9
Annex 4
DOCUMENT
Title
Towards P~inciplea for NHIS, ISD/78/13 Rev. 4
Development of Health Information Systems, WHA31.20, 19 May 1978
WPR/HST/80.9 Add.l Managerial Process for Health Development, WHA3l.43,
WPR/HST/80.l0
24 May 1978
WHO(1979): Seminar on National Health Information Systems, WHO Chronicle, 33: 338-342
WPR/HST/80.l0 Add.l WHO(l979): National Heal th Information Systems in South-East Asia, WHO Chronicle, 33: 177-179
Health Management WPR/HST/80.11 HMISD Conceptual Phase Information System (HMIS) - Objective and Scope
HMIS - MANAGERS' WPR/HST/80.l2 PERSPECTIVE
HMIS - STATISTICAL WPR/HST/80.l3 SUPPORT AND ACTIVITIES
WPR/HST /80 • 14
National Health Information Systems - Health Planning and Management Aspects, by Dr Laurence A. Malcolm
The Role of Health Statistics in Health Information System Activities, by Mr K. Uemura
Final Report of the Rt8ional Seminar on Indicators Relevant to Maternal end Child Health, held in Manila, Philippines, fro~ 13-19 December 1978
Annex 4
No.
6
AGENDA ITEM
Description
HMIS - DF.VELOPMENTAL APPROACH AND RELATED TECHNOLOGICAL SUPPORT
7 HMIS TEST RUN
7.J Overview
7.2 Field visit to test run area - Penang
B HMIS DEVELOPMENT STRATEGY
8. 1 National Overall Strategy
B.2 Role of International Agencies
9 CLOSING CEREMONY
- 68 -
No.
WPR/HST /80.15
WPR/HST/BO.16
WPR/HST/BO.17
DOCUMENT
Title
Proceedings of the 6th SEAHIC Workshop, held in Kuala Lumpur, from 13-19 February 1979
Report of the Consultation on the Reorientation of the Health Statistics Programme, held 1n Geneva, from 1-5 May 197B
Viewgraphs on Towards General Principles for National Health Information Systems, by Dr S.H. Mandil
WPR/HST/80.17 Add.!
WPR/HST/BO.IB
WPR/HST /BO. 19
Information Bu9jetins: WPRHST/IB/l
WPR/HST/IB/2
WPR/HST/IB/3
WPR/HST/IB/4
WPR/HST/IIl/5
Viewgraphs on Data Rase Management, by Dr S.H. Mandi!
Test Run Strategy and Activi ties, by Dr Chee Chin Siang
HMISD Protocol
Information about the workahop
Provisional List of Participants, Temporary Adviser, Consultant, anQ Secretariat
List of Documents
Bibl iography
Working in r.roup~
_. __ 'c ___ ------------ '--------___ -L ________________ I
- 69 -
ANNEX 5
BIBLIOGRAPHY
Attached is a list of references, publications and documents, which are relevant in the development and management of Health Information Systems.
The contents are as follows:
1. Health Information Systems and Services - WHO documents issued for the Interregional Consultation on National Health Information Systems, San Jose. Costa Rica, 14-20 Nov~ber 1979 ••••••••••••••••••••••••••••••••••••••.•• 1
2. Other References ••.••••.••••••••..••••••••••••••••••••••••... 2
3. Modern Trends in Health Statistics ••••••••••••••••••••••••••• 3
4.
5.
Essential Reports, Documents and Publications and Useful References
Computers and Info~tion Systems ••••••••••••••••••••••.•..•.
ENCL.: Aa .~ ...
4
16
- 70 -
Annex 5
1. Health Information Systems and Services - WHO documents issued for the Interregional Consultation on National Health Information Systems, San Jose, Costa Rica, 14-20 November 1979
Rcpo~t - Interregional Consultation on National Health Information Systems, San Jose, Costa Rica, 14-20 November 1979 (doc. NHIS/IR/BO.l)
Towards Principles for National Health Information Systems (NHIS) (doc. NHIS/IR/79.4)
Information System - Organization and Functions @oc. NHIS/IR/79.S)
Development and Promotion of Health Information Systems in Egypt - Concept and General Strategy (doc. NHIS/IR/79.6)
Health Information System for Management of Health Services in the Philippines (doc. NHIS/IR/79.7)
Information Services 1n the Administration and Development of Health Care in the USSR (doc. NHIS/IR/79.B)
Health Information Systems: A review of developmental efforts in Indonesia ~oc. NHIS/IR/79.9)
Health Information Systems in Lesotho (doc. NHIS/IR/79.l0)
Relationship with National and International Information Systems (doc. NHIS/IR/79.INF.DOC.l)
Seminar on National Health Information Systems (doc. NHIS/IR/79.INF.DOC.2)
National Health Information Systems in South-East Asia (doc. NHIS/IR/79.INF.DOC.3;
Exploration of a common strategy for the development of health statistics for the use of national health services (doc. NHIS/IT/78.INF.DOC.4)
Seminar on vital and health statistics, Damacus, 18-25 September 1972 (doc. NHIS/IR/79.INF.DOC.5)
Basic concepts for the development of national health information systems (doc. NHIS/IR/79.INF.DOC.6)
Health information systems, Copenha~n, 18-22 June 1973 (doc. NHIS/IR/79.INF.DOC7)
Report on a consultative meeting on national health information systems Development. New Delhi, 18-22 December 1978 (doc. NHIS/IR/79.INF.DOC.8)
Report of the WHO consultation on the role of health statistics in studies of human reproduction and in family planning programmes (doc. NHIS/IR/79.INF.DOC.9)
Assistance to countries in planning and operating national health information systems (doc. NHIS/IR/79.INF.DOC.10)
New approaches in health statistics (doc. NHIS/IR/79.INF.DOC.ll)
Some health literature considerations in the decision of national health information systems (NHIS/IR/79.INF.DOC.12)
- 71 -
Annex 5 2. Other References
BLUMENTHAL, S.C., Management Information Systems: a Framework for Planning and Development, 1st ed. Prentice Hall, Inc., New Jersey, USA, 1969
gURCH, J.G., STRATER, F.R., Information Systems, Theory and Practice 1st ed., Hamilton Publishing Co., Santa Barbara, Calif., 1974 '
CARPENTER, R.G. (1978) A review of developed and developing computer applications in medicine, WHO Document HSM/MC/78.1
DAVIS, B.G., Management Information Systems, 1st ed., McGraw Hill, USA, 1974
DONABEDIAH, A., Specifying Requjrements for Health Care, 2nd ed., Harvard College, USA, 1974
FERRERO, C., Conceptos sobre sistemas de Informacion en Salud, working document ST-PLEV-SI No.3, 2nd version, PAHO/WHO, Lima, 1976
Health information systems: Meeting 10 February 1977. Proc. roy. Soc .. Med., 10, 701-708, 1977
LEVIN, R., KIRKPATRICK, Ch., Quantitative Approaches to Management, 2nd ed., McGraw Hill, USA, 1971
LINDLEY, D.V., Making Decisions, 2nd ed., John Wiley and Sons Inc., Great Britain, 1973
McKEAN, R.N., Efficiency in Government through System Analysis, 1st ed., John Wi! ey and Sons Inc., USA, 1958
MEADOW, Ch. T., The Analysis of Information Systems, 2nd ed., Melville Publishing Co., Los Angeles, Calif., 1973
National Institute of Mental Health, The Design of Management Information Systems for Mental Health Organizations, a Primer, 1st ed., US Department of Health, Education and Welfare, USA, 1976
Pan American Health Organization, Advisory Regional Committee on Health Statistics, Seventh Meeting, 1st ed., PAHO/WHO, Washington, DC, USA, 1976
SEAMIC (1976) Health information for national health planning in Southeast Asia.·· Proceedings of the Third Workshop, Singapore, 1976.
SEAMIC (1978) Health planning and health information in Southeast Asia. Proceedings of the Fourth Workshop, Bangkok, 1977.
SEAMIC (1978) Approaches to documentation and s~atistica1 informa~ion ~n primary health care. Proceedings of the F~fth Workshop, Man~la 1978
SUCHMAN, E.A., Evaluative Research, 8th ed., Russell Sage Foundation, .lISA ... 1974
VAN COURT HARE, Systems Analysis, A diagnostic Approach, 1st ed., Harcourt Brace and World Inc., USA, 1967
WHITE, K.L. et al. (1977). Health Services: Concepts and information for national planning and management. Public Health Papers No. 67. Geneva, WHO.
WHO. Regional Office for Europe: Information systems for health services J
Copenhagen, 1979
- 72 -
Annex 5
3. Modern Trends in Health Statistics
BAILEY, N. T.J. (1977) Mathematics, statistics and systems for health. Chichester, England, Wiley.
EeE (1977) Report of the Seminar on Statistical Services in Ten Years' Time, Wa~hington, D.C. 21-25 March 1977
HOLLAND, W.W. et aI, ed. (1979) Measurement of levels of health. WHO Regional Publications European Series No.7, Copenhagen.
SEAMIC (1979) The development of operational, with special reference to community. health. Workshop, Kuala Lumpur, 1979.
performance and impact indicators Proceedings of the Sixth
UN (1977) The organization of national statistical services: a review of major issues. Studies in Methods, Series F, No. 21 (ST/ESA/STAT/SER.F/21)
WHO (1971) Statistical indicators for the planning and evaluation of public health programmes. Techn. Rep, Ser. No. 472
WHO (1972) Statistical principles in public health field studies. Techn. Rep. Ser, No. 510
WHO (1974) New approaches in health statistics. Techn. Rep. Ser. No. 559
~lO (1978) Lay reporting of health information.
- 73 -
Annex 5
4. Essential Reports, Documents and Publications and Useful References
(For WHO publications: E: English, F = French, R " Russian, S = Spanish, E/F Ililingual edition, *under preparation).
4. I Slatititical series and analytical regorts
4. I. I Basi c data
World Health Statistics Annual (E/F)
Vol. I
Vol. II Vol. III
Vital statistics and causes of death Infectious diseases: cases and deaths Health personnel and hospital establishments
Mortality from malignant neoplasms, 1955-1966, Parts I and II, Geneva, WHO, 1970 (E/F)
Cancer incidence 1n five continents, UICC, 1966
Cancer incidence 1n five continents, Vol. II, UICC, 1970
Cancer incidence 1n five continents, Vol. III, IARC, 1976 (E)
Air quality in selected urban areas. 1973-1974. WHO Offset Publication No. (1976) (E, F)
30,
Air quality in selected urban areas. 1975-1976. WHO Offset Publication No. 41, (E, F)
Animal Health Yearbook. FAO-WHO-OIE (E/F/R) (latest issue: 1977)
Demographic Yearbook. United Nations (latest issue: 1977)
Statistical Yearbook. United Nations (latest issue: 1978)
Selected world demographic indicators by countries, 1950-2000. UN, 1975, (Document ESA/P/WP.55)
World Population trends and prospects by country, 1950-2000: summary report of the 1978 assessment. UN, 1979. (ST/ESA/SER.R/33)
World Health Statistics Quarterly (ElF)
Weekly Epidemiological Record (E/F)
Sixth Report on the World Health Situation, 1973-1977. Part 1: Global Analysis (in press); Part 2: Review by country and area. WHO, 1980, (E, F*, R*. S~,)
Health conditions lTI the Americas, 19·73-1976. PAHO/WHO, Sci. Publ. No. 364, 1978 (E, 5)
Ileal th services 1n Europe, 2nd ed., Copenhagen, IlliO, 1974 (E, F, R)
- 74 -
Annex 5
SELBY, P. Health in 1980-1990. A predictive study based on an international inquiry sponsored by the Henry Dunant Institute of the Red Cross, Geneva, and Sandoz Ltd., Basel. Basel, Karger, 1974.
Report on the world social situation. UN, 1978 (E/CN.5/557, ST/ESA/87)
PUFFliR, R.R. and WYNNE GRIFFITH , G •. Pattern of urban mortality: report of the Inter-American Investigation of Mortality. PAHO/WHO Sci. Publ. No. lSI, 1967 (E, S)
PUFFER, R.R. and SERRANO, C.V. Patterns of "mortality in childhood: report of the Inter-American Investigation of Mortality in Childhood. PAHO/WHO Sci. Publ. No. 262, 1975 (E, S)
A WHO report on social and biological effects on perinatal mortality, Vols. 1 and 2. Geneva, WHO, 1978 (E)
Health and the family: studies on the demography of family life cycles and their health implications. Geneva, WHO, 1978 (E)
Myocardial infarction community registers. Copenhagen, Public Health in Europe 5, WHO 1976 (E, F)
WHO/HS/NAT.COM. documents (E, F): Altogether, 366 documents were issued up to end 1979 on various topics relating to activities of national committees on vital and health statistics or equivalents and other national and international statistical studies.
~IO/HS/NAT.COM./74.325 gives a list of documents issued ~n this ser~es up to 1974.
4.2 WHO Expert Committees, Study Groups, etc.
WHO Technical Report Series No.5, 1950 (Report on the first session of the WHO Expert Committee on Health Statistics) (E, F)
WHO Technical Report Series No. 25, 1950 (Report on the second seSSion of the ~!O Expert Committee on Health Statistics) (E, F)
WHO Technical Report Series No. 53, 1952 (Third report of the WHO Expert Committee on Health Statistics) (E, F, S)
WHO Technical Report Series No. 85, 1954 (Report on the First International Conference on National Committees) (E, F)
WIlO Technical Report Series No. 133, 1957 (Fifth report of the WHO Expert Committee on Health Statistics) (E, F, S)
Imo Technical Report Series No. 137, 1957 (Measurements of the levels of health: report of a Study Group) (E, F, S)
WHO Technical Report Series No. 164, 1959 (Sixth report of the WHO Expert Committee on Health Statistics) (E,"F, S)
WHO Technical Report Series No. 218, 1961 (Health and morbidity surveys: seventh report of the WHO Expert Committee on Health Statistics (E, F, R, S)
- 75 -
Annex 5
WHO Technical Report Series No. 261, 1963 (Hospital statistics: eishth replHt of the WHO Expert Committee on Health Statistics) (E, F, R, S)
~!O Tcchnical Report Series No. 336, 1966 (Sampling methods in morbidity surveys and public health investigations: tenth report of the WHO Expert Committee on Health Statistics (E, F, R, S)
WHO Technical Report Series No. 365, 1967 (Epidemiological methods in the study of chronic diseases: eleventh report of the WHO Expert Committee on Health Statistics (E, F, R, S)
WHO Technical Report Series No. 389, 1968 (Morbidity statistics: twelfth report of the WHO Expert Committee on Health Statistics (E, F, R, S)
WHO Tecllnical Report Series No. 429, 19~9 (Statistics of health services and of their act1v1t1es: thirteenth report of the WHO Expert Committee
on Ilealth statistics) (E, F, S)
~!() Technical Report trends and levels: (E, F, R, S)
Series No. 440, 1970 (Programme of analysis of mortality report of a joint UN/WHO meeting, Geneva, 1968)
~!O Technical Report Series No. 466, 1971 (Methodology for family studies of genetic factors: report of a WHO Scientific Group) (E, F, R, S)
~IO Technical Report Series No. 472, 1971 (Statistical planning and evaluation of public health programmes: of the WHO Expert Committee on Health Statistics (E,
indicators for the fourteenth report
F, S)
WHO Technical Report Series No. 490, 1972 (Techniques for the collection and reporting of data on community water supply: report of a WHO Scientific Group) (E, F, S)
~IO Technical Report Series No. 559, 1974 (New approaches in health statistics: report of the Second International Conference of National Committees on Vital and Health Statistics) (E, F, S)
ECE/WHO.Second joint ECE/WHO meeting on health statistics, 1976 (Document CES/Ar.. 36/18, ICP/DHS 003/11) (E, F, R, S)
~!() Technical Report Series No. 587, 1976 (Statistical indices of family hC3lth: report of a WHO Study Group) (E, F, S)
~IO Technical Report Series No. 593, 1976 (Methodology of nutritional surveillance: report of a joint FAO/UNICEF/WHO Expert Committee) (E, F, S)
WHO Technical Report Series No. 632, 1979 (Cancer statistics: report of a ~I()/IARC Expert Cortnnittee) (E, F, S)
\~II() Ikconunendations and statements of WHO expert group in relation to health statistics (Document WHO/HS/NAT.COM/75.345) (E, F)
\{IIO Technical Report Series, No. 510, 1972 (Statistical principles in public health field studies: fifteenth report of the WHO Expert Committee Oil Health Statistics) (E, F, S)
- 76 -
Annex 5
4.3 Demography, epidemiology and health statistics - general
4.1.t Demo~raphy
UN Multilingual demographic dictionary. Population studies No. 29, 1958, (ST/SOA/Ser.A/29)
UN Principles and recommendations for a vital statistics system. 1973, (ST/STAT/SER.M/19/Rev. 1)
BENJAMIN, B. Health and vital statistics. London, George Allen & Unwin Ltd. 1968
BOGUE, D.G. Principles of demography, New York, Wiley, 1968.
PRESSART, R. Statistical demography. New York, Saint Martin's Press, 1978
SHRYOCK, H.S. and SIEGEL, J.S. Methods and materials of demography. 2 volumes. Washington, D.C., Department of Commerce and Census, 1971 (Revised editior in press)
4.3.2 Epidemiology
~IO Technical Report Series No. 365, 1967 (Epidemiological methods in the study of chronic diseases: eleventh report of the WHO Expert Committee on Health Statistics)
BENSON, A.S., ed. Control of communicable diseases ~n man, (An official report of the American Public Health Association, 12th ed.1975
ALDERSON, M. An introduction to epidemiology. London, Macmillan, 1976
HOLLAND, W.W. Data Handling in Epidemiology, Oxford Medical Publications, 1970
LILIENFELD, A. Foundationsof epidemiology. Oxford University Press, 1976
4.3.3 Health statistics, biostatistics, medical statistics and computing
BOURKE, G.J. & McGILVRAY, J. Interpretation and Uses of Medical Statistics, Oxford, Blackwell Scient. Publ., 1969
CARPENTER, R.G. in medicine.
A review of developed and developing computer applications WHO, 1978 (Do·cument HSM/MC/78.1)
COLTON, T. Statistics in medicine. Boston, Little Brown, 1974
CURIEL, D. et al. Trends in the study of morbidity and mortality. WHO Public Health Papers No. 27 (1965)
HILL, A.B. A short textbook of medical statistics, 10th ed., London, Hodder and Stoughton, 1977 (Previous editions had the title: Principles of Medical Statistics)
LEAVERTON, P.E. A Review of biostatistics (a programme for self-instruction), rowa, University of Iowa Press, 1973
- 77 -
Annex 5 ----LEDERMANN, S. Notions pratiques de statistique a l'usage du corps medical.
Documentation medica1e permanente du medecin praticien, Paris, 1956, No. 25
LEGAY, J. -M. et a1. Exercices de statis tique pour bio10gis tes, Paris, Flanmmrion, 1966
LOHBARD, O. Biostatistics for the health professions, New York, Appleton Century Crofts, 1975
MORTON, R. A study guide to epidemiology and biostatistics, Baltimore, University Park Press, 1979
SCHWARTZ, D. Methodes statistiques a t'usage des medecins et des biologistes, Paris, Flammarion, 1963
SEPETLIEV, D. & PASKALEV, T. Medizinska statistika. Sofia, Medicina i Fizkultura, 1968 (in Russian)
SWAROOP, S. Introduction to Health Statistics, Edinburgh & London, E.S. Livingstone, 1960
VALLERON, A. J. & LAZAR, P. Exercices progranunes de statistique a l'usage des medecins et biologistes. Paris, Flanunarion, 1966.
4.3.4 General statistics
CHEVRY, C.R. Pratique des enquetes statistiques, Paris, P.U,F., 1962
DIXON, W.J. & MASSEY, F.J. Introduction to statistical analysis. 3rd ed., New York, McGraw-Hill, 1969
FISHER, R.A. Statistical methods for research workers. 14th ed., Edinburgh, Oliver & Boyd, 1970
KENDALL, M.C. & BUCKLAND, W.R. A dictionary of statistical terms. Edinburgh, Oliver & Boyd, 1957'
KENDALL, M.G. & STUART, A. The advanced theory of statistics. Vol. 1: 4th cd., Vol. 2: 3rd ed., Vol. 3: 3rd ed., London, Griffin, 1977
SNEDECOR, C.W. & COCHRAN, W.G. Statistical methods. 6th ed., Ames, Iowa, Iowa State University Press, 1967
4.4 Methodology in health management and research
4.4. I flea 1 th management
I\J\ILI';Y. N.T.J. Mathematics, statistics and systems for health. Chichester, England, Wiley, 1977 (Wiley Series in Probability and Mathematical Statistic;)
IlAYLET, R. The selection of health indicators under specific conditions in the developing countries .. WllO, 1979 (Document IVHO/HS/NAT.COH./79.361) (E.
BROOKE, E.H. The current and future use of registers in health information systems. WHO Offset Publication, No.8 (1974) (E, F)
- 78 -
Annex 5
GRUNDY, F. & REINKE, W.A. Health practice research and formalized managerial methods. WHO Public Health Papers No. 51 (1973) (E, F, R, S)
BOLLAND, W.W., IPSEN, J. & KOSTRZEWSKI, J. Measurement of levels of health. WHO Regional Publication, European Series No. 7 (1979) (E)
LEOWSKl, J. Review and analysis of health and health-related indicators with emphasis on indicators for primary health care. WHO 1978, OJocument WHO/HS/NAT.COM/78.359) (E, F)
SLUCANKO, I.C. & CERKOVNYJ, G.F. Statistical information Ln the management of health services, Moscow, Medicina, 1976 (in Russian)
WHITE, K.L. et a1. Health services: concepts and information for national planning and managements. WHO Public Health Papers, No. 67 (1977) (E, F, S)
WILSON, J.M.G. & JUNGNER, G. The principles and practice of screening for disease. WHO Public Health Papers No. 34, (1968) (E, F, R, S)
HALL, T.L. & MEJIA, A. Health manpower planning: principles, methods, lssues. Geneva, WHO, 1978 (E, F, S)
4.4.2 Medical records
Study Groups on Hospital Medical Records, WHO, 1970 (Document WHO/HS/NAT.COM/ 70.252)
Research in the field of Routine Hospital Record Techniques. WHO, 1970 (Document WHO/HS/NAT. COM. /70.256)
Training of Doctors and Nurses in the Establishment and Use of M2dical Records. WHO, 1970 (Document WHO/HS/NAT.COM/70.257)
Training of Staff of Medical Record Departments. WHO, 1970 (Document WHO/HS/NAT.COM/70.258)
Requirements of Medical Records - The Clinician's Point of View. WHO, 197C (Document WHO/HS/NAT.COM/70.259)
Medical Record Linkage. Preventive Medicine.
The Method and its Importance for Clinical and WHO, 1971 (Document WHO/HS/NAT.COM/7l.272)
The Problem oriented Medical Record. WHO, 1972 (Document WHO/HS/NAT.CmI/72.28J)
The Role of the Medical Record Professional in the Development and Use of Health Statistics. WHO, 1975 (Document WHO/HS/NAT.COM/75.340)
Study Group on Primary Health Records. WHO, 1978 (Document WHO/HS/NAT.C0:1/78.357
Reporting, Processing and Using Data Generated from Non-hospital Health and Medical Records, WHO, 1979 (Document WHO/HS/NAT.CO~!/79.364)
II , I
I !
I I
J
- 79 -
Annex 5
**ACHESON, E.D. The Patient, His Record and Society. Medical Journal of Australia, l, No.7, 1972
BENJAMIN, Bernard, ed., Medical Records. London: William Heinemann Medical Books, 1977
**FEINSTEIN, Alvan R. The Problems of the "Problem Oriented Medical Recurd". Annals of Internal Medicine, 1973
HUFFMAN, Edna K. Medical Record Management, 6th ed., Berwyn, Illinois: Physicians' Record Company, 1972
* *MONSON , Roberta A. The POMR and the Physician. Hospitals, Journal of the American Hospital Association, ~, 1975
**TUFO, Henry M. & SPEIDEL, Joseph H. Problems with Medical Records. Medical Care. November-December 1971
AMERICAN HOSPITAL ASSOCIATION Medical Record Departments 1n Hospitals - Guide to Organization. Chicago: AHA, 1972
4.4.3 Confidentiality of patient health information
BALDWIN, J.A., LEFF J. & WING, J.K. Confidentiality of psychiatric data 1n medical information systems. Br. J. Psychiatry 128, 417-27, May 1976
BERNSTEIN, A.H. Unauthorized disclosure of confidential information. Hospitals 48 (21), 126, 128, 130, Nov. 1974
BRITTON, A.H. Rights to privacy in medical records. J. Leg. Med. l. (7), 30-7 July-Aug. 1975
HIRSH, H.L. Medicolegal implications of medical records. Leg. Med. Annual, 171-88, 1975
4.4.4 International health classifications and nomenclature
WHO. Manual of the international statistical classification of diseases, injuries and causes of death, Ninth Revision. Vols 1 and 2. 1977. (E,F,R~S*)
WHO. Basic tabulation list with alphabetical index. 1978 (E,F~S*)
WHO. International classification of procedures in medicine. Vols 1 and 2, 1978. (E,F~')
WHO. International classification of diseases for oncology, 1976. (E.F,S)
WHO. Application of the international classification of diseases to dentistry and stomatology (ICD-DA), 1978. (E,F)
** Available in Spanish from PAHO/AMRO
- 80 -
Annex 5
WHO. International classification of impairments, disabilities and handicaps, 1980 (E,F*)
WHO. Lay reporting of health information, 1978 (E,F,S)
World Organization of National Colleges, Academies, and Academic Associations of General Practitioners/Family Physicians (WONCA). International classification of health problems in primary care, 2nd ed. ICHPPC-2, 1979.
RUTTER, M., et al. A multi-axial classification of child psychiatric disorders. Geneva, WHO, 1975. (E,F)
WHO. Mental disorders: glossary and guide to their classification in accordance with the Ninth Revision of the International Classification of Diseases. 1978 (E,F)
croMS. International nomenclature of diseases, Vol. III. Diseases of the lower respiratory tract. 1st ed. 1979.
Course for the reorientation of trained Instructor's notes. Part 1: General. V30PCS 7/77 London, WHO and Office of
4.4.5 Survey methodology
coders to the use of lCD-9. Part 2: Mortality. Part 3: Morbidity.
Population Census & Surveys (E)
ARMITAGE, P. National health survey systems in the European Economic Community. Luxembourg, Commission of the European Communities, 1977.
COCHRAN, W.G. Sampling techniques. 3rd ed., London, Wiley, 1977.
KlSH, L. Survey sampling. London, Wiley, 1965.
U.S. National Health Planning Information Center: references on methodologies for community health Springfield, Aspen Syst. C., 1977.
4.4.6 Health economics
Selected bibliography/ status assessment.
ABEL SMITH, B. Paying for health services: a study of the costs and sources of finance in six countries. WHO Public Health Papers No. 17 (1963).
ABEL SMITH, B. An international study of health expenditure and its relevance for health planning .. WHO Public Health Papers No. 32 (1967)
BRUNET-JAILLY, J. Essai sur l'economie generale de la sante. Pa~is, Cujar, 1971
COOPER, M.H., and CULYER, A.J. Health Economics: Selected readings. London, Penguin Books, 1973
- 81 -Annex 5
FELDSTEIN, M.S. Economics analysis for health serv~ce efficiency. Amsterdam, North Holland, 1967.
JOLLY, D. Economie de la sante: bibliographie choisie et annotee. Paris, Dunod, 1977.
LEVY, E. et a1. Economie du systeme de sante. Paris, Dunod, 1975.
LEVY, E. et a1. Evaluer Ie coilt de la maladie. Paris, Dunod, 1977.
RVSCH, G. Economique medicale. Paris, Flammarion, 1973. ;
RVSCH, G. Un systeme statistique repondant a l'etude et a la conduite de l'economie sanitaire. Geneva, WHO, 1979. (Document WHO/HS/NAT.COM./79.363 (E, F)
TRIOMPHE, A. Economie medicale. Paris, Heures de France, 1975.
