Embed Size (px)
Citation preview
A national update on Men’s Health statisticsin Scotland and Europe
Matt Maycock, PhDInvestigator Scientist
Social and Public Health Sciences Unit, University of Glasgow
Men's Health in Scotland – is it still a lost cause? Seminar hosted by MHFS and NHS Forth Valley
Wednesday, June 17th 2015: 13:00 – 16:00
Overview of the presentation
• Men’s health in Scotland
• Overview of key issues in men’s health
• Men’s use of services
• What can be done about this?
• Examples from the UK and Scotland
Scottish Men’s Health – Summary
• In 2010 the healthy life expectancy among women in Scotland was 61.9 years, almost two years more than the healthy life expectancy for men of 59.5 years.
• Heart disease incidence and mortality is consistently higher for males than it is for females, across all age groups. Up to the age of 75, stroke incidence and mortality rates are higher for males.
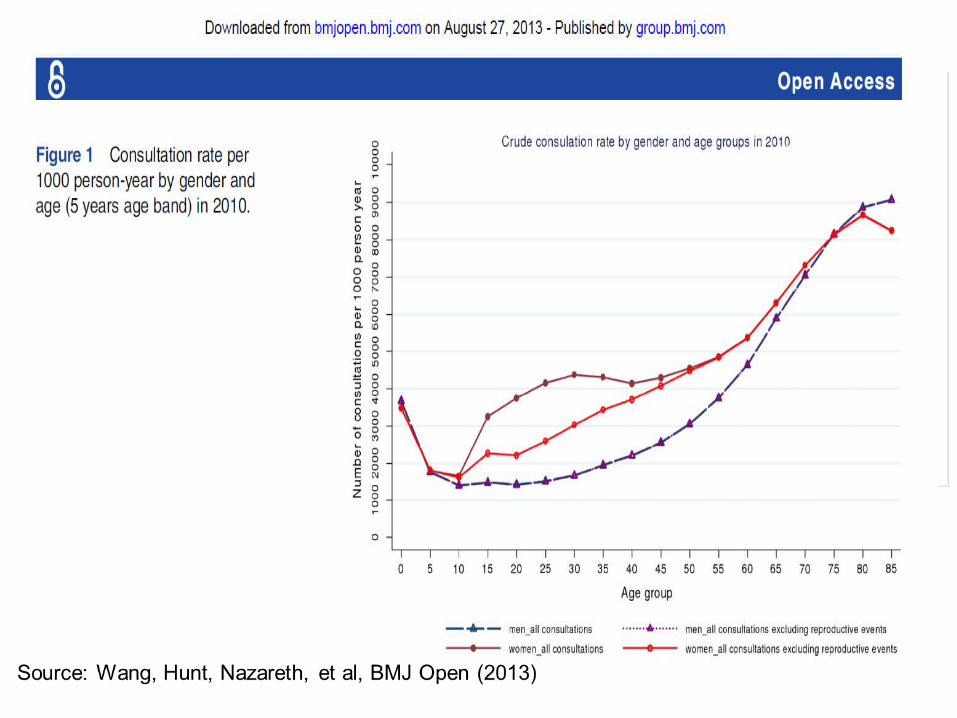
• Men consult their GP less often than women. For the years 2003/4 to 2011/12, the number of consultations per 1,000 populations has been approximately 50% higher for women than for men.
• In 2010/11 males were 17% more likely to attend an NHS Scotland emergency department than females, with 274 attendances per 1,000 population for males versus 235 for females.
• Men were more likely than women to be hazardous or harmful drinkers: 27% of men drank at hazardous or harmful levels compared to 19% of women.
• Men were also significantly more likely to drink above the recommended daily limit on their heaviest drinking day in the previous week (43% of men compared to 34% of women).
• In 2010/11, rates of alcohol related hospital admissions for males were more than double females rates (1,020 per 100,000 population compared to 395 per 100,000 population).
• There was no real difference in smoking prevalence between men and women. The rate for men was slightly higher but the difference was not significant (26% compared with 24%). However, men smoked an average of 2 cigarettes per day more than women (15.2 compared with 13.3) and started smoking at a slightly younger age (17.2 years) than women (17.8 years).
Scottish Health Survey (2012) Alcohol/Smoking
• There was a small but significant gender difference in the proportion of men and women eating 5 or more portions of fruit and vegetables per day (24% of women compared with 21% of men) with a similar pattern in the mean number of portions eaten per day (women ate 3.4 portions compared to 3.1 for men).
