Embed Size (px)
Citation preview

Composite Indicator of Potentially
Avoidable Hospitalizations
Yana Gurevich, MD, MPH Canadian Institute for Health Information Presentation to HCQI experts meeting November 14, 2014
1

Project Background
2

Project background • Multiple HCQI indicators measuring potentially
avoidable hospitalizations:
– Asthma
– Chronic Obstructive Pulmonary Diseases (COPD)
– Congestive Heart Failure (CHF)
– Hypertension (HTN)
– Uncontrolled diabetes without complications
– Diabetes short-term complications
– Diabetes long-term complications
3

Project background
Purpose:
• Explore validity and utility of a composite
indicator versus a number of disease specific-
indicators
• Explore the extent to which a composite
indicator improves international comparability
4

Project background
Scope:
• to utilize currently collected indicators of
potentially avoidable hospitalizations
• potentially avoidable hospitalizations for
selected chronic conditions
– for which access to appropriate primary care
could prevent the need for the current
admission to hospital
5

Results
6

Approach
• To address the potential effect of different coding
practices internationally, subgroups were created
• Subgroups represent conditions that can
potentially be coded as a principal diagnosis
interchangeably:
– Asthma + COPD
– CHF + HTN
– 3 Diabetes (uncontrolled, short-term and long-term
complications)
• The overall composite was also calculated
7

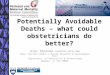
Asthma + COPD, 2011 (or nearest year)
8
0
50
100
150
200
250
300
350
400
450
500
Ag
e-S
ex S
tan
dard
ized
Rate
(p
er
100,0
00)
Asthma
COPD
COPD + Asthma

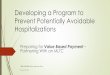
CHF + Hypertension, 2011 (or nearest year)
9
0
100
200
300
400
500
600
700
800
900
Ag
e-S
ex S
tan
dard
ized
Rate
(p
er
100,0
00)
CHF
Hypertension
CHF + Hypertension

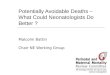
Diabetes, 2011 (or nearest year)
10
0
50
100
150
200
250
300
350
400
450
Ag
e-S
ex S
tan
dard
ized
Rate
(p
er
100,0
00)
Uncontrolled
ST
LT
Diabetes Overall

Overall Composite, 2011 (or nearest year)
11
0
200
400
600
800
1000
1200
1400
Ag
e-S
ex S
tan
dard
ized
Rate
(p
er
100,0
00)
COPD + Asthma
CHF + Hypertension
Diabetes Overall
Overall

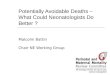
Overall Composite, 2011 (or nearest year)
12
24% 29%
47%
22%
59% 46% 47% 52% 41%
30% 18%
41%
55%
28%
48% 49% 49%
34%
19%
33% 35%
22%
28%
20%
34% 52%
54%
35% 67%
26% 39% 42% 38%
31% 52%
27%
46% 27%
53%
33% 34% 29%
39% 58% 31%
45% 58%
46% 61% 36%
24%
16% 18%
12% 15% 15% 11% 10%
29% 18%
55%
13% 19% 19% 19%
17% 21% 27%
23% 36%
20%
20%
26%
19%
30%
0
200
400
600
800
1000
1200
1400
Ag
e-S
ex S
tan
dard
ized
Rate
(p
er
100,0
00)
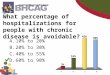
Diabetes Overall
CHF + Hypertension
COPD + Asthma

Overall Composite, 2011 (or nearest year)
International Variation
13
Highest Rate
(per 100,000) Lowest Rate
(per 100,000) Variation
Asthma 151 11 14-fold
COPD 378 23 16-fold
COPD and Asthma 451 58 8-fold
CHF 595 57 10-fold
Hypertension 374 1 374-fold
CHF and Hypertension 810 58 14-fold
Diabetes Uncontrolled 181 3 60-fold
Diabetes Short-term 65 8 8-fold
Diabetes Long-term 271 19 14-fold
Diabetes Overall 405 54 8-fold
Overall 1,339 363 4-fold

Summary of findings
• Results suggest that differences in coding
practices between interchangeable codes do
exist (e.g. Austria, Korea for HTN & CHF)
• Rankings continue to be similar
• Two years of results show similar patterns
• Composite indicator shows reduction in
international variation
• Additional work is required to finalize the
methodology of the composite indicator
14

Suggested methodological adjustments
• Explore exclusion of deaths:
– hospitalization where death occurs is mostly likely not
immediately avoidable
• Explore exclusion of patients age 75 and older:
– older patients have higher morbidity and mortality and are
more likely to require a hospitalization which is not
avoidable
• Refine definitions of the individual conditions as
determined by the UK R&D project
15

Discussion
16

Considerations for the composite indicator
in its current form
Advantages:
• Provides a simple, easy to communicate overall
assessment of primary care
• Has defined scope: avoidable hospitalizations for
selected chronic conditions
• Groups individual conditions in a clinically meaningful
way
• Improves face validity and international comparability
• Allows for inclusion of primary health care indicators in
Health at a Glance
17

Considerations for the composite indicator
in its current form
Disadvantages:
• Not covering the whole universe of potentially
avoidable hospitalizations
– Revising the scope will require substantial R&D work
• Several countries do not submit data for one or more
of the individual conditions, which may result in
exclusion from a composite
18

Key questions
• Do HCQI experts support reporting potentially
avoidable hospitalizations as a composite
indicator in general?
• Do HCQI experts agree with the scope of this
composite indicator as:
– Potentially avoidable hospitalizations for selected
chronic conditions, for which access to appropriate
primary care could prevent the need for the current
admission to hospital?
19

Recommendations for data collection
• Collect data for all 7 chronic conditions
(including hypertension)
• Collect information to support completion of R&D
work:
– Collect counts with and without in-hospital deaths for
the 7 conditions
– Question set to identify any country-specific coding
standards for current selection of chronic conditions
and why data is missing (e.g. not collected vs.
alternate coding practice)
20

Acknowledgments
Canada’s project team • Yana Gurevich, Sunita Karmakar-Hore, Mahbubul Haq
Ireland • Deirdre Mulholland
Israel • Yael Applbaum, Anat Ekka-Zohar, Shulamit Gordon
Italy • Fabrizio Carinci
New Zealand • Vladimir Stevanovic
Singapore • Denise Lee
South Korea • Sun Min Kim, Kyoung Hoon Kim
United Kingdom • Veena Raleigh, Candida Ballantyne
21

22
Thank You!