-
8/8/2019 Normal and Abnormal Torsional Development in
Children
1/5
CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 302, p. 22-268
1994 J. 8. Lippincott Company
Normal and Abnormal TorsionalDevelopment in Children
Guy Fabry, M.D., Ph.D., Liu Xue Cheng, M.D.,and Guy Molenaers,
M.D.
This study presents findings in a series of 123children with
intoeing gait. The intoeing wascaused by increased femoral
anteversion(IFA) in 70% of the cases, and internal tibialtorsion
(I")n 30%. Rotation of the hips,thigh-foot angle, Q-angle, and
computed to-mography measured anteversion and tibialtorsion divided
the two groups very clearly.In the IFA group, 40.3% of the patients
pre-sented with an externally rotated tibia and59.7% had an
internally rotated tibia. In theIT" group, the anteversion was
normal forage and the tibial torsion was significantlydecreased.
Eighty children who correctedtheir intoeing gait, and of whom 83.4%
hadIFA, were also reviewed: a decrease in ante-version was observed
in 20.5% of the pa-tients; 62.9% showed no decrease in
antever-sion.
In an article published 20 years ago," 864anteversion studies
were performed in 432normal children from one to 16 years oldusing
the Dunlap-Shands m e t h ~ d . ~hesestudies showed a decrease in
anteversionfrom an average of 32' at age one to 16'From Orthopaedic
Department, University HospitalPellenberg, Katholieke Universiteit
Leuven, Belgium.Reprint requests to Guy Fabry, M.D., University
Hos-pital, O rthopaedic Department, W eligerveld
1,B-3212Pellenberg, Belgium.Received: September 16, 1993.Revised:
November 18, 1993.Accepted: November 22, 1993.
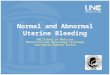
at age 16 (Fig. 1). Children with intoeingshowed an average
anteversion of 42.68'compared with an average of 24.14' in
thenormal group. The children with intoeingwere reevaluated after
an average follow-uptime of five years six months (154 hips).They
showed no significant decrease inanteversion, which averaged
39.48". It wasnoted that after the age of eight no signifi-cant
change in anteversion occurred. Thestudy also showed that
conservative treat-ment did not effectively alter the antever-sion.
An additional important finding was acompensatory external rotation
of the tibia(ERT) that created a malalignment of thepatella in 30%
of children in the first groupand 50% in the second group.
A review of the literature sho ws thatthe findings of this early
article have notbeen challenged significantly, an d, to theauthors
' know ledge, no other large serieshas been published. A review of
1 25 chil-dren with rotational abnormalities waspublished by
Cahuzac et al.,' classifyingthem clinically according to their
gaitpattern. They observed that 30% walkedwith internal rotation of
the knees andouttoeing fe et, resulting in com
pensatoryERT.Svenningsen et al. 3 studied hip rotationand intoeing
gait in 761 normal subjects,from age four years to adult. Sixteen
percentof the subjects had an intoeing gait, decreas-
22
-
8/8/2019 Normal and Abnormal Torsional Development in
Children
2/5
Number 302May, 1994 Torsional Development in Children 23
AG E IN YEARS
Fig. 1. Normal anteversion (N) and comparison of femoral torsion
in 154 hips in 77 patients withintoeing (2) after five years six
months' follow-up time (1 = first study, 2 = after follow-up, N
=normal). (Reprinted with permission from Fabry, G., MacEwen, G.
D., and Shands, Jr., A. R.: Torsionof the femur. J. Bone Joint.