• There was no significant difference in the prevalence of obesity, although men were more likely to be overweight than women (69% compared with 61%).
• For children, a lower proportion of boys are in the healthy weight range than girls, although the size of the gap has varied over recent years. The indicators also show that a higher proportion of men than women meet the physical activity recommendations, with 45% of men meeting the requirements compared to a third of women.
• There was a small but significant difference in the prevalence of cardio-vascular disease (CVD) between men and women, with men being more likely to have a CVD condition (16% vs 14%).
Scottish Health Survey (2012) Diet/Obesity/CVD
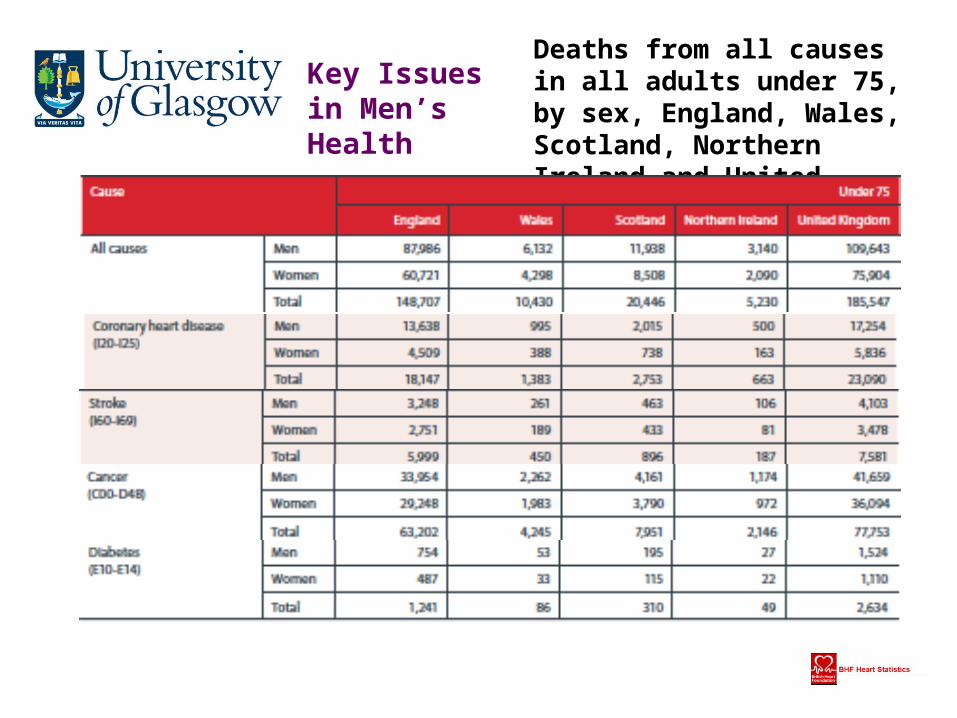
Deaths from all causes in all adults under 75, by sex, England, Wales, Scotland, Northern Ireland and United Kingdom 2010
Key Issues in Men’s Health
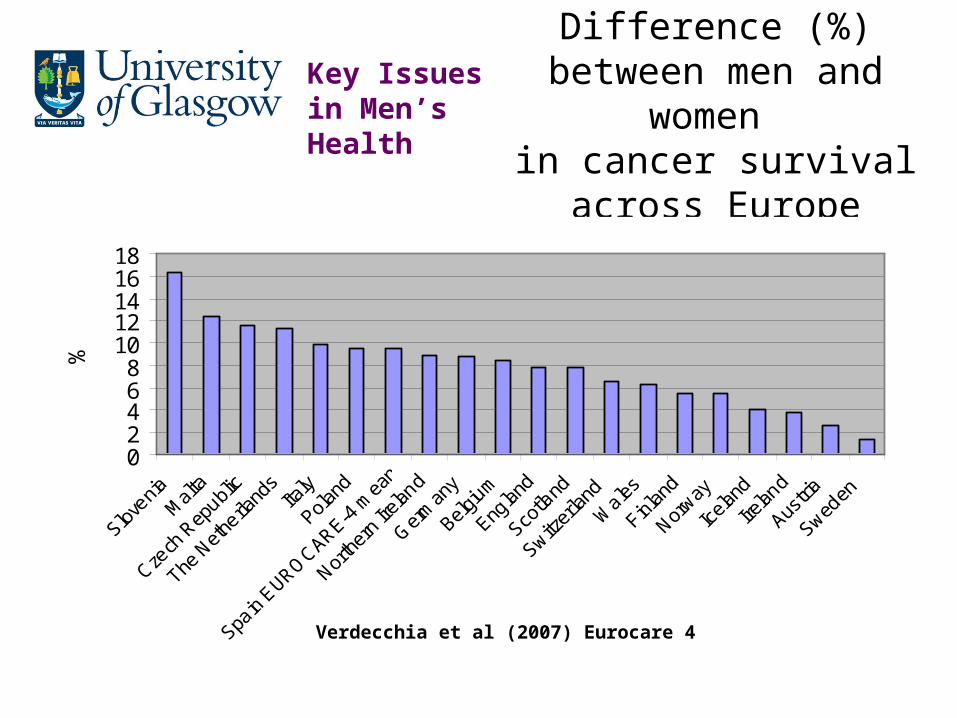
Difference (%) between men and women
in cancer survival across Europe
02468
1012141618
%
Verdecchia et al (2007) Eurocare 4
Key Issues in Men’s Health
• Middle-aged men twice as likely to have diabetes as women.
• Men twice as likely to not know they have diabetes.
• In Scotland there were also significantly more men (6%) than women (4%) with diabetes.
DiabetesKey Issues in Men’s Health
More women than men diagnosed with common mental health problems, but:• Almost three quarters of people who kill themselves are men.• 73% of adults who “go missing” from home are men.• 90% of rough sleepers are men.• Men are three times more likely than women to be alcohol
dependent.• Men are more than twice as likely to use Class A drugs.• 79% of drug-related deaths occur in men.
Key Issues in Men’s Health Mental Health
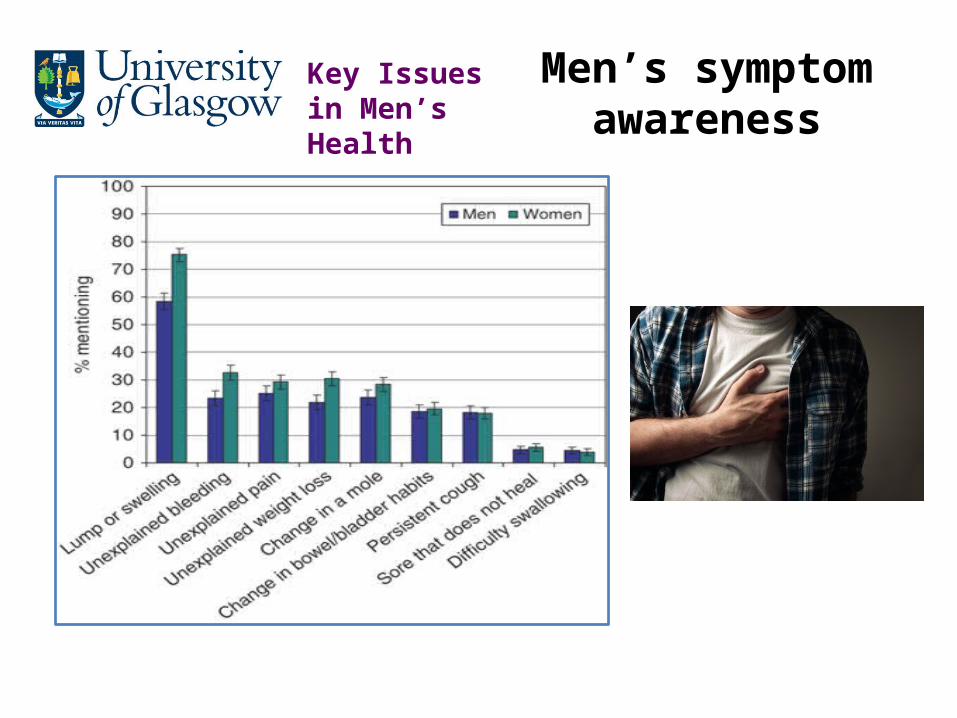
Men’s symptom awareness
Key Issues in Men’s Health
Men are less likely than women to:
• See a GP
• Attend for a Health Check
• Opt for bowel cancer screening
• Visit a pharmacy
• Have a dental check-up
Key Issues in Men’s Health
Key Issues in Men’s Health
Key Issues in Men’s Health
• Men on average visit a pharmacy four times a
year.
• Average for women may be closer to 18
times per year.
• Nearly half (47%) of people accessing the
New Medicines Service – a free advice
service for people taking a new medicine for
a long term condition are men. ‐
Key Issues in Men’s Health
NPA interim review: men’s uptake ofpharmacy services (Nov 2012)
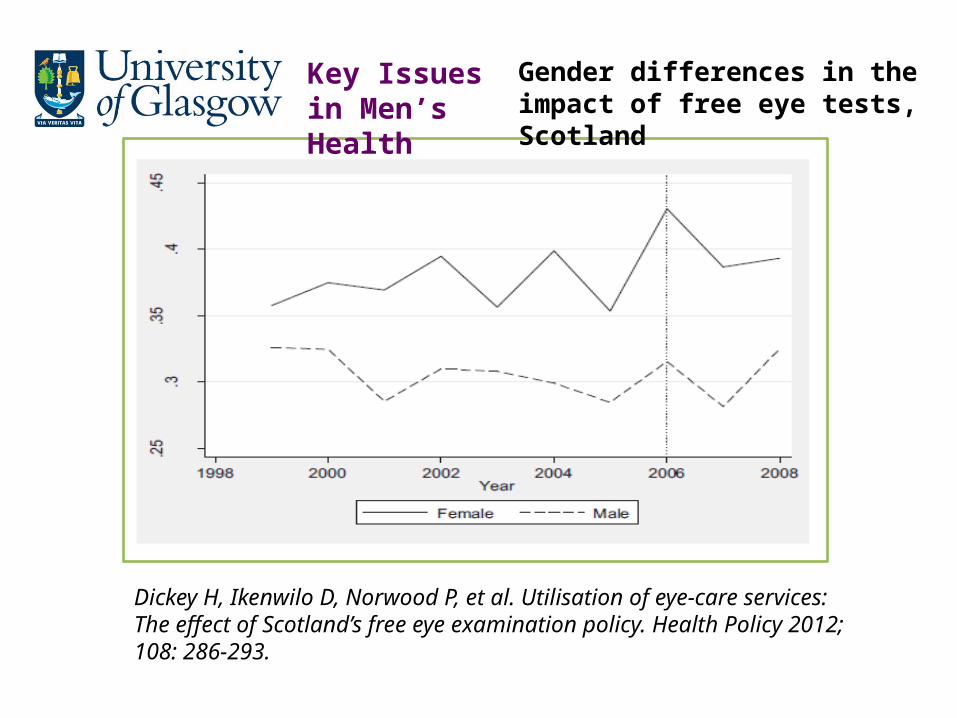
Dickey H, Ikenwilo D, Norwood P, et al. Utilisation of eye-care services: The effect of Scotland’s free eye examination policy. Health Policy 2012; 108: 286-293.
