Embed Size (px)
Citation preview

Non-Small Cell Lung Cancer
Corey J. Langer, MD, FACP
Medical Director, Thoracic Oncology
Fox Chase Cancer Center
Philadelphia, PA

Case 2Early Stage NSCLC
• 53-year-old AA woman with 30 pack-year smoking history presents with vague DOE and cough after quitting smoking
• CXR demonstrates a 3 cm spiculated mass in the RML
• FNA shows a moderately differentiated adenocarcinoma with papillary and mucinous features
• IHC stains are positive for TTF-1
• CT and PET are otherwise entirely negative with no other sites of involvement
– The mediastinum appears normal

Case 2Early Stage NSCLC
• She undergoes RMLobectomy and mediastinal node dissection
• Final pathology confirms a 3.2 x 3.0 cm RML adenocarcinoma with microscopic involvement in 3/5 peri-bronchial nodes, 2/5 hilar nodes and 2 of 6 subcarinal nodes.
– Remaining mediastinal nodes are negative

Case 2Early Stage NSCLC
Is there a role for adjuvant therapy for this patient?
1. Yes
2. No

Case 2Early Stage NSCLC
Is there a role for adjuvant therapy for this patient?
1. Yes
2. No
Answer: Yes, adjuvant therapy would be appropriate for this patient.

Case 2Early Stage NSCLC
Which regimen has been shown in phase III studies to yield a survival advantage in this situation?
1. Cisplatin + paclitaxel
2. Cisplatin + docetaxel
3. Cisplatin + vinorelbine
4. Cisplatin + gemcitabine
5. Carboplatin + paclitaxel

Case 2Early Stage NSCLC
Which regimen has been shown in phase III studies to yield a survival advantage in this situation?
1. Cisplatin + paclitaxel
2. Cisplatin + docetaxel
3. Cisplatin + vinorelbine
4. Cisplatin + gemcitabine
5. Carboplatin + paclitaxel
Answer: Cisplatin/vinorelbine has been shown to yield a survival
advantage in phase III studies.

Le Chevalier et al. Proc Am Soc Clin Oncol. 2003;22:2. Abstract and oral presentation. Arriagada et al. N Engl J Med. 2004;350:351.
*Each center selected chemotherapy regimen†Optional, but predefined by N stage at each center
Select eligibility criteria:
• Stage I-III
• Complete surgical resection within 60 days
• Age ≤ 75
(N = 1,867)
RANDOMIZE*
Cisplatin 80 mg/m2 q 3 wk 4 ORCisplatin 100 mg/m2 q 4 wk 3-4 ORCisplatin 120 mg/m2 q 4 wk 3
PLUS
Etoposide 100 mg/m2 3 days/cycle ORVinorelbine 30 mg/m2 weekly ORVinblastine 4 mg/m2 weekly OR Vindesine 3 mg/m2 weekly
(N = 935)
Observation ± Thoracic RT ≤ 60 Gy†
(N = 932)
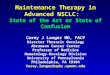
Randomized International Adjuvant Lung Cancer Trial (IALT): Design

IALT: Overall Survival
Observation ± RT
Chemotherapy
Months
164286432602774935181308450624775932
At risk:
0
20
40
60
80
100
0 12 24 36 48 60
HR = 0.86 [0.76-0.98]P < 0.03O
vera
ll S
urvi
val (
%)
Median 5-yr OS (mos) OS (%)
Chemotherapy 50.8 44.5Observation ± RT 44.4 40.4
Le Chevalier et al. Proc Am Soc Clin Oncol. 2003;22:2. Abstract and oral presentation. Arriagada et al. N Engl J Med. 2004;350:351.

IALT Trial: Results
ARM Adjuvant chemo Control
Number of enrollees 935 932
Dead from disease progression 361 405
Tx-related deaths (N) 14 2
Compliance with RT (%) 71 85
Median DFS (mos.) 39.4 34.3
2-yr DFS (%) 61 55
5-yr DFS (%) 39 34
Median Survival Time (mos.) 50.8 44.4
2-yr OS (%) 70 67
5-yr OS (%) 44.5 40.4

Additional Perspectives from IALT
• Benefit seen across most demographic variables: gender, type of surgery, use of RT, geographical location
• Decreased Benefit
– PS 2; ≥ 65; Stage I/II; T1 vs. T2,3
• Stage-Specific LTS
Adjuvant Control Abs %↑
Stage I 65.6 64.9 0.7
Stage II 46.5 43.2 3.3
Stage III 37.4 29.9 7.5

Criticisms of IALT
• Heterogenous staging, chemo and application of RT (HR favored stage III, not stage I or II)
• Study actually closed earlier than planned because of emerging interest in neoadjuvant Tx
• Bio-correlatives still pending (could there have been molecular imbalances?)
• Elderly (> 75) excluded; how do we address this expanding cohort?
• Why was this trial positive when so many similar trials proved negative?

Other Recent Negative Trials of AdjuvantCT in Completely Resected NSCLC
Study CountryCT
Regimen# of
PatientsOutcome
on OS
INT 0115
ALPI/EORTC
BLT
USA
Italy/Europe
International
VP16-P x 4
MVP x 3
V-P x 4
462
1197
481
Negative
Negative
Negative

Recently Completed Positive Randomized Adjuvant Trials in Early Stage NSCLC
Stage No. Intervention
CALGB 9633 IB 500 Carboplatin/paclitaxel
NCI-C IB-II 480 Cisplatin/vinorelbine
ANITA I-IIIA 840 Cisplatin/vinorelbine
IALT I-IIIA 1,870 Cisplatin/vincalkaloids or
Cisplatin/etoposide
2004-2006: Paradigm Shift

BR 10: NCI-Canada Trial of Adjuvant Vinorelbine and Cisplatin in Resected NSCLC
Schema
Resected stage IB and II NSCLC
Stratified by:• Nodal status• RAS mutation status
(N = 482)
Arm A q 4w 4 cycles
Cisplatin 50 mg/m2 days 1, 8
Vinorelbine 25 mg/m2 day 1, 8, 15, 21
Arm BObservation
RANDOMIZE
• Started July 1994• Completed April 2001
Winton et al. NEJM. 2005;352:2589-2597.

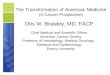
BR 10: NCI-Canada Trial of Adjuvant Vinorelbine and Cisplatin in Resected NSCLC
Survival
0 24 48 72 96
Months
0
20
40
60
80
100
Vinorelbine/cisplatin
Observation
HR = 0.7; P = 0.012
% S
urvi
val
5-year survival: 69% vs. 54%
Winton et al. NEJM. 2005;352:2589-2597.

