Embed Size (px)
Citation preview
1
Cardiac Imaging
a t l a s imagen cardíaca
Normal Anatomy Anatomia normal
Chapter / Tema
11.1 Anatomical Basis of Cardiac Imaging
Bases anatómicas de la imagen cardíaca
Normal Cardiac Anatomy Anatomía cardíaca normal
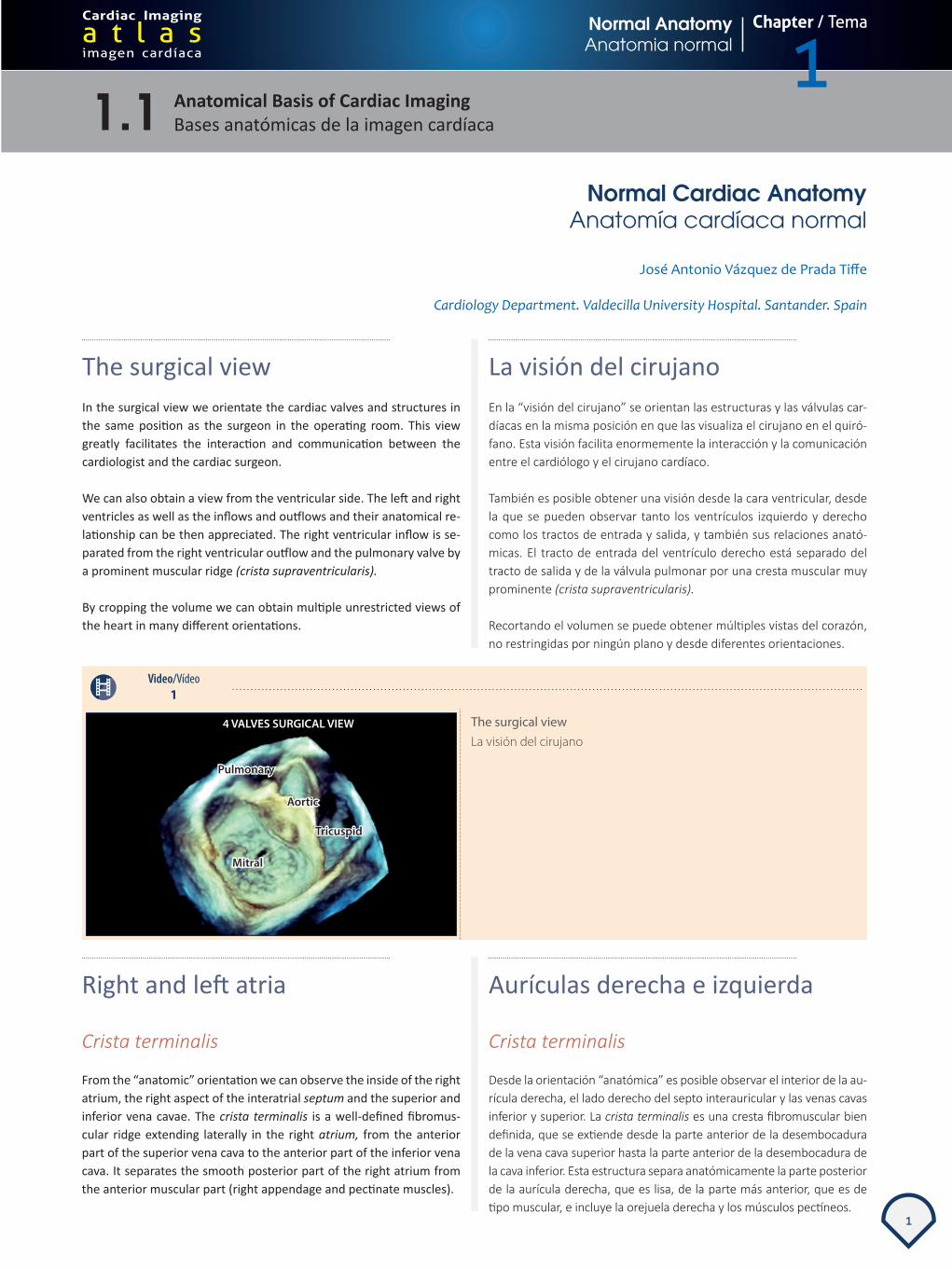
The surgical viewIn the surgical view we orientate the cardiac valves and structures in the same position as the surgeon in the operating room. This view greatly facilitates the interaction and communication between the cardiologist and the cardiac surgeon.
