Embed Size (px)
Citation preview
NHS DUMFRIES AND GALLOWAY
PRIMARY CARE GUIDELINE FOR THE
MANAGEMENT OF PATIENTS ON
WARFARIN
Author Gordon Loughran, Prescribing Support Pharmacist, on behalf of
NHS Dumfries & Galloway’s Patient Safety in Primary Care Group
Publication date July 2013
Review date July 2015
CONTENTS
Page
Introduction 1
Initiating warfarin 2
Contra-indications and special considerations 4
Patient education 5
Indications, target INRs and duration of treatment 6
Starting regimens 7
Maximum INR testing recall periods in maintenance therapy 10
Dose adjustments in maintenance therapy 11
Management of bleeding 13
Interactions with warfarin 15
Appendix 1 – Quick reference guide 24
References 26
1
INTRODUCTION
These guidelines have been developed by NHS Dumfries & Galloway’s
Patient Safety in Primary Care Group in conjunction with Dumfries & Galloway
Royal Infirmary’s Haematology Department. The aim is to ensure a safe,
effective and reliable approach to the management of adult patients in
Primary Care receiving treatment with warfarin. The prescribing information
contained within these guidelines is issued on the understanding that it is
considered to represent the best practice from available evidence and
national guidelines at the time of issue.
The guidelines offer advice to healthcare professionals on issues that must be
considered both prior to starting treatment and on an ongoing basis
throughout treatment. They also offer advice on how to initiate warfarin, the
regularity of INR checks, how to adjust doses, how to manage bleeding whilst
on warfarin, how to take account of interacting drugs and what education
should be provided to patients upon starting treatment and during it.
A quick reference guide containing key information has been prepared and
healthcare professionals may find this useful when needing to quickly access
the information they will most commonly need.
The guideline will be reviewed and updated on an ongoing basis taking into
account any changes in national guidance and evidence base. An
important point to note is that the guideline does not address the use of
newer anticoagulants such as dabigatran, rivaroxaban and apixaban since
its aim, as stated previously, is to ensure the safe, effective and reliable
management of patients on warfarin.
2
Initiating warfarin
The following good practice points are taken from SIGN Guideline 129 –
Antithrombotics: Indications and management:-
• After clinical assessment has demonstrated an indication for oral
anticoagulant treatment, the patient’s medical history, drug history,
and compliance with medication should be assessed
• The indication for oral anticoagulants, the appropriate target
therapeutic range of the INR, and the proposed duration of treatment
should be recorded in the case records, along with other medications
• A baseline blood sample should be obtained prior to starting warfarin
to assess FBC, LFTs, U &Es, APTT/PT and CrCl. This may
showcontraindications or risk factors for bleeding, such as anaemia,
thrombocytopenia, renal failure, or aprolonged prothrombin time due
to liver disease
• Many drugs affect the response to warfarin, most by enhancing, but
some by suppressing the anticoagulant effect. The patient’s drug
regimen should be simplified if appropriate to reduce the possibility of
drug interactions
• Where possible, non-interacting drugs within a class should be selected
and aspirin avoided unless combination therapy is indicated
• In patients with peptic ulcer, H. pylori eradication therapy should be
considered
• Patients should be advised to take their daily dose of warfarin at a fixed
time
• An anticoagulant treatment booklet should be issued to patients
(available from: [email protected]).
Other good practice points:-
• An annual review of the patient’s health should be carried out in
patients on long-term warfarin to determine the ongoing suitability of
prescribing the drug
• Methods should be in place to ensure that the quality of service being
offered to patients on warfarin is safe, effective and consistent.
• INR monitoring should be carried out by trained staff and systems in
place to audit clinical performance
• An appropriate recording and documentation system should be in
place. This must include documentation of cumulative records of INRs
and warfarin doses
• Every INR result and dosage should be entered in the patient’s Yellow
Book. The practice record should serve as the patient’s primary and
permanent record.
3
• A patient recall system should be in place and the following factors
should be considered:-
o Formal arrangements for processing reports to ensure that the
result reaches the appropriate clinician timeously
o INR results not within range or marked as urgent should reach the
appropriate clinician on the day of receipt
o A system is in place for informing patients of results and dose
changes
o Arrangements for weekends and public holiday periods are
clearly set out
o Practice guidelines exist detailing referral pattern to secondary
care when needed
When transferring patients from primary to secondary care the following
should be carried out:-
• Advise the patient to take their Yellow Book to the specialist that are
going to be seeing
• Notify the specialist that the patient is on warfarin and give the details
of the GP responsible for monitoring the patient
• Inform secondary care of the following:-
o Indication for warfarin
o Target INR
o Current dose
o Date when warfarin started
o Recent changes and INR results
o Cocomitant medications
o Comorbid conditions including any recent worsening in any of
these
4
Contra-indications and special considerations
Definitive contra-indications to warfarin are as follows:-
• Haemorrhagic stroke
• Clinically significant bleeding
• History within the previous 72 hours of major surgery with risk of severe
bleeding
• Within 48 hours postpartum
• 1st and 3rd trimesters of pregnancy
• Use with interacting drugs which may lead to significantly increased risk
of bleeding
• Known hypersensitivity to warfarin
The decision to use warfarin is however, very much dependent on patient’s
individual circumstances and is often a balance of risks and benefits. An
individual assessment of these risks and benefits should therefore always be
made prior to commencing treatment and, as a minimum, on an annual
basis thereafter. If doubt exists over the suitability of a patient for warfarin
therapy, specialist advice should be sought. A risk/benefit assessment should
be made each time the patient’s condition or circumstances change.
Situations and conditions in which a risk/benefit assessment should made are
shown below. It should be noted however, that this list is not exhaustive and
clinicians should always exercise their clinical judgement when deciding
whether or not a patients is suitable for warfarin therapy.
Special considerations:-
• Known bleeding tendency
• Thrombocytopenia
• Uncontrolled hypertension
• Uncompensated liver cirrhosis
• Non-compliance with medication and/or with monitoring
• Drug abuse
• Trauma related activities and recurrent falls
• Recent trauma or surgery to central nervous system or eyes
• Contraception and pregnancy
• Purple toes syndrome
• Avoid intra-muscular injections where possible
• Intra-articular injections are contra-indicated in patients receiving
warfarin treatment
5
Patient education
Prior to commencing warfarin, patients should be supplied with an
anticoagulation treatment booklet (Yellow Book) and counselled on the
following points:-
• Reason for anticoagulation
• Strength of different tablets
• The need to take warfarin at the same time every day
• The importance of having regular INR checks
• To always carry their Yellow Book
• Never to double their dose in the event of a missed dose
• The potential for warfarin to interact with many medications
• To discuss with their GP or pharmacist any change in medication
• To not start taking any Over The Counter or herbal/complimentary
medications without speaking to their GP or pharmacist
• The potential for warfarin to be affected by changes in diet and to
inform their GP if they make any major changes to their diet
• The potential for warfarin to be affected by alcohol consumption
and to moderate their intake and avoid binge drinking
• The potential for interaction between warfarin and cranberry juice
and grapefruit juice – see section on “Drug Interactions” on page 15
of this guideline
• The need to seek urgent medical attention if they experience any
unusual or unexplained bleeding or bruising
• To inform their dentist that they are taking warfarin
• Women of childbearing age should be informed of the potential
teratogenicand harmful effects of wafarin on the foetus and
advised accordingly on methods of contraception and to inform
their GP if they become pregnant or are planning to become
pregnant
6
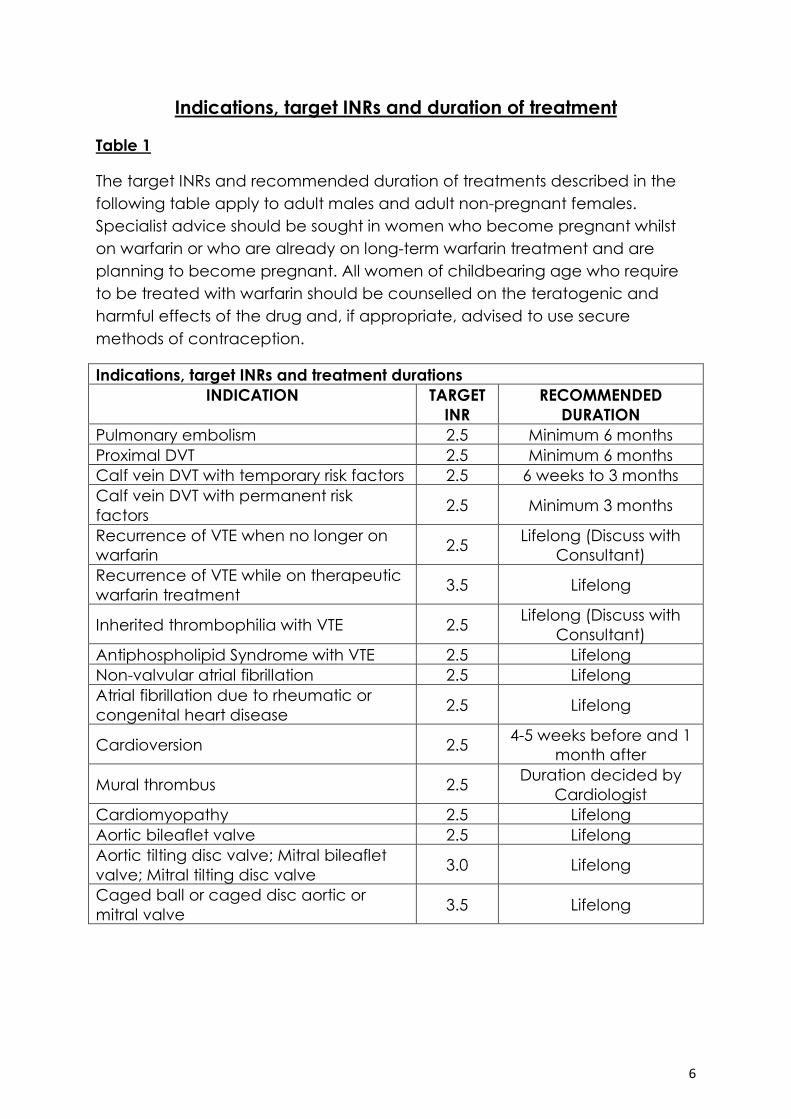
Indications, target INRs and duration of treatment
Table 1
The target INRs and recommended duration of treatments described in the
following table apply to adult males and adult non-pregnant females.
Specialist advice should be sought in women who become pregnant whilst
on warfarin or who are already on long-term warfarin treatment and are
planning to become pregnant. All women of childbearing age who require
to be treated with warfarin should be counselled on the teratogenic and
harmful effects of the drug and, if appropriate, advised to use secure
methods of contraception.
