Embed Size (px)
DESCRIPTION
case presentation
Citation preview
Non-small cell lung cancer
Prepared by:Chan Lai Jie, A136321
Year 4,Semester 1,UKM
Non-small cell lung cancer
Definition: A group of lung cancers that are named for the kinds of cells
found in the cancer and how the cells look under a microscope. The three main types of non-small cell lung cancer are squamous cell carcinoma, large cell carcinoma, and adenocarcinoma. Non-small cell lung cancer is the most common kind of lung cancer.
Pathophysiology: Both exposure (environmental or occupational) to particular
agents and an individual’s susceptibility to these agents are thought to contribute to one’s risk of developing lung cancer. In the United States, active smoking is responsible for approximately 90% of lung cancer cases. Occupational exposures to carcinogens account for approximately 9-15% of lung cancer cases.
The types of non-small cell lung cancer are named for the kinds of cells found in the cancer and how the cells look under a microscope: Squamous cell carcinoma: Cancer that begins in squamous cells,
which are thin, flat cells that look like fish scales. This is also called epidermoid carcinoma.
Large cell carcinoma: Cancer that may begin in several types of large cells.
Adenocarcinoma: Cancer that begins in the cells that line the alveoli and make substances such as mucus.
Signs and symptoms NSCLC is often insidious, producing no symptoms until the disease is well
advanced. Early recognition of symptoms may be beneficial to outcome. At initial diagnosis, 20% of patients have localized disease, 25% of
patients have regional metastasis, and 55% of patients have distant spread of disease. Symptoms depend on the location of cancer (Spiro SG et al. 2007)
The most common signs and symptoms of lung cancer include the following: Cough Chest pain Shortness of breath Coughing up blood Wheezing Hoarseness Recurring infections such as bronchitis and pneumonia Weight loss and loss of appetite Fatigue

Metastatic signs and symptoms may include the following: Bone pain Spinal cord impingement Neurologic problems such as headache, weakness or
numbness of limbs, dizziness, and seizures
Diagnosis Testing After physical examination and CBC, chest x-ray is often the
first test performed. Chest radiographs may show the following:
Pulmonary nodule, mass, or infiltrate Mediastinal widening Atelectasis Hilar enlargement Pleural effusion
There are several methods of confirming diagnosis, with the choice determined partly by lesion location. These methods include the following:
Bronchoscopy Sputum cytology Mediastinoscopy Thoracentesis Thoracoscopy Transthoracic needle biopsy (CT- or fluoroscopy-guided)
Staging A chest CT scan is the standard for staging lung cancer. The
TNM (tumor-node-metastasis) staging system from the American Joint Committee for Cancer Staging and End Results Reporting is used for all lung carcinomas except small-cell lung cancer. The TNM takes into account the following key pieces of information:
T describes the size of the primary tumor N describes the spread of cancer to regional lymph nodes M indicates whether the cancer has metastasized

Medical Management
- Surgery : Lobectomy – removing a section of the lungPneumonectomy – removing the entire lungWedge resection – removing part of a lobe
- Chemotherapy
- Radiation
Physiotherapy Managementa) Gravity-assisted drainageb) Chest wall vibrationsc) Manual lung hyperinflation
(King D, Morrell A 1992)(a) to (c): assist in the reexpansion of atelectatic lung (Stiller K et al., 1996) Provide short-term improvement in total lung-thorax compliance
(Jones AY, Hutchinson RC, Oh TE, 1992) and expiratory flow rate (MacLean D et al., 1989)
Positioning to optimize gas exchange and subsequently increase lung volume Moderate unilateral effusion: side ly. with affected lung uppermost
because greater perfusion and ventilation in the lower lung. V/Q is usually mismatched if the affected lung is dependant.
(Gillespie and Rehder, 1987) However, if patients present with large effusion, side ly. with the
unaffected lung uppermost showed to increased PaO2 d/t decreased compression. (Chang et al. 1989)
Deep breathing exercise / Thoracic expansion exercise lungs cannot be expanded under pressure of fluid. Is performed after the effusion has been drained.
