Embed Size (px)
Citation preview
1
NHS England – 10 Year Strategy Why we urgently need a fresh approach to catalyse the adoption of high-value new models of care
NHS System Transformation :
Design & Delivery VA
vision2action
Prof. Robert Harris Director of Strategy NHS England
85
90
95
100
105
110
115
120
125
130
135
140
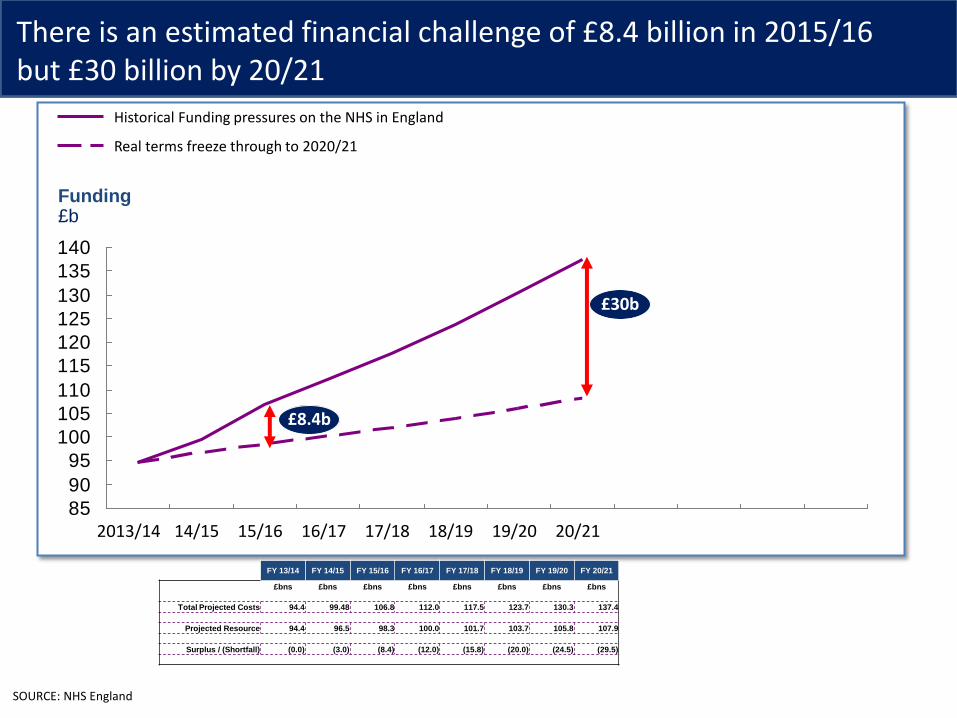
Funding £b
£8.4b
£30b
20/21 19/20 18/19 17/18 16/17 15/16 14/15 2013/14
Real terms freeze through to 2020/21
Historical Funding pressures on the NHS in England
SOURCE: NHS England
FY 13/14 FY 14/15 FY 15/16 FY 16/17 FY 17/18 FY 18/19 FY 19/20 FY 20/21
£bns £bns £bns £bns £bns £bns £bns £bns
Total Projected Costs 94.4 99.48 106.8 112.0 117.5 123.7 130.3 137.4
Projected Resource 94.4 96.5 98.3 100.0 101.7 103.7 105.8 107.9
Surplus / (Shortfall) (0.0) (3.0) (8.4) (12.0) (15.8) (20.0) (24.5) (29.5)
There is an estimated financial challenge of £8.4 billion in 2015/16 but £30 billion by 20/21
3
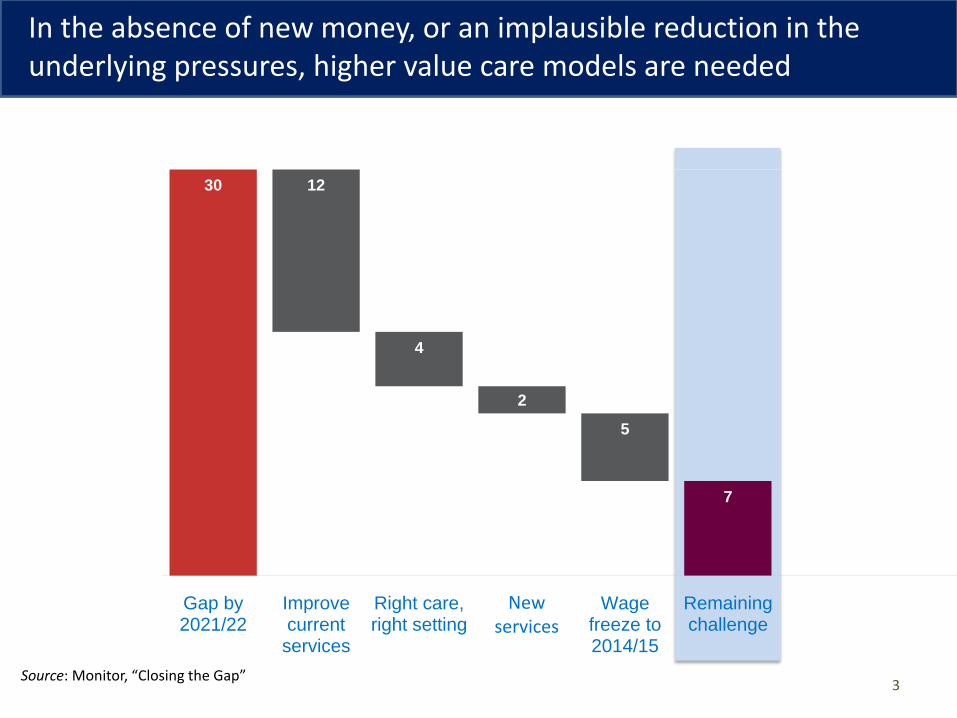
30 12
4
2
5
7
Gap by2021/22
Improvecurrentservices
Right care,right setting
Innovatenew
services
Wagefreeze to2014/15
Remainingchallenge
New services
Source: Monitor, “Closing the Gap”
In the absence of new money, or an implausible reduction in the underlying pressures, higher value care models are needed
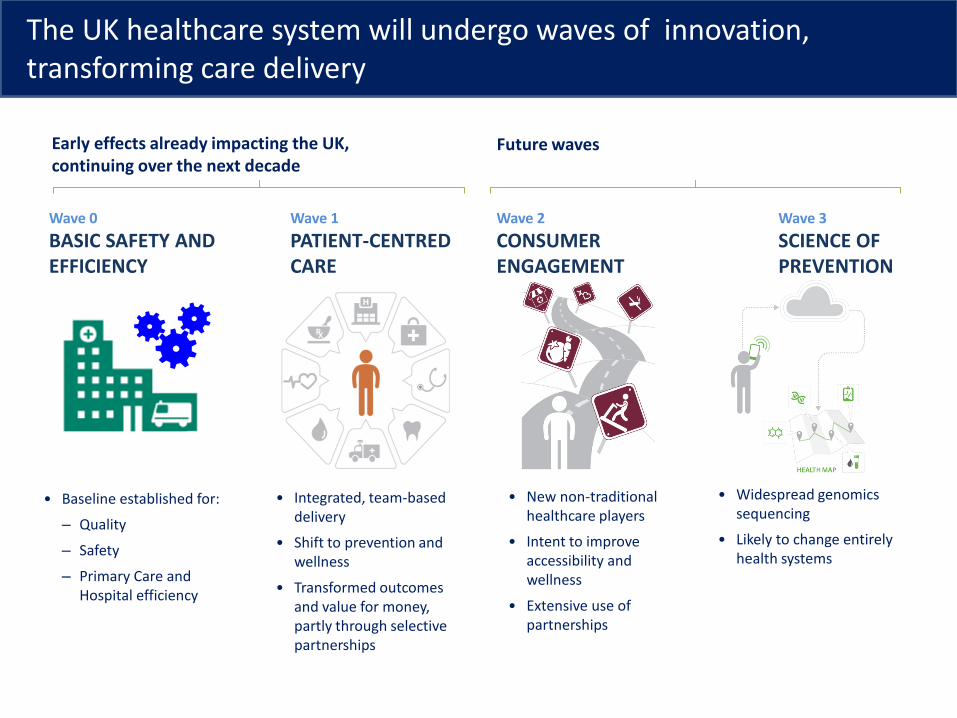
• Integrated, team-based delivery
• Shift to prevention and wellness
• Transformed outcomes and value for money, partly through selective partnerships
• New non-traditional healthcare players
• Intent to improve accessibility and wellness