Indications, target INRs and treatment durations
INDICATION TARGET
INR
RECOMMENDED
DURATION
Pulmonary embolism 2.5 Minimum 6 months
Proximal DVT 2.5 Minimum 6 months
Calf vein DVT with temporary risk factors 2.5 6 weeks to 3 months
Calf vein DVT with permanent risk
factors 2.5 Minimum 3 months
Recurrence of VTE when no longer on
warfarin 2.5
Lifelong (Discuss with
Consultant)
Recurrence of VTE while on therapeutic
warfarin treatment 3.5 Lifelong
Inherited thrombophilia with VTE 2.5 Lifelong (Discuss with
Consultant)
Antiphospholipid Syndrome with VTE 2.5 Lifelong
Non-valvular atrial fibrillation 2.5 Lifelong
Atrial fibrillation due to rheumatic or
congenital heart disease 2.5 Lifelong
Cardioversion 2.5 4-5 weeks before and 1
month after
Mural thrombus 2.5 Duration decided by
Cardiologist
Cardiomyopathy 2.5 Lifelong
Aortic bileaflet valve 2.5 Lifelong
Aortic tilting disc valve; Mitral bileaflet
valve; Mitral tilting disc valve 3.0 Lifelong
Caged ball or caged disc aortic or
mitral valve 3.5 Lifelong
7
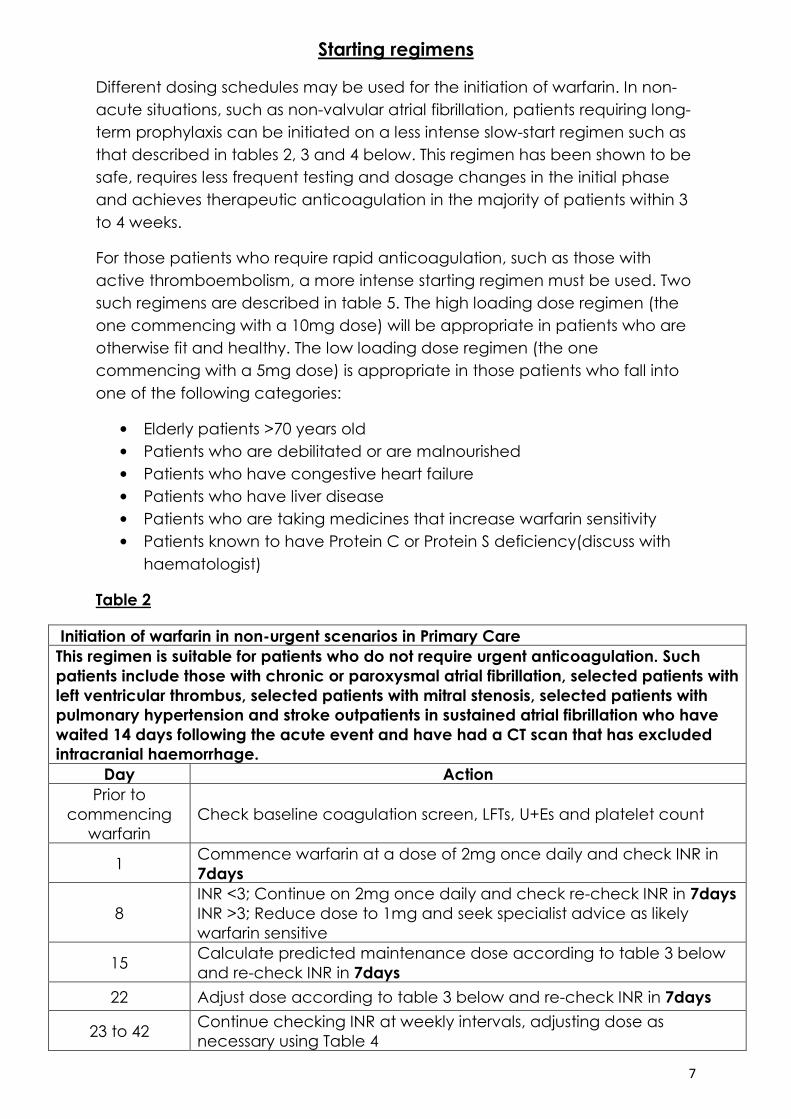
Starting regimens
Different dosing schedules may be used for the initiation of warfarin. In non-
acute situations, such as non-valvular atrial fibrillation, patients requiring long-
term prophylaxis can be initiated on a less intense slow-start regimen such as
that described in tables 2, 3 and 4 below. This regimen has been shown to be
safe, requires less frequent testing and dosage changes in the initial phase
and achieves therapeutic anticoagulation in the majority of patients within 3
to 4 weeks.
For those patients who require rapid anticoagulation, such as those with
active thromboembolism, a more intense starting regimen must be used. Two
such regimens are described in table 5. The high loading dose regimen (the
one commencing with a 10mg dose) will be appropriate in patients who are
otherwise fit and healthy. The low loading dose regimen (the one
commencing with a 5mg dose) is appropriate in those patients who fall into
one of the following categories:
• Elderly patients >70 years old
• Patients who are debilitated or are malnourished
• Patients who have congestive heart failure
• Patients who have liver disease
• Patients who are taking medicines that increase warfarin sensitivity
• Patients known to have Protein C or Protein S deficiency(discuss with
haematologist)
Table 2
Initiation of warfarin in non-urgent scenarios in Primary Care
This regimen is suitable for patients who do not require urgent anticoagulation. Such
patients include those with chronic or paroxysmal atrial fibrillation, selected patients with
left ventricular thrombus, selected patients with mitral stenosis, selected patients with
pulmonary hypertension and stroke outpatients in sustained atrial fibrillation who have
waited 14 days following the acute event and have had a CT scan that has excluded
intracranial haemorrhage.
Day Action
Prior to
commencing
warfarin
Check baseline coagulation screen, LFTs, U+Es and platelet count
1 Commence warfarin at a dose of 2mg once daily and check INR in
7days
8
INR <3; Continue on 2mg once daily and check re-check INR in 7days
INR >3; Reduce dose to 1mg and seek specialist advice as likely
warfarin sensitive
15 Calculate predicted maintenance dose according to table 3 below
and re-check INR in 7days
22 Adjust dose according to table 3 below and re-check INR in 7days
23 to 42 Continue checking INR at weekly intervals, adjusting dose as
necessary using Table 4
8
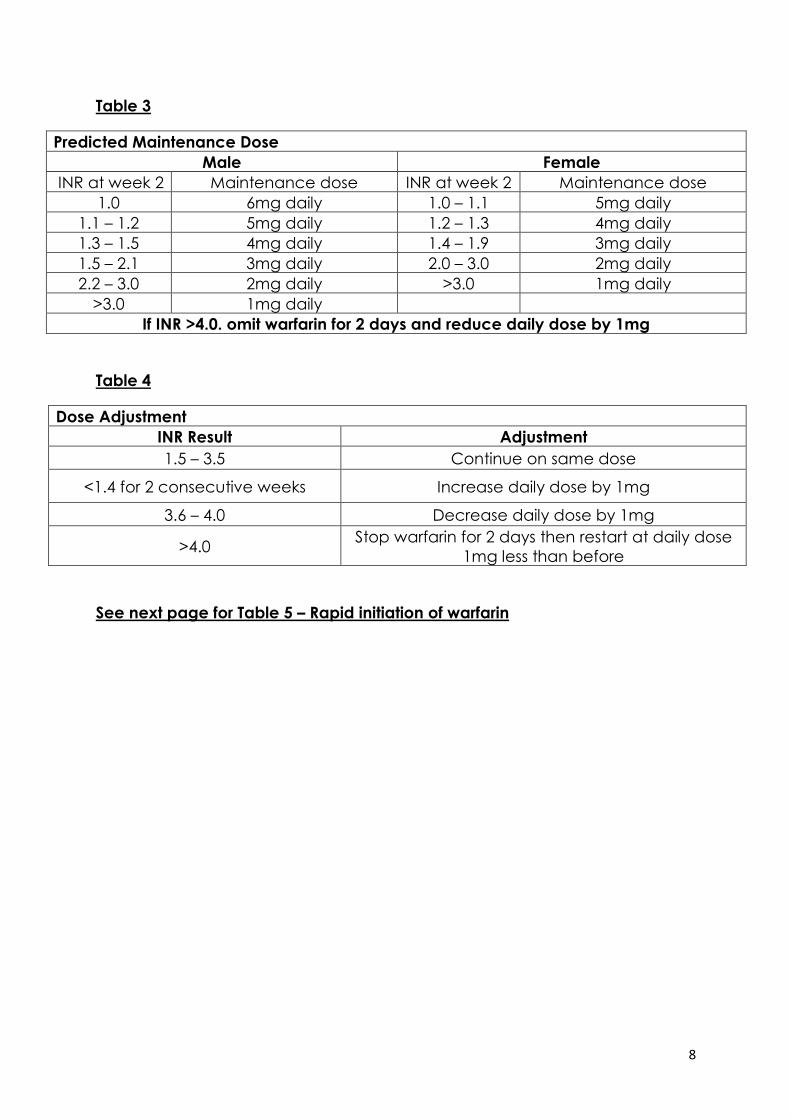
Table 3
Predicted Maintenance Dose
Male Female
INR at week 2 Maintenance dose INR at week 2 Maintenance dose
1.0 6mg daily 1.0 – 1.1 5mg daily
1.1 – 1.2 5mg daily 1.2 – 1.3 4mg daily
1.3 – 1.5 4mg daily 1.4 – 1.9 3mg daily
1.5 – 2.1 3mg daily 2.0 – 3.0 2mg daily
2.2 – 3.0 2mg daily >3.0 1mg daily
>3.0 1mg daily
If INR >4.0. omit warfarin for 2 days and reduce daily dose by 1mg
Table 4
Dose Adjustment
INR Result Adjustment
1.5 – 3.5 Continue on same dose