(Dechman, 1993) Benefits:
Increases lung volume (Jones et al., 1997) Increases ventilation and decreases airway resistance (Menkes and
Britt, 1980) Increases diffusion (Prabhu et al., 1994) Increases oxygen saturation (Ruggier et al., 1994; Dallimore et al.,
1998) With slow breathing, improves basal ventilation (Reid and Loveridge,
1983)
Can be performed together sustained maximal hold (SMI) for 3 sec To ensure transpulmonary pressure are sufficiently generated and
maintain for an appropriate length of time to expand the atelectatic alveoli.
(Bakow, 1977)
CASE STUDYSubjective Name : Mrs C RN : 141P09001353 Age : 56 Gender : Female Date of Admitted: 22/9/2014 Date of Assessment: 30/9/2014 Dr. Diagnosis: Non-small cell lung cancer
stage IV metastatic to brain
Dr Mx: Conservative Refer chest physio
Present problem: Pt c/o SOB during exertion and bilateral leg weakness
Current Hx: 22/09/14 – admitted d/t breathlessness 23/9/14 – sudden cardiac arrest in ward , resuscitated &
intubated with SIMV mode 24/09/14 – extubated and put on biPAP 25/09/14 – patient not tolerable , intubated with SIMV mode
Past Hx: History of admission to PHKL since 2011. Dec of 2011
- admitted d/t unproductive cough for 3/12 and SOB on exertion for 1/12 - Dr’s management : pleural biopsy, bronchoscopy & insertion of Lt. chest tube- Final Diagnosis : metastatic adenocarcinoma lung
PMHx: Nil
Past Surgical Hx: Nil
Medication: Potassium chloride in IVD 1pieNACL 12hourly Xanax 0.5mg Paracetamol 500mg 8hourly Dexamethasone 1mg daily
Investigation: CXR done on 29/9/2014, AP view
Interpretation: Consolidation in Lt. upper lobe has increased Dense consolidation with loss of volume seen in Lt. lower lobe Opacities in the Rt. Lung appears more
ABG analysis on 29/09/2014pH : 7.471PCO2: 41.5 mmHgPO2 : 181.2 mmHgHCO3 : 29.6 mmol/L
Interpretation: Acute Metabolc alkalosis
Family Hx: Father died at 89 (past hx of pulmonary tuberculosis)
Social Hx:- Married with 3 children - non-smoker - no alcohol consumption- no allergies
Home environment: Stay together with husband and daughter
Occupation: Housewife
Hobby: No specific hobby
Changes in daily activities 3 months ago, sudden onset of lower limbs weakness but still able
to walking independently and cooking.
Premorbid Status: Able to ambulate independently at home.
Patient’s Goal: Hope not to get breathlessness easily in daily life
Objective Assessment General Observation:
Pt is a moderate-sized, middle-aged Chinese lady, ly. on the bed with prop up at about 30 ̊.
Pt is conscious, alert, able to follow commands.
Local Observation: Pt is on P/SIMV, FiO2=0.6 PEEP=5 Ppeak=15 Pt has CBD and ETT attached Pt has artline at Rt. cubital fossa. Pt has central venous line with Triple lumen in jugular vein Pt has non-pitting edema on Rt. hand ̊redness, ̊ cyanosis
Breathing level: Diaphragmatic Breathing pattern: Rapid & Shallow Chest deformity: Nil Cough reflex:
Present but poor
Palpation: Auscultation
Transmitted sound scattered around the lung Fine crackles over bilateral lower lobes Decreased air-entry on bibasal lower lobes
Fermitus : Yes (Rt. > Lt.)