• Extensive use of partnerships
• Widespread genomics sequencing
• Likely to change entirely health systems
• Baseline established for:
– Quality
– Safety
– Primary Care and Hospital efficiency
Wave 0
BASIC SAFETY AND EFFICIENCY
Wave 1
PATIENT-CENTRED CARE
Wave 2
CONSUMER ENGAGEMENT
Wave 3
SCIENCE OF PREVENTION
Early effects already impacting the UK, continuing over the next decade
Future waves
The UK healthcare system will undergo waves of innovation, transforming care delivery
Examples of WHAT type of value system players could release
▪ Acute productivity gain ▪ Integrated care gain ▪ Shift to most efficient care setting ▪ Reduced input costs ▪ Promote self management ▪ Invest heavily in prevention
Examples of HOW NHS England can help the system create value
▪ Create the right £ incentives ▪ Free up managerial capacity by
reducing bureaucratic burden ▪ Build capability to implement
change ▪ Ensure the right organisational
structure ▪ Flex rules
NHS England needs to focus on system levers it can use to drive change
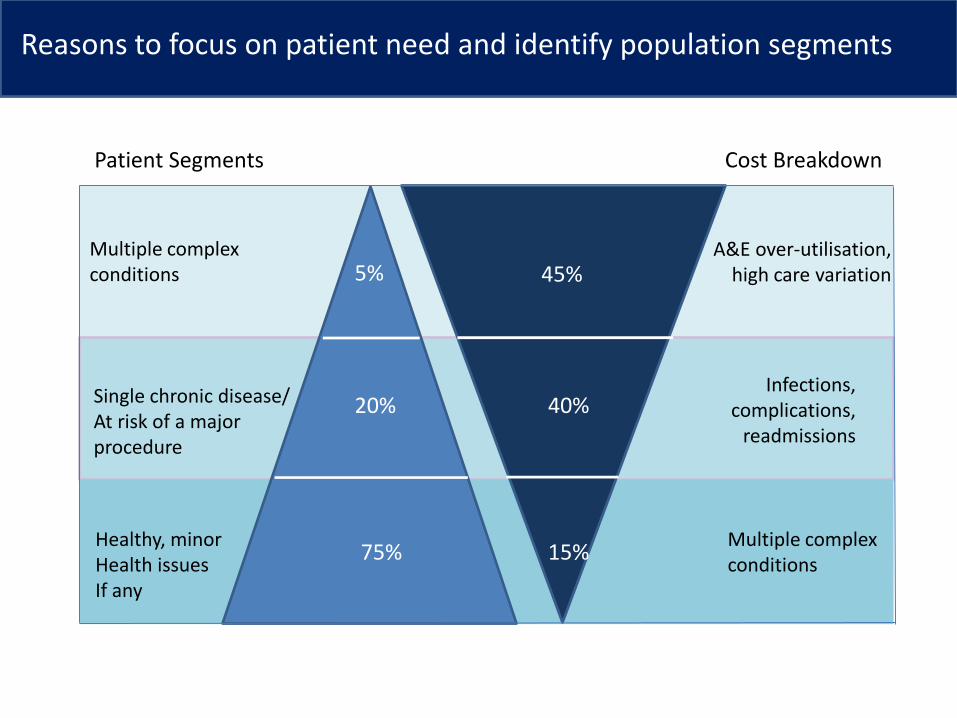
5% 45%
20% 40%
75% 15%
Multiple complex conditions
Single chronic disease/ At risk of a major procedure
Healthy, minor Health issues If any
A&E over-utilisation, high care variation
Infections, complications,
readmissions
Multiple complex conditions
Patient Segments Cost Breakdown
Reasons to focus on patient need and identify population segments
SOURCE: FIMS 2010/11; NHS programme budgets 2010/11; Laing & Buisson
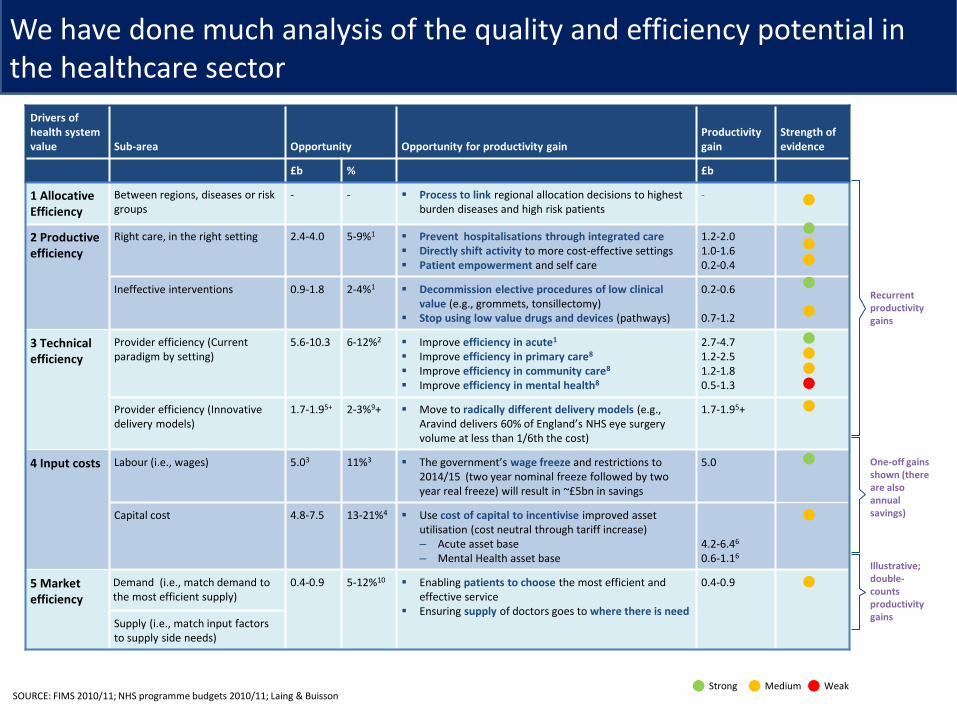
