Embed Size (px)
Citation preview

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 1/16
Official reprint from UpToDate
www.uptodate.com ©2017 UpToDate
Skeletal tuberculosis
Authors: Malcolm McDonald, PhD, FRACP, FRCPA, Daniel J Sexton, MD
Section Editor: C Fordham von Reyn, MD
Deputy Editor: Elinor L Baron, MD, DTMH
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Apr 2017. | This topic last updated: Dec 14, 2016.
INTRODUCTION — Skeletal tuberculosis (TB) refers to TB involvement of the bones and/or joints. It is anancient disease; features of spinal TB have been identified in Egyptian mummies dating back to 9000 yearsago [1,2], and analysis of 483 preColumbian skeletons in Chile showed lesions consistent with bonytuberculosis in 2 percent of cases [3]. Subsequently, molecular studies have established the presence ofMycobacterium tuberculosis complex DNA in ancient bony specimens [2,4].
Clinical issues related to skeletal TB will be reviewed here. Other aspects of TB are discussed separately.(See related topics.)
EPIDEMIOLOGY — Skeletal tuberculosis (TB) accounts for 10 to 35 percent of cases of extrapulmonarytuberculosis (10.8 percent of United States extrapulmonary cases in 2013) and, overall, 2.3 percent of allUnited States TB cases reported in 2013 [59]. Reported rates of extrapulmonary TB are higher amongimmigrants from endemic areas to developed countries; this may be due in part to immigration screeningprocedures for pulmonary TB [10]. One retrospective review of skeletal TB between 1980 and 1994 in Francenoted 103 cases of spinal TB; 68 percent of patients were foreign born, the majority from Africa [11]. Theproportion of skeletal TB among HIVinfected individuals is comparable with the proportion of skeletal TBamong HIVuninfected individuals [12,13].
The most common form of skeletal TB is Pott’s disease, a disease of the spine; this entity comprisesapproximately half of musculoskeletal TB cases. The next most common form of musculoskeletal TB istuberculous arthritis, followed in frequency by extraspinal tuberculous osteomyelitis [14].
PATHOGENESIS — During primary M. tuberculosis infection, bacillemia may lead to seeding of organisms inbone and/or synovial tissue. In most cases, small foci of infection are confined by local adaptive immuneprocesses, and infection is subclinical. Following primary infection, reactivating foci may be contained by thecellular immune response. CD4 and CD8 lymphocytes play important roles, as does interferongamma [15].Reactivation of infection with progression to clinically apparent disease may occur when local immunedefenses fail, as in the setting of malnutrition, advancing age, HIV infection, or renal failure [16].
Active tuberculosis (TB) disease can develop immediately or after decades of latent infection. In highlyendemic regions, musculoskeletal TB usually manifests clinically in the year following primary lung infectionand therefore occurs most frequently in relatively young patients. Outside endemic areas, musculoskeletal TBis more commonly associated with late reactivation of infection and occurs mainly in adults.
Two types of bone and joint involvement associated with TB infection have been described: the caseousexudative type and the granular type [17]. The caseous exudative type is characterized by bone destruction,local swelling, abscess formation, sinus formation, and constitutional symptoms; it occurs most often inchildren. The granular type is more insidious and less destructive than the caseous exudative type, andabscess formation is less common; it occurs most often in adults. However, hostparasite interactions intuberculosis are dynamic, often with mixed patterns and transitions along a continuum [18].
®
®