Key Issues in Men’s Health
Gender differences in the impact of free eye tests, Scotland
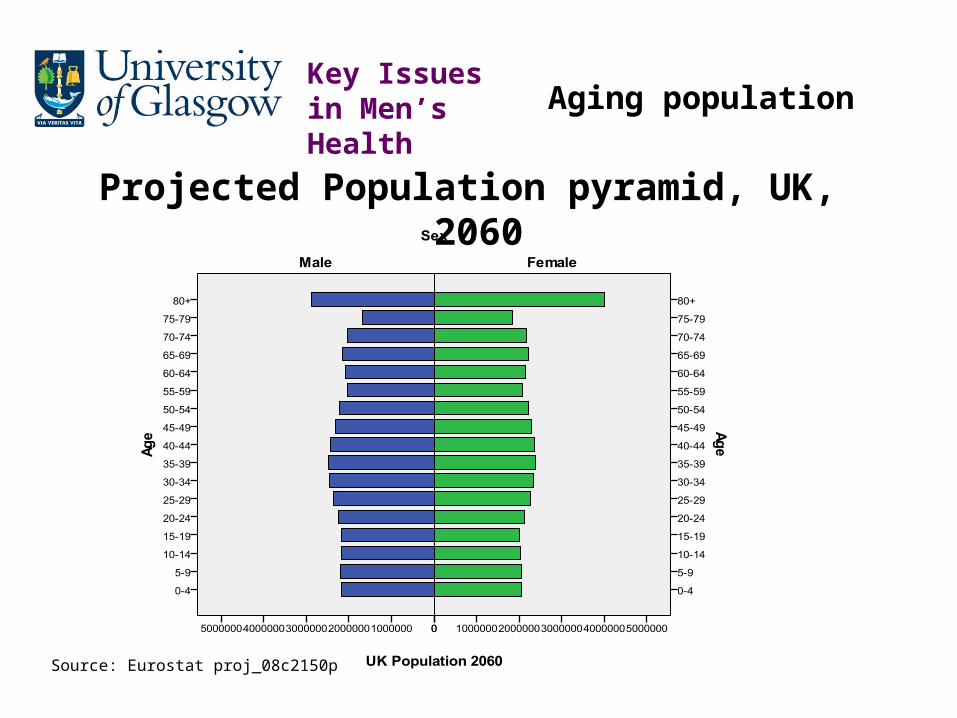
Projected Population pyramid, UK, 2060
Source: Eurostat proj_08c2150p
Key Issues in Men’s Health Aging population

Standing break 1…
…and questions?


Football Fans in Training: a gender sensitised weight loss, physical activity and healthy lifestyle programme for men
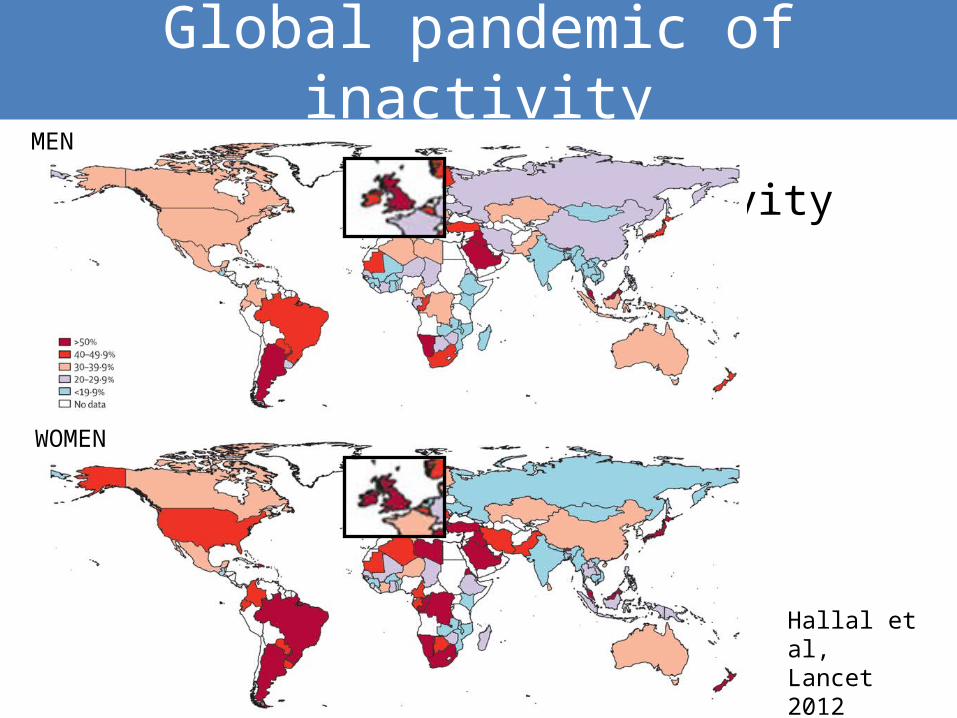
Global pandemic of inactivity
• Global pandemic of inactivity
Hallal et al, Lancet 2012
MEN
WOMEN
Men and weight loss
• 5-10% weight loss can produce significant health benefits (NICE 2006; SIGN 2010)
• Traditional weight management services do not reach many men
Less than 15% of referrals to commercial sector
(Jebb et al Lancet 2011)
Only 23% of attendees at NHS weight management services (Counterweight Br J Gen Pract 2008)
Many men think
slimming and dieting
are just “for
women” …
Gough Soc Sci Med 2007;64(2):326-37
…and may prefer to control their weight through exercise
Pliner et al. Pers Soc Psychol Bull 1990;16(2):263-73.