Percussion note: Stoney dull at Lt Upper and lower lobes Resonance sound at Right lungs
Chest expansion: Manubriosternal jt : Poor Xiphisternal jt : Poor 10th rib : Poor
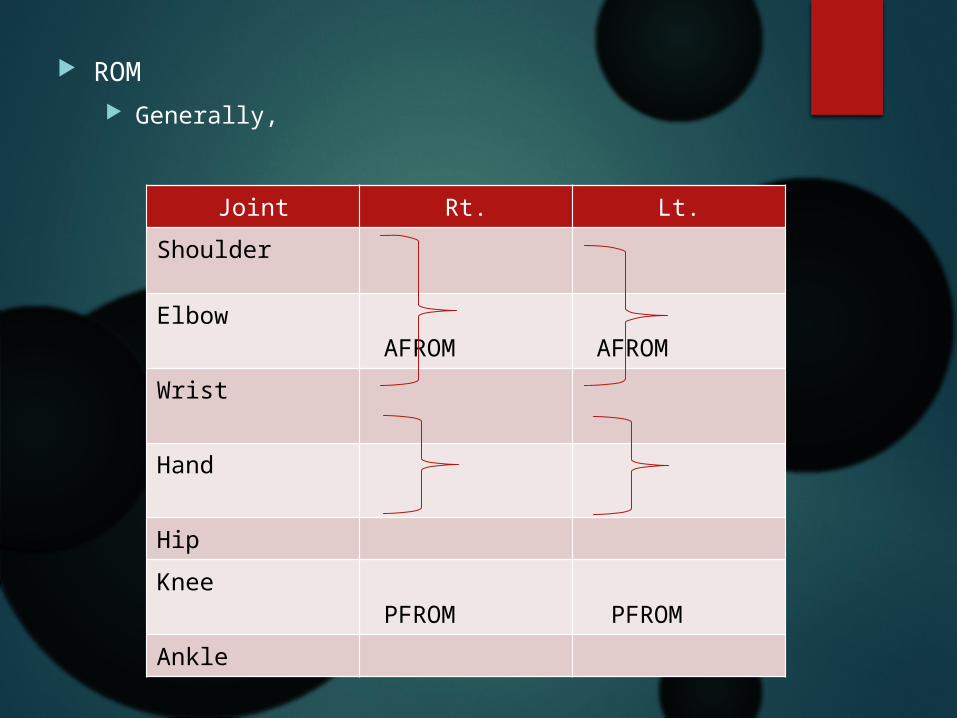
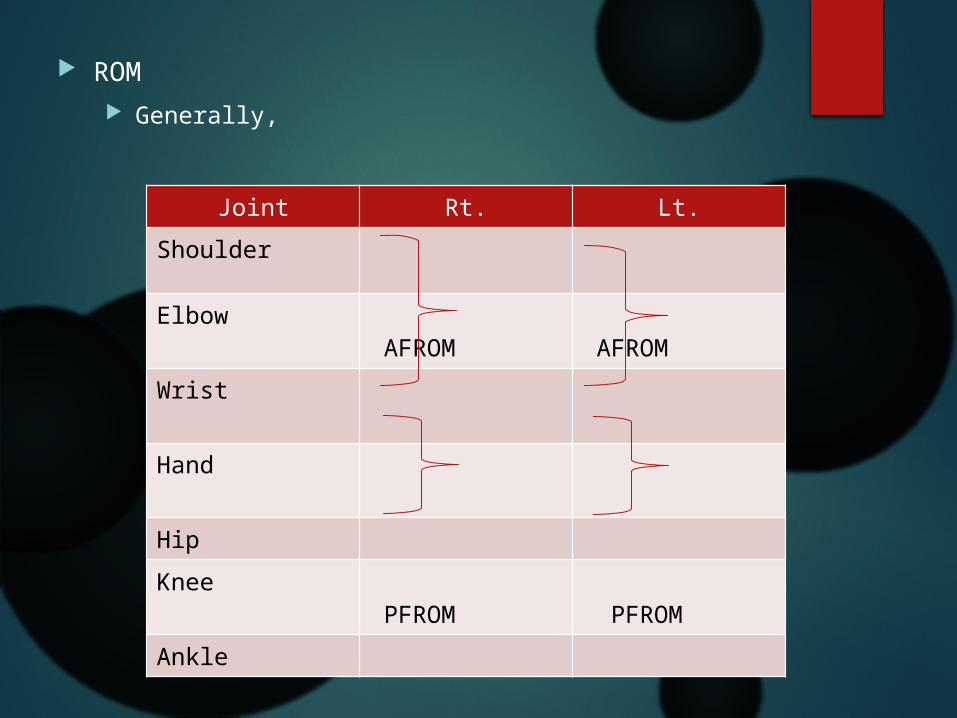
ROM Generally,
Joint Rt. Lt.Shoulder
Elbow AFROM
AFROM
Wrist Hand Hip Knee
PFROM PFROM
Ankle
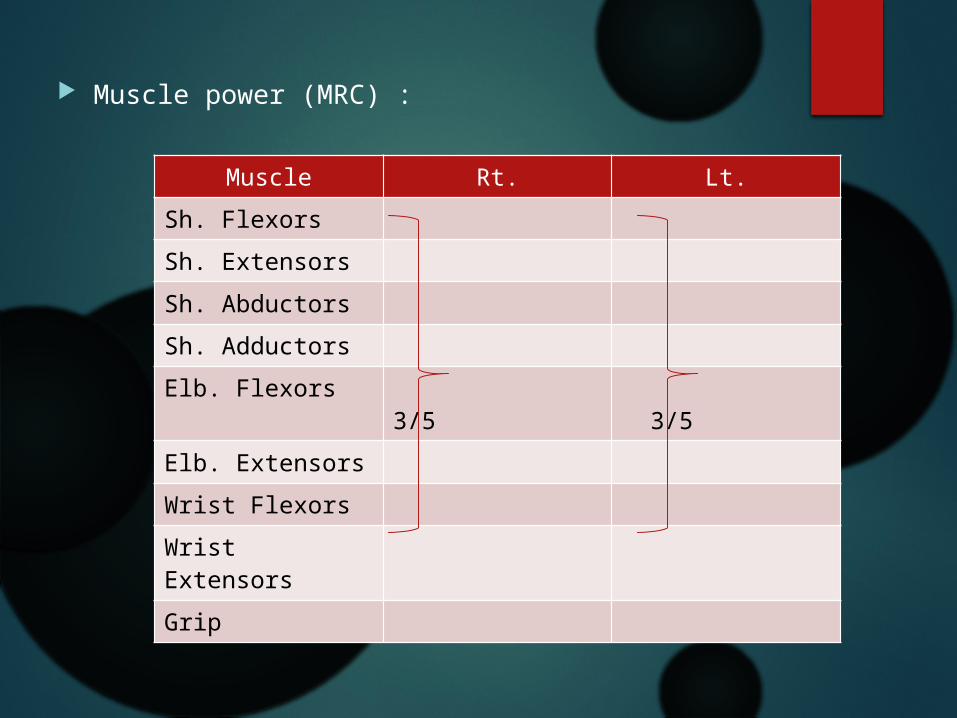
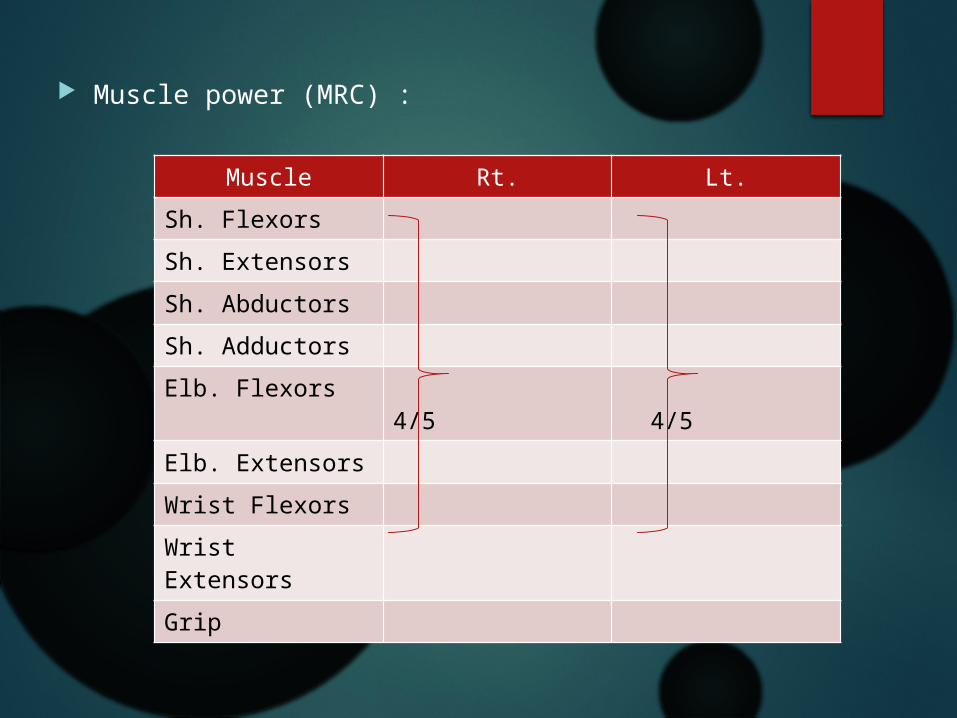
Muscle power (MRC) :
Muscle Rt. Lt.Sh. FlexorsSh. ExtensorsSh. AbductorsSh. Adductors Elb. Flexors 3/5 3/5Elb. ExtensorsWrist Flexors Wrist ExtensorsGrip
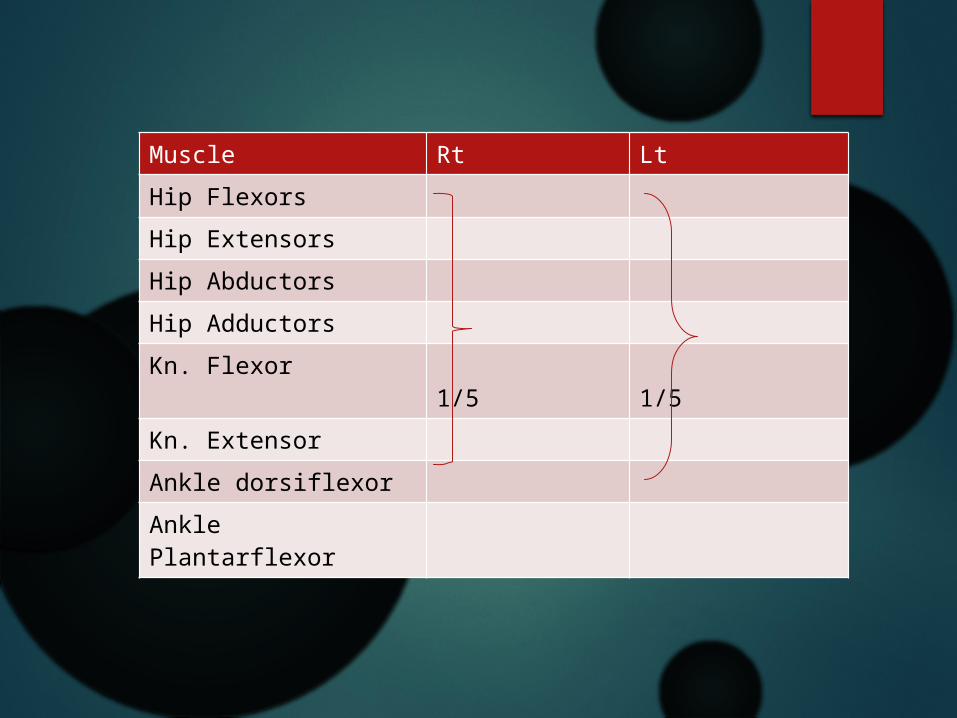
Muscle Rt LtHip FlexorsHip ExtensorsHip AbductorsHip AdductorsKn. Flexor 1/5 1/5Kn. ExtensorAnkle dorsiflexorAnkle Plantarflexor
Vital Signs: HR: 69 bpm Temp : 37.0 ̊C BP: 105/54 mmHg PR: 69 bpm RR: 20 breath/min SpO2: 100% on P/SIMVInterpretation: Pt on mild tachypnea