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 2/16
Rarely, bones and joints are involved in contiguous spread of TB from another site. Contiguous spread froman apical pulmonary focus of active TB, for example, can lead to atlantoaxial TB, involving the joint betweenthe first and second cervical vertebrae [19].
CLINICAL MANIFESTATIONS — Forms of skeletal tuberculosis (TB) include spondylitis (Pott’s disease),arthritis, and osteomyelitis. From published series of spinal TB, there is wide variation in reported rates ofactive concomitant pulmonary TB at the time of diagnosis of the spinal TB [11,20,21]. The largest reportseries including nearly 700 cases had the lowest reported rate (2.7 percent) [21]. The proportion is likely to besimilarly variable for other TB bone and joint infections, but series are too small to provide reliable data.Virtually any bone can be infected with M. tuberculosis. The diagnosis may be delayed when unusual bonessuch as the hyoid or digits are infected or when multifocal bony involvement is present.
Spondylitis (Pott's disease) — Tuberculous spondylitis (Pott’s disease) most commonly affects the lowerthoracic and upper lumbar region; disease involving the cervical and upper thoracic region is less common[22,23]. Infection generally begins with inflammation of the anterior aspect of the intervertebral joints; typically,it spreads behind the anterior ligament to involve the adjacent vertebral body. Once two adjacent vertebraeare involved, infection enters the adjoining intervertebral disc space. This tends to occur later in Pott'sdisease than in bacterial vertebral osteomyelitis and may have the radiographic appearance of relative discsparing. Eventually, the avascular disc tissue dies; there is vertebral narrowing and subsequent vertebralcollapse. Gibbus deformity, a form of structural kyphosis, distorts spinal canal anatomy (image 1). The spinalcord is then at risk of compression, resulting in paraplegia [24]. Occasionally, lateonset paraplegia occursdue to osteophytes and other chronic degenerative changes at a site of prior infection. Formation of a "coldabscess" (soft tissue mass) at the site is common. Noncontiguous spinal disease (eg, disease at more thanone level) is uncommon, although in one South African series it was described in 16 of 98 cases [25].
The most common symptom is local pain, which increases in severity over weeks to months, sometimes inassociation with muscle spasm and rigidity. The muscle spasm can extend beyond the diseased area. Insome cases, a characteristic erect posture and "aldermanic" gait may be observed in which the patient walkswith short, deliberate steps to avoid jarring of the spine [26]. Constitutional symptoms such as fever andweight loss are present in less than 40 percent of cases [12,20,2729].
The diagnosis of Pott’s disease is frequently delayed as a result of its subacute course, especially in regionswhere the incidence of tuberculosis is relatively low [12,20]. In endemic areas, the clinical presentation alsotends to be relatively late due to limited access to medical care; in these settings, patients have symptomsand signs of cord compression at the time of diagnosis in 40 to 70 percent of cases [20,30]. Thus, latediagnosis is a major factor in determining the outcome of the disease [31].
Arthritis
Infectious — Tuberculous arthritis can occur in virtually any joint, but it tends to occur in the hip or theknee; usually, it is monoarticular. However, multifocal lesions are reported in 10 to 15 percent of cases indeveloping countries [32]. Hip involvement is the most common presentation, the most difficult to diagnose,and the most debilitating [6]. Clinical manifestations include swelling, pain, and/or loss of joint function thatprogresses over weeks to months. The joint is generally "cold" (eg, erythema, warmth, and other signs ofacute infection are usually absent). Constitutional symptoms, fever, and weight loss occur in only about 30percent of cases [27].
Patients who present late in the course of disease often have evidence of joint destruction including localdeformity and restricted range of motion. Some patients with advanced disease have draining sinuses.Granulomatous changes typically accompany synovial proliferation in tuberculous arthritis, with joint effusionand erosion of cartilage. The consequences are slowly progressive destruction, disorganization of jointarchitecture, and potential deformity.
Some data suggest that total hip replacement in the setting of active TB is acceptable if undertaken inassociation with appropriate debridement and antituberculous therapy [33].