• Almost 4 million fans pass through Scottish Premier League club turnstiles each season
(SPFL 2010)
• Most are male; a large proportion from low SES backgrounds
• Powerful social and psychological connections (often life-long and cross-generational)
(Hirt et al 2010)
Traditional male sporting environment

FFIT weight loss components
Alcohol awareness
Weight loss
Long-term behaviour change strategies
BANTER
Food• Portion sizes• Healthy, balanced diet
INCREASED PHYSICALACTIVITY
Goal 5-10% weight loss
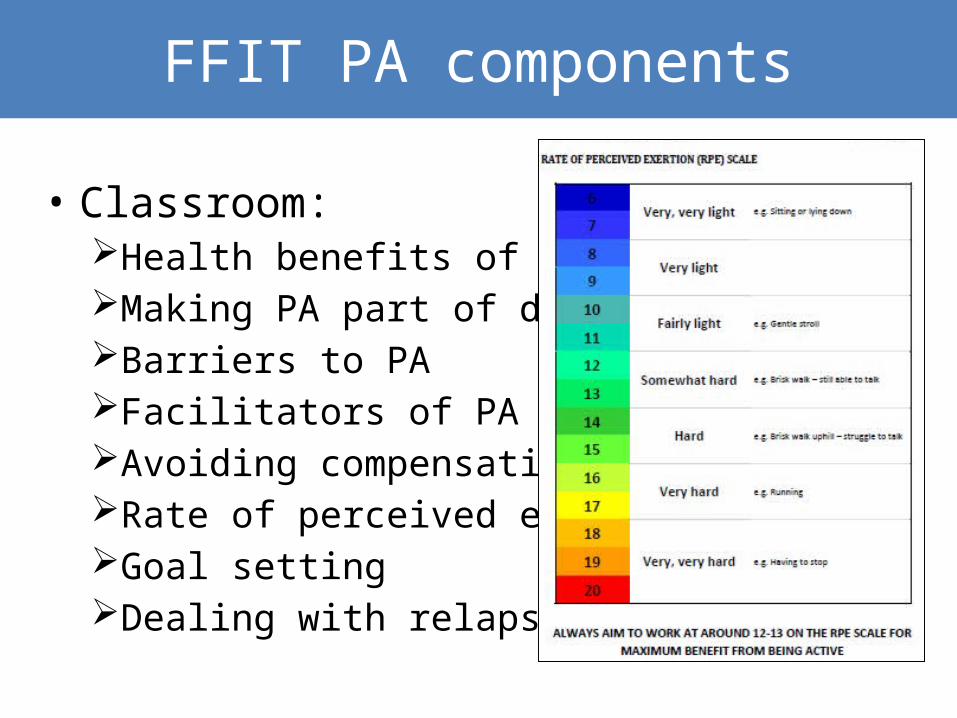
FFIT PA components
• Classroom:Health benefits of PAMaking PA part of daily lifeBarriers to PAFacilitators of PAAvoiding compensationRate of perceived exertionGoal settingDealing with relapse
• “Homework”Target: 45-60 mins moderate PA on most days of week Incremental, personal pedometer-based brisk
walking programme (Fitzsimons, Baker et al. 2012)
Progression to other activities (swimming/cycling)Use of local facilitiesMeeting up to exercise together
FFIT PA components
FFIT PA components
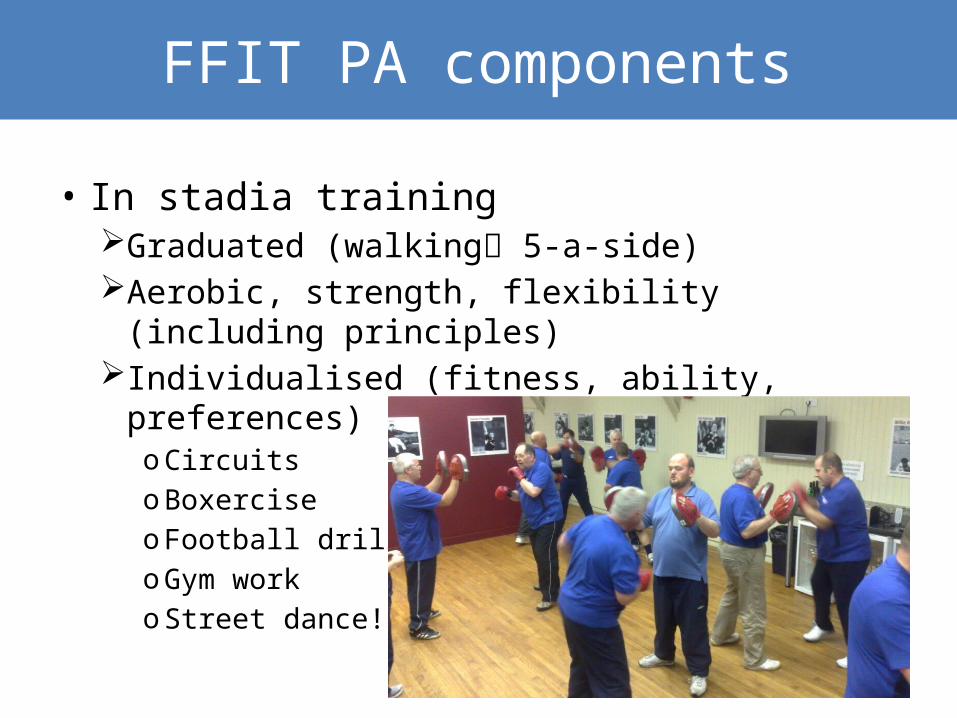
• In stadia trainingGraduated (walking 5-a-side)Aerobic, strength, flexibility (including principles)Individualised (fitness, ability, preferences)
oCircuitsoBoxerciseo Football drillsoGym worko Street dance!
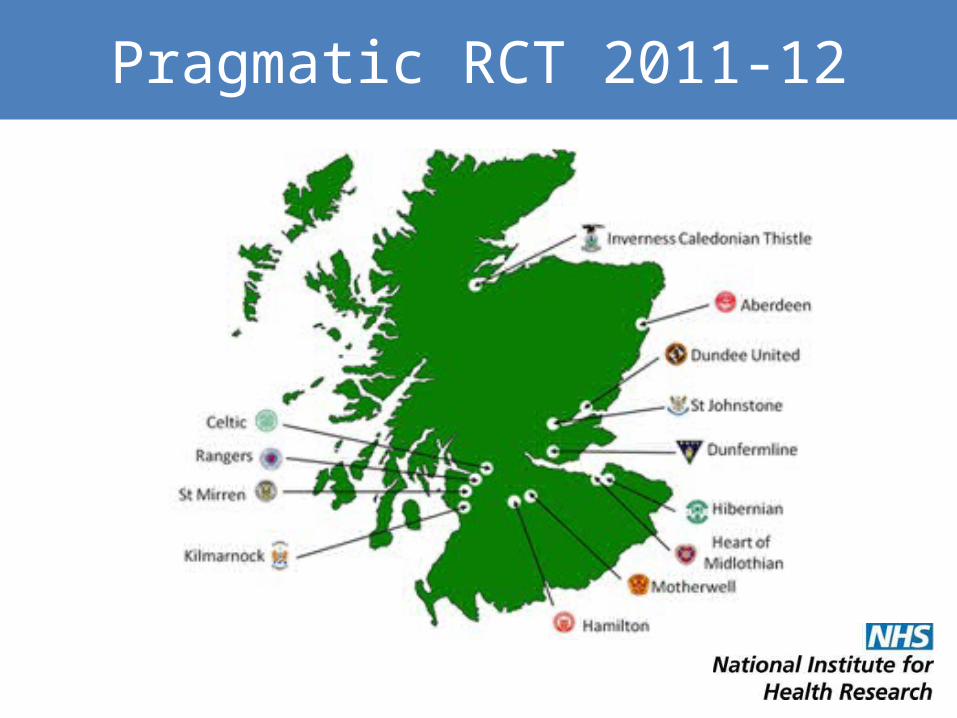
Pragmatic RCT 2011-12
World-leading research
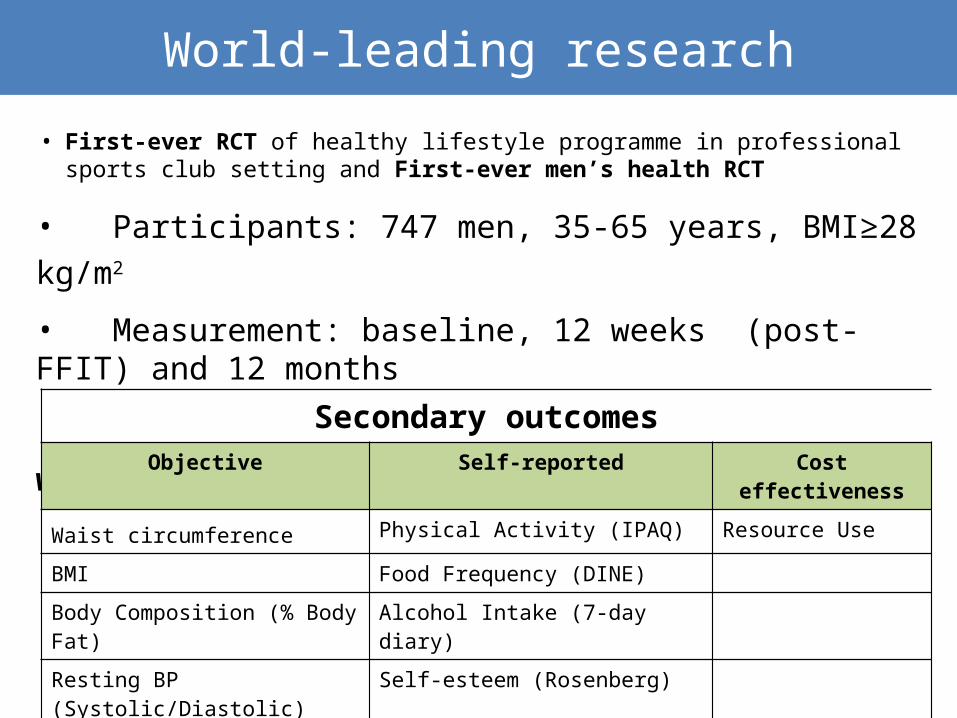
• Participants: 747 men, 35-65 years, BMI≥28 kg/m2
• Measurement: baseline, 12 weeks (post-FFIT) and 12 months
• Primary outcome: objectively-measured weight loss at 12 months
• First-ever RCT of healthy lifestyle programme in professional sports club setting and First-ever men’s health RCT
Secondary outcomesObjective Self-reported Cost effectiveness
Waist circumference Physical Activity (IPAQ) Resource Use
BMI Food Frequency (DINE)
Body Composition (% Body Fat) Alcohol Intake (7-day diary)
Resting BP (Systolic/Diastolic) Self-esteem (Rosenberg)
Positive and Negative Affect (PANAS)
Health-related Quality of Life (SF-12)

Results – who did FFIT attract?
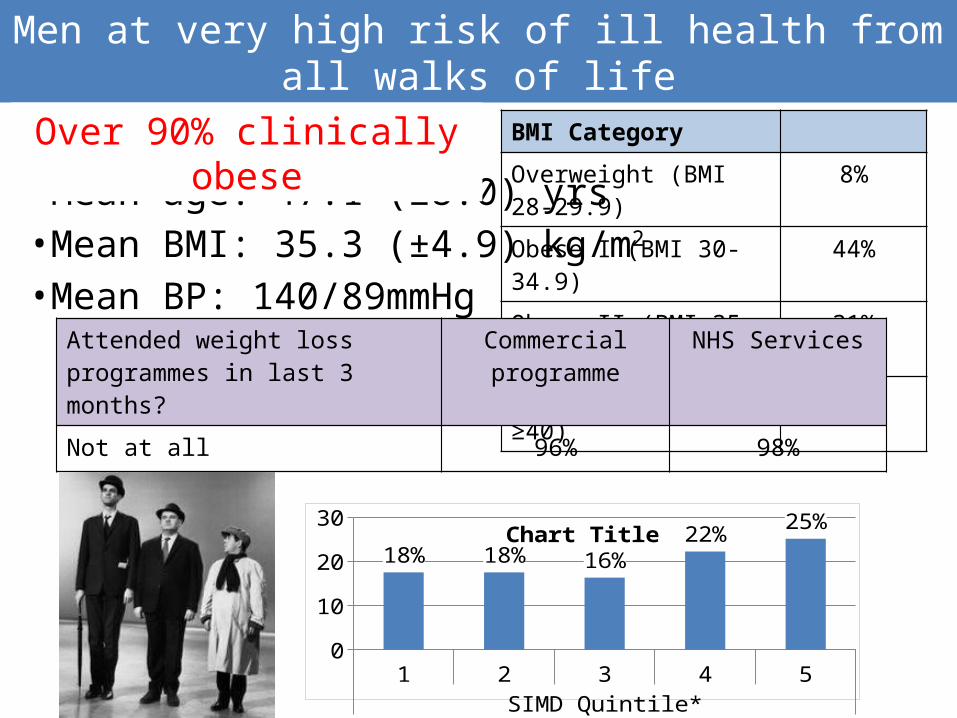
Men at very high risk of ill health from all walks of life
• Mean age: 47.1 (±8.0) yrs • Mean BMI: 35.3 (±4.9) kg/m2
• Mean BP: 140/89mmHg