We can also obtain a view from the ventricular side. The left and right ventricles as well as the inflows and outflows and their anatomical re-lationship can be then appreciated. The right ventricular inflow is se-parated from the right ventricular outflow and the pulmonary valve by a prominent muscular ridge (crista supraventricularis).
By cropping the volume we can obtain multiple unrestricted views of the heart in many different orientations.
La visión del cirujanoEn la “visión del cirujano” se orientan las estructuras y las válvulas car-díacas en la misma posición en que las visualiza el cirujano en el quiró-fano. Esta visión facilita enormemente la interacción y la comunicación entre el cardiólogo y el cirujano cardíaco.
También es posible obtener una visión desde la cara ventricular, desde la que se pueden observar tanto los ventrículos izquierdo y derecho como los tractos de entrada y salida, y también sus relaciones anató-micas. El tracto de entrada del ventrículo derecho está separado del tracto de salida y de la válvula pulmonar por una cresta muscular muy prominente (crista supraventricularis).
Recortando el volumen se puede obtener múltiples vistas del corazón, no restringidas por ningún plano y desde diferentes orientaciones.
Video/Vídeo1
The surgical viewLa visión del cirujano
Right and left atria
Crista terminalis
From the “anatomic” orientation we can observe the inside of the right atrium, the right aspect of the interatrial septum and the superior and inferior vena cavae. The crista terminalis is a well-defined fibromus-cular ridge extending laterally in the right atrium, from the anterior part of the superior vena cava to the anterior part of the inferior vena cava. It separates the smooth posterior part of the right atrium from the anterior muscular part (right appendage and pectinate muscles).
Aurículas derecha e izquierda
Crista terminalis
Desde la orientación “anatómica” es posible observar el interior de la au-rícula derecha, el lado derecho del septo interauricular y las venas cavas inferior y superior. La crista terminalis es una cresta fibromuscular bien definida, que se extiende desde la parte anterior de la desembocadura de la vena cava superior hasta la parte anterior de la desembocadura de la cava inferior. Esta estructura separa anatómicamente la parte posterior de la aurícula derecha, que es lisa, de la parte más anterior, que es de tipo muscular, e incluye la orejuela derecha y los músculos pectíneos.
José Antonio Vázquez de Prada Tiffe
Cardiology Department. Valdecilla University Hospital. Santander. Spain

2
Normal Anatomy Anatomía normal
Chapter / Tema
1Cardiac Imaging
a t l a s imagen cardíaca
Video/Vídeo2
Crista terminalisCrista terminalis
Right and left atria
From the “anatomic” orientation we can observe the inside of the right atrium, the right aspect of the interatrial septum and the superior and inferior vena cavae. Rotating 180O we can observe the left aspect of the interatrial septum and the entry of the right upper pulmonary vein.
Aurículas derecha e izquierda
Desde la orientación “anatómica” se puede observar el interior de la aurícula derecha, el lado derecho del septo interauricular y las venas cavas inferior y superior. Si se rota la imagen 180º, es posible obser-var el lado izquierdo del septo interauricular y la desembocadura de la vena pulmonar superior derecha en la aurícula izquierda.
Video/Vídeo3
Right and left atriaAurículas derecha e izquierda
Eustachian ridge and Eustachian valve
From the “anatomic” orientation we can observe the inside of the right atrium. The Eustachian ridge is a well-defined fibromuscular crescent-shaped structure reaching from the inflow of the inferior vena cava to the interatrial septum, at the anterior limit of the fossa ovalis. To the right of the Eustachian ridge lies the exit of the coronary sinus. In some patients (< 10%), there is a cavity (“pouch”) in the sub-eusta-chian region (between the septal insertion of the ridge and the fossa ovalis). This pouch can make difficult the cannulation of the coronary sinus. Remnants of the Eustachian valve can be observed as very thin filaments extending from the inflow of the inferior vena cavae to the proximal aspect of the Eustachian ridge.
Cresta de Eustaquio y válvula de Eustaquio
Desde la orientación “anatómica” se puede observar el interior de la aurícula derecha. La cresta de Eustaquio es una estructura fibromus-cular bien definida, de morfología crescente y que se extiende desde la desembocadura anterior de la vena cava inferior hacia el septo interau-ricular, en el límite anterior de la fosa oval. Hacia la derecha y anterior a la cresta de Eustaquio se observa la desembocadura del seno coro-nario. En algunos pacientes (< 10%) existe una pequeña cavidad tipo “bolsa marsupial” en la región localizada entre la cresta de Eustaquio y la fosa oval. Esta bolsa puede dificultar la canulación del seno coro-nario. En ocasiones se puede observar los remanentes de la válvula de Eustaquio como unos filamentos muy finos que se extienden desde la desembocadura de la cava inferior hacia el aspecto proximal de la cresta de Eustaquio.