WHO. Health Economics. WHO Public Health Papers No. 64 (1975)(E, F, S)
4.4.7 Research methodology
ARMITAGE, P. Sequential medical trials. Thomas, Springfield, Ill., 1960
ARMITAGE, P. Statistical methods in medical research. Oxford, Blackwell Scientific Publications, 1971.
BAILEY, N.T.J. The mathematical theory of communicable diseases. 2nd ed., London, Griffin, 1975.
CHIANG, C.L. Life table and mortality analysis. Geneva, WHO, 1978 (E)
COCHRAN, W.G. and COX, G.M. Experimental designs. 2nd ed., New York, Wiley, 1957.
COX, D.R. Planning of experiments. New York, Wiley, 1965.
DAVID, H.A. Methods of paired comparisons. New York, Hafner, 1963.
FINNEY, D.l. Statistical method in biological assay. 3rd ed., London, Griffin, 1978.
FISHER, R.A. and YATES, F. Statistical tables for biological agricultural and medical research. 6th ed., London, Longman, 1974.
HILL, A.B. Controlled clinical trials. Thomas, Springfield, Ill., 1960.
PLACKETT, R.L. Principles of regression analysis. New York, Oxford University Press, 1960.
POLLOCK, T.M. Trials of ~ro~hylactic agents for the control of communicable diseases. WHO Monograph Ser. No. 52 (1966) (E, P, R, S)
- 82 -
Annex 5
SCHEFFE, H. The analysis of variance. New York, Wiley, 1959.
SIEGEL, S. Nonparametric statistics for the behavioural sc~ences. New York, McGraw-Hill, 1956.
WHO. Adequacy of sample size (Document HSM/73.1) (E)
WHO. Manual of mortality analysis: a manual on methods of analysis of national mortality statistics for public health purposes. 1977 (E)
4.5 Practical guidelines on statistical methods for specific health problems
4.5.1 Communicable diseases
TARIZZO, M.L., ed. Field methods for the control of trachoma. Geneva, WHO, 1973 (E, F, R)
UEMURA, K. Statistical methods. In: Epidemiology and control of schistosomiasis (Bilharziasis). Basel, S. Karger, 1973
SWAROOP, S, Statistical methods in malaria eradication. WHO Monograph Series, No. 51 (1966) (E, F, R, S)
4.5.2 Nutrition
DE VILLE DE GOYET, C., et al. The management of nutrirional emergencies in large populations. 1978
Nutritional status of populations: A manual on anthropometric appraisal of trends. WHO, 1970 (Document WHO/NUTR/70.l29) (E, F)
SOMMER, A. Field guide to the detection and control of xerophthalmia. Geneva, WHO, 1978 (E, F, S)
4.5.3 Maternal and child health
A growth chart for international use ~n maternal and child health care: Guidelines for primary health care personnel. Geneva, WHO, 1978 (E, F)
4.5.4 Noncommunicable diseases
Oral health surveys. Basic methods. 2nd ed., Geneva, WHO, 1977.
~IO Handbook for standardized cancer registries. Geneva, WHO Offset Publication, No. 25 (1976) (E, F)
MACLENNAN, R., et al. Cancer registration and its techniques. Lyon, rARC Sci. Publ., No. 21 (1978) (E)
- 83 -
Annex .5
ROSE, G.A. and BLACKBURN, H. Cardiovascular survey methods. WHO Monograph Series, No. 56 (1968) (E, F, R, S)
The epidemiology of road traffic accidents. Copenhagen, WHO Regional publications, European Series, No.2 (1976) (E, F)
4,5.5 Mental health
REID, D.D. Epidemiological methods in the study of mental disorders. WHO Public Health Papers No.2 (1960) (E, F, R, S)
KRAMER, M. Application of mental health statistics. Geneva, WHO, 1969 (E, F, R)
LIN, T.Y. and STANJLEY, C.C. The scope of epidemiology in psychiatry. WHO Public Health Papers No. 16 (1962) (E, F, R, S)
4.5.6 Other
ANDERSON, K.L. et al. Habitual physical activity and health. Copenhagen, WHO Regional Publications, European Series No.6, (1978) (E, F)
4.6 Education and training ~n health statistics and related subjects
Inter-regional Conference on the training of health statistics personnel, Kampala, 1968 (with emphasis on intermediate level), WHO, 1968 (Document (WHO/HS/NAT.COM/68.238)
Consultation on Education and Training in Health Statistics, 1971, WHO, 1972 (Document WHO/HS/NAT.COM/72.286)
Directory of health statistics training courses in WHO Hember States WHO, 1973 (Document WHO/HS/NAT/COM/73.300) (E, F) (follow-up in preparation)
Travelling Seminar for Teachers of Vital and Health Statistics, UK/USA, 1973. WHO, 1974 (Document WHO/HS/NAT.COM/74.3l7) (E, F)
~)rkshop on educational issues for teachers of health statistics and related subjects, Cardiff, UK, 1977. WHO, 1979 (Document WHO/HS/NAT.COM/ 79.362) (E, F)
LOWE, C.R. and LWANCA, S.K., ed. Health statistics: teachers c.f medical students. A Handbook sponsored Oxford, Oxford University Press, 1978 (E, F)
a manual for by the lEA and WHO.
~IO. Health Statistics and Medical Students: A guide for teachers (In preparation)
The successful teaching of statistics to every medical student (conclusions and recommendations of an inter-regional conference held in Pakistan, 1978) rEA/WHO publication, 1979 (E)
- 84 -
Annex 5
Ep idemio logy: A Guide to Teaching Methods. lEA/WHO sponsored, Church ill 1. i vings tone, Edinburgh
4.7 Others
UN, 1'l7,). Dirpctory of international statistics (ST/ESA/STAT/SER.M/56)
UN, 1977. Integrated list of statistical questionnaires (E/CN.31AC.l/R4)
- 85 -
Annex 5
5. Computers and Information Systems (All publications are from John Wiley & Sons, Inc. unless otherwise indicated.)
Adam~, J.M. and Iladen, D.J.
Adams, J.M. and Haden, D.J.
Albrecht, R. L., Finkel, L. 811d nrown, J .R.
Anger, A.L.
Rnnk~, P.M. and Doupnik, J.
Rarns, A. and Porat, 0.1.
flrnwn, P.J.
Cardenas, A.F., Martin, M.A. and Presser, L.
Schriher, T.J.
Armstrong, J.S.
Arnold, R.R., Hill, H.C. and Nichols, A.V.
Reckpr, H. B.
R"er, S.
Bel'f, S.
Sisson, R.L. and Canning,R.G.
Ma 1 i, P.
Easton, Allan
Social Effects of Computer Use and tHsuse
Computers: Appreciation, Applications: An Introduction
Rasic 2nd ed. (Wiley Selfteaching Guides)
Computer Science: The pL/I Language
Introduction to Co~puter Science
Introduction to Microcomputers and Microprocessors •
Macroprocessors: And Techniques for Portable Software (Wiley Series in Computing)
Computer Science
Fundamentals of Flowcharting
Long-range Forecasting: From Crystal Ball to Computer
Modern Data Processing, 3rd ed.
Functional Analysis of Information Networks: A Structured Approach to the Data Communications Environment (Business Data Processing: A Wiley Series)
Decision and Control: The Meaning of Operational Research and Management Cyhernetics
Platform for Change
Computer Applications
How to Manage hv Objectives
DeCision Making
Annex 5
l)f'cl<l'r, R.S.
Donald, A.C.
E i lon, S.
E lIon, S.
Garrett
Rlalock, H.M.
Hill, A.B.
Cochran, W.G.
Kish, I..
Jess .. n, R.J.
Finney, D.J.
Kendall, H.G.
Siegel S.
Hills, M.
Armitage, P.
Railey, N.T.J.
Rourke, G.J. and McGilvray, J.
Daniel, W.W.
Dunn, O.J.
- 86 -
The DP Security Came, Fundamentals of Data Processing Security
Management, Information & Systems
Aspects of Management
Management Control
Hospital Computer Systems and' Procedures
Social Statistics
A Short Textbook of Medical Statistics
Sampling Techniques
Survey Sampling
Statistical Survey Techniques
The Theory of Experimental Design
Rank Correlation Methods
Nonparametric Statistics for the Behavioral Sciences
Statistics for Comparative Studies
Stat tsrical Methods in Medical Resl Irch
Mati !IIIatics, Statistics and S ys t !illS for Hea 1 th
Interpretation and Uses of Medi~al Statistics
Bio!'tatistics: for \na lys is in Sci{ lces
A Foundation the Health
Basjc Statistics: A Primer for the Bioredical Sciences
c: ros sman, S. I. and TIJrn('r, J.E.
lIill, A.II.
Routh, .J. 1.
Armitage, P.
Bailey. N. T.J.
lIail<,y, N.T.J. and Thompson, M.
dl' Jonge, II.
Emmens, C.W.
Feinstein, A.R.
Finnt"y, D.J.
J a za t d, N. T •
Kilpatrick, S.J.
Wilts, L.J.
Cox, P.R.
Marks, E.S.
Pollard, A.H., ~!!
Sundgren, C.
Olle, T.W.
- 87 -
Annex 5
Mathematics for the Biological Sciences
Statistical Methods in Clinical and Preventive Medicine
MathPmatical Preparation for the Health Sciences
Sequential Medical Trials
The Mathematical Theory of Communicable Diseases
Systems Aspects of Health Planning
Quantitative Methods in Pharmacology
Principles of Biological Assay
Clinical Judgment
Probit Analysis
Approaches to the Development of Health Indicators
Statistical Principles in Health Care Information
Medical Survey~ and Clinical Triale
Demography
Population Growth Estimation: A Handbook of Vital Statistics Measurement
Demographic Techniques
Theory of Data Rases
Current and Future Trends in Data Base Hanagement
Annex 5
RlIckley, J .W., Sharp, 0.1.. Nagaraj, M.R. & Schench, J.
Cagan C.
Copeland, R.M. & Dascher, P.E.
Couger, J.D. & Knapp, R.W.
Couger, J.D. ~Id McFadden,F.
Fitzgerald, J. & Eason, T.S.
Fitzgerald, J.tI. & Fitzgerald, A.I'.
Maciariello, J.A.
Makridakis, S. & Wheelwright, S.C.
Mambert, W.A.
Myers, G.J.
Sargent, H.
Schellenberger, R. & Roseman, F .G.
sprowls, R.C.
Stern, R. and ~lern, N.
- 88 -
Management Problem Solving with APL
Data Management Systems
Student Study Guide for Managerial Accounting: An Introduction to Planning Information Processing & Control
Systems Analysis Techniques
Introduction to Computer Based Information Systems
Fundamentals of Data Communications
The Fundamentals of Systems Analysis
Program-Management Control Systems
Forecasting: Method. and Applications
Effective Presentation: A Short Course for Professional.
The Art of Software Testing
Fishbowl Management: A Participative Approach to Systematic Management
Policy Formulation and Strategy Management
Management Data Bases
Principles of Data Processing
SLsson, R.L. & Canning, R.C.
Thierauf, R.J. Klekamp,R.C. & Geedtng, D.W.
Toan, A.B.
Walton, T.F.
Weaver, B.N. & Bishop, W.L.
White, D.J.
Wren, D.A.
Wren, D.A. and Voich, D.
Yu ill, B. F.
- 89/90 -
Annex 5
Computer Applications: A Short Course for Non-EDP Hanagers
Hanagement Principles "and Practices: A Contingency and Questionnaire Approach
Using Information to Hanage
Communications and Data Mana&ement
The Corporate Memory: A Profitable And Practical Approach to Information Hanagement and Retention Systems
Decision Methodology
The Evolution of Hanagement Thought
Principles of Management: Process and Behavior
Organizations and Management
- 91 -
SUMMARY OF EVALUATION ON THE REGIONAL WORKSHOP ON NATIONAL HEALTH INFORMATION SYSTEMS
Kuala Lumpur. Malaysia 16 - 25 June 1980
An evaluation questionnaire was distributed to each of the
ANNEX 6
20 participants of this workshop. All 20 participants completed the questionnaire and information furnished was used to assess the results and conduct of the workshop.
The responses to most of the queries in the evaluation questionnaire requiring yes/no answers are tabulated in Annex 1. The "yes" replies indicate favourable answers. A column on "no" answer was added in Annex lao The detailed reponses of the participants to these questions are contained in Annex lb.
The objectives of the workshop were:
(a) To exchange views and information on the present status of the health information systems in countries in the WHO Western Pacific Region;
(b) To identify problems related to existing health information systems supporting the planning, management and evaluation functions of ministries/departments of health;
(c) To establish a framework for a national health information system to serve managerial functions and explore alternative strategies for its development;
(d) To consider the role of international agencies in the promotion and development of national health information systems.
The above-mentioned objectives of the workshop had been achieved according to 92.6% of the replies, not achieved, 3.7% and no answer, 3.71. Six respondents (30.0%) felt that there were more efficient ways to achieve the workshop objectives such as:
providing the participants with the main papers of the workshop before its start;
suggesting more examples of systems and plain forms;
conducting the workshop at country level and involving participants from the high level of the Ministry;
scheduling the field trip half-way through the workshop;
preparing a manual on the establishments, operation and function of the HMIS.
Favourable comments on the new skills and concepts discussed in the workshop were as follows: new skills or concepts have been learnt by the participants (95.0%) and these skills can be applied in their country (85.0%) •
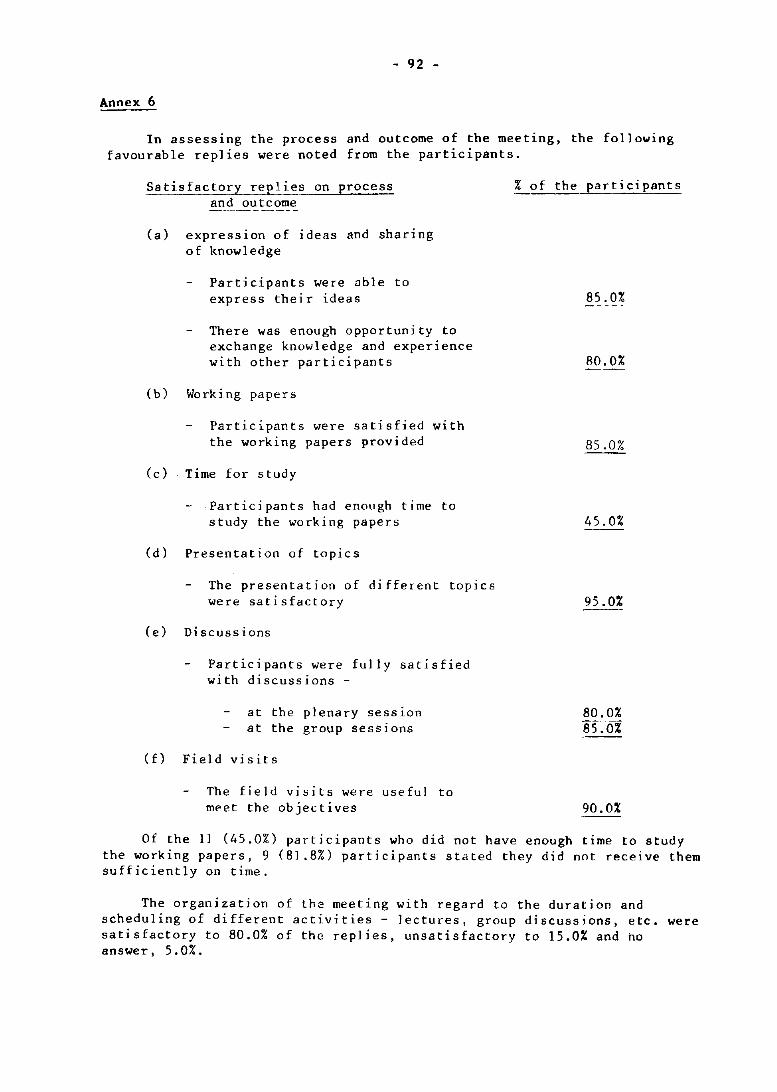
- 92 -
Annex 6
In assessing the process and outcome of the meeting, the following favourable repl ies were noted from the participants.
Satisfactory replies on process and outcome
(a) expression of ideas and sharing of knowledge
Participants were able to express their ideas
There was enough opportunity to exchange knowledge and experience with other participants
(b) Working papers
Participants were satisfied with the working papers provided
(c) Time for study
Participants had enough time to study the working papers
(d) Presentation of topics
The presentation of different topics were satisfactory
(e) Discussions
Participants were fully satisfied with discussions -
at the plenary seSS10n at the group sessions
(f) Field visits
The field visits were useful to meet the objectives
% of the participants
85.0%
80.0%
85.0%
4S .0%
95.0%
80.0% 85~O%
90.0%
Of the 11 (45.0%) participants who did not have enough time to study the working papers, 9 (BI.B%) participants stated they did not receive them sufficiently on time.
The organization of the meeting with regard to the duration and scheduling of different activities - lectures, group discussions, etc. were satisfactory to 80.0% of the replies, unsatisfactory to 15.0% and ho answer, 5.0%.
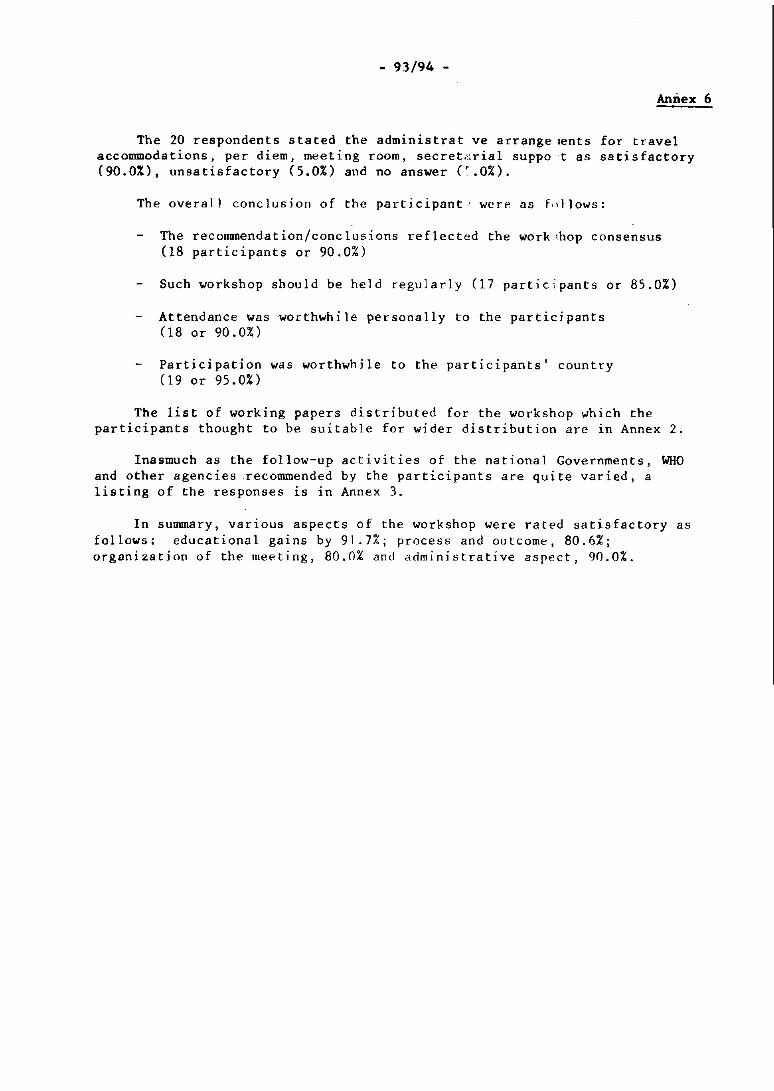
- 93/94 -
Annex 6
The 20 respondents stated the administrat ve arrange lents for travel accommodations, per diem, meeting room, secret;o;rial suppa t as satisfactory (90.0%), unsatisfactory (5.0%) and no answer (' .0%).
The overall conclusion of the participant' wcre as f.,llows:
The recommendation/conclusions reflected the work ,hop consensus (18 participants or 90.0%)
Such workshop should be held regularly (17 participants or 85.0%)
Attendance wasworthwh i Ie personally to the partici pants (18 or 90.0%)
Participation was worthwhile to the participants' country (19 or 95.0%)
The list of working papers distributed for the workshop which the participants thought to be suitable for wider distribution are in Annex 2.
Inasmuch as the follow-up activities of the national Governments, WHO and other agencies recommended by the participants are quite varied, a listing of the responses ~s ~n Annex 3.
In summary, various aspects of the workshop were rated satisfactory as follows: educational gains by 91.7%; process and outcome, 80.6%; organization of the meeting, 80.0% and administrative aspect, 90.01.
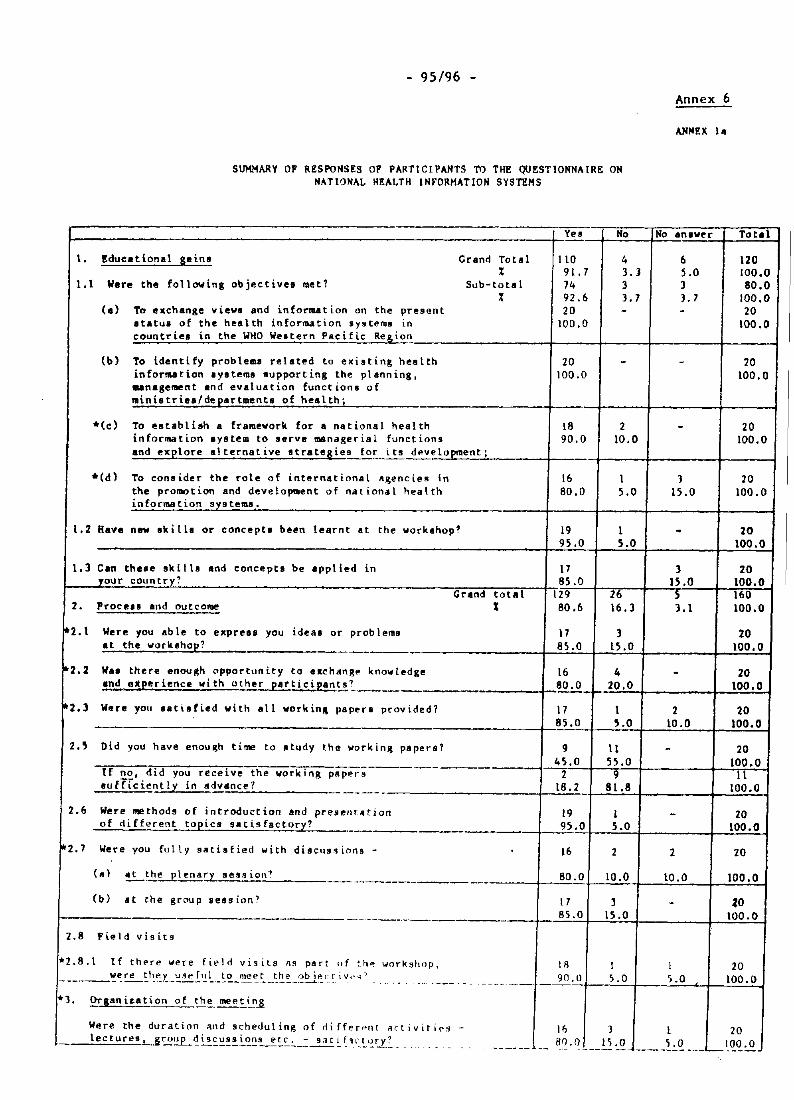
- 95/96 -
SUMMARY OF RESPONSES OF PARTICIPANTS TO THE QUESTIONNAIRE ON NATIONAL HEALTH INFORHATION SYSTEMS
Yel No
1. Educe tiona I saina Grand Total 110 4 % 91.7 3. J
1.1 Were the following objective. met? Sub-total 74 3 % 92.6 3.7
(a) To ""change view. and infonut ion on the present 20 -• tatul of the hea lth in forru t ion 'Y9temll in 100.0 countries in the WHO Wei tern Pac i f ic ReS!lon
(b) To identify prob lema related to exi.ting health 20 -inforlUtion ,y"t"ma lupporting the planning, 100.0 unage"",nt and evaluation funct Lonl of mini.tri.a/de~artment. of health;
*(c) To establiah a framevork for a national hea lth 18 2 in forma t ion Iystem to serve manager is 1 funtt iong 90.0 10.0 and exelore alternative etrate&ie9 for it! deve topment ;
*(d) To consider the role of international Agencies in 16 1 the prorDOt ion and development of national hea 1 th 80.0 5.0 info("l'lUItion sl9tems.
l. 2 Ha.,. new ok ill. ar concepti been learnt at the workahop? 19 I 95.0 5.0
1.3 Can thue sk it ta and conceptI be applied in 17 your countr_y? 85.0
Grand total 129 26 2. Procell!l and outc01'lle I 80.6 \6.1
*2.1 Were you ab Ie to ."pre .. you ideas or problema 17 3 at the vork.hop? 85.0 15.0 ._-
·2.2 W .. there enough opportunity to exchangp. knowledge 16 4 .nd e~eerience vi th other patt iei I!an~.~ '~ ___ 80.0 20,0
'2.3 Were you .. tiofled vith .11 "orkin~ paper. provided? 17 1 85.0 5.0
2.5 Did you have enou ~h time to study the "orkin~ paper.? 9 11 45.0 55.0
If no, did you receivl! the working papp.r s 2 9 ou ff (dent 1 y in advance? 18.2 81.8 --.--- -
2.6 Were me thod. of in troduct ion and present" tion 19 I of <Ii fferent topics sa t is fac tory? 95.0 5.0 -.-- ----
102.7 Were you fu 1 \ Y s8tisfied "i th ditJcu9~ion9 - 16 2
(. ) ~~~~~ sess iOI\~ 80.0 10.0 --... - .~.---------------(b) at the group sess ion? 17 J
85.0 15.0 ---,-----_._--2.8 Fiel d visits
*2. 8. \ If thpre were fi~ 1 d vi fi i l s ." part or thp. workshop, \ R 1 ___ ~,:~~t~t::.r.. __ ':.."P ~,~ ~_~~_~-:~~_~~:._~~i~~.~. i v,· 'l" - .... - . . --- 90.0 5.0 ---_.-._---,-_. *3. Orl4ni~ation of the meet~n-s
Were the durat ion and schedul ing of rli ff(,[Prlc RctivitiC':9 - 16 3
Annex 6
No anlve-r Total
6 120 5.0 100.0 3 80.0 ),7 100.0 - 20
100.0
- 20 100.0
- 20 100.0
3 20 15.0 100.0
- 20 100.0
3 20 15.0 100.0 S 160 3.1 100.0
20 100.0
- 20 100,0
2 20 LO .0 100.0
- 20 100.0
11 100.0
- 20 100.0
2 20
10.0 100.0
- %0 100.0
1 20 '0.0 100.0
1 20 lee tures L..&t"ouP _~i!.:.~!!i.'?~~!.~~~_.:2..:~ ~'~'~.<':'~ ~~.~_ .. . . ------- -.- 8~·12 ___ ~ ~Q. ____ ~'_Q. ___ L_l.<!.<!.o!!.
