Embed Size (px)
Citation preview

Becoming a colposcopist: Colposcope case studies
Seon-Kyung Lee, M.D.
Department of Obstetrics and Gynecology College of Medicine, Kyung Hee
University

Value of Colposcopy
• Cytology is an effective screening method, and
colposcopy with directed biopsy is the critical
diagnostic step for women with cervical cytologic
abnormalities
• Decrease diagnostic conization and hysterectomy.
• Limitation;
It takes some time and experience to properly
analyze what you see.

Role of colposcopist
1. Colposcopist must be able to locate the disease.
2. Colposcopically assess the severity of lesions.
3. Determine the most severe lesion to biopsy.
4. Correlate the colposcopic impression with the cytologic and histologic findings.
5. Then the colposcopist determines the appropriate management or treatment.

Practical knowledge
• Precisely localise TZ,
• Recognize normal and
abnormal TZ,
• TZ with gland opening, sq.met
aplasia, columnar epithelium
• Clinical skills – Punch biopsy,
LLETZ

Colposcopy: Work-up
• Explain to the patient.
• Inspect the vagina and cervix and apply 3-5% acetic acid.
• Position the colposcope and focus on the cervix with the desired magnification (7X-15X).
• Drawings the lesion topography and lesion grade(s)
• Biopsy samples should be obtained from all abnormal lesions.
• A cytobrush or ECC may be used to evaluate the endocervical pathology.
• Hemostatic agent can be applied to each biopsy site.
• Results should be reviewed to confirm.

Diagnostic accuracy of colposcopy
• Calculated based on the agreement of the
colposcopic impression with the histologic
interpretation within one histologic grade.
• Limitations;
Colposcopy is highly sensitive in well-trained hands,
but has low specificity, and, thus, is not a good
screening tool.

Colposcopical scoring system
• Colposcopy is a subjective diagnostic method with high sensitivity and low specificity.
• Because of low specificity, the scoring system for colposcopic findings is important when deciding on the necessity of cervical biopsy, and it contributes to the decreasing of unnecessary biopsy.

Colposcopic accuracy
• The colposcopic accuracy index threshold of 80%
appears to be a reasonable proficiency level and a
useful goal for training programs.
• The colposcopist may overestimate minor benign
cervical epithelial and vascular alterations that
mimic low-grade premalignant disease features. The
error is common when the colposcopist has
knowledge of a preexisting minor cytologic smear
abnormality.

Colpo. Appearance of Benign Lesions
• Keratosis, Erosions and Ulcers, Cervicitis, Atrophy, Nabothian cysts, Ectopy, Deciduosis, Endometriosis, Endocervical polyps.
• The difficulty lies in learning to distinguish low-grade lesions from immature metaplasia which also exhibits aceto-whitening and fine vascular patterns.
• Due to the variability of the colposcopic appearance of low-grade lesions, the accuracy and reproducibility of diagnosis is less than that of higher grade lesions.

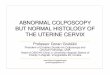
Colpo. Appearance of Benign Lesions
nabothian cyst cervical polyp

Colpo. Appearance of Benign Lesions
immature squamous metaplasia(pinkish white hue)
crypt opening

Colpo. Appearance of Benign Lesions
immature squamous metaplasia
mild acetowhite lesion with fine mosaic and irregular margin

Colpo. Appearance of LSIL
• Flat with a smooth surface, except condylomas.
• Leukoplakia
; benign hyperkeratosis or low-grade HPV lesions.
• Variable aceto-whitening; faint
• Irregular, “feathered” or “geographic” outer borders.
• Partial iodine uptake
• Either featureless or have fine mosaicism or
punctation.

Colpo. appearance of Low Grade Lesion
mildly dense acetowhite lesion
irregular geographical margin

Colpo. appearance of HPV infection
• Condylomas may arise within TZ or as skip lesions
within the mature squamous epithelium.
• The papillary spike-like projections of acuminate
warts and the regular projections(asperites) on
surface of flat condylomas with colposcopic
magnification.
• It also may be a bright aceto-white, which is
characteristic of condyloma.