Bed mobility: Rolling : Pt able to do rolling by herself under supervision
Analysis
• Reduce air entry on bibasal lower lobes d/t secretion retention.
• Retention of secretion due to sedative effect and reduced cough reflex
• Decrease chest expansion d/t reduce in thoracic mobility
• Rapid & shallow breathing pattern d/t incorrect breathing technique
• Reduce muscle power d/t prolonged immobilization

Short Term Goals
Improve airway clearance within 2 days.
Improve the breathing pattern within 3 days.
Improve chest expansion within 3 days.
Improve muscle power within one week
Long Term Goals
To regain optimal cardiovascular and respiratory function within one month
To maintain airway clearance. To maintain joint range and
muscle power
Plan
Airways clearance techniques Breathing exercise Thoracic mobility exercise Active free exercise/Active-assisted exercise Ankle circulatory exercise Positioning Pt education
Intervention Half ly.; deep breathing exercise; 5 reps;
3sets Half ly.; thoracic mobility exercise: bilateral
arms elevation during inspiration and lowering during expiration; 5 reps; 3sets
Half ly.; active free exercise for both upper limbs; 5 reps
Sup. ly. with bilateral leg elevation; bilateral ankle dorsiflexion and plantarflexion; 30 reps
Lt side ly.; gentle vibration over Rt lateral and posterior basal (Jennifer A Pryor, 2003)
Rt side ly.; gentle vibration over Lt lateral and posterior basal (Jennifer A Pryor, 2003)
Supine ly.; suction done by S/N via ETT and oral
Position pt in Rt. Side ly. : prop up to 30 ̊ Patient education:
Encourage side ly. on Rt side (Gillespie and Rehder, 1987) Ask pt to do the breathing exs and ankle circulatory exs taught
hourly.