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 3/16
Inflammatory (Poncet's disease) — Poncet’s disease is an acute symmetrical polyarthritis involving large
and small joints associated with active extrapulmonary, pulmonary, or miliary TB. In general, there is
inflammation of the involved joints but no objective evidence of active TB [3437]. Poncet’s disease is
relatively rare, and the pathogenesis is unclear; it is probably immune mediated [36]. HIV coinfection is also a
risk factor [38,39]. The arthritis generally resolves within a few weeks of initiation of antituberculosis therapy,
with no residual joint destruction [35,40].
Prosthetic joint infection — Rarely, M. tuberculosis can cause infection at the site of a prosthetic joint.Diagnosis has been described at the time of initial arthroplasty as well as subsequent to hardware placement
[41].
For cases in which TB is identified at the time of initial arthroplasty, the diagnosis is typically a surprise to the
surgeon who sends abnormalappearing bone for histopathologic examination or culture at the time of joint
replacement. These patients generally have a favorable outcome after standard antituberculous
chemotherapy, even if the joint prosthesis is not removed.
For cases in which infection is identified following hardware placement, a dormant nidus of infection
reactivates, and patients subsequently present with clinical findings of an infected prosthesis. These patients
often have painful, malfunctioning prostheses, and hardware removal is required for cure. Some patients with
lateonset tuberculous prosthetic joint infections have coexisting bacterial infection that may mask or obscure
the underlying coinfection with M. tuberculosis.
Osteomyelitis — In addition to tuberculous vertebral osteomyelitis (Pott's disease), tuberculous osteomyelitis
can occur in virtually any bone, including the ribs, skull, hand, wrist, phalanx, pelvis, and long bones. The
onset is often insidious but, in rare cases, the onset may be acute or subacute [42]. Typically, osteomyelitis
occurs at a single site. However, rarely bony involvement can be multifocal. The location and presentation
can be variable as illustrated by the following case reports:
In some cases, bony infection may spread to contiguous soft tissues or even adjacent joints. Rarely,
involvement of multiple bones may be associated with erroneous diagnosis of metastatic malignancy [5153].
An antecedent history of trauma may lead to diagnostic confusion; tuberculous can develop in a bone or joint
injured by previous trauma or surgery. Tuberculous osteomyelitis frequently presents as a "cold abscess" with
swelling, modest erythema or pain, and little or no local warmth [14]. Spontaneous drainage may occur.
Other clinical manifestations — Musculoskeletal tuberculosis can occur as an abscess in the epidural
space (creating pressure on the spinal cord), as an extraspinal soft tissue mass (eroding ribs and adjacent
structures), or as a psoas abscess (which can track down to the groin). (See "Psoas abscess".)
Radiography — Radiographic imaging can be useful to identify and establish the anatomy of
musculoskeletal TB, although there are no pathognomonic radiographic findings.
In the setting of tuberculous spondylitis (Pott's disease), radiographic abnormalities are usually first observed
in the anterior aspect of a vertebral body, with demineralization of the end plate and loss of definition of the
bony margin [54]. Subsequently, the opposing vertebra becomes involved and, in some cases, a
paravertebral abscess may be seen. Involvement of contiguous vertebrae is common, although it is
Sternal osteomyelitis due to M. tuberculosis may follow coronary artery bypass surgery [43] as apresentation of underlying mediastinal tuberculosis [44] or as primary sternal osteomyelitis [45].
Bony tuberculosis of the rib may present as a breast mass or chest wall mass [46,47].
Tuberculosis of the small bones of the hand can occur spontaneously in patients with no clinical signs of
pulmonary tuberculosis [48].
Tuberculous mastoiditis can extend into the skull and produce facial nerve palsy [49].
Lytic bony tubercular lesions in areas as unusual as the symphysis pubis, sacroiliac joint, and elbow can
be misdiagnosed as metastatic malignancy [50].

