Embed Size (px)
Citation preview

New Insights on Warfarin: How CYP 2C9 & VKORC1 Information
May Improve Benefit-Risk Ratio
Brian F. Gage, MD, MScAssociate Professor of Medicine,
Washington University in St. Louis
Blood Thinner Service Medical Director,
Barnes-Jewish Hospital

Overview
• Cytochrome P450 (CYP) 2C9
• Vitamin K Epoxide Reductase, Complex 1 (VKORC1)
• Derivation of pharmacogenetics-based warfarin dosing
• Validation of pharmacogenetics-based warfarin dosing

CYP2C9CYP2C9
CYP1A1CYP1A1CYP1A2CYP1A2CYP3A4CYP3A4
Oxidized Vitamin KOxidized Vitamin K Reduced Vitamin KReduced Vitamin K
OO22
HypofunctionalHypofunctionalF. II, VII, IX, XF. II, VII, IX, X
Protein C, S, ZProtein C, S, Z
Functional Functional F. II, VII, IX, XF. II, VII, IX, X
Proteins C, S, ZProteins C, S, Z
γ--glutamyl glutamyl carboxylasecarboxylase
Vitamin K Vitamin K ReductaseReductase
COCO22
WarfarinWarfarin
Calumenin

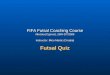
Time to Anticoagulation-Related Outcomes
Higashi. Higashi. JAMAJAMA. 2002;287:1690. 2002;287:1690--1698.1698.
Pro
po
rtio
n w
/ou
t S
tab
le D
ose
Pro
po
rtio
n w
/ou
t S
tab
le D
ose
No. at RiskNo. at RiskVariantVariant 5858 3333 1717 66 66 33 22 22 22Wild TypeWild Type 127127 3939 1919 1010 66 33 33 22 22
5858 2323 1616 99 99 66 44 33127127 7171 5454 3434 2222 1010 66 00
1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
0.00.000 100100 200200 300300 400400 500500 600600 700700 800800 900900 10001000
FollowFollow--up, dup, d
=8.30; =8.30; PP=0.004=0.0042211
Time to Stable DosingTime to Stable Dosing1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
0.00.000 400400 36003600
FollowFollow--up, dup, d
=6.21; =6.21; PP=0.01=0.012211
Time to First Serious orTime to First Serious orLifeLife--Threatening BleedThreatening Bleed
Ble
edB
leed
-- fre
e S
urv
ival
free
Su
rviv
al12001200 20002000 28002800
CYP2C9 variant
CYP2C9 variant
Wild type
Wild type

Effect of CYP2C9*2 on Warfarin Dose
S. Sanderson et al. Genet Med. 2005 Feb;7

Effect of CYP2C9*3 on Warfarin Dose
S. Sanderson et al. Genet Med. 2005 Feb;7

Vitamin K epoxide reductase, complex 1 (VKORC1)
• Mutations in VKORC1 Cause Warfarin Resistance and Multiple Coagulation Factor Deficiency Type 2
• VKORC1 synthesizes vitamin K epoxide reductase (VKOR), which resides in the endoplasmic reticulum of the hepatocyte and other cells– VKOR is inhibited by warfarin, especially S-warfarin
• S-warfarin is metabolized by CYP2C9
– VKOR activity is required for post-translational modification (γ-glutamyl carboxylation) of Glu residues on clotting factors II, VII, IX, X and proteins C, S, and Z
• VKORC1 may or may not be part of a complex

VKORC1 SNPs and Warfarin Dose
• Hypothesis: informative SNPs in VKORC1 correlate with warfarin dose
• We collaborated with Mark Rieder and Allan Rettie at University of Washington– To sequence this gene in archived DNA (N = 47)
from CEPH families and from the Coriell depository
– To correlate informative SNPs (inferred haplotypes) in 186 patients
• To correlate the 4 tagSNPs and inferred haplotypes in a larger cross-sectional study

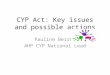
Effect of VKORC1 Inferred Haplotype on Warfarin Dose
Rieder MJ, Reiner AP, Gage BF et al. Effect of VKORC1 haplotypes on transcriptional regulation and warfarin dose. N Engl J Med. Jun 2005.
3673 = rs9923231 aka -1639, a promoter SNP (M. Wadelius; H. Yuan; E. Sconce)
6484 = rs9934438 aka C1173T, (M. Wadelius; H. Yuan; L. Bodin; D’Andrea);
6853 = rs17886369
7566 = rs2359612

VKORC1 Distributions Stratified by Race
Group B haplotypes had larger doses, more mRNA transcript for VKORC1, and were more frequent in white and African-American pts.
Group A haplotypes had smaller doses and were more frequent in Asian pts.

Pyrosequencing in Dr. Eby’s and McLeod’s Labs: Thanks to Sharon, Christi, Rhonda
Pyrogram of VKORC1 6853 heterozygote subject. The sequence for nucleotides is: G/C G A G C G.
Frequency of VKORC1-6853C allele: 37% in white and 24% in black pts.

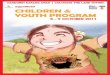
Effect of VKORC1 Haplotype on Warfarin Dose
Stratified by VKORC1 haplotype and CYP2C9 status
Primary cohort: UW (N=185);
Replication cohort: Wash U (N=368).
All participants were Caucasian.