BMI Category
Overweight (BMI 28-29.9) 8%
Obese I (BMI 30-34.9) 44%Obese II (BMI 35-39.9) 31%
Obese III (BMI ≥40) 17%
Attended weight loss programmes in last 3 months?
Commercial programme
NHS Services
Not at all 96% 98%
Over 90% clinically obese
1 2 3 4 5SIMD Quintile*
05
1015202530
18% 18% 16%22% 25%Chart Title

What makes men want to attend FFIT?What makes men want to attend FFIT?
Hunt et al, 2014, BMC Public Health
‘Push’ and ‘Pull’: football club a powerful draw
I was very aware that, every time I was buying a new suit ... the trouser size was getting bigger, and I just wasn’t happy with that, and I just wanted to address it. And with it being, having a tie in with the team I’ve supported all my life, I felt that the two kind of – they, it fitted nicely. It meant I could do something and I could maybe get a wee sneaky peek behind the scenes at Fir Park. [Club04_12wkFG_P2]
I’ve struggled with my weight since, maybe, early-twenties and I’ve tried various diets, various things, .... So, when I seen this advertised in the paper ... I think the main thing that drew us to it was because it’s Hibs. You’re going to be involved at Hibs, whether it just be at the ground, stadium ... That was what really attracted me to it. [Club07_12wkFG_P1]
Men like meP1: The good thing was, straight from the start, we all had something in common with each other. Rather than being sixteen strangers, we’d all something in common, and that was the club and a love for it. P5: Two things in common. We were fat and we supported [the club]. P1: …and that was the big factor. So no matter, you met up the first few weeks, you didn’t know each other’s names, we immediately were able to converse with each other easily.
[Club03_12wkFG]
Insider viewJust the enjoyment of coming along and being involved in the club .. even walking round [stadium], to me, was an exciting part of the Monday night, and you know, walking up and down the terraces. You might only be restricted to one area when you come to a game, but you know, the fact that you’ve got carte blanche, you can go wherever you like, other than the pitch.
[Club02_12wkFG_P1]
Men were immediately comfortable and receptive

Standing break 2 …
…and questions so far?

Results – was FFIT effective?
