Embed Size (px)
DESCRIPTION
This addition to the 'Picture of Health' series of reports looks at the NHS Health Check services being delivered in the North East of England using Health Diagnostics systems and software.
Citation preview

A Picture Of Health
NHS Health Checks Case Study:The North East of England
Case study

NHS Health Checks Case Study:The North East of England
2
Case study A Picture Of Health The North East of England
The North East of England is well known as being an area of relative poor health compared to much of the rest of England, with the average life expectancy of a man in County Durham being eight years lower than that of his counterpart in the UK’s most affluent borough, Kensington and Chelsea in London.¹ The reasons are complex, but many are rooted in differences in lifestyle and behaviour. In the North East, smoking remains the biggest killer, with 5,500 people dying each year from smoking-related illnesses – more than the total dying from accidents, HIV, alcohol, drug abuse and suicides put together.
Free NHS Health Checks were introduced in 2009 for persons aged 40 to 74 in a mission to reduce health inequalities by identifying those most at risk of stroke, heart disease, diabetes and kidney disease, and direct them towards treatment or behaviour modification programmes such as smoking cessation and healthy eating courses. The Department of Health estimates that universal uptake of health checks throughout the country could prevent 9,500 heart attacks and strokes each year, and expects that 20 per cent of people screened will be at high risk, with this figure being greater in areas of high deprivation.² The ultimate aim is to test 20 per cent of the population every five years, to reach 100 per cent in total, over the cycle. However, in 2011-12, two thirds of PCTs were failing to provide enough checks to meet their target of 20 per cent of the eligible population each year.
In the face of unprecedented NHS budget cuts, and massive structural organisation, many are questioning the economic case for NHS Health Checks, despite diabetes and obesity ‘epidemics’ existing nationwide. However, funding for health checks has been ring-fenced, so in the near-term what seems to be more pressing is information recently obtained from GP surgeries which revealed health check uptake falling nationwide, with just 54 per cent attending a check in 2011/12 compared to 60 per cent in 2010/11.
At present, there is huge inequality in the provision of health checks within and between PCTs. However, as a general rule, people with poor health behaviours who live in areas of relative deprivation are often those who don’t show up for a health check. This is why health economists such as Professor Alan Maynard, who was interviewed for the first report which accompanies this case study, urges, ‘Target the poorer, but go to where they go –Asda or Lidl rather than Waitrose’. Indeed, the ability to tap into local knowledge is a major reason behind the transfer of public health back to local authority control: Namely, making best use of local knowledge and local authorities’ ability to coordinate and integrate different agencies at the local level
From April 2013, responsibility for public health – including commissioning and providing health checks - will transfer from the NHS to local authorities. It remains to be seen how provision will vary geographically after the transfer, but what is certain is not only that funding for NHS Health Checks has been ring-fenced, but that the target for checks will remain 20 per cent of the eligible population.
Introduction: National inequalities in health check provision

