Embed Size (px)
Citation preview

Proc. Nat. Acad. Sci. USAVol. 72, No. 1, pp. 152-156, January 1975
Nonrandom Chromosomal Abnormalities in Hematologic Disorders of Man(quinacrine fluorescence/trisomy 8/leukemia)
JANET D. ROWLEY
Department of Medicine, The University of Chicago, and The Franklin McLean Memorial Research Institute (operated by theUniversity of Chicago for the United States Atomic Energy Commission), Chicago, Illinois 60637
Communicated by Leon 0. Jacobson, October 16, 1974
ABSTRACT A nonrandom pattern of chromosomalabnormalities occurs in bone marrow cells obtained frompatients with hematologic disorders who have an abnormalkaryotype involving a C group chromosome. An additionalnumber 8 chromosome is the most common abnormality,found in more than one-half of the patients studied. Anadditional number 9 chromosome and the loss of all or partof a number 7 are abnormalities that occur more oftenthan might be expected by chance. It is proposed thatspecific human chromosomal abnormalities may be re-lated to different specific etiologic agents.
The presence of the Philadelphia (Ph') chromosome in bonemarrow cells from patients with chronic myelogenous leu-kemia (CML) (1) is a nonrandom change that occurs in about90% of all patients who have this disease (2). Abnormalitiesinvolving C group chromosomes (X plus nos. 6 through 12)are frequently seen in patients with various hematologic dis-orders, but these abnormalities are generally considered to behighly variable or random (3, 4). This impression is derivedfrom studies in which conventional staining procedures areused that do not permit identification of individual chromo-somes.
In the present study, individual C group chromosomes areidentified by their banding pattern with the use of quinacrinefluorescence (5). The cells that were analyzed had been ob-tained from 21 patients with various hematologic diseases.Consistent patterns of chromosomal abnormalities, seen inthese patients, were confirmed by analysis of case reportsfrom other laboratories.
MATERIALS AND METHODS
Patients Studied by Author. Twenty-one patients, who hadan abnormality of a C group chromosome that was detectedwith conventional Giemsa stain, were selected for this study.The group consisted of six patients with CML in the acutephase, 10 patients with acute leukemia (AL), three patientswith polycythemia vera (PV), and one patient each with re-fractory anemia and neutropenia.Chromosomes were prepared from bone marrow cells as
described (6). Peripheral blood cells were cultured for 24 and48 hr without phytohemagglutinin to obtain immature mye-loid cells in division and for 72 hr with phytohemagglutininto provide lymphocytes in division.
Cells in metaphase were stained with quinacrine mustardand were photographed with a Leitz photomicroscope
equipped with Ploem epi-illumination (7). The same cells,stained with Giemsa, were photographed either before orafter quinacrine fluorescence. The duplicate photographs wereused to identify the chromosomes according to the Parisnomenclature (8).
Patients Studied by Others. Accurate karyotypes determinedwith banding techniques, either quinacrine or Giemsa, wereavailable for an additional 29 patients who had some hemato-logic disorder and a C group aberration. Results for 23 of thesepatients from 13 laboratories were obtained from publishedreports (9-24); results for six patients came from personalcommunications by H. Van den Berghe, A. de la Chapelle,S. F. Pan, and C. C. Lin. These 29 patients included threewith CML in the acute phase (9, 10), one with Ph' negativeCML (11), 12 with AL (12-18), four with PV (11, 19), andnine with other disorders such as refractory anemia (with orwithout ring sideroblasts) (17, 20), neutropenia (21), andmyelofibrosis (22-24).
RESULTS
Patients Studied by Author. Gains of one or more C groupchromosomes occurred in 15 patients, whereas loss of all or
part of a C group chromosome occurred in six.The results of the analysis of the chromosomes involved in
the changes are summarized in Table 1. All six patients withCML in the acute phase had one or more extra C group chro-mosomes; every patient had at least one additional chromo-some no. 8 (ref. 7). Three of these patients had two extra Cgroup chromosomes, the second being a no. 8, a no. 10, or an
X (in a male). The 10 patients with AL showed an abnormal-ity of a C group chromosome, which consisted of a gain in sixpatients and a loss in four. An additional no. 8 chromosomewas present in five patients and an additional no. 11 (ref. 25)was present in one. Three female patients whose marrow cellshad 45 chromosomes were lacking one X and, in addition, hada translocation involving the long arm of no. 8 (8q22) and thelong arm of either no. 21 or no. 17 (26, 27). A no. 7 chromo-some was missing in one male patient whose leukemic cellsshowed a hypodiploid number.