Strauss et al. Proc Am Soc Clin Oncol. 2004;22(No 14S):621s Abstract 7019
Paclitaxel and Carboplatin Following Resection in Stage IB NSCLC
CALGB 9633
T2 N0 M0
Stage IB
NSCLC
Paclitaxel 200 mg/m2
+
Carboplatin AUC 6
q 3w x 4 cycles N = 173
ObservationN = 171
Randomized within 4-8 weeks of resection
Stratified by:• Squamous vs. adenocarcinoma
• Poorly differentiated vs. other
• Mediastinoscopy: yes or no
Complete Surgical
Resection
• Started July 1994• Completed April 2001

Paclitaxel and Carboplatin Following Resection in Stage IB NSCLC
CALGB 9633
0 20 40 60 80
0
20
40
60
80
100
Months
% S
urvi
val
Paclitaxel/carboplatin
Observation
HR = 0.62; P = 0.028
4-year survival: 71% vs. 59%
Strauss et al. Proc Am Soc Clin Oncol. 2004;22(No 14S):621s Abstract 7019

Adjuvant Navelbine International Trialist Association (ANITA Study)
Open, Multicentric (101 centers), Phase III Study(840 patients enrolled)
Douillard J-Y et al. Lancet Oncol 7:719, 2006
Surgery
Observation
Chemotherapy (Vinorelbine/CDDP)*
*Vinorelbine (30 mg/m2) q wk x 16 + Cisplatin 100 mg/m2 q 4 wks x 4

Months
Sur
viva
l Dis
trib
utio
n F
unct
ion
1.00
0.75
0.50
0.25
00 20 40 60 80 100 120
OBS. NVB + CDDP
Median (mos.) 43.8 65.8
P-value 0.013
Hazard Ratio 0.79 [0.66 - 0.95]
ObsNVB + CDDP
ANITA Trial Overall Survival (ITT Population)
Douillard J-Y et al. Lancet Oncol 7:719, 2006

ANITA Trial Results
Arm Observation Adjuvant
No 433 407
RFS (mo) 21 36
Median Surv (mos.)* 44 66
2-yr OS 63 68
5-yr OS 43 51
7-yr OS 37 48
5-yr OS by Stage
Stage I 62 63
Stage II 39 52
Stage III 26 42
* P = 0.002; HR 0.79 (0.66-0.95)
Douillard J-Y et al. Lancet Oncol 7:719, 2006

ANITA Trial Adjuvant Toxicities
Neutropenia Gr 3+4 86%
Febrile Neutropenia 12.5%
Nausea/Vomiting Gr 3+4 27%
Aesthenia 28%
Constipation 5%
Peripheral Neuropathy 3%
Drug-Related Fatality 1%
Douillard J-Y et al. Lancet Oncol 7:719, 2006

Scorecard for Adjuvant CTSubset Analyses as of 2005
Stage IA IB II IIIA
ALPI
IALT
NCI-C
CALGB
ANITA
Not tested Positive Negative

Positive Adjuvant Trials: NSCLC
Trial Stage Control Adj P-value Rel Surv
IALT I-III 40.5% 44.5% < 0.03 10%
BR10 IB-II 54% 69% 0.012 28%
CALGB IB 59% 71% 0.028 20%
ANITA I-III 43% 51% 0.013 19%

ASCO: 2006
0 2 4 6 8
Survival Time (Years)
0.0
0.2
0.4
0.6
0.8
1.0
Pro
babi
lity
ObservationChemo
0 1 2 3 4 5 6 7 8 9
HR = 0.80; 90% CI: 0.60-1.07 P = 0.10
ASCO: 2004
0 2 4 6 8
Survival Time (Years)
0.0
0.2
0.4
0.6
0.8
1.0
Pro
babi
lity
0 1 2 3 4 5 6 7 8 9
HR = 0.62; 90% CI: 0.44-0.89 P = 0.028
ObservationChemo
CALGB 9633: Overall Survival Then and Now

CALGB 9633 (ASCO 2006)
Arm CbP Obs P-value
MS 95m 78m 0.10
DFS 89m 52m 0.03
Recurred or Dead 43% 52%
5-yr DFS 52% 48% 0.21
3-yr OS* 79% 70%
5-yr OS^ 59% 57% 0.375
• Median F/U still short: < 5 yrs; • 150 deaths required for final analysis; yet only 131 have died• ^5-yr OS still significantly better for tumors ≥ 4 cm (HR = 0.62; P = 0.04)
Strauss et al. Proc Am Soc Clin Oncol. 2006; Abstract 7007.

CALGB 9633 Survival: Patients with Tumors ≥ 4.0 cm
0 2 4 6 8
Survival Time (Years)
0.0
0.2
0.4
0.6
0.8
1.0
Pro
ba
bilit
y
ObservationChemo
0 1 2 3 4 5 6 7 8 90 1 2 3 4 5 6 7 8 9
HR = 0.66; 90% CI: 0.45-0.97
P = 0.04
N = 97
N = 99

NSCLC 2006Positive Adjuvant Trials
Trial Stage Control Adj P-value Rel Surv
IALT I-III 40.5% 44.5% <0.03 10%
BR10 IB-II 54% 69% 0.012 28%
CALGB IB 57% 60% 0.10 5%
ANITA I-III 43% 51% 0.013 19%

Scorecard for Adjuvant CTSubset Analyses: Updated (ASCO 2006)
Stage IA IB II IIIA
ALPI
IALT
NCI-C
CALGB
ANITA
Not tested Positive
Negative Indeterminate

Stage-Specific Hazard RatiosRecent Adjuvant Trials
Trial IB II IIIA
IALT 0.95 0.93 0.79
BR-10 0.94 0.59 N/A
ANITA 1.10 0.71 0.69
CALGB 0.80 N/A N/A
JCOG (UFT) 0.48 N/A N/A
LACE 0.92 0.83 0.83
Negative Positive
Indeterminate Not tested

ECOG 1505: Adjuvant Bevacizumab
Investigator Choice of 3 chemo regimens^ Allows ≥ 4cm
RANDOM IZE
Chemotherapyx 4 cycles
Elibility:• Resected IB^ -IIIA• Lobectomy• No prior chemo• No planned XRT• No h/o CVA/TIA• No ATE w/in 1-yr
Stratified:• Stage• Histology• Gender• Chemotherapy
regimen
Chemotherapyx 4 cycles
+Bevacizumab
x 1-year

Chemotherapy Regimens
• Therapy to start 6-12 weeks post-operatively– Investigator Choice of Chemo x 4 cycles (12 wks)
• Carboplatin/Paclitaxel– Carboplatin AUC 6, Paclitaxel 200 mg/m2 both d 1 q21 d
• Cisplatin/Vinorelbine– Cisplatin 75 mg/m2 d 1, Vinorelbine 25 mg/m2 d1,8 q21 d
• Cisplatin/Docetaxel– Cisplatin 75 mg/m2 d 1, Docetaxel 75 mg/m2 d 1 q21 d
• Cisplatin/Gemcitabine– Cisplatin 75 mg/m2 d 1, Gemcitabine 1,250 mg/m2 d1,8 q 21 d
• Bevacizumab 15 mg/kg q 21 days x 12 months