NHS Health Checks Case Study:The North East of England
3
Case study A Picture Of Health The North East of England
From April, NHS Health Checks will continue to be provided by a combination of public and private providers, and it is logical to assume that the success of NHS Health Checks will continue to rely upon a collaborative approach between the two. Indeed, The School of Public Health North East recently stated, “Transformational change across the public sector in the North East is no longer an option. New models of collaborative leadership - designed to promote joined-up working to tackle complex health challenges - are urgently needed. The government’s recent proposals for changes in the organisation and delivery of public health, and the shift of responsibility towards local government, have major implications across the North East... Without new models of working, the important recommendations of the NHS and public health white papers, the Marmot Review on Health inequalities, and the expectations of QIPP will not be met.” (QIPP stands for Quality, Innovation, Prevention and Productivity).
Despite the inequalities highlighted above, ‘stars’ stand out. This case study is intended to provide evidence of some well-run, highly-targeted and competently managed NHS Health Check programmes in the North East, where all but one PCT has relied on Health Diagnostics to supply solutions and support to the providers of NHS Health Checks.’ Health Diagnostics Limited (HD) provides the consumables, analysers and software to capture patient data, share the data on-screen, print the data in a report, and relay the data securely back to the patient’s GP. Its portable systems enable checks to be performed in almost any site, and by any willing provider (AWP). Although Health Diagnostics does not carry out the tests directly, the organisation provides the end-to-end services required to implement the checks, and the firm’s role in the North East is widely recognised.
The success of any mass screening initiative relies on successful gathering and handling of data. A recent article2 in the BMJ cited various challenges to implementation of NHS Health Checks: “The challenges of data communication between providers and primary care need to be overcome.” This is why it is imperative for providers to maintain a fast ‘closed loop’ between those performing the checks and the patient’s GP: All data must revert back to GPs. However, in addition, the BMJ article points out that although a typical surgery list of 5,600 patients will have to provide health checks and follow up support for approximately 330 patients each year, most of the checks need not be carried out by a GP, but by nurses, health care assistants, active lifestyle schemes and so on: “Although primary care computer systems capture data on risk factors and prescriptions, they contain little information on lifestyle factors such as physical activity and diet. Computer templates to allow this information to be captured will be essential to evaluate improvements in lifestyle factors.”
Collaboration, coordination, cooperation are key
Health Diagnostics has developed its systems to ensure data can get back into any GP practice system, as well as providing the software capabilities to assess the success or failure of 12 week programmes, such as weight loss courses. (At present, there are several types of software used in GP surgeries, but Health Diagnostics can return data to each and every type.)
In summary, the ability to improve patient behaviour and lifestyle lies partly in enabling data to be shared between patient, GP and those helping via intervention. In the new public health landscape, it will also mean local authorities can assess the performance of such interventions.
It all starts with data

NHS Health Checks Case Study:The North East of England
4
Case study A Picture Of Health The North East of England
Data must also be stored securely and confidentially, as was highlighted recently in media reports about a primary care trust found to have broken the Data Protection Act by passing patient information to a company commissioned to carry out NHS Health Checks - without patients’ consent: Contact details of 3,700 patients identified as likely to benefit from a cardiovascular health check were passed from GP practices to a private provider, and one patient complained after being telephoned by the company. Patients as well as healthcare professionals must have confidence that personal data will be held securely, and shared only in accordance with the appropriate information governance arrangements – and the law. Health Diagnostics’ software enables data to be wiped from lap top computers as soon as the digital upload of health check data is complete.
Trust in the data from GPsIf GPs are to accept the results of health check data obtained by other parties such as pharmacy, or ‘any qualified provider’ into their clinical systems, a standardised format which guarantees accuracy is essential. NHS County Durham,and NHS South of Tyne and Wear are assisted with this issue by the underwriting of its screening programme by Health Diagnostics’ quality assurance in association with Bolton NHS Foundation Trust. The Bolton Quality Assurance Scheme (BQAS) involves Bolton sending out a serum sample every month to all participating sites using cholesterol testing units supplied by Health Diagnostics to test that both operator and analyser are performing to standard. In the words of Gilbert Wieringa, Consultant Biochemist at the Royal Bolton Foundation Trust, “Quality assurance is likely to become a commissioning requirement should high street settings wish to provide services to NHS patients. By insisting now, Health Diagnostics are putting the foundations in place.”
Patient data security
Any qualified provider which is offered a Service Level Agreement (SLA) to deliver checks must sign up to NHS County Durham’s Quality Assurance programme to insure they do the following:-
• Accurately follow the QA of all testing equipment • Attend refresher training and clinical supervision • Sign up to their waste management protocol • Have necessary monitoring and audit processes in place • Have GPs trust that the data is accurate
In addition to assuring that all testing equipment and health professionals meet the necessary standards, a quality thread runs right throughout every aspect of Health Diagnostics’ delivery model. From the back office support – rated “excellent” by the majority of users – to the accredited training of those delivering the checks, the quality of each element is crucial to the overall standard of the service. See the diagram overleaf for a visual depiction of how quality feeds into each step of the process.