D’Andrea et al. and VKORC1, Blood
• Genotyped 147 warfarin-treated patients for common SNPs in VKORC1
• Found that 1173 did not affect mRNA processing.
VKORC1
1173
Genotype
Warfarin Dose
(mg/d)
CC (37%) 6.2
CT (47%) 4.8
TT (16%) 3.5
P < 0.002

M. Wadelius et al. The Pharmacogenomics Journal
(2005)• Genotyped 200 warfarin-treated patients for
common SNPs in VKORC1.
• found VKORC1 C1173T, which explained 29% of the variability in warfarin dose
• Combined VKORC1 SNP, the CYP2C9*2 and CYP2C9*3 SNPs, and clinical factors, to derive a regression model that accounted for 56% of the variability in the warfarin dose.

M. Wadelius et al. The Pharmacogenomics Journal (‘05)
rs2359612

L. Bodin et al. Measured FVII & INRs in 222 Patients after 1 dose of Acenocoumarol:

E. Sconce et al. ‘05 Derived (N = 297) & Validated (N=38) a Dosing Algorithm using
VKORC1, CYP2C9, Age, Height
R2 = 54%-64%

6 (6%)30 (3%)Takes amiodarone, N (%)
4.8 (1.6)4.8 (1.6)Therapeutic warfarin dose mean (SD)
2.4 (0.4)2.4 (0.4)Target INR mean (SD)
60 (60%)584 (65%)Men, N (%)
84 (84%)743 (83%)Caucasian, N (%)
2.0 (0.24)2.0 (0.26)Body surface area, mean (SD), m2
67 (13) 65 (14)Age, mean (SD), y
Variables
Validation (N = 100)
Derivation(N = 900)
Development and Validation of a Warfarin Dosing Algorithm at Washington University
Gage BF, Eby C, Johnson JA, Rieder MJ, Ridker PM…McLeod H. [ASH abstract]

Warfarin Dosing Equation in Derivation Cohort, N= 900
52%-5% (0 to –10%)-0.053Simvastatin or fluvastatin11
52%9% (2% to 16%)0.085Smokes10
51%-12% (–1% to –17%)-0.126African American9
51%-24% (–15% to –32%)-0.277Amiodarone8
49%8% (5% to 12%)0.161Target INR, per 0.5 increase7
48%-33% (–19% to –44%)-0.395African American * VKOR5808
6
47%-7% (–6% to –9%)-0.007Age, per decade5
43%-20% (–16% to –23%)-0.2182C9*24
39%-33% (–29% to –38%)-0.4082C9*33
32%12% (10% to 14%)0.454BSA, per 0.25 m22
22%-27% (–25% to –30%)-0.319Caucasian * VKOR6853C1
R2 after entry
Effect on Warfarin Dose CoefficientVariableEntry into
Model

Mean Absolute Error, by Dosing StrategyEmpiric Therapy with 5 mg 1.79 mgClinical-based regression model 1.55 mgPharmacogenetics-based dosing 1.31 mg
R2 = 26% for clinical model.
Accuracy in Validation Cohort (N = 100)
(P<0.0001 vs. standard dose; P = 0.02 vs. clinical dose)
R2 = 56% for pharmacogenetics model, but lower in African-Americans
By reducing the dosing error from 1.79 to 1.31 mg, pharmacogenetics should be able to increase the time in range in month one by 2%-4% and should decrease adverse events in patients w/ usual genotypes

Future Studies• SNP discovery in targeted genes: APOE, calumenin,
Factors II, VII, IX, X, γ-GCx• Quantifying the relationship between new SNPs and
warfarin dose– VKORC1 SNPs specific to African-American populations.– Factor VII G-402A & G-401T– Factor II 165Thr>Met– APOE
– γ-GCx• Prospective validation of a pharmacogenetics- dosing model
– Would benefit from a platform that could quickly and economically genotype individuals

Conclusions• The maintenance warfarin dose can be estimated from
clinical and pharmacogenetic factors that can be obtained at the time of warfarin initiation – > 50% of the variability in the warfarin dose can be
predicted from regression model using 2 genes: CYP2C9 and VKORC1
• Although no dosing algorithm has been prospectively validated, the relationship between SNPs in these genes and the therapeutic warfarin dose is biologically and statistically compelling
– For patients initiating warfarin therapy, we estimate a 2%-4% increase in time in the therapeutic INR range in month one with less benefit thereafter
• After month 1, pharmacogenetic knowledge may allow for more cautious dose escalation patients with CYP2C9*2 or CYP2C9*3

Methods for this Prospective, Open-labeled Study
Patients are scheduled for elective orthopedic surgery
Screen for exclusion criteria, obtain consent for clinical trial, gather sample for genotyping, and obtain non genetic data
Determine CYP2C9 genotype (in commercial lab run by Mark Linder) and estimate pharmacogenetic dose
5- or 10-mg dose of warfarin taken the day before surgery
To OR
Inpatient (daily INR) and outpatient pharmacogenetics-based warfarin doses (2-3x/week INR) to be adjusted and monitored by anticoagulation service for 6 weeks
Tim
e
D. Voora et al. Thromb Haemost 2005

Results

Time Until INR > 4 or Major Bleed