<1.4 for 2 consecutive weeks Increase daily dose by 1mg
3.6 – 4.0 Decrease daily dose by 1mg
>4.0 Stop warfarin for 2 days then restart at daily dose
1mg less than before
See next page for Table 5 – Rapid initiation of warfarin
9
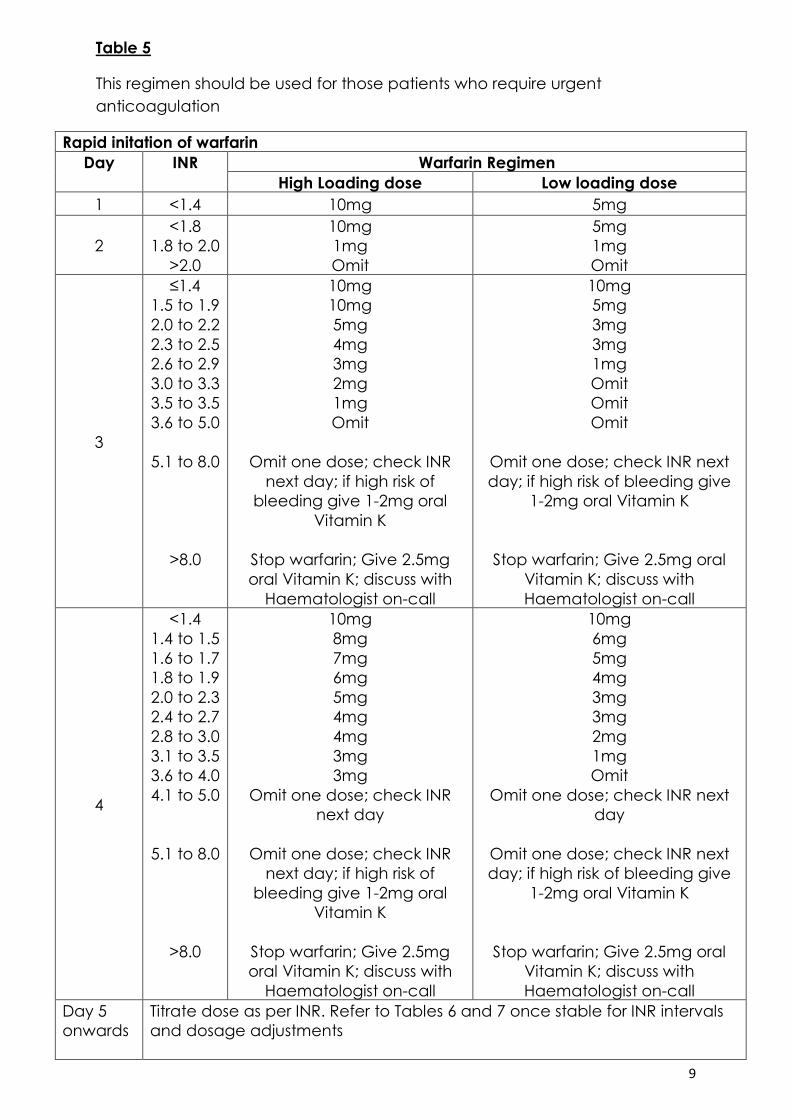
Table 5
This regimen should be used for those patients who require urgent
anticoagulation
Rapid initation of warfarin
Day INR Warfarin Regimen
High Loading dose Low loading dose
1 <1.4 10mg 5mg
2
<1.8
1.8 to 2.0
>2.0
10mg
1mg
Omit
5mg
1mg
Omit
3
≤1.4
1.5 to 1.9
2.0 to 2.2
2.3 to 2.5
2.6 to 2.9
3.0 to 3.3
3.5 to 3.5
3.6 to 5.0
5.1 to 8.0
>8.0
10mg
10mg
5mg
4mg
3mg
2mg
1mg
Omit
Omit one dose; check INR
next day; if high risk of
bleeding give 1-2mg oral
Vitamin K
Stop warfarin; Give 2.5mg
oral Vitamin K; discuss with
Haematologist on-call
10mg
5mg
3mg
3mg
1mg
Omit
Omit
Omit
Omit one dose; check INR next
day; if high risk of bleeding give
1-2mg oral Vitamin K
Stop warfarin; Give 2.5mg oral
Vitamin K; discuss with
Haematologist on-call
4
<1.4
1.4 to 1.5
1.6 to 1.7
1.8 to 1.9
2.0 to 2.3
2.4 to 2.7
2.8 to 3.0
3.1 to 3.5
3.6 to 4.0
4.1 to 5.0
5.1 to 8.0
>8.0
10mg
8mg
7mg
6mg
5mg
4mg
4mg
3mg
3mg
Omit one dose; check INR
next day
Omit one dose; check INR
next day; if high risk of
bleeding give 1-2mg oral
Vitamin K
Stop warfarin; Give 2.5mg
oral Vitamin K; discuss with
Haematologist on-call
10mg
6mg
5mg
4mg
3mg
3mg
2mg
1mg
Omit
Omit one dose; check INR next
day
Omit one dose; check INR next
day; if high risk of bleeding give
1-2mg oral Vitamin K
Stop warfarin; Give 2.5mg oral
Vitamin K; discuss with
Haematologist on-call
Day 5
onwards
Titrate dose as per INR. Refer to Tables 6 and 7 once stable for INR intervals
and dosage adjustments
10
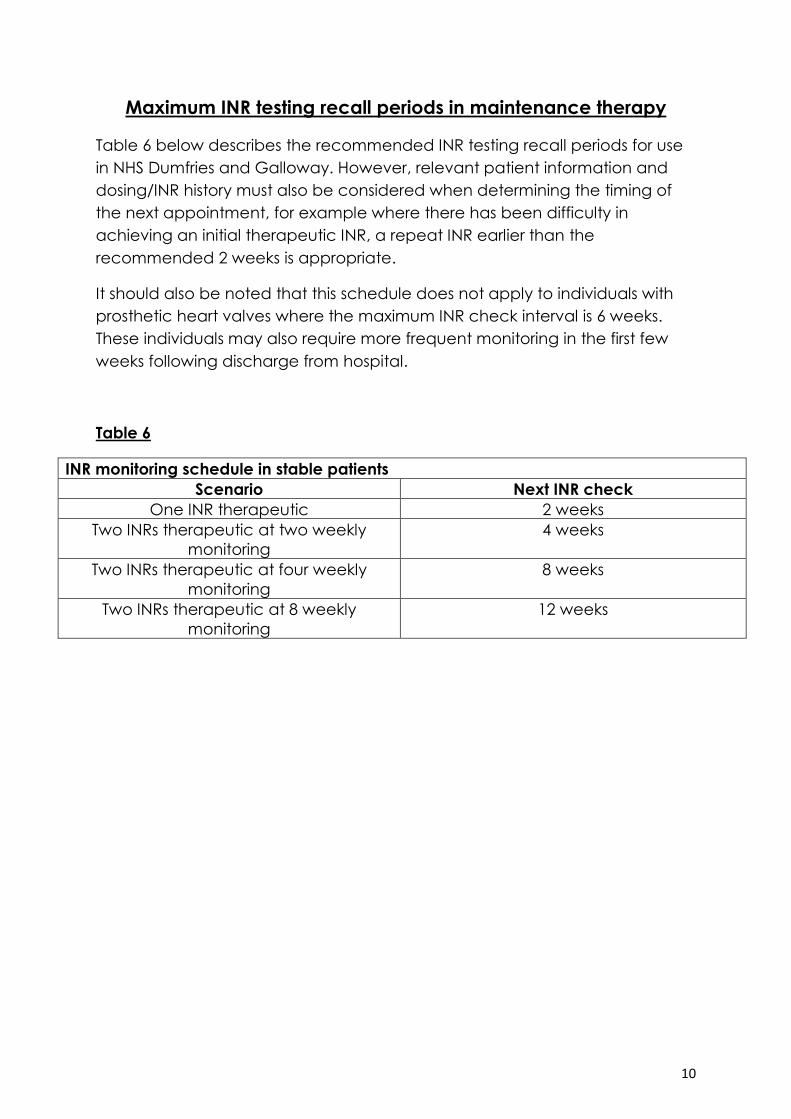
Maximum INR testing recall periods in maintenance therapy
Table 6 below describes the recommended INR testing recall periods for use
in NHS Dumfries and Galloway. However, relevant patient information and
dosing/INR history must also be considered when determining the timing of
the next appointment, for example where there has been difficulty in
achieving an initial therapeutic INR, a repeat INR earlier than the
recommended 2 weeks is appropriate.
It should also be noted that this schedule does not apply to individuals with
prosthetic heart valves where the maximum INR check interval is 6 weeks.
These individuals may also require more frequent monitoring in the first few
weeks following discharge from hospital.
Table 6
INR monitoring schedule in stable patients
Scenario Next INR check
One INR therapeutic 2 weeks
Two INRs therapeutic at two weekly
monitoring
4 weeks
Two INRs therapeutic at four weekly
monitoring
8 weeks
Two INRs therapeutic at 8 weekly
monitoring
12 weeks
11
Dose adjustments in maintenance therapy
Table 7 on the next page details when warfarin dosage adjustments should
be made, how these adjustments should be made and what additional
monitoring, if any, is required. The following important points should always be
borne in mind however:-
• Dose adjustments are not required for minor INR fluctuations where the
result is within +/- 0.5 of the target INR
• Dose adjustments should never be made in isolation – the patient’s
dosing history and other relevant patient factors need to be
considered at all times
• Fluctuations of INR of more than 0.5 from the patient’s target should
always be investigated and corrected where possible. Potential causes
such as a previous change in warfarin dose, poor patient compliance,
concomitant medications, change in diet, change in alcohol intake,
initiation of an interacting drug and intercurrent illness, should always
be considered.
12
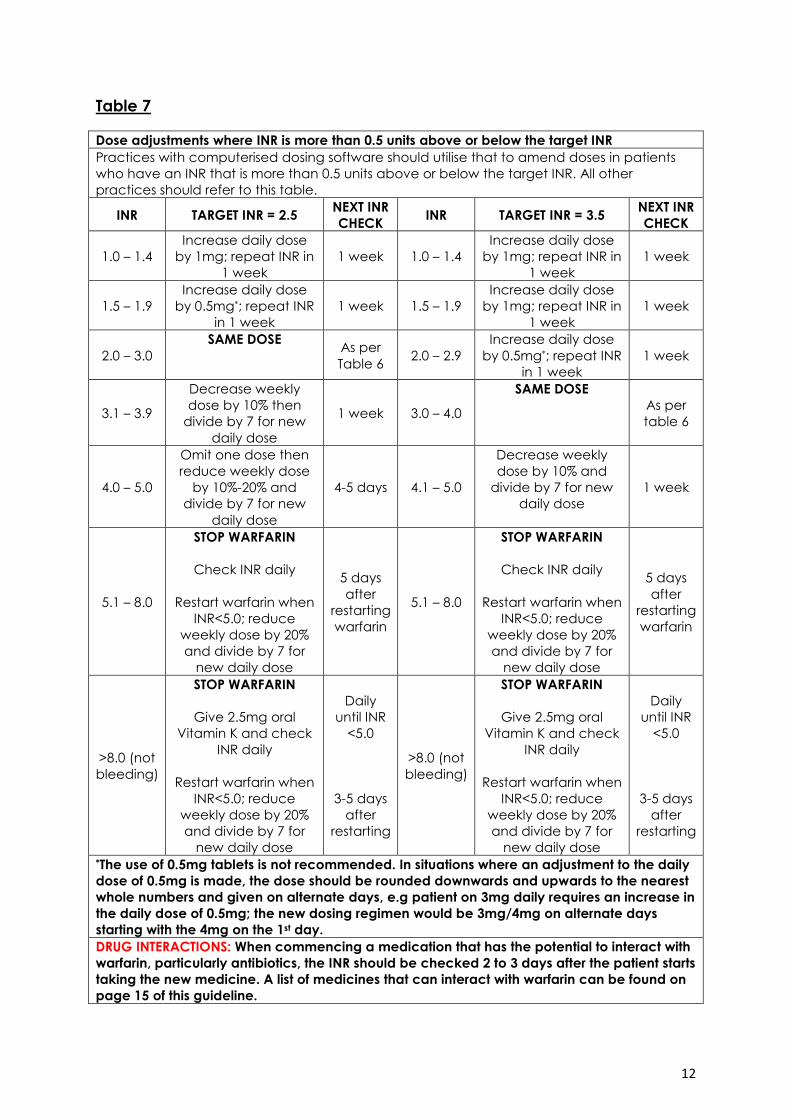
Table 7
Dose adjustments where INR is more than 0.5 units above or below the target INR
Practices with computerised dosing software should utilise that to amend doses in patients
who have an INR that is more than 0.5 units above or below the target INR. All other
practices should refer to this table.
