Embed Size (px)
Citation preview

Thyroid Disease:Nodules and Thyroid
Dysfunction 2019
James V. Hennessey MDAssociate Professor of Medicine
Harvard Medical School
COPYRIG
HT

Case 1
● 28 year old woman sees OB for routine visit● ROS:
– Negative except for occasional dysphonia● PE: BP 122/78, HR 72 BPM, 5’ 5”, 120 lbs.● Thyroid Exam: 2.5 cm smooth nodule left
– Moves easily with swallowing– 1 cm left SCM lymph node palpable
COPYRIG
HT

Thyroid Nodule Prevalence
Mazzaferi EL. NEJM. 1993;328:553-559.
•Detected by ultrasound/autopsyq Detected by palpation
• By age 30, ~20% of the population has a thyroid nodule (women>men)
• Likely hood of malignancy is higher in the extremes of age (<20 years, >70 years)
• Lifetime likelihood of a nodule is ~ 60%
COPYRIG
HT

15 X ↑
Ahn HS et al. 2014 NEJM 371(19):1765-1767
COPYRIG
HT

Thyroid Cancer• THYROID CANCER FACTS
• 53,990 cases in U.S. 2018 (Estimate)• 3 Women : 1 Man
• @ 0.005% of U.S. population
• < 4% fatal (2060 deaths in 2018 estimated)• 1.1 Women : 1 Man• @ 0.3% cancer deaths in US (27.5% are aged 75-84)
Cancer Facts and Figures 2018 American Cancer Society
COPYRIG
HT

Risk Factors for malignancy: Patient History● Surgical Dx of thyroid cancer in contralateral lobe
● Ionizing Irradiation (XRT) as child/adolescent
● Calcitonin > 100 pg/mL
● PET positive thyroid nodule
● Low dietary iodine intake
● Thyroid cancer in first degree relative
http://www.cancer.org/cancer/thyroidcancer/detailedguide/thyroid-cancer-risk-factors
COPYRIG
HT

Thyroid Nodule Laboratory Diagnosis
● TSH– Suppressed C/W thyrotoxicosis
● Malignancy unlikely– Elevated C/W hypothyroidism
RADIONUCLIDE SCANNINGIndication:
•Thyrotoxic nodule identification (TSH < normal)•99mTc (False +s), 131-I (Rads) or 123-I (Std)
Haugen BR et al. 2016 Thyroid 26(1):1-133
COPYRIG
HT

Thyroid UltrasoundIndication: normal to TSH–Defines a distinct nodule vs. abnormal parenchyma–Role to guide FNA (cystic, posterior)–MNG nodule selection–Useful in f/u of low risk patient, incidentaloma
● MRI / CT SCANNING–Offer little in pre-operative diagnosis–Contrast administration may delay Dx &/or Rx
Haugen BR et al. 2016 Thyroid 26(1):1-133
COPYRIG
HT

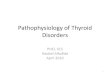
Papillary Thyroid Cancer Appearance on U/S
Tae et al. Thyroid 2007 17:461-466
58 male, 10 mm mass+ microcalcifications
39 female, 9 mm mass+ irregular margins
COPYRIG
HT

Ultrasound Pattern = Risk●High Suspicion = 70-90% Cancer Risk
●Intermediate suspicion = 10-20% Risk
●Low Suspicion = 5-10% Risk of cancer
●Very Low suspicion = <3% Risk cancer
●Benign (Purely cystic)Haugen BR et al. 2016 Thyroid 26(1):1-133
COPYRIG
HT

Who to Biopsy? R8Sonographic Risk Pattern Estimated
Malignancy Risk
Consider Biopsy
Strength of Recommendation
Quality of Evidence
High Suspicion >70-90% > 1 cm Strong Moderate
Intermediate Suspicion 10-20% > 1 cm Strong Low
Low Suspicion 5-10% > 1.5 cm Weak Low
Very Low suspicion < 3% > 2 cm Weak Moderate
Benign < 1% No Strong Low
FNA NOT recommended for nodules not meeting above criteria, including ALL nodules < 1cm
Strong Moderate
Haugen BR et al. 2016 Thyroid 26(1):1-133
COPYRIG
HT