3
1.1 Anatomical Basis of Cardiac Imaging Bases anatómicas de la imagen cardíaca
Normal Cardiac Anatomy Anatomía cardíaca normal
Video/Vídeo4
Eustachian ridge and Eustachian valveCresta de Eustaquio y válvula de Eustaquio
Thebesian valve
From the “anatomic” orientation we can observe the inside of the right atrium and the superior and inferior vena cavae. At the right of the Eustachian ridge we can see the coronary sinus, and the remnants of a Thebesian valve. The Thebesian valve is the embryological rem-nant of the right sinoatrial valve, guarding the coronary sinus ostium.
There are several types and different degrees of development of The-besian valves, ranging from complete absence of the valve to well de-veloped and obstructive valves. Developed valves can interfere with cannulation of the coronary sinus.
Válvula de Tebesio
Desde la orientación “anatómica” es posible observar el interior de la au-rícula derecha, el lado derecho del septo interauricular y las venas cavas inferior y superior. Hacia la derecha de la cresta de Eustaquio se puede ver el seno coronario y los restos de la válvula de Tebesio. La válvula de Tebesio es el remanente embriológico del velo derecho de la válvula del seno venoso, que guarda la desembocadura del seno coronario.
Hay varios tipos y diferentes grados de desarrollo de las válvulas de Tebesio, que van desde su ausencia hasta la presencia de válvulas muy desarrolladas y obstructivas. En este último caso, las válvulas pueden interferir y dificultar la canulación del seno coronario.
Video/Vídeo5
Thebesian valveVálvula de Tebesio
Interatrial septum
Right and left interatrial septum
From the “anatomic” orientation we can observe the inside of the right atrium, the right aspect of the interatrial septum and the right aspect of the fossa ovalis. Note that the superior and inferior vena cavae are
Septo interauricular
Lados izquierdo y derecho del septo interauricularDesde la orientación “anatómica” es posible observar el interior de la aurí-cula derecha, el lado derecho del septo interauricular y el lado derecho de

4
Normal Anatomy Anatomía normal
Chapter / Tema
1Cardiac Imaging
a t l a s imagen cardíaca
in the true anatomic position. After a 180⁰ rotation of the image, we observe the left aspect of the interatrial septum, the left aspect of the fossa ovalis and the exit orifice of the foramen ovale tunnel.
la fosa oval. Se puede observar que las venas cavas superior e inferior están es su posición anatómica correcta. Tras una rotación de la imagen de 180⁰ se puede observar el lado izquierdo del septo interauricular, así como el lado izquierdo de la fosa oval y el orificio de salida del túnel del foramen oval.
Video/Vídeo6
Right and left aspect of the interatrial septumLados izquierdo y derecho del septo interauricular
Patent foramen ovale
A patent foramen ovale can be observed in up to 25% of the adult nor-mal population. From the left atrial “anatomic” orientation we crop the interatrial septum from above and then tilt the septum to observe the foramen ovale tunnel in the left aspect of the interatrial septum. After rotating again the septum 180⁰ to get back to the right atrial ana-tomic orientation, we crop the lower aspect of the right atrium to get a better view of the entry to the tunnel from the right side.
Foramen oval permeable
Se puede observar la persistencia de un foramen oval permeable hasta en el 25% de la población adulta sana. Desde la orientación anatómica en la aurícula izquierda se recorta el septo interauricular desde arriba y se le inclina ligeramente para observar el túnel del foramen oval en su recorrido por el septo interauricular izquierdo. Después se rota de nuevo el septo 180⁰ para volver a la orientación anatómica desde la aurícula derecha y se recorta la aurícula derecha desde abajo para observar ade-cuadamente la entrada del túnel del foramen oval desde el lado derecho.