Surg. 55A:1726, 1993.)
ing in frequency from 30% in the four-year-old group to 4% in
adults. They report asignificant correlation between intoeing
andincreased internal hip rotation or decreasedexternal hip
rotation. The decrease in inter-nal hip rotation with age was very
similar tothat found for fem oral anteversion in normalsubjects in
the authors' original study.4studied 30 childrenwith intoeing who
showed a decrease ofanteversion from an average of 42" at ageseven
to 28" at age 16, suggesting that sig-nificant regression of the
anteversion canoccur after eight years of age. The internalrotation
of the hips also decreased, but notto normal values, and correlated
with theincreased anteversion. They conclude thatall but five of
the 30 children had a normalgait at the last examination,
suggesting thatwith increased anteve rsion, most of the cor-rection
has occurred at the tibial level.These finding s differ from those
of the cu r-rent authors' earlier study. However, theypoint out
that this series was much smallerand that anteversion at age 16 is
stillabnormal.The problem of compensatory externaltibial rotation
has led many authors to study
Svenningsen et al.
anterior knee pain in adolescents in view ofrotational
deformities of the leg^.^,'^^,'^ Theproblem of possible secondary
changes inknees and hips is far from elucidated. In-creased
anteversion does not correct fullywith age and malrotation at the
knee seemsto be frequent. In this paper, a recent studyon a series
of children with intoeing gait,with a more de tailed analysis of
the differentcomponents of the deformity, is presented.MATERIALS
AND METHODSA consecutive group of 123 children was ana-lyzed during
a period of approximately sixmonths for torsion problems of the
lower ex-TABLE 1. Characteristicsof AllSubjects
NO.of Average age GenderGroup Limbs (Yeam) M FIFA 124 6.9 ? 2.9
43 43ITT 43 6.9 2 2.7 18 19COR 54 8.2 -c 2.8 36 44
IFA, increased femoral anteversion; ITT,nternal tibial
torsion;COR, spontaneously corrected intoeing gait.
-
8/8/2019 Normal and Abnormal Torsional Development in
Children
3/5
Clinical Orthopaedics24 Fabry et al. and Related ResearchTABLE
2. Clinical and Computed TomographicMeasurementsSign IFA In COR
MR 73.2 2 12.4 53.5 2 8.7 61.8 ? 14.4LR 19.9 5 11.6 32.4 f 10.5
29.1 t 9.8TFA -4.3 t 10.3 -13.2 2 10.2 2.3 t 8.2Q-angle 16.2 % 5.8
13.2 2 6.2 16.9 2 5.8AV 39.1 t 7.9 24.0 2 5.6TT 12.6 t 11.8 -5.3 2
9.6MR.medial rotation of the hip; LR. lateral rotationof the hip;
TFA, thigh-foot angle; AV, anteversion;V, tibial torsion; IFA,
increased femoral anteversion;In.nternal tibial torsion; COR,
spontaneouslycorrected intoeing gait.
tremities. One hundred twenty-four limbsshowed an increased
femoral anteversion (IFA)an d 43 an increased internal tibial
torsion ( I n ) .We a lso reviewed 80 children with intoeing wh
ocorrected their gait during a mean period of 5.2years (Table
1).Clinical evaluation included the determina-tion of medial (MR)
and lateral rotation (LR) ofthe hip in prone position with the knee
flexed,the thigh-foot angle (TFA), and the Q-angle.Radiographic
measurements included deter-mination by computed tomography (CT)
scan ofthe anteversion according to Weiner et al.," andthe tibial
torsion ('IT) according to Jacob e l a[.'Th e current authors
established normal antever-sion of 24"based on values from their
originala r t i ~ l e . ~ormal tibial torsion is 30".'
LR in the IFA group; in the IT T group, MRand LR are within
normal limits. The TFAis low normal in the IFA group, but lessthan
normal in the ITT group.The Q-angle is increased in the IFA andI'IT
group, although less so in the latter.The anteversion is
significantly increased inthe IFA group and normal for age in
theITT group. The TI' is less than normal inthe IFA group and
significantly decreasedin the I'IT group.In the correction group,
there is also alarge discrepancy between MR and LR; theTFA is low
normal, but the Q-angle isclearly increased. No CT measurementswere
done in this group because of radiationhazards to the children.