Abnormalities in the C group were found in the three pa-tients with PV; one had an additional no. 8 and no. 9 chromo-some, one had an extra no. 9 (28), and the third had a deletionof no. 7 distal to 7q22 (29). The two other patients, one withrefractory anemia and the other with neutropenia, had an
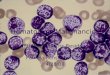
extra no. 8 chromosome (Fig. 1) and a missing no. 7 chromo-some (29), respectively.
Thus, thirteen of the 21 patients had an additional no. 8
152
Abbreviations: CMIL, chronic myelogenous leukemia; AL, acuteleukemia; PV, polycythemia vera; DMBA, 7,12-dimethylbenz-(a)anthracene.
Dow
nloa
ded
by g
uest
on
July
12,
202
0

Nonrandom Chromosomal Abnormalities 153
FIG. 1. Karyotype of a bone marrow cell obtained from a patient with refractory anemia and stained with quinacrine mustard. An
additional no. 8 chromosome is the only abnormality detected; the karyotype of this cell is 47, XY, +8.
chromosome, 3 were lacking an X, and three were lacking allor part of no. 7. An extra no. 9 chromosome was present intwo patients, one of whom also had an extra no. 8. Two pa-
tients had either an extra X or no. 10, as well as an extra no. 8,and one patient had an extra no. 11 chromosome.
Phytohemagglutinin-stimulated lymphocytes from thesepatients showed a normal karyotype. The chromosome changein the marrow cells, therefore, represents a somatic mutationsuperimposed on the individual's normal chromosomal pat-tern.
Patients Studied by Others. Of the 29 patients studied inother laboratories, 22 had gained a C chromosome, six hadlost one, and in one patient one C chromosome was gainedand another was lost. The proportion of patients with chro-mosomal gains found in the author's laboratory was not sig-nificantly different from that in other laboratories (15/21 and22/28, respectively). The combined results (Table 2) show a
very highly significant excess of patients who have gained Cchromosomes as compared with those who have lost a Cchromosome.Of the 23 patients (11, 15, 17, 19-21) who had additional
chromosomes, 14 had gained a no. 8 and one had gained a no.
8 and lost an X chromosome (15). An additional no. 9 was
observed in seven patients (18, 19, 22, 23), including twopatients with PV who also had an extra no. 8. An extra no. 10chromosome was seen in one patient (9), and an extra no. 11in another. The cells of one patient had an extra no. 12chromosome, with the later addition of a no. 7 (10). Whenchromosomal losses were present, four individuals had lost allor part of no. 7 (12-14, 24), and one had lost a no. 9 (16). Theloss of an X chromosome in two patients was associated withthe gain of a no. 8 in one of them (15).When additional chromosomes were present, no. 8 was the
one most frequently observed by others (15 of 23 patients),as well as in the author's laboratory (13 of 15). When chro-
mosomes were lost, no. 7 was the autosome most frequently af-fected. Since the results from both groups of patients weresimilar, they were combined in Table 2. The data have beenanalyzed to determine whether the specific chromosomalchanges are significantly different statistically from a randompattern. The probability that 28 of 38 chromosomal gainswould involve the same chromosome (no. 8) is <0.00001. Thepattern of gains of the other chromosomes was analyzed byelimination of those patients in whom a no. 8 alone or no. 8and another chromosome were involved; this left 10 patients.The probability that six of 10 chromosome gains, not involvingno. 8, would affect the same chromosome (no. 9) is 0.008.An analysis of the chromosomes lost reveals that the prob-ability that at least seven of 12 of these would affect the samechromosome (no. 7) is 0.002.
DISCUSSIONNonrandom changes affecting three C group chromosomeshave been identified in this study. The addition of a no. 8chromosome is the most frequent abnormality; an additionalno. 9 is seen much less commonly but still occurs significantly
TABLE 1. Author's data: number of patients showing Cgroup abnormalities
Chromosome abnormality
Disorder -7 -X +X +8 +9 +10 +11
CMIacute phase (1)* 6 (1)*AL 1 3 5 1PV it 1 1(1)*Other 1 1
Total 3 3 (1) 13 1(1) (1) 1
* ( ) In addition to no. 8.t Lacks 7q distal to 7q22 (q = long arm of a chromosome).