Drivers of health system value Sub-area Opportunity Opportunity for productivity gain
Productivity gain
Strength of evidence
£b % £b
1 Allocative Efficiency
Between regions, diseases or risk groups
- - Process to link regional allocation decisions to highest burden diseases and high risk patients
-
2 Productive efficiency
Right care, in the right setting 2.4-4.0 5-9%1 Prevent hospitalisations through integrated care Directly shift activity to more cost-effective settings Patient empowerment and self care
1.2-2.0 1.0-1.6 0.2-0.4
Ineffective interventions 0.9-1.8 2-4%1 Decommission elective procedures of low clinical
value (e.g., grommets, tonsillectomy) Stop using low value drugs and devices (pathways)
0.2-0.6 0.7-1.2
3 Technical efficiency
Provider efficiency (Current paradigm by setting)
5.6-10.3 6-12%2 Improve efficiency in acute1
Improve efficiency in primary care8
Improve efficiency in community care8
Improve efficiency in mental health8
2.7-4.7 1.2-2.5 1.2-1.8 0.5-1.3
Provider efficiency (Innovative delivery models)
1.7-1.95+ 2-3%9+ Move to radically different delivery models (e.g.,
Aravind delivers 60% of England’s NHS eye surgery volume at less than 1/6th the cost)
1.7-1.95+
4 Input costs Labour (i.e., wages) 5.03 11%3 The government’s wage freeze and restrictions to
2014/15 (two year nominal freeze followed by two year real freeze) will result in ~£5bn in savings
5.0
Capital cost 4.8-7.5 13-21%4 Use cost of capital to incentivise improved asset
utilisation (cost neutral through tariff increase) – Acute asset base – Mental Health asset base
4.2-6.46
0.6-1.16