Multiple Nodules R20
● When multiple nodules > 1 cm are present, FNA based upon US pattern– Strong Recommendation, Mod Qual evidence
● If multiple sonographically similar low or very low risk nodules are present, malignancy risk is low, reasonable to FNA largest (1.5-2.0 cm) and observe others.– Weak Recommendation, Low Qual evidence
Haugen BR et al. 2016 Thyroid 26(1):1-133
COPYRIG
HT

Malignancy Prediction: Bethesda System
● Category Malignant risk What next?● Non-Diagnostic 1-4+% Re-do (U/S)● Benign 0-3% Clinical F/U● Atypical 5-15% Re-do (U/S)● Follicular Neoplasm 15-30% Lobectomy● Suspect malignancy 60-75% Total Tx● Malignant 97-99% Total Tx In
determinate
FNA = fine needle aspiration
Cibas ES et al. Am J Clin Path.2009(132):658-65
COPYRIG
HT

Indeterminate: What Next?● Mutation Panel
– BRAF, RET, RAS, RET/PTC, PAX8/PPARγ etc. – High Positive Predictive value (60+%)– High Negative Predictive value (90+%)
● Multigene classifier: identify benign nodule– High Negative predictive value (94-95+%)
● TSH Receptor mRNA in circulation– High Positive Predictive value (96%)
COPYRIG
HT

FNA Disposition
IndeterminateInadequate
MalignantBenign
Repeat FNAUS guidance
Inadequate
Close F/USurgery?
Surgery Repeat FNACytogenetics?
FollowSurgeryT-Tx?
Surgery ?Hemi Tx
Mutation Mut. Neg. “B9”@
COPYRIG
HT

Case 2● 72-year-old man
– palpitations over 2 months– 14 lb. weight loss over 6 months– recent insomnia
PE: BP 152/84, P 112 BPM, irregular● Eyes: alert stare present● Thyroid: 3.5 cm left nodule, freely movable● Cor: Irregularly irregular rhythm, no M/G/R● Lungs: bibasilar rales, LE: 1+ edema
What additional work-up is needed?
COPYRIG
HT

Case 2: Next Steps
ECG Results: Atrial fibrillation with ventricular response of 110 BPM
Lab Results:● TSH <0.05 (0.4-4.2 mIu/mL)● FT4 2.1 (0.8-1.8 ng/dL)● TT3 345 (80-200 ng/dL)
COPYRIG
HT

Thyrotoxicosis Classification and Etiology● Classification: all may have signs & symptoms1
– Overt T-Tox: ↓ TSH, ↑ FT4, ↑ T3– Subclinical T-Tox: ↓ TSH, normal FT4 and T3
● Etiology:1. Graves’ disease (GD), autoimmune, stimulating TSH-receptor antibodies (TRAbs)2. Toxic Nodular disease, growth and autonomomy2
● Multinodular (TMNG) or Adenoma (TA) ● TAs have somatic TSH receptor activating mutations3
● Both susceptible to iodine induced T-Tox● TMNG Incidence increases with age and in Iodine deficiency4
1. Bahn RS, et al. Thyroid. 2010;21(6):593-646. 2. Berghout A, et al. Am J Med. 1990;89:602. 3. Martin FI, et al. Med J Aust. 1996;164:200-
203. 4. Laurberg P, et al. J Intern Med. 1991;229:415.
COPYRIG
HT