Chemotherapy Regimens
• Therapy to start 6-12 weeks post-operatively– Investigator Choice of Chemo x 4 cycles (12 wks)
• Carboplatin/Paclitaxel– Carboplatin AUC 6, Paclitaxel 200 mg/m2 both d 1 q21 d
• Cisplatin/Vinorelbine– Cisplatin 75 mg/m2 d 1, Vinorelbine 25 mg/m2 d1,8 q21 d
• Cisplatin/Docetaxel– Cisplatin 75 mg/m2 d 1, Docetaxel 75 mg/m2 d 1 q21 d
• Cisplatin/Gemcitabine– Cisplatin 75 mg/m2 d 1, Gemcitabine 1,250 mg/m2 d1,8 q 21 d
• Bevacizumab 15 mg/kg q 21 days x 12 months

Case 2Early Stage NSCLC
Which marker has been shown to be predictive of benefit in this situation?
1. EGFR
2. RAS
3. TTF-1
4. ERCC-1
5. HER-2

Case 2Early Stage NSCLC
Which marker has been shown to be predictive of benefit in this situation?
1. EGFR
2. RAS
3. TTF-1
4. ERCC-1
5. HER-2
Answer: ERCC-1 has been shown to be predictive of benefit.

Immunohistochemical Staining of the Excision Repair Cross-Complementing 1 (ERCC-1) Protein as Predictor for Benefit of Adjuvant
Chemotherapy (CT) in the International Lung Cancer Trial (IALT)
Soria et al., ASCO 2006 Abstract 7010

IALT Trial
• 761 pts. (28 centers,14 countries) evaluable for ERCC-1 expression
• ERCC-1 repairs cisplatin-DNA adducts, so expression indicates platinum resistance
• ERCC-1 a “double-edged sword”; worse prognosis of NSCLC if low expression, but more responsive to platinum

ERCC-1-Negative TumorsOverall Survival
224 194 161 121 81 47202 163 120 91 59 35
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5YearsNo at risk
Chemotherapy
Control
Control
Chemotherapy
Ove
rall
Sur
viva
l
Adjusted HR = 0.65, 95% PI [0.50-0.86] P = 0.002
Soria et al. Proc Am Soc Clin Oncol. 2006; Abstract 7010.

ERCC-1-Positive TumorsOverall Survival
346285121147165336996127149170
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5Years
No at risk
Chemotherapy
Control
Ove
rall
Sur
viva
l
Control
Chemotherapy
Adjusted HR = 1.14, 95% CI [0.84-1.55]P = 0.40
Soria et al. Proc Am Soc Clin Oncol. 2006; Abstract 7010.

Results of ERCC-1 Analysis5-Year Survival
• Overall positivity = 44% (H-score > 1.0)
• Significant correlation of ERCC-1 expression seen with age (lower in younger pts.), histological subtype (lower in adenocarcinoma), and pleural invasion (lower if no pleural invasion)
Chemo
(N = 389)
Control
(N = 372)
HR
P-value
ERCC-1 negative
(N = 426)47%
56 mos.
39%
42 mos.
0.65
.002
ERCC-1 positive
(N = 335)
40%
50 mos.
46%
55 mos.
1.14
.40
Predictive Adjusted Analysis (5-year survival)
Soria et al. Proc Am Soc Clin Oncol. 2006; Abstract 7010.

Case 2Early Stage NSCLC
Is there a role for adjuvant XRT in patients with N2 involvement?
1. Yes
2. No
3. Controversial

Case 2Early Stage NSCLC
Is there a role for adjuvant XRT in patients with N2 involvement?
1. Yes
2. No
3. Controversial
Answer: The use of adjuvant XRT in patients with N2 involvement is
controversial.

Adjuvant Radiotherapy
Local recurrence went from 41% to 3% with RTx
Weisenburger et al, NEJM 1986.
LCSG 773
T2N1, T3, chest wall, N2completely resected (R0)
squamous cell carcinoma only
ObservationN = 108
Adjuvant RTx 50 Gy/6 wks
N = 102

Adjuvant Radiotherapy
N2 appeared to gain 1 month in survival...
Stephens et al, Br J Cancer 1996.
MRC Lung Cancer Working Party
T1-2 N1-2 NSCLCcompletely resected (R0)
N = 306
ObservationAdjuvant RTx
40 Gy/15 fractions

Adjuvant RadiotherapyMeta-Analysis 1998
• Individual data from 9 randomized trials including 2,128 patients
• Treatment details (staging, surgery, RT) highly variable among series
• PORT: better local control: 29% fewer local recurrences - 195 LR vs. 276 LR for no RT
• Overall HR = 1.21 (1.08-1.34) ~ survival decrement of 7% at two years (55% vs. 48%)
• Increase risk greater for early stage patients (Stage I/II vs. III)
Lancet 25 July 1998.

PORT Meta-AnalysisSurvival Curves
Stewart et al, Lancet 1998.

PORT Heterogeneity of Hazard
• No increased risk for patients with N2 disease
• Patients with the least to gain have the most to lose
Stewart et al, Lancet 1998.

PORT Meta-AnalysisMethodologic Flaws
• Variable and unspecified staging• Variable and unspecified interval between resection and
PORT• Inadequate RT
– Suboptimal doses– Poor treatment planning– Outmoded techniques (e.g: use of low-energy photons or 60Co
for a substantial proportion of patients)
• Inclusion of N0 patients
• Unpublished data (2 of 9 studies)• Relatively short F/U (< 4 yrs)

Risks of PORT with Modern Technology
• Retrospective review
– 202 patients treated with surgery and PORT for Stage II and III disease
– Median dose 55 Gy
– Actuarial rate of death from intercurrent disease was 13.5% compared to expected rate of 10%
Machtay et al JCO 2001.