5 Market efficiency
Demand (i.e., match demand to the most efficient supply)
0.4-0.9 5-12%10 Enabling patients to choose the most efficient and
effective service Ensuring supply of doctors goes to where there is need
0.4-0.9
Supply (i.e., match input factors to supply side needs)
One-off gains shown (there are also annual savings)
Illustrative; double- counts productivity gains
Recurrent productivity gains
Strong Medium Weak
We have done much analysis of the quality and efficiency potential in the healthcare sector
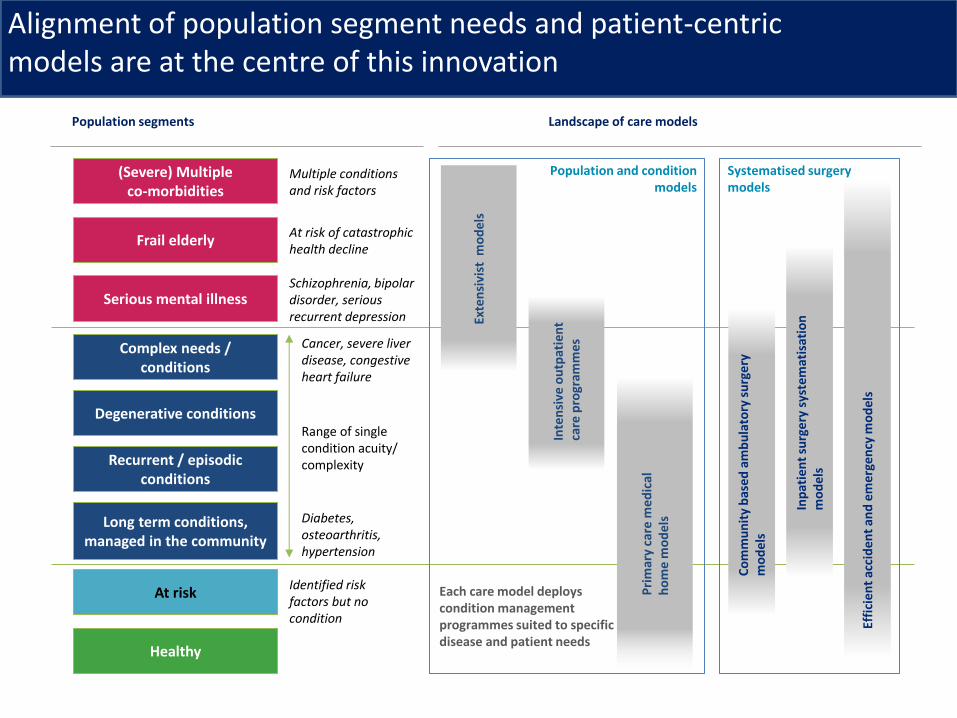
Population segments Landscape of care models
Exte
nsi
vist
mo
del
s
Inte
nsi
ve o
utp
atie
nt
care
pro
gram
mes
Pri
mar
y ca
re m
ed
ical
h
om
e m
od
els
Systematised surgery models
Co
mm
un
ity
bas
ed a
mb
ula
tory
su
rge
ry
mo
del
s
Inp
atie
nt
surg
ery
sys
tem
atis
atio
n
mo
del
s
Effi
cie
nt
acci
den
t an
d e
me
rge
ncy
mo
del
s
Population and condition models
Each care model deploys condition management programmes suited to specific disease and patient needs
Complex needs / conditions
Recurrent / episodic conditions
Long term conditions, managed in the community
Degenerative conditions
(Severe) Multiple co-morbidities
Frail elderly
At risk
Healthy
Serious mental illness
Cancer, severe liver disease, congestive heart failure
Multiple conditions and risk factors
Schizophrenia, bipolar disorder, serious recurrent depression
At risk of catastrophic health decline
Diabetes, osteoarthritis, hypertension
Range of single condition acuity/ complexity
Identified risk factors but no condition