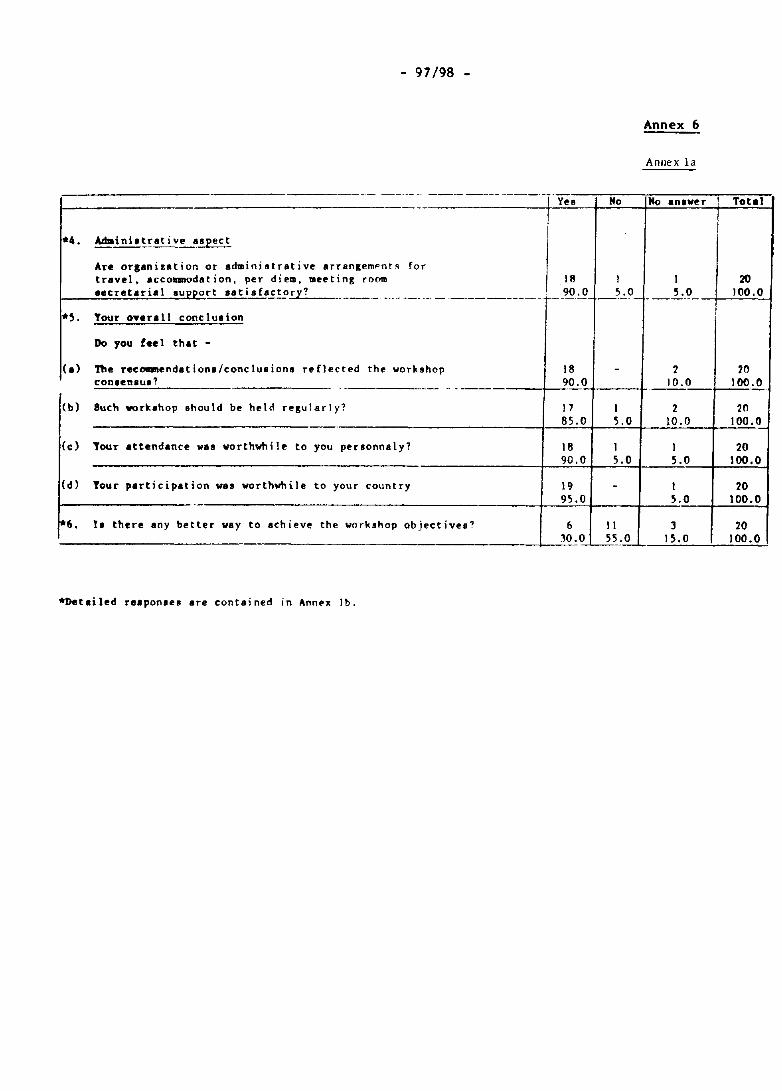
- 97/98 -
Annex 6
Anllex la
.- --.. -. -_.- ---- .. ---.--.--~,,----,-:::-----:--=~,..... Y~s No No .nlv~r ! Total
I----------------------·------+-!:~-I-~-~~=.!.-~=~
*4. Adainiltrative aspect
Ar@ orlanization or administrative arr8ngempnt~ for travel, accommodation, per diem, meeting room 18 I 20 eecr~tarial.u ort eat i. facto.:.r ... y..;? _________ .. __ .. __ ---------.-r--~'.Q 5 .0 __ .1:.()_ ~~!.:I O~O'.!'~0-1
*~. Tour o.erall conclulion
Do you teel that -
(a) The recommend.tionl/conclusion. reflected the workshop con,en.us?
(b) Such work.hop ohould be held resularly?
18 ______ -1----".90. O~.---+
J7 I
1 20 10.0 100.0 -----
2 20 8 5 .~O+--~!.::...+----!.~~+-!.:::.:'.!. 5.0 10.0 100.0
(c) Tour attendance was vorthvhi Ie to you personnaly?
(d) Tour participation was worthwhile to your country
6. II there any better way to achiev~ the work.hop objectives?
18 90.0
19 95.0
6 . __________________ ~~JO.O
*Detailed reaponlel are contained in Ann~x lb.
I 5.0
11 55.0
I 20 5.0 100.0
I 20 5.0 100.0
3 20 15.0 100.0
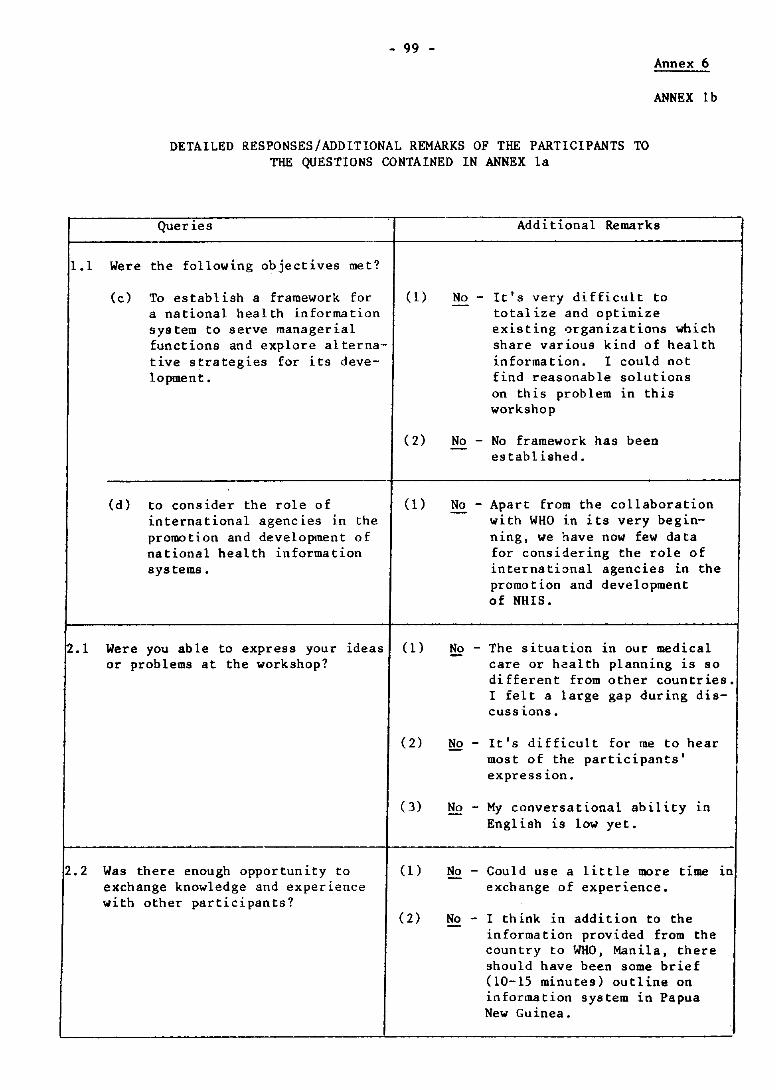
- 99 -Annex 6
ANNEX lb
DETAILED RESPONSES/ADDITIONAL REMARKS OF THE PARTICIPANTS TO THE QUESTIONS CONTAINED IN ANNEX la
Queries
1.1 Were the following objectives met?
(c) To establish a framework for a national health information system to serve managerial functions and explore alternative strategies for its development.
(d) to consider the role of international agencies 1n the promotion and development of national health information systems.
(1)
(1)
Additional Remarks
No - It's very difficult to totalize and optimize existing organizations which share various kind of health information. I could not find reasonable solutions on this problem 1n this workshop
No - No framework has been - established.
_No_ - Apart from the collaboration with WHO 1n its very beginning, we have now few data for considering the role of international agencies Ln the promotion and development of NHIS.
2.1 Were you able to express your ideas (1) or problems at the workshop?
No - The situation ln our medical care or health planning lS so different from other countries. I felt a large gap during disCUSSlons.
2.2 Was there enough opportunity to exchange knowledge and experience with other participants?
(2) No - It's difficult for me to hear most of the participants' expression.
(3) No - My conversational ability 1n English 1S low yet.
(1) No - Could use a little more time in exchange of experience.
(2) No - I think 1n addition to the information provided from the country to WHO, Manila, there should have been some brief (10-15 minutes) outline on information system in Papua New Guinea.
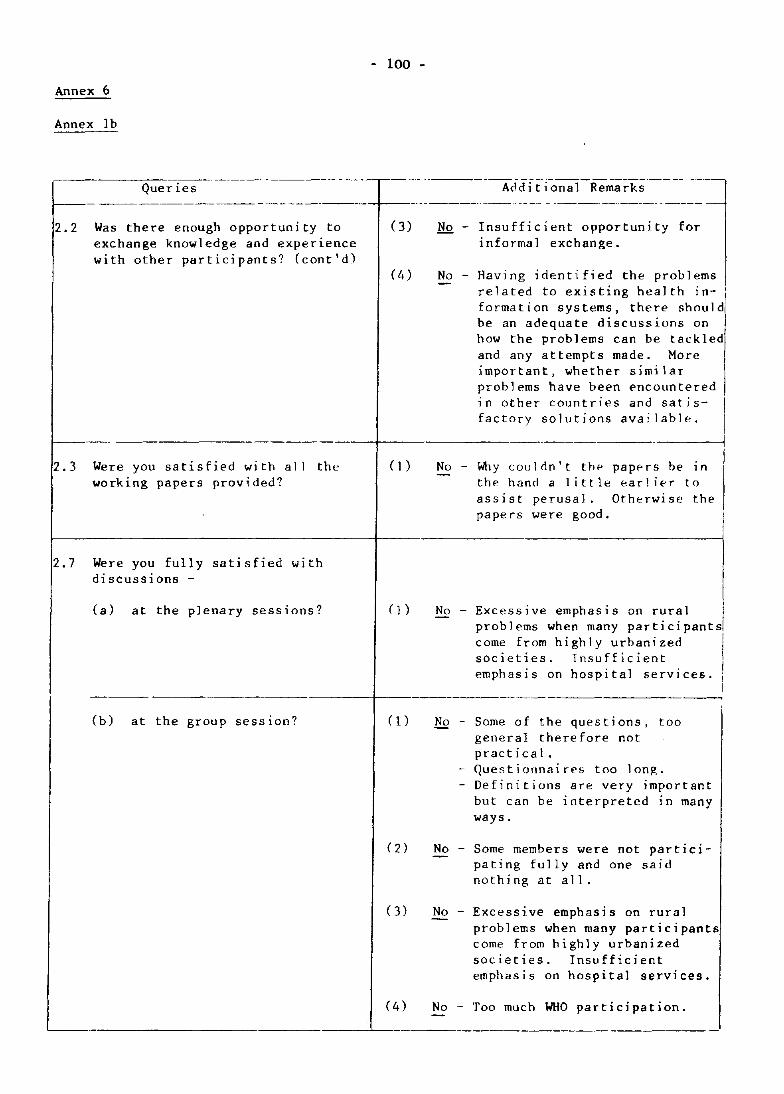
- 100 -
Annex 6
Annex Ib
Quer ies --~---~-----,--- ---~~---AddTtTon:;;]Rema~ks--- ---~
r--- ---------- -~----------+-------------- -~------ - ------------------
2.2 Was there enough opportunity to exchange knowledge and experience with other participants? (cont'd)
(3) No - Insufficient opportunity for informal exchange.
0.) No - Having identi fied the problems related to existing health in- i formation systems, there should' be an adequate discussions on how the problems can be tackled and any attempts made. More important, whether similar problems have been encountered 1 n other countri es and sat i s- I factory solutions available.
r--------------------------------+-------------------------------------4
2.3 Were you satisfied wi th all working papers provided?
the
2.7 Were you fully satisfied with discussions -
(a) at the plenary sessions?
(1)
( I )
No - Why couldn't th .. papers be 1n the hand a little earlier to assist perusal. Otherwise the papers were good.
No - Excessive emphasis on rural problems when many participants come from highly urbanized I societies. Insufficient I emphasi s on hospi tal servi ces. j
i ------------------------+-~------------------------------
(b) at the group session? (1)
(3)
(4)
No - Some of the questions, too general therefore not practical.
- Questionnaires too long. - Definitions are very important
but can be interpreted ln many ways.
No - Some members were not participating fully and one said nothing at all.
No - Excessive emphasis on rural --problems when many participants come from highly urbanized societies. Insufficient emphas i s on hospital services.
No - Too much WHO participation. --- -
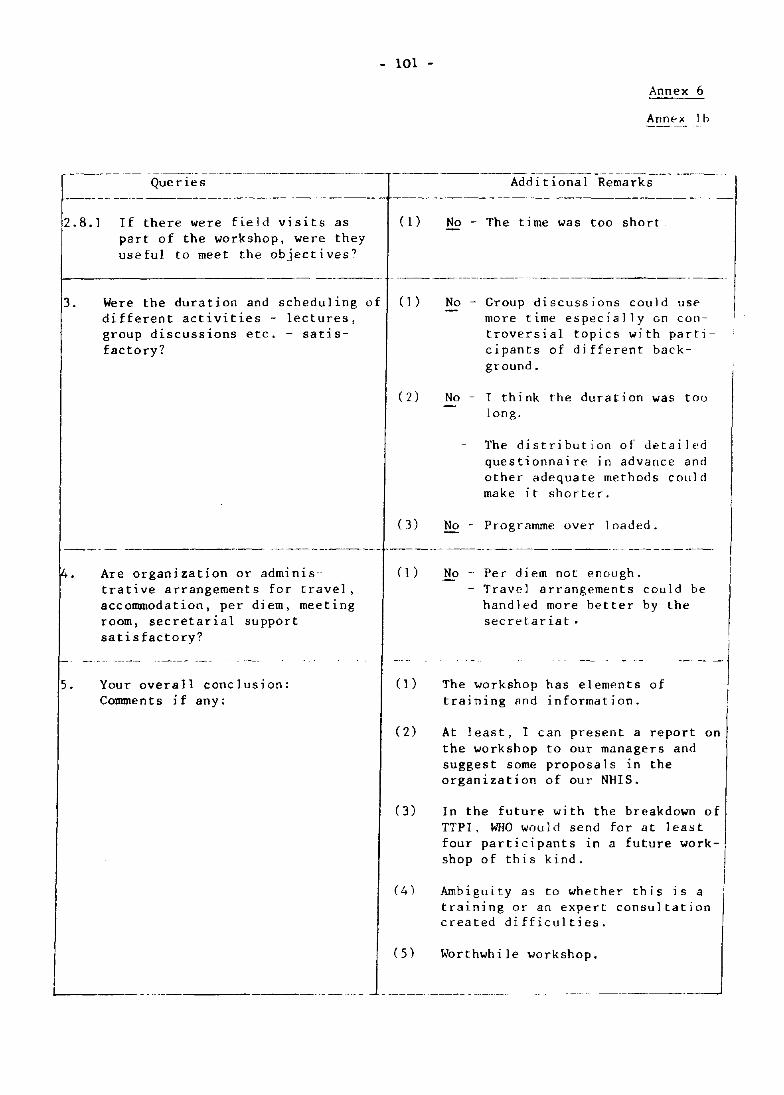
Queries
2.8.1 If there were field visits as part of the workshop, were they useful to meet the objectives?
- 101 -
([)
Annex 6
Annf'x 1 b
Additional Remarks
No - The time was too short
\------------------- ------ - ---------------- -----------------
3.
4.
5.
Were the duration and scheduling of (1) different activities - lectures,
No - Group discussions could use more time especially on controversial topics with participants of different background.
group discussions etc. - satis-factory?
Are organization or administrative arrangements for travel, accommodation, per diem, meeting room, secretarial support satisfactory?
Your overall conclusion: Comments if any:
(2) No - 1 think the duration was too long.
The distribution of detailed questionnaire in advance and other adequate methods cOl,ld make it shorter.
(3) No - Programme over loaded.
(])
(J)
No - Per diem not enough. - Travel arrangements could be
handled more hetter by the secretariat.
The workshop has elements of training and information.
(2) At least, I can present a report on the workshop to our managers and suggest some proposals in the organization of our NHIS.
(3) In the future with the breakdown of TTPI. WHO would send for at least four participants in a future workshop of this kind.
(4) Ambiguity as to whether this is a training or an expert consultation created difficulties.
(5) Worthwhile workshop.
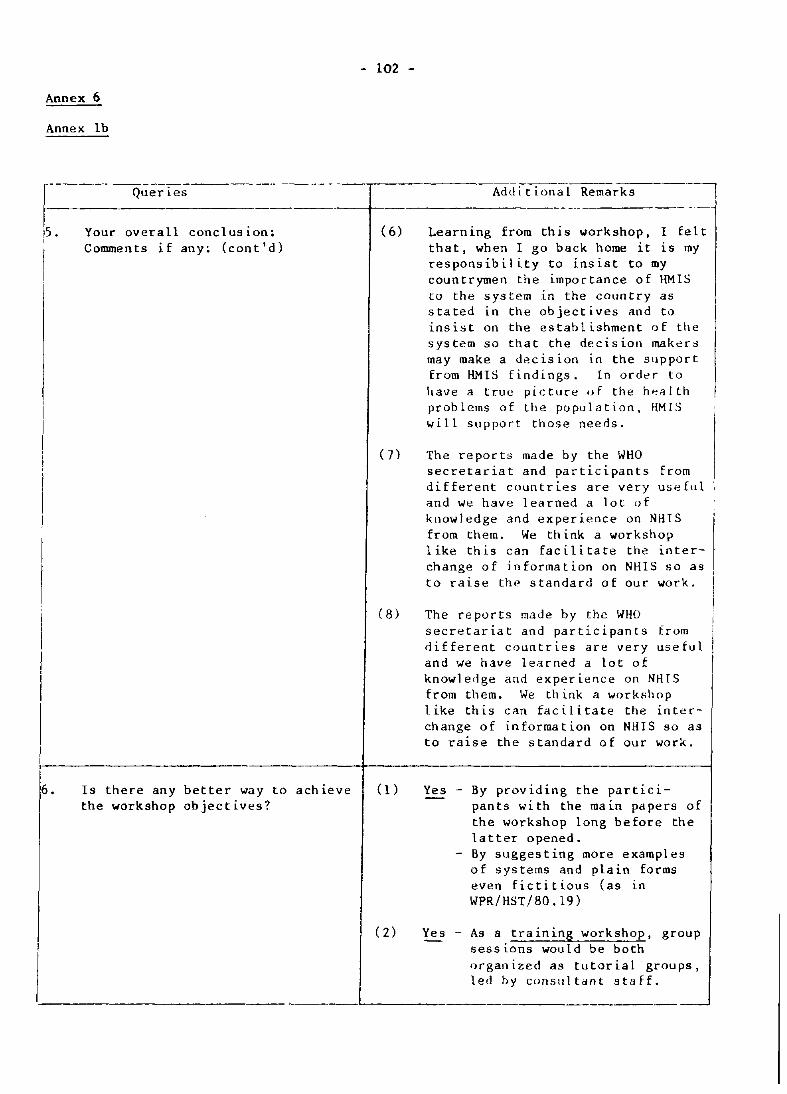
- 102 -
Annex 6
Annex Ib
1
--------~-----------~·-______,___,_cc ~-~--------Queries Additional Remarks
-----------------5. Your overall conclusion; (6) Learning from this workshop, I felt
6.
Comments if any: (cont'd) that, when I go back home it is my responsibility to insist to my countrymen the importance of HMIS to the system in the cOI/ntry as stated in the objectives and to insist on the establishment of the system so that the decision makers may make a decision in the support from HMIS findings. In order to have a true picture of the h~~lth prob lems 0 f the po pu 1 a t ion, HM I S will support those needs.
Is there any better way to achieve the workshop objectives?
(7) The reports made by the WHO secretariat and participants from different countries are very useful and we have learned a lot of kllowledge and experience on NHIS from them. We think a workshop like this can facilitate the interchange of information on NHIS so as to raise the standard of our work.
(8) The reports made by the WHO secretariat and participants from different countries are very useful and we have learned a lot of knowledge and experience on NHIS from them. We think a worksllop like this can facilitate the interchange of information on NHIS so as to raise the standard of our work.
(1) Yes - By providing the participants with the main papers of the workshop long before the latter opened.
- By suggesting more examples of systems and plain forms even fictitious (as in WPR/HST/80.19)
(2) Yes - As a training workshop, group sessions would be both organized as tutorial groups, led by consl/Itant staff.
' _____________________________________ L-_____________________________________ ___
6. Is there any better way to achieve the workshop objectives? (cont 'd)
- l03jl04 -
Annex 6
Annex lb
(3) Yes - Workshops should be conducted in country level and to involv participants from the high level of the ministry.
(4) Yes - Possibly the field trip would have been timed earlier in the workshop about half-way through, to have an earlier break in the monotony of the workshop.
(5) Yes - Prepare a manual of operation to HMIS, and submit to all countries in SPC, as a guide for such country in implementing the HMIS system. The manual will be a guide, how to establish the system and operate and their functions.
- 105 -Annex 6
ANNEX 2
2.4 Specify which of the working papers distributed for the workshop are suitable for wider distribution?
(1) Dr Mandil, especially eKplained clearly and very practical terms. Mr Subramanian.
(2) Dr Malcolm's paper/Mr Subramanian.
(3)
Mr UellD.lra. Or Mandil.
(4) WPR/HST/80.12 by Dr Malcolm. WPR/HST/80.13 by Mr Uemura.
( 5)
(6) WPR/HST/80.7 WPR/HST/80.15. WPR/HST/SO .1S.
(7) All the reports done by WHO consultants (Mr Subramanian, Dr Malcolm, Mr Uemura, Dr Mandil), and also some others (WPR/HST/SO.19) are suitable for wider distribution.
(S) WPR/HST/SO.13. Role of Health Statistics In Health Information
WPR/HST/SO.12. WPR/HST/80.14.
System Activities.
(9) View-graphs on Data Base Management (with some additional text).
(10)
(11) WPR/HST/SO.6. Health Information Systems in the Western Pacific
(12)
(13 )
(14)
Region. WPR/HST/80.7. Report, Interregional Consultation in National
Health Information System.
Viewgraphs on Data Management. Test Run Strategy and Activities. Principles for NHIS.
V1ewgraphs on Towards General Principles for NHIS. Viewgraphs on Data Base Management.
(15) Principles of NHIS including the viewgraphs. The Role of Health Statistics in Health Information System Activities NHIS Health Planning and Management Aspects. Steps in Health Information System Development Process.
- 106 -
Annex 6
Anne){ 2
(16) WPR/HST/BO.7 Report on Interregional Consultation on NHIS, Costa Rica.
WPR/HST/BO.B Towards Principles for NHIS.
(l7) National Information Systems Health Pllnnin~ and Management Aspects.
( 18)
The Role of Health Statistics in Ilealth Information System Activities. Viewgraphs on Tow~rds General Principles for National Health Information Systems.
WPR/'IST/80.6 9 .June 19~O ('I r Su'>raman ian). WPR/HST/RO.11 '.~PR/HST/RO.17 . WPR/HST/BO.17 A<j,i • I . WPR/HST I 80.12 19 June 1980 ( f)r Malcolm).
WPR/HST1RO.fi ') .J1l1e 19'i1) (Mr SuOram.1" ian). WPR/HST/80.11 ,~PR IHST IBO. 17. WPR lAST 181). J 7 Arid .1. WPR IHST IBI). J 2 19 June 19BO (Or 'Ialcolml.
- 107 -
Annex 6
ANNEX 3
(1) - (1) - (1) -
(2) Promotion ~y Ministry of Health of good things in relation to HMIS in the cOllnt ry.
(3) Forming committees responsible for establishing HMIS.
(4) To commit more deeply to the activities of ~HO and other agencies.
( '» -
(6) To re-examine the existing HMIS.
(7) E9ta~li8hment and development of a NHIS, with conventional method~ at the beginning, then introduction on a rational basis of EOP.
(II) -
(2) Technical cooperation in fellowships and other training.
(3) Assist in HMIS development.
(4) To organize small meetings on more definite concrete problems of NHIS.
( '» -
(6) To give .~ome a<illise and technical report
(2) Other member countries in the region who have already had H.'HS experience.
(3) possible consultation between member states In this region, who have already had programmes on HMIS.
( 4)
('» -
(6 )
(7) To sketch a model of (7) Training of EDP NHIS presumably to meet programmers. the needs of the region cOllntries (like the report of WHO experts on Selection of Drugs).
(~) - Provide expertise in technology support and training.
- Visit to consult with the country personnel on some other related matters.
(8) -
---------------------------------------------------------------------------------------
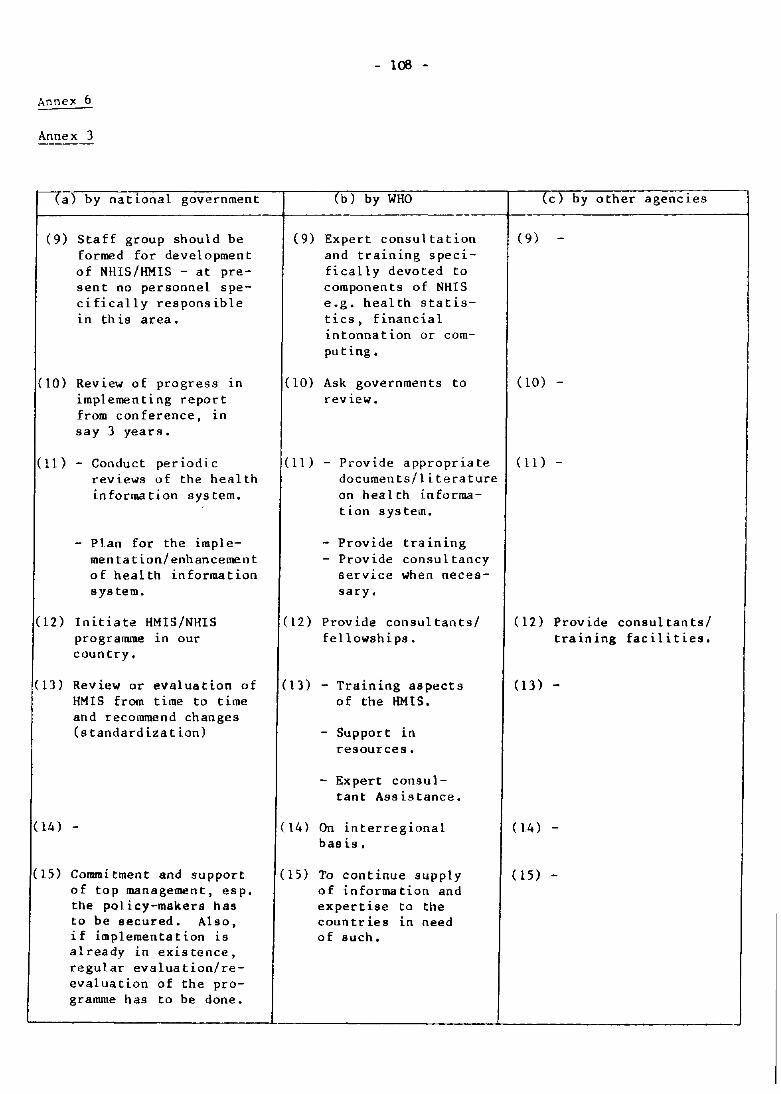
Annex 6
Annex 3
(a) by national government
(9) Staff group should be formed for development of NHIS/HMIS - at present no personnel specifically responsible 1n th is area.
(10) Review of progress In implementing report from conference, In say 3 years.
(11) - Conduct periodic reviews of the health information system.
- Plan for the implementation/enhancement of health information sys tern.
(12) Initiate HMIS/NHIS programme in our country.
(13) Review or evaluation of HMIS from time to time and recommend changes (standardization)
(14) -
(15) Commitment and support of top management, esp. the policy-makers has to be secured. Also, if implementation IS already in existence, regular evaluation/reevaluation of the programme has to be done.
- 106 -
(b) by WHO
(9) Expert consultation and training specifically devoted to components of NHIS e.g. health statistics, financial intonnation or compu t ing.
(10) Ask governments to rev iew.
(c) by other agencies
(9) -
(10) -
(11) - Provide appropriate (11)documents/literature on health informa-tion system.
- Provide training - Provide consultancy
service when necessary.
(12) Provide consultants/ fellowships.
(13) - Training aspects of the HMIS.
- Support in resources.
- Expert consultant Assistance.
(14) On interregional bas is.
(15) To continue supply of information and expertise to the countries in need of such.
(12) Provide consultants/ training facilities.