Video/Vídeo7
Patent foramen ovaleForamen oval permeable
Pulmonary veins
Left pulmonary veins
From the “surgical” orientation we can observe the left atrium from above. To the left we can observe, side by side, the left atrial appen-
Venas pulmonares
Venas pulmonares izquierdas
Desde la orientación del cirujano se observa la aurícula izquierda desde arriba. En el lado izquierdo es posible ver, lado a lado, la orejuela iz-

5
1.1 Anatomical Basis of Cardiac Imaging Bases anatómicas de la imagen cardíaca
Normal Cardiac Anatomy Anatomía cardíaca normal
Video/Vídeo8
Left pulmonary veinsVenas pulmonares izquierdas
dage and the left superior pulmonary vein, separed by a well-defined ridge, the Marshall ligament. The Marshall ligament is a vestigial fold of the pericardium containing fibrous and nervous filaments envelo-ped in fat bands, and contains the oblique vein of Marshall, that drains into the coronary sinus. With an anterior tilt, the left lower pulmonary vein can be appreciated.
quierda y la vena pulmonar superior izquierda, separadas por una cresta bien definida (ligamento de Marshall). El ligamento de Marshall es un vestigio embriológico del repliegue pericárdico que contiene filamentos fibrosos y nervios envueltos en bandas grasas. También contiene la vena oblicua de Marshall, que drena en el seno coronario. Con una inclina-ción anterior se puede observar la vena pulmonar inferior izquierda.
Right pulmonary veins
From the “anatomic” orientation we can observe the inside of the right atrium, the right aspect of the interatrial septum and the supe-rior and inferior vena cavae. Rotating 180⁰ we can observe the left aspect of the interatrial septum and the entry of the right upper pul-monary vein.
Venas pulmonares derechas
Desde la orientación “anatómica” es posible observar el interior de la aurícula derecha, el lado derecho del septo interauricular y las venas cavas inferior y superior. Con una rotación de 180⁰ se observa el lado izquierdo del septo interauricular y la desembocadura de la vena pul-monar superior derecha.
Video/Vídeo9
Right pulmonary veinsVenas pulmonares derechas
Cardiac valves
Normal mitral valve with undefined leaflet scallopsFrom the surgical view we observe the anterior and posterior leaflets of the mitral valve.
Válvulas cardíacas
Válvula mitral normal con segmentos no definidosDesde la orientación del cirujano se observa el velo anterior y el velo posterior de la válvula mitral.

6
Normal Anatomy Anatomía normal
Chapter / Tema
1Cardiac Imaging
a t l a s imagen cardíaca
Example 1. The anterior leaflet is bigger than the posterior leaflet. The leaflets and the anterolateral (ALc) and posteromedial (PMc) commi-sures are sharply defined both from the atrial and from the ventricular side. However, there is no clear definition or separation of the diffe-rent scallops of the leaflets.
Example 2. Same orientation, and again we observe clearly the lea-flets and the commisures, without separation in scallops.
This is a completely normal finding.
Ejemplo 1. El velo anterior es mayor que el velo posterior. Los velos y las comisuras (anterolateral y posteromedial) están claramente de-finidos, tanto desde el lado auricular como desde el lado ventricular. Sin embargo, no se puede apreciar una definición o separación de los diferentes segmentos de los velos.
Ejemplo 2. En la misma orientación, de nuevo se observa con claridad los velos y las comisuras, pero sin definirse una separación en segmentos.
La falta de definición de los segmentos es un hallazgo completamente normal.
Video/Vídeo10
Normal mitral valve with undefined leaflet segmentsVálvula mitral normal con segmentos no definidos
Normal mitral valve with separate leaflet scallopsFrom the surgical view, we observe the anterior and posterior lea-flets of the mitral valve from the side and then from the ventricular side.
Example 1. The anterior leaflet is bigger than the posterior leaflet. The posterior leaflet has some indentations, clearly separating the sca-llops (P1, P2 and P3). During systole, many aditional small “scallops” without actual indentation can be identified (*).
Example 2. In this case, the posterior leaflet scallops (P1, P2 and P3) are separated by very sharp indentations almost reaching the mitral annulus (“cleft like” indentations), but the systolic closing of the valve is competent.
Example 3. In some individuals, some extra scallops at the commi-sural level can be present (commisural segments c and c), which can be differentiated from the ordinary posterior leaflet scallops (P1, P2 and P3).
All the anatomical variations described for the former 3 examples can be considered as completely normal findings.
Válvula mitral normal con separación de los segmentos Desde la orientación del cirujano se observa los velos anterior y pos-terior de la válvula mitral, primero desde el lado auricular y después desde el lado ventricular.
Ejemplo 1. El velo anterior es mayor que el velo posterior. El velo pos-terior tiene algunas indentaciones, que separan los segmentos con claridad (P1, P2 y P3). Durante la sístole se puede observar múltiples “festones” de pequeño tamaño que no se corresponden con indenta-ciones (*).