Colpo. appearance of HPV infection
The bright aceto-white and the asperites on the surface

Colpo. appearance of HSIL
• Sharply demarcated lesion edges
• “lesion within a lesion” or “border within a border”
• More prompt and persistent aceto-white change
• Absence of vessels due to increased lesion density
• “Coarse” vascular patterns (punctation, mosaicism,
or both) ,“Umbilicated” mosaic patterns suggests
CIN 3 / carcinoma-in-situ.

Colpo. appearance of HSIL
dense acetowhite lesion with sharp demarcated margins
internal borders within lesion

Colpo. appearance of HSIL
dense acetowhite lesion with
rolled out margins
coarse punctation and mosaic
with umbilication

HSIL site and Topography
• The most severe disease is found at the most
proximal (cephalad) extent of lesion.
• Size of lesions variable but tends to correlate with
severity of disease and risk of occult invasion
• Size of lesion correlates with risk of treatment failure

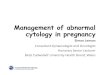
Colpo. Findings of Adenocarcinoma in Situ
• The colposcopic findings are often subtle and nonspecific.
The two primary findings are
(1) a wide area of eversion and
(2) ginger root–like vessels.
• Approximately 40% of adenocarcinoma in situ (ACIS) will have an associated SIL.
• ASCCP guidelines for AGC require colposcopic evaluation and directed biopsies, ECC and D&C for women over 35 years of age.

Colpo. Findings of Adenocarcinoma in Situ
Pap; ASC-H, HPV(HC); -
Biopsy: AIS endocervix
CIS exocervix
Pap ; HSIL, HPV; 18+
Biopsy; adenocarcinoma,
eversion and root–like vessels.

Colpo. appearance of Invasive cancer
The surface is irregular but the borders tend to be sharply defined.
In some cases, subtle ulceration can be the only feature present.
ulcerative lesion; 12-3 ‘oclockexophytic mass

Vaginal colposcopy
• Indicated when cytology suggests disease in:
1) patients with a normal cervix
2) in patients in whom the cervix is absent
• The entire surface area of the vagina is examined, including
that behind the blades of the speculum.
• In post hysterectomy patients, the lateral invagination of the
vaginal vault must be carefully evaluated.
• Areas of VaIN are typically discrete with slightly elevated
borders and are pinkish or white in color.

Colpo. appearance of VaIN
Pap; HSIL post-TAH state, Pap; mod.dysplasia

Colposcopy in pregnant women
• Cervix must be handled atraumatically in order to
avoid bleeding of the congested, hyperaemic tissues.
• The degree of acetowhitening and the confusing
angioarchitecture, with coarse punctation and
mosaicism, may give the impression that the lesion
is severer than it is.

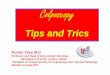
Colposcopy During Pregnancy
progressive eversion of the scj onto the
ectocervix makes colposcopy
satisfactory more often.
Increased vascularity produces a
cyanotic, bluish hue.

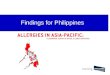
CASE STUDY
23 year old
Pap ; benign cellular
change
Colpo.index; 0-2, SPI
Bx ; 10 o’clock, chonic
cervicitis
HPV(HC); negative

CASE STUDY
53 year old
Pap ; LSIL
Colpo.index; 3-5, r/o HSIL
Bx ; 10 o'clock
CIS
HPV(HC); positive

CASE STUDY
38 year old
Pap ; AGUS
Colpo.index; 0-2, r/o
endocervical lesion
Bx ; 5 o'clock
cervicitis
HPV(HC); negative
Dx Tx conization

CASE STUDIES from ASCCP

CASE STUDY from ASCCP
A 25-year-old G2 P1011, her first Pap test showed ASC-US. She was then lost to follow-up until this current examination.
Question
The cytology shows:
a. negative for intraepithelial lesion or malignancy.
b. ASC-US.
c. LSIL
d. HSIL

CASE STUDY from ASCCP
A 25-year-old G2 P1011, her first Pap test showed ASC-US. She was then lost to follow-up until this current examination.
Question
The cytology shows:
a. negative for intraepithelial lesion or malignancy.
b. ASC-US.
c. LSIL
d. HSIL

The patient was evaluated with colposcopy.
Question 1
Colposcopic findings include:
a. atypical vessels, corkscrew vessels.
b. coarse mosaic pattern with
punctation and sharp borders.
c. microglandular hyperplasia.
d. cervical ectopy.
e. condyloma.
Question 2
The most likely colposcopic
impression is:
a. metaplasia, cervicitis.
b. CIN 1.
c. CIN 3.
d. microinvasive cancer.