(13) -
(14) -
(15) -
~----------------------~-------------________ -L ________________________ _
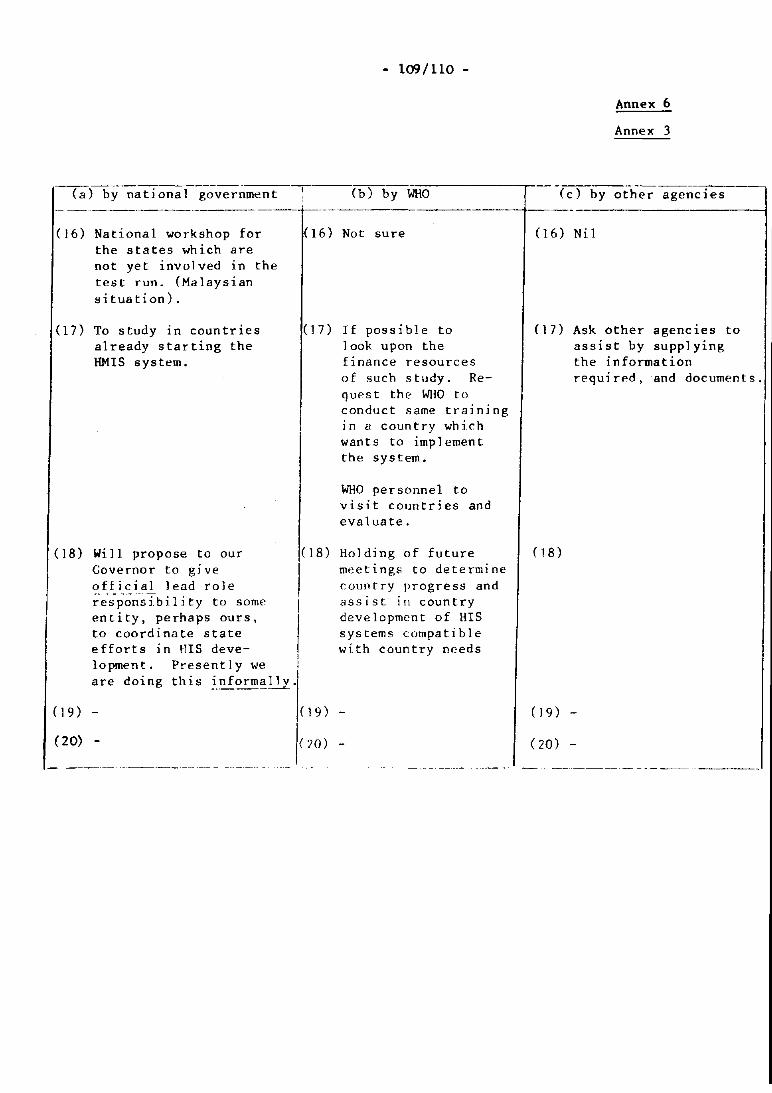
(16) National workshop for the states which are not yet involved in the test run. (Malaysian si tuation).
(17) To study in countries already starting the HMIS system.
(18) Will propose to our Governor to give off icial lead role re-spon-sibility to some entity, perhaps ours, to coordinate state efforts in HIS development. Presently we are doing this inf~ally.
(9) -
(20) -
- 109/110 -
(b) by WHO
(I6) Not sure
el7) If possible to look upon the finance resources of such study. Reques t the WIIO to conduct same training in a country which wants to implement the system.
WHO personnel to visit countries and evaluate.
(18) Holding of future meetings to determine country progress and assist in country development of HIS systems compatible with country needs
(19) -
(20 )
Annex 6
Annex 3
(c) by other agencies
(]6) Nil
(17) Ask other agencies to assist by supplying
(18 )
the information required, and documents.
( J 9) -
(20)
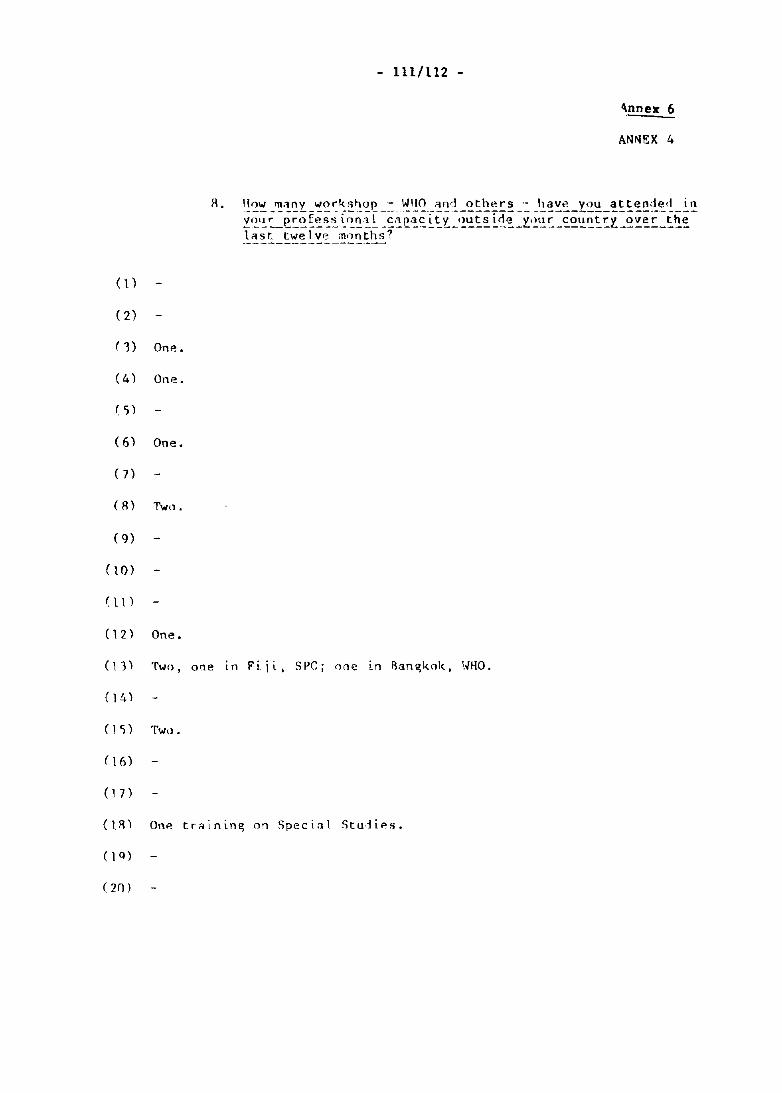
- 111/112 -
\nnex 6
ANNEX 4
(1)
(2)
( 'I) One.
(4 ) One.
( 5)
( 6) One.
(7)
(R) Two.
( 9)
(IO)
0\ )
(12) One.
(11) Two, onE! In Fiit, SPC; one In flan~kok, '.mo.
( 1 'i) Two.
( 16)
(IR) One trainin~ on Special Stu1ies.
(0)
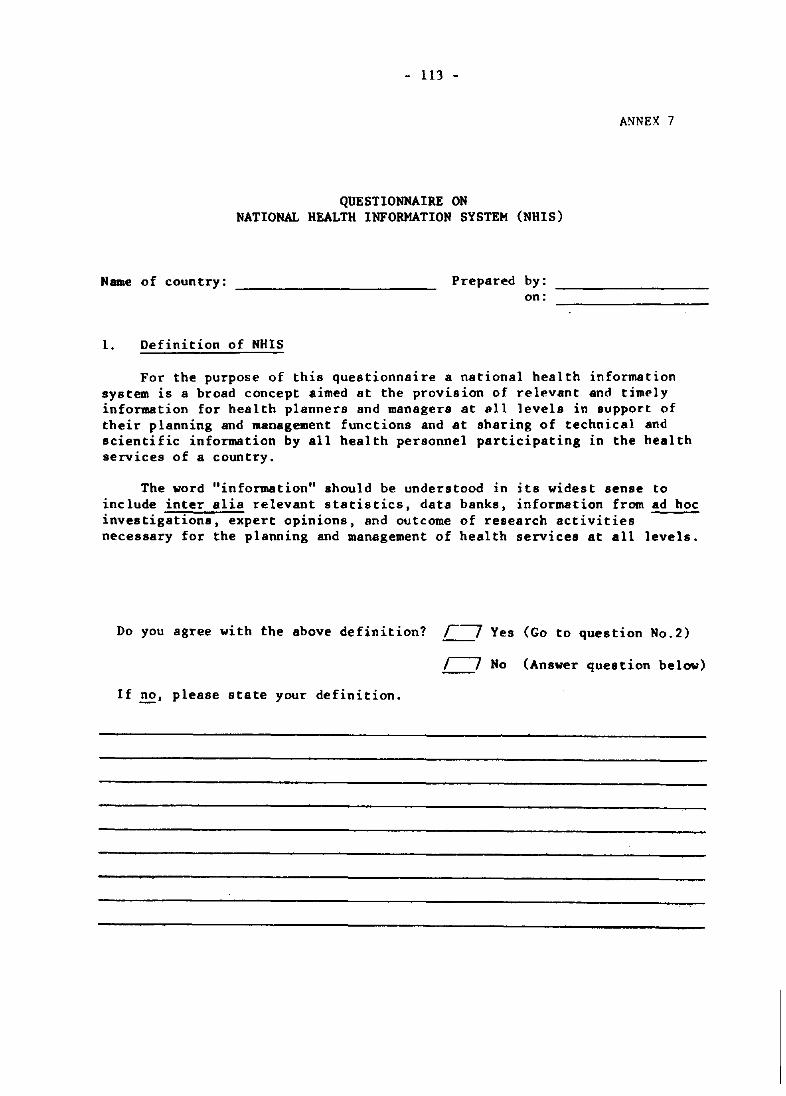
- 113 -
QUESTIONNAIRE ON NATIONAL HEALTH INFORMATION SYSTEM (NHIS)
Name of country:
1. Definition of NHIS
Prepared by: on:
ANNEX 7
For the purpose of this questionnaire a national health information system is a broad concept aimed at the provision of relevant and timely information for health planners and managers at all levels in support of their planning and management functions and at sharing of technical and scientific information by all health personnel participating in the health services of a country.
The word "information" should be understood in its widest sense to include inter alia relevant statistics, data banks, information from ad hoc investigations, expert opinions, and outcome of research activities necessary for the planning and management of health services at all levels.
Do you agree with the above definition? r-~ Yes (Go to question No.2)
r---7 No (Answer question below)
If ~, please state your definition.
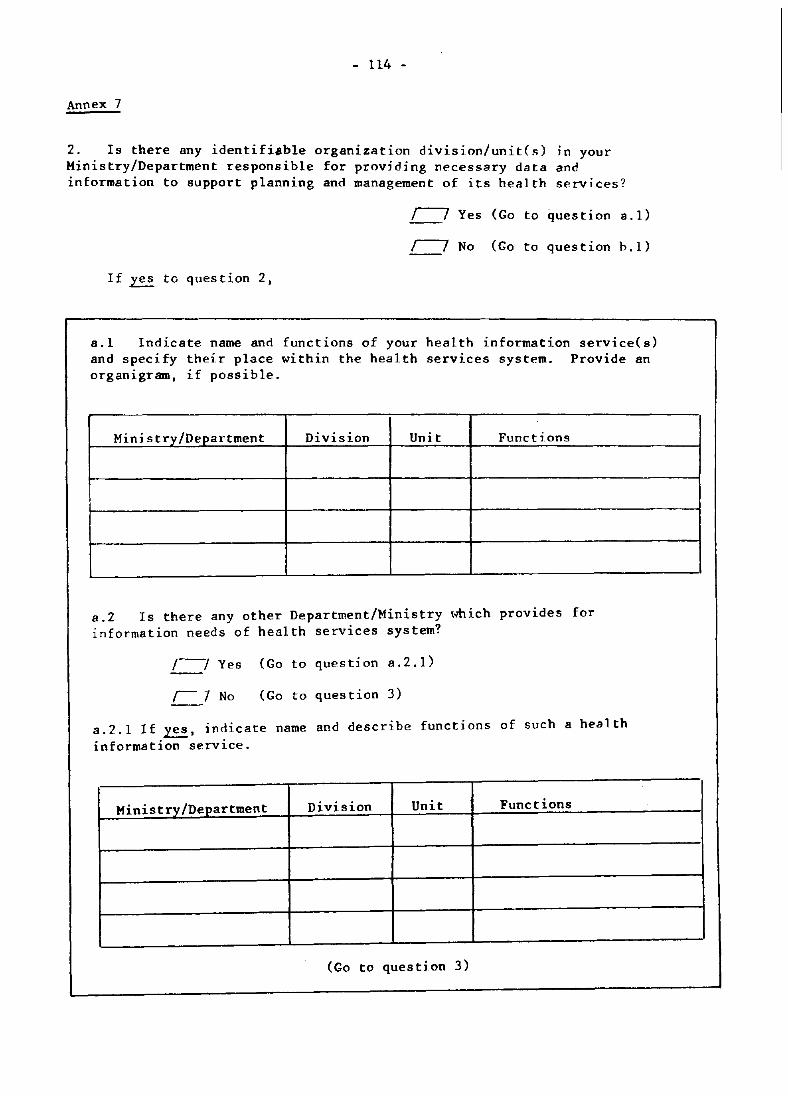
- 114 -
Annex 7
2. Is there any identifiable organization division/unitC~) In your Ministry/Department responsible for providing necessary data and information to support planning and management of its health services?
r---7 Yes (Go to question a.l)
r---? No (Go to question h.l)
If ~ to question 2,
a.l Indicate name and functions of your health information service(s) and specify their place within the health services system. Provide an organigram, if possible.
Hi ni s t ~ylDE!.£.artment Division Unit Functions
a.2 Is there any other Department/Ministry ,.hich provides for information needs of health services system?
/--1 Yes (Go to question a.2.1)
I I No (Go to question 3)
a.2.1 If ~, indicate name and describe functions of such a heal th information service.
Ministry/Department Division Unit Functions
(Go to question 3)
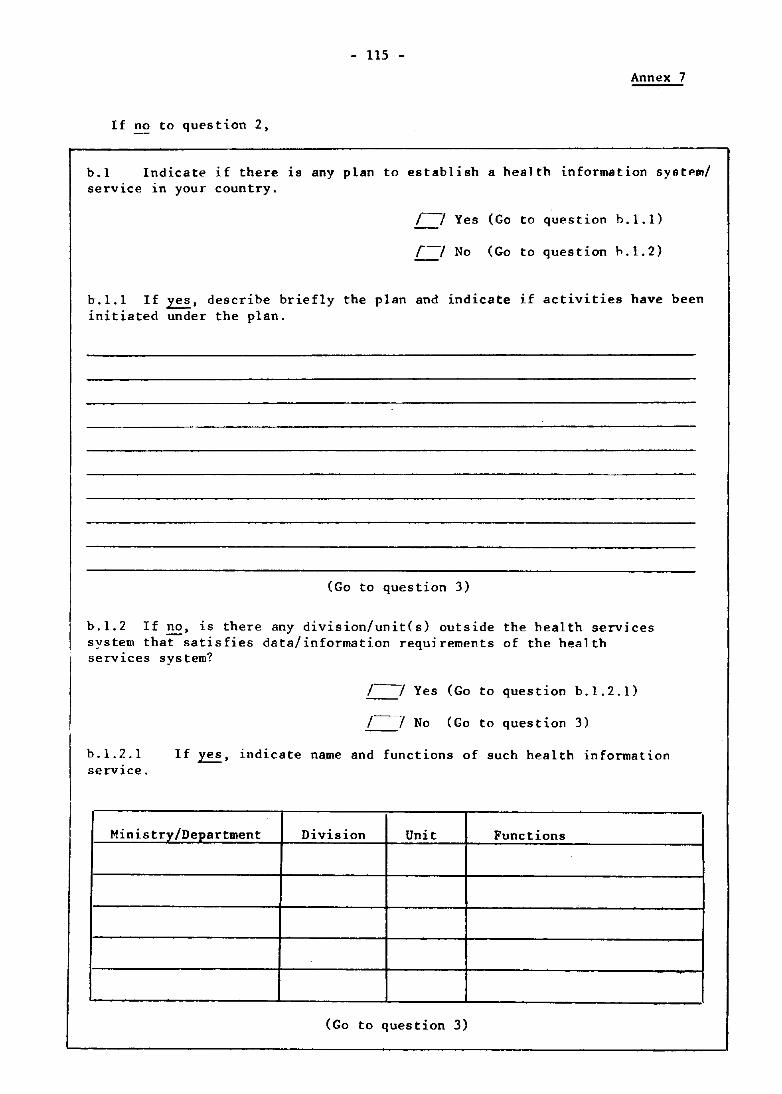
- 115 -
Annex 7
If no to question 2,
b.l Indicate if there ~s any plan to establish a health information system/ service in your country.
r~ Yes (Go to question b.l.l)
r--7 No (Go to question h.I.2)
h.l.l If~, describe briefly the plan and indicate if activities have been initiated under the plan.
(Go to question 3)
b.I.2 If no, is there any division/unites) outside the health services system thatsatisfies data/information requirements of the health services system?
/---7 Yes (Go to question b.l.2.1)
/---7 No (Go to question 3)
b.1.2.1 service.
If ~, indicate name and functions of such health information
Ministry/Department Division Unit Functions
(Go to question 3)
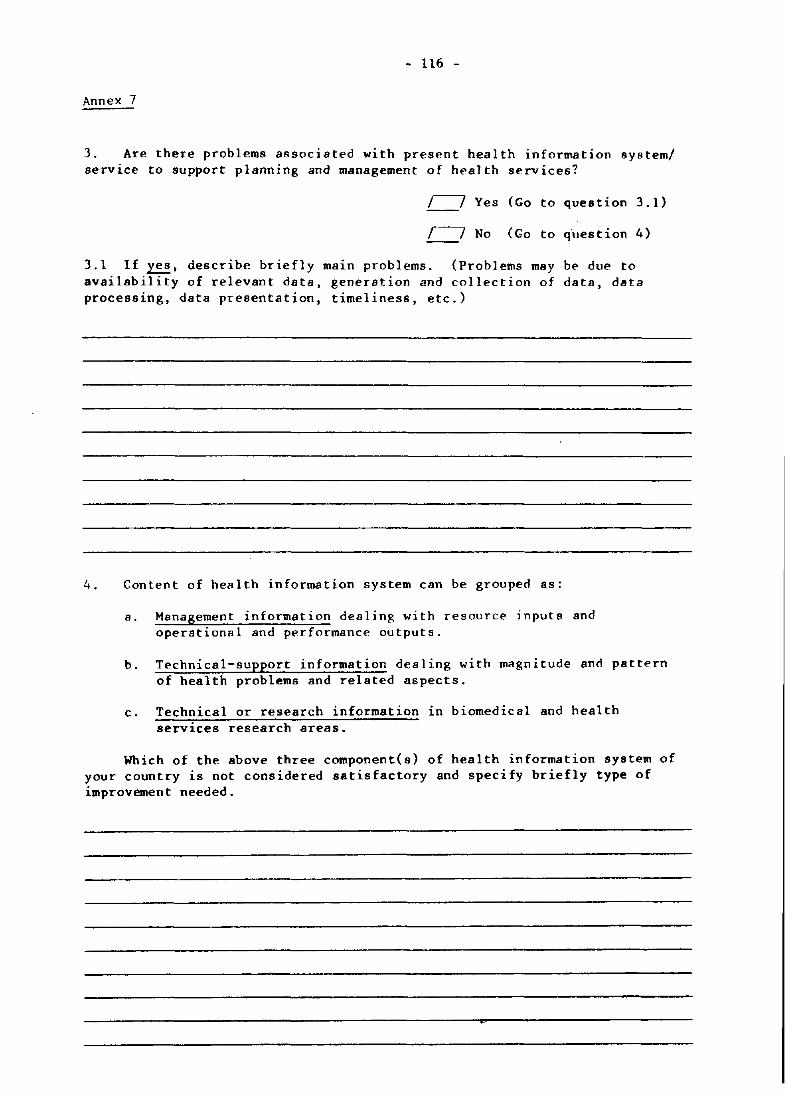
- 116 -
Annex 7
3. Are there problems associated with present health information systeml service to support planning and management of health services?
I~ Yes (Go to question 3.1)
~ No (Go to question 4)
3.1 If~, describe briefly main problems. (Problems may be due to availability of relevant data, generation and collection of data, data processing, data presentation, timeliness, etc.)
4. Content of health information system can be grouped as:
a. Management information dealing with resource inputs and operational and performance outputs.
b. Technical-support information dealing with magnitude and pattern of health problems and related aspects.
c. Technical or research information in biomedical and health services research areas.
Which of the above three component(s) of health information system of your country is not considered satisfactory and specify briefly type of improvement needed.
•
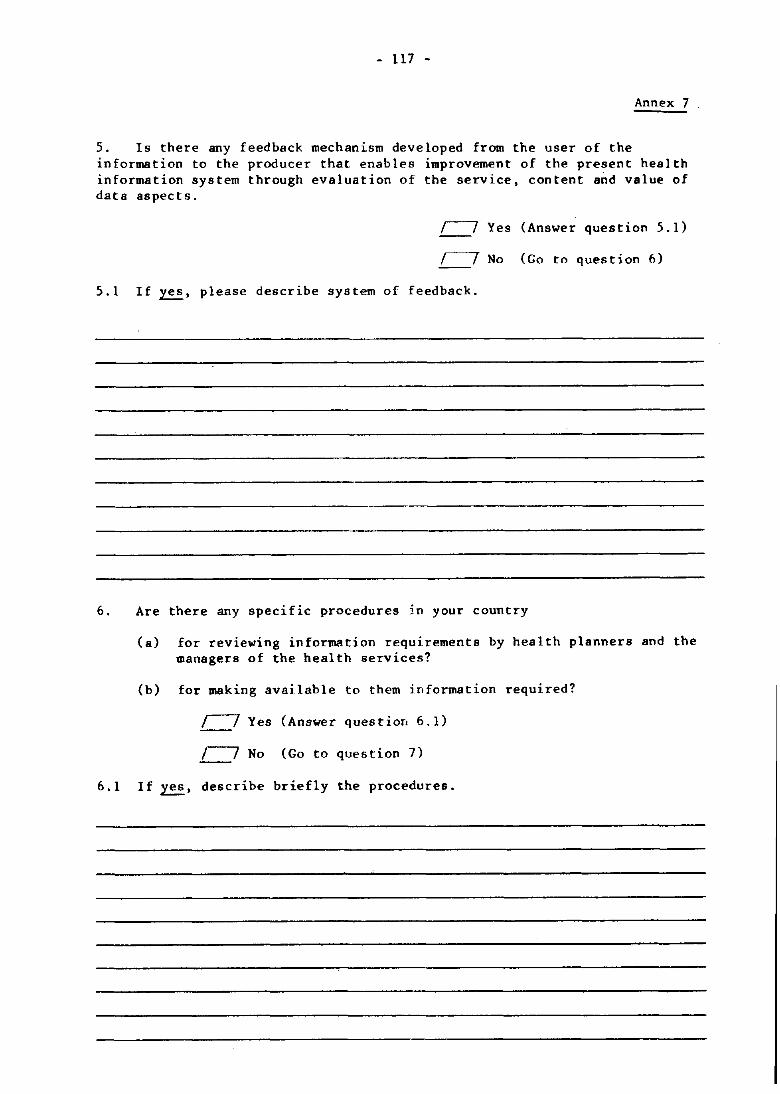
- 117 -
Annex 7
5. Is there any feedback mechanism developed from the user of the information to the producer that enables improvement of the present health information system through evaluation of the service. content and value of data aspects.
r---7 Yes (Answer question 5.1)
,---y No (Go to question 6)
5.1 If~. please describe system of feedback.
6. Are there any specific procedures in your country
6.1
(a) for reviewing information requirements by health planners and the managers of the health services?
(b) for making available to them information required?
/I Yes (Answer question 6.1)
/~ No (Go to question 7)
If ~. describe briefly the procedures.
- 118 -
Annex 7
7. Is there any identifiable organization division/unites) in your Ministry/Department or in any other Ministries/Departments responsi~le only for developing an information system/sub-system to support plannin~ and .anagement of its health services?
/~ Yes (Answer question 7.1)
/---y No (Go to question 8)
7.1 If~. indicate name and functions of such a unit or division.
Ministry/Department Division Unit Functions
8. Pleaae list any points not raised in this questionnaire that are considered important for the success of the proposed Workshop on National Health Information System.

- 119/120 -
ANNEX 8
REPORT
INTERREGIONAL CONSULTATION ON NATIOOAL HEALTH INFORMATION SYSTEMS
San Jos~, Costa Rica, 14-20 November 1979
- 121 -
WORLD HEALTH ORGANIZATION
ORGANISATION MONDIALE DE LA SANTE
INTERREGIONAL CONSULTATION ON NATIONAL HEALTH INFORMATION SYSTEMS
San Jose, Costa Rica, 14-20 November 1979
1. Introduction • . . • • . •
2. Definitions and objectives
3. A review of the present status of NHIS
4. Users and uses • • .
5. Types and sources of information
6. Establishing and developing a NHIS
7. Support and collaboration
8. Conclusions and recommendations
Annexes I to V
1. Introduction
REPORT
CONTENTS
ANNEX 8
NHIS/IR/SO .1
ORIGINAL: ENGLISH
1
2
3
5
6
7
S
8
10
National health information systems (NHIS) are now generally recognized as necessary fundamental and integral elements of national programmes of health service development. If we are to achieve "Health for all by the year 2000", the efforts that will be needed must be planned, executed and monitored on the basis of the best and most comprehensive information that can be made available to all involved. Such information is needed at all levels of programmes and by workers as well as by the people themselves.
The World Health Assembly (resolution WHA31.20), in addition to urging Member States to develop or strengthen their health information systems, requested the Director~General to develop principles for national health information systems (NHIS) in close collaboration with Member States. Subsequent resolutions have reiterated the importance of reliable information about national health and national health programmes. Since health information is not an end in itself but simply a means for facilitating the task of improving health, the kinds of principles being sought are ones that will permit available or obtainable information to have the maximum impact in improving health. Even the wealthiest countries are now faced with financial and manpower constraints and it will be necessary to tailor health information systems and the information they make available to the health needs of each individual country.
The issue of this document does not constitute formal publication, It should not be reviewed, abstracted or Quoted without the agreement of the World Health Organization, Authors alone are responsible for views expressed in signed articles,
Ce document ne constltue pas une publication,
II ne doit faire robjet d'aucun compte rendu ou resume ni d'aucune citation sans rautorisatlon de l'Organisation Mondiale de la Sante, Les opinions exprimees dans les articles signes n'engagent que leurs auteurs,
Annex 8
NHIS/IR/ao .1 page 2
- 122 -
WHO has therefore embarked upon a programme of intercountry and interregional consultation designed to facilitate the exchange of experience and expertise and to foster the development of NHIS in every country. The meeting in Costa Rica in November 1979 was part of this programme. Representatives from every WHO Region were present.
All participants in the consultation were agreed that the consultation must result in a report addressed to everyone involved in the struggle for health for all. This report is designed to help the reader to:
(a) prepare an effective argument for the development and maintenance within ea~h Member country of a national health information system (NHIS) suitable for that country's needs and related to its programme for reaching health for all by the year 2000;
(b) develop a ~~IS in a Member country and promote its effective and continuous use as a tool for planning, executing and appraising a programme of efforts directed towards attaining the highest possible levels of health throughout that country;
(c) use such technical and other support as is available nationally and internationally to assist a Member country to develop a NHIS appropriate to its needs,
The consultation was based on discussion in working groups and in plenary sessions and was focused on a series of working documents and information documents prepared for and by WHO and by members of the consultation with experience of NHIS in their own countries.
Although members of the consultation were unanimous about general principles, there were inevitably differences of technical opinion about the best way to achieve the detailed implementation of NHIS. The differences are reflected in the report and it is hoped that the variety of opinions will be as helpful to readers as it was to the participants.
2. Definitions and objectives
I t is important to define the term NHIS. The word "national" should be taken to mean "covering all of a country or territory", however fragmentary or ill-distributed this coverage might be. The expression "health information" requires rather special consideration. Information is not the same as data nor is it the same as knowledge. Data may be analysed and processed, so as to yield information, as for example when raw statistical data are used to compute incidence or prevalence rates. The function of information is to increase knowledge or understanding, and health information is information which contributes to the improvement of that knowledge and understanding which informs the decisions that are made in developing and m,maging a programme to improve health and health care.
In our present context the word "system" presents a number of difficulties of definition, The word is usually understood to mean "a set of elements with known relations between the elements" and most systems are seen as having an orientation towards some identifiable goal. Thus, a health information system is more than a collection of health information services; to be viewed as a system such a collection of information services needs to exhibit coordination and a sense of purpose.
Thus a NHIS comprises a coordinated set of operations whose collective function is to assemble, analyse, interpret and transmit to appropriate users such information as i's needed to plan, execute and appraise a national programme of efforts to promote health, to prevent illness and to ensure the treatment of the sick.