Clinical rotation
RESULTS TABLE 3. Comparison by Student'sTable 1documents the
characteristics of allsubjects. Only the pathologic limbs
wereconsidered fo r further analysis, as normal Probabilityvalues
have been well established in previ- IRT ERT of Similarityous
publications. The average age of thean older age for the correction
group. Male-female distribution was almost even.The distribution of
intoeing patients ac-cording to the pathology is as follows: IFA,
TT 5.3 t 7.9 21.6 t 9.9 0.00
of Tw o
groups did not vary significantly, excep t for MR 73.0 5 10.8
74.6 i7 12.1 0.79LR 22.2 +- 11.4 16.5 t 10.2 0.14Q-angle 14.9 t 5.6
16.2 5 5.3 0.006TFA -9.0 t 8.5 0.1 2 6.6 0.00
38.2 2 7.8 40.6 % 8.2 0.8170%; I n , 30%. The clinical and CT
mea-surements are listed in Table 2. mere s asignificant increase
in MR and decrease in IRT, internal rotation tibia;ERT,external
rotation tibia:MR,medialrotationof the hip; LR, ateral rotation of
the hip; TFA, thigh-footangle; AV, anteversion;n,ibial torsion.
-
8/8/2019 Normal and Abnormal Torsional Development in
Children
4/5
Number 302May, 1994 Torsional Development in Children 25
L
P 50Uc0
Q>Q
-.- 40c5 30.c00 2omc-
10
IFA
1- NormalI I0 4 8 12 16 20
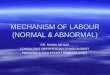
Fig. 2. Comparison of anteversion of the IFAversus normal
group.
measurements correlated very well with ra-diographic
determination^.^^'^In the correction group, 83.4% of patientswith
intoeing had IFA. A decrease in antever-sion was observed in 11
patients (20.5%),and 34 (62.9%) patients developed compen-satory
ERT. Seven pa tients with IT T and twowith metatarsus adductus
showed a correc-tion of their deformity.The IFA group w as divided
into two sub-groups, IRT and ERT. The IRT group (74limbs) walked
with internally rotated kneesand feet, the ERT group (50 limbs)
withinternally rotated knees and straight forwardor outward
pointing feet.Table 3 lists the different measurementsin the two
subgroups. Medial rotation, LR,and anteversion remain abnormal as
ex-pected, with no difference between the twogroups. There is a
significantly higher Q-angle, TFA , and TT in the ERT group.
Thedata were evaluated by Student's t-test.DISCUSSIONThe primary
cause of intoeing in midchild-hood is IFA and less frequently ITT.
heauthors' study shows a frequency of 70%and 30% respectively at an
average age ofseven years. The I l T usually corrects
spon-taneously before age seven." Figure 2shows the degrees of
anteversion of the IFA
IFA
0 3 6 9 12 15Fig. 3. Comparison of tibial torsion in IFA andI l
T groups.
group, plotted against the normal curve.Again, no significant
decrease in antever-sion appears to occur after age eight.
Thecomparison of tibial torsion in the IFA andthe ITT group is
interesting. In the lattergroup, the TT has a slight tendency to
de-crease, and in the former a definite increaseof TT ccurs with
age (Fig. 3). This is alsoreflected in the ERT subgroup (Table
3),with a very significant increase in externaltibial torsion,
causing the Q-angle to in-crease and the intoeing gait to correct.
Fiftylimbs (40.3%) in the IFA group presentedwith this deformity.
This is a somewhathigher percentage than the 30% of C ahuzace t
aL2According to Staheli et aZ.," the meanntMR is 50" in male and
40" in female pa-tients. The mean L R is 45" (range, 25'45")in both
genders. The mean TFA is 10"(range , -5"-30"). Tibia1 torsion ave
rages20" (range, 0'4 5"). All data refer to mid-childhood
(approximately seven years ofage). The tibial torsion measured by
CT av-erages 30". The Q-angle, as determined byBrattstrom,'
averages 8"to 10" in male, and10" to 20" in female patients.
According toHughston and Walsh? however, a Q-angleof more than 10"
is considered pathologic.