Thyrotoxicosis Etiology Continued
3. Painless and Subacute Thyroiditis (SAT)– Inflammation of thyroid tissue ® TH release– Painful SAT: post viral ® fever, thyroid pain1
– Painless SAT underlies 10% “hyperthyroidism”2
● Occurs postpartum3 (PPT), with lithium4, cytokines5 (Interferon alpha), and 5-10% of amiodarone6 T-Tox
– Results in changing Thyroid function abnormalities– May spontaneously resolve to euthyroidism
1. Fatourechi V, et al. JCEM. 2003;88:2100. 2. Williams I, et al. J EpidemiolCommunity Health. 1983;37:245. 3. Gerstein HC. Arch Intern Med. 1990;150:1397.
4. Miller KK, et al. Clin Endo. 2001;55:501. 5. Roti E. Am J Med. 1996;101:482. 6. Cohen-Lehman J, et al. Nat Rev Endocrinol. 2010;6:34-41.
COPYRIG
HT

Clinical Evaluation● Comprehensive H&P, VS: PR, BP, RR, BMI
– Thyroid: +/- tender, symmetry, nodularity– Gen PE: Pulmonary, Cardiac, Neurologic
● +/- Edema, eye signs, pretibial myxedema● Biochemical evaluation:
– TSH most sensitive and specific (intact pituitary)– FT4 and TT3 simultaneously with high suspicion
● Otherwise reflex FT4 and TT3 for suppressed TSH
Bahn RS, et al. Thyroid. 2010;21(6):593-646. de los Santos ET, et al. Arch Intern Med. 1989;149:526-532.
Spencer CA, et al. JCEM. 1990;70:453.
COPYRIG
HT

Determination of Etiology
● Radioactive Iodine uptake (RAIU) – Should be performed when the clinical presentation
(ophthalmopathy, PTMyx) is not diagnostic of Graves’● Exception
– Pregnancy (TSH R antibodies)– Obvious signs and symptoms of Graves’ disease
● Radioactive Iodine thyroid scan– Should be added in the presence of thyroid nodularity
Ross DS, et al. Thyroid. 2016 26(10):1343-1421.
COPYRIG
HT

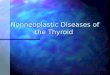
Hyperthyroidism-Differential Diagnosis
(RAIU)
Increased AbsentGraves� DiseasehCG mediated
Hot NoduleMultinodular Goiter
ThyroiditisIodine excess
Exogenous THEctopic TH
Radioactive Iodine Uptake
TSH < 0.01
Slide courtesy of A Hollenberg M. D.
COPYRIG
HT

Management of Hyperthyroidism
● Symptomatic Management:– Beta-adrenergic blockade
● For elderly, resting HR >90, coexistent CV Disease● All with symptomatic thyrotoxicosis
●Directed Interventions based on Etiology
Ross DS, et al. Thyroid. 2016 26(10):1343-1421.
COPYRIG
HT

Who Should be Treated?● Overt hyperthyroidism due to Graves’
– Treatment with any of the following● 131-I, antithyroid medication (ATD), thyroidectomy
● Overt hyperthyroidism due to TMNG/ TA– Treatment with any of the following
●131-I, thyroidectomy, ATD (occasionally)
●Subclinical hyperthyroidism?
Ross DS, et al. Thyroid. 2016 26(10):1343-1421.
COPYRIG
HT

Subclinical Thyrotoxicosis Rx?Factor TSH (<0.1 mUL) TSH (0.1 – 0.5
mU/L)Age >65 Yes Consider treating
Age <65 with comorbidities
Heart disease Yes Consider treating
Osteoporosis Yes NoMenopausal Consider treating Consider treating
Hyperthyroid symptoms Yes Consider treating
Age <65, asymptomatic Consider treating No
Ross DS, et al. Thyroid. 2016 26(10):1343-1421.
COPYRIG
HT

Anti-Thyroid Drug Recommendations● PTU not be considered 1st line ATD therapy
– Methimazole (MMI) preferred in children and adults
● PTU may be considered over MMI:– 1st Trimester of pregnancy
● Until more is known with potential MMI embryopathy● Consider switch to MMI in 2nd and 3rd to ¯ risk liver dz
– In Thyroid Storm● Advantage T4®T3 conversion inhibition
– Reaction to MMI (NOT AGRANULOCTOSIS) in whom 131-I or surgery are not possible
Ross DS, et al. Thyroid. 2016 26(10):1343-1421.
COPYRIG
HT