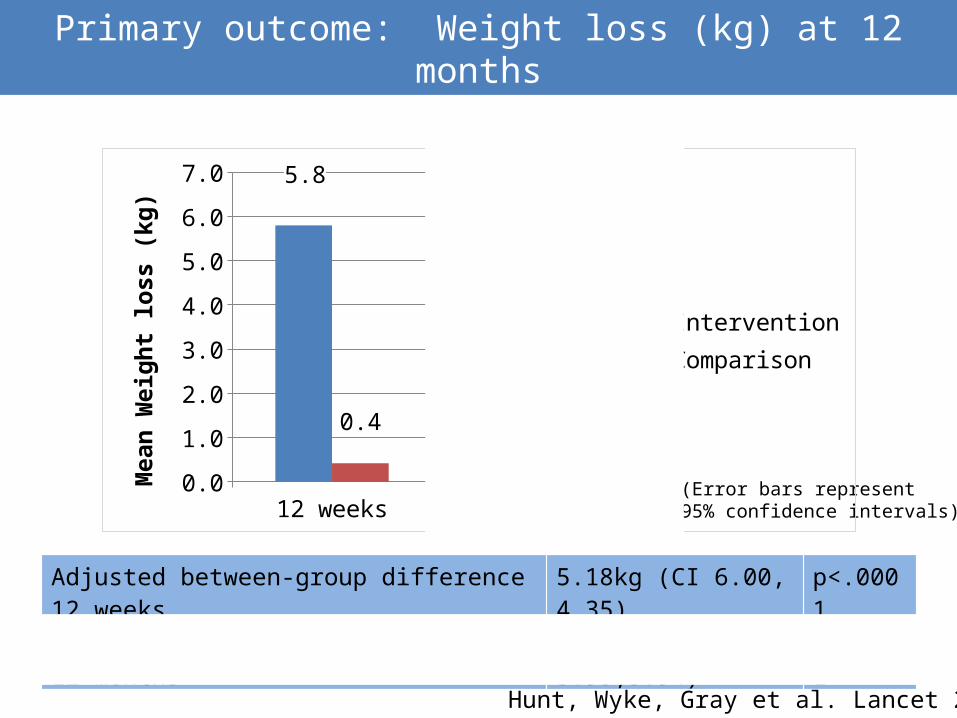
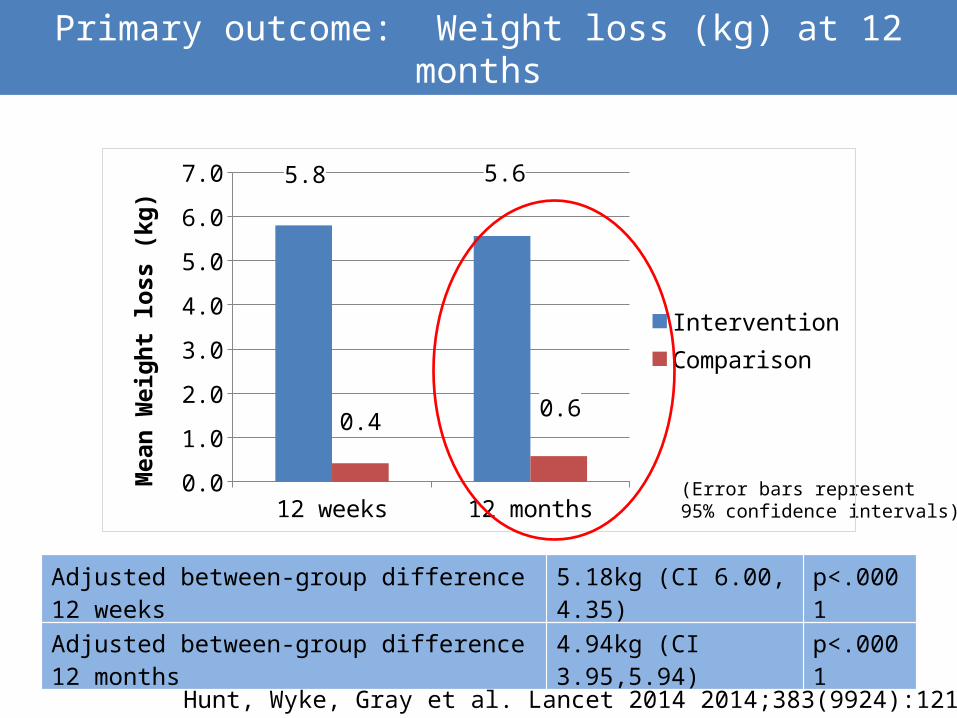
Primary outcome: Weight loss (kg) at 12 months
(Error bars represent 95% confidence intervals)
Adjusted between-group difference 12 weeks 5.18kg (CI 6.00, 4.35) p<.0001
Adjusted between-group difference 12 months 4.94kg (CI 3.95,5.94) p<.0001
12 weeks 12 months0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0 5.8 5.6
0.4 0.6
InterventionComparison
Mea
n W
eigh
t los
s (k
g)
Hunt, Wyke, Gray et al. Lancet 2014
Primary outcome: Weight loss (kg) at 12 months
(Error bars represent 95% confidence intervals)
Adjusted between-group difference 12 weeks 5.18kg (CI 6.00, 4.35) p<.0001
Adjusted between-group difference 12 months 4.94kg (CI 3.95,5.94) p<.0001
12 weeks 12 months0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0 5.8 5.6
0.4 0.6
InterventionComparison
Mea
n W
eigh
t los
s (k
g)
Hunt, Wyke, Gray et al. Lancet 2014 2014;383(9924):1211-21

Results – How did FFIT work?