INR TARGET INR = 2.5 NEXT INR
CHECK INR TARGET INR = 3.5
NEXT INR
CHECK
1.0 – 1.4
Increase daily dose
by 1mg; repeat INR in
1 week
1 week 1.0 – 1.4
Increase daily dose
by 1mg; repeat INR in
1 week
1 week
1.5 – 1.9
Increase daily dose
by 0.5mg*; repeat INR
in 1 week
1 week 1.5 – 1.9
Increase daily dose
by 1mg; repeat INR in
1 week
1 week
2.0 – 3.0
SAME DOSE As per
Table 6 2.0 – 2.9
Increase daily dose
by 0.5mg*; repeat INR
in 1 week
1 week
3.1 – 3.9
Decrease weekly
dose by 10% then
divide by 7 for new
daily dose
1 week 3.0 – 4.0
SAME DOSE
As per
table 6
4.0 – 5.0
Omit one dose then
reduce weekly dose
by 10%-20% and
divide by 7 for new
daily dose
4-5 days 4.1 – 5.0
Decrease weekly
dose by 10% and
divide by 7 for new
daily dose
1 week
5.1 – 8.0
STOP WARFARIN
Check INR daily
Restart warfarin when
INR<5.0; reduce
weekly dose by 20%
and divide by 7 for
new daily dose
5 days
after
restarting
warfarin
5.1 – 8.0
STOP WARFARIN
Check INR daily
Restart warfarin when
INR<5.0; reduce
weekly dose by 20%
and divide by 7 for
new daily dose
5 days
after
restarting
warfarin
>8.0 (not
bleeding)
STOP WARFARIN
Give 2.5mg oral
Vitamin K and check
INR daily
Restart warfarin when
INR<5.0; reduce
weekly dose by 20%
and divide by 7 for
new daily dose
Daily
until INR
<5.0
3-5 days
after
restarting
>8.0 (not
bleeding)
STOP WARFARIN
Give 2.5mg oral
Vitamin K and check
INR daily
Restart warfarin when
INR<5.0; reduce
weekly dose by 20%
and divide by 7 for
new daily dose
Daily
until INR
<5.0
3-5 days
after
restarting
*The use of 0.5mg tablets is not recommended. In situations where an adjustment to the daily
dose of 0.5mg is made, the dose should be rounded downwards and upwards to the nearest
whole numbers and given on alternate days, e.g patient on 3mg daily requires an increase in
the daily dose of 0.5mg; the new dosing regimen would be 3mg/4mg on alternate days
starting with the 4mg on the 1st day.
DRUG INTERACTIONS: When commencing a medication that has the potential to interact with
warfarin, particularly antibiotics, the INR should be checked 2 to 3 days after the patient starts
taking the new medicine. A list of medicines that can interact with warfarin can be found on
page 15 of this guideline.
13
Management of bleeding
All patients receiving treatment with warfarin should be continuously assessed
for signs and symptoms of bleeding. Risk factors for bleeding include:-
• Previous history of bleeding
• Recent surgery
• Hypertension
• Cerebrovascular disease or stroke
• Serious heart disease or recent MI
• Renal insufficiency
• Liver disease
• Other pre-existing bleeding disorder e.g. thrombocytopenia
• Age >65 years
• Severe anaemia
• Diabetes
• Concomitant medications that potentiate bleeding
Major bleeding always requires immediate hospital admission and includes
the following scenarios:-
• GI bleeding
• Intracranial bleeding
• Intra-articular bleeding
• Intraspinal bleeding
• Intra-ocular bleeding
• Retroperitoneal bleeding
Non-major bleeding may be managed in Primary Care if it is judged to be
safe to do so and includes the following scenarios:-
• Haemoptysis
• Purpura
• Unexplained or excessive haematomas
• Epistaxis
• Haematuria
14
Non-major bleeding should be managed as follows:-
• Check INR
• If INR >5, omit warfarin and continue to check INR daily until it is <5
• Once INR is <5, restart warfarin at a weekly dose 20% lower than
previous weekly maintenance dose
• Where reversal of warfarin is judged to be necessary, Vitamin K should
be administered by slow intravenous injection at a dose of 2mg
• Admission to hospital for assessment and observation should be
considered where judged appropriate
• When bleeding occurs whilst INR is in the therapeutic range, further
investigations to identify the cause of the bleed should be carried out
15
Interactions with warfarin
Warfarin interacts with many drugs and, often, these interactions can be
unpredictable as patients may be taking more than one interacting drug.
The most desirable course of action when considering prescribing a drug that
is likely to interact with warfarin is, wherever possible, to instead choose one
that won’t interact. Where no alternatives exist, caution must be exercised.
When commencing a medication that has interacting potential,the INR
should be checked 2 to 3 days after the patient starts taking the new
medicine. For specific advice on individual drugs, table 8 that follows can be
used as a reference however it is important to note that this list is not
exhaustive and nor is it intended to be. It provides details of some of the more
commonly encountered and significant interactions with warfarin but where
any doubt exists, the latest edition of the BNF (www.bnf.org)or the relevant
manufacturer’s Summary of Product Characteristics (SPC) (can be found at
www.medicines.org.uk) should be checked.
One particular point to noteis with regards antibiotics - if a patient is unwell
enough to require one, then it may be prudent to increase the frequency of
INRmonitoringas above, even if no specific drug interaction is expected.
Care must also be taken when using herbal/complimentary medicines
concomitantly with warfarin since many of these have the potential to
interact with it. In the absence of data, it must be assumed that the
herbal/complimentary medicine in question can interact with warfarin.
Furthermore, patients must be asked at the start of treatment and at each
review thereafter, whether they are taking any herbal/complimentary
medicines. This is especially important during any investigation of unexplained
bleeding or abnormal INR. The following table contains information on some
of the more commonly used herbal/complimentary medicines.
16
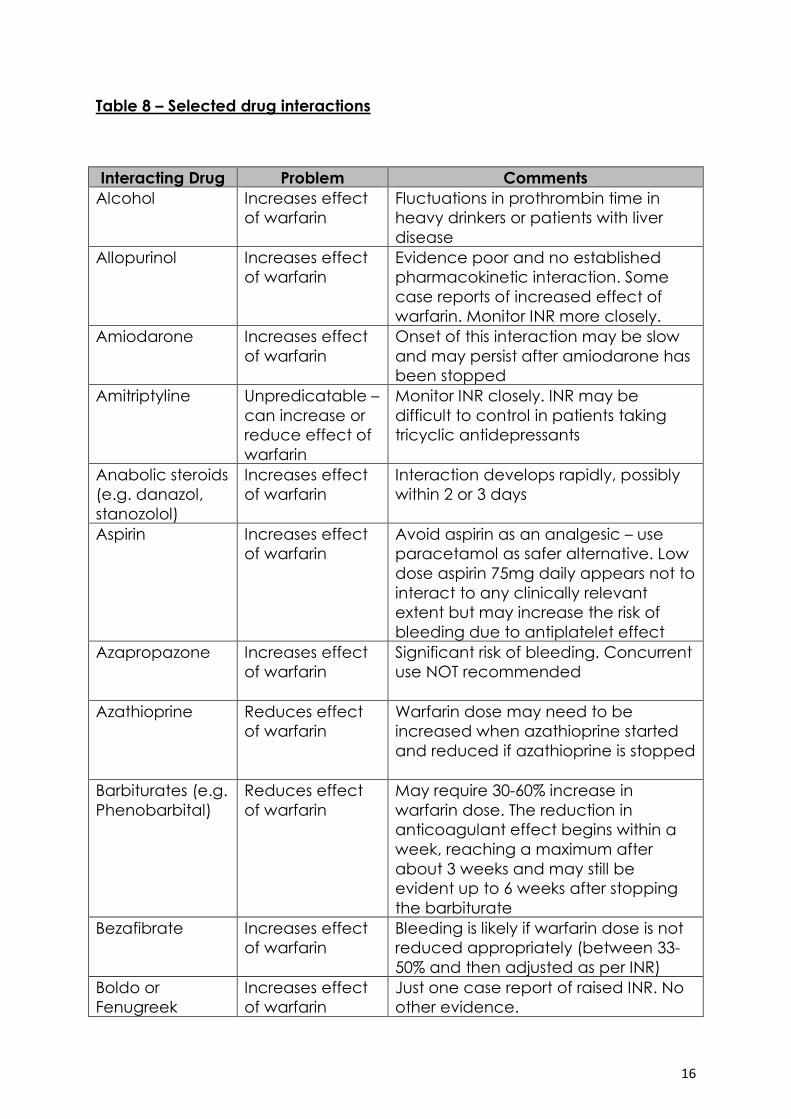
Table 8 – Selected drug interactions
Interacting Drug Problem Comments
Alcohol Increases effect
of warfarin
Fluctuations in prothrombin time in
heavy drinkers or patients with liver
disease
Allopurinol Increases effect
of warfarin
Evidence poor and no established
pharmacokinetic interaction. Some
case reports of increased effect of
warfarin. Monitor INR more closely.
Amiodarone Increases effect
of warfarin
Onset of this interaction may be slow
and may persist after amiodarone has
been stopped
Amitriptyline Unpredicatable –
can increase or
reduce effect of
warfarin
Monitor INR closely. INR may be
difficult to control in patients taking
tricyclic antidepressants
Anabolic steroids
(e.g. danazol,
stanozolol)
Increases effect
of warfarin
Interaction develops rapidly, possibly
within 2 or 3 days
Aspirin Increases effect
of warfarin
Avoid aspirin as an analgesic – use
paracetamol as safer alternative. Low
dose aspirin 75mg daily appears not to
interact to any clinically relevant
extent but may increase the risk of
bleeding due to antiplatelet effect
Azapropazone Increases effect
of warfarin
Significant risk of bleeding. Concurrent
use NOT recommended
Azathioprine Reduces effect
of warfarin
Warfarin dose may need to be
increased when azathioprine started
and reduced if azathioprine is stopped
Barbiturates (e.g.
Phenobarbital)
Reduces effect
of warfarin
May require 30-60% increase in
warfarin dose. The reduction in
anticoagulant effect begins within a
week, reaching a maximum after
about 3 weeks and may still be
evident up to 6 weeks after stopping
the barbiturate
Bezafibrate Increases effect
of warfarin
Bleeding is likely if warfarin dose is not
reduced appropriately (between 33-
50% and then adjusted as per INR)
Boldo or
Fenugreek
Increases effect
of warfarin
Just one case report of raised INR. No
other evidence.

17
Interacting Drug Problem Comments
Carbamazepine Reduces effect
of warfarin
Increase INR monitoring when
introducing carbamazepine to
patients already on warfarin.
Requirement to increase warfarin dose
is likely.Oxcarbazepine does not
appear to interact to the same extent.
Cefaclor Increases effect
of warfarin
Refer to NHS Dumfries & Galloway
Antibiotic Guidance for Primary Care
for appropriate alternatives for the
specific indication.
Celecoxib Increases effect
of warfarin
Large case controlled study from UK
General Practice Research Database
points to an increased risk of bleeding
when celecoxib used with warfarin
similar to that seen with the non-
selective NSAIDs
Chamomile Potential
increase in effect
of warfarin
One case report of raised INR with
bleeding complications. No
pharmacokinetic interaction
established. Not possible to reliably
draw a link between chamomile use
and any effect on warfarin.
Cimetidine Increases effect
of warfarin
Unpredictable but common
interaction. Use ranitidine instead.