Ejemplo 2. En este caso, los segmentos del velo posterior (P1, P2 y P3) están separados por indentaciones muy profundas, que prácticamente alcanzan el anillo mitral (indentaciones tipo pseudo-cleft). Sin embar-go, el cierre sistólico es perfectamente competente.
Ejemplo 3. En algunos individuos se puede observar segmentos adicio-nales a nivel de las comisuras (segmentos comisurales c-c) diferencia-dos de los segmentos posteriores habituales (P1, P2 y P3).
Todas las variaciones anatómicas descritas en los 3 ejemplos anteriores se pueden considerar como hallazgos completamente normales.

7
1.1 Anatomical Basis of Cardiac Imaging Bases anatómicas de la imagen cardíaca
Normal Cardiac Anatomy Anatomía cardíaca normal
Video/Vídeo11
Normal mitral valve with separate leaflet scallopsVálvula mitral normal con separación de los segmentos
Aortic valve and adjacent structures
In the anatomic orientation, we observe the anteriorly located right atrium and the more posterior left atrium next to the Valsalva sinuses and the aortic valve. From this position we can appreciate a well-de-fined Eustachian ridge. Rotating and cropping the image, we observe laterally the aortic valve and the left ventricular outflow, as well as the left atrium and the mitral valve. We get the image back to the anato-mic orientation, and an anterior tilt shows the orifice of the coronary sinus right below the Eustachian ridge.
Cropping of the aortic valve shows a fine fluttering of the three lea-flets, which is a common finding in young, healthy persons. A 180⁰ rotation shows the left ventricular outflow tract, with its usual elip-tical shape.
Válvula aórtica y estructuras adyacentes
En la orientación anatómica se observa la aurícula derecha situada an-teriormente y la aurícula izquierda situada más posteriormente, junto con los senos de Valsalva y la válvula aórtica. Desde esta posición se puede apreciar una cresta de Eustaquio bien definida. Rotando y recor-tando la imagen se observa lateralmente la válvula aórtica y el tracto de salida del ventrículo izquierdo, así como la aurícula izquierda y la válvula mitral. Si se vuelve a la orientación anatómica y una inclinación anterior, se muestra la desembocadura del seno coronario justo debajo de la cresta de Eustaquio.
El recorte de la válvula aórtica muestra un fino “aleteo” de los tres ve-los, que es un hallazgo normal en personas jóvenes sanas. Una rotación de 180⁰ muestra el tracto de salida del ventrículo izquierdo con su ha-bitual configuración en forma de elipse.
Video/Vídeo12
Aortic valve and adjacent structuresVálvula aórtica y estructuras adyacentes
Tricuspid valve
From the “surgical” orientation we observe the right atrium from above. We can see the tricuspid annulus and valve. During systole, in the ante-rosuperior quadrant, part of the right atrial appendage with some pecti-nate muscles can be appreciated. The tricuspid valve has three leaflets:
Válvula tricúspide
En la orientación anatómica se observa la aurícula derecha situada anterior-mente y en la orientación del cirujano se observa la aurícula derecha desde arriba. Es posible apreciar el anillo tricuspídeo y la válvula tricúspide. Duran-te la sístole se puede apreciar parcialmente la orejuela derecha y sus mús-

8
Normal Anatomy Anatomía normal
Chapter / Tema
1Cardiac Imaging
a t l a s imagen cardíaca
• Septal leaflet. • Anterior leaflet. • Posterior leaflet.
culos pectíneos en el cuadrante anterosuperior. La válvula tricúspide tiene tres velos:
• Velo septal. • Velo anterior. • Velo posterior.
Video/Vídeo13
Tricuspid valveVálvula tricúspide

9
References Bibliografía
References/Bibliografía 1.11. Faletra F, Ho SY, Auricchio A. Anatomy of Right Atrial Structures by Real-Time 3D Transesophageal Echocardiography. J Am Coll Cardiol Img
2010; 3; 966-975.
2. Faletra F, Demertzis S, Pedrazzini G, et al. Three-Dimensional Transesophageal Echocardiography in Degenerative Mitral Regurgitation. J Am Soc Echocardiogr 2015; 28: 437-448.
3. Mlynarski R, Mlynarska A, Haberka M, et al.The Thebesian valve and coronary sinus in cardiac magnetic resonance. J Interv Card Electrophysiol 2015; 43: 197-203.
4. García Fernández MA, Gómez de Diego JJ, Nuñez Gil IJ, et al. Atlas De Anatomía Cardíaca. Correlación con las técnicas de imagen. CTO Editorial, SL. Madrid, 2011.





