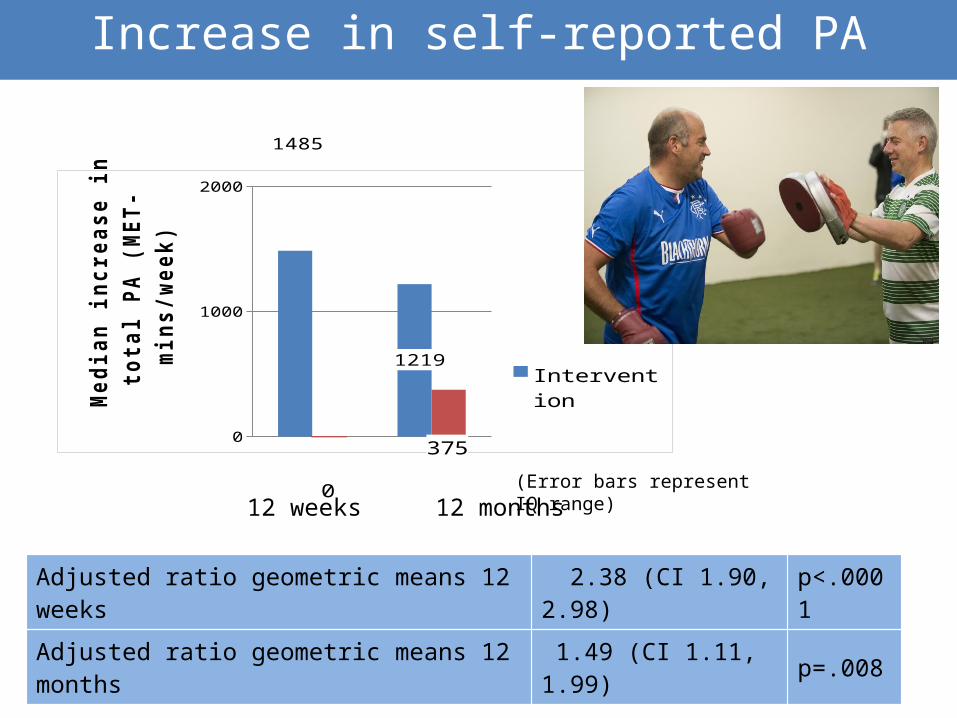
Increase in self-reported PA
Adjusted ratio geometric means 12 weeks 2.38 (CI 1.90, 2.98) p<.0001
Adjusted ratio geometric means 12 months 1.49 (CI 1.11, 1.99) p=.008
(Error bars represent IQ range)
0
1000
2000
1485
1219
0
375
InterventionComparison
Me
dia
n in
cre
ase
in t
ota
l PA
(M
ET
-min
s/w
ee
k)
12 months12 weeks
The value of the pedometer and walking– The pedometer was widely accepted and its use
quickly became routinized in men’s daily lives
– A valued technology for motivation, self-monitoring, and goal-setting
It’s given me a good kick up the backside… every day after I’ve had my shower and got dressed, the first thing that I do is put my pedometer on…it’s made me consciously go out of my way to walk more. (TI-6)
The value of the pedometer and walking
• It’s an amazing wee device. .. Before you maybe thought you’d been staying active but when you look at your pedometer you realise you hadnae. (TI-18)
• I love that part of it but I never go out without my (pedometer). It really is amazing. I wear it every day and record it every day .. That’s tangible, something you can touch and see … I think eveybody was highly delighted wi’ the pedometer (TI-12)
The value of the pedometer and walking
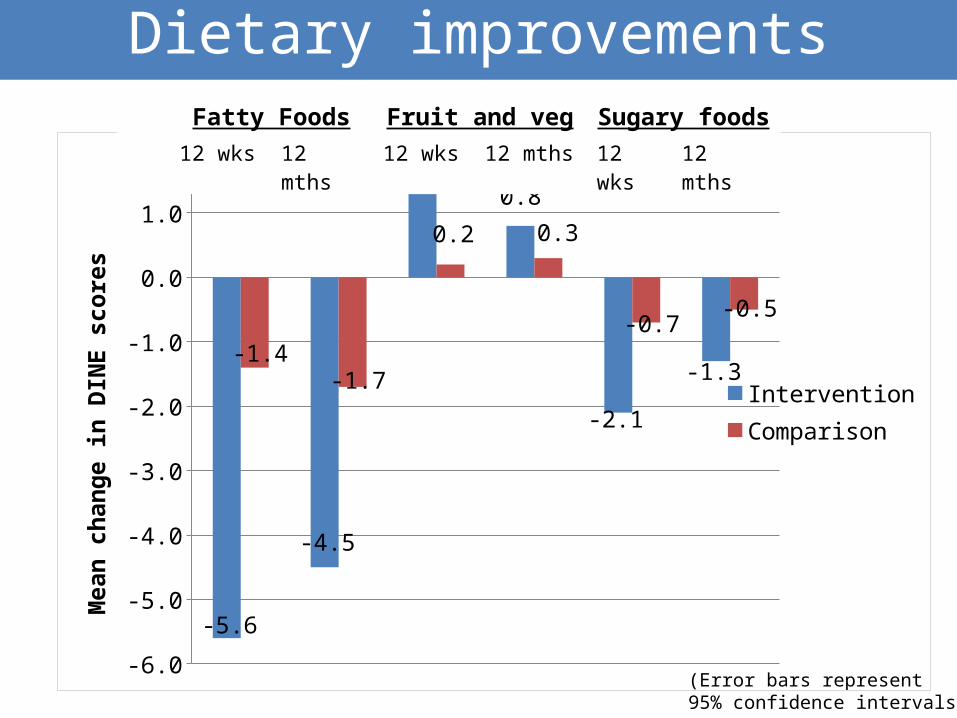
(Error bars represent 95% confidence intervals)
-6.0
-5.0
-4.0
-3.0
-2.0
-1.0
0.0
1.0
2.0
-5.6
-4.5
1.6
0.8
-2.1
-1.3-1.4
-1.7
0.2 0.3
-0.7-0.5
InterventionComparison
Mea
n ch
ange
in D
INE
scor
esFatty Foods Fruit and veg Sugary foods
12 wks 12 mths 12 wks 12 mths 12 wks 12 mths
Dietary improvements
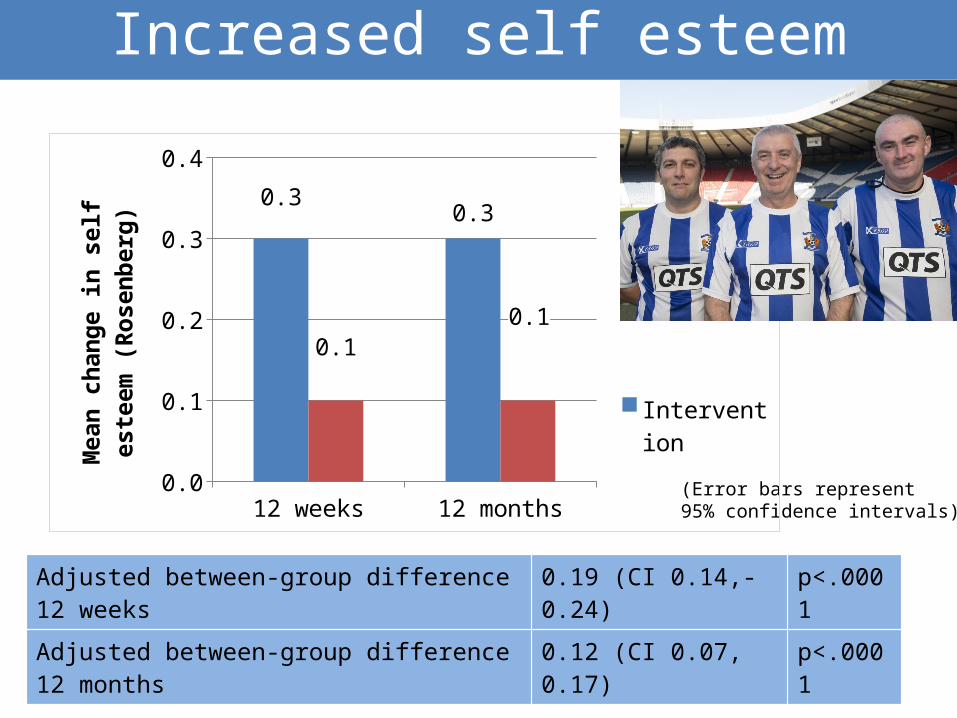
Increased self esteem
Adjusted between-group difference 12 weeks 0.19 (CI 0.14,-0.24) p<.0001
Adjusted between-group difference 12 months 0.12 (CI 0.07, 0.17) p<.0001
(Error bars represent 95% confidence intervals)12 weeks 12 months
0.0
0.1
0.2
0.3
0.4
0.30.3
0.10.1
InterventionComparison
Mea
n ch
ange
in s
elf e
stee
m
(Ros
enbe
rg)
‘Effervescence’ and renegotiation of identityEffervescence and group identity
P2: The group helped, eh, because to be honest… there was naebody took a disliking to anybody and we aw got on. We were on the park and we were help, ken, “come on, dae this.” And we were aw hoping that everybody came every week and lost weight, eh?