Case 3● 73 year old woman presents with a 3 year
history of cold intolerance, constipation, dry skin and feeling very tired.
● Her TSH values have been 4.5-5.6 mIu/ml.● ROS now includes increasing fatigue, hair loss,
and a new worry of “brain fog”.● She asks if she should be on thyroid hormone
replacement as she now has all of the hypothyroid symptoms and shares an article on bio-identical hormone replacement therapies.
COPYRIG
HT

But What is an Upper Normal TSH?
NHANES III: 4.12 mU/L (Thyroid risk free)1
NHANES III: Age adjusted (Thyroid risk free)2
Age group 97.5 centiles % > 4.5 mU/L20–29 years 3.56 mIU/liter 2.4%70-79 years 5.9 mIU/liter 9.9%>80 years 7.49 mIU/liter 12.0%
Not all elevations of TSH levels = Hypothyroidism!!!!1. Hallowell JG et al. 2002 JCEM 87:489-992. Surks et al. 2007JCEM 92: 4575–4582
COPYRIG
HT

Differential Dx: Tiredness in 1° Care● Meta-analysis of 26 studies for diagnosis● Prevalence of diagnoses:
– Anemia- 2.8% Malignancy- 0.6%– Somatic Dz- 4.3% Depression- 18.5%
● In studies with control groups (no tiredness), prevalence of somatic Dz (Diabetes, anemia, hypothyroidism) was identical to those with tiredness. Hence association may not be causal– Depression more frequent with tiredness
Stadje R et al. 2016 BMC Family Practice 17:147
COPYRIG
HT

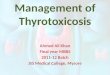
Canaris GJ, et al. Arch Intern Med. 2000;160(4):526-534.
Reported Symptoms and TSH Levels
COPYRIG
HT

Carle A et al. Am J Med 2016;129(10):1082-92
Subjects < 50 years
Subjects > 50 yearsCOPYRIG
HT

HypothyroidismOvert: Elevated TSH, low FT4
Non-specific symptomsCardiovascular manifestations
CVD risk, Hypertension, Hyperlipidemia, CHFPulmonary, Musculoskeletal, Neurologic, PsychiatricSkin/connective tissue, Renal/electrolyte abnormalitiesGastrointestinal/liver, Hematologic and HemostaticPituitary and adrenal dysfunction
Subclinical: Elevated TSH, normal FT4Little to no symptoms, milder metabolic changes
COPYRIG
HT

Hypothyroidism Etiology● Iodine deficiency (most common world wide)
● Chronic autoimmune thyroiditis (Hashimoto’s)– More frequent in women than men– Increases in frequency with age
● Iatrogenic– 131-I or surgical treatment, external beam irradiation– Drugs: thionamides, lithium, amiodarone, interferon-alfa,
interleukin-2, tyrosine kinase inhibitors (sunitinib)
● Central hypothyroidism: insufficient active TSH– Tumors: pituitary, hypothalamus Drugs: Rexanoids (Bexarotene)– Infiltrative, inflammatory, surgical, irradiation
Andersson M, et al. Pub Health Nutr. 2007;10:1606. Vanderpump MP, et al. Clin Endocrinol (Oxf). 1995;43:55-68.Hollowell JG, et al. JCEM. 2002;87(2):489-499. Huber G, et al. JCEM. 2002;87:3221.
COPYRIG
HT

Who to Treat● TSH > 10 mIu/ml considered for Rx
– Due to risk of CHF and CV mortality
● TSH > upper “normal” & < 10 mIu/ml– Treatment based on individual factors
● Positive TPO antibodies● ASCVD, CHF or risk of same● Symptoms c/w hypothyroidism ????
Garber JR, et al. Thyroid. 2012;22:1200-1235.
COPYRIG
HT