OBS
NVB + CDDP
PORT OBS(N = 144)
NVB + CDDP(N = 88)
Median (mos.) 33.3 47.4
5-Yr survival (%) 33 44.6
5-Yr overall survival 43 51
Overall Survival in Patients Receiving PORTANITA Trial
Douillard J-Y et al. Lancet Oncol 7:719, 2006

Median Overall Survival:
65.7 mos. CT
31.2 mos. OBS
46.6 mos.
93.6 mos.
50.2 mos.
25.9 mos.
CT + PORT
CT
PORT
OBS
Duration of Survival (Months)
0 20 40 60 80 100 120
0.00
0.25
0.50
0.75
1.00
Su
rviv
al
Dis
trib
uti
on
Fu
nc
tio
nOverall Survival in N1 Patients
ANITA Trial
Douillard J-Y et al. Lancet Oncol 7:719, 2006

0.00
0.25
0.50
0.75
1.00
0 20 40 60 80 100 120
Su
rviv
al
Dis
trib
uti
on
Fu
nc
tio
n
Median Overall Survival:
32.6 mos. CT
20 mos. OBS
47.4 mos.
23.8 mos.
22.7 mos.
12.7 mos.
CT + PORT
CT
PORT
OBS
Overall Survival in N2 PatientsANITA Trial
Duration of Survival (Months)
Douillard J-Y et al. Lancet Oncol 7:719, 2006

0.00
0.25
0.50
0.75
1.00
0 20 40 60 80 100 120
Su
rviv
al
Dis
trib
uti
on
Fu
nc
tio
n
Median Overall Survival:
32.6 mos. CT
20 mos. OBS
47.4 mos.
23.8 mos.
22.7 mos.
12.7 mos.
CT + PORT
CT
PORT
OBS
Overall Survival in N2 PatientsANITA Trial
Duration of Survival (Months)
RT Effect? Or Serendipity?
Douillard J-Y et al. Lancet Oncol 7:719, 2006

ANITA5-Year Survival According to Treatment
N0 N1 N2
Observation 62.3% 31.4% 16.6%
PORT 43.8% 42.6% 21.3%
Chemotherapy 59.7% 56.3% 34.0%
Chemotherapy + PORT
44.4% 40.0% 47.4%
Douillard J-Y et al. Lancet Oncol 7:719, 2006

PORT Stage II-III SEER Data
• 7,465 pts, lobectomy or pneumonectomy (1988-2002)• > 4 mos. survival post-op• Median F/U: 3.5-years
Lally et al., JCO 2006.

Conclusions
• No role for PORT in N0 (N1?) patients
• Role of PORT in N2 patients remains controversial
• Modern RT techniques essential
• Recent randomized trials with chemo do not show increased toxicity with RT
• Randomized trials are necessary

“Lung ART”P.I. Dr. Cécile Le Pechoux
Sponsors: FNCLCC, IFCT, LARS-G, EORTC
• Completely resected N2 NSCLC
• Primary end-point: DFS
• Sample size: 700 pts
SURGERY
Conformal RT54 Gy/27-30 fxs
No post-op RT
• Pre- or post-op chemotherapy allowed• Concomitant chemo not allowed

Case 3Advanced NSCLC
• 49-year-old WM with 25 pack-year smoking history presents with 5 lb weight loss, rib pain and dyspnea
• PE shows a 2 cm (L) mid-cervical node with decreased breath sounds at the (L) base
• CXR demonstrates a (L) pleural effusion, with a mass abutting the lateral chest wall
• CT of the neck, chest and abdomen reveals a 3.8 cm spiculated mass invading the chest wall in the (L) mid-lung, a moderate (L) pleural effusion, mediastinal and (L) hilar adenopathy, and (L) mid-cervical and supraclavicular nodes. The (R) adrenal appears nodular and enlarged (~3 cm). The liver appears normal.
• Pleural tap confirms adenocarcinoma, as does FNA of the (L) mid-cervical node
• MRI of the brain is negative

Case 3Advanced NSCLC
Phase III data suggest a benefit for which of the following regimens?
1. Carboplatin + paclitaxel + bevacizumab
2. Carboplatin + paclitaxel + erlotinib
3. Cisplatin + gemcitabine + bevacizumab
4. Cisplatin + gemcitabine + erlotinib
5. 1 and 3

Case 3Advanced NSCLC
Phase III data suggest a benefit for which of the following regimens?
1. Carboplatin + paclitaxel + bevacizumab
2. Carboplatin + paclitaxel + erlotinib
3. Cisplatin + gemcitabine + bevacizumab
4. Cisplatin + gemcitabine + erlotinib
5. 1 and 3
Answer: Phase III data suggest a benefit for regimens 1 and 3.

Case 3Advanced NSCLC
• The patient receives 6-cycles of gemcitabine + carboplatin + bevacizumab
• He gains weight, with complete resolution of rib pain and dyspnea and enters a PR radiographically

Case 3Advanced NSCLC
What is indicated at this point?
1. Maintenance bevacizumab
2. Maintenance erlotinib + bevacizumab
3. Maintenance docetaxel
4. Observation (active surveillance)

Case 3Advanced NSCLC
What is indicated at this point?
1. Maintenance bevacizumab
2. Maintenance erlotinib + bevacizumab
3. Maintenance docetaxel
4. Observation (active surveillance)
Recommended Approach: At this point, maintenance bevacizumab should be considered
for this patient.

Cisplatin-Based Therapyin Advanced NSCLC
• Improves survival
– Median: 2 mos.
– 1-yr: 10% survival increase
– Hazard rate reduction of 26%
• Relieves symptoms: 66%-78% in Stage III/IV
• Improves QoL
• Cost-effective

NSCLC: Standard Agents
OLD (pre-1990) NEWER (post-1990)• Cisplatin • Paclitaxel• Etoposide • Docetaxel• Vinblastine • Gemcitabine• Ifosfamide • Vinorelbine• Mitomycin-C • Irinotecan • Carboplatin
LATEST (post-2000)• Pemetrexed• Gefitinib• Erlotinib• Bevacizumab

Metastatic NSCLC Survival Advances

Are We Making Progress in NSCLC?
• Modest, but real increase in survival
• Potential explanations
– New agents

Are We Making Progress in NSCLC?
• Modest, but real increase in survival
• Potential explanations
– New agents
– Stage migration
– Selection bias
– Second-line Tx
– Improved BSC

Current Treatment Options for NSCLCNCCN Guidelines
• Chemotherapy and targeted therapy (inoperable or unresectable, locally advanced or metastatic disease)
– First-line
• Gemcitabine plus platinum-based chemotherapy
• Taxanes (docetaxel or paclitaxel) plus platinum-based chemotherapy
• Vinorelbine, single-agent or in combination with platinum-based chemotherapy
• Addition of bevacizumab in selected pts
– Second-line
• Docetaxel (after failure of prior platinum-based chemotherapy)
• Pemetrexed (after prior chemotherapy)
• Erlotinib (approved 11/04)
– Third-line
• Erlotinib or gefitinib* (after failure of both platinum-based and docetaxel chemotherapies)
*now only approved for those who have already demonstrated a benefit to gefitinib
Pfister et al. J Clin Oncol. 2004;22:330.Ginsberg et al. Non–small cell lung cancer. In: Cancer: Principles & Practice of Oncology. 2001:925.