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 4/16
uncommon to see noncontiguous spinal TB at multiple levels. As infection progresses, the disc space
becomes obliterated with anterior wedging and angulation. Reactive sclerotic changes remain localized and
the remainder of the vertebral structures is often spared (image 2).
In some patients, spinal tuberculosis presents with osteolytic lesions in the absence of disc space
involvement; these lesions may occur at multiple sites. In one study of 103 French patients with spinal
tuberculosis, spinal tuberculosis without disc involvement was observed in about half of cases; plain
radiographs demonstrated osteolytic lesions and multiple involved sites [11].
In the setting of tuberculous arthritis, local soft tissue swelling, osteopenia, and bone destruction (with relative
preservation of cartilage space) are observed. Subsequent findings include structural collapse, sclerotic
changes, and soft tissue calcification (image 3). In some cases, Phemister triad may be observed: juxta
articular osteopenia, peripherally located osseous erosions, and gradual narrowing of the joint space (image
4) [55,56].
In the setting of tuberculous osteomyelitis in children, cystic changes may be seen in the metaphyses of long
bones and in flat bones, such as the skull. In tuberculous osteomyelitis involving a hand or foot, phalangeal
bone(s) may have a ballooned appearance.
Computerized tomography (CT), myelography, and magnetic resonance imaging (MRI) are all useful tools in
the diagnosis of musculoskeletal TB [22,5761]. MRI is particularly valuable in demonstrating soft tissue
extension and encroachment on nearby vital structures, such as the spinal cord (image 5 and image 6 and
image 7 and image 8) [62].
Chest radiography is not a sensitive test for the diagnosis of skeletal TB since there is no evidence of active
chest disease in more than half of cases [5,14,20,63]. However, chest radiography should always be obtained
since it may inform decisions regarding isolation. The diagnosis of skeletal tuberculosis should be considered
in patients with focal bony or joint abnormalities and a chest radiograph compatible with old or active
tuberculosis. (See "Diagnosis of pulmonary tuberculosis in HIVuninfected adults".)
DIAGNOSIS
General principles — The greatest challenge in diagnosis of skeletal tuberculosis (TB) is to consider the
diagnosis, especially since there is no evidence of active chest disease in more than half of cases. In
addition, delays in diagnosis are common given the indolent nature of tuberculous bone and joint disease.
Clinical clues usually come from the history, which should include questions about the country of origin and
history of prior known or possible TB contact. In addition, the diagnosis of skeletal tuberculosis may be
overlooked in patients with HIV infection and relatively high CD4 counts and no other signs or symptoms of
tuberculosis.
The diagnosis of musculoskeletal TB is established by microscopy and culture of infected material. Tissue
may be obtained by needle aspiration and/or biopsy; computed tomography (CT) guidance is useful in
regions where available.
Biopsy and culture — The diagnosis of musculoskeletal TB is established by microscopy and culture of
infected material [6466]. Drug susceptibility testing of isolates is essential. Tissue may be obtained by needle
aspiration and/or biopsy. CT guidance is useful in regions where available [67,68].
The diagnosis of tuberculous arthritis can be established by synovial biopsy. Synovial fluid may be examined
[69], but findings are usually nonspecific; the white cell count can be high or low, with preponderance of either
neutrophils or lymphocytes [70].
In the setting of one or more draining sinuses, culture of this material may be useful, although, in some cases,
cultures may demonstrate colonizing bacteria or fungi that are erroneously assumed to be the causative
pathogen.

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 5/16
The high cost and technical demands of rapid automated growth systems and nucleic acid detection methods
often limits their use in the poorest countries with the highest incidence of tuberculosis [71]. The Xpert
MTB/RIF assay is an automated nucleic acid amplification test that can simultaneously identify M.tuberculosis and rifampin resistance; it has been shown to be fast and accurate in diagnosingmusculoskeletal tuberculosis in children and adults [72,73]. This assay is discussed further separately. (See"Diagnosis of pulmonary tuberculosis in HIVuninfected adults".)
Additional issues related to diagnostic microbiology are discussed further separately. (See "Diagnosis of
pulmonary tuberculosis in HIVuninfected adults".)
Differential diagnosis — The differential diagnosis of skeletal TB includes subacute or chronic infections
due to pathogens or diseases such as Staphylococcus aureus osteomyelitis, brucellosis, melioidosis,actinomycosis, candidiasis, and histoplasmosis, depending upon epidemiologic factors. Multifocal bone
involvement may be confused for metastatic malignancy.
The differential diagnosis of Pott’s disease includes degenerative disc and facet joint disease,
spondyloarthropathy, vertebral body collapse due to osteopenia (due to a variety of causes such as
osteoporosis and chronic corticosteroid therapy), pyogenic spinal infection, and malignancy. Each of these
can present with similar clinical features; the main challenge for diagnosis of tuberculosis is consideration of
the diagnosis. Most of these conditions can be distinguished with imaging studies where available.
TREATMENT
General approach — Treatment of musculoskeletal tuberculosis consists of antimicrobial therapy. In some
cases, surgical intervention is also warranted.
Antimicrobial therapy — The approach to selection of antituberculous therapy for treatment of
musculoskeletal tuberculosis is generally the same as that for pulmonary tuberculosis. The drug regimen
varies with whether or not the patient has HIV infection or drugresistant tuberculosis. These issues are
discussed in detail separately. (See "Treatment of drugsusceptible pulmonary tuberculosis in HIVuninfected
adults" and "Treatment of pulmonary tuberculosis in HIVinfected adults" and "Treatment and prevention of
drugresistant tuberculosis".)
The optimal duration of therapy for treatment of musculoskeletal tuberculosis is uncertain. For most patients
receiving firstline agents, six to nine months of therapy is sufficient [74]. A longer duration of therapy (9 to 12
months) is warranted for patients on regimens that do not include rifampin and/or for patients with extensive
or advanced disease, particularly if it is difficult to assess the response to therapy [74,75].
Data are limited on the optimal drug regimen and duration for treatment of musculoskeletal infections due to
drugresistant M. tuberculosis. In one small series, 14 of 15 patients were cured with combinedmedical/surgical therapy (eight patients) or medical therapy alone (seven patients). Treatment was continued
for 18 to 24 months; followup ranged from 5 months to 4.5 years [76].
Previously, longer therapeutic courses (12 to 18 months) have been favored for musculoskeletal TB because
of concerns about poor drug penetration into osseous and fibrous tissues. However, several studies have
shown that six to ninemonth regimens containing rifampin are at least as effective as longer courses without
rifampin [7782]. The efficacy of shortercourse therapy is illustrated by the following:
A large prospective cohort study in Hong Kong demonstrated that 6 months of antituberculous therapy
combined with surgery (radical resection of the lesion and insertion of autologous bone grafts) was
comparable in efficacy with 9 to 18 months of antituberculous therapy alone [77].
In three randomized trials of shortcourse chemotherapy for spinal tuberculosis in Hong Kong, India, and
Korea reported after five years of followup, six and ninemonth regimens with isoniazid and rifampin
produced comparable results with 18 months of isoniazid with either ethambutol or paraaminosalicylic
acid [80].