The operation of any programme of health care involves the making of decisions at all levels. Decisions must be taken concerning the care of individuals, the choice of priorities at every level, the allocation of resources and the recruitment and training of personnel. People using health care also have to take decisions on whether to use the services, when and in what circumstances. Decisions may be taken on the basis of prescribed rules, personal
- 123 - Annex 8
NlllS/lR/SO .1 page 3
experience, intuitive judgement or at random. It is nearly always better (b~t not necessarily easier) to take decisions on the basis of knowledge or understanding and these usually depend wholly or partly on the availability of relevant information. A NHIS aims at furnishing information that is timely and relevant to the decisions that have to be made in the development and operation of the health programme.
The justification of considering such disparate kinds of information as statistics, technical literature and knowledge of public attitudes to health within a common information system is that these different kinds of information are all relevant to the making of important decisions at all levels of a health care programme. Health care itself is complex and involves the integration of many different kinds of resources both material and personal. An effective NHIS needs to be no less complex and equally focused on the health needs of the people.
The coordination required of a NHIS does not necessarily mean that the component elements of the system should be administratively the responsibility of a single department. Many of the component elements of a NHIS may represent functioning elements of other systems. For example, health statistics may be the responsibility of a general government statistics department and a service of health literature information may be well established within a national library service. Nevertheless, if the component elements are to represent an effective NHIS then their coordination will need to be systematically promoted.
The precise administrative structure of a NHIS will depend on the structure of the ndministration of a country's health services. In some countries all kinds of health services and all health programmes are managed by a common management system. In other countries each main programme (for example the family health programme, the communicable disease programme, the cancer programme) has its own management system - an arrangement often referred to as a "vertical" system. In general the NHIS will develop lines similar to those of the health services management.
The consultation commended a definition of a NHIS contained in a working paper prepared by WHO. This definition is as follows: "A National Health Information System is a family of mechanisms and procedures primarily intended to acquire, analyze and provide within a country the information required (a) by all levels of health planners and mal1agers for the planning, p~ogramming, budgeting, monitoring, control, evaluation and coordination of national health programmes, and (b) by other members of the health professions - specifically health care personnel (for example, medical and public health personnel, sanitary engineers, dental workers, pharmacists, and auxiliary personnel of all categories), health research workers, and educators and trainers of health personnel - each in support of their respective roles in the national health programme. The system also provides specific health information to users outside the health sector, particularly national policy-makers, socioeconomic planners and the general public".
It is worth noting that it is not necessary for a NHIS to be based on highly sophisticated data processing technology - although systems that are so based are often much less expensive than one might initially expect. What is most important is that the system should serve the needs of its users. Systems based on simple data processing are often more successful than elaborate ones because they can more easily be understood by users who may consequently be able to obtain a better service from them.
3. A review of the present status of NHIS
In terms of the most rigorous definition few Member States can be said to have a comprehensive and integrated NHIS at the present time that provides all the information support needed by all the users. Nevertheless, components of a NHIS exist in every Nember State under various organizational designations, such as a planning and statistics department. a health statistical bureau. a central bureau of health intelligence, a central health information section, etc. These components of a NHIS are often administratively separate not only from each other but also from the health service programmes that they serve. Each generally consists of local, intermediate and central information services, as well as specialpurpose information services supporting specific programmes (e.g. immunization or malaria control) at all these levels.
Annex 8
NHI S /IR/80 .1 rage 4
- 124-
The most important basis of the NHIS is provided by the health care personnel working at the local level in health centres, hospitals, etc. At this level data are gathered, which, ~len properly collated and analysed, will provide important information at each decisionmaking level. In many developing countries, particularly in the rural areas, health care may be provided by lay or paramedical personnel and is often based on traditional methods. The heal th information needed to facilitate the management of primary health care must be obtained from these personnel.
Also at the local level, health information is kept by health care personnel for the management of health care for individual patients. Locally, these records are usually kept in a more or less systematic way, but they may not conform to a cammon national pattern. Hospital records are usually standardized within a hospital and sometimes between hospitals, but health records kept by other health workers may vary Widely from one health worker to another. Health records contain health and other personal information about individual patients or families as well as about the activities of the health worker. In addition to their primary purpose of providing information in support of the day-to-day work of the health worker, the information in the health records can provide the basis for statistics on the use of resources, on the outcome of treatment and on the health status of the population. Thus the information can become useful for health planners and managers of community health services. However, there are a number of constraints on the use of health records as a basis for a NHIS in many countries:
(a) lack of standardization of health records in a country may render the aggregation and analysis of information very difficult;
(b) the data are not usually available in a form that lends itself to systematic statistical analysis of other large-scale processing;
(c) as health records are usually established only for people who make use of preventive or treatment services, the coverage of the health records may embrace only a fraction of the population, particularly in rural areas; the information may therefore relate to only a very limited portion of the entire population of the country;
(d) considerations of the confidentiality of medical records may impede the wider use of data drawn from such records.
Many countries make use of health surveys - in some cases concentrating on disease or health problem and in other cases aiming to assess gene~al health. may be periodic or continuous, they may be based on interviews or examinations. advantage that they can be purpose-designed but they do require special efforts costly.
a single Such surveys
They have the and are often
Although important components of a NHIS do exist in most countries, their functional effectiveness in contributing to the management of health programmes and services is limited by several factors.
There is often no overall design for the NHIS and systems are often inadequately related to the health programmes they serve. The existence of many uncoordinated information services often hampers the efficient and orderly acquisition, analysis, dissemination and use of information. Because of its complexity, a NHIS may take a long time to develop and development often proceeds incrementally. However, the absence of an overall design may lead to a nonintegrated system or to a disproportionate evolution of its components. The building of an overall design is in itself a gradual process.
The distributed information may lack immediate relevance to the country's health and health service needs. This may arise from the adoption of an unsuitable model of health information collection and processing; from poor coverage in the areas where health needs are greatest; from inadequate communication between potential users of information and those who collect and disseminate it; from deficiencies in data processing capability which render the information
- 125 - Annex 8
NJHS/IR/SO.l page 5
out of date by the time it is available and from a commitment to the compilation of historical series at the expense of responsiveness to current information needs. These deficiencies particularly affect health statistical services.
Health literature services also are often insufficiently focused on the health needs of the country and the services they provide may be restricted to the routine distribution of literature or to the provision of library services. Important relevant information may therefore not be accessible to decision-makers in the place and at the time it is needed.
Health personnel - field workers and managers - may not sufficiently appreciate the value of information in their daily work. This lack of appreciation may stem from lack of appropriate tr aining but it often stems mainly from having had to "per atc withou t sui tab Ie information in the past. Many health workers have learned to do without information simply because it has not been available. It must be stressed that information does not always make decision-making easier; decisions based on adequate information are likely to be better decisions.
No NHIS can possibly levels of the programme. local in application.
aim to provide all kinds of information needed by workers at all Much of the relevant information will be transitory in nature and
However, a system should be capable of discovering what information be able to remedy most of the deficits or, at least, develop means for is lacking and should
remedying them.
4. Users and uses
Although the effectiveness of a NHIS will depend on the use that is made of it, it will also depend on those responsible for it having a clear understanding of its users and its uses.
It is possible to categorize both users and uses in a variety of ways: some participants stressed the different information needs of users at different levels of a country·s pc)Jitical subdivision (e.g. provinces, towns, villages, etc.), while others stressed the helpflllness of
distinguishing operational components of the whole programme of health efforts (e.g. family health services, communicable disease control services, etc.). Others felt that it was useful to divide users into those with a clear perception of their information needs, and those without or into those who expressed a demand for information and those who really needed it. The best categorization will depend on the country's situation, the structure of its health services and the status of its information system.
The consultation stressed that different information needs are encountered by those in management roles, those providing services in the field and those responsible for research directed towards the scientific support of health efforts. The needs of teachers and trainers of health personnel deserve particular attention. It is important to remember the information needs of personnel outside the health service sector: other ministries and other workers have important needs for health information.
It is important to remember that providers of basic data are often also users of health information and a good service of information to users often brings the added benefit of improving the reliability and timeliness of the basic data reporting.
Deficiencies of management have impeded the effective development and implementation of health programmes at country, intercountry and regional levels. WHO has been actively concerned to remedy this by strengthening management structures and functions (e.g. by introducing medium-term programming, programme evaluation, etc.). The consultation strongly supported this activity and stressed the development of NHIS as a coordinating factor in health services management.
Annex 8
NHI S /IR/SO .1 page 6
- 126 -
Health information has applications at all stages of the planning, execution and appraisal of a programme of efforts designed to raise levels of health. It is relevant to the identification of health care need, to taking stock of resources, to the setting of specific objectives, to budgeting, to manpower provision and the associated training programmes, to the monitoring of progress and to the periodic assessment of achievements, shortfalls and the need for replanning. An effective health progratmne is one which involves the whole community in these activities and information relevant to these issues will be needed by the general public, by health personnel at all levels, by managers and administrators and by political leaders. A well designed NlIlS will be one that effectively and efficiently meets these wide ranging needs.
5. Types and sources of information
To some extent a description of users and uses will specify the types of information required. Nevertheless most NHIS will have to be developed from existing information systems and it is useful to categorize these. Currently available information includes:
(a) health and medical records of individuals which are needed for management of personal preventive and primary care activities at the clinical level as well as for more elaborate medical care;
(b) information on the incidence and prevalence of significant illness and on changes in these variables associated with the health care programme;
(c) mortality statistics - especially in relation to the need to calculate health indices such as expectation of life, infant and maternal mortality rates, etc.;
(d) general demographic information which may be needed for planning maternity, paediatric or geriatric services or other specialized services for the needs of demographically definable groups;
(e) information on knowledge, attitudes and practices relating to health or the use of health services among the members of the population being served: information on acceptance and satisfaction is also valuable;
(f) information on environmental influences on health;
(g) information on the use of and demand for health and medical services and on changes in these variables associated with the health programme;
(h) information on resources needed by the programme;
(i) information on legislative or administrative developments relevant to the progranune;
(j) information derived from the literature of medical science and practice and from related disciplines including the often very important "fugitive" literature of unpublished reports.
It may be useful to re-categorize information for the specific purposes of developing NHIS. Information may be categorized according to its sources, its presentation, its users, its uses, or in terms of the methods of collection, analysis or dissemination. The specific needs of a country and the state of development of its information system will usually determine the best taxonomy.
It is important to assess the different types of information in terms of a system of priority - especially if a start must be made with the most important types before lese important types can be afforded.
- 127 - Annex 8
NlUS/IR/80 .1 page 7
The c~iteria which may influence priorities are: relevance to the health programme, accessibility, cost, and timeliness of availability. Rough data that are available when needed are usually worth more than highly refined information that is available too late.
A comprehensive NHIS may be described in terms of three principal elements. The first element is involved in describing the health status of the people in as complete and as quantitative a manner as is possible and in conveying the necessary information to those who need to set the objectives of health service activity. The second is concerned with providing as complete an analysis as possible of present and developing resources of manpower, technology and materials needed by the programme concerned to raise health status. The third concerns the distribution of technical scientific and other necessary information from the relevant literature to workers at all levels of the programme. Health workers must be taken to include not only health service managers and policy makers, and health professionals but others whose professional activities have an influence on the people·s health and especially the people themselves. Each has a need for relevant information on health status, on services resources and on technical aspects of the promotion and maintenance of health.
6. Establishing and developing a NHIS
There are some general principles that merit prior statement:
(a) each country must develop its own NHIS appropriate to its own needs and resources;
(b) it may be wise to begin selectively but a long-range plan should guide each step;
(c) it is wise to base the developing NHIS on information and information services that already exist;
(d) the form and function of a NHIS should be determined by the form and function of the country's system of health and related services;
(e) a NHIS should be capable of flexible development as the situatio<l and information needs change;
(f) good and adequate information that is actually available may be much better than the best imaginable info~ation which may be too costly to obtain;
(g) the quality and reliability of the information sources of a NHIS will depend on the extent to which there is appreciation of its value and use by potential providers of data and users of information;
(h) information supports but does not replace the functions of managerial or other personnel;
(i) economy in collection, storage and distribution of information is important _ it is rarely justifiable to collect information for which no use can be specified;
(j) providers of data should also be receivers of information;
(k) information is needed on the NHIS and its operation - it merits regular appraisal just like any other component of the overall health programme.
With these principles in mind a strategy for NHIS development can be outlined. First, it is necessary to establish information needs. Although necessary, this may be a long and complex process since it must be based on an explicit and detailed statement of health service objectives. Objectives need to be stated in terms that lead to a clear specific3tion of suitable indicators of progress. A list of objectives will generate a list of basic data needs.
Annex 8
:-,,,1 S /lR/80 .1 page 8
- 128 -
Second, the capability of the existing information system to meet the specifiable needs should be assessed. Shortfalls and redundancies should be noted for correction, but what ~lready exists is likely to be the best foundation on which to build the new system.
Third, there should be developed a plan to remedy the deficiencies in a sequence determined by a suitable process of prioritization. This will involve the use of the criteria discussed earlier. It is nevertheless wise to design for the longer future as well as for immediate needs. An ideal strategy encompasses the long-term development of a comprehensive NHIS even if it begins by implementing selected elements of high priority. It can be wasteful not to plan beyond immediately realizable goals.
Fourth, the NHIS will need to be given a suitable institutional form. The precise nature of this will depend on each country's needs and resources and on existing institutions.
Developing a mIlS also involves preparing its actual and potential users so that they may not only use the information provided but, also play a central role in developing the system and in specifying the information required and in establishing priorities. Basic professional training for both health workers and managers must stress the importance of using and asking for relevant information. Programmes of continuing education will also be needed - indeed, continuing education is itself involved in the distribution of information and the NHIS will need to collaborate closely with educational programmes. So far as the people themselves are concerned, the NHIS will need to collaborate fully with health educational !iervices in providing necessary information to all.
7. Support and cooperation
The role of international agencies is particularly important in providing financial and technical support. Cooperation between one country and another is most simply organized as .1 two-country collaboration. Generally a better method is by means of subregional or regional cooperation. Various informal and formal arrangements are available through WHO and its regional offices and through other health organizations.
Collaboration may involve the direct coordinating functions of national and international financing and developing agencies. This may involve interchange of technical experience and training or other exchange. Reference library facilities may be shared. The United Nations is now encouraging such interchange by means of Technical Cooperation among Developing Countries (TCDC). Other facilities include technical cooperation through UNOTC and UNESCO or UNFPA.
However, WHO is the main agency for promoting technical cooperation in the health field. Its services include direct involvement by advisory services, staff and equipment provision, or by the network of collaborating centres and the work of expert committees. Training support is also available as is a service of reference libraries and information retrieval. Countries, and personnel within countries, should k~ow more of what is available in these ways.
Any country feeling the need for collaborative exchange in developing NHIS may begin by contacting WHO so as to explore possibilities concerning consultants, international staff collaboration or other help. Nationals can be trained with WHO help, workshops can be organized and help may be channelled from neighbouring countries with appropriate experience.
8. Conclusions and recommendations
Every country needs a NHIS and no country need do without one. The necessary advice and technical collaboration is obtainable. A wide range of published and other helpful advice is available.
- 129 - Annex 8
NlUS/IR/80 .1 page 9
A soundly pLanned and executed NHIS is central to the effective implemcntation of a national effort towards "Health for all by the year 2000". The participants in the consultation are confident that this goal can be achieved and that National Health Information Systems will playa crucial part in its achievement. The consultation formulated its recommendations as follows.
L. ALL countries slH>uld proceed without delay to the implementation, operation and development of a NHIS appropriate to the needs of their own programme for achieving "Health for all by the year 2000". Special attention should be given to the needs of primary care services. Progress should be guided by the principles of this report.
2. To that end, all countries should identify their needs for:
(a) technical advice and collaboration;
(b) material resources needed for setting up, strengthening or developing a NHIS.
3. Countries having need of cooperation beyond their own resources should either take steps to obtain it by direct negotiation with a country or countries capable of supplying the required collaboration, or should approach WHO or another international agency for advice and help in obtaining it.
4. WHO should take immediate steps:
(a) to help develop a general framework and guidelines for NHIS adaptable tu any country's specific needs;
(b) to inform Member countries of what types of advice and collaboration are available and how to obtain them;
(c) to explore the possibility of establishing an international pool of financiaL resources to which Member countries might apply as and when they need such collaboration;
(d) to arrange regular consultations with Member countries to maintain a continuous appraisal of needs and of how they might best be met; one way in which this might be accomplished is by meetings of the personnel responsible for NHIS in neighbouring countries between which exchange of experience might be most profitable;
(e) WHO should identify and maintain a list of available consultants classified according to their expertise;
(f) WHO should examine the suitability of introducing computer and micro-processor and problems arising from the non-availability of computer and micro-processor software for local languages. Many of the problems may be soluble by sharing of countries' experience;
(g) to commit resources to the development of international support services for development of NHIS.
5. The first step in developing a NHIS will usually be to begin the education and training of personnel. This should not be delayed until other aspects of the system are ready to be introduced because suitably trained personnel will be needed to develop the overall design. WHO should stimulate the development of education and training programmes in Member States and on an intercountry basis.
6. Those responsible for planning, implementing and operating national heaLth programmes should formulate their health care objectives in terms which facilitate the development of matching information systems and should commit themselves to the development of such systems.
Annex 8
NHIS/IR/SO.l p:lge 10
- 130 -
i\NNEX 1
LIST OF PARTICIPANTS
Mr Kamel AI-Saleh, Head, Vital and Health Statistical Division, Ministry of Public Health, Kuwait, Arabian Gulf, Al-Shaab, Kuwait
Mr Ayikoe Amavi, Statisticien demographe a la Direction generale de la Sante publique, Lome, Togo
Miss Mary Corning, Assistant Director, International Programs, National Library of Medicine, Bethesda, Md., USA
Dr Aziz EI Kholy, Secretary General, Board of Health, Ministry of Health, Cairo, Egypt (Chairman)
Dr A.R. Eltom, Head, Department of Community Medicine, Faculty of Medicine, University of Khartoum, Khartoum, Sudan
Dr Z. s. Gangbo, DHP, Quart ier Ayimlonf ide Portonovo, Co tonou, Repub lique populaire du Benin
[)r I:<llllsis Comaa, Under-Secretary of State for the Minister's Office and I)i n'ctor of Heal th Profile Project, Ministry of Health, Cairo, Egypt
Mr 1.t1is Carlos Comez, Chief, Office, Ministry of Health, Bogota, Colombia
Ilr ~;lligekoto Kailwra, Director, Hospital Computer Center, Universi ty of Tokyo Hospital, Tokyo, Japan
Professor Jon Kun Kim, Director Institute of Health and Environmental Research, School of Public Health, Seoul National University, Seoul, Republic of Korea
Dr A.A. Loedin, Head, National Institute of Health Research and Developmen~, hinistry of Health, Jakarta, Indonesia
Mr N.R. Mosenene, Planning Officer, Central Planning and Development Office, Maseru, Lesotho
Prof('ssor V. Ovtcharov, All-Union Institute for Research on Social Hygiene ;111,1 1'L1II1;(' Heal th Administration, Moscow, USSR (not able to attend)
Dr B.A. Qureishi, Director, Jinnah Postgraduate Medical Center, Karachi, Pakistan
Ms Evangeline Razon, Deputy Director for Information Systems, Management Information Service, Ministry of Health, Manila, Philippines
Mr W. Rodriguez, Head, Division of Information, Ministry of Health, Bogota, Colombia
Professor Alwyn Smith, Professor of Epidemiology and Social Oncology, University of M~nchester, Department of Epidemiology and Social Research, University HospItal of South Manchester, Manchester, UK (Rapporteur)
Dr Carlos Valerin, Director, Executive Division, Ministry of Health of Costa Rica, San Jose, Costa Rica
i I I I
- 131 -
WHO/HQ
Mr D.N. Berg, Technical Officer, Information Systems Programme
Dr S. Flache, Assistant Director-General
Mr L. Roy, Statistician, Health Service Information Systems
Annex 8
NHIS/IR/80 .1 page 11
Annex I
Dr B. Skrinjar, Chief, Development of Health Statistical Services (Secretary)
Mr K. Uemura, Director, Division of Health Statistics
AFRO
Dr J.C. Alary, Regional Officer, Health Statistics
AMRO
Dr P. Ehrlich, Deputy Director
Dr C. Ferrero, Regional Adviser on National Health Information Systems
Dr P.J. Rey, Project Manager, Information System on Nutrition, San Jos&, Costa Rica
Eng. V. Vuolo, Technical Officer, Information System on Nutrition, San Jose, Costa Rica
EURO
Dr A. Weber, Director, Health Information
EMRO
Dr E.I. Hammoud, Regional Adviser, Vital Health Statistics
- 132 -Annex 8
NHIS!IlV80.l page 12
ANNEX II
1.
AGENDA
""tinn"l Health Inform"tion Systems
1.1 General review of existing situation, guiding principles of a national health information system and steps for syste~5 development
1.2 National experience in the development of their Natinnal Health Information System
2. Users and their needs
2.1 Types of information
2.2 Hays of assessing needs for information
3. Development of National Health Information Systems
3.1 Principles
3.2 Steps to be undertaken
4. (;unc0pts, definitions and objectives
S. Technic"l c(>-operation in the development of l'ational Health Information Systems
5.1 Intercountry co-operation
5.2 Co-operation of IlliO
5.2.1 Types of services expected
- development of guidelines, methodology
- training
- direct involvement in NHIS development
5.2.2 Mechanisms to be developed
6. Cone Ius ions and recomr.;cndat ions
, , II II
II "
"
II II ii
- 133 -
WORKING PROGRAMME
Tuesday, 13 November
4-6 p.m. Informal meeting and coffee
Wednesday, 14 November
8.30 a.m.
9.00 a.m.
10.00 a.m.
10.30 a.m.
10.40 a.m.
12.30 p.m.
1.30 p.m.
2.45 p.m.
Registration
Opening session
Coffee
PLENARY SESSION Nomination of Chairman, Rapporteur and Consultation Officers
PLENARY SESSION: National Health Information System: existing situation, guiding principles and steps in system's development
Paper: Towards principles for National Health Information Systems (NHIS)
Discussio~questions
Lunch break
PLENARY SESSION: Continuation of morning session: countries' presentations
Papers:
- System of information in Costa Rica - Development and promotion of health
information systems in Egypt. Concept and general strategy
- Information system for management of health services in the Philippines
Discussio~questions
Coffee
Annex 8
NHIS/ IIv' 80.1 page 1)
ANNEX III
Lic. Rodrigo Carazo Odin, President of the Republic of Costa Rica
Dr Carmelo Calvosa Chacon, Minister of Health, Costa Rica
Dr S. Flache, ADG, WHO/HQ Dr P. Ehrlich, Deputy Regional
Director, WHO/AMRO Dr Emigdio Balbuena, WHO Country
Representative
Dr S. F 1 ache, ADG, IJIIO/IIQ
Mr K. Uemura, WHO/HQ
IJr C. Valerin, Costa fUCa Dr A. M. t;l Kh<>ly, EhYl't
Ms Evangeline M. Razon
Annex 8
NHIS/ IIv' 80.1 ,'age 14
Annex II I
\ .15 p.m.
4.30 p.m.
- 134 -
PLENARY SESSION: Continuation of countries' presentations
Papers:
- Health information system for management of health services in USSR
- Information system development in Indonesia National health information system in Lesotho
Discussion/questions
End of session
Thursday, 15 November
9.30 a.m.
1(1.45 a.m.
11. I r) a.lll.
1.2.30 p.llI.
1.30 p.m.
2.45 p.m.
3.15 p.m.
4.30 p.m.
PLENARY SESSION: National Health Information System: countries I reports. discussion
analysis of Presentation and
WORKING GROUPS' DISCUSSION - Usc'rs 01 NlitS and their needs:
- types of information needed - ways of assessing needs for
information
LlIncil break
WORKING GROUPS' DISCUSSION (con tinua tion) - Users and their needs
Coffee
WORKING GROUPS' DISCUSSION (continuation)
End of session
Friday, 16 November
9.30 a.m.
10.15 a.m.
10.45 a.m.
PLENARY SESSION - Presentation of groups' reports on
Users and their needs for information. Discussion
WORKING GROUPS' DISCUSSION - Development of National Health
Information System: - principles of NHIS - steps to be undertaken
Coffee
Professor A. A. Loedin, Indonesia
Dr R. Mosenene, Lesotho
Dr C. L. Gomez, Colombia
Mr K. Uemura, WiIO/HQ
Dr C. Ferrero, WHO/AMRO
11.15 a.m.
12.30 p.m.
1. 30 p.m.
2.45 p.m.
3.15 p.m.
3.40 p.m.
- 135 -
WORKING GROUPS' DISCUSSION (con tinuation)
Lunch break
WORKING GROUPS' DISCUSSION - Continuation of discussion on
Development of NHIS
Coffee
WORKING GROUPS' DISCUSSION (continuation)
End of session
Monday, 19 November
9.30 a.m.
10.15 a.m.
10.45 a.m.
11.15 a.m.
12.30 p.m.
1.30 p.m.
2.45 p.m.
3.15 p.m.
4.30 p.m.
PLENARY SESSION - Presentation of groups reports on
Development of NHIS and discussion
WORKING GROUPS' DISCUSSION - Concepts, definitions and objectives
Coffee
WORKING GROUPS' DISCUSSION (continuation)
Lunch break
WORKING GROUPS' DISCUSSION - Technical co-operation in the
development of National Health Information Systems - intercountry co-operation - co-operation of WHO
Types of services expected: development of guidelines, methodology training direct involvement in NHIS development
- mechanisms to be developed
Coffee
WORKING GROUPS' DISCUSSION (continuation)
End of session
Tuesday, 20 November
9.30 a.m. PLENARY SESSION - Presentation of groups' reports on
NHIS's concepts, definitions, objectives and discussion
Annex 8
NHIS/rR/BO.l page 15
Annex III
Dr B. Skrinjar, WHO/HQ
Dr E. Hammoud, WHO/EMRO Dr B. A. Qureishi, Pakistan
Annex 8
mHS/ IR/80.1 ','age 16
Annex III
10.45 a.m.
11.15 a.m.
12.30 p.m.
1.30 p.m.
2.45 p.m.
3.15 p.m.
4.30 p.m.
- 136 -
Coffee
PLENARY SESSION - Presentation of groups' reports on
Technical co-operation in NHIS's development and dicussion
Lunch break
PLENARY SESSION - Conclusion of the Consultation:
presentation and plenary discussion
Coffee
PLENARY SESSION - Plenary discussion and closing session
End of session
An introduction has been made before the working groups started discussion on a new subject area, to orient the groups about the output expected from the discussion.
Reference
NHIS/IR/79.1
NHIS/IR/79.l Add.l
NHIS/IR/79.2
NHIS/IR/79.3
NHIS/IRI79.4
NHIS/IR/79.5
NHIS/IR/79.6
NHIS/IRI79.7
NHIS/IRI79.8
NHIS/IR/79.9
NHIS/IRI79.l0
- 137 -
WORKING PAPERS AND AUTHORS
Title
Draft Agenda
Working Programme
List of Participants
Working Papers and Authors
Towards Principles for National Health Information Systems (NHIS)
Information System - Organization and Functions
Development and Promotion of Health Information Systems in Egypt - Concept and General Strategy
Health Information System for Management of Health Services ~n
the Philippines
Information Services in the Administration and Development of Health Care in the USSR
Health Information Systems: A review of development efforts in Indonesia
Health Information Systems ~n Lesotho
Author
Annex 8
NHIS!IIV80.1 page 17
ANNEX IV
Dr S. Mandil (prepared for the WHO Standing Committee on Information)
Carlos Valerin Costa Rica
Dr Aziz El Kholy Egypt
Ms E.M. Razon Philippines
Dr V. Ovcarov USSR
Dr M.R.W. Soetopo Dr S. Goenawan Indonesia
Dr P.. 'tosenene Lesotho
Note: All documents are available in English, French and Spanish except No. NHIS!IR/79.l0which is available in English only.