Proc. Nat. A cad. Sci. USA 72 (1975)
Dow
nloa
ded
by g
uest
on
July
12,
202
0

Proc. Nat. Acad. Sci. USA 72 (1975)
TABLE 2. All data: number of patients showing C group abnormalities
Chromosome abnormality
Disorder -7 -9 -X +X +7 +8 +9 +10 +11 +12 Refs.
CML-acute (1)* (1)t 7 1(1)* 1 7,9, 10, aPh' negative 1 11AL 4 1 4(1)* 10 1 2 12-18,25-27,a-cPV 1i 4 2(3)* 11,19,28,29,cOther 2§ 6 3 17,20-24,29,d
Total 711 1 4(1) (1) (1) 2811 6(3)1 1(1) 2 1
* ( ) In addition to no. 8.t ( ) In addition to no. 12.1 Lacks 7q distal to q22.§ 7p distal to 7pll is lacking in one patient (p = short arm of a chromosome).¶ Chromosome is involved in loss or gain more frequently than would be expected (P < 0.008).Refs.: personal communication from (a) Van den Berghe, H.; (b) de la Chapelle, A.; (c) Pan, S. F.; and (d) Lin, C. C.
more often than would be expected by chance. When chromo-somes are lost, no. 7 is the one most frequently affected.
There is no satisfactory explanation for the apparentlyidentical karyotypes, i.e., +8, +9, -7, found in patientswith leukemia and with nonleukemic disorders such as re-fractory anemia or neutropenia, although the latter groupshows an increased potential for leukemic transformation.The frequent occurrence in hematologic disorders of ab-normalities of chromosome 8, as an extra chromosome or in atranslocation (26, 27, 30), is perplexing. It is possible that theassociation is the result of the particular genes carried on thischromosome. The observations-that the gene for glutathionereductase may be located on chromosome 8 (31) and that apatient with refractory anemia and a +8 karyotype showedincreased amounts of this enzyme (32) provide preliminaryevidence to support this proposition. It is also possible, how-ever, that chromosome no. 8 is the site of insertion or activa-tion of a specific oncogenic virus or of other agents. The +8karyotype may represent one step or one mutation in a two-step (33) or multiple-step (34) system of carcinogenesis.
It has been stated previously (3, 4) that the association ofthe Ph' chromosome with CML was exceptional, since it ap-
RAT
LEUKEMIArFIG. 2. Rous sarcoma virus and 7, 12-dimethylbenz(a)an-
thracene (DMBA) injected intraperitoneally into rats produce sar-comas that are histologically indistinguishable. The virus-inducedsarcoma shows a specific karyotype, A (addition of one medium-sized telocentric and then one medium and one small subtelo-centric chromosome), whereas the DMIBA-induced sarcoma showsa different specific karyotype, B (trisomy for the long telocentricchromosome). DMBA administered orally produces leukemia;the chromosomal pattern of the leukemic cells (karyotype B) isidentical to that seen in the DMBA-produced sarcoma.
peared that other chromosomal changes in hematologic dis-orders were quite variable. The evidence presented here in-dicates that the variability is more apparent than real, andthat it is a reflection of the inadequate techniques previouslyavailable for chromosomal identification. It is probable thatother nonrandom patterns will be observed as cells from morepatients are analyzed with the new techniques. In fact, Vanden Berghe et al. have recently reported (35) that a deletionof chromosome no. 5 (5q-) occurred in three of their patientswith refractory anemia. It has been found that about 20% ofpatients with PV have a deletion of chromosome no. 20(20q-) (36); this same abnormality is occasionally seen inpatients with sideroblastic anemia (37). It may be possible toshow that patients with these particular chromosomal ab-normalities have some specific features, e.g., clinical or cyto-chemical, that distinguish them from the larger group of pa-tients with superficially similar disorders.