Ciprofloxacin Increases effect
of warfarin
Unpredictable and potentially serious
interaction. Increased INR monitoring
required. Use a different antibiotic if
possible – refer to NHS Dumfries &
Galloway Antibiotic Guidance in
Primary Care.
Ciprofibrate Increases effect
of warfarin
Bleeding likely if warfarin dose is not
reduced appropriately (between 33-
50% and then adjusted as per INR)
Clarithromycin Increases effect
of warfarin
Increases in INR have been reported.
Across all macrolides, studies suggest
interactions are occasional but
unpredictable. Those that metabolise
warfarin slowly (the elderly and those
on low doses) appear to be most at
risk. Increased INR monitoring is
recommended.
Clopidogrel Mild bleeding
even though INRs
remain stable
and in range
Increased risk of bleeding due to
antiplatelet effect. Manufacturer
advises avoid concomitant use.
18
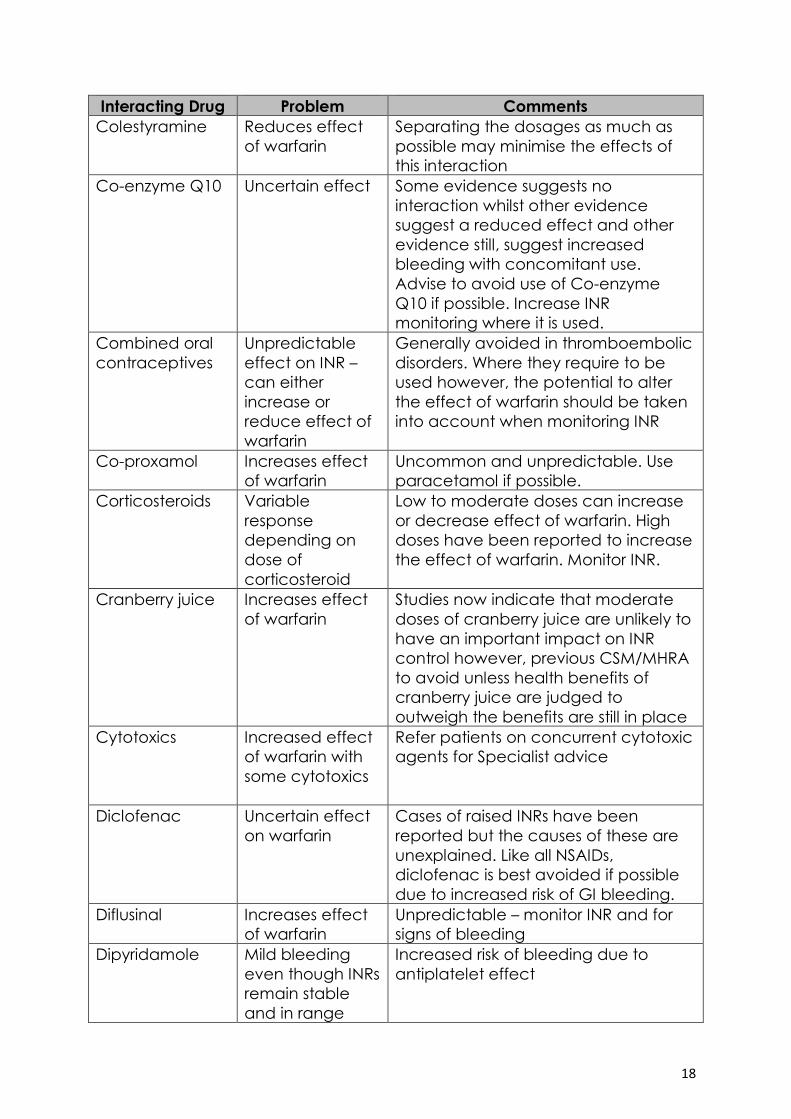
Interacting Drug Problem Comments
Colestyramine Reduces effect
of warfarin
Separating the dosages as much as
possible may minimise the effects of
this interaction
Co-enzyme Q10 Uncertain effect Some evidence suggests no
interaction whilst other evidence
suggest a reduced effect and other
evidence still, suggest increased
bleeding with concomitant use.
Advise to avoid use of Co-enzyme
Q10 if possible. Increase INR
monitoring where it is used.
Combined oral
contraceptives
Unpredictable
effect on INR –
can either
increase or
reduce effect of
warfarin
Generally avoided in thromboembolic
disorders. Where they require to be
used however, the potential to alter
the effect of warfarin should be taken
into account when monitoring INR
Co-proxamol Increases effect
of warfarin
Uncommon and unpredictable. Use
paracetamol if possible.
Corticosteroids Variable
response
depending on
dose of
corticosteroid
Low to moderate doses can increase
or decrease effect of warfarin. High
doses have been reported to increase
the effect of warfarin. Monitor INR.
Cranberry juice Increases effect
of warfarin
Studies now indicate that moderate
doses of cranberry juice are unlikely to
have an important impact on INR
control however, previous CSM/MHRA
to avoid unless health benefits of
cranberry juice are judged to
outweigh the benefits are still in place
Cytotoxics Increased effect
of warfarin with
some cytotoxics
Refer patients on concurrent cytotoxic
agents for Specialist advice
Diclofenac Uncertain effect
on warfarin
Cases of raised INRs have been
reported but the causes of these are
unexplained. Like all NSAIDs,
diclofenac is best avoided if possible
due to increased risk of GI bleeding.
Diflusinal Increases effect
of warfarin
Unpredictable – monitor INR and for
signs of bleeding
Dipyridamole Mild bleeding
even though INRs
remain stable
and in range
Increased risk of bleeding due to
antiplatelet effect
19
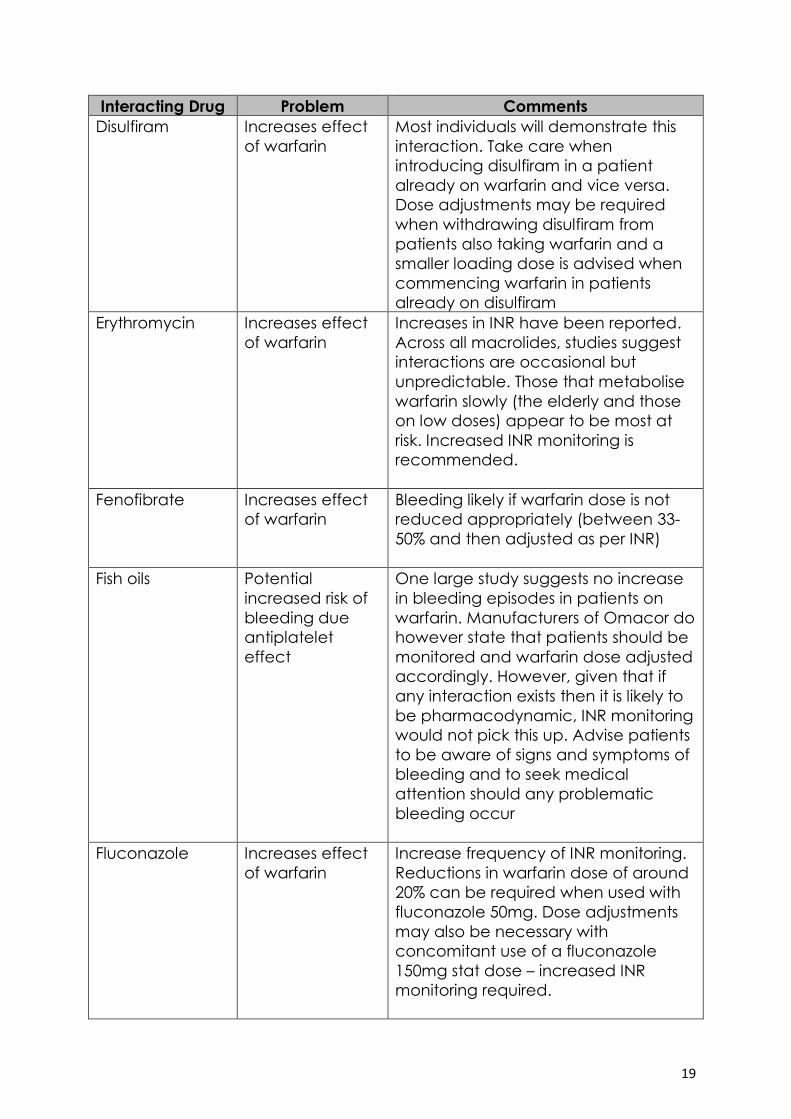
Interacting Drug Problem Comments
Disulfiram Increases effect
of warfarin
Most individuals will demonstrate this
interaction. Take care when
introducing disulfiram in a patient
already on warfarin and vice versa.
Dose adjustments may be required
when withdrawing disulfiram from
patients also taking warfarin and a
smaller loading dose is advised when
commencing warfarin in patients
already on disulfiram
Erythromycin Increases effect
of warfarin
Increases in INR have been reported.
Across all macrolides, studies suggest
interactions are occasional but
unpredictable. Those that metabolise
warfarin slowly (the elderly and those
on low doses) appear to be most at
risk. Increased INR monitoring is
recommended.
Fenofibrate Increases effect
of warfarin
Bleeding likely if warfarin dose is not
reduced appropriately (between 33-
50% and then adjusted as per INR)
Fish oils Potential
increased risk of
bleeding due
antiplatelet
effect
One large study suggests no increase
in bleeding episodes in patients on
warfarin. Manufacturers of Omacor do
however state that patients should be
monitored and warfarin dose adjusted
accordingly. However, given that if
any interaction exists then it is likely to
be pharmacodynamic, INR monitoring
would not pick this up. Advise patients
to be aware of signs and symptoms of
bleeding and to seek medical
attention should any problematic
bleeding occur
Fluconazole Increases effect
of warfarin
Increase frequency of INR monitoring.
Reductions in warfarin dose of around
20% can be required when used with
fluconazole 50mg. Dose adjustments
may also be necessary with
concomitant use of a fluconazole
150mg stat dose – increased INR
monitoring required.