Annex 8
NHIS/rR/SO.l page IS
Annex IV
Reference
NHIS/IR/79. INF.DOC.l
NHIS/TR/79.INF.DOC.2
NHTS/IR/79.INF.DOC.3
KIITS/TR/79.INF.DOC.4
NHTS/IR/79.INF.DOC.5
NHIS/IR/79.TNF.DOC.6
NHIS/IR/79.INf.DOC.7
XIITS/IR/79.TKF.DOC.8
NIIIS/IR/79.I~F.DOC.9
~HTS/1R/79. TNF.DOC. 10
NHlS/IR/79.INF.DOC.ll
NHI S/ IR/79. INf. DOC. 12
- 138 -
INFORMATION DOCUMENTS
Title
Relationship with National and International Information Systems
Seminar on National Health Information Systems
National Health Information Systems in South-East Asia
Exploration of a Common Strategy for the Development of Health Statistics for the Use of National Health Services
Se~;nar on Vital and Health Statistics, Damascus, J8-22 September 1972
Basic Concepts for the Development of National Health Information Systems
Health Information Systems, Copenhagen. 18-22 June 1973
Report on a Consultative lleeting on National Health Information Systems Development. New Delhi. 18-22 December 1978.
Report of the WHO Consultation on the Role of Health Statistics in Studies of Human Reproduction and in family Planning Programmes.
Assistance to Countries in Planning and Operating National Health Information Systems
New Approaches in Health Statistics
Some Health Literature Considerations in the Design of National Health Information Systems
- 139 -
INAUGURAL ADDRESS BY THE PRESIDENT OF THE REPUBLIC OF COSTA RICA
RODRIGO CARAZO ODIO
Annex 8
NHIS/I~BO.l page 19
ANNEX V
Your meeting in this country is very welcome to the Government and will be of great benefit to the people of Costa Rica. You will be discussing communication systems that will provide the community as a whole with appropriate information so that the work carried out in the health field, the successes that are achieved and the objectives that are set are known to everyone responsible for playing a leading part in health activities and to everyone who has the good fortune to benefit from those activities. In declaring this meeting officially open I cannot resist the temptation to make a few comments on what the lofty goal of health for all, which we have set ourselves to attain in the remaining years of this century, means for me. Although the world today shows a depressing picture of political turmoil, economic difficulties and social injustice, every person now alive has a part to play in achieving this very noble objective of a new economic order and in fulfilling mankind's duty to establish more and better social justice, The international social justice for which we are striving means giving every person on this planet enjoyment of the rights conferred upon him by being human; when we assert that it is imperative for every person to have his human rights guaranteed, we are not trying to discharge our responsibility by making proclamations: no, we do want all human beings to enjoy the rights of the human being; this is why the new international economic order and greater social justice form an integral part of human rights. It is simply not possible to separate legal, social and economic benefits from the rights of man.
The responsibility of everyone of us in this vital struggle to improve the present condition of mankind is a responsibility that must be shouldered in every sector; in the health sector there are vast areas of the world where the inhabitants are clamouring for health, and in our own region, which cannot be considered one of the most destitute, there are many communities that today, almost at the end of the twentieth century, are scarcely yet awakening to health consciousness, for awareness of health is not common to all men; there are many people who believe that their lot is inescapably gloomy; that they have to lead a short life in which there is much suffering, little is achieved and little is contributed; the wonderful gift of life is looked upon as a kind of by-product of the species and not as the exercise of human rights on earth.
I regard health activities, health efforts, as something that should not be left in the hands of the experts alone. We shall never be able to attain such noble objectives as health for all unless the people as a whole participate in this important process. The mouilization of the community, the motivation of all its inhabitants, therefore constitutes a basic health tool. In order to seek health people must have awareness, in order to seek health a man musl have awareness, and it is not possible to achieve this awareness at all levels unless people at all levels share in the training process, in the implementation process, and in the everyday activities to promote health. The government cannot distribute health; it is imperative that the individual should want it and struggle for it, it is essential for every member of the community to direct his conduct as a human being so that, with his participation, the benefits Df health will be attained. In Costa Rica a group of experts working in a wide variety of fields are trying to ensure that every single member of the community takes part in a community health programme and becomes aware of his responsibilities. However many hospitals we have, however good our government poliCies, they will be of no use to us if they are paternalistic. There is an urgent need for human advancement, for mobilization of and participation by the people; that is why the communications media are vital for creating community awareness, and that is why it is important that communication with the community concerning the aims of health activities should playa leading role in your deliberations.
Annex 8
~;r!ls/ 111/ 80. 1 "age 20
Annex V
- 140 -
Those of us who are involved - you and I and all mankind - have a tremendous responsibility to support the political organizations known as countries or nations -whichever designation you prefer. None of these countries, none of the organiz<ltions on our planet, will be able to give to all something that all are not prepared to recei V(', and if we want health for all it is essential to make everyone aware of his right and his duty to attain this benefit.
We are living at a time when what is good is not news, when men's successes in promoting their wellbeing go unremarked; news. always has to be bad if it is to be worth publishing and attract some people's attention. We are living at a time when the triumphs of men and communities count for nothing; at a time when only the failures of men and the failures of communities are considered important enough to publish. If in one of our hospitals we perform a thousand successful operations, that is not news; news is how and when a problem could not be overcome; that is why it is important that when we talk about communication we bring people to see the bright side of their existence, and that is why you, as experts in this important task of imparting accurate information to the community and to the world, should do so in an objective spirit, a spirit that people have lost so that as they seem to take pleasure in passing on only what is bad and nothing that is good. It is important, therefore, that we should make people feel they have a part to play on this earth, feel that each one of us has a personal role in this drama of humanity. It is essential that we make cur message constructive for there is all too much destructive communication in our time, It is important that we should clearly convey to man that he is on this earth to procreate and produce an increasingly happy world, because there are many people who remind him daily of the failures of mankind and, in the exercise of what they call freedom of expression, remind him only of mankind's disasters. The communications media never tell us how to achieve happiness ill a community; but they tell us every day how misfortune has befallen a human being or a community. How important it is, therefore, that we should be conscious advocates of "ptimism, conscious advocates of objectivity; how important it is that information should be constructive, so that people realize that their role on earth is not a role of destruction. How important it is that we at this meeting should find ways of getting people to imitate the good things, ways of getting people to learn useful things, ways of getting mankind to seek social justice through constructive action and not through protest and violence. How important it is that each one of us should be able to say that we are constructing a new world economic order, one element of which must be the target which you and I, all of us, have set ourselves: health for all by the end of this century.
A hearty welcome, and thank you.
- 141/142 -
HEALTH MANAGEMENT I NFORMA TlON SYSTEM DEVELOPMENT PROJECT
Technical Report No. 1
CONCEPTUAL PHASE
Ministry of Health Government of Malaysia
Kuala Lumpur
in collaboration with
Wortd Health Organization Wester n Paci fic R f;!9 ional Office
Manila, PhillJ){)ines November f979
Annex 9
1.
2.
3.
143
Annex 9
CONTENTS
INTRODUCTION .. ..... ,. ........................... ,. .......... . FORMULATION OF PRINCIPLES . ...................... ,. . ,. .... . 2.1 2.2 2.3 2.4
Objective Target Approach Outputs
· .................... ,. . ,. .................. . · . ,. ................................................................ .. ......................................... , ............................ .. · .................................................................... ,.
2.4.1 2.4.2
Principles Framework.
................................................... ,. ..
..................................................... BAS IS FOR ORGANIZATIONAL STUDY ........................................ 3.1 Objecthe 3.2 Target 3.3 Approach
3.3.1
3.3.1.1 3.3.1.2 3.3.2
3.4 Outputs
· ..................................................................... . · ............................. ,. ................................. .. • ....................... II ................. ,. ...................... ..
Guidelines for hierarchical identification for subsystems Identification Identification Guidelines for
. " ........................ . of subsystems ............. of sub-subsystems identification of
......... functions
and associated areas of concern
............................................
1
1
1 1 1 1
1 3
13
13 13 13
13 19 21
27
29
- 144 -
Annex 9 1. INTRODUCTION
In Sect ion S: Project Outputs of the Protocol for the' Projecc (Of
Health Management Information Systems Development (IIMISD), it was stated that documents giving procedural details as also relevant outputs of each phase of the project will be prepared as the project progresses from onr phase to the other. The present document relates to Phase 1: Conceptu.1 Phase which is concerned with formulation of principles governing the iniol-mation system and with the development of a basis for the organizationsl study of the Ministry of Healtll. This has to he studied In relation to Section 3.2.2 Conceptual Phase of the Protocol for the proJect.
2. FORMUlATION OF PRINCIPLES
The objective of this step is to get at an agreed set of prine-ipl .. and establish a framework that must guide the development of a ration811lcd information system so that the consumer/user requirements can be effectively and efficiently satisfied.
2.2 Target
By February 1976, the Information System Development Croup (ISnc) should I,ave a document detailing tile principles and framework that have been approved by the Steering Committee.
2.3 Approach
The members of the Steering Committee will deliberate on their perspectives on desirable characteristics of an information system and In that process identify the principles and establish a framework for development of an information system.
2.4 Outputs
2.4_1 ?rinciples
In carrying out this project, certain basic principles underlying information systems development will be adhered to. The first is that the inforonation system has to he developed in the country context and hence no Dlodel external to the country situation can be imposed. Sulutions should not be prejudged and premature institutionalization of any aspects -nll.npowel- resources, electronic dat<~ process ing (EDP) fac i J it ies. etc. - of the systems should be avoided since it only aids i,l self-perpetuation of dysfunctions in che system. Technological and manpower requirements a8 also the data elements of the system should be the off-shoots of the project findings and thus should be the end products and not be the constraints. However, for the project itself, any flexihle mechanism that can bring together needed resources, expertise and support to solve [he given problem would be acceptable provided the development efforts, procell Imd the outcome are not constrained by these mechanisms.
- 145 -
Annex 9
Data are un interpreted statement of facts. Information is data recorded, processed, reduced and presented in an understandable format for meaningful interpretation. Information is data and its relationship. An example is given as follows:
DATA BASE DEVELOPMENT
Information Data Elements
Prevalence rate Number of cases
Relevant population
Coverage Number of cases under care
Number of cases
Continuity of care • Number under uninterrupted care
Number of cases under care
Relationship can be over relevant denominator, over time or over space. For example, number of tuberculosis cases in 1979 (data) can be related to population in 1979 to yield prevalence figure. Number of tuberculosis cases in 1979 can be related to number of tuberculosis cases in 1978 or number of tuberculosis cases 1n 1979 in area A can be compared with the number of tuberculosis cases 1n 1979 in area B.
Also, utilization of data should be the point of departure. transport by recording and reporting becomes means to information thus data collection and transmission cannot be an end in itself.
Data flow and The
project will aim at minimizing information cost through an effective and efficient data generation, reduction and information extraction procedures as well as mechanisms for storage, retrieval and transmission of relevant information to the right person at the right time (with the right frequency) and in the right format. If the information system is to serve the overall requirements of the Ministry at all levels and also to cater to individual divisional requirements, a high degree of collaboration between and among the designers and users of the system is necessary. Any information system must satisfy the requirements of managerial functions of the Ministry which are guided by the five basic tenets, viz. efficacy, effectiveness, efficiency, equity and expectation achievement. For the purpose of the project, the following definitions will be used: Efficacy is the intrinsic technical value of therapeutic, diagnostic, preventive or rehabilitative regimens, as established through clinical trials and effectiveness is the application of efficacious modes of intervention for all those in population who can benefit from them. Efficiency is the pr~dent and economical use of resources to effective interventions for
- 146 -
Annex 9
eligihle population. Equity relates to the availahility of appropriat~ and
adequ8Le care to needed population and thus to right of sccess to care. Finally, expectation achievement is the results achieved by the serviCe! In
relation to targets and efforts expended. In this respect, development efforts must emphasize l :
purposeful selection of data parsimony and simplicity population and patients as the basic units primacy of patients and service concerns validity and reliability con hdent iality comparabil ity
Also, information system to be developed to support the managerial snd technical functions of the Ministry must not operate independently nor form another dimension to the Ministry's functions. The information system should provide an effective and efficient support with a built-in mechanism to adapt and respond to satisfy the Ministry's requirements to assist decision-making at every level of the management in the Ministry. Contents of the information system to be designed must he based on the question, who needs to know what and why. That is, it should be very clear as to what--reports need to be generated and what data must be collected and processed to produce them.
Data collection as it provides inputs to contents of information system must not result In additional workload on operational units whose main concern is patient ~nag~~...!: .. Additional reqUlTements for data clallsilication and standardization lihould, howev.!r, be ensured in developing data generation activities.
2.4.2 Framework
The framework is one of the more campi icated elements of the information system development exercise but it is the foundation and its existence and influence serve to fulfill the stated objectives more than any other item in the project requirements. The framework will define the application boundaries and their interfaces for all divisions concerned, be they professional or administrative-finance/service. It will also provide ample opportunities for assessing commonalities with a view to avoid overlapping development by making clear the priorities from a technical point of view. It allows for possibilities of undertaking development of large integrated systems in manageable chullks, with the assurance that these chunks will properly interface with each other. At the same time, it reduces the number of isolated "islands of mechanization" which might otherwise continue to be developed, operated, maintained and constantly
IWhite (1974) gives the six p's for the collection of data as parsimonious, problem-oriented, person-specific, population-based, provid~r-related, payment-related and practical. (White, K.L.: lIealth Information and Nation's Health, Management Informatio~ .. ~.:;tems for Public H~alth/Communil) Health Agencies, National League for Nurs:,.1g, New York, 197/1, pp. 17-28 .
- 147 -
Annex 9
changed or redone to meet new interface and reporting requirements. Given the framework, it will be possible to delineate tasks to be undertaken to fulfill the objective and identify various modules to be developed for one or more of the divisions or other sub-units of the Ministry. These modules will be detailed through a joint user-system staff assessment process, and finally, approved by the ultimate system-users, viz., Directors and Programme Managers.
Lastly, it also enables one to distinguish stable operational control elements from everchanging management information aspects of the system and thus serves to absorb and safeguard systems elements from the impact of changes in the pattern of management control and organization.
Information system must be viewed as a tool for policy and management decision-making and hence the system must be able to provide the right information for the right people at the right time in the right form and at the lowest possible cost.
The framework for development of an information system to support the managerial functions of the Ministry is given below:
Health services can be considered as a goal-directed behavioural system operating in an environment influenced by political, legislative and socioeconomic development factors. Performance of any health services system depends to a great extent on the interaction between health services and population individually or collectively and the effectiveness increases as the health services increases its ability to recognize and make timely, adequate and appropriate responses to the problem. Health services can again be conceptualized as having two distinct though interrelated components, viz., service delivery and service support subsystems. Performance of the health services system is thus entirely determined by the degrees of interaction between these two (service delivery and service support) sub-systems. Service delivery can be seen with patient -individual or collective - management and service support with service management. Service support consisting of service management including technology improvement has three main functions, viz., strategic or policy planning, management control and operational control which together with service delivery, viz., actual action or operations, form a package for health services systems performance.
Service delivery to population, individually or collectively, has been taken as the end product of the Ministry's activities which contribute to overall objective of the Ministry. Linkages among decisions and operations between and within a given echelon is presented in page 5. At the peripheral level, a number of actions (operations) towards service delivery take place from or through a centre which we call "activity centre". Associated with this action are decisions to be taken so that operations do lead to anticipated impact and are performed effectively and efficiently. The decision centre is one where decisions are made by management level people to prescribe the decision rules that govern the actions of one or more activity centres.
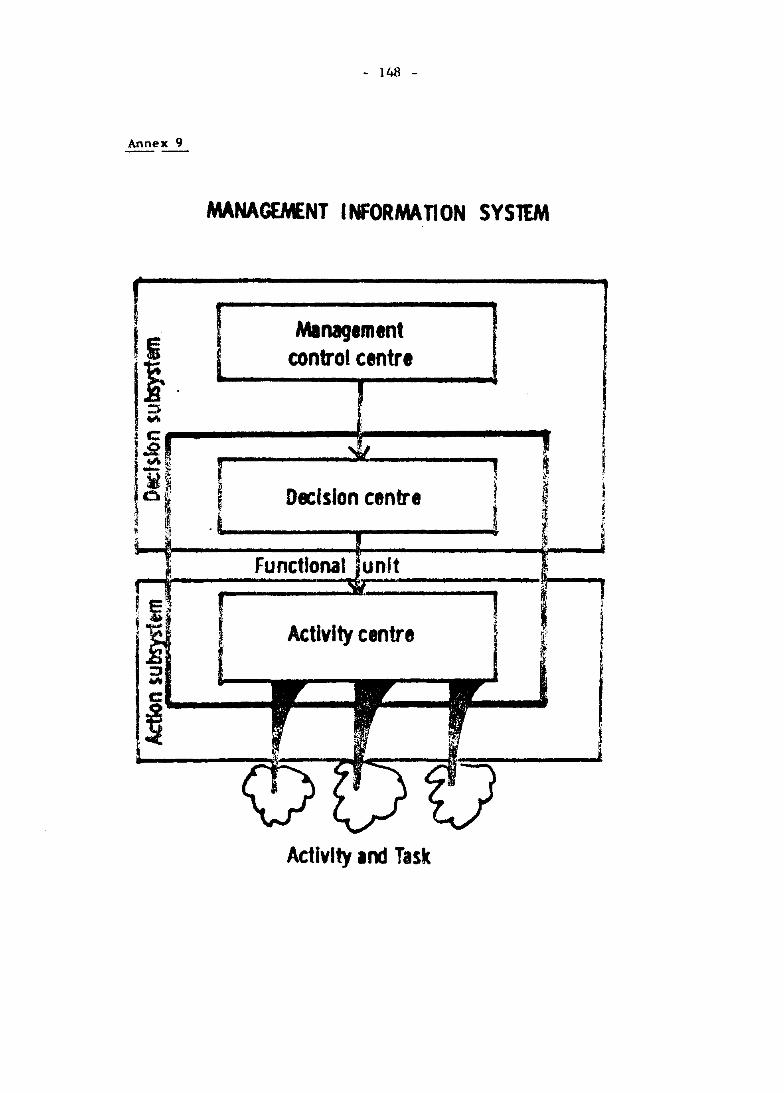
Annex 9 --
- 148 -
MANAGEMENT I NFORMA TI ON SYSTEM
Management control centre
Decision centre
Functional . unit
Activity centre
Activity 100 Task
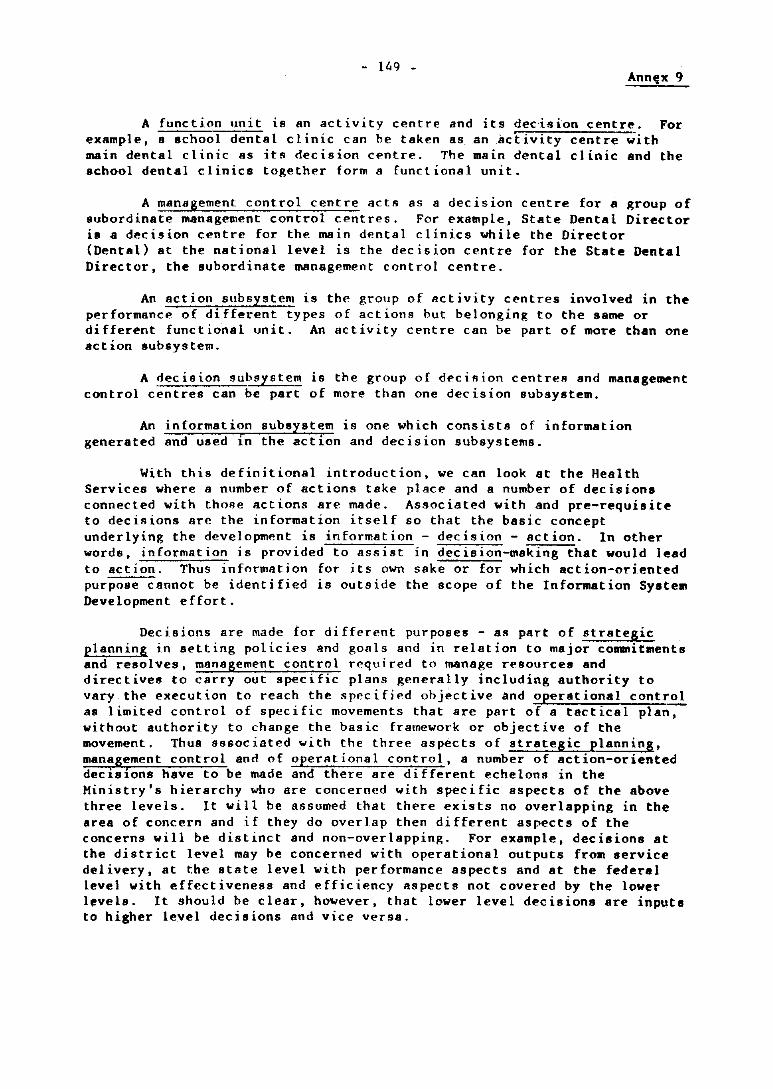
- 11.,9 -Annt:x 9
A function unit is an activity centre and its decision centre. For example, a school dental clinic can be taken as .. an activity centre with main dental clinic as itR decision centre. The main dental clinic and the school dental clinics together form a functional unit.
A management control centre acts as a decision centre for a group of subordinate management control centres. For example, State Dental Director is a decision centre for the main dental clinics while the Director (Dental) at the national level is the decision centre for the State Dental Director, the subordinate management control centre.
An action subsystem is the group of activity centres involved in the performance of different types of actions out belonging to the same or different functional unit. An activity centre can be part of more than one action subsystem.
A decision subsystem is the group of decision centres and management control centres can be part of more than one decision subsystem.
An information subsystem is one which consists of information generated and used in the action and decision subsystems.
With this definitional introduction, we can look at the Health Services where a number of actions take place and a number of decisions connected with those actions are made. Associated with and pre-requisite to decisions are the information itself so that the basic concept underlying the development is information - decision - action. In other words, information is provided to assist in decision-making that would lead to action. Thus information for its own sake or for which action-oriented purpose cannot be identified is outside the scope of the Information Syatem Development effort.
Decisions are made for different purposes - as part of strategic planning in setting policies and goals and in relation to major commitments and resolves, management control required to manage resources and directives to carry out specific plans generally including authority to vary the execution to reach the specified objective and operational control as limited control of specific movements that are part of a tactical plan, without authority to change the basic framework or objective of the movement. Thus associated with the three aspects of strategic planning, management control and of operational control, a number of action-oriented decisions have to be made and there are different echelons in the Ministry's hierarchy who are concerned with specific aspects of the above three levels. It will be assumed that there exists no overlapping in the area of concern and if they do overlap then di fferent aspects of the concerns will be distinct and non-overlapping. For example, decisions at the district level may be concerned with operational outputs from service delivery, at the state level with performance aspects and at the federal level with effectiveness and efficiency aspects not covered by the lower levels. It should be clear, however, that lower level decisions are inputs to higher level decisions and vice versa.
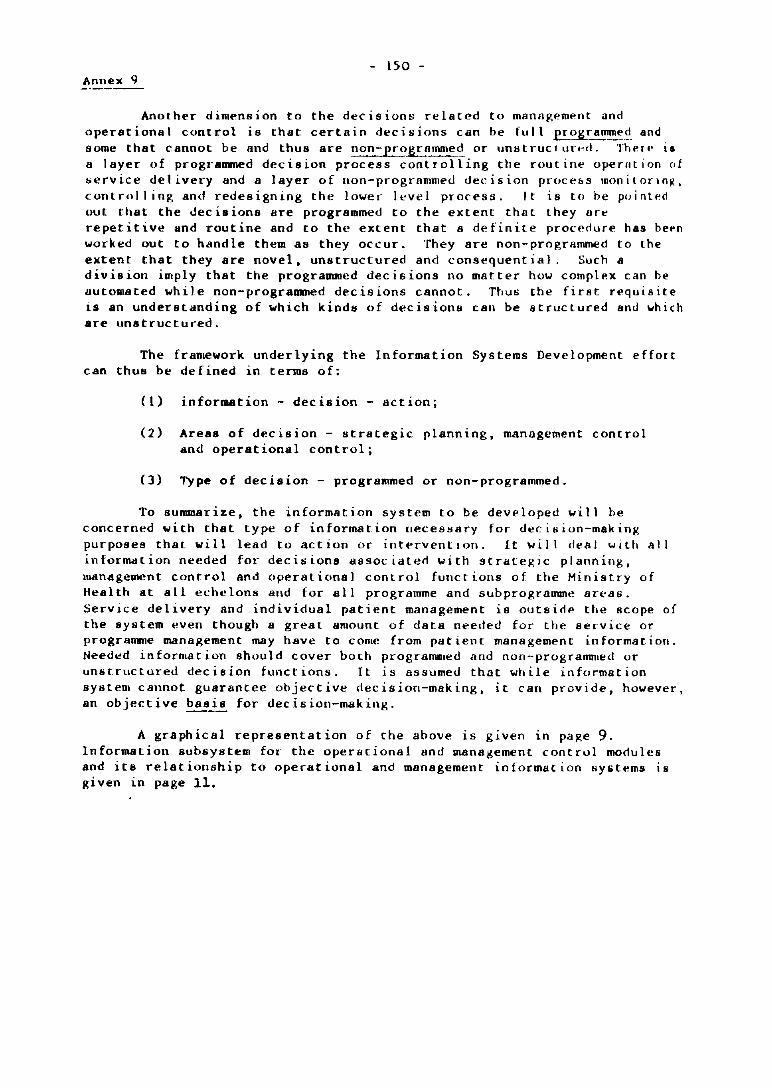
- 150 -Annex 9
Another dimension to the decisions related to manajl,em .. nt and operational control is that certain decisions can be full £'!:"~ltr.:.~~,,~. and some that cannot be and thus are non-proQ!mme<!. or unlltrucl tll".·e!. TheIl' is a layer of programmed decision process controlling the routine oper-ution of service delivery and a layer of non-progrflmmed decision procebs monilorJn~, controllinll, and redesigning the lower level process, It is to he pointl'd out that the decisions are programmed to the extent that they are repetitive and routine and to the extent that a definite procedure has bepn worked out to handle them as they occur, They are non-prog,rammed to the extent that they are novel, unstructured and consequential. Such a division imply that the programmed decisions no matter how compl .. x can he automated while non-programmed decisions cannot. Thus the first requisite 15 an understanding of which kinds of decisions can be structured and which are unstructured.
The framework underlying the Information Systems Development effort can thus be defined in terms of:
0) information - decision - action;
(2) Areas of decision - IItrategic planning, management control and operational control;
(3) Type of decision - programmed or non-programmed.
To sununarize, the in format ion sys tern to be deve loped wi II he concerned with that type of information neceS!iary for deci"ion-making purposes that will lead to action or interventlon. It will deal with all inform<ltion needed for decisions <lssoeiaterl with strategic planning. management control and operational control functions of the Ministry of Heal th at all eehc Ions and for a 11 programme and sub programme an.-as. Service delivery Bnd individual patient management is outsid .. the Bcope of the system even though a great aRlount of data needed for the service or programme management may have to COme from patient management information. Needed in forma t ion should cover bOlh programDled and non-progrannned or Un/H.rllctured decision functions. It is assumed that while information system cannot guarantee objective decision-making, it can provide, however. an objective basi..!. for decision-making.
A graphical representation of the ahove is given in pajl,e 9. Information suhsYlltem for" the operational and management control modules and its relationship to operational and management information "Ylitems is given 1n page ll.
- 151/ 152 -
MANAGEMENT I NFORMATI ON SYSlEM
~ ~ ~
1------"'-""'" ~ ~ Manage- ~
ment control 9'
Operational control ........
~ ..... r--------------------~~
\. Activities performance
Annex 9
~ ~ ~ E .
