Embed Size (px)
Citation preview

New Mexico’s Racial and Ethnic Disparities Report Card
Vicky Howell, Ph.D., Office of Policy and Performance
New Mexico Department of Health

2
Overview of the Report Card
Funded through a State Partnership Grant to Improve Minority Health from the U.S. Department of Health and Human Services, Office of Minority Health
Modeled after North Carolina’s report card
Developed in a user-friendly format for the public
Updated annually
Generated the American Indian Health Disparities Report Card
Imitation is the best form of flattery – Delaware used New Mexico’s 2006 format

Purpose of the Report Card In New Mexico
Serves as the focal point for planning and activities geared towards reducing health disparities
Creates a cohesive approach to identifying health disparities
Increases awareness of health disparities
Elicits private, public and community input on possible solutions
Drives the activities of the Office of Health Equity
3

Format – Changes over Time
Added trend graphs (2007)
Added national comparisons and gender data (2007)
Added section on changes in disparity (2008)
Added Pertussis indicator (2008)
Added table of contents (2009)
Added summary data (2010)
Adding fall-related deaths (2011)
4

5
Topics Covered
1. Mother and Child Health (prenatal care, infant mortality, teen births)
2. Chronic Disease (adults with diabetes not receiving services, diabetes deaths, adult obesity, youth obesity)
3. Infectious Diseases (adults 65+ no pneumonia vaccination, pneumonia & influenza deaths, Chlamydia, hepatitis B, HIV/AIDS, Pertussis)
4. Violence and Injury (motor vehicle deaths, suicide, youth suicide, homicide)
5. Risk Behaviors (smoking, drug induced deaths, alcohol-related deaths)

6
2002-2004 2003-2005 2004-2006 2005-2007 2006-2008 2007-20090
5
10
15
20
25
30
35
40
45
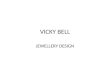
Trend in Pneumonia and Influenza DeathsPer 100
African-American American Indian or Alaska Native
Asian or Pacific Islander Hispanic
White New Mexico
United States

7
Methodology
Indicators reflect areas in which New Mexico’s rates are higher than the national rate (e.g. suicide), or
Demonstrate large disparities between populations (e.g. hepatitis B, infant mortality), or
Demonstrate both high New Mexico rates and large disparities between populations (e.g. teen births, drug-induced deaths)

8
Methodology
Rates are calculated using standard practice for vital statistics and survey data
Handled small populations by using a 3-year rolling average
Disparity ratio calculated based on comparison of rates but only for populations with at least 20 cases during time period
Reference (comparison) group is determined by using the population with best (lowest) rate and at least 20 cases during time period

9
Sources of Data
Vital Statistics (Birth and Death Certificates)
Behavioral Risk Factor Surveillance System
Youth Risk and Resiliency Survey
Infectious Disease Surveillance

Uses of Report Card
Program Planning
Grant Writing
Academic Classes
Conferences
Legislative Hearings
Public Events
Community Awareness/Planning/Activities10

Challenges
Challenges -Grades (love them or hate them)–Perception of Rating Populations Not Disparities
–Program Perception of Rating Program Performance
Small Populations– Total New Mexico population just over 2 million
– Black/African-American population of <50,000– Asian population of <30,000
11

Lessons Learned
Realized that the report card needed to be community-friendly vs. a technical epidemiological report in order for it to be used effectively
Consolidation of data on health disparities all in one document increases awareness
Serves as a key reference for planning, targeted activities and evaluation
Color and pictures help
Can’t please everyone (e.g. grades)
12

Key Collaborations
Within the Division
– Policy, data, and desktop publishing perspectives
External to Division
– Advisory group
– Data sources
13

Link to New Mexico’s
Racial and Ethnic Health Disparities
Report Card
http://nmhealth.org/dpp/health_disparities.shtml
14