The mean age of the ERT group is oneyear older than the IR T
group. Ex ternal rota-tion of the tibia is present at all ages,
and
-
8/8/2019 Normal and Abnormal Torsional Development in
Children
5/5
Clinical Orthopaedics26 Fabry et al. and Related Researchdoes
not show a tendency to decrease. Ofthe children reviewed after
their intoeinggait had been corrected, in 34 (75.5% ofthe 45
children with IFA) it occurred bycompensatory ERT. A substantial
numberof children with IFA develop torsionalmalalignment syn drom e
with an increasedQ-angle and possible consequences for theknee
function. Correction of either the ante-version or the ERT does not
seem to occur.Since it is not yet clear what the conse-quences of
an uncorrected anteversion ormalalignment for the knee or hip are,
thera-peutic restraint is indicated. However, oncemalalignment has
occurred it is irreversible.When anteversion in excess of 50" with
ex-tremes of MR and LR of the hip is diag-nosed, it should be
corrected before ERToccurs (usually after eight years of age).Once
rotational malalignment of the limboccurs, correction at two levels
should onlybe considered in severe cases, or in thosepatients with
painful knees.References
Brattstrom, H.: Patella alta in non-dislocating k neejoints.
Acta Orthop. Scand. 4 1578, 1970.Cdhuzac, J . P., Hobatho, M. C.,
Baunin, C., Bou-lot, J., Darmana, R., and Autefage,
A.:Classifica-tion of 125 children with rotational
abnormalities.Part B. J. Pediatr. Orthop. 159 , 1992.Dunlap, K.,
Shands Jr., A . R., Hollister Jr., L. C.,Gaul, J. S., and Streit,
H. A,: A new method fordetermination of torsion of the femur. J.
BoneJoint Surg. 35A:289, 1953.
4. Fabry, G., MacEwen, G . D., and Shands Jr.,A. R.: Torsion of
the femur. J . Bone Joint Surg.55A:1726, 1973.5. Fairbank, J. C.,
Pynsent, P. B., Van Poortvliet,J. A., and Philips, H.: Mechanical
factors in theincidence of knee pain in adolescents and
youngadults. J. Bone Joint Surg. 66B:685, 1984.6. Hughston, J. C.,
and Walsh, W. M.: P roximal anddistal reconstruction of the
extensor mechanismfor patellar subluxation. Clin. Orthop.
144:36,1979.7. Insall, J., Falvo, K. A., and Wise, D. W.:
Chondro-malacia patellae. A prospective study. J. BoneJoint Surg. 5
8 A 1 , 1976.8. Jacob, R. P., Haertel, M., and Stussi, E.:
Tibia1torsion calculated by computerized tomographyand compared to
other methods of measurements.J. Bone Joint Surg. 62B:238, 1980.9.
Lefort, G., Cottalorda, J., Lefebvre, F., Buch-Pil-Ion, M. A., and
Daoud, S.:Les instabilites fkmoro-patellaires chez I'enfant et
I'adolescent. Rev. Chir.Orthop. 77:491, 1991.10. Staheli, L. T.:
Torsion-treatment indications. Clin.Orthop. 247:61, 1989.
1 1 . Staheli, L. T., Corbett, M., and Wyss, C.: Lower-extremity
rotational problems in children: No rmalvalues to guide management.
J. Bone Joint Surg.67A:39, 1985.12. Svenningsen, S ., Apalset, K.,
Terjesen, T., andAnda, S. : Regression of femoral anteversion.
Aprospective study of in-toeing children. Acta Or-thop. Scand.
60:170, 1989.13. Svenningsen, S., Terjesen, T., Auflem, M .,
andBerg, V.: Hip rotation and in-toeing gait. A studyof normal
subjects from four years until adult age.Clin. Orthop. 251:177,
1990.14. Turner, M. S., and Smilie, I. S.: The effect oftibia1
torsion on the pathology of the knee. J. BoneJoint Surg. 63B:396,
1981.15. Weiner, D. S., Cook, A. J. , Hoyt Jr., W. A., Ora-vec, C.
E.: Computed tomography in the measure-ment of femoral anteversion.
Orthopaedics 1 :299,1978.