I think self-encouragement is, we’re there, because we’re part of a group, we were all encouraging each other. It’s not, you were no longer an individual. You were part of a team [Club07_12wkFG_P1]
Renegotiation of habitual practice and masculine identity
Blokes don’t do it…Until we get that support from each other and then we start looking at portion controls, and what you’ve said there, what’s on the labels – blokes would just go and look for the easy option. That’s what men do. [Club12_12wkFG_P4]
It was funny, listening to men – and I don’t want to sound sexist – but men going on about weighing themselves in the morning and what diet they were on and what they were eating, and, “I had my porridge every morning,” and I think and it was good. And there was a really camaraderie about the course. [Club10_12wkFG_P1]
What men said helped them
Self-monitoringI find that the pedometer even now it’s my conscience. If I can look back seven days and say, “Phew, I’m only averaging about seven thousand. I usually should be doing eight or nine”. It’ll make me go for a longer walk some time later in the week. [Club10_12mthFG_P2]
Behaviour change techniques
Implementation intentions I think the thing for me is actually the planning of stuff […] You know about how, if you
want tae walk you’re gonna have to plan about “When am I gonna walk?” An’ also I quite often end up staying at hotels or whatever for work, an’ you have to know, “What am I gonna eat? Where am I gonna eat?” So you have to do a bit more planning about how you do that. […] You have to sort of try an’ work something out there so you don’t end up goin’ to Greggs or whatever.
[Club05_12mthFG_P3]
Barriers to maintenance
Injury and illnessI’ve got bother wi’ my Achilles heels and I stopped all my walking altogether […] then I started getting doon. [Club10_P4]
Weather I put it doon tae weather, because this year in particular there’s been a hell of a lot of rainfall and you cannae get, you cannae go on the bowling green […] because it’s been flooded for aboot three days. So you cannae get, that’s your activity oot the window. [Club10_P6]
Life events My brother passed away which is one o’ the difficult things […] basically he died in his early fifties […] it was his heart that caused problems, so you think that well that kinda would inspire you, but to a certain extent that was probably one of the worst times where, you know, things were going wrong and it was just, you know, feeling bad and eating. [Club09_P5]
Job related factors/lack of time, lack of money
Is FFIT is cost effective?
YES!Within trial analysis• Programme cost c£165 per man
• Incremental cost-effectiveness:£13,847 per QALY gained - well below NICE thresholds for
cost-effectiveness£20,000/QALY: 0.72; £30,000/QALY: 0.89
Long term analysis• Gained 0.43 life years (95% CIs - 0.32, 0.56) and 0.38 QALYs
(95% CIs - 0.25, 0.55)• £2,535 per life year gained; £2,810 per QALY gained• If decision maker willing to pay £5,000 per QALY, no
uncertainty that FFIT is cost-effective

Conclusions
• FFIT succeeds in helping men satisfy basic psychological needs in relation to PA
• Participants describe a trajectory of competence– internalisation associated with successful
maintenance?• Difficulties encountered included injury, illness,
life events and job related issues
• Men feel attracted to/comfortable in football club setting
• Being with men like me permits challenges to traditional male identities weight loss and behaviour change
• Importance of role of wider social context in negotiating lifestyle change
• Satisfaction of basic psychological needs can promote sustained change
• Promising emerging findings from other settings
What has FFIT shown us?
FFIT website: www. ffit.org.uk
Challenges views on men’s willingness to
engage positively with their health – men
can and men will!
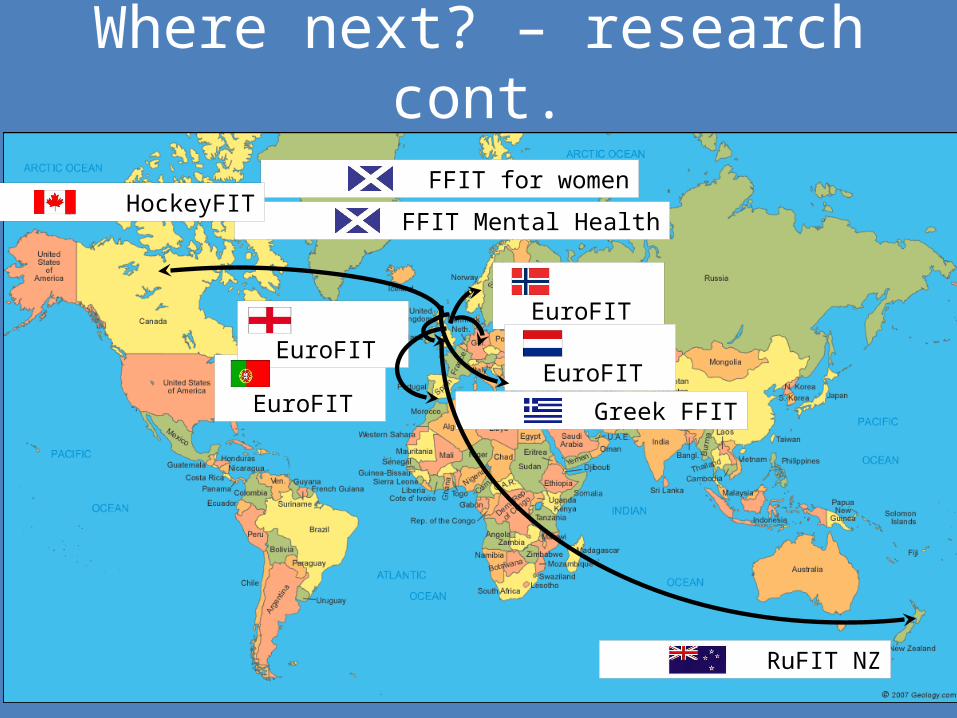
Where next? – research cont.
FFIT for women
FFIT Mental Health
Greek FFIT
EuroFIT
EuroFIT EuroFIT
EuroFIT
HockeyFIT
RuFIT NZ
Acknowledgements
Thanks to Participants, coaches, MRC/CSO SPHSU Survey Office and Gender and HealthTeam, Tayside Clinical Trials Unit
Collaborators Sally Wyke, Kate Hunt, Cindy Gray, Chris Bunn, Annie Anderson, Shaun Treweek, Peter Donnan, Nanette Mutrie, Jim Leishman Elizabeth Fenwick, Alan White, Adrian Brady, Petra Rauchaus, Eleanor Grieve, Nicki Boyer
FFIT Programme Delivery SPL Trust – Billy Singh, Euan Miller, Stuart McPhee, Mark Dunlop and Iain Blair, Coaches in SPL clubs
FFIT Programme Funding Scottish Government, Football Pools
Research Funding SPL Trust, CSO, MRC/CSO SPHSU Gender and Health programme, NIHR PHR programme, Bupa Foundation, EU FP7
This RCT was funded by the National Institute of Health Research Public Health Research (NIHR PHR) programme (project number 09/3010/06). The views expressed here are those of the authors and not necessarily those of the NIHR PHR programme or the Department of Health

Standing break 3…
…and final questions?
• Hunt K, Wyke S, Gray CM et al. In: Sports-based health interventions: case studies from around the world. New York: Springer, [in press].
• Wyke S, Hunt K, Gray CM et al. Public Health Research [in press]• Hunt K, Gray CM, Maclean A et al. BMC Public Health 2014;14:50• Hunt K, Wyke S, Gray CM et al. The Lancet 2014;383:1211-21• MacLean A, Hunt K, Gray CM et al. International Journal of Men’s
Health 2014;13:121-138• Gray CM, Hunt K, Mutrie N et al. BMC Public Health 2013;13:232 • Gray CM, Hunt K, Mutrie N et al. International Journal of Behavioral
Nutrition and Physical Activity 2013;10:121• Hunt K, McCann C, Gray CM, Mutrie N, Wyke S. Health
Psychology 2013;32:57-65






