NHS Health Checks Case Study:The North East of England
5
Case study A Picture Of Health The North East of England
Delivery
Provider set up
Back office
The issue of quality assurance was raised as a major challenge to the future of health check implementation in the BMJ article mentioned above, where it is stated, “A key challenge will be quality assurance, details of which are currently lacking.” In recognition of this, and to stay one step ahead, Health Diagnostics and the Bolton NHS Foundation Trust have worked collaboratively towards quality assurance, joining forces to design a scheme which can assure absolute quality in the standard of testing done by health check providers. Conducting quality assurance (QA) of testing analysers, such as those used to test cholesterol in the
Quality assurance within health check delivery
blood, is routine and compulsory for equipment used in pathology services. Bolton’s laboratory medicine service specialises in this field, as was recognised by an award won for ‘Efficiency in Clinical Support Services’ at the 2012 Health Service Journal awards. When it comes to NHS Health Checks, to date, no governing body has put in place mandatory standards to ensure cholesterol analysers are routinely checked to be performing correctly. Health Diagnostics, however, has always insisted that providers using such systems regularly confirm that their procedures are checked for accuracy and reliability.
The Quality Framework
Stringent QA scheme for point care equipment. Health Diagnostics partner with award winning Royal Bolton Trust
Health Diagnostics is ISO27001 accredited and software is CE marked Patient focused software that is rated ‘excellent’ by the majority of users
Support services rated as ‘excellent’ by the majority of users
Registered with the ICO and CfH
Approved and patient-focussed CVD risk assessment tool
All deliverers undergo accredited training
Informative and comprehensive client reports
Electronic transfer of data to any GP clinical system
Close monitoring of sites and performance
Thorough follow up on QA results
Data

NHS Health Checks Case Study:The North East of England
6
Case study A Picture Of Health The North East of England
In the spring of 2011, the first six months of a pilot GP-based NHS Health Check Point of Care Testing (POCT) was held across South of Tyne and Wear (SOTW), led by Sue Collins, South Tyneside’s Health Engagement Lead. NHS South of Tyne and Wear is an expansive region, serving Gateshead, South Tyneside and Sunderland Teaching PCT. The pilot proved highly successful with GPs, and since then the number of GP practices offering the checks has risen exponentially. In 2011, 34% of practices in Gateshead and 26% in South Tyneside were delivering checks and 30% in Sunderland, whereas in 2012, 67% of practises in Gateshead offered checks, 72% in South Tyneside and 54% in Sunderland.
The annual report for SOTW published the following results about individuals who were checked:-
• 3,617 health checks completed in total • 27% (n=976) of individuals were classed as ‘high risk’ • 34% (n=1,234) of individuals were classed as ‘moderate risk’ • 39% (n=1,403) of individuals were classed as ‘low risk’ • 70% (n=2,526) of patients experienced the check as a ‘one stop shop’ • 1,820 questionnaires were received: A 50% response rate
In August 2012, an on-street survey with 601 individuals was conducted to identify and interview those who had been checked and those who had not. (Those who had been checked are referred to as ‘patients’ and those who had not as ‘non-patients’.) 48% of respondents had experienced a NHS Health Check. The illustrations opposite indicates what they said they had received advice about (based on 281 responses). 45% of patients reported they had followed ‘all or some’ of the advice. Interestingly, only 6% of those who had been given advice on smoking cessation reported they had not followed the advice.
Case study 1: NHS South of Tyne and Wear
In rating various elements of their experience of the NHS Health Check, patients on-street indicated high levels of satisfaction. Patients were asked to indicate how likely they would be to recommend the NHS Health Check to a friend or relative using a Net Promoter Score Question:
Patient experience
Using a scale where 0 is ‘Not at all likely’ and 10 is ‘Very likely,’ how likely would you be to recommend a friend or relative to have a NHS Health Check?
Detractors (scores 0 – 6) Passives (scores 7 – 8) Promoters (scores 9 – 10)
This is extremely high for an NPS score, indicating that word of mouth and recommendations from family and friends who have a NHS Health Check could be powerful if utilised effectively.