2003 ASCO Guidelines for Stage IV NSCLC
• 2-drug combination regimen recommended as first-line chemotherapy
– Non-platinum-based chemotherapy potential alternative in first-line therapy
– Consider single-agent therapy for elderly or patients with PS 2
• 3 agents: no advantage over 2
• 4 to 6 cycles of chemo for non-progressors
• No proven role for maintenance or consolidation with cytotoxics

ECOG 1594Treatment Schema
Schiller JH et al. N Engl J Med. 2002;346:92-98.
Arm A* q 3 wkStage IIIB or IV
NSCLC Stratified by:• Extent of disease • PS• Weight loss• Brain metastases
(N = 1,207)
Cisplatin: 100 mg/m2, day 1Gemcitabine: 1,000 mg/m2, days 1,8,15 (N = 301)
Docetaxel: 75 mg/m2, day 1Cisplatin: 75 mg/m2, day 1 (N = 304)
Arm C q 3 wk
Paclitaxel: 225 mg/m2, day 1Carboplatin: AUC=6, day 1 (N = 299)
Arm D q 3 wk
Arm B q 4 wk
Paclitaxel: 135 mg/m2, day 1Cisplatin: 75 mg/m2, day 2 (N = 303)
RANDOM
I
ZE
*Control arm

ECOG 1594Survival
NS = not significant.
% S
urvi
val
Months
Cisplatin + paclitaxel 7.8; P = NSCisplatin + gemcitabine 8.1; P = NSCisplatin + docetaxel 7.4; P = NSCarboplatin + paclitaxel 8.1; P = NS
Median survival (mo)100
80
60
40
20
0
0 5 10 15 20 25 30
Schiller JH et al. N Engl J Med. 2002;346:92-98.

ORR = overall response rate; TTP = time to tumor progression.
ECOG 1594Efficacy
Paclitaxel-Cisplatin(N = 288)
Gemcitabine-Cisplatin(N = 288)
Docetaxel-Cisplatin(N = 289)
Paclitaxel-Carboplatin
(N = 290)
ORR (%) 21 22 17 16
TTP (mos.) 3.4 4.2 3.7 3.1
Median survival (mos.)
7.8 8.1 7.4 8.1
1-year survival (%) 31 36 31 34
2-year survival (%) 10 13 11 11
Schiller JH et al. N Engl J Med. 2002;346:92-98.

E4599: Phase III Trial of Bevacizumab/Paclitaxel/Carboplatin
in First-Line Advanced NSCLC
Stratified by
• Disease stage
• Degree of weight loss
• Prior radiotherapy
• Measurable disease
Bevacizumab 15 mg/kg q 3wk until
progression of disease or
unacceptable toxicity
First-line treatment of
patients with stage IIIB with malignant
pleural effusion,or IV, or recurrent
NSCLC(N = 878)
Bevacizumab (BV)15 mg/kg q 3wk
+ PC × 6 (BV/PC)
Paclitaxel 200 mg/m2
carboplatin AUC 6 (PC) q 3wk × 6
(no crossover permitted)
Progression of disease or
unacceptable toxicity
End points• Primary
– Overall survival
• Secondary
– Response rates
– Progression-free survival
– Toxicity
Avastin® (bevacizumab) prescribing information. South San Francisco, Calif: Genentech; 2006.

E4599: Patient Characteristics
Patients, %
(N = 878)
Stage IIIB disease 12
Previous weight loss ≥ 5% 28
Age ≥ 65 years 43
Male sex 55
Sandler et al. NEJM 2006.

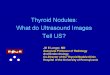
E4599: Overall Survival
HR = 0.80; P = .013
BV/PC 51.0% 22.0% 12.3 mos.
PC 44.4% 15.4% 10.3 mos.
0.0
0.2
0.4
0.6
0.8
1.0
Pro
port
ion
surv
ivin
g
0 6 42 4818 30
12 mos. 24 mos. Median
12 24 36
444 318 1 0104 9190 36 5
434 340 3 0127 25216 54 8
PC
BV/PC
MonthsPatients at risk
Median 12.3 mos.
Median 10.3 mos.
Sandler et al. NEJM 2006.

E4599: Investigator Assessed* Progression-Free Survival
Genentech, data on file.
HR: 0.65, P < .0001
BV/PC 56.0% 21.0% 6.4 mos.
PC 39.0% 9.0% 4.8 mos.
0.0
0.2
0.4
0.6
0.8
1.0
Pro
port
ion
with
PF
S
0 6 42 4818 30
6 mos. 12 mos. Median
12 24 36
444 126 0 013 127 2 0
434 201 0 021 370 6 1
PC
BV/PC
MonthsPatients at risk
Median 6.4 mos.
Median 4.8 mos.
*Based on investigator assessment which was not independently verified.

E4599: Outcome*
Arm CbP CbPB
RR (%) 15 35
PFS (mos.) 4.8 6.4
MS (mos.) 10.2 12.5
1-yr OS (%) 43.7 51.9
2-yr OS (%) 16.9 22.1
* All Differences were statistically significant P < 0.05
Sandler et al. NEJM 2006.

Randomized Trials with CT ± Targeted Therapies in Treatment-Naïve NSCLC
TRIAL TARGET CT GROUP COMMENT
ZD1839 EGFR GC AstraZeneca Closed, no benefit
ZD1839 EGFR PC AstraZeneca Closed, no benefit
OSI 774 EGFR PC Genentech/OSI Closed, no benefit
OSI 774 EGFR GC Genentech/OSI Closed, no benefit
AG3340 MMP PC Agouron Closed, no benefit
AG3340 MMP GC Agouron Closed, no benefit
BMS275291 MMP PC BMSO Closed, no benefit
Lonafarnib FT (ras) PC Schering Closed, no benefit
ISIS 3521 PKC PC ISIS Closed, no benefit
Targretin RXR PC Ligand Closed, no benefit
E4599 VEGF PC ECOG Closed, positive

E4599: Key Entry Criteria
• Key inclusion criteria– First-line locally advanced, metastatic, or recurrent NSCLC
– ECOG PS 0 or 1
– Measurable or non-measurable disease
• Key exclusion criteria*– Patients with predominant squamous histology
– Central nervous system metastases
– Gross hemoptysis (≥ 0.5 tsp of red blood) added with Protocol Amendment 1
– Unstable angina
– Patients receiving therapeutic anticoagulation*Patients were not excluded from study E4599 due to tumor location or unclassified histology (not otherwise specified, NOS).
Sandler et al. NEJM 2006.

Phase III Study of Bevacizumab + Cisplatin + Gemcitabine in Chemo-Naïve Patients with Advanced or Recurrent NSCLC (B017704)
PDPD
PDPD
PDPD
Bevacizumab
Bevacizumab
2
2
1
1
Placebo 7.5 + CGPlacebo 7.5 + CG
Bevacizumab15mg/kg + CGBevacizumab15mg/kg + CG
Bevacizumab7.5mg/kg + CGBevacizumab
7.5mg/kg + CG
Placebo 15 + CGPlacebo 15 + CG
• Previously untreated,• IIIb, IV or recurrent• non-squamous
NSCLC• No tumor invasion of
major blood vessels• No ≥ Gr 2 hemoptysis• No brain mets
• Previously untreated,• IIIb, IV or recurrent• non-squamous
NSCLC• No tumor invasion of
major blood vessels• No ≥ Gr 2 hemoptysis• No brain mets
RANDOMIZE
RANDOMIZE
• Primary Objective: PFS
• Statistical Analysis: median PFS 4.5 months placebo versus 6.4 months bevacizumab (corresponding to a hazard ratio of 0.7)
Manegold et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7514.