20
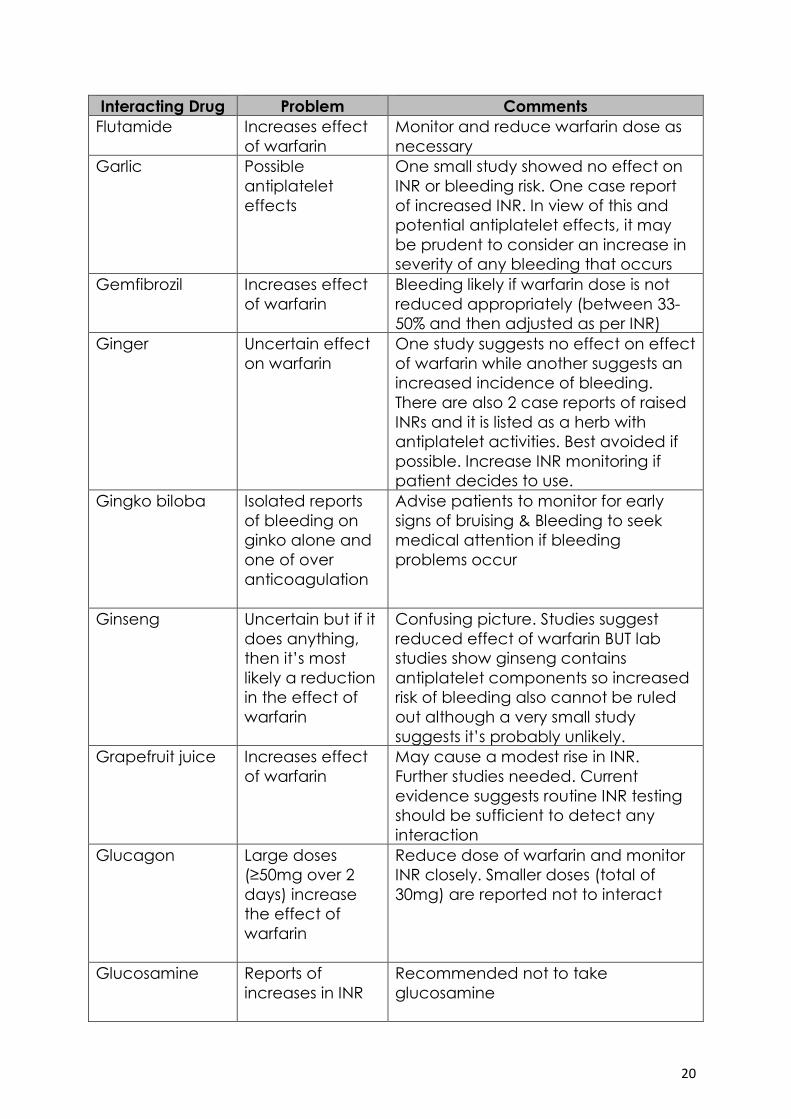
Interacting Drug Problem Comments
Flutamide Increases effect
of warfarin
Monitor and reduce warfarin dose as
necessary
Garlic Possible
antiplatelet
effects
One small study showed no effect on
INR or bleeding risk. One case report
of increased INR. In view of this and
potential antiplatelet effects, it may
be prudent to consider an increase in
severity of any bleeding that occurs
Gemfibrozil Increases effect
of warfarin
Bleeding likely if warfarin dose is not
reduced appropriately (between 33-
50% and then adjusted as per INR)
Ginger Uncertain effect
on warfarin
One study suggests no effect on effect
of warfarin while another suggests an
increased incidence of bleeding.
There are also 2 case reports of raised
INRs and it is listed as a herb with
antiplatelet activities. Best avoided if
possible. Increase INR monitoring if
patient decides to use.
Gingko biloba Isolated reports
of bleeding on
ginko alone and
one of over
anticoagulation
Advise patients to monitor for early
signs of bruising & Bleeding to seek
medical attention if bleeding
problems occur
Ginseng Uncertain but if it
does anything,
then it’s most
likely a reduction
in the effect of
warfarin
Confusing picture. Studies suggest
reduced effect of warfarin BUT lab
studies show ginseng contains
antiplatelet components so increased
risk of bleeding also cannot be ruled
out although a very small study
suggests it’s probably unlikely.
Grapefruit juice Increases effect
of warfarin
May cause a modest rise in INR.
Further studies needed. Current
evidence suggests routine INR testing
should be sufficient to detect any
interaction
Glucagon Large doses
(≥50mg over 2
days) increase
the effect of
warfarin
Reduce dose of warfarin and monitor
INR closely. Smaller doses (total of
30mg) are reported not to interact
Glucosamine Reports of
increases in INR
Recommended not to take
glucosamine
21
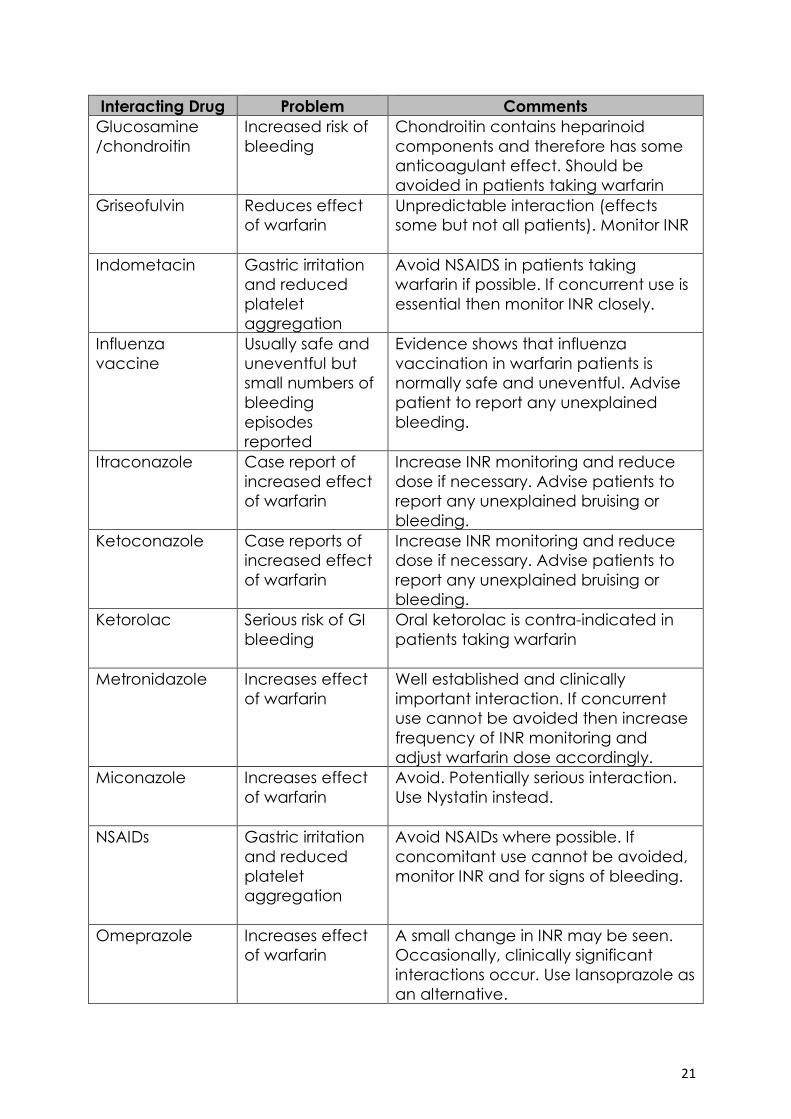
Interacting Drug Problem Comments
Glucosamine
/chondroitin
Increased risk of
bleeding
Chondroitin contains heparinoid
components and therefore has some
anticoagulant effect. Should be
avoided in patients taking warfarin
Griseofulvin Reduces effect
of warfarin
Unpredictable interaction (effects
some but not all patients). Monitor INR
Indometacin Gastric irritation
and reduced
platelet
aggregation
Avoid NSAIDS in patients taking
warfarin if possible. If concurrent use is
essential then monitor INR closely.
Influenza
vaccine
Usually safe and
uneventful but
small numbers of
bleeding
episodes
reported
Evidence shows that influenza
vaccination in warfarin patients is
normally safe and uneventful. Advise
patient to report any unexplained
bleeding.
Itraconazole Case report of
increased effect
of warfarin
Increase INR monitoring and reduce
dose if necessary. Advise patients to
report any unexplained bruising or
bleeding.
Ketoconazole Case reports of
increased effect
of warfarin
Increase INR monitoring and reduce
dose if necessary. Advise patients to
report any unexplained bruising or
bleeding.
Ketorolac Serious risk of GI
bleeding
Oral ketorolac is contra-indicated in
patients taking warfarin
Metronidazole Increases effect
of warfarin
Well established and clinically
important interaction. If concurrent
use cannot be avoided then increase
frequency of INR monitoring and
adjust warfarin dose accordingly.
Miconazole Increases effect
of warfarin
Avoid. Potentially serious interaction.
Use Nystatin instead.
NSAIDs Gastric irritation
and reduced
platelet
aggregation
Avoid NSAIDs where possible. If
concomitant use cannot be avoided,
monitor INR and for signs of bleeding.
Omeprazole Increases effect
of warfarin
A small change in INR may be seen.
Occasionally, clinically significant
interactions occur. Use lansoprazole as
an alternative.
22
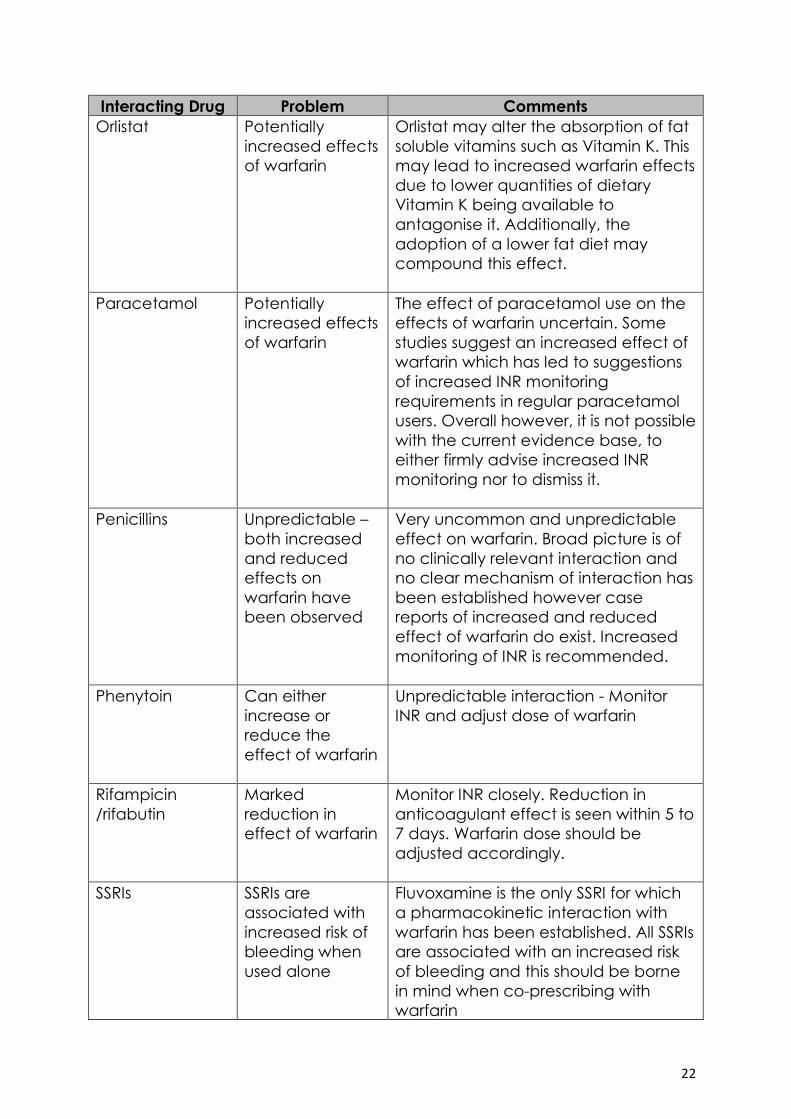
Interacting Drug Problem Comments
Orlistat Potentially
increased effects
of warfarin
Orlistat may alter the absorption of fat
soluble vitamins such as Vitamin K. This
may lead to increased warfarin effects
due to lower quantities of dietary
Vitamin K being available to
antagonise it. Additionally, the
adoption of a lower fat diet may
compound this effect.