Question 1
Colposcopic findings include:
a. atypical vessels, corkscrew vessels.
b. coarse mosaic pattern with
punctation and sharp borders.
c. microglandular hyperplasia.
d. cervical ectopy.
e. condyloma.
Question 2
The most likely colposcopic
impression is:
a. metaplasia, cervicitis.
b. CIN 1.
c. CIN 3.
d. microinvasive cancer.
The patient was evaluated with colposcopy.

CASE STUDY from ASCCP
A 26 year-old woman, G4 P2012, was seen for her first
prenatal visit at 9 weeks gestation. A Pap test at that
time was read as HSIL. Her previous Pap test results,
performed 3 years ago, was read as normal.
Question
The next step in the management of this patient is:
a. To repeat Pap test in 3 months.
b. reflex testing for high-risk human papillomavirus.
c. immediate colposcopy.
d. colposcopy post partum.

A 26 year-old woman, G4 P2012, was seen for her first
prenatal visit at 9 weeks gestation. A Pap test at that
time was read as HSIL. Her previous Pap test results,
performed 3 years ago, was read as normal.
Question
The next step in the management of this patient is:
a. To repeat Pap test in 3 months.
b. reflex testing for high-risk human papillomavirus.
c. immediate colposcopy.
d. colposcopy post partum.
CASE STUDY from ASCCP

The patient underwent a colposcopy at 13 weeks' gestation.
Question 1
What colposcopic features are
present in Figures?
a. fine punctation.
b. coarse mosaic pattern with
punctation.
c. leukoplakia.
d. atypical blood vessels.
Question 2
The colposcopic impression is:
a. CIN 1.
b. CIN 2.
c. CIN 3.
d. microinvasive cancer.
e. Either (b) or (c).

Question 1
What colposcopic features are
present in Figures?
a. fine punctation.
b. coarse mosaic pattern with
punctation.
c. leukoplakia.
d. atypical blood vessels.
Question 2
The colposcopic impression is:
a. CIN 1.
b. CIN 2.
c. CIN 3.
d. microinvasive cancer.
e. Either (b) or (c).
The patient underwent a colposcopy at 13 weeks' gestation.

The patient was seen again at 28 weeks with no change in the colposcopic impression.
She delivered at term and was seen back
in the clinic at 6 weeks postdelivery. At
that time, a Pap test and colposcopy
were done.
Question
The colposcopic impression is:
a. CIN 1.
b. CIN 2.
c. CIN 3.
d. normal.

She delivered at term and was seen back
in the clinic at 6 weeks postdelivery. At
that time, a Pap test and colposcopy
were done.
Question
The colposcopic impression is:
a. CIN 1.
b. CIN 2.
c. CIN 3.
d. normal.
The patient was seen again at 28 weeks with no change in the colposcopic impression.

CASE STUDY from ASCCP
A 26 year old G1 P1001 presented for evaluation of a LSIL
Pap test. In this clinic, women found to have ASCUS x 2
or LSIL Paps were invited to enroll in an IRB approved
study conducted through the local University.
Women with biopsy-proven CIN1 or less were followed with
surveillance Paps and Cervicography™ every 4-6 months
and annual colposcopy. In this case, HPV DNA is positive
for High Risk (HR) types.

The cervigram and findings of her repeat cytology
Question 1Her initial cervigram was interpreted as:
a. negative; normal cervix; squamous metaplasia
b. positive; compatible with low grade lesion
c. positive; probable normal variant
d. positive; compatible with high grade lesion
Question 2The cytology shows:
a. negative for intraepithelial lesion or
malignancy
b. atypical squamous cells of undetermined
significance
c. LSIL; parakeratosis
d. high grade squamous intraepithelial lesion

Question 1Her initial cervigram was interpreted as:
a. negative; normal cervix; squamous metaplasia
b. positive; compatible with low grade lesion
c. positive; probable normal variant
d. positive; compatible with high grade lesion
Question 2The cytology shows:
a. negative for intraepithelial lesion or
malignancy
b. atypical squamous cells of undetermined
significance
c. LSIL; parakeratosis
d. high grade squamous intraepithelial lesion
The cervigram and findings of her repeat cytology