NHS Health Checks Case Study:The North East of England
7
Case study A Picture Of Health The North East of England
Why patients refuse health checksNon-PatientsIn line with sample quotas, 52% of respondents had not experienced a NHS Health Check. Respondents were asked to indicate their propensity to have an NHS Health Check, after a description was given outlining what it involved and how it is carried out:
69% indicated they were ‘quite likely’ or ‘very likely’ to have a check.
19% stated that they had been invited to have a health check by the GP, of these there were three main reasons they had not had the NHS Health Check:
• 28% forgot • 20% were too busy • 16% did not feel they needed to have it done because they felt healthy
How to attract reluctant patients for health checksNon-patients were asked to identify from a prompted list which approach would most likely encourage them to book a health check and which venue they would prefer to go to for the check.
Benefits of health checks at point of careSue Collins points, “POCT testing in general is beneficial because it can support somebody to change their behaviour. But the further away a person is from their actual results, for instance if results are given over the phone or via letter, the less likely they are to take advice because it’s easier to ignore. Conversely, one-stop-shop testing enables support or advice to be gained instantly by a nurse or other healthcare provider.” This motivational aspect came out in the county’s patient feedback evaluation, with some quotes provided below:-
• “It’s great; you get the results straight away” • “Gives you the chance to put things right” • “I’ve got a family history so was able to discuss my worries”
Practical recommendationsHealth Diagnostics worked with Sue Collins at NHS SOTW as the health check service provider, enabling consistent, monthly data collection. Sue explains, “Health Diagnostics’s software, Health Options, is commented upon by all parties, including patients, nurses, and so on because it is very user-friendly. It naturally leads the user through the process, and is very visual - which helps in explaining things. When we were rolling out the POCT, we wondered how to get nurses up and running, so I created a half day course in conjunction with Health Diagnostics. There was no way I could train everyone myself, so they helped me with the bespoke nurse training.”
Sue recommends the following:-“Don’t underestimate the time it takes to set up a project; good planning and lead-in time are essential for smooth implementation. Appropriate training, updates and quality control are essential for accurate near-patient cholesterol results. It is essential to give practise staff enough time to deliver the check in one appointment, and to perform quality checks.”
(7% stated ‘Other’)

NHS Health Checks Case Study:The North East of England
8
Case study A Picture Of Health The North East of England
NHS County Durham has taken a long-term, pragmatic view in terms of health prevention, and started delivering health checks in 2009 via general practice to help reach its targets of closing the ‘gap in health inequalities by 0.4 years’ and adding ‘1.5 years to life expectancy by 2013.’
However, not long afterwards, the county’s heads of public health found that uptake varied markedly in terms of patients’ age, gender and socio-economic profile. Dr Mike Lavender, a Consultant in public health medicine at NHS County Durham, explained, ‘‘There was a huge variation in terms of health checks being delivered by GP practices, so we knew we had to do something in the communities which the practices weren’t reaching. That was the first step. We also saw that men and women in the younger age-groups (40s to mid 50s) really weren’t going in for the health check. This isn’t particularly surprising for that age group, as they may not see heart disease as particularly being a problem. They may be working, they can’t get time off etcetera, so the community programme was aimed at that younger adult population.’’
Case Study 2: Durham - Mini-Health Mots: predict and prevent by ‘Catching Them Young’
The response came in 2011 when a community programme was piloted which targeted the younger populations by offering a ‘Mini Health MOT’ to those aged 16 to 40. Dr Lavender explains that by broadening the age bracket, “You’re accessing people at the teachable moment, as well as maximising all the effort and investment that has gone into training the staff who deliver the service.” The pilot used Health Diagnostics’ services and support, and the pilot’s success meant it moved into its second year in 2012, having secured the following outcomes between April 2011 and March 2012:-
• 3378 people accessed a Mini Health MOT. • 483 clients were eligible for an NHS Health Check. • 418 clients in total were signposted to lifestyle intervention services, including 113 to physical activity, 64 to local stop smoking services, 183 to the health trainer team and 58 to healthy cooking courses.
The decision to offer Mini Health MOTs happened to tie in well with freshly-voiced concerns from Diabetes UK about the need to screen between the ages of 25 and 40 for diabetes amongst people of Asian, African and Caribbean descent, due to their higher risk compared to Europeans.
In addition to the Mini Health MOTs, Durham’s health leads decided to target residents who weren’t engaging or accessing traditional NHS services, so in April 2011, they implemented the Check4Life project which was headed up by health improvement lead, Jacqui Deakin. Deakin describes the project as, “A non-medical lifestyle intervention to promote heart health and reduce the risk and prevalence of cardiovascular disease in disadvantaged communities.” Check4Life involved events where individuals were given a ten to fifteen minute health assessment, including measuring waist circumference, BMI calculation, blood pressure check, and asking some health-related questions.
The ‘look and feel’ of the events mimicked the government’s widely advertised Change4Life campaign by adopting similar branding, and taking advantage of familiar touch points, such as the general need to be more active and eat healthily. Deakin explains, “We incorporated many of the marketing themes of the national Change4Life campaign into our Check4Life promotion... to take advantage of its recognisable brand which was already embedded in people’s awareness.”
Check4life: Using familiar ‘Touch Points’