Paracetamol Potentially
increased effects
of warfarin
The effect of paracetamol use on the
effects of warfarin uncertain. Some
studies suggest an increased effect of
warfarin which has led to suggestions
of increased INR monitoring
requirements in regular paracetamol
users. Overall however, it is not possible
with the current evidence base, to
either firmly advise increased INR
monitoring nor to dismiss it.
Penicillins Unpredictable –
both increased
and reduced
effects on
warfarin have
been observed
Very uncommon and unpredictable
effect on warfarin. Broad picture is of
no clinically relevant interaction and
no clear mechanism of interaction has
been established however case
reports of increased and reduced
effect of warfarin do exist. Increased
monitoring of INR is recommended.
Phenytoin Can either
increase or
reduce the
effect of warfarin
Unpredictable interaction - Monitor
INR and adjust dose of warfarin
Rifampicin
/rifabutin
Marked
reduction in
effect of warfarin
Monitor INR closely. Reduction in
anticoagulant effect is seen within 5 to
7 days. Warfarin dose should be
adjusted accordingly.
SSRIs SSRIs are
associated with
increased risk of
bleeding when
used alone
Fluvoxamine is the only SSRI for which
a pharmacokinetic interaction with
warfarin has been established. All SSRIs
are associated with an increased risk
of bleeding and this should be borne
in mind when co-prescribing with
warfarin
23
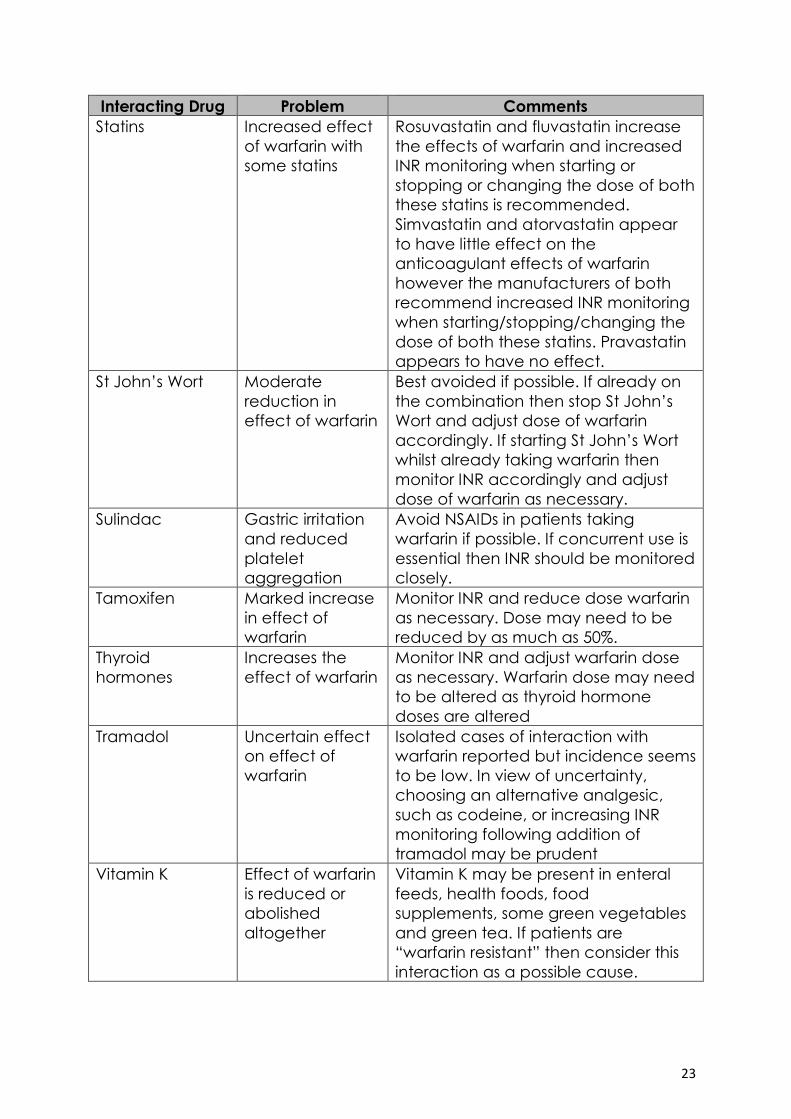
Interacting Drug Problem Comments
Statins Increased effect
of warfarin with
some statins
Rosuvastatin and fluvastatin increase
the effects of warfarin and increased
INR monitoring when starting or
stopping or changing the dose of both
these statins is recommended.
Simvastatin and atorvastatin appear
to have little effect on the
anticoagulant effects of warfarin
however the manufacturers of both
recommend increased INR monitoring
when starting/stopping/changing the
dose of both these statins. Pravastatin
appears to have no effect.
St John’s Wort Moderate
reduction in
effect of warfarin
Best avoided if possible. If already on
the combination then stop St John’s
Wort and adjust dose of warfarin
accordingly. If starting St John’s Wort
whilst already taking warfarin then
monitor INR accordingly and adjust
dose of warfarin as necessary.
Sulindac Gastric irritation
and reduced
platelet
aggregation
Avoid NSAIDs in patients taking
warfarin if possible. If concurrent use is
essential then INR should be monitored
closely.
Tamoxifen Marked increase
in effect of
warfarin
Monitor INR and reduce dose warfarin
as necessary. Dose may need to be
reduced by as much as 50%.
Thyroid
hormones
Increases the
effect of warfarin
Monitor INR and adjust warfarin dose
as necessary. Warfarin dose may need
to be altered as thyroid hormone
doses are altered
Tramadol Uncertain effect
on effect of
warfarin
Isolated cases of interaction with
warfarin reported but incidence seems
to be low. In view of uncertainty,
choosing an alternative analgesic,
such as codeine, or increasing INR
monitoring following addition of
tramadol may be prudent
Vitamin K Effect of warfarin
is reduced or
abolished
altogether
Vitamin K may be present in enteral
feeds, health foods, food
supplements, some green vegetables
and green tea. If patients are
“warfarin resistant” then consider this
interaction as a possible cause.
24
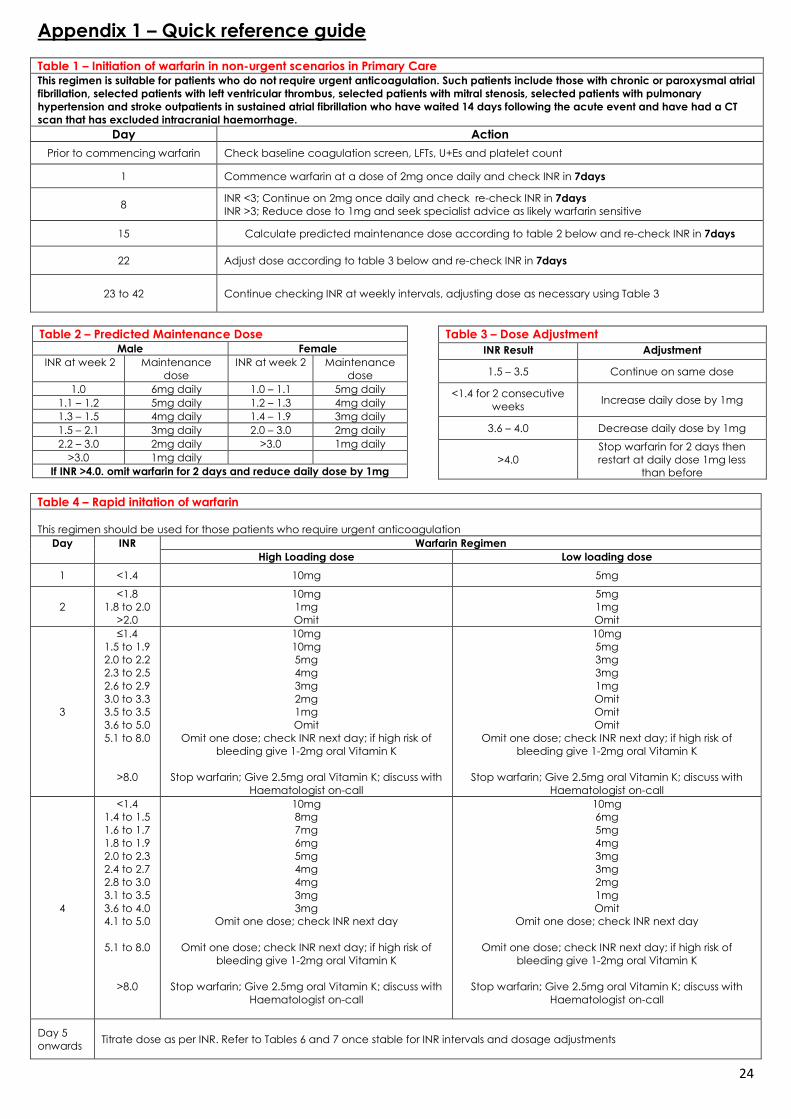
Appendix 1 – Quick reference guide
Table 1 – Initiation of warfarin in non-urgent scenarios in Primary Care This regimen is suitable for patients who do not require urgent anticoagulation. Such patients include those with chronic or paroxysmal atrial
fibrillation, selected patients with left ventricular thrombus, selected patients with mitral stenosis, selected patients with pulmonary
hypertension and stroke outpatients in sustained atrial fibrillation who have waited 14 days following the acute event and have had a CT
scan that has excluded intracranial haemorrhage.