14 months after initial enrollment, the image of her cervix is shown (Figure ). HPV DNA is positive for HR types.
Question 1
Colposcopic findings seen include:
a. atypical vessels, corkscrew vessels,
condyloma
b. dense acetowhite epithelium; absent
vessels; straight border
c. mosaic
d. cervical ectopy
Question 2
The next step in her management would be:
a. re-appoint for study follow-up in 4-6 months
b. repeat colposcopy and biopsy
c. LLETZ
c. cryosurgery

14 months after initial enrollment, the image of her cervix is shown (Figure ). HPV DNA is positive for HR types.
Question 1
Colposcopic findings seen include:
a. atypical vessels, corkscrew vessels,
condyloma
b. dense acetowhite epithelium; absent
vessels; straight border
c. mosaic
d. cervical ectopy
Question 2
The next step in her management would be:
a. re-appoint for study follow-up in 4-6 months
b. repeat colposcopy and biopsy
c. LLETZ
c. cryosurgery

CASE STUDY from ASCCP
20 year old Female G0 with a history of LSIL presented to another colposcopist.
Question
This colposcopic image is most consistent with:
a. satisfactory colposcopy, three low-grade acetowhite lesions seen.
b. unsatisfactory colposcopy, no evidence of any abnormalities.
c. unsatisfactory colposcopy, endocervical lesion seen.
d. satisfactory colposcopy, one abnormal lesion seen at 5- to 7-o'clock.
e. None of the above.

CASE STUDY from ASCCP
20 year old Female G0 with a history of LSIL presented to another colposcopist.
Question
This colposcopic image is most consistent with:
a. satisfactory colposcopy, three low-grade acetowhite lesions seen.
b. unsatisfactory colposcopy, no evidence of any abnormalities.
c. unsatisfactory colposcopy, endocervical lesion seen.
d. satisfactory colposcopy, one abnormal lesion seen at 5- to 7-o'clock.
e. None of the above.

Question 1
During colposcopy, the preferred course of action would be:
a. no biopsies necessary.
b. to biopsy the lesion at 5- to 7-o'clock position.
c. to perform ECC only.
d. to perform multiple biopsies of lesions noted that appear abnormal.
e. immediate LEEP at the time of colposcopy.
Question 2
The preferred course of management would be:
a. LEEP
b. cryotherapy.
c. return colposcopy evaluation within 6 months.
d. vaginal antibiotic therapy,
e. conization with ECC

Question 1
During colposcopy, the preferred course of action would be:
a. no biopsies necessary.
b. to biopsy the lesion at 5- to 7-o'clock position.
c. to perform ECC only.
d. to perform multiple biopsies of lesions noted that appear abnormal.
e. immediate LEEP at the time of colposcopy.
Question 2
The preferred course of management would be:
a. LEEP
b. cryotherapy.
c. return colposcopy evaluation within 6 months.
d. vaginal antibiotic therapy,
e. conization with ECC

CASE STUDY from ASCCP
A 19-year-old, G0, presents for evaluation after a Pap test
showing a LSIL. This was her first abnormal Pap test
and her previous Pap test 1 year earlier was normal. Her
coitarche at age 16 years, and 12 total lifetime sexual
partners.
The patient returned 1 year later for a repeat Pap test. This
time the Pap was reported as HSIL.

The patient underwent a colposcopic examination with a biopsy.
Question 1
The colposcopic appearance of the cervix was
most consistent with:
a. squamous metaplasia
b. CIN 1
c. CIN 2,3
d. adenocarcinoma in situ (AIS)
e. squamous carcinoma
Question 2
The histological diagnosis is consistent with:
a. squamous metaplasia
b. mild dysplasia (CIN 1)
c. moderate dysplasia (CIN 2)
d. severe dysplasia (CIN 3)
e. squamous carcinoma

Question 1
The colposcopic appearance of the cervix was
most consistent with:
a. squamous metaplasia
b. CIN 1
c. CIN 2,3
d. adenocarcinoma in situ (AIS)
e. squamous carcinoma
Question 2
The histological diagnosis is consistent with:
a. squamous metaplasia
b. mild dysplasia (CIN 1)
c. moderate dysplasia (CIN 2)
d. severe dysplasia (CIN 3)
e. squamous carcinoma
The patient underwent a colposcopic examination with a biopsy.