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 6/16
One small retrospective study from the United Kingdom did report a high rate of relapse with a sixmonthcourse of therapy (62 percent); no relapse was observed among patients who received nine months oftreatment [82]. In contrast, a Chinese study reported that, in selected patients and combined with appropriatesurgical intervention, ultrashortcourse therapy of 4.5 months was as successful as a 9month course andassociated with fewer side effects [83].
Surgery — Surgical intervention is warranted for patients in the following circumstances [24,47,84,85]:
Forms of surgical intervention may include decompression, use of hardware for stabilization of spine, abscessdrainage, and/or debridement of infected material [23,85]. For the most part, surgical intervention is safe andsometimes effective in improving neurological deficits; various approaches have been described, dependingon site of infection and related abscess formation [8688]. In some circumstances, reconstructive surgery maybe important once antimicrobial therapy has been completed [5]. Hardware is rarely needed for stabilization ofdebrided bony lesions [89]. Minimally invasive surgical approaches such as videoassisted thoracoscopicanterior surgery have been used successfully to manage patients with neurological symptoms and/orextensive bony destruction involving the thoracic or lumbar spine [90].
The role of surgery in treatment of other presentations of musculoskeletal tuberculosis is not always clear[91]. In one retrospective review of 70 adults with thoracic spinal tuberculosis in India, medical therapy alonewas successful in 69 of 70 patients (mean followup of 40 months) [84]. Criteria for exclusion includedadvanced neurologic deficits, worsening neurologic deficits while on antituberculous therapy, and kyphosisgreater than 40 degrees on presentation. Abscess was observed on presentation in 44 patients (21 of whichwere epidural), and 7 patients had signs of cord compression at the time of presentation. Routine surgicalintervention is not warranted [89,92].
Similar results were noted in a retrospective analysis of 52 children with TB of the knee [93]. The outcome ofmedical therapy without synovectomy was excellent in children who presented with signs and symptoms ofsynovitis as long as the joint space was normal.
Monitoring clinical response — The response to therapy may be monitored by clinical indicators such aspain, constitutional symptoms, mobility, and neurologic findings. The role of inflammatory markers inmonitoring the response to TB therapy is limited. It is not useful to perform serial radiographs sinceradiographic findings may appear to progress during appropriate treatment [94].
In one study of 43 patients with Pott's paraplegia, the most important prognostic factor that predicted sixmonth outcome included muscle power, paraplegia score, sensoryevoked potentials (SEPs), and motorevoked potentials (MEPs) [95]. Patients with mild weakness and lower paraplegia scores were more likely torecover completely by six months than patients with more severe prognostic indicators.
For patients on antituberculous therapy for skeletal TB in the setting of antiretroviral treatment (ART) for HIVinfection, it is important to monitor for immune reconstruction inflammatory syndrome (IRIS). IRIS typicallypresents with paradoxical progression of TB clinical manifestations and constitutional symptoms in the firstfew weeks following initiation of ART. In the setting of skeletal TB, new clinical manifestations may appear
In a randomized trial of 203 Korean patients comparing four different treatment regimens [(1) isoniazidplus rifampin for six months, (2) isoniazid plus rifampin for nine months, (3) isoniazid plus ethambutol orparaaminosalicylic acid for nine months, or (4) isoniazid plus ethambutol or paraaminosalicylic acid for 18months], a favorable outcome was achieved in 77 percent of cases after three years from the start oftherapy; those who received the ninemonth regimen with isoniazid plus ethambutol or paraaminosalicylicacid required additional treatment [81].
Patients with spinal disease and advanced neurological deficitsPatients with spinal disease and worsening neurological deficits progressing while on appropriate therapyPatients with spinal disease and kyphosis >40 degrees at the time of presentationPatients with chest wall cold abscess