Day Action
Prior to commencing warfarin Check baseline coagulation screen, LFTs, U+Es and platelet count
1 Commence warfarin at a dose of 2mg once daily and check INR in 7days
8 INR <3; Continue on 2mg once daily and check re-check INR in 7days
INR >3; Reduce dose to 1mg and seek specialist advice as likely warfarin sensitive
15 Calculate predicted maintenance dose according to table 2 below and re-check INR in 7days
22 Adjust dose according to table 3 below and re-check INR in 7days
23 to 42 Continue checking INR at weekly intervals, adjusting dose as necessary using Table 3
Table 4 – Rapid initation of warfarin
This regimen should be used for those patients who require urgent anticoagulation
Day INR Warfarin Regimen
High Loading dose Low loading dose
1 <1.4 10mg 5mg
2
<1.8
1.8 to 2.0
>2.0
10mg
1mg
Omit
5mg
1mg
Omit
3
≤1.4
1.5 to 1.9
2.0 to 2.2
2.3 to 2.5
2.6 to 2.9
3.0 to 3.3
3.5 to 3.5
3.6 to 5.0
5.1 to 8.0
>8.0
10mg
10mg
5mg
4mg
3mg
2mg
1mg
Omit
Omit one dose; check INR next day; if high risk of
bleeding give 1-2mg oral Vitamin K
Stop warfarin; Give 2.5mg oral Vitamin K; discuss with
Haematologist on-call
10mg
5mg
3mg
3mg
1mg
Omit
Omit
Omit
Omit one dose; check INR next day; if high risk of
bleeding give 1-2mg oral Vitamin K
Stop warfarin; Give 2.5mg oral Vitamin K; discuss with
Haematologist on-call
4
<1.4
1.4 to 1.5
1.6 to 1.7
1.8 to 1.9
2.0 to 2.3
2.4 to 2.7
2.8 to 3.0
3.1 to 3.5
3.6 to 4.0
4.1 to 5.0
5.1 to 8.0
>8.0
10mg
8mg
7mg
6mg
5mg
4mg
4mg
3mg
3mg
Omit one dose; check INR next day
Omit one dose; check INR next day; if high risk of
bleeding give 1-2mg oral Vitamin K
Stop warfarin; Give 2.5mg oral Vitamin K; discuss with
Haematologist on-call
10mg
6mg
5mg
4mg
3mg
3mg
2mg
1mg
Omit
Omit one dose; check INR next day
Omit one dose; check INR next day; if high risk of
bleeding give 1-2mg oral Vitamin K
Stop warfarin; Give 2.5mg oral Vitamin K; discuss with
Haematologist on-call
Day 5
onwards
Titrate dose as per INR. Refer to Tables 6 and 7 once stable for INR intervals and dosage adjustments
Table 2 – Predicted Maintenance Dose Male Female
INR at week 2 Maintenance
dose
INR at week 2 Maintenance
dose
1.0 6mg daily 1.0 – 1.1 5mg daily
1.1 – 1.2 5mg daily 1.2 – 1.3 4mg daily
1.3 – 1.5 4mg daily 1.4 – 1.9 3mg daily
1.5 – 2.1 3mg daily 2.0 – 3.0 2mg daily
2.2 – 3.0 2mg daily >3.0 1mg daily
>3.0 1mg daily
If INR >4.0. omit warfarin for 2 days and reduce daily dose by 1mg
Table 3 – Dose Adjustment
INR Result Adjustment
1.5 – 3.5 Continue on same dose
<1.4 for 2 consecutive
weeks Increase daily dose by 1mg
3.6 – 4.0 Decrease daily dose by 1mg
>4.0
Stop warfarin for 2 days then
restart at daily dose 1mg less
than before
25
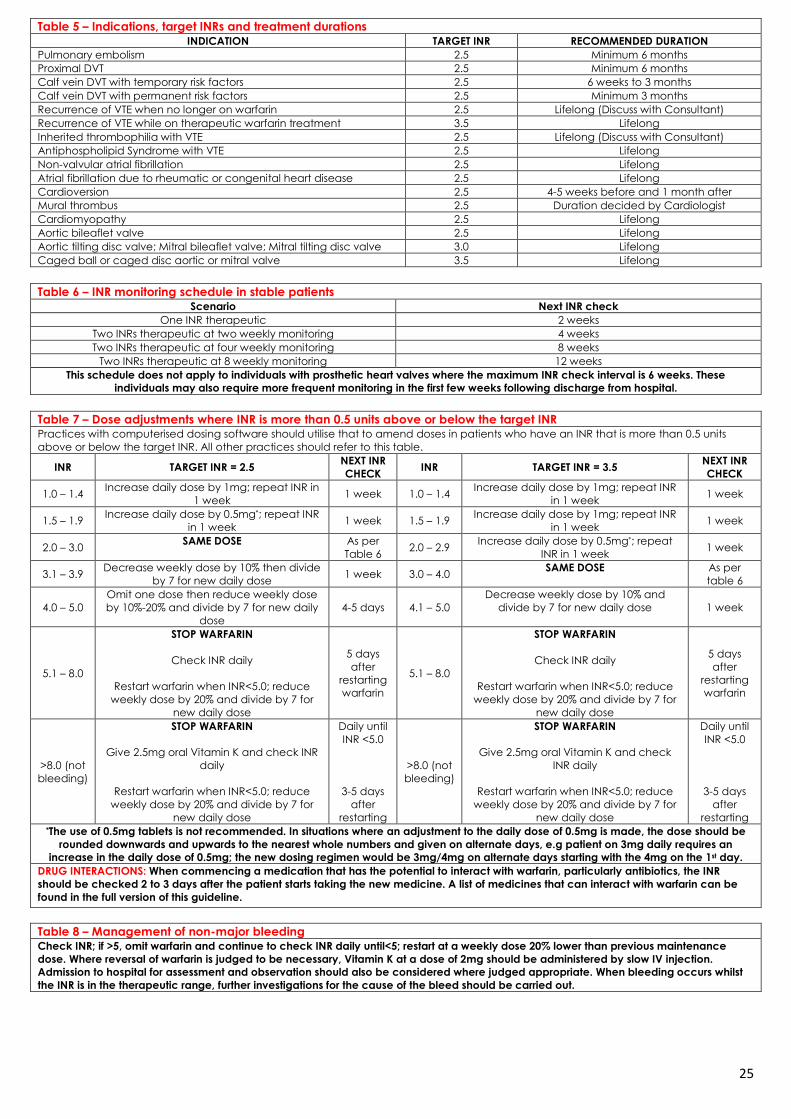
Table 5 – Indications, target INRs and treatment durations INDICATION TARGET INR RECOMMENDED DURATION
Pulmonary embolism 2.5 Minimum 6 months
Proximal DVT 2.5 Minimum 6 months
Calf vein DVT with temporary risk factors 2.5 6 weeks to 3 months
Calf vein DVT with permanent risk factors 2.5 Minimum 3 months
Recurrence of VTE when no longer on warfarin 2.5 Lifelong (Discuss with Consultant)
Recurrence of VTE while on therapeutic warfarin treatment 3.5 Lifelong
Inherited thrombophilia with VTE 2.5 Lifelong (Discuss with Consultant)
Antiphospholipid Syndrome with VTE 2.5 Lifelong
Non-valvular atrial fibrillation 2.5 Lifelong
Atrial fibrillation due to rheumatic or congenital heart disease 2.5 Lifelong
Cardioversion 2.5 4-5 weeks before and 1 month after
Mural thrombus 2.5 Duration decided by Cardiologist
Cardiomyopathy 2.5 Lifelong
Aortic bileaflet valve 2.5 Lifelong
Aortic tilting disc valve; Mitral bileaflet valve; Mitral tilting disc valve 3.0 Lifelong
Caged ball or caged disc aortic or mitral valve 3.5 Lifelong
Table 6 – INR monitoring schedule in stable patients Scenario Next INR check
One INR therapeutic 2 weeks
Two INRs therapeutic at two weekly monitoring 4 weeks
Two INRs therapeutic at four weekly monitoring 8 weeks
Two INRs therapeutic at 8 weekly monitoring 12 weeks
This schedule does not apply to individuals with prosthetic heart valves where the maximum INR check interval is 6 weeks. These
individuals may also require more frequent monitoring in the first few weeks following discharge from hospital.
Table 7 – Dose adjustments where INR is more than 0.5 units above or below the target INR Practices with computerised dosing software should utilise that to amend doses in patients who have an INR that is more than 0.5 units
above or below the target INR. All other practices should refer to this table.
INR TARGET INR = 2.5 NEXT INR
CHECK INR TARGET INR = 3.5
NEXT INR
CHECK
1.0 – 1.4 Increase daily dose by 1mg; repeat INR in
1 week 1 week 1.0 – 1.4
Increase daily dose by 1mg; repeat INR
in 1 week 1 week
1.5 – 1.9 Increase daily dose by 0.5mg*; repeat INR
in 1 week 1 week 1.5 – 1.9
Increase daily dose by 1mg; repeat INR
in 1 week 1 week
2.0 – 3.0 SAME DOSE As per
Table 6 2.0 – 2.9
Increase daily dose by 0.5mg*; repeat
INR in 1 week 1 week
3.1 – 3.9 Decrease weekly dose by 10% then divide
by 7 for new daily dose 1 week 3.0 – 4.0
SAME DOSE As per
table 6
4.0 – 5.0
Omit one dose then reduce weekly dose
by 10%-20% and divide by 7 for new daily
dose
4-5 days 4.1 – 5.0
Decrease weekly dose by 10% and
divide by 7 for new daily dose 1 week
5.1 – 8.0
STOP WARFARIN
Check INR daily
Restart warfarin when INR<5.0; reduce
weekly dose by 20% and divide by 7 for
new daily dose
5 days
after
restarting
warfarin
5.1 – 8.0
STOP WARFARIN
Check INR daily
Restart warfarin when INR<5.0; reduce
weekly dose by 20% and divide by 7 for
new daily dose
5 days
after
restarting
warfarin
>8.0 (not
bleeding)
STOP WARFARIN
Give 2.5mg oral Vitamin K and check INR
daily
Restart warfarin when INR<5.0; reduce
weekly dose by 20% and divide by 7 for
new daily dose
Daily until
INR <5.0
3-5 days
after
restarting
>8.0 (not
bleeding)
STOP WARFARIN
Give 2.5mg oral Vitamin K and check
INR daily
Restart warfarin when INR<5.0; reduce
weekly dose by 20% and divide by 7 for
new daily dose
Daily until
INR <5.0
3-5 days
after
restarting *The use of 0.5mg tablets is not recommended. In situations where an adjustment to the daily dose of 0.5mg is made, the dose should be
rounded downwards and upwards to the nearest whole numbers and given on alternate days, e.g patient on 3mg daily requires an
increase in the daily dose of 0.5mg; the new dosing regimen would be 3mg/4mg on alternate days starting with the 4mg on the 1st day.
DRUG INTERACTIONS: When commencing a medication that has the potential to interact with warfarin, particularly antibiotics, the INR
should be checked 2 to 3 days after the patient starts taking the new medicine. A list of medicines that can interact with warfarin can be
found in the full version of this guideline.
Table 8 – Management of non-major bleeding Check INR; if >5, omit warfarin and continue to check INR daily until<5; restart at a weekly dose 20% lower than previous maintenance
dose. Where reversal of warfarin is judged to be necessary, Vitamin K at a dose of 2mg should be administered by slow IV injection.
Admission to hospital for assessment and observation should also be considered where judged appropriate. When bleeding occurs whilst
the INR is in the therapeutic range, further investigations for the cause of the bleed should be carried out.
26
References
Keeling D, Baglin T, Tait C, Watson H, Perry D, Baglin C, et al.Guidelines on oral
anticoagulation with warfarin – fourthedition. Br J Haematol 2011;154(3):311-
24
The British NationalFormulary no. 65. London: British Medical Association
and Royal Pharmaceutical Society of Great Britain; 2012.
Scottish Intercollegiate Guidelines Network (SIGN).Antithrombotics:
Indications and management. Edinburgh: SIGN; 2006. (SIGN publication no.
129). [cited 2nd July 2013] Available
fromhttp://www.sign.ac.uk/pdf/SIGN129.pdf
Oates A, Jackson PR, Austin CA, Channer KS.A new regimen for starting
warfarin therapy in out patients. Br J ClinPharmacol 1998; 46: 157-161
Kim YK, Nieuwlaat R, Connolly SJ, Schulman S, Meijer K, Raju N, Kaatz S and
Eikelboom JW. Effect of a simple two-step warfarin dosing algorithm on
anticoagulant control as measured by time in therapeutic range: a pilot
study. J ThrombHaemost2010; 8: 101-106
Baxter K (ed), Stockley’s Drug Interactions 10. [online] London:
Pharmaceutical Press <http://www.medicinescomplete.com/> (Accessed on
2nd July 2013).