CASE STUDY from ASCCP
A 27-year-old, G5 P3013, presents to the clinic for prenatal care at 20 weeks.
The patient has a history of abnormal Pap tests dating back 7 years. Colposcopic exams and biopsies have shown low-grade squamous intraepithelial lesion (LSIL). Her last Pap test 2 years ago was normal.
The patient’s current Pap test was read as HSIL.

Question 1
The findings on colposcopy are consistent with:
a. CIN 1
b. CIN 2,3
c. invasive cancer
d. metaplasia
Question 2
The next step in the management of this patient is:
a. repeat cytology and colposcopy in 8 weeks
b.repeat cytology and colposcopy in 12 Weeks
c. cold-knife conization
d. repeat cytology and colposcopy 6 weeks postpartum
e. either (b) or (d)

Question 1
The findings on colposcopy are consistent with:
a. CIN 1
b. CIN 2,3
c. invasive cancer
d. metaplasia
Question 2
The next step in the management of this patient is:
a. repeat cytology and colposcopy in 8 weeks
b. repeat cytology and colposcopy in 12 weeks
c. cold-knife conization
d. repeat cytology and colposcopy 6 weeks postpartum
e. either (b) or (d)

CASE STUDY from ASCCP
A 22-year-old presents with HPV positive ASC-US
Papanicoloau smear. She has no previous history of
abnormal Pap smears and has been screened in the
past. She does not smoke.
Question
Appropriate management options for this patient include:
a. repeat HPV testing in 12 months
b. Pap at 6 and 12 months
c. colposcopy
d. HPV DNA specific typing

CASE STUDY from ASCCP
A 22-year-old presents with HPV positive ASC-US
Papanicoloau smear. She has no previous history of
abnormal Pap smears and has been screened in the
past. She does not smoke.
Question
Appropriate management options for this patient include:
a. repeat HPV testing in 12 months
b. Pap at 6 and 12 months
c. colposcopy
d. HPV DNA specific typing

Consensus guidelines for the management of women with abnormal cervical cancer screening tests
ASC-H, LGSIL, HGSIL, squamous cell cancer:
colposcopic evaluation and biopsy of abnormal sites is
recommended.
• ASC-US:
Repeat cytologic evaluation at 6 and 12 months
“Reflex” testing for the presence of high-risk HPV serotypes.
If either of these strategies results in abnormal findings,
colposcopy is indicated.
• AGC:
colposcopic, endocervical and endometrial evaluation, and sampling in addition to HPV testing.
• AIS, adenocarcinoma: excisional procedures

Question 1
The best answer which fits this colposcopic
picture is:
a. satisfactory colposcopy with high grade lesion
b. unsatisfactory colposcopy with no lesion seen
c. satisfactory colposcopy no lesion seen
d. satisfactory colposcopy with low grade lesion
seen
Question 2
Which management option is NOT appropriate
in this patient:
a. ECC
b. repeat Pap and HPV in 6-12 months
c. HPV DNA testing for high risk virus at 12
months
d. loop excision

Question 1
The best answer which fits this colposcopic
picture is:
a. satisfactory colposcopy with high grade lesion
b. unsatisfactory colposcopy with no lesion seen
c. satisfactory colposcopy no lesion seen
d. satisfactory colposcopy with low grade lesion
seen
Question 2
Which management option is NOT appropriate
in this patient:
a. ECC
b. repeat Pap and HPV in 6-12 months
c. HPV DNA testing for high risk virus at 12
months
d. loop excision

Thank you !

이선경
• 연자약력;경희대학교 의과대학 의학과 졸업 1979.2
미국 Vanderbilt university medical center special fellowships in gynecologic oncology 1991.11 --- 1992 10
경희대학교 동서신의학병원 산부인과과장경희대학교 의과대학 산부인과 주임교수
• 학회활동: 대한부인종양-콜포스코피학회; 이사, 학술위원회 위원대한부인종양연구회 연구위원회 위원대한 산부인과학회; 이사, 학술위원회 위원, 논문심사위원
한국 자궁경부확대촬영 연구회 판독위원, 회장미국 질확대경-자궁경부병리학회 정회원세계 부인암학회 정회원