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 7/16
and/or resolved manifestations may reappear. IRIS is discussed further separately. (See "Immunereconstitution inflammatory syndrome".)
SOCIETY GUIDELINE LINKS — Links to society and governmentsponsored guidelines from selectedcountries and regions around the world are provided separately. (See "Society guideline links: Diagnosis andtreatment of tuberculosis".)
SUMMARY AND RECOMMENDATIONS
Skeletal tuberculosis (TB) refers to TB involvement of the bones and/or joints. Musculoskeletal TBaccounts for 10 to 35 percent of cases of extrapulmonary tuberculosis and for almost 2 percent of TBcases overall. The proportion of skeletal TB among HIVinfected individuals is comparable with theproportion of skeletal TB among HIVuninfected individuals. (See 'Epidemiology' above.)
Tuberculous spondylitis (Pott's disease) is the most common form of skeletal TB; it usually affects thelower thoracic and upper lumbar region. Infection begins with inflammation of the intervertebral joints andcan spread to involve the adjacent vertebral body. Once two adjacent vertebrae are involved, infectioncan involve the adjoining intervertebral disc space, leading to vertebral collapse. Subsequent kyphosiscan lead to cord compression and paraplegia. (See 'Spondylitis (Pott's disease)' above.)
The most common symptom of tuberculous spondylitis (Pott's disease) is local pain, which increases inseverity over weeks to months, sometimes in association with muscle spasm and rigidity. A characteristicerect posture and "aldermanic" gait may be observed in which the patient walks with short, deliberatesteps to avoid jarring of the spine. Constitutional symptoms such as fever and weight loss are relativelyuncommon. (See 'Spondylitis (Pott's disease)' above.)
Tuberculous arthritis tends to occur in the hip or the knee and is usually monoarticular. Clinicalmanifestations include swelling, pain, and/or loss of joint function that progresses over weeks to months.The joint is generally "cold" (eg, erythema, warmth, and other signs of acute infection are usually absent).(See 'Arthritis' above.)
Tuberculous osteomyelitis can occur in virtually any bone, including the ribs, skull, phalanx, pelvis, andlong bones. Typically, osteomyelitis occurs at a single site. The onset is often insidious but, in rare cases,the onset may be acute or subacute. Tuberculous osteomyelitis frequently presents as a "cold abscess"with swelling, modest erythema or pain, and little or no local warmth. (See 'Osteomyelitis' above.)
The diagnosis of musculoskeletal TB is established by microscopy and culture of infected material.Tissue may be obtained by needle aspiration and/or biopsy; guidance with computed tomography orultrasound to obtain tissue is useful in regions where available. Radiographic imaging can be useful toidentify and establish the anatomy of musculoskeletal TB, although there are no pathognomonicradiographic findings. (See 'Diagnosis' above.)
Treatment of musculoskeletal tuberculosis consists of antituberculous therapy. The approach to selectionof therapy for treatment of musculoskeletal tuberculosis is generally the same as that for pulmonarytuberculosis and is discussed in detail separately. (See "Treatment of drugsusceptible pulmonarytuberculosis in HIVuninfected adults" and "Treatment of pulmonary tuberculosis in HIVinfected adults"and "Treatment and prevention of drugresistant tuberculosis".)
The optimal duration of therapy for treatment of musculoskeletal tuberculosis is uncertain. For patientsreceiving treatment with firstline agents in the absence of extensive or advanced disease, we suggest 6months of therapy (rather than 9 or 12 months) (Grade 2B). A longer duration of therapy (9 to 12months) is warranted for patients on regimens that do not include rifampin and/or for patients withextensive or advanced disease. (See 'Antimicrobial therapy' above.)
Surgical intervention is warranted for patients with spinal disease and advanced neurological deficits orworsening neurological deficits progressing while on appropriate therapy, as well as for patients with