Phase III: Bevacizumab/Cisplatin/Gemcitabine PFS: Primary Analysis
Arm CGPCGBv
(7.5 mg/kg)
CGBv
(15 mg/kg)
No. Patients 347 345 351
Med. PFS (mos.) 6.1 6.7 6.5
HR -- 0.75 0.82
95% CI -- 0.62, 0.91 0.68, 0.98
P-value -- 0.0026 0.0301
Manegold et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7514.

Phase III: Bevacizumab/Cisplatin/Gemcitabine PFS: Primary Analysis (ITT)
No. at risk
Placebo + CG 347 228 122 36 12 3 0
Bv 7.5 + CG 345 251 150 52 18 3 0
Bv 15 + CG 351 238 148 46 16 5 0
1.0
Pos
sibi
lity
of P
FS
0.8
0.6
0.4
0.2
0.0
1.0
Time (months)
0.8
0.6
0.4
0.2
0.0
0 6 12 183 9 15
Bv 7.5mg/kg + CG
Placebo +CG
Bv 15mg/kg + CG
Placebo
CG
(N = 347)
Bv 7.5 mg/kg
CG
(N = 345)
Bv 15 mg/kg
CG
(N = 351)
Median PFS (mos) 6.1 6.7 6.5
HR
[95% CI]
- - - 0.75
[0.62, 0.91]
0.82
[0.68, 0.98]
P-value - - - 0.0026 0.0301
Manegold et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7514.

Phase III: Bevacizumab/Cisplatin/Gemcitabine PFS: Primary Analysis (NPT Censored*)
Arm CGPCGBv
(7.5 mg/kg)
CGBv
(15 mg/kg)
No. Patients 347 345 351
Med. PFS (mos.) 6.1 6.7 6.6
HR -- 0.68 0.74
95% CI -- 0.56 ,0.83 0.60, 0.90
P-value -- 0.0001 0.0021
*7% of pateints receive non-protocol antineoplastic therapy (NPT) prior to disease progression
Manegold et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7514.

Phase III: Bevacizumab/Cisplatin/Gemcitabine Overall Response
Arm CGPCGBv
(7.5 mg/kg)
CGBv
(15 mg/kg)
No. Patients 324 323 332
OR (%) 20 34 30
P-value -- < 0.0001 0.0017
Dur. of Resp. (mos.) 4.7 6.1 6.1
Manegold et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7514.

Phase III: Bevacizumab/Cisplatin/Gemcitabine Conclusions
• Statistically significant progression-free survival advantage for either low- or high-dose bevacizumab in combination with GC compared to GC alone
• Significant increase in response rate
• Survival data immature
• No new safety signals; no untoward toxicity
Manegold et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7514.

Erlotinib: First-Line Lung Cancer TRIBUTE
• Primary Endpoint: Survival• Secondary Endpoints: Symptomatic progression/QOL, response rate
NSCLC • IIIB/IV• PS 0/1• No prior chemotherapy
Stratification:• IIIB vs IV• Weight loss• Measurable vs. evaluable
RANDOMIZE
Carbo/Paclitaxel x 6+ Placebo
Carbo/Paclitaxel x 6+ Erlotinib
*Genentech Sponsored (US)

Erlotinib: First-Line Lung Cancer TRIBUTE
• Primary Endpoint: Survival• Secondary Endpoints: Symptomatic progression/QOL, response rate
NSCLC • IIIB/IV• PS 0/1• No prior chemotherapy
Stratification:• IIIB vs IV• Weight loss• Measurable vs. evaluable
RANDOMIZE
Carbo/Paclitaxel x 6+ Placebo
Carbo/Paclitaxel x 6+ Erlotinib
NEGATIVE
*Genentech Sponsored (US)

Erlotinib: First-Line Lung Cancer TALENT
*Roche Sponsored (EU)
• Primary Endpoint: Survival• Secondary Endpoints: Symptomatic progression/QOL, response rate
NSCLC • IIIB/IV• PS 0/1• No prior chemotherapy
Stratification:• IIIB vs IV• Weight loss• Measurable vs. evaluable
RANDOMIZE
Gemcitabine/Cisplatin x 6+ Placebo
Gemcitabine/Cisplatin x 6+ Erlotinib

Erlotinib: First-Line Lung Cancer TALENT
*Roche Sponsored (EU)
• Primary Endpoint: Survival• Secondary Endpoints: Symptomatic progression/QOL, response rate
NSCLC • IIIB/IV• PS 0/1• No prior chemotherapy
Stratification:• IIIB vs IV• Weight loss• Measurable vs. evaluable
RANDOMIZE
Gemcitabine/Cisplatin x 6+ Placebo
Gemcitabine/Cisplatin x 6+ Erlotinib
NEGATIVE

TRIBUTE & TALENT Trials
Arm CPE CP
No. Pts. 526 533
OR (%) 21.5 19.3
TTP (mos.) 5.1 4.9
MS (mos.) 10.8 10.6
Arm GPE GP
No. Pts. 586 586
TTP (mos.) 5.4 5.6
MS (mos.) 9.9 10.1
1-yr OS (%) 41 42
Gatezemeier et al. Proc Am Soc Clin Oncol. 2004; Abstract 7010.Herbst et al. Proc Am Soc Clin Oncol. 2004; Abstract 7011.

Maintenance or Consolidation Therapy
Is There a Role?

Immediate vs. Delayed Second-Line Docetaxel in Advanced NSCLC
Eligibility• NSCLC Stage IIIB/IV • Chemo-naïve• ECOG PS 0-2• CNS Mets allowed
GC Phase
Gemcitabine, 1000 mg/m2,
d1, 8 Carboplatin AUC 5, d1
q 21 days x 4
RANDOMIZE
Immediate Docetaxel
75mg/m2 d1 q 21 days until PD or
maximum of 6 cycles
Delayed Docetaxel
BSC → start therapy at PD75mg/m2 on d1 q 21 days,
until PD or maximum of 6 cycles
CR, PRSD
• Primary endpoint: – Overall survival – HR = 1.43
Fidias et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7516.

Immediate vs. Delayed DocetaxelPatient Disposition
Chemo-naϊveStage IIIB/IV
NSCLC
N = 562
GC PhaseN = 552
(388 received 4 cycles)
Off Study
N = 245
RandomizedSD, PR,
CRN = 307
ImmediateN = 153
Delayed
N = 154
ImmediateTreatedN = 142
DelayedTreatedN = 91
Treated
ORR 29%
Fidias et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7516.