This nonrandom pattern is not restricted to diseases ofthe bone marrow. It has been known for some time that cellsin most meningiomas are lacking a chromGsome no. 22 (38).These cells tend to lose chromosomes; no. 8 is the one mostfrequently lost, no. 1 is next, and then no. 9 (39). Patientswith diseases of the lymphatic system, such as Burkitt'slymphoma, multiple myeloma, and ataxia-telangiectasia, haveabnormalities of chromosome 14 (see McCaw et al. for review*).Cells obtained from polyps of the colon have shown an extrano. 14 chromosome and, in one patient, an extra no. 8 as well(40). On the basis of these data, it appears that only certainchromosomes are found to be abnormal, and that these chro-mosomes are affected in a variety of somatic mutations, someof which are associated with malignancy.Chromosomal abnormalities have also been analyzed in ex-
perimental tumors in animals, and two important conclusionscan be drawn from this work (Fig. 2). First, both Roussarcoma virus and 7,12-dimethylbenz(a)anthracene (DMBA)produce sarcomas in the same strain of inbred rats; thesetumors are histologically indistinguishable. The majority oftumors produced by the virus have one specific chromosomalpattern (41) which is distinctly different from the specific
* McCaw, B. K., Hecht, F., Harnden, D. G. & Tcplitz, R.,Regulatory Locus for Lymphocyte Proliferation on Chromosome 14,manuscript in preparation.
154 Medical Sciences: Rowley
Dow
nloa
ded
by g
uest
on
July
12,
202
0

Nonrandom Chromosomal Abnormalities 155
MAN
KARYOTY
FIG. 3. The etiologic agents (examples labeled "X" and "Y")that produce various hematologic diseases in man are unknown.Certain nonrandom karyotypic patterns, such as an additionalchromosome no. 8 (+8) or a no. 9 (+9), have been observed inleukemia, polycythemia vera, and the anemias. It is postulatedthat one specific agent, "X", may be associated with one specifickaryotype, e.g., +8, whereas a different agent, "Y", will be as-
sociated with a different karyotype, +9.
karyotype observed in the majority of tumors produced byDMBA (42). Secondly, DMBA, if administered to the same
species of rats by a different route, produces leukemia (43).The chromosomal pattern seen in these leukemic cells isvirtually identical to that observed in the sarcomas. Thus, as
Mitelman et al. (41) have stated, the karyotypic changeis agent-specific and independent of the type of tumor pro-duced.
The situation in man is admittedly much more complexbecause of the genetic heterogeneity. Nevertheless, a similarmodel can be proposed for man (Fig. 3). Specific karyotypicpatterns, such as extra no. 8 or no. 9 chromosomes, are ob-served in histologically different disorders, such as leukemia,PV, and anemias. When the appropriate techniques for de-tecting the etiologic agents in these diseases have been de-veloped, it may be found that one agent is associated with one
specific karyotype, such as +8, and that another agent will beassociated with a different specific karyotype, even thoughboth etiologic agents are capable of producing the same spec-trum of clinical diseases (44). If this is so, then the converse
may be true, i.e., a specific chromosomal abnormality ischaracteristic of a specific etiologic agent. This concept ofagent-chromosome specificity, discussed elsewhere (44), hasreceived further support from two recent observations.Studies with somatic cell hybrids have indicated that the Tantigen gene of simian virus 40 and the genome of the virus
are located on human chromosome 7 in human cell linestransformed by simian virus 40 (45). A similar investigationsuggested that human chromosome 19 carries the structuralgene for the poliovirus receptor (46).
Investigators can learn much from the more controlled sys-tems of carcinogenesis in inbred animals or in tissue culturesin vitro, but a careful study of the chromosomal abnormalitiesfound in the tissties of patients with malignant or premalig-nant disorders may provide important clues to the funda-mental mechanisms of tumor progression in man.
I acknowledge the expert technical assistance of Judith lvikuta,Margaret Ikeda, Brooke Kountz, and David Potter, and thewholehearted support of members of the Section of Hematology.The statistical analysis of the data was performed by ShelbyHaberman. This work has been supported by the United StatesAtomic Energy Commission, the Leukemia Research Foundationof Chicago, and the Otho S. A. Sprague Memorial Institute.
1. Nowell, P. C. & Hungerford, D. A. (1960) "A minute chro-
mosome in human chronic granulocytic leukemia," Science132, 1197.
2. Whang-Peng, J., Canellos, G. P., Carbone, P. P. & Tjio, J.H. (1968) "Clinical implications of cytogenetic variants inchronic myelocytic leukemia (CML)," Blood 32, 755-766.
3. Sandberg, A. A. & Hossfeld, D. K. (1970) "Chromosomalabnormalities in human neoplasia,"' Annu. Rev. Med. 21,379-408.
4. Fitzgerald, P. H., Crossen, P. E. & Hamer, J. W. (1973)"Abnormal karyotype clones in human acute leukemias:Their nature and clinical significance," Cancer 31, 1069-1077.