Who to Treat● TSH > 10 mIu/ml considered for Rx
– Due to risk of CHF and CV mortality
● TSH > upper “normal” & < 10 mIu/ml– Treatment based on individual factors
● Positive TPO antibodies● ASCVD, CHF or risk of same● Symptoms c/w hypothyroidism ???
● Thyroid hormones should NOT be used to treat “hypothyroid symptoms” without biochemical confirmation of hypothyroidism
Garber JR, et al. Thyroid. 2012;22:1200-1235.
COPYRIG
HT

Subclinical Hypothyroidism: Systematic Review and Meta-analysis
§ 21 RCTs comparing thyroid hormone therapy with placebo or no therapy in nonpregnant adults with SCHypothyroidism.
§ 2192 adults randomized, followed 3-18 mos., TSH lowered to 0.5-3.7 mIu/L with LT4 and essentially unchanged (4.6-14.7) without.
§ Assessment of general quality of life (QOL) and thyroid related symptoms (TRS).
Feller M et al. JAMA 2018;320(13):1349-1359
COPYRIG
HT

Results: Benefit (95% CI)
Feller M et al. JAMA 2018;320(13):1349-1359
QOL
TRS
COPYRIG
HT

Bekkering et al. 2019 BMJ doi:10.1136/bmj.l2006
COPYRIG
HT

● 1. Dx of TSH in nonpregnant adult● 2. Confirmation of persistent SCHypo
– TSH 4.5-14.9 mU/L: Repeat with FT4, 1-3 mo.– TSH > 15 mU/L: Repeat with FT4, 1-2 weeks
● 3. Indications for treatment
Biondi B et al. JAMA 2019 322(2):153-60
Subclinical Hypothyroidism
COPYRIG
HT

COPYRIG
HT

1. Dx of TSH in nonpregnant adult2. Confirmation of persistent SCHypo
• TSH 4.5-14.9 mU/L: Repeat with FT4, 1-3 mo.– TSH > 15 mU/L: Repeat with FT4, 1-2 weeks
3. Indications for treatment4. Treatment follow up
– If Rx initiated, F/U TSH in 6 weeks– Once TSH at target, F/U TSH Q year
Biondi B et al. JAMA 2019 322(2):153-60
Subclinical Hypothyroidism
COPYRIG
HT

What Should We Treat With?
● Hypothyroidism should be treated with L-thyroxine monotherapy
Garber JR, et al. Thyroid. 2012;22:1200-1235.
COPYRIG
HT

What Should We Treat With: 2● The evidence does NOT support using L-
thyroxine and L-triiodothyronine (T4/T3) combinations to treat hypothyroidism
● However, a Randomized Double Blind X-over trial of TH extract vs. LT4 at euthyroid doses2
● NS difference in Symptoms or Neurocognitive function● TH extract was preferred by 48.6% of participants2
Garber JR, et al. Thyroid. 2012;22:1200-1235Jonklass J et al. 2018 Thyroid 28(11):1416-14242-Hoang TD et al. 2013 JCEM 98(5):1982-90.
COPYRIG
HT

Therapy Targets for LT4 Replacement
●Replacement Doses: – 1.6-1.7 mcg/kg/day (0.8 mcg/lb.)– Lower start doses:
● Elderly, symptomatic CAD (12.5-15 mcg/d)
– Initial full replacement for :● Younger and without cardiac symptoms.
● Best outcomes when taken fasting, with water only, 30-60 minutes before breakfast– Alternative, at bedtime 4 hours after last meal
Garber JR, et al. Thyroid. 2012;22:1200-1235.
COPYRIG
HT

Follow up of LT4 RxTitrate TSH into the “normal range”
-- Walsh JP et al. 2006 JCE&M 91(7):2624-30-- Samuels MH et al. 2018 JCEM 103(5):1997-08
●Pregnancy Goal ● 1st Trimester < 2.5 mIU/L● 2nd Trimester < 3.0 mIU/L● 3rd Trimester < 3.5 mIU/L
– Frequency of pregnancy sampling Q 4 weeks 1st ½● > X 1 @ 26-32 wks
Garber JR, et al. Thyroid. 2012;22:1200-1235.
COPYRIG
HT

Questions?COPYRIG
HT