,Cf-'£\'A:lC Of "ffi£ I ',f0R.'AA no,,- 5Y5TEM
HE: ~c·_ i<CHY
Non-~~rr,~ C:>ntrol
:--~~_-l~J----~---~I~'~f~'1--1-1~ -".;~;;-i;.-;;,:-I~:.<,;.,.~;: S-;,;;m-
L M:M I I ;:. MonoQ~ I r-----------'
I • COlItrol I Mel _-.__ I I~ MOOu;. I MeM , ,en -
r - - -l- ----'- - § 1
---------l
[~-'--I M --'
I
I 1
: 1- --- ; I~---- ----: I Q,:)/. J : I ~ (';><'(0'.'01'01 L I I Cor·lrd t I ~
-- - L Mo:oc~!! - L ___ -_-~ ±I I----' I L ________ _
L _________ _
o ;g
-;.- -=>-
--1----- ------~--_i----, I I Oyerol O(V!: ':':l~!rOl :r.fou,,:,"".:;:-or. S/s'cm
I~CM I -o;.:~ J 11- II I I ! --- --------------------.J ~-- ---- ---------------I
I
Source: Man.ge!1l~nt lnfo,:n",on Svstems: a fnm<"ork for planning and development, by Sherrr.a1 C Llumenrhal.
printed by Prenr('e-Ha:l. Inc .. EnglewoodCliffi. Newlers.:y. 1969, p_ 3:\.
> ::I j
" )C
-0
..... '" w
--..... '" .,.
- 155/156 -Annex 9
3. BASIS FOR ORGANIZATIONAL STUDY
3.1 Objective
The objective of this step is to develop a basis for an organizational study of the Ministry of Health with "information system approach" perllpec t i ve.
3.2 Target
By February 1976, the ISDG should have a list of different manage~nt functions performed by various Divisions of the Ministry of Health at different echelons with areas of concern related to different functions specified and approved by the Steering Committee.
3.3 Approach
Given the principles and framework for development of an information system, the necessary steps to be followed in designing a user oriented, dynamic and responsive information system is given on page 15. The present IItep is concerned wi th the phase I of the "development procesll and steplI".
Ellllentially, in an information system, data can be characterized in terms of what programme areas need them, for what purpose, at what level and with what frequency these are needed and with what complementary data these are to be considered for meaningful interpretations. For example, dental programme will have planning, programming and budgeting lind evaluation functionR at national level and monitoring and control of dental servicell activities at dental clinic level. Infnrmation neE'ded at national level lMy tor certain functions be the same as those needed at dental clinic level. It is thus absolutely necessary to identi fy the levels and functionll for each programme areas as a basis for specifying information. The function-data relationship is given in page 17.
The ISDG will initially define the boundaries of the System and identify its functional components (subsytems). These subsystems will be further studied to isolate the lowest identifiable and distinct functional component. These lowest identifiable components will be used to identify the sreaA of concern. These will be submitted to the Steering Committee for deliberations and approval. ThE' following guidelines will be used:
3.3.1 Guidelines for hierarchical identification of subsystems
Health services system i~ a ~oal-directed controllable behavioural system which consumes resources. Hence it can be examined in terml! of input-output relationships of the processor. Input i8 the energizing or start-up component on which the system operates. Output is the reslll t of an operation. In very real sense, output stands for the achievements of purpose, goal or objective for which the system is organized. Process is the operation that makes possible the trans[on,ation of input into ouput. Under theAe concepts w,. shall identi fy the sub-systems up to that level in the r.lnct ialHl1 hierarchy where it becomes the lowpst identifiahle aggregate of functional elements. Note that we follow a "functional" approach and not II "/ltructural" one. Thus various divisions of Ministry have no spN:isl significance except fQr its relationship to different functional components.
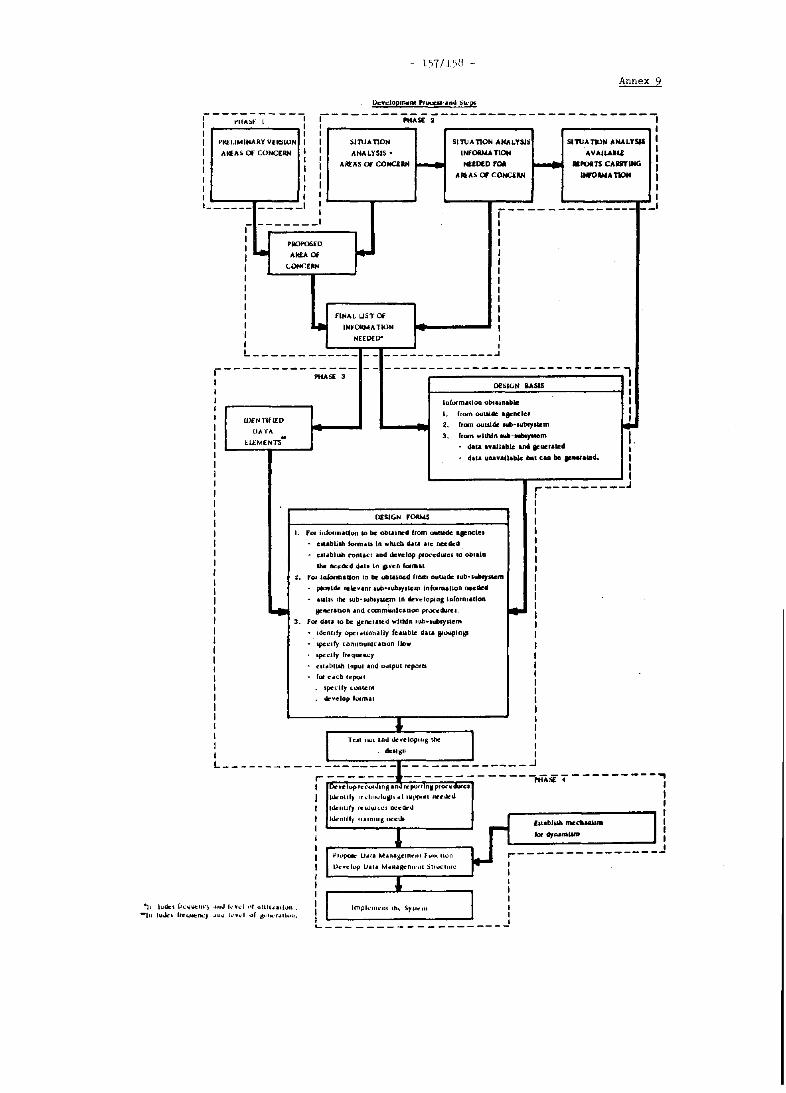
Annex 9
Uc.".:lopnwnt 'r~·.,"" !:ik·e
r---;:I~;~- - -, -- ------PttAsE ;------------- - -------. 1 I 1
1 I
+>tu::LlMINARY YEICiION
AiC£AS Of CONCERN
1 1 1 1 1
slruAnoN
ANALYSIS •
ARrAS Of' CONCI:IN r--I SIl\JAnON AHAL!S!:'; SlnJATIllN ANALYSIS
INFOINATION AYAJU.IU: I
NEEDED rOA ..... _POITS CAlIITlNG I I
1 AIliAS 01 COHCiRH UWo .... 110M I 1 1 1 1
------ _____ 1 1------ --- --- __ I
.- ------- I I
I PIlOf'OS[D I I .. • I I ..... 0<
I I CONCERN I 1 I I I I I I I 1 FINAL UST Of I I ~ INH)MMA Tk)N I I NEEDED- I I 1 L ____________ - - _ ____________ .J
r----------~;-;- - - --------------------------1 I OflilGN OASIS I 1 I 1 lalarm.ciDO obI.1I:I"'. I 1
I. fram o.ttadc apneic, I 1 Ul£NTlfIEO ~ I .. from ouw4f: eub·,ublySlcm
OA·fA I
I: U:Mt:NT:t 3. from wldlJn .... -..,...m I I Gala .nuable .nd .... u.tI!::d 1
I da.a uuvallablc bill CUI be ......... 4. I I I I I I ,.. _________ J
I 1 I I I
DESIGN F""" I I. rot j'lfo'lna'hm ID be: obcalned from OIIC1.1.111e: •• ocle.
I ellabllsb formAu In ",tueb Uta .'e needed
I cSlabluh conlUI Ind develop ploct::d~el co oblal. I lhe fto:t:*d da'a In lP"cn fOfmA' I ,. fo, 'alarm.Uon 10 be "tallied rlOltl ouuade l"b'I~'k:rn I I ,*",Idc fcleunl lub·nlbtYUCQl In"-manon needed
I IWlIl the Mlb·.ubJy~ In 4n".lopinl Information
~ I ~ FRI!I.tl.on and commUnlcauorI pI..-.:.:;durel.
I 3. fOl' data 10 be gcncrakd within lub .. aubsyl&cm
I . IdeAlity opc,.,lon.l1y 'cauble dua I'0upln~ I . apeelfy [ommunl[aUlln now I I I
lptc1fy (tequuo,;y
I cu .. hlUb Inpul and uUlpullepalu.
I lor C Icb ''''poll
I lpedfy cootenl
I .velop 'orm.u I I
" I I Tell IWl .ml dcwelop"'1!. lhe I I dn'-,II
L ___ ---- - - -;:. _____ ~ -=-l-=-- -=. - - - - --~:::~ ... n~ 7 - -- - -- ---
)0 .,ml kv.:l ,,' IJIIHlOl'hm. ·11 ludl:1 (''':''IUot"III·
-Ill luJu bC"IIIII::Ik:Y .IU" k .. .,J .." gt.:' ... ·'.lh ....
I ! Dr Vlt lup Ie (,Uldl nM a noJ It pot 'Inl P'IXC (lUte.
I 11,-""111), ,rdlll .. luiPt.1 UII'P'If' .Wlt."
I hkntll) rUOW'lCI 1M:l'drr1.l
I hknrUy II.lnm" Ol'cJJ EllablUb mc~ballUm I I
I I lor drrwaLIIII
I I ""Ipok U .. I, M"nagem<,nl fl,III.-Ilon .---------------I I)c .. c:lvp 1)11. M.Q.lKCn,,·ul :)lIu[I",o: 1
I I
I " 1 I I I I hnpklll~·nl Ih" SY"O:III 1
I 1 I 1 ~-------------------
., I I I
• I I I
.J
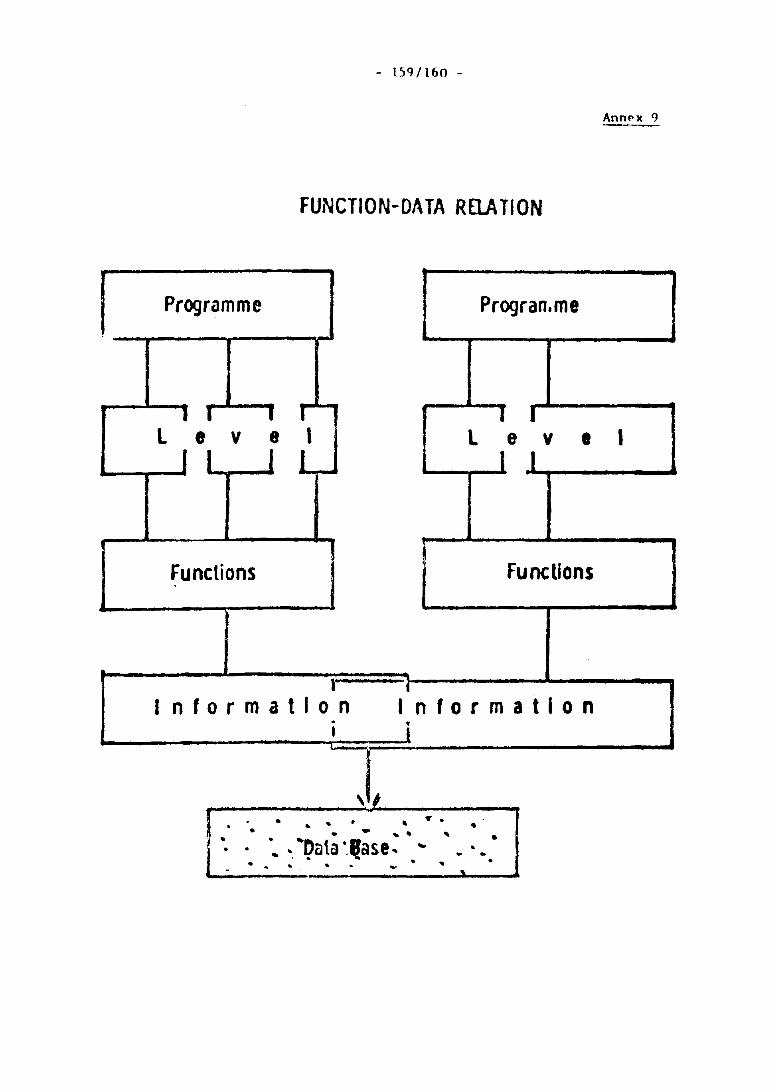
- lS'I/l60 -
Annf'x 9
FUNCTION-DATA RElATION
Programme Progran.me
I I I I I I l e v e I l e v • I
I I J I J 1
Functions Functions
1 I
I nformatlon Information . j I
-j
. . -.,.. ...... ,. ... .... . .. ,.. , .
" .. ' Data ".Ilase.. ~ ~ •• . .. ',. .. .. - .......... .....1
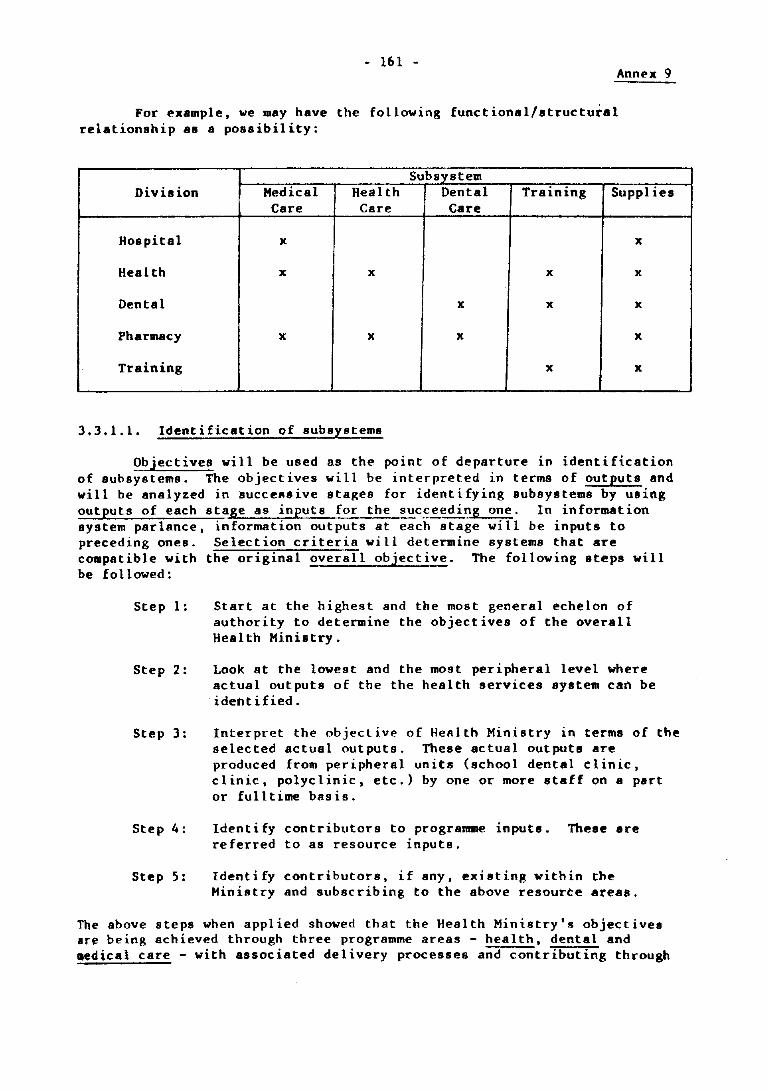
• 161 . Annl'X 9
For example, we may have the following functional/structural relationship as a possibility:
Subsystem Division Medical Health Dental Training Suppl iI's
Care Care Care
Hospital x x
Health x x x x
Dental x x x
Pharmacy x x x x
Training x x
3.3.1.1. Identification of subsystems
Objectives wi 11 be used as the point of departure in identi fication of subsystems. The objectives will be interpreted in terms of outputs and will be analyzed in successive stages for identifying subsystems by using outputs of each stage as inputs for the suc~eeding one. In information system parlance, information outputs at each stage wi 11 be inputs to preceding ones. Selection criteria will determine systems that are compatible with the original overall objective. The following steps will be followed:
Step 1:
Step 2:
Step 3:
Step 4:
Step 5:
Start at the highest and the most general echelon of authority to determine the objectives of the overall Health Ministry.
Look at the lowest and the most peripheral level where actual outputs of the the health services system can be ideM i fied .
Interpret the objective of Health Ministry in terms of the selected actual outputs. These actual outputs are produced from peripheral units (school dental clinic, clinic, polyclinic, etc.) by one or more staff on a part or fulltime basis.
Ident i fy contributors to programme inputs. These are referred to as resource inputs.
Identify contributors, if any, existing within the Ministry and subscribing to the above resource areas.
The above steps when applied showed that the Health Ministry's objectives are being achieved through three programme areas - health, dental and .edical care - with associated delivery processes and contributing through
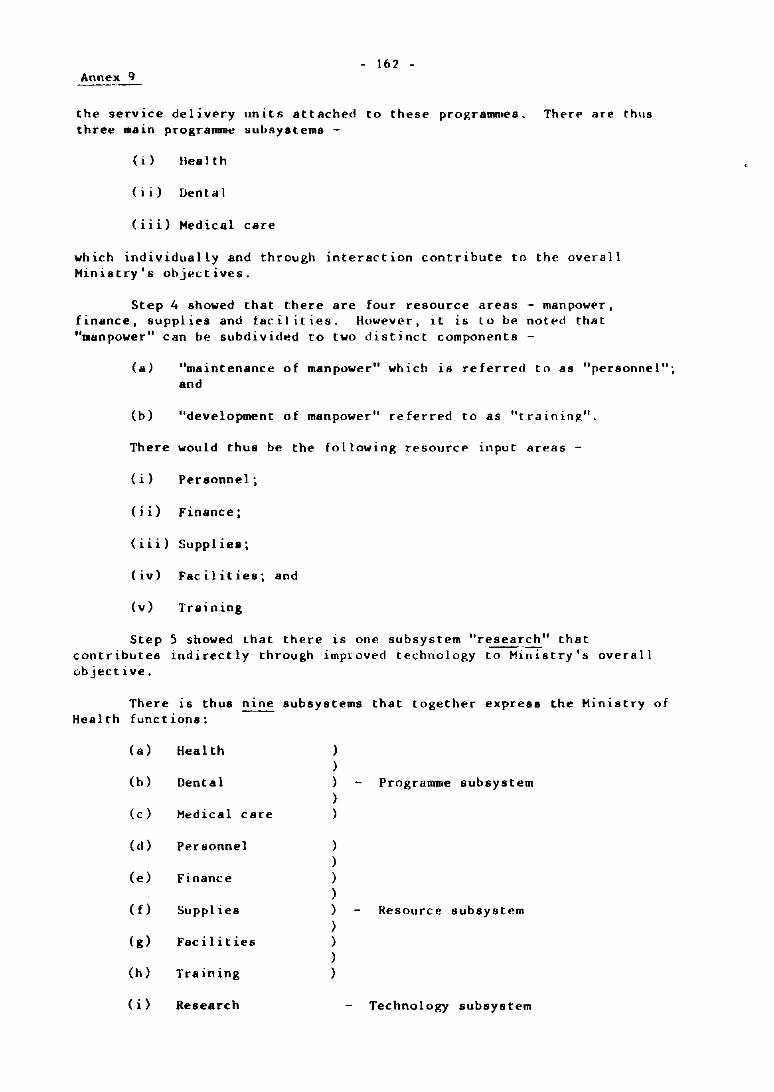
- 162 -Annex 9
the service delivery units attached to these programmes. There are thus three Main programme subsystems -
(i) lIealth
(ii) Ilental
(iii) Medical care
which individually and through interaction contribute to the overall Ministry's objectives.
Step 4 showed that there are four resource areas - manpower, finance, supplies and facilities. However, it is LO be noted that "manpower" can be subdivided to two disti nct components -
(a) "maintenance of manpower" which is referred to as "personnel"; and
(b) "development of manpower" referred to as "traininl!,".
There would thus be the following resource input areas -
(i) Personnel;
(ii) Finance;
(iii) Suppliea;
(iv) Facilities; and
(v) Training
Step 5 showed that there is one subsystem "research" that contributes indirectly through impl-oved technology to Ministry's overall objective.
There IS thus nIne Health functions:
(a) Heal th
(h) Ilental
(c) Medical care
(d) Personnel
(e) Finance
(f) Supplies
(g) Facilities
(h) Training
(i) Research
subsystems that together express the Ministry of
) )
) Programme subsystem ) )
) )
) ) ) Resource subsystem ) ) ) )
Technology subsystem
- 161 -Annex 9
3.3.1.2 Identification of sub-subsystem
For each subsystem,
Start with the objective of the subsystem that is consistent with the Miniatry of Health objective;
List all organizational subdivisions In each subsystem, e.g. MCH, Health Education, Epidemiology;
Liat programme functions of these subdivisions;
Identify subprogrammes by splitting organizational divisions to functional components and specifying objectives of the subprograll1llle in relation to the objective of subsystem. This can be done by identifying the specific target ~roup to which services are primarily directed.
e.g., HeH Division has maternal care,
(a) Maternal care aimed at pregnant women at prenatal, natal and post-natal stage;
(b) Family planning aimed at women of child-bearing age;
(c) Child care aimed at infants, toddlers and pre-schoolchildren;
(d) School health aimed at schoolchildren;
(e) General sanitation aimed at improving community environment.
Separate those subprogrammes which directly contribute to the output of the parent programme subsystem, e.g., maternal care, child care, tuberculosis control, personal dental care, etc. which has direct interface with and contributes to target group. Generally, these are service delivery subprogramme or sub-subsystem.
Classify the remaining subdivisions whose functions provide support and hence indirectly contribute to the output of the service delivery sub-subsystems, e.g., health education, applied food and nutrition and epidemiology, laboratory. These are support sub programmes or sub-subsystems.
For the Ministry of Health, sub-subsystems are given in pages 22 and
Figure I on page 25 gives the suh-subsystems which together form ~he functional components of the Ministry of Health.
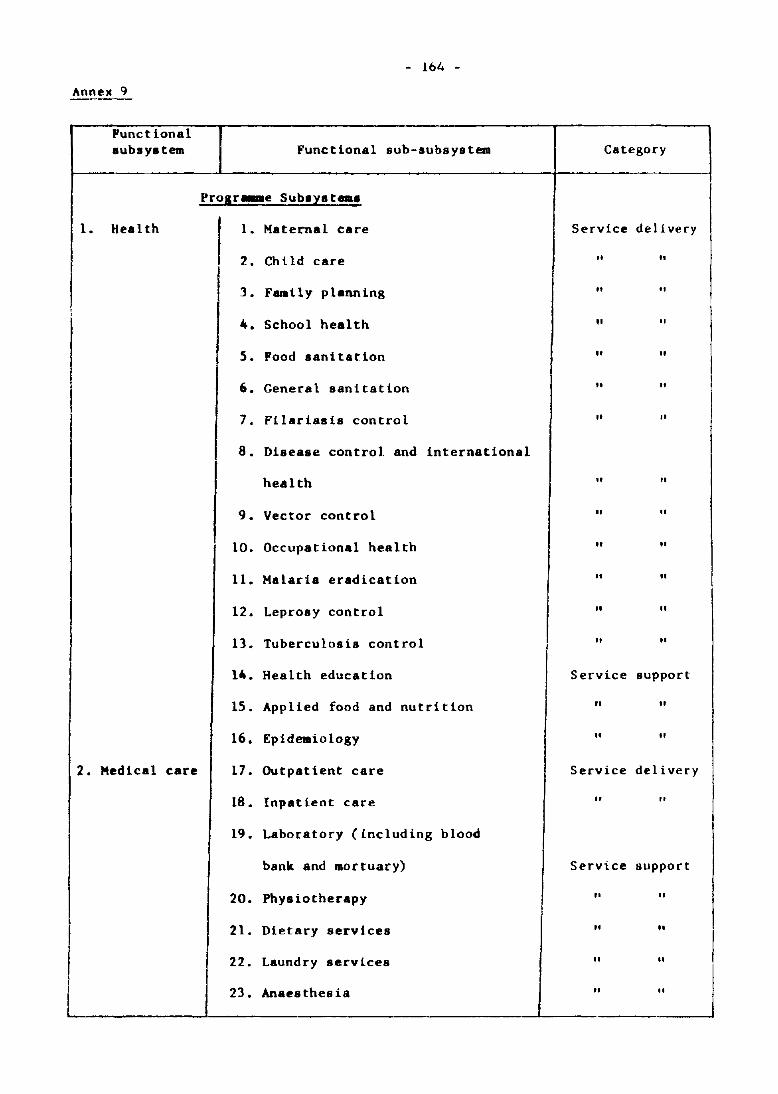
- 164 -
Annex 9 -----
Functional aubsyatem Functional sub-subsystem Category
-
Progr ... e Subayat ...