Patients at Risk
I: 153 72 27 11 5D 154 28 10 4 2
Please note: the PFS curves only showed up to 24 months since very few patients left without PD/survival 24 months after randomization.
therapy Delayed Immediated
Pro
po
rtio
n S
urv
ivin
g
0.0
0.2
0.4
0.6
0.8
1.0
Progression Free Survival (months)0 3 6 9 12 15 18 21 24
Immediate vs. Delayed DocetaxelPFS: Total Randomized Population
Immediate (N = 153)
Delayed (N = 154)
LRP-Value
Median PFS (mos.) (95% CI)
6.5(4.4, 7.2)
2.8(2.6, 3.4)
< 0.0001
12-month PFS(95% CI)
20%(13, 26)
9%(5, 14)
Fidias et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7516.

Overall Survival Time (months)
Sur
viva
l Pro
babi
lity
I: 153 111 56 27 12 5 2D: 154 98 45 22 9 3 2
Immediate vs. Delayed DocetaxelOverall Survival: Total Randomized Population
Immediate (N = 153)
Delayed (N = 154)
LRP-Value
Median OS, (mos.) (95% CI)
11.9(10.0, 13.7)
9.1(8.0, 11.2)
0.071
12-mo survival (95% CI)
48.5%(39.9, 57.1)
38.3% (30.0, 46.5)
Patients at Risk
Fidias et al. Proc Am Soc Clin Oncol. 2007; Abstract LBA7516.

Immediate vs. Delayed DocetaxelConclusions
• Significant improvement in PFS
• Trend toward improved OS (underpowered)
• Thought-provoking, hypothesis-generating, but….
Not yet ready for prime time

Case 3Advanced NSCLC
• Patient receives bevacizumab alone for 10 months with excellent quality of life
• Unfortunately, 15 months after diagnosis, he develops H/A and subtle (R) arm weakness
• MRI of the brain demonstrates multiple space-occupying lesions with vasogenic edema
• CT confirms new pulmonary nodules and regrowth of the (R) adrenal lesion
• He receives WBRT with complete resolution of his neurologic symptoms
• He is offered salvage therapy

Case 3Advanced NSCLC
Which would be an inappropriate salvage therapy?
1. Docetaxel
2. Erlotinib
3. Pemetrexed
4. Double-dose pemetrexed

Case 3Advanced NSCLC
Which would be an inappropriate salvage therapy?
1. Docetaxel
2. Erlotinib
3. Pemetrexed
4. Double-dose pemetrexed
Correct answer: Double-dose pemetrexed would be inappropriate salvage
therapy.

Approved Second-Line Therapies for Advanced and Metastatic Disease
Clinical Efficacy

TAX 317B: Second-Line NSCLCSchema
Shepherd et al. J Clin Oncol. 2000;18:2095.
Stage IIIB or IV NSCLC Stratified by:
• PS• Best response
to cisplatin
N = 204
Arm ADocetaxelN = 104
Arm B q 3wControl
Best supportive careN = 100
RANDOMIZE
RANDOMIZE
Docetaxel 75 mg/m2 q 3w
N = 55
Docetaxel 100 mg/m2 q 3w
N = 49
Premed: Dexamethasone 8 mg PO bid 5 days (first dose 24 hr prior to each docetaxel infusion) for the docetaxel groups.

TAX 317B: Second-Line NSCLCSurvival
Median survival 7.5 vs. 4.6 mos.; P = 0.011-year survival 37% vs. 12%; P = 0.003
100
80
60
40
20
0
90 3 6 12 15 18 21
Months
% S
urvi
val
Docetaxel 75 mg/m2
Best supportive care
Shepherd et al. J Clin Oncol. 2000;18:2095.

TAX 320B: Second-Line NSCLCSchema
Fossella et al. J Clin Oncol. 2000;18:2354.
Stage III/IV locally advanced or metastatic NSCLC
Stratified by:• Response to previous
platinum-based therapy• PS
N = 373
Arm A q 3wDocetaxel 75 mg/m2
N = 125
Arm B q 3wDocetaxel 100 mg/m2
N = 125
Arm C q 3wControl
Vinorelbine 30 mg/m2 days 1, 8, 15 or ifosfamide 2 mg/m2 days 1-3
N = 123
RANDOMIZE

Months
% S
urvi
val
100
80
60
40
20
0
0 3 6 9 12 15 18 21
Docetaxel 100 mg/m2
Docetaxel 75 mg/m2
Vinorelbine/ifosfamide
Docetaxel 75 mg/m2 vs. vinorelbine/ifosfamide1-year survival 30% vs. 20%; P=0.05, 2 Median 5.7 vs. 5.6 mos. (NS)
Docetaxel 100 mg/m2 vs. vinorelbine/ifosfamide1-year survival 23% vs. 20%Median 5.5 vs. 5.6 mos. (NS)
Docetaxel vs. Vinorelbine or Ifosfamide
TAX 320B: Second-Line NSCLCSurvival
NS = not significant. Fossella et al. J Clin Oncol. 2000;18:2354.

Pemetrexed vs. Docetaxelfor Second-Line NSCLC
Schema
Hanna et al. J Clin Oncol. 2004;22:1589.
Stage IIIB or IV NSCLC
Stratified by:• PS• Prior platinum or paclitaxel
therapy• Number of prior therapies• Best response to chemotherapy• Time since last chemotherapy• Geographic region
N = 571
Arm A q 3w Pemetrexed 500 mg/m2 day 1
N = 283
Arm B q 3wDocetaxel 75 mg/m2 day 1
N = 288
RANDOMIZE

Pemetrexed vs. Docetaxelfor Second-Line NSCLC
Overall Survival (ITT)
ITT = intent to treatHR = hazard ratioCI = confidence intervalMST = median survival time
Sur
viva
l Dis
trib
utio
n
Months
0.00
0.25
0.50
0.75
1.00
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0 22.5
MST 8.3 mos.1-yr OS: 29.7%
HR = 0.99
95% CI of HR (0.82, 1.20)
MST 7.9 mos.1-yr OS: 29.7%
Pemetrexed (N = 283)
Docetaxel (N = 288)
Hanna et al. J Clin Oncol. 2004;22:1589.

Pemetrexed vs. Docetaxelfor Second-Line NSCLCProgression-Free Survival (ITT)
ITT = intent to treatHR = hazard ratioCI = confidence intervalMPFS = median progression-free survival
0.00
0.25
0.50
0.75
1.00
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0
Months
%
Pro
gres
sion
MPFS = 2.9 mos.
MPFS = 2.9 mos.
HR = 0.97
95% CI of HR (0.82, 1.16)
Pemetrexed (N = 283)
Docetaxel (N = 288)
Hanna et al. J Clin Oncol. 2004;22:1589.

Pemetrexed vs. Docetaxelfor Second-Line NSCLC
Response Rates
46.445.8
9.1 8.8
0
5
10
15
20
25
30
35
40
45
50
CR and PR Stable Disease
Pemetrexed (N = 264)
Docetaxel (N = 274)
Per
cent
(%
)
[CI=5.9,13.2] [CI=5.7,12.8]
Hanna et al. J Clin Oncol. 2004;22:1589.