NHS Health Checks Case Study:The North East of England
9
Case study A Picture Of Health The North East of England
Health Diagnostics’s Health Options software enables branding of printed reports for patients using any logo or digital artwork provided.
In order to target areas within the county’s top 30 per cent deprivation percentile, NHS County Durham’s Check4Life road shows and community events are held in areas of high footfall, such as town centres and supermarkets, following liaison with local ambassadors and volunteers to establish busy areas which are also those most in need of help. Jacqui explains: “We’ve learnt a huge amount in terms of what a potential setting needs to have for a successful C4L Road show venue - for example, adequate car parking.” Evidence from Durham suggests that in order to boost uptake, lifestyle health checks should be available at local community venues during fixed times each week, in addition to sporadic, one-off events held at, for example, Durham cricket club.
Make it accessible, make it regular
Coordinate with local counties
Several stakeholders in the health check arena have pointed out the need for a bigger, more ambitious and integrated approach to health checks, with better coordination between GPs, practice nurses and practice managers. In recognition of this, NHS County Durham has gone as far as to operate as a single PCT with its neighbouring county, Darlington. Dr Lavender explains: “We work closely across the North East, from Northumberland down to Tees Valley, and we meet regularly. There have been discussions conducted on behalf of the LAs to establish a single agreement to which we can all work. This would be much easier to manage.” The success of such a cross-border approach was further assisted by the fact both counties’ used Health Diagnostics’s services for software and consultancy in health screening.

NHS Health Checks Case Study:The North East of England
10
Case study A Picture Of Health The North East of England
A key idea behind commissioning health checks, from the outset, was to put patients at the centre. By extension, patient data must be put to the best possible use if outcomes are to be optimised: Whilst the long-term monetary pay back from health checks is hard to predict, what is useful in the short term is knowing if or how an individual signposted for behaviour modification is progressing. With this in mind, the health improvement team at NHS County Durham approached Health Diagnostics and asked if the organisation could build into their software a way of capturing the outcomes from the additional services the team provide; a way of tracking the outcomes of its weight loss, exercise, smoking cessation programmes, and so on.
The majority of the programmes run by the Health Improvement team are 12 weeks long: A significant investment. One way in which teams monitor change in individuals is through progress trackers. The Health Improvement team wanted these progress trackers ‘computerising’ in order to ‘close the loop’ by recording the outcome data in one central location. So, Health Diagnostics developed its Health Options functionality to incorporate the existing questionnaires and trackers used by the team.
This feature is now available to all PCTs and providers, allowing those running programmes to determine, for example, whether or not someone identified as ‘obese’ during a heath check went on to attend and complete the recommended weight-loss programme they were signposted to.
This functionality allows PCTs to measure and evaluate the outcomes of the programmes they’re running accurately, as well as truly integrating the care pathways they’ve established for their local populations. The same will be true for local authorities when they take over in April.
Putting patients at the centre and measuring their success
Below is an example of a spreadsheet into which all of the recorded data is fed. From this, the effectiveness of the programmes can be readily gauged and the outcomes measured. Such information on the numbers of individuals completing the follow up phone calls and subsequently altering their behaviour is an invaluable - yet not widely available - function to date.