5. Caspersson, T., Zech, L., Johansson, C. & Modest, E. J.(1970) "Identification of hmnan chromosomes by DNA-binding fluorescent agents," Chromosoma 30, 215-227.
6. Rowley, J. D., Blaisdell, R. K. & Jacobson, L. 0. (1966)"Chromosome studies in preleukemia. I. Aneuploidy ofgroup C chromosomes in three patients," Blood 27, 782-799.
7. Rowley, J. D. (1973) "A new consistent chromosomal ab-normality in chronic myelogenous leukemia identified byquinacrine fluorescence and Giemsa staining," Nature 243,290-293.
8. Paris Conference (1971) "Standardization in Human Cyto-genetics (1972)," in Birth Defects: Original Article Series(The National Foundation, New York) Vol. 8, no. 7.
9. Beck, W. S. & Chesney, T. McC. (1973). "Case records ofthe Massachusetts General Hospital (Case 18-1973),"N. Engl. J. Med. 288, 957-963.
10. Kaffe, S., Hsu, L. Y. F. & Hirschhorn, K; (1974) "Acquiredtrisomies 12 and 7," Lancet 2, 261-262.
11. Hsu, L. Y. F., Alter, A. & Hirschhorn, K. (1974) "Trisomy 8in bone marrow cells of patients with polyethemia vera andmyelogenous leukemia," Clin. Genet., in press.
12. Petit, P., Alexander, AIi. & Fondu, P. (1973) "M~onosomy 7in erythroleukemia," Lancet 2, 1326-1327.
13. MacDougall, L. G., Brown, J. A., Cohen, M. l\'I. & Judisch,J. M. (1974) "C-monosomy myeloproliferative syndrome:A case of 7-monosomy," J. Pediat. 84, 256-259.
14. Schmidt, R.* Darj 14. & Nitowsky, H. Mi. (1974) "Cytoge-netic studies in myeloproliferative disorders," Amer. Soc.Human Genet., Abstr. 77A.
15. Mitelman, F. & Brandt, L. (1974) "Chromosome bandingpattern in acute myeloid leukemia," Scand. J. Haemat., inpress.
16. Lampert, F., Phebus, C. K., Hiihn, D., Meyer, G. & Grei-fenegger, lvI. (1972) "Leukemic xanthomatosis with a miss-ing no. 9 chromosome," Z. Kinderheilk. 112, 251-260.
17. Jonasson, J., Gahrton, G., Lindsten, J., Simonsson-Linde-malm, C. & Zech, L. (1974) "Trisomy 8 in acute myelo-blastic leukemia and sideroachrestic anemia," Blood 43,557-563.
18. Rutten, F. J., Hustinx, T. W. J., Scheres, J. M. J. C. &Wagener, D. J. T. (1974) "Trisomy-9 in the bone marrow ofa patient with acute myelomonoblastic leukaemia," Brit. J.Haenmat. 26, 391-394.
19. Wurster-Hill, D. H., Whang-Peng, J. & McIntyre, 0. R.(1974) for the Polycythemia Vera Study Grobp, "Cytoge-netic abnormalities in polycythemia vera," Scminars i.tHematology, in press.
20. Hellstrom, K., Hagenfeldt, L., Larsson, A., Lindsten, J.,Sundelin, P. & Tiepolo, L. (1971) "An extra C chromosomeand various metabolic abnormalities in the bone marrowfrom a patient with refractory sideroblastic ahaemia,"Scand. J. Haemat. 8, 293-806.
21. de la Chapelle, A., Schroder, J. & Vupio, P. (1972) "8-Trisomy in the bone marrow. Report of two cases," Clin.Genet. 3, 470-476.
22. Davidson, W. lvi. & Knight, L. A. (1973) "Acquired trisomy9," Lancet 1, 1510.
23. Knight, L. A., Davidson, W. lv. & Cuddigan, B. J. (1974)"Acquired trisomy 9," Lancet 1, 688.
24. lvlarsh, W. L., Chaganti, R. S. K., Gardner, F. H., Mayer,K., Nowell, P. C. & German, J. (1974) "Mvapping humanautosomes: evidence supporting assignment of Rhesus to theshort arm of chromosome no. 1," Science 183, 966-968.