Pemetrexed vs. Docetaxelfor Second-Line NSCLC
Hematological Toxicities
Pemetrexed Docetaxel
Grade 3/4 (% patients) (N = 265) (N = 276) P-value
Neutropenia 5.3 40.2 < .001
Febrile Neutropenia 1.9 12.7 < .001
Infect w/ Gr 3/4 Neutropenia 0 3.3 .004
Anemia 4.2 4.3 1.00
Thrombocytopenia 2 < 1 .116
Hanna et al. J Clin Oncol. 2004;22:1589.

Pemetrexed vs. Docetaxelfor Second-Line NSCLC
Hospitalizations, Transfusions & Growth Factors
Pemetrexed Docetaxel (N = 265) (N = 276) P-value
Patients with ≥ 1 hosp. 31.7% 40.6% .032due to an adverse event
Total hospitalizations 1.5% 13.4% < .001 due to febrile neutropenia
G-CSF/GM-CSF 2.6% 19.2% < .001
Erythropoietin 6.8% 10.1% .169
Red blood cell 16.6% 11.6% .085transfusions
Hanna et al. J Clin Oncol. 2004;22:1589.

Phase III Trial of Erlotinib in Advanced NSCLC (BR.21): Schema
• Primary End Point: Overall survival
• Secondary: Time to deterioration, PFS, ORR, duration of response , QOL, safety
Erlotinib 150 mg/d+ best supportive care
N = 488
Placebo+ best supportive care
N = 243
RANDOMIZE
2:1 randomization to the experimental arm.
Stage IIIB/IV locally advanced or metastatic NSCLC
• PS 0-3• ≥1 failed prior chemotherapy regimen• ≥18 years• No prior HER1/EGFR inhibitors• No prior malignancies or uncontrolled
CNS metastasesStratified by
• Center• PS (0/1 vs 2/3)• Response to prior therapy
(CR/PR:SD:PD)• Prior regimens (1 vs 2)• Prior platinum (Yes vs No)
N=731
Shepard et al. J Clin Oncol. 2004; 22(suppl)622. Abstract 7022 and oral presentation.

Phase III Trial of Erlotinib in Advanced NSCLC (BR.21): Schema
• Primary End Point: Overall survival
• Secondary: Time to deterioration, PFS, ORR, duration of response , QOL, safety
Erlotinib 150 mg/d+ best supportive care
N = 488
Placebo+ best supportive care
N = 243
RANDOMIZE
2:1 randomization to the experimental arm.
Stage IIIB/IV locally advanced or metastatic NSCLC
• PS 0-3• ≥1 failed prior chemotherapy regimen• ≥18 years• No prior HER1/EGFR inhibitors• No prior malignancies or uncontrolled*
CNS metastasesStratified by
• Center• PS (0/1 vs 2/3)• Response to prior therapy
(CR/PR:SD:PD)• Prior regimens (1 vs 2)• Prior platinum (Yes vs No)
N=731
Shepard et al. J Clin Oncol. 2004; 22(suppl)622. Abstract 7022 and oral presentation.
POSITIVE

*Adjusted for stratification factors at randomization, and HER1/EGFR status.
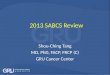
BR.21: Overall Survival
42.5% improvement in median survival
HR = 0.73; P < 0.001*
Erlotinib(N = 488)
Placebo(N = 243)
Median survival (mos.) 6.7 4.7
1-year survival (%) 31 21
Months
% S
urvi
val
Erlotinib
Placebo
100
0 5 10 15 20 25 30
80
40
20
0
60
Adapted from Shepherd et al. J Clin Oncol. 2004;22(suppl):622. Abstract 7022 and oral presentation;Data on file, Genentech, Inc.

BR.21: Survival Across Subgroups
Circle size proportional to subset size.
0 1 2 3
All patients 731
PS 0-1 486
PS 2-3 245
Male 475
Female 256
<65 y 452
65 y 279
Adenocarcinoma 365
Squamous cell carcinoma 222
Other histology 144
Prior wt loss <5% 486
Prior wt loss 5%-10% 132
Prior wt loss >10% 81
Never smoked 146
Current/ex-smoker 545
1 prior regimen 364
2 prior regimens 367
Decreasedrisk of death
Increasedrisk of death
Subset n
Data on file, Genentech, Inc.

BR.21: Survival by Gender
Adapted from Shepherd et al. J Clin Oncol. 2004;22(suppl)622. Abstract 7022 and oral presentation;Data on file, Genentech, Inc.
Female
HR = 0.80 (95% CI, 0.59-1.07)RR = 14.4%
Months
% S
urvi
val
0 5 10 15 20 25
Placebo(N = 83)
Erlotinib(N = 173)
100
80
60
40
0
20
Male
HR = 0.76 (95% CI, 0.62-0.94)RR = 6.0%
MS: 5.7 vs. 4.5 mos.
Months
% S
urvi
val
0 5 10 15 20 25
Placebo(N = 160)
Erlotinib(N = 315)
100
80
60
40
0
20

BR.21: Survival by Histology
Squamous Cell Carcinoma
0 5 10 15 20 25
HR = 0.67 (95% CI, 0.50-0.90)RR = 3.8%
MS: 5.6 vs. 3.6 mos.
1.00
Months
0.75
0.50
0.25
0
Sur
viva
l dis
trib
utio
n fu
nctio
n
Placebo(N = 78)
Erlotinib(N = 144)
HR = 0.72 (95% CI, 0.56-0.92)RR = 13.9%
MS: 7.8 vs. 5.4 mos.
Adenocarcinoma
Months
Sur
viva
l dis
trib
utio
n fu
nctio
n
0 5 10 15 20 25
Placebo(N = 119)
Erlotinib(N = 246)
0
1.00
0.75
0.50
0.25
Adapted from Shepherd et al. J Clin Oncol. 2004;22(suppl)622. Abstract 7022 and oral presentation;Data on file, Genentech, Inc.

BR.21: Survival by Smoking History
Never Smoked
HR = 0.42 (95% CI, 0.28-0.64)RR = 24.7%
Months
% S
urvi
val
0 5 10 15 20 25
100
80
60
40
0
20
Placebo(N = 42)
Erlotinib(N = 104)
Current and Ex-smokers
HR = 0.87 (95% CI, 0.71-1.05)RR = 3.9%
Months
0 5 10 15 20 25
100
80
60
40
0
20
Placebo(N = 187)
Erlotinib(N = 358)
% S
urvi
val
Adapted from Shepherd et al. J Clin Oncol. 2004;22(suppl)622. Abstract 7022 and oral presentation;Data on file, Genentech, Inc.

ASCO 2007 – NSCLC
Commentary