Evaluation
Pt is cooperate and able to perform all the exercises taught.
Sputum: Colour: whittish Amount: large Consistency: loose
Airflow: Airflow increase from 0.2 L to 0.3 L during perform
deep breathing exercise
Vital Signs: HR: 80 bpm BP: 146/60 mmHg PR: 72 bpm RR: 28 breath/min SpO2: 100% on P/SIMVInterpretation: Pt’s on tachypnea
Auscultation: Crackles disappears Air entry improve for bibasal lower lobes Transmitted sound remain
Review
Reassess auscultation, chest expansion, breathing level, breathing pattern
Review intervention
Follow Up(08/10/2014)
Subjective
Dr Mx: Ventilator mode change to CPAP
Present problem: Pt c/o SOB during turning by S/N
Investigation: CXR done on 08/10/2014, AP view
Analysis: Opacities in the right lung reduce Consolidation in Lt. upper lobe has reduced Volume loss in left lower lobe
Objective General Observation:
Pt is a moderate-sized, middle-aged Chinese lady, ly. on the bed with prop up at about 30 ̊.
Pt is conscious, alert, able to follow commands but look lethargic.
Local Observation: Pt is on CPAP, FiO2=0.35 PEEP=5 Ppeak=15 Pt has CBD and ETT attached Pt has artline at Rt. cubital fossa. Pt has central venous line with Triple lumen in jugular vein Pt has non-pitting edema on Rt. hand ̊redness, ̊ cyanosis
Breathing level: Diaphragmatic Breathing pattern: Rapid & Shallow Chest deformity: Nil Cough reflex:
Present but poor
Palpation: Auscultation
Transmitted sound scattered around the lung Fine crackles over bilateral lower lobes Decreased air-entry on bibasal lower lobes
Fermitus : Yes (Rt. > Lt.)
Percussion note: Stoney dull at Lt Upper and lower lobes Resonance sound at Right lungs
Chest expansion: Manubriosternal jt : Poor Xiphisternal jt : Poor 10th rib : Poor
ROM Generally,
Joint Rt. Lt.Shoulder
Elbow AFROM
AFROM
Wrist Hand Hip Knee
PFROM PFROM
Ankle
Muscle power (MRC) :
Muscle Rt. Lt.Sh. FlexorsSh. ExtensorsSh. AbductorsSh. Adductors Elb. Flexors 4/5 4/5Elb. ExtensorsWrist Flexors Wrist ExtensorsGrip
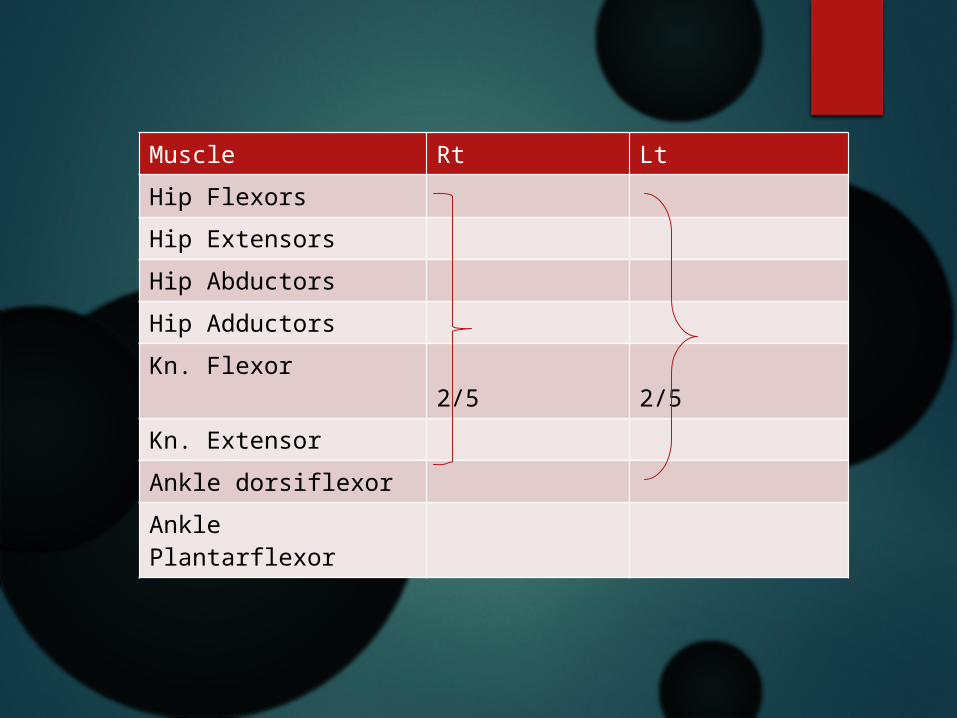
Muscle Rt LtHip FlexorsHip ExtensorsHip AbductorsHip AdductorsKn. Flexor 2/5 2/5Kn. ExtensorAnkle dorsiflexorAnkle Plantarflexor
Vital Signs: HR: 101 bpm BP: 114/91 mmHg PR: 101 bpm RR: 38 breath/min SpO2: 97% Interpretation: Pt. on tachycardia and tachypnea
Bed mobility: Rolling : Pt able to do rolling by herself under supervision
Analysis
• Reduce air entry on bibasal lower lobes d/t secretion retention.