NHS Health Checks Case Study:The North East of England
11
Case study A Picture Of Health The North East of England
It needn’t be expensive
A flexible mind-set and back office reap rewards
Pressures upon health care resources are under unprecedented pressure, however, Jacqui Deakin points out that, “As part of the QIPP* agenda, NHS County Durham was required to generate £300,000 worth of productivity and performance – without any extra money at all. We therefore had to extensively review and reshape our service in order to achieve these targets – all of which we have done.” Local Authorities have been promised funding equivalent to that of PCTs’ expenditure for health checks. However, as concerns still exist about affordability, it has been widely suggested that local authorities should maximise use of existing providers to maintain quality of provision.*Quality, Innovation, Prevention, Productivity
Pharmacy is a key provider of NHS Health Checks in the North East, as elsewhere in England, though there are big differences in provision within and between regions. Strong support from providers such as Health Diagnostics can be key to helping pharmacists’ day-to-day experience of providing checks. It can also help prevent laborious tasks and save time. Julie Evason, CEO of Health Diagnostics explains: “We are very quick to adapt when clients want new features from our service. For instance, Richmond PCT pointed out they were having to ask pharmacists to manually fill out a specific form with health check data and send the forms off to health trainers. So, they asked us if we could remove this need by inserting the form into our software, which would be automatically populated. Durham wanted to track the data from the activity programmes, so we introduced generic changes to the software so that all other providers could benefit from the new feature. It’s about having a flexible mind-set.”
In a similar vein, Jacqui Deakin has praised the‘back office’ facility provided by Health Diagnostics:“The support they’ve given us has been absolutely fantastic. We wouldn’t have been able to do the work we’ve done without the support of their team.”
0
10
20
30
40
40 - 49 50 - 59 60 - 69 70 - 74
50
60
70
80
Low, CVD <10%
Med, CVD 10% - 19.9%
Low, CVD >=20%
0
50
100
40 - 49 50 - 59 60 - 69 70 - 74
150
250
200
Low, CVD <10%
Med, CVD 10% - 19.9%
Low, CVD >=20%
0
10
20
30
40
40 - 49 50 - 59 60 - 69 70 - 74
50
60
70
80
Low, CVD <10%
Med, CVD 10% - 19.9%
Low, CVD >=20%
0
50
100
40 - 49 50 - 59 60 - 69 70 - 74
150
250
200
Low, CVD <10%
Med, CVD 10% - 19.9%
Low, CVD >=20%
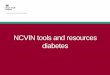
Male CVD Risk by Age to date: Jul 2009 - Jun 2012
Female CVD Risk by Age to date: Jul 2009 - Jun 2012
Charts show findings from the three years pharmacies have been conducting NHS Health Checks tests in County Durham