Alignment of population segment needs and patient-centric models are at the centre of this innovation
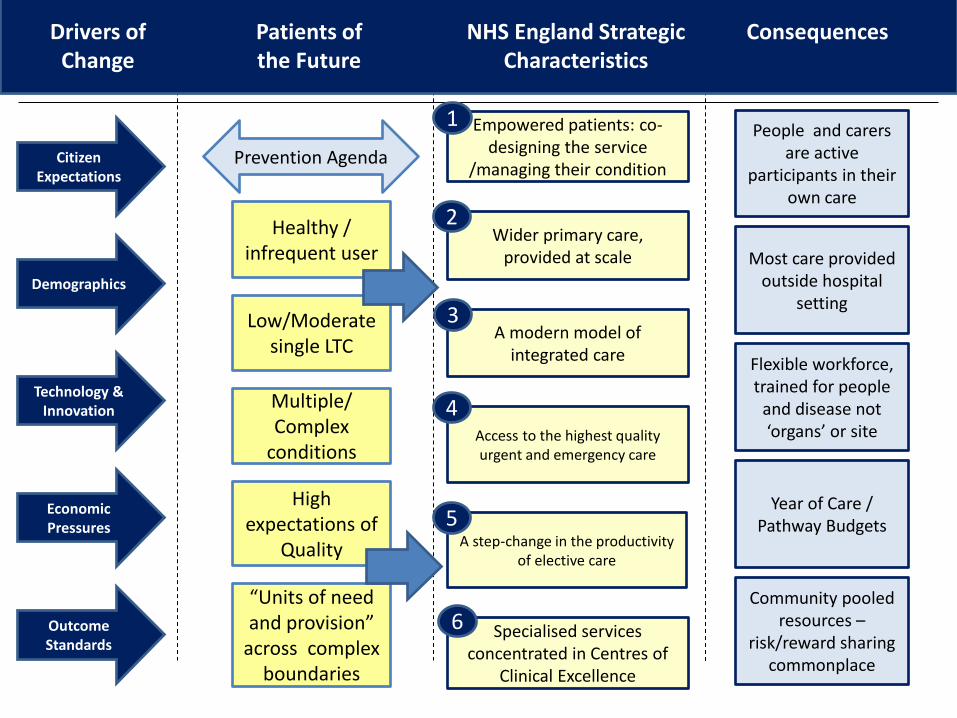
Prevention Agenda
Low/Moderate single LTC
High expectations of
Quality
“Units of need and provision”
across complex boundaries
Empowered patients: co-designing the service
/managing their condition
Wider primary care, provided at scale
A modern model of integrated care
Access to the highest quality urgent and emergency care
A step-change in the productivity of elective care
Outcome Standards
Economic Pressures
Technology & Innovation
Demographics
Citizen Expectations
Specialised services concentrated in Centres of
Clinical Excellence
Healthy / infrequent user
Multiple/ Complex
conditions
1
2
3
4
5
6
People and carers are active
participants in their own care
Most care provided outside hospital
setting
Flexible workforce, trained for people
and disease not ‘organs’ or site
Year of Care / Pathway Budgets
Community pooled resources –
risk/reward sharing commonplace
Drivers of Change
Patients of the Future
NHS England Strategic Characteristics
Consequences
10
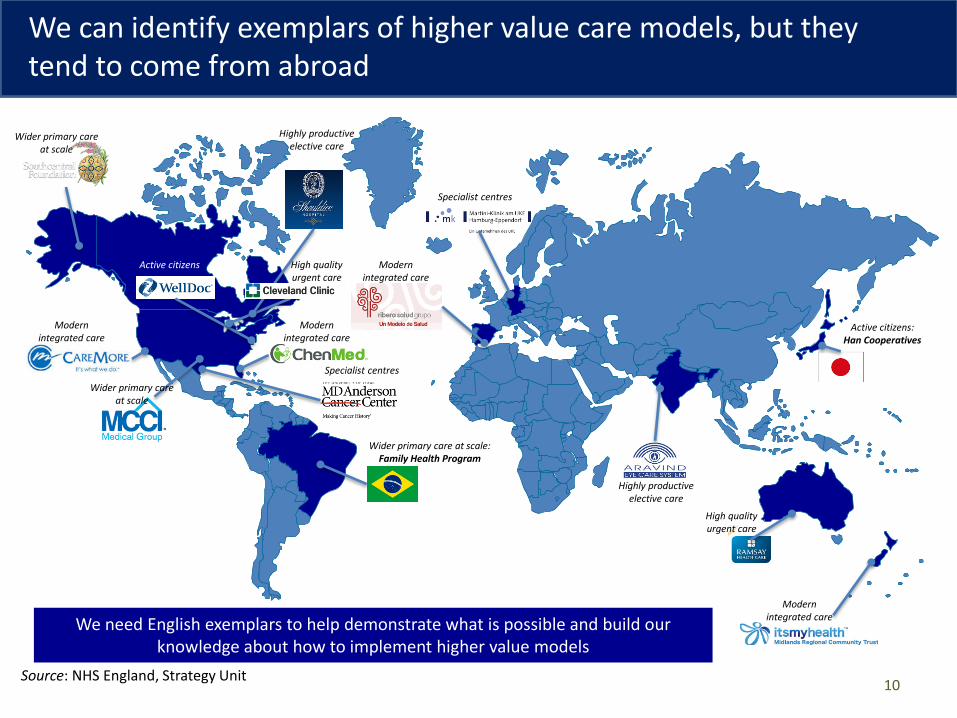
Modern integrated care
Modern integrated care
Wider primary care at scale
Modern integrated care
Active citizens: Han Cooperatives
Active citizens
Specialist centres
Specialist centres
High quality urgent care
Highly productive elective care
Wider primary care at scale
Wider primary care at scale: Family Health Program
Highly productive elective care
Modern integrated care