• Retention of secretion due to sedative effect and reduced cough reflex
• Decrease chest expansion d/t reduce in thoracic mobility
• Rapid & shallow breathing pattern d/t incorrect breathing technique
• Reduce muscle power d/t prolonged immobilization
Plan
Airways clearance techniques Breathing exercise Thoracic mobility exercise Active free exercise/Active-assisted exercise Ankle circulatory exercise Positioning Pt education
Intervention Half ly.; deep breathing exercise; 5 reps;
3sets Half ly.; thoracic expansion exercise:
breath against hands on lateral chest wall; 5 reps; 3sets
Half ly.; active assisted exercise for both lower limbs; knee bending and straightening exercise; 5 reps; 3 sets
Lt side ly.; gentle vibration over Rt lateral and posterior basal (Jennifer A Pryor, 2003)
Rt side ly.; gentle vibration over Lt lateral and posterior basal (Jennifer A Pryor, 2003)
Supine ly.; suction done by S/N via ETT and oral
Position pt in Rt. Side ly. : prop up to 30 ̊ Patient education:
Encourage side ly. on Rt side (Gillespie and Rehder, 1987) Ask pt to do the breathing exs and ankle circulatory exs taught
hourly.
Evaluation Pt appears paradoxical breathing pattern
after performing breathing exercise, so let pt to rest.
Vital Signs: HR: 111 bpm BP: 169/152 mmHg PR: 111 bpm RR: 39 breath/min SpO2: 97%Interpretation: Pt. on tachycardia, tachypnea and hypertension.
Sputum: Colour: whittish Amount: large Consistency: loose
Auscultation: Crackles disappears Air entry improve for bibasal lower lobes Transmitted sound remain
Airflow: Airflow increase from 0.2 L to 0.3 L during perform deep
breathing exercise
Review
Reassess auscultation, chest expansion, breathing level, breathing pattern, coughing effort
Review intervention KIV sitting up patient after pt tolerate with CPAP
References Russell T. Attridge. Pharmacotherapy Conference November 20, 2009 Jennifer A Pryor. Physiotherapy for Respiratory and Cardiac Problems
Adults and Peadiatrics. 3rd Edition. 2004 Alexandra Hough. Physiotherapy in Respiratory Care: An evidence-based
approach to respiratory and cardiac management. 3rd Edition. 2001. Richard W. Light. Management of parapneumonic effusions.Egyptian
Journal of Bronchology. 2008. Vol 2, No 1. John G. Bartlett. Practice Guidelines for the Management of Community-
Acquired Pneumonia in Adults. Clinical Infectious Diseases 2000;31:347–82
G. Ntoumenopoulos. Chest physiotherapy for the prevention of ventilator-associated pneumonia. Intensive Care Med (2002) 28:850–856
Beatrice Tucker and Sue Jenkins. The effect of breathing exercises with body positioning on regional lung ventilation. Australian Physiotherapy.1996. Vol 42,No 3.
Bakow, E. Sustained maximal inspiration-a rationale for its. Respiratory care. 1977. Vol 22 No 4.