1. Health 1. Haternal care Service delivery
2. ChUd care " "
I 3. Family planning " "
4. School health " "
5. Food sanitation " "
6. General sanitation " "
7. Filariaaia control " "
8. Disease control and international
health " "
9. Vector control " "
10. Occupational health II "
11. Halaria eradication " "
12. Leproay control " "
13. Tuberculosis control " "
14. Health education Service support
15. Applied food and nutd tion " II
16. Epidemiology " II
I 2. Medical care 17. Outpatient care Service delivery
18. Inpatient care II "
19. Laboratory (including blood
bank and mortuary) Service support
20. Physiotherapy II II
21. Dietary services II "
I I 22. Laundry services " "
~ I
I 23. Anaesthesia II
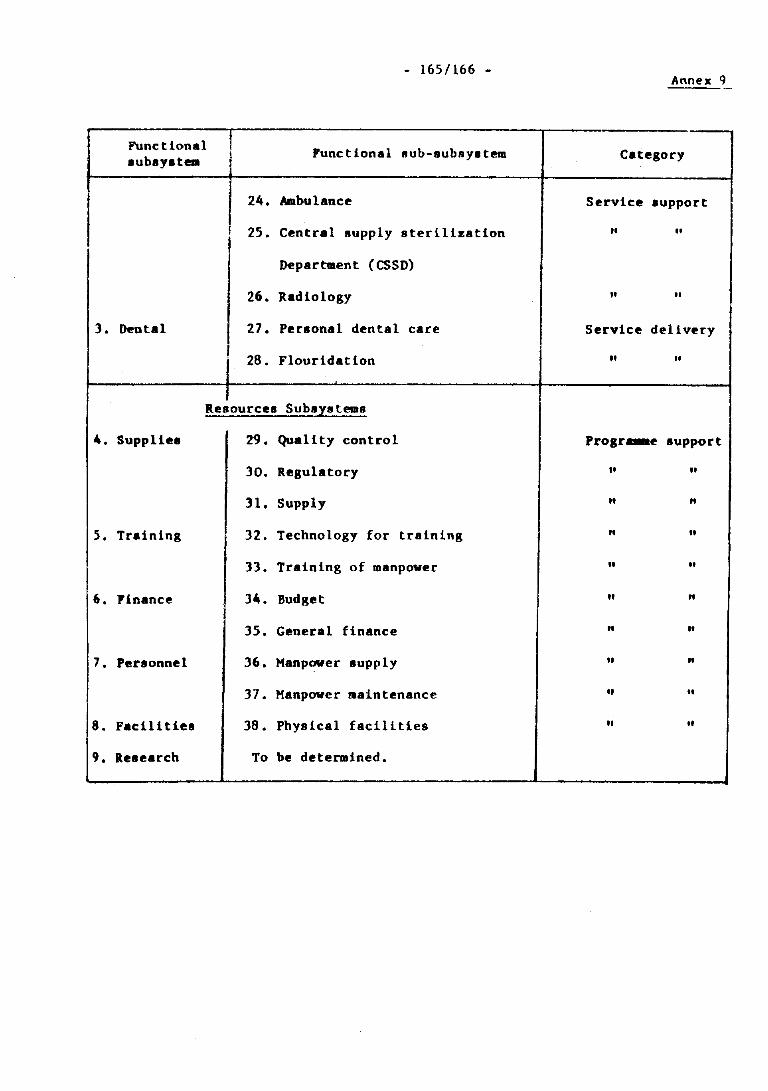
- 165/166 -Annex 9
Functional Functional lIub-subsystem Category lublYltem
24. Ambulance Service lupport
J 25. Central supply s teril iza tion ,. "
Department (esSD)
26. Radiology " "
3. Dental 27. Personal dental care Service delivery
28. Flouridation " "
Resources SubsIstem"
4. Suppliel 29. Quality control Progr_e support
30. Regulatory ,. "
31. Supply " "
5. Training 32. Technology for training " "
33. Training of manpower " "
6. Finance 34. Budget " "
35. General finance n "
7. Personnel 36. Manpower supply " n
37. Manpower ..aintenance " "
8. FaciUties 38. Physical facilities " "
9. Research To be determined.
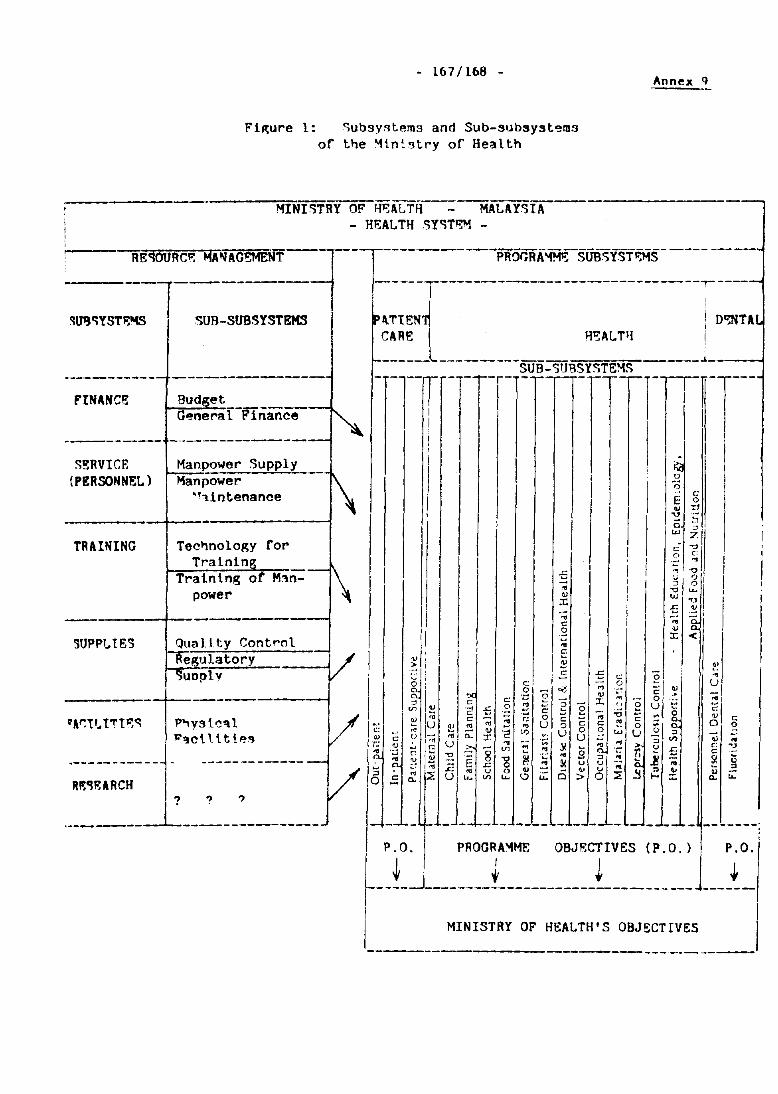
- 167/168 -
F1p;ure 1: <;ub3y~tem3 and Sub-slJbsyst<;!ms of t~e ~ln~~try of Health
MINffiRY OF HBALTH----"MALAY.~T.A --- HEAL TH ,,)Y')T~ -
CARE H'!:AL TIl
------ --------SUB-')UBSY')TE~5
Annex q
____ ..4 __ ._~
FINANce r- -irTr-')!I!RVICF.
(PERSONNEL)
TRAINING
-------------Manpower Supply Manpower
·''l.intenance
Tec~nolop;y for Train1n
Training 0
power
------~----------------~ SUPPl.IES
.. -----------
? ? ?
._------ ,-"--
o
'"
- 169/170 -Annex Q
3.3.2 Cuidelines Cor identification of functions and aSBoci~ted Areas of concern
The objective at this stage lS to get at a preliminary set of areas of concerns at different echelons of the Ministers of Health for various programmes and for different managerial functions.
Given that the Miniatry's activities can be grouped to distinct programme subsystems, it is clear that each of these sub-subsystems achievp their specific objectives through actual task performance Or operations and through _naserial functions to guide, direct and support these operations. Each of the sub-subsystems - be they resourc~ or programme -have certain managerial functions to be performed and these may consist of:
(i) planning
(ii) programming/budgetting
(iii) implementation - monitoring/control
(iv) evaluation and
(v) coordination
In addition there may be purely administrative/secretariat functions which, for the purpose of this HHIS project, have been kept out. The above managerial functions CRn be performed singly or in combination .t various echelons of the Ministry. It is to be noted, however, that the echelons performing these functions may vary from progra~ to programme, e.g. for finance aubsystem they may b" national, state and district. while for health subsystem they may be national. state, district, unit (e.g. main health centre) subunit (e.g. health subcentre) and sub-subunits (e.~. midwife clinics Different echelons can be stated as:
( i) na t ional
(ii) state
(iii) district
(iv) unit (e.g. MHC, hospitals)
(v) subunit (SHC, specialists in hospitals)
(vi) sub-subunit (e.g. MCQ, wards in hospitals)
Each of thel!le functions perfomed at difff'rent echelons will, however. hove specific objectives and specific areas of concern. For example, while monitoring at health eubcentre would deal with operational output. by the
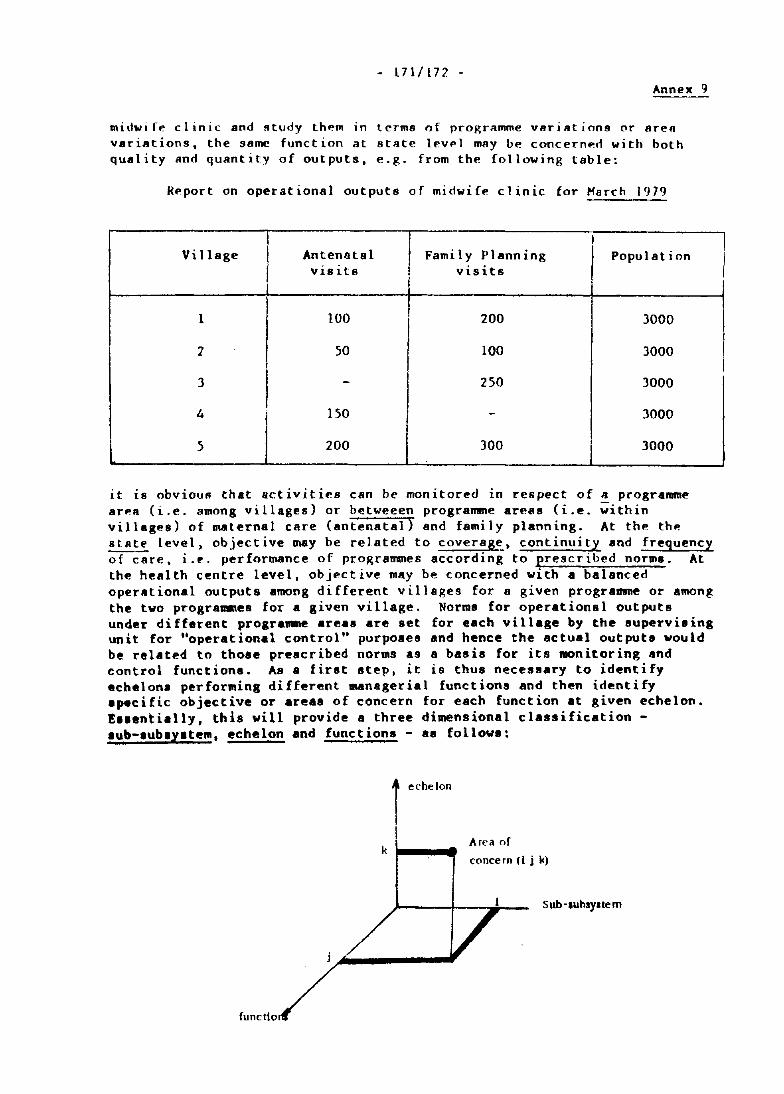
- 171/172 -Annex Cj
midwi fe clinic and Rtudy them in terms of programme varillt ions or area variations, the same funct ion at stllte leve1 may be concernerf wi th both quality and quantity of outputs, e.g. from the following table:
Report on operational outputs of midwife clinic lor March 1979
I Village Antenatal Family Planning Population
v is its visits
1 100 200 )000
'1 50 100 )000
I 3 - 250 3000
4 150 - 3000
5 200 300 3000
it i8 obvious that activities can be monitored in respect of II programme arell (i.e. among villages) or hetweeen programme areas (i.e. ;ithin vil1agf!8) of IMternal care (antenatal) and family planning. At the thO! ~ level, objective may he related to coveragt:.. continuity lind frequency of care. i.r'. performance of programmes according to prescribed norms. At the health centre level, objective may be concerned with a balanced operlltional outputs among different villages for a given programme or among the two programDes for a given village. Norms for operational outputs under different programme areas are set for each village by the supervising unit for "operational control" purpoaes and hence the actual outputs would be related to those prescribed norms as a basis for its monitoring and control functions. As a first step, it is thus necessary to identify echelons performing different managerial functions and then identify .pecific objective or areas of concern for each function at given echelon. E •• entially, this will provide 8 three dimensional classification -lub-IublYltem, echelon and functions - aa follow.:
I echelon
I k
Area of
concern (I j k)
Sub ·Iuhsylle m
I
I 1 I I
- 173/174 -Annex 9
Si.nce util ization of information is th., point of departure for information system development, it would bl' possible to identify information needs once the objectives/areas of concerns are clearly specified and described in terms of the three dimensions. Tsble ~iven on page )1 give!! a possible framework for identi fying i.nformation needs in thi~ perspective. At this stage of this phase, however, efforts would be directed in establishing only items 2, ] and 4 of the table for each lIub-lIubsystem (item I L The objl'ctivf' wi 11 be to identi fy who performs what functions and why. Following steps will be followed:
Step 1:
Step 2:
Step J:
Step 4:
Step 5:
Identify the programme managers/divisional directors responsible for each of the sub-subsystem.
ldenti (y di fferent decis ion-making echelons of the Ministry. Note that we are concerned with service management and not with service delivery/patient management.
Identify functions performed at each echelon.
Specify the objective of their functions.
Specify the areas of concern.
3.4 Outputs: l.is!: of sub-subsystem!! are given on pages ~ and 2:5 and an example of the results for different progranane areas as seen by th .. programme managers/divisional directors is given on pages " and ". Such a list wss prepsred for each of the 38 sub-subsystems a. a provisional ba.i. for the next phase and hence is not included here.
The Directors with their programme managers used the.e result! to identify the information needed, designation of perRon at a given echelon needing that information and frequency with which they are needed.
It should be noted and emphasized at this stage that this is a preliminary set to be used as a basis for the next phase - situation analysis. Civen this theoretical basis and the findings of Phase II: Situation Analysis, a final set have to be established. This final set will determine what information is needed, by whom (echelon and designation) it-rs-needed, when (frequency) it-rs-needed and why (function. and area of con~ern) it is needed. Sub-subsystem, echelon, function and frequency will thus become attrlbutes of the needed information.
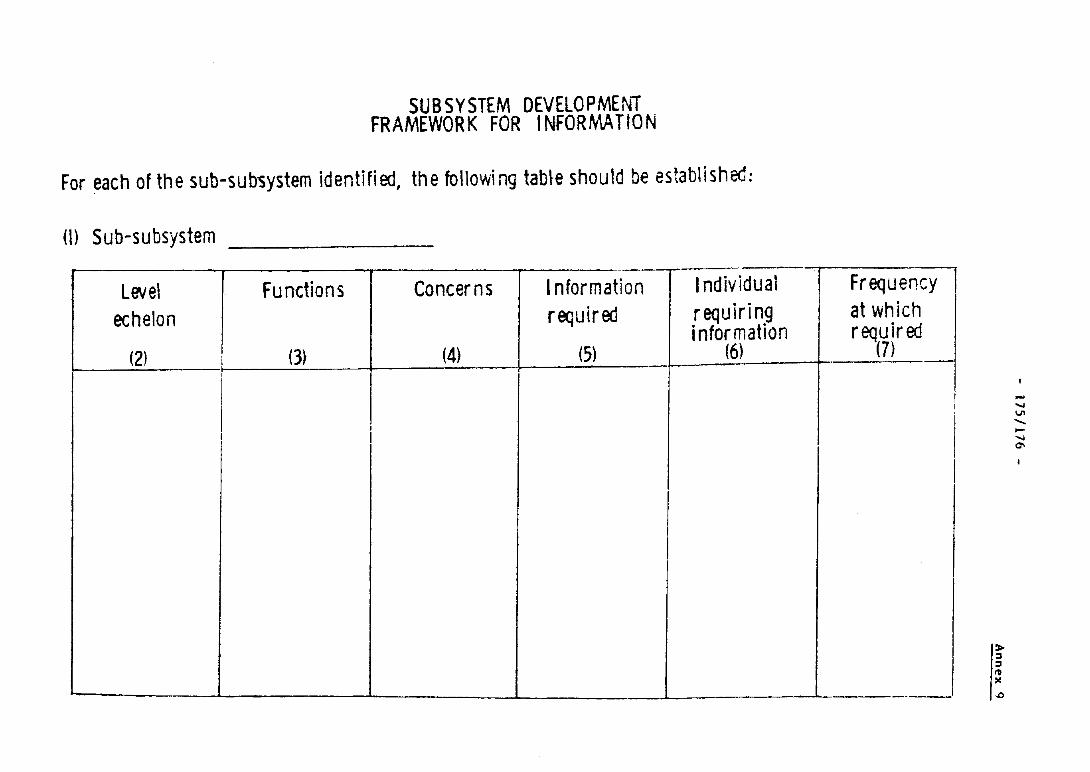
SUBSYSTEM DEVELOPMENT FRAMEWORK FOR I NFORMA TION
For each of the sub-sub~ystem identified, the following tab~e should be established:
(l) Sub-subsystem --------
level Functions Concerns Information Individual
echelon required requiri n9 i nfor mation
(2) (3) (4) (5) (6)
I I I
I 1 I I
Frequency 1 I
at which required
(7) . --
! I
I
I I
---
I~ I; ,:
... .... ...., ...... -.... 0\
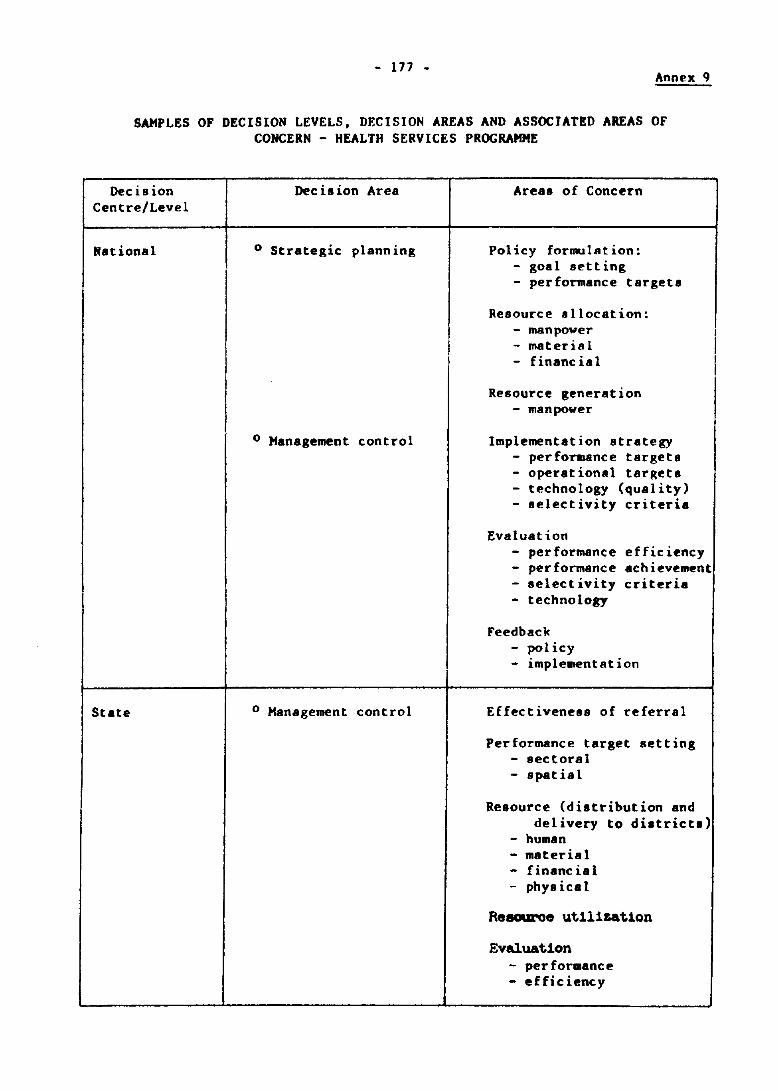
- 177 - Annex 9
SAMPLES OF DECISION LEVELS, DECISION AREAS AND ASSOCIATED AREAS OF CONCERN - HEALTH SERVICES PROGRAMME
Decision Centre/Level
National
State
Dec is ion Area
o Strategic planning
o Management control
o Management control
Areas of Concern
Policy formulation: - goa I set t ing - performance targets
Resource sllocation: - manpower - material - financial
Resource generation - manpower
Implementation strategy - performance targets - operational targets - technology (quality) - selectivity criteria
Evaluation - performance efficiency - performance achievement - selectivity criteria - technology
Feedback - pol icy - implementation
Effectiveness of referral
Performance target setting - sectoral - spatial
Resource (distribution and delivery to district.)
- human - material - financial - phy.ical
Reaouroe utilizat10n
Evaluation - performance - efficiency
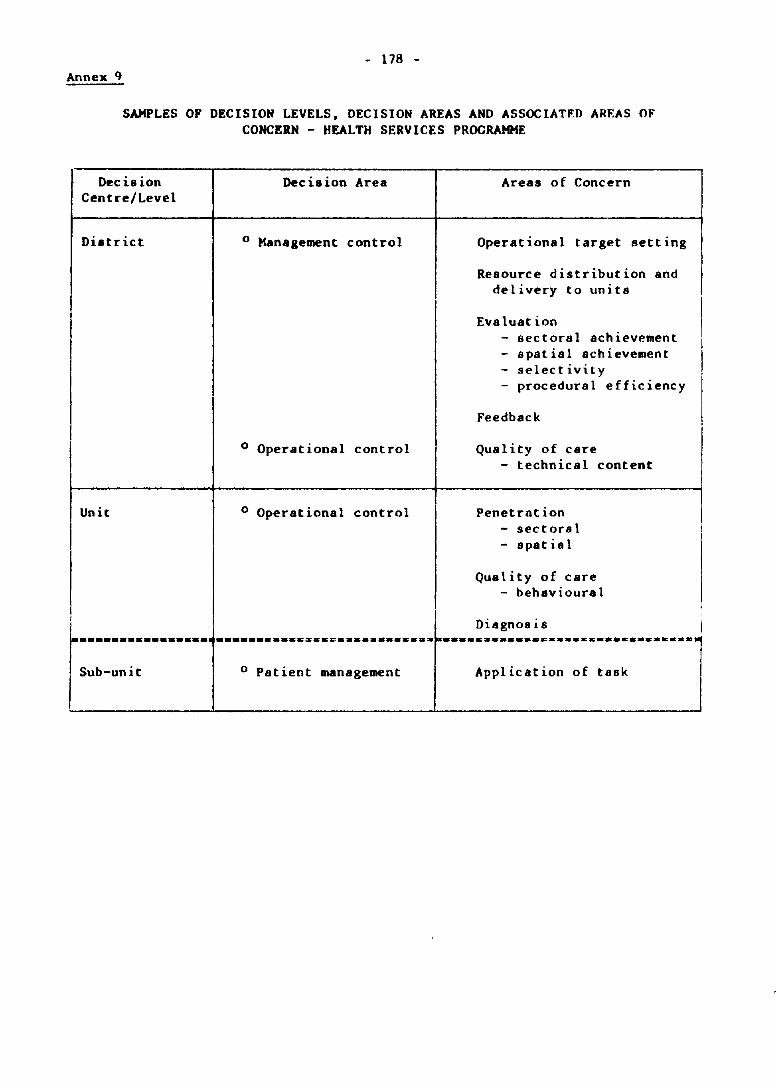
- 178 -Annex I}
SAMPLES OF DECISION LEVELS, DECISION AREAS AND ASSOCIATFD AREAS OF CONCERN - HEALTH SERVICES PROGRAMME
Decision Centre/Level
District
Unit
Decision Area
o Management control
o Operational control
o Operational control
Areas of Concern
Operational target setting
Resource distribution and delivery to units
Evaluation - sectoral achievement - spatial achievement - selectivity - procedural efficiency
Feedback
Quality of care - technical content
Penetrntion - sectoral - spatial
Quality of care - behavioural
~ Diagnosis I I :::::::: ............ :.:::::::-::::::::::---." .... :::~:::::::-::-::::··_·_··-1

- 179/180 -
TEST RUN STRATEGY AND ACTIVITIES
by
Dr Chee Chin Seang Deputy Director (Health)
Office of the Medical and Health Director Penang. Malaysia
ANNEX 10
- 181 -
Annex 10
HMIS TEST RUN
1. OBJECTIVES OF THE TEST RUN
1.1 To test the applicability of the basic documents in the field
(a) to find out the required data elements are obtainable from the existing source documents or from any other existing sources
(b) to find out whether there is a need
(i) to modify existing source documents or to develop new sources
(ii) for new instructions to be issued so that the required data will be recorded into the source documents.
1.2 To test out the instruction manuals, which accompany the basic documents, under field situation, in order to find out whether:
(a) the instructions are clear enough to result in the correct data being recorded into the basic documents by the operational staff;
(b) there is a need to amend the instruction manuals.
1.3 To identify any problems associated with a "non-parallel" run so that they can be solved or overcome before they undermine the confidence of the managerial, supervisory and operational staff particularly in the new information system.
1.4 To identify any other problems (operational/technical) associated with the new information system and find solutions for them.
1.5 To identify the training needs, and the preferred method of training and subsequently to work out the strategy for training on a long term basis.
1.6 To identify resource requirements (manpower/supplies/finance, etc.) by types and quantity so that successful implementation of the new information system is insured.
1.7 To test and re-design where necessary the communication flow (reporting system) for effective and efficient flow of appropriate and adequate information to managers/supervisors at various levels.
- 182 -
Annex 10
2. ROLES AND RESPONSIBILITIES OF STATE-LEVEL COORDINATOR AND FOCAL GROUP IN THE TEST-RUN AREA
2.1 State level Coordinator
2.1.1 To be responsible for the smooth implementation of the test-run.
2.1.2 To provide liaison between ISDG team and state officers involved in the test-run.
2.1.3 To coordinate and facilitate:
(i) (ii)
(iii)
(iv)
(v)
2.2 Focal group:
the release of staff for training the arrangement of transportation for ISDG member the provision of typist, clerical assistance and office boys when necessary the printing, collection and distribution of formats the purchase locally and supply of necessary stationery and office requirements
2.2.1 To assist HMIS in the selection of local staff for training and in the organization and supervision of such training.
2.2.2 To act as counterparts to respective ISDG members.
2.2.3 To report on necessary changes to formats and instr'Jction manuals to the relevant ISDG members.
2.2.4 To select key personnel in a district or institution who will then be responsible for the supervision of proper recording of data and the early reporting of any problems which may be encountered from time to time.
2.2.5 To be responsible for the transmission of decisions! solutions to these problems to the operational staff, and, at the same time, ensure that no unilateral changes to the basic documents or reports are made.
2.2.6 To ensure the discontinuation of old record books, registers which have been replaced by HMIS.
2.2.7 To inform ISDG members of any ad hoc requests from National Directors of Programmes for information, which h~ve not earlier been cleared by HMIS.
- 183 -
Annex 10
3. TRAINING STRATEGY
3.1 Training objective:
To develop a preferred method of training for each of the sub-systems or sub-sub system which can be used on a long term basis for its expansion and extension to other districts, states, and finally encompassing the whole nation.
3.2 Training strategy:
(a) The role of ISnG member will be:
(i) to work out the training content and method of training for the respective sub-system/sub-sub system.
(ii) To identify the supervision in each sub-system or sub-sub system and train them in the filling of forms. In turn, these supervisors will constitute the cores of local trainers.
(b) Interrruptions to daily operations of units/centres should be minimized.
3.3 Training (operational aspects):
(a) Locate the most suitable training places.
(b) The ISnG members will train the supervisory staff.
(c) Trained supervisory staff will in turn train the operational staff. The ISnG members will supervise, check and assist in the training of operational staff.
(d) Forms and instruction manuals will be sent to the trainees one week before training starts for them to study and subsequently to seek clarification of doubts and problems during the training sessions.
(e) Training will be in the form of lectures which will highlight the following:
(i) the purpose and value of the various forms
(ii) the need for accurate recording
(iii) the sources from which the data elements can be obtained.
This will be followed by practicals in the form of mode entry of data into the forms, during which the trainees are taught on the proper use of the instruction manuals.
- 184 -
Anne" ]0
(f) The training of operational staff may be on a one to one basis or in groups.
(g) Ultimate objective of the training strategy is to make use of the trained staff from test-run area to train staff in other parts of the country, so that the multiplier effect of thp training strategy will ultimately result in the training of all the staff on the country within the shortest possible time schedule.
4. DURATION OF THE TEST-RUN
Ideally, it should be tested for a dlJration of on(> calpndar year. This will enable the information on health activities/performance within the one year period to be captured.
This also facilitates the preparation and testing of weekly, monthly, quarterly or annual reports.
5. FEEDBACK MECHANISM
This mechanism starts as soon as the training ~s completed and the formats utilized. Feedback has to be regularly asked for by ISDG and Focal group members, as well as an ad hoc basis.
5.1 Any inconsistency arising from data collection should DP notified to ISOG members who wi 11 sugges t so lut ion to overcome it.
5.2 ISDG members should check the timeliness of information which is sent (communication flow) in the form of reports to the relevant managers.
5.3 [SDG should during the period of test-turn:
(i) evaluate the information requirements that have been captured 1n the new HMIS;
(ii) ensure that information obtained is actually being utilized by the managers who have requested for such information during situational analysis.
5.4 ISDG members should make random checks at the operational level to find out:
(i) the practicability of the formats; and
(ii) the problems associated with the filling of formats.
5.5 Problems, both technical and operational should be discussed between focal group and ISDG for possible solutions in order to rectify the situation.
- 185 -
Annex 10
6. EXPERIENCE OF HMIS TEST RUN
6.1 Technically, HMIS 1S an improvement over the old system of information collection, as
(a) it is more systematically and critically designed to gather useful and relevant information for management purposes; and
(b) it reduces unnecessary and overlapping information collection by local staff.
6.2 However, like any new information system, it tends to meet with a certain degree of resistance since change-over requires a degree of re-orientation of thinking and procedures.
6.3 The test-run was carried in an area which was compact but large enough to bring out the complexity of operations and variety of problems. This is important as it facilitates identification of various factors (such as training needs, supervision, logistics, information flow, feedback, etc.) which need to be considered in the nation-wide implementation of the newly designed information system.
6.4 Some of the critical areas, apart from information relevance and meaningfulness per se, where activities have to be formulated and developed for the smooth implementation of HMIS, are as follows:
(a) information related to training of various levels of management in the utilization of information;
(b) development of management environment in the assigning of authority and responsibility to solve problems encountered;
(c) development of feedback procedures.
6.5 In addition to the general summary above, participants will be able to identify in some detail problems in connexion with HMIS test-run when they visit the Project area in Penang.