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 8/16
Use of UpToDate is subject to the Subscription and License Agreement.
Topic 7658 Version 24.0
spinal disease and kyphosis >40 degrees at the time of presentation. (See 'Surgery' above.)

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 9/16
GRAPHICS
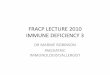
Pott's disease in a young child
A gibbous deformity has occurred as a consequence of collapse of the 8th, 9th, and 10ththoracic vertebral bodies with sparing of the posterior vertebral elements. The paravertebralabscess is extensive projecting laterally and anteriorly (arrows). Bony debris is present in theabscess.
Courtesy of Charles E Putnam, MD.
Graphic 60628 Version 5.0

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 10/16
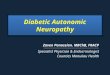
Pott's disease in an adult
Posterioanterior thoracic spine film from a patient with Pott's disease shows thecontours of a tuberculous paraspinal mass (arrows) with destruction of the T78disc space and adjacent vertebral bodies.
Courtesy of Charles E Putnam, MD.
Graphic 72424 Version 5.0

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 11/16
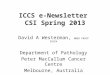
Tuberculosis arthritis
Tuberculous arthritis of the left wrist with destructive changes in the carpalbones (arrow) and radius and prominent soft tissue swelling (arrowhead).
Courtesy of Charles E Putnam, MD.
Graphic 77123 Version 3.0

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 12/16
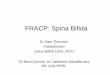
Tuberculosis of the right hip
Plain film of the right hip in a 28yearold woman with painful joints and aproductive cough demonstrates complete loss of the joint space and destructionof the cartilage and adjacent joint surfaces with severe periarticular bonydemineralization (arrows).
Courtesy of Jonathan Kruskal, MD.
Graphic 65352 Version 2.0

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 13/16
Tuberculosis of the spine (Pott's disease)
Magnetic resonance imaging (MRI) with T1weighted fatsaturated image showinganterior vertebral body destruction with relative sparing of adjacent discs and anabscess spreading beneath the anterior longitudinal ligament.
Courtesy of Denis Spelman, MBBS, FRACP, FRCPA, MPH.
Graphic 86251 Version 4.0

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 14/16
Tuberculosis of the spine (Pott's disease)
Magnetic resonance imaging (MRI) of 17yearold fisherman showingtuberculous infection of adjacent thoracic vertebrae with intervening discdestruction and an anterior paraspinal abscess.
Courtesy of Malcolm McDonald, PhD, FRACP, FRCPA.
Graphic 86252 Version 4.0

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 15/16
Tuberculosis of the spine (Pott's disease)
Magnetic resonance imaging (MRI) of 17yearold fisherman (coronal section)showing a large tuberculous paraspinal abscess and pleural involvement.
Courtesy of Malcolm McDonald, PhD, FRACP, FRCPA.
Graphic 86253 Version 4.0

5/6/2017 Skeletal tuberculosis - UpToDate
https://www.uptodate.com/contents/skeletal-tuberculosis/print?source=see_link 16/16
Postsurgical drainage and fixation of spinal tuberculosis(Pott's disease)
Plain film of 17yearold fisherman following surgical drainage and spinalfixation.
Courtesy of Malcolm McDonald, PhD, FRACP, FRCPA.
Graphic 86254 Version 3.0