NHS Health Checks Case Study:The North East of England
12
Case study A Picture Of Health The North East of England
Train up staff
Health checks within Pharmacy: how to do them betterAlthough some PCTs have recently decommissioned certain services from pharmacy, the NHS Commissioning Board has published figures suggesting pharmacy as a potentially invaluable place through which to engage the public on health issues, and points out that, “1.2 million people visit a community pharmacy every day.4”
Dawn Cruickshank is Superintendant Pharmacist at County Durham’s pharmacy chain, John Low Limited, responsible for one of the PCT’s highest performing pharmacies in terms of the number of NHS Health Checks delivered. John Low delivered 406 checks between July 2009 and September 2012, and referred 71 high risk individuals to their GP. By way of comparison, one of the poorer performing pharmacies in the area in terms of health check provision had conducted just 16 tests during the same period. This gulf in performance is symptomatic of the varying levels that exist across the UK when it comes to conducting NHS Health Checks.
Be proactiveThe John Low team’s success has centred on a proactive approach towards getting high-risk individuals tested for cardiovascular disease. Its actions have included working with local counsellors on directing mail shots to people living in areas of high deprivation, to ensuring that everyone who works in the pharmacy is ‘clued up’. Dawn Cruickshank explains: “Whenever we do accuracy checks on our prescriptions, at the same time we look to see if the patient is eligible for a health check. If they’re within the age bracket and not taking any medicines which would make them ineligible, we’ll include a health check leaflet with their prescription. All the girls on the counter are really geared up and enthusiastic about recruiting anyone eligible who comes into the pharmacy.”
There are four members of staff at John Low Ltd who are trained to deliver the NHS Health Checks. “It’s crucial to have more than one individual that you’re relying on to be able to do the tests - partly to accommodate for holidays and sickness, but also because success requires a team approach.” Dawn ensures targets for recruiting people for health checks are included in staff development reviews: “This has meant that they’re all quite focussed on it.”
Educate the youngThe pharmacy has identified a major difference in the type of people being tested in the pharmacy compared to those being tested by GPs: “Initially, GP’s were targeting the higher age ranges because those were the people who were likely to have higher absolute risk. A lot of the people that we’re getting through the door however are of younger age ranges. Despite people in this demographic having a lower absolute risk, a lot of the time when you look at the relative risk, they’re number one in the queue to develop cardiovascular disease. [This represents a] fantastic preventative aspect to the tool, because you’re getting people at the ‘reachable’ moment. The customers are able to see from the very visual Health Options software how their lifestyle could impact their future health.... It’s a change in mind set from just dealing with prescriptions, to bearing in mind everything that might be available for a patient. The service makes economic sense, and it can be really rewarding to hear clients who’ve taken the lifestyle pathway come back, saying ‘I’ve given up smoking!’ or ‘I’ve lost two stone!’”

NHS Health Checks Case Study:The North East of England
13
Case study A Picture Of Health The North East of England
Successful outcomes from NHS Health Checks are difficult to quantify, because they are, by nature, a long-term method of reducing health inequality. Without a doubt, by focussing on prevention rather than cure, a health check can enable those who may otherwise not access healthcare services the chance to do so. However, there has been a fair amount of criticism aimed at the NHS Health Checks programme recently, which has focussed on various issues, including the challenge of insuring quality assurance, and communication between providers of the checks and primary care.
The case study above demonstrates how certain providers are ‘ahead of the game’, having factored in these challenges already. The example of the North East proves that successful programmes require clued-up and enthusiastic leadership. Understanding localities and the
Conclusion: where there’s a will, good support, and joined up thinking - there’s a way
demographics of communities served is key to engaging the individual - regardless of the location of the health check. Be it via a person’s GP or local pharmacy it is front line staff, explains Dr Lavender, who “know the local culture, language and attitude, so are in a good position to animate the service.”
Julie Evason, CEO of Health Diagnostics, adds, “No PCT project is the same. All have their nuances, but many of our clients are surprised at the effort we’ll put into their specific projects, which they see as a major offering. We provide a very personalised service which draws on 28 years’ experience in developing this kind of programme, ten of which have been with Health Diagnostics. Since NHS Health Checks were introduced 4 years ago, we’ve felt well-placed to see our clients through forthcoming changes and challenges ahead.”

NHS Health Checks Case Study:The North East of England
14
Case study A Picture Of Health The North East of England
A Picture Of Health
NHS Health Checks Case Study:The North East of England
References
1. Department of Health Putting prevention first – vascular checks:
risk assessment and management, 2008
2. BMJ Unanswered questions over NHS health checks http://www.
bmj.com/content/342/bmj.c6312
3. QOF Plus Towards world class healthcare for all, 2010.
4. Securing Excellence in Commissioning Primary Care June 2012