We need English exemplars to help demonstrate what is possible and build our knowledge about how to implement higher value models
High quality urgent care
Source: NHS England, Strategy Unit
We can identify exemplars of higher value care models, but they tend to come from abroad
11
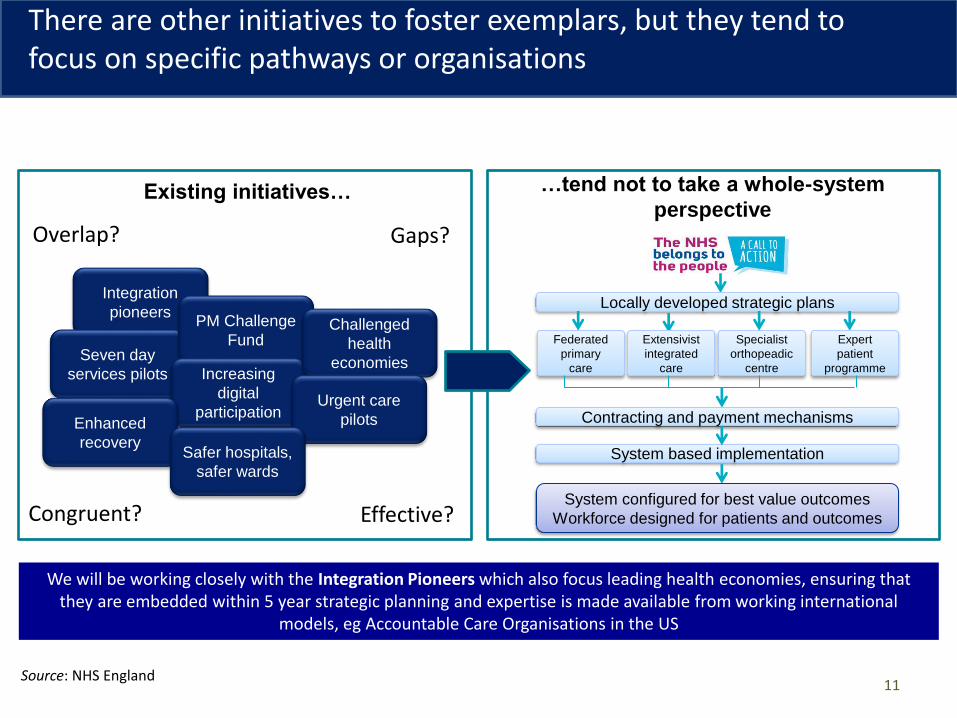
Locally developed strategic plans
Federated
primary
care
Extensivist
integrated
care
Specialist
orthopeadic
centre
Expert
patient
programme
Contracting and payment mechanisms
System based implementation
System configured for best value outcomes
Workforce designed for patients and outcomes
There are other initiatives to foster exemplars, but they tend to focus on specific pathways or organisations
Integration
pioneers
Seven day
services pilots
PM Challenge
Fund
Increasing
digital
participation
Challenged
health
economies
Urgent care
pilots
Existing initiatives… …tend not to take a whole-system
perspective
Enhanced
recovery Safer hospitals,
safer wards
We will be working closely with the Integration Pioneers which also focus leading health economies, ensuring that they are embedded within 5 year strategic planning and expertise is made available from working international
models, eg Accountable Care Organisations in the US
Overlap?
Congruent? Effective?
Gaps?
Source: NHS England
12
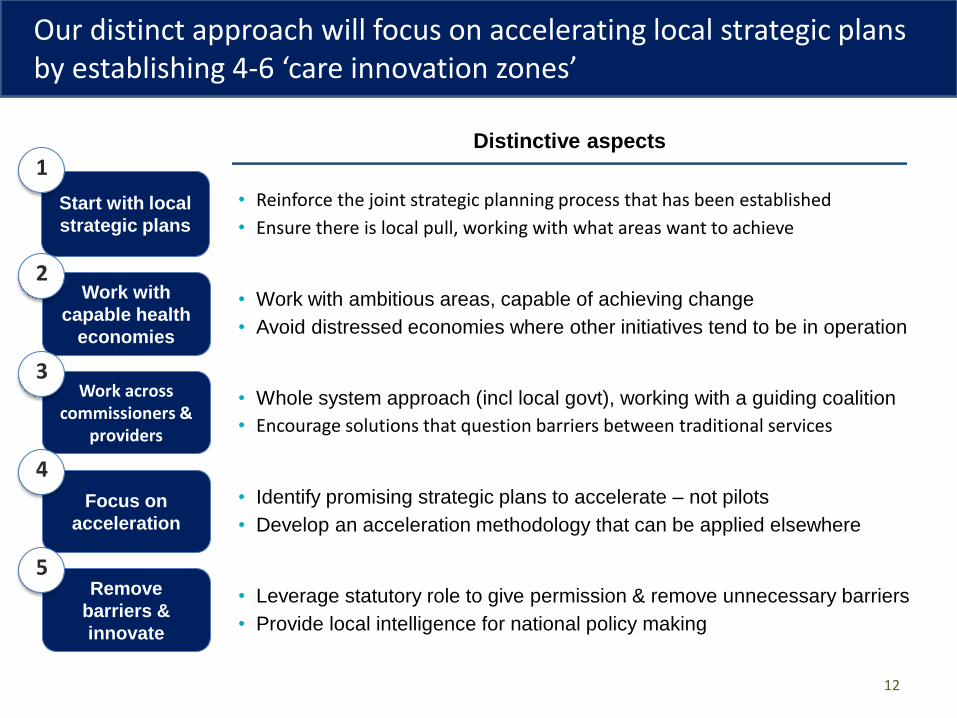
Start with local
strategic plans
Focus on
acceleration
Work with
capable health
economies
Work across commissioners &
providers
Distinctive aspects
Remove
barriers &
innovate
• Reinforce the joint strategic planning process that has been established
• Ensure there is local pull, working with what areas want to achieve
• Work with ambitious areas, capable of achieving change
• Avoid distressed economies where other initiatives tend to be in operation
• Whole system approach (incl local govt), working with a guiding coalition
• Encourage solutions that question barriers between traditional services
• Identify promising strategic plans to accelerate – not pilots
• Develop an acceleration methodology that can be applied elsewhere
• Leverage statutory role to give permission & remove unnecessary barriers
• Provide local intelligence for national policy making
1
2
3
4
5
Our distinct approach will focus on accelerating local strategic plans by establishing 4-6 ‘care innovation zones’
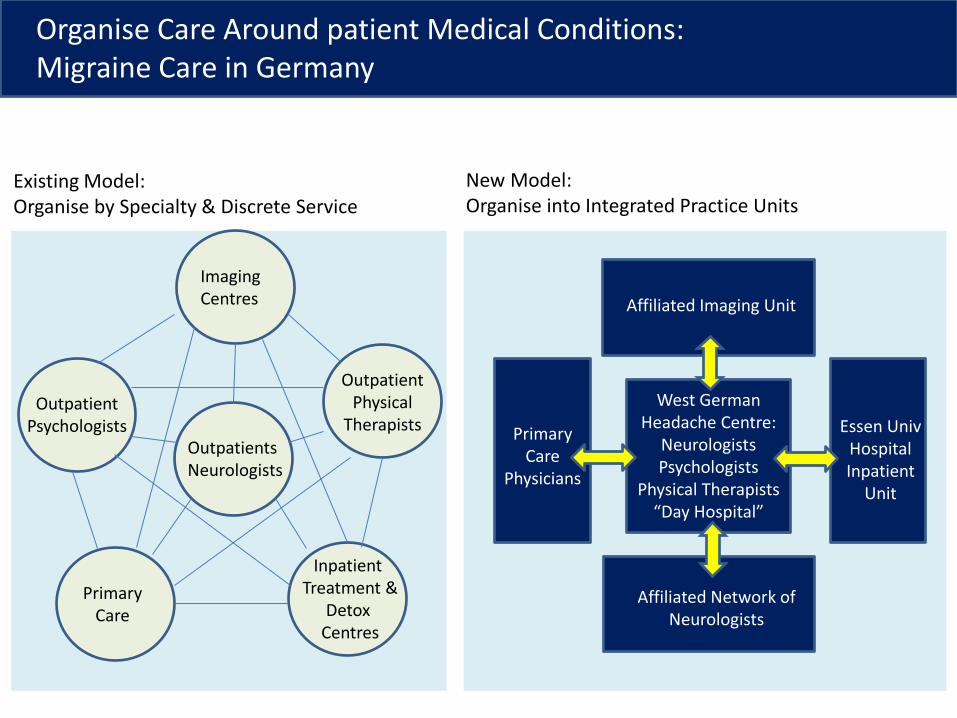
Outpatient Psychologists
Imaging Centres
Primary Care
Outpatients Neurologists
Inpatient Treatment &
Detox Centres
Outpatient Physical
Therapists
Existing Model: Organise by Specialty & Discrete Service
Affiliated Imaging Unit
West German Headache Centre:
Neurologists Psychologists
Physical Therapists “Day Hospital”
Affiliated Network of Neurologists
Primary Care
Physicians
Essen Univ Hospital Inpatient
Unit
New Model: Organise into Integrated Practice Units
Organise Care Around patient Medical Conditions: Migraine Care in Germany
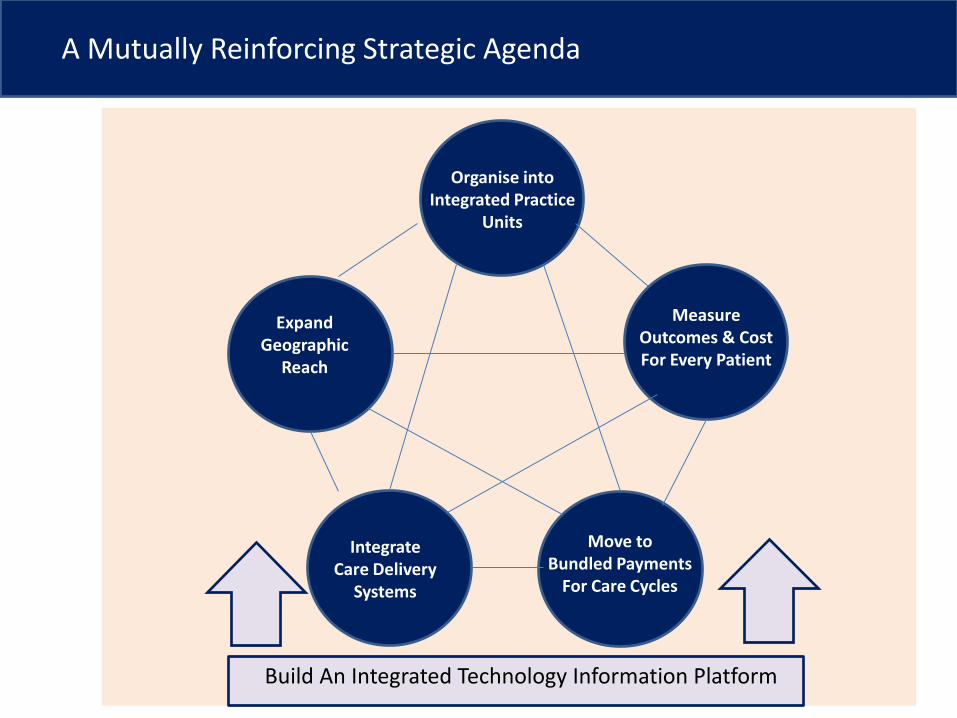
Expand Geographic
Reach
Organise into Integrated Practice
Units
Integrate Care Delivery
Systems
Move to Bundled Payments
For Care Cycles
Measure Outcomes & Cost For Every Patient
A Mutually Reinforcing Strategic Agenda
Build An Integrated Technology Information Platform
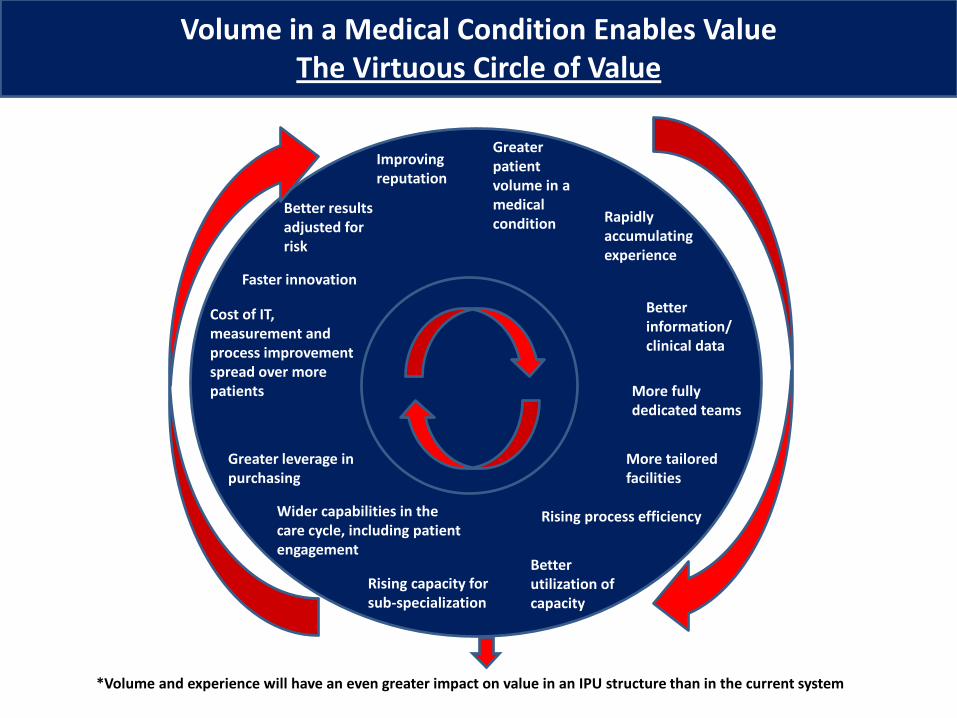
*Volume and experience will have an even greater impact on value in an IPU structure than in the current system
Better utilization of capacity
Rising capacity for sub-specialization
Better results adjusted for risk
Improving reputation
Greater patient volume in a medical condition Rapidly
accumulating experience
Better information/ clinical data
More fully dedicated teams
More tailored facilities
Rising process efficiency Wider capabilities in the care cycle, including patient engagement
Greater leverage in purchasing
Cost of IT, measurement and process improvement spread over more patients
Faster innovation
Volume in a Medical Condition Enables Value The Virtuous Circle of Value
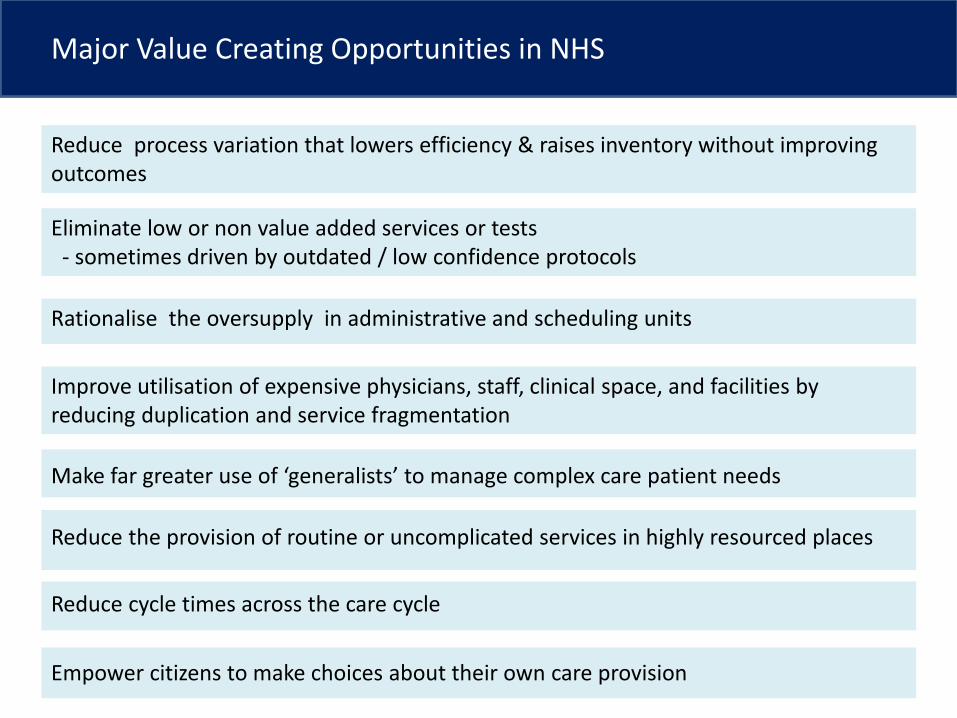
Major Value Creating Opportunities in NHS
Reduce process variation that lowers efficiency & raises inventory without improving outcomes
Eliminate low or non value added services or tests - sometimes driven by outdated / low confidence protocols
Rationalise the oversupply in administrative and scheduling units
Improve utilisation of expensive physicians, staff, clinical space, and facilities by reducing duplication and service fragmentation
Make far greater use of ‘generalists’ to manage complex care patient needs
Reduce the provision of routine or uncomplicated services in highly resourced places
Reduce cycle times across the care cycle
Empower citizens to make choices about their own care provision





