Proc. Nat. Acad. Sci. USA 7. (1975)
Dow
nloa
ded
by g
uest
on
July
12,
202
0

Proc. Nat. Acad. Sci. USA 72 (1975)
25. Rowley, J. D. (1974) "Abnormalities of chromosome 1 inmyeloproliferative disorders," Cancer, in press.
26. Rowley, J. D. (1973) "Identification of a translocation withquinacrine fluorescence in a patient with acute leukemia,"Ann. G&ngt. 16, 109-112.
27. Rowley, J. D. (1974) "Missing sex chromosomes and trans-locations in acute leukemia," Lancet 2, 835-836.
28. Rowley, J. D. (1973) "Acquired trisomy 9," Lancet 2, 390.29. Rowley, J. D. (1973) "Deletions of chromosome 7 in haema-
tological disorders," Lancet 2, 1385-1386.30. Sakuri, M., Oshimura, M., Kakati, S. & Sandberg, A. A.
(1974) "8-21 Tranmlocation and missing sex chromosomes inacute leukemia," Lancet 2, 227-228.
31. Kucherlapati, R. S., Nichols, E. A., Creagan, R. P., Chen,S., Borgaonkar, D. S. & Ruddle, F. H. (1974) "Assignmentof the gene for glutathione reductase to human chromosome8 by somatic cell hybridization," Amer. Soc. Human Genet.,Abstr. 51A.
32. de la Chapelle, A. (Rotterdam Conference) (1974) "Secondinternational workshop on human gene mapping," in BirthDefects: Original Article Series (The National Foundation,New York), in press.
33. Knudson, A. G. (1971) "Mutation and cancer: Statisticalstudy of retinoblastoma," Proc. Nat. Acad. Sci. USA 68,820-823..
34. Ashley, D. J. B. (1969) "The two "hit" and multiple "hit"theories of carcinogenesis," Brit. J. Cancer 23, 313-328.
35. Van den Berghe, H., Cassiman, J. J., David, G., Fryns, J. P.,Michaux, J. L. & Sokal, G. (1974) "A distinct haematologicaldisorder with deletion of the long arm of a no. 5 chromo-some," Nature, 251, 437-438.
36. Reeves, B. R., Lobb, D. S. & Lawler, S. D. (1972) "Identityof the abnormal F-group chromosome associated with poly-cythaemia vera," Humangenetik 14, 159-161.
37. de Grouchy, J., de Nava, C., Zittoun, R. & Bousser, J.(1966) "Analyses chromosomiques dans l'an6mie sidero-blastique idiopathique acquise," J. Nouv. Rev. Franc.Hematol. 6, 367-388.
38. Mark, J., Mitelman, F. & Levan, G. (1972) "On the specific-ity of the G abnormality in human meningiomas studied bythe fluorescence technique," Acta Pathol. Microbiol. Scand.A 80, 812-820.
39. Mark, J., Levan, G. & Mitelman, F. (1972> "Identificationby fluorescence of the G-chromosome lost in human menin-giomas," Hereditas 71, 163-168.
40. Mitelman, F., Mark, J., Nilsson, P. G., Dencker, H.,Norryd, C. & Tranberg, K.-G. "The chromosome bandingpattern in human colonic polyps," Hereditas, in press.
41. Mitelman, F., Mark, J., Levan, G. & Levan, A. (1972)"Tumor etiology and chromosome pattern," Science 176,1340-1341.
42. Mitelman, F. & Levan, G. (1972) "The chromosomes ofprimary 7,12-dimethylbenz(a)anthracene-induced rat sar-comas," Hereditas 71, 325-334.
43. Sugiyama, T., Kurita, Y. & Nishizuka, Y. (1967) "Chromo-some abnormality in rat leukemia induced by 7,12-dimethyl-benz(a)anthracene," Science 158, 1058-1059.
44. Rowley, J. D. (1974) "Do human tumors show a chromo-some pattern specific for each etiologic agent?" J. Nat.Cancer Inst. 52, 315-320.
45. Croce, C. M., Girardi, A. J. & Koprowski, H. (1973) "As-signment of the T-antigen gene of simian virus 40 to humanchromosome C-7," Proc. Nat. Acad. Sci. USA 70, 3617-3620.
46. Miller, D. A., Miller, 0. J., Dev, V. G., Hashmi, S., Tran-travahi, R., Medrano, L. & Green, H. (1974) "Humanchromosome 19 carries a poliovirus receptor gene," Cell 1,167-173.
156 Medical Sciences: Rowley
Dow
nloa
ded
by g
uest